
PICTORIAL REVIEW MRI of the rotator interval of the shoulder€¦ · · 2012-01-11PICTORIAL...
8
PICTORIAL REVIEW MRI of the rotator interval of the shoulder J.C. Lee a , S. Guy a , D. Connell a , A. Saifuddin a,c, *, S. Lambert b,c Departments of a Radiology and b Orthopaedics, The Royal National Orthopaedic Hospital NHS Trust, Stanmore, Middlesex, UK, and c The Institute of Orthopaedics and Musculoskeletal Sciences, University College London, UK Received 4 July 2006; received in revised form 7 November 2006; accepted 22 November 2006 The rotator interval of the shoulder joint is located between the distal edges of the supraspinatus and subscapularis tendons and contains the insertions of the coracohumeral and superior glenohumeral ligaments. These structures form a complex pulley system that stabilizes the long head of the biceps tendon as it enters the bicipital groove of the humeral head. The rotator interval is the site of a variety of pathological processes including biceps tendon lesions, adhesive capsulitis and anterosuperior internal impingement. This article describes the anatomy, function and patho- logy of the rotator interval using magnetic resonance imaging (MRI). ª 2007 The Royal College of Radiologists. Published by Elsevier Ltd. All rights reserved. Introduction The rotator interval of the shoulder refers to the interspace between the supraspinatus and subsca- pularis tendons through which courses the long head of biceps tendon. Separate terms have been applied to the musculotendinous separation around the coracoid process (anterior rotator interval) and to the separation of the supraspinatus and infraspinatus muscles and their corresponding tendons around the scapular spine (posterior rotator interval). 1 In this paper, the term rotator interval refers to the anterior rotator interval. This article reviews the relevant anatomy, clinical and radiological features of disor- ders of the rotator interval. The normal rotator interval Anatomy The rotator interval subtends a medially based triangular space bordered superiorly by the leading edge of the supraspinatus tendon, inferiorly by the superior aspect of the subscapularis tendon, me- dially by the base of the coracoid process and laterally by the long head of biceps tendon and its sulcus (Fig. 1). Cadaveric and arthroscopic studies have described the macroscopic constituents of the rotator interval. 2e4 The medial rotator interval contains the long head of biceps tendon as it inserts into the superior glenoid labrum. As the biceps tendon passes laterally through the rotator interval, it is covered superficially by fibres of the coracohumeral ligament whilst a condensation of the superior glenohumeral ligament and the joint capsule lie deep to it (Fig. 2). The superior glenohumeral ligament, which arises from the supraglenoid tubercle adjacent to the long head of biceps tendon, inserts into the lesser tuberosity, forming the anterior covering band of the long head of biceps tendon in its sulcus (Fig. 2). The coracohumeral ligament arises from the proximal third of the dorsolateral aspect of the coracoid process and passes through the rotator interval in union with the superior glenohumeral ligament (Figs. 1 and 2). The coracohumeral ligament fibres then fan out laterally to insert into the greater tuberosity and bicipital sheath, as well as fusing with the anterior fibres of supraspinatus and supe- rior fibres of subscapularis tendon insertions. 5 The * Guarantor and correspondent: A. Saifuddin, Department of Radiology, The Royal National Orthopaedic Hospital NHS Trust, Brockley Hill, Stanmore, Middlesex, HA7 4LP, UK. Tel.: þ44 20 8909 5443; fax: þ44 20 8909 5281. E-mail address: [email protected] (A. Saifuddin). 0009-9260/$ - see front matter ª 2007 The Royal College of Radiologists. Published by Elsevier Ltd. All rights reserved. doi:10.1016/j.crad.2006.11.017 Clinical Radiology (2007) 62, 416e423
Transcript of PICTORIAL REVIEW MRI of the rotator interval of the shoulder€¦ · · 2012-01-11PICTORIAL...

Clinical Radiology (2007) 62, 416e423
PICTORIAL REVIEW
MRI of the rotator interval of the shoulder
J.C. Leea, S. Guya, D. Connella, A. Saifuddina,c,*, S. Lambertb,c
Departments of aRadiology and bOrthopaedics, The Royal National Orthopaedic Hospital NHS Trust,Stanmore, Middlesex, UK, and cThe Institute of Orthopaedics and Musculoskeletal Sciences,University College London, UK
Received 4 July 2006; received in revised form 7 November 2006; accepted 22 November 2006
The rotator interval of the shoulder joint is located between the distal edges of the supraspinatus and subscapularistendons and contains the insertions of the coracohumeral and superior glenohumeral ligaments. These structures forma complex pulley system that stabilizes the long head of the biceps tendon as it enters the bicipital groove of thehumeral head. The rotator interval is the site of a variety of pathological processes including biceps tendon lesions,adhesive capsulitis and anterosuperior internal impingement. This article describes the anatomy, function and patho-logy of the rotator interval using magnetic resonance imaging (MRI).ª 2007 The Royal College of Radiologists. Published by Elsevier Ltd. All rights reserved.
Introduction
The rotator interval of the shoulder refers to theinterspace between the supraspinatus and subsca-pularis tendons through which courses the long headof biceps tendon. Separate terms have been appliedto the musculotendinous separation around thecoracoid process (anterior rotator interval) and tothe separationof the supraspinatus and infraspinatusmuscles and their corresponding tendons around thescapular spine (posterior rotator interval).1 In thispaper, the termrotator interval refers to the anteriorrotator interval. This article reviews the relevantanatomy, clinical and radiological features of disor-ders of the rotator interval.
The normal rotator interval
Anatomy
The rotator interval subtends a medially basedtriangular space bordered superiorly by the leading
* Guarantor and correspondent: A. Saifuddin, Department ofRadiology, The Royal National Orthopaedic Hospital NHS Trust,Brockley Hill, Stanmore, Middlesex, HA7 4LP, UK. Tel.: þ44 208909 5443; fax: þ44 20 8909 5281.
E-mail address: [email protected] (A. Saifuddin).
0009-9260/$ - see front matter ª 2007 The Royal College of Radiodoi:10.1016/j.crad.2006.11.017
edge of the supraspinatus tendon, inferiorly by thesuperior aspect of the subscapularis tendon, me-dially by the base of the coracoid process andlaterally by the long head of biceps tendon and itssulcus (Fig. 1).
Cadaveric and arthroscopic studies havedescribed the macroscopic constituents of therotator interval.2e4 The medial rotator intervalcontains the long head of biceps tendon as itinserts into the superior glenoid labrum. As thebiceps tendon passes laterally through the rotatorinterval, it is covered superficially by fibres ofthe coracohumeral ligament whilst a condensationof the superior glenohumeral ligament and thejoint capsule lie deep to it (Fig. 2). The superiorglenohumeral ligament, which arises from thesupraglenoid tubercle adjacent to the long headof biceps tendon, inserts into the lesser tuberosity,forming the anterior covering band of the longhead of biceps tendon in its sulcus (Fig. 2). Thecoracohumeral ligament arises from the proximalthird of the dorsolateral aspect of the coracoidprocess and passes through the rotator interval inunion with the superior glenohumeral ligament(Figs. 1 and 2). The coracohumeral ligament fibresthen fan out laterally to insert into the greatertuberosity and bicipital sheath, as well as fusingwith the anterior fibres of supraspinatus and supe-rior fibres of subscapularis tendon insertions.5 The
logists. Published by Elsevier Ltd. All rights reserved.

MRI of the rotator interval of the shoulder 417
transverse humeral ligament is a broad band thatpasses between the lesser and greater tuberositiesconverting the intertuberculous groove into a canal.The combination of the coracohumeral, superiorglenohumeral and transverse humeral ligaments,
Figure 1 Line drawing of the rotator interval in sagit-tal section. A, acromion process; C, coracoid process;H, humeral head; LHBT, long head of biceps tendon; CHL,coracohumeral ligament; SGHL, superior glenohumeralligament; sst, supraspinatus tendon; sct, subscapularistendon.
Figure 2 Diagrammatic representation of the bicepsreflective pulley system. CHL, coracohumeral ligament;SGHL, superior glenohumeral ligament; C, coracoid pro-cess; LHBT, long head of biceps tendon; H, humeralhead; GT, greater tuberosity; LT, lesser tuberosity.
and the subscapularis tendon insertion, is referredto as the biceps ‘‘reflective pulley’’ or ‘‘sling’’.The principal function of the biceps pulley is to pre-vent medial subluxation of the biceps tendon out ofthe intertuberculous groove during active move-ment and to increase biomechanical efficiencyduring biceps contraction.
Magnetic resonance imaging (MRI) ofthe rotator interval
Standard imaging planes for MRI of the shoulderinclude coronal oblique, sagittal oblique and axialsequences. The oblique sagittal plane, takenparallel to the glenoid fossa and orthogonal tothe long axis of the rotator interval and cuff, is thesingle most valuable sequence to evaluate theinterval and its contents.6 A combination of protondensity and T2-weighted (T2W) spin-echo or turbospin-echo, high-resolution (<3 mm) sequencesusing a high image matrix is recommended.
The capsular component of the normal rotatorinterval passes from the anterior edge of the supra-spinatus tendon to the superior edge of the sub-scapularis tendon and should be thin, smooth and ofuniform low signal intensity on the sagittal obliquesequence (Fig. 3). The capsule may be very thin and
Figure 3 Sagittal oblique PD-weighted fast spin-echoMRI image demonstrating the normal rotator intervalcapsule as a thin, hypointense band (arrows) extendingfrom the anterior margin of supraspinatus to the supe-rior margin of subscapularis. The long head of bicepstendon (long arrow) is identified between the rotatorinterval capsule and the humeral head.

418 J.C. Lee et al.
difficult to discern, and the presence of high signalintensity fluid and/or synovitis will outline thestructure more clearly. The coracohumeral liga-ment is identified as a single or double hypointenseband extending from the posterior aspect of thecoracoid process into the rotator interval (Fig. 4).
The biceps tendon can be identified betweenthe rotator interval capsule and the humeral head(Fig. 3). In the sagittal oblique plane, the medialedge of the long head of biceps tendon lies imme-diately deep to the coracohumeral ligament. Thetransverse humeral ligament, which forms the lat-eral boundary of the rotator interval, is optimallydemonstrated on axial images as a thin hypo-intense line bridging the bicipital groove (Fig. 5).
The superior glenohumeral ligament may bedifficult to define on conventional shoulder MRI,being optimally imaged on axial MR arthrography(MRA; Fig. 6). In fact, some authors believe that allof the structures of the rotator interval are opti-mally imaged using direct MRA. Chung et al.7 per-formed a cadaveric study comparing standard MRIand MRA on the same shoulder. The authors foundthat only the extra-articular portion of the longhead of biceps tendon was seen in all cases onstandard MRI whilst on direct MRA, the intra-articular course of the long head of biceps tendoncould also be reliably identified (Fig. 7). In the studyof Chung et al., the superior glenohumeral ligamentwas not identified at all on standard MRI sequencesand the coracohumeral ligament was seen in only60% of the specimens, whereas both ligamentswere seen in all cases on MRA. Chung et al. alsorecommended a dedicated sequence perpendicularto the coracohumeral ligament/superior glenohum-eral ligament complex to fully evaluate thesestructures and the long head of biceps tendon. In
our experience, this extra sequence frequentlyadds little to the diagnosis. Isolated rupture of therotator interval capsule may be missed on axialand coronal oblique planes and should be assessedon the sagittal oblique acquisition.8
Function and clinical lesions of therotator interval
The rotator interval is a defined anatomical spacebut its constituent parts play several importantroles in the shoulder. Instability of the long head ofbiceps tendon and the glenohumeral joint, as wellas synovial changes in adhesive capsulitis, are allrecognized pathological processes that involve therotator interval.
Long head of biceps tendon abnormalities
Pulley lesionsThe biceps pulley is formed by the intimatearrangement between the coracohumeral, superiorglenohumeral and transverse humeral ligamentsplus the subscapularis tendon, as mentioned above(Fig. 2). These structures act together to form themedial wall of the superior biceps pulley preventingmedial subluxation of the long head of biceps ten-don. It is important to note that biceps instabilitymay be due to avulsion of the superior glenohumeralligament/coracohumeral ligament complex, as wellas the more widely recognized tear of the subscapu-laris tendon.
Disorders of the biceps tendon are optimallyimaged using a combination of axial and sagittalT2W sequences.9 Biceps tendon subluxation is
Figure 4 (a) Sagittal oblique T2W fast spin-echo sequence demonstrating the normal coracohumeral ligament asa thin, hypointense band (arrowhead) extending from the posterior aspect of the coracoid process to the rotatorinterval. The ligament is surrounded by fat. (b) Axial T2*W gradient echo. (c) Coronal PD-weighted fast spin-echosequences demonstrating the normal coracohumeral ligament (arrows).

MRI of the rotator interval of the shoulder 419
diagnosed when the tendon is seen to lie on themedial ridge of the bicipital sulcus (Fig. 8) whilsta dislocated tendon may lie within the subscapula-ris tendon (Fig. 9) or come to lie anterior to thesubscapularis tendon.10 Lesions of the reflectionpulley of the biceps tendon have also been de-scribed with MRA and features include irregularityof the superior margin of the subscapularis tendon,extra-articular contrast collection and biceps ten-don subluxation.11
In one arthroscopic study of ‘‘hidden’’ rotatorinterval lesions in patients with supraspinatus ten-don tears, there was a 27% incidence of subscapu-laris tears and 47% of these were associated withinvolvement of the superior glenohumeral ligament
Figure 5 Axial T2*W gradient echo MRI image demon-strating the transverse humeral ligament (long arrow)bridging the bicipital groove and covering the longhead of biceps tendon (short arrows). Note also the sub-scapularis tendon (arrowhead).
Figure 6 Axial T1W fat-suppressed direct MR arthro-gram demonstrating the superior glenohumeral ligament(arrow).
and medial fibres of the coracohumeral ligament.12
Ten percent of supraspinatus tendon tears wereassociated with involvement of the lateral fibresof the coracohumeral ligament. Therefore, retrac-tion of the subscapularis must infer at least a partialtear of the coracohumeral ligament.
Figure 7 Coronal oblique T1W fat-suppressed directMR arthrogram demonstrating the entire length of theintra-articular portion of the long head of biceps tendon(arrowheads).
Figure 8 Axial PD-weighted fast spin-echo MRI imagedemonstrating a partial articular side tear of the subsca-pularis tendon with subluxation of the long head ofbiceps tendon (arrow), which is lying on the medial ridgeof the proximal aspect of the bicipital groove.
420 J.C. Lee et al.
Biceps tendinopathy and tendon tearsDegenerative changes within the biceps tendon arecommonly associated with rotator cuff tears.13
Biceps tendinopathy is diagnosed when there isincreased intra-tendinous signal intensity withina swollen long head of biceps tendon (Fig. 10),and is commonly with associated with synovitisand adhesions within the tenosynovial sheath. Par-tial or complete tears of the long head of bicepstendon tendon are associated with tears of the sub-scapularis and supraspinatus tendons and are iden-tified on conventional MRI with a reported accuracyof 79%.14 Partial tears are diagnosed when thereis either a longitudinal region of increased intra-tendinous signal intensity reaching the edge of anon-expanded tendon, or when there is an abruptchange in diameter of the long head of biceps ten-don on serial axial images. The lack of biceps ten-don swelling may distinguish partial tears fromtendinopathy, but occasionally, it may not be possi-ble to separate the two conditions on MRI. A com-plete tear of the long head of biceps tendon willmanifest as an empty biceps tendon sheath.
Anterosuperior internal impingementAnterosuperior internal impingement is a recentlydescribed condition in which there is shoulder painprovoked by anterior elevation and internal rota-tion of the glenohumeral joint, with no symptoms orsigns of instability.15 Depending upon the degree ofelevation of the arm, impingement occurs betweenthe long head of biceps tendon and pulley regionwith the superior most aspect of the labrum, or
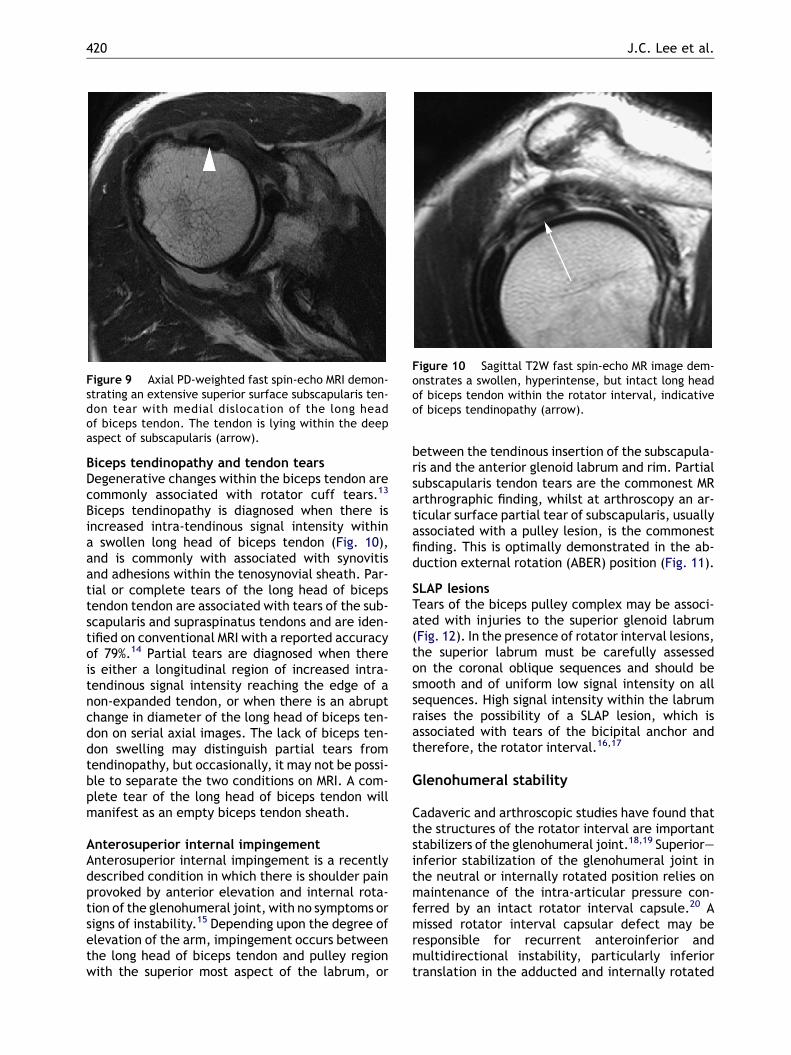
Figure 9 Axial PD-weighted fast spin-echo MRI demon-strating an extensive superior surface subscapularis ten-don tear with medial dislocation of the long headof biceps tendon. The tendon is lying within the deepaspect of subscapularis (arrow).
between the tendinous insertion of the subscapula-ris and the anterior glenoid labrum and rim. Partialsubscapularis tendon tears are the commonest MRarthrographic finding, whilst at arthroscopy an ar-ticular surface partial tear of subscapularis, usuallyassociated with a pulley lesion, is the commonestfinding. This is optimally demonstrated in the ab-duction external rotation (ABER) position (Fig. 11).
SLAP lesionsTears of the biceps pulley complex may be associ-ated with injuries to the superior glenoid labrum(Fig. 12). In the presence of rotator interval lesions,the superior labrum must be carefully assessedon the coronal oblique sequences and should besmooth and of uniform low signal intensity on allsequences. High signal intensity within the labrumraises the possibility of a SLAP lesion, which isassociated with tears of the bicipital anchor andtherefore, the rotator interval.16,17
Glenohumeral stability
Cadaveric and arthroscopic studies have found thatthe structures of the rotator interval are importantstabilizers of the glenohumeral joint.18,19 Superioreinferior stabilization of the glenohumeral joint inthe neutral or internally rotated position relies onmaintenance of the intra-articular pressure con-ferred by an intact rotator interval capsule.20 Amissed rotator interval capsular defect may beresponsible for recurrent anteroinferior andmultidirectional instability, particularly inferiortranslation in the adducted and internally rotated
Figure 10 Sagittal T2W fast spin-echo MR image dem-onstrates a swollen, hyperintense, but intact long headof biceps tendon within the rotator interval, indicativeof biceps tendinopathy (arrow).

MRI of the rotator interval of the shoulder 421
arm. Sectioning of the rotator interval capsule incadaveric shoulder joints was found to increaseranges of flexion, extension, adduction and exter-nal rotation.21 Conversely, imbrication of the cap-sule reduced the ranges of all these movements.If a rotator interval defect is not closed in a patientwith instability, along with the normal capsulorra-phy, then there may be recurrent postoperativesymptoms.18,19,21 Detecting and closing a rotatorinterval defect arthroscopically may be difficultas the rotator interval is regularly used as the ante-rior portal in shoulder arthroscopy, reducing thechance of discovering lesions of this area.
Type I and II rotator interval lesionsNobuhara and Ikeda first described the term‘‘rotator interval lesion’’ as a cause of painfulshoulder syndrome characterized by inferiorinstability in the rotator interval.22 The authorsdefined two sub-types: type I, a contracted state,is characterized by a superficial post-inflammatorycontraction of the coracohumeral ligament andsubacromial bursa following an injury to the rota-tor interval. It is possible, with the acceptancethat the rotator interval is predominantly responsi-ble for superioreinferior stability, that the type I
Figure 11 T2W fast spin-echo direct MR arthrogram inthe abduction external rotation (ABER) position showingsimpingement (curved arrow) between the insertion ofsubscapularis (straight arrow) and the anterosuperioraspect of the glenoid labrum (arrowhead).
lesion described by these authors is in fact partof the emerging syndrome of sub-coracoid im-pingement (Fig. 13).23 The type II lesion occurs ina younger patient group, and is characterized byinstability with inflammatory change within thedeeper tissues of the rotator interval.
Figure 12 Coronal oblique fat-suppressed T1W fastspin-echo direct MR arthrogram image demonstrating adetached tear of the superior glenoid labrum (arrow)extending into the longheadofbiceps tendon (arrowhead).
Figure 13 Axial T2W GE image obtained in internal ro-tation showing marked reduction in the space betweenthe lesser tuberosity (long arrow) and the tip of thecoracoid process (short arrow) with hyperintensity ofthe intervening subscapularis tendon.

422 J.C. Lee et al.
Adhesive capsulitis
Primary myofibroblastic transformation is thoughtto initiate contracture of the coracohumeral liga-ment component of the rotator interval tissue inthe early stages of idiopathic frozen shoulder(adhesive capsultitis).24 As the rotator intervalshortens in the mediolateral and craniocaudaldirections the relative gliding of the anterior mar-gin of the supraspinatus tendon and the cranialmargin of the subscapularis tendon is restrictedand external rotation range is diminished. In at-tempted external rotation the humeral head isthen obligatorily displaced downward and back-ward. In attempted sagittal plane flexion the hu-meral head is displaced inferiorly: the thickenedinterval tissue can obstruct further elevation byoccupying the subcoracoid space.
Mengiardi et al. described a coracohumeralligament thickness greater than 4 mm on sagittaloblique MR arthrographic images as a specificsign of adhesive capsulitis.25 MRI may also showthickening of the rotator interval capsule and exu-berant synovitis surrounding the coracohumeralligament, which may enhance after intravenousgadolinium injection (Fig. 14).26
Figure 14 Sagittal oblique T1W fast spin-echo MR imagedemonstrating enhancing soft-tissue (arrowheads) sur-rounding the coracohumeral ligament (straight arrow),extending towards the intra-articular portion of longhead of biceps tendon (curved arrow).
Conclusion
The rotator interval is a complex anatomicalregion, which can give rise to a variety of clinicalsymptoms and signs. The imaging features ofrotator interval lesions are also variable and themost subtle rotator interval lesions, consisting ofsmall tears of the deep surface of the subscapu-laris tendon or leading edge of the supraspinatustendon may easily be overlooked on conventionalMRI unless particular attention is given to thisregion.
References
1. Miller SL, Gladstone JN, Cleeman E, et al. Anatomy of theposterior rotator interval: implications for cuff mobilisa-tion. Clin Orthop 2003;408:152e6.
2. Jost B, Koch PP, Gerber C. Anatomy and functional aspectsof the rotator interval. J Shoulder Elbow Surg 2000;9:336e41.
3. Bennett WF. Technical note: visualisation of the anatomy ofthe rotator interval and bicipital sheath. Arthroscopy 2001;17:107e11.
4. Clark J, Sidles JA, Matsen FA. The relationship of the gleno-humeral joint capsule to the rotator cuff. Clin Orthop 1990;254:29e34.
5. Agur AMR. Grant’s Atlas of Anatomy. Baltimore: Williamsand Wilkins; 1992.
6. Ho CP. MR imaging of the rotator interval, long biceps andassociated injuries in the overhead-throwing athlete.Magn Reson Imaging Clin N Am 1999;7:23e37.
7. Chung CB, Dwek JR, Cho GJ, et al. Rotator cuff interval:evaluation with MR imaging and MR arthrography of theshoulder in 32 cadavers. J Comput Assist Tomogr 2000;24:738e43.
8. Seeger LL, Lubowitz J, Thomas BJ. Tear of the rotator inter-val. Skeletal Radiol 1993;22:615e17.
9. Nidecker A, Guckel C, von Hochstetter A. Imaging the longhead of biceps tendonda pictorial essay emphasizing mag-netic resonance. Eur J Radiol 1997;25:177e87.
10. Cervilla V, Schweitzer ME, Ho C, et al. Medial dislocationof the biceps brachii tendon: appearance at MR imaging.Radiology 1991;180:523e6.
11. Bennett WF. Subscapularis, medial and lateral head coraco-humeral ligament insertion anatomy: arthroscopic anatomyand incidence of ‘‘hidden’’ rotator interval lesions. Arthro-scopy 2001;17:173e80.
12. Weishaupt D, Zanetti M, Tanner A, et al. Lesions of thereflection pulley of the long biceps tendon. MR arthro-graphic findings. Invest Radiol 1999;34:463e9.
13. Murthi AM, Vosburgh CL, Neviaser TJ. The incidence ofpathologic changes of the long head of the biceps tendon.J Shoulder Elbow Surg 2000;9:382e5.
14. Beall DP, Williamson EE, Ly JQ, et al. Association of bicepstendon tears with rotator cuff abnormalities: degree ofcorrelation with tears of the anterior and superiorportions of the rotator cuff. AJR Am J Roentgenol 2003;180:633e9.
15. Gerber C, Sebesta A. Impingement of the deep surface ofthe subscapularis tendon and the reflection pulley on theanterosuperior glenoid rim: a preliminary report. J ShoulderElbow Surg 2000;9:483e90.

MRI of the rotator interval of the shoulder 423
16. Beltran J, Jbara M, Maimon R. Shoulder: labrum and bicipi-tal tendon. Top Magn Reson Imaging 2003;14:35e49.
17. Bencardino JT, Beltran J, Rosenberg ZS, et al. Superiorlabrum anterioreposterior lesions: diagnosis with MR arthro-graphy of the shoulder. Radiology 2000;214:267e71.
18. Cole BJ, Rodeo SA, O’Brien SJ, et al. The anatomy andhistology of the rotator interval of the shoulder. Clin Orthop2001;390:129e37.
19. Field LD, Warren RF, O’Brien SJ, et al. Isolated closure ofrotator interval defects for shoulder instability. Am J SportsMed 1995;23:557e63.
20. Harryman DT, Sidles JA, Harris SL, et al. The role ofthe rotator interval capsule in passive motion and stabilityof the shoulder. J Bone Joint Surg Am 1992;74-A:53e66.
21. Itoi E, Berglund LJ, Grabowski JJ, et al. Superioreinferiorstability of the shoulder: role of the coracohumeral
ligament and the rotator interval capsule. Mayo Clin Proc1998;73:508e15.
22. Nobuhara K, Ikeda H. Rotator interval lesion. Clin Orthop1987;223:44e50.
23. Giaroli EL, Major NM, Lemley DE, et al. Coracohumeralinterval imaging in subcoracoid impingement on MRI. AJRAm J Roentgenol 2006;186:242e6.
24. Bunker TD, Anthony PP. The pathology of frozen shoulder:a Dupuytren-like disease. J Bone Joint Surg Br 1995;77:677e83.
25. Mengiardi B, Pfirrmann CWA, Gerber C, et al. Frozenshoulder: MR arthrographic findings. Radiology 2004;233:486e92.
26. Connell D, Padmanabhan R, Buchbinder R. Adhesive capsu-litis: role of MR imaging in differential diagnosis. Eur Radiol2002;12:2100e6.


















