Pictorial Essay: Multinodular Disease: A High-Resolution CT Scan … · 2015. 7. 28. · such as...
13
DOI 10.1378/chest.129.3.805 2006;129;805-815 Chest P. Naidich Suhail Raoof, Alexey Amchentsev, Ioannis Vlahos, Ajay Goud and David Algorithm High-Resolution CT Scan Diagnostic Pictorial Essay: Multinodular Disease: A http://chestjournal.org/cgi/content/abstract/129/3/805 and services can be found online on the World Wide Web at: The online version of this article, along with updated information ). ISSN: 0012-3692. http://www.chestjournal.org/misc/reprints.shtml ( of the copyright holder may be reproduced or distributed without the prior written permission Northbrook IL 60062. All rights reserved. No part of this article or PDF by the American College of Chest Physicians, 3300 Dundee Road, 2007 Physicians. It has been published monthly since 1935. Copyright CHEST is the official journal of the American College of Chest Copyright © 2006 by American College of Chest Physicians on April 15, 2008 chestjournal.org Downloaded from
Transcript of Pictorial Essay: Multinodular Disease: A High-Resolution CT Scan … · 2015. 7. 28. · such as...

DOI 10.1378/chest.129.3.805 2006;129;805-815 Chest
P. Naidich Suhail Raoof, Alexey Amchentsev, Ioannis Vlahos, Ajay Goud and David
AlgorithmHigh-Resolution CT Scan Diagnostic Pictorial Essay: Multinodular Disease: A
http://chestjournal.org/cgi/content/abstract/129/3/805and services can be found online on the World Wide Web at: The online version of this article, along with updated information
). ISSN: 0012-3692. http://www.chestjournal.org/misc/reprints.shtml(of the copyright holder may be reproduced or distributed without the prior written permission Northbrook IL 60062. All rights reserved. No part of this article or PDFby the American College of Chest Physicians, 3300 Dundee Road,
2007Physicians. It has been published monthly since 1935. Copyright CHEST is the official journal of the American College of Chest
Copyright © 2006 by American College of Chest Physicians on April 15, 2008 chestjournal.orgDownloaded from

Pictorial Essay: Multinodular Disease*A High-Resolution CT Scan Diagnostic Algorithm
Suhail Raoof, MD, FCCP; Alexey Amchentsev, MD; Ioannis Vlahos, MD;Ajay Goud, MD; and David P. Naidich, MD, FCCP
The evaluation of patients presenting with multinodular pulmonary disease provides an impor-tant clinical challenge for physicians. The differential diagnosis includes an extensive list ofbenign and malignant processes making the management of these cases frequently problematic.With the introduction of high-resolution CT (HRCT) scanning, the ability to assess variouspatterns of diffuse multinodular disease has evolved into an essential part of the diagnosticprocess. The purpose of this article is to develop an approach to the diagnosis of multinodularparenchymal disease using HRCT scan pattern recognition as a point of departure.
(CHEST 2006; 129:805–815)
Key words: algorithm; multinodular; multiple nodules
Abbreviations: HP � hypersensitivity pneumonitis; HRCT � high-resolution CT; ILD � interstitial lung disease;LCH � Langerhans cell histiocytosis; LIP � lymphocytic interstitial pneumonitis; RB � respiratory bronchiolitis
F or the purposes of this report, multinodulardisease will be defined in a patient in which
there are too many nodules to easily count on routineCT scan studies, with most of these nodules measur-ing � 1 cm in diameter. While the most commoncause of multiple pulmonary nodules is metastaticdisease, it is apparent that this definition encom-passes a wide range of lung diseases, both benign andmalignant. It is our contention that use of a dedi-cated diagnostic algorithm1 based on characteristichigh-resolution CT (HRCT) scan features coupledwith clinical findings can provide either a specific
diagnosis or a markedly shortened list of differentialdiagnoses in a majority of patients presenting withdiffuse lung nodules.
Algorithm Overview
Due to its ability to evaluate the lung parenchymain cross-section, eliminating the superimposition ofdensities, CT scanning offers a unique opportunity toevaluate lung nodules in exquisite detail.2 This in-cludes first the ability to assess lesions by anatomicdistribution, and second by morphology.3–5
Anatomic Localization
This includes the consideration of the followingpatterns: diffuse vs focal or clustered; central (peri-bronchovascular) vs peripheral (subpleural or peri-fissural); and upper vs lower lung distribution. Mostimportantly, nodules also need to be characterizedby their relation to secondary lobular anatomy allow-ing a distinction between centrilobular nodules andthose that predominantly involve the lobular periph-ery, including the interlobular septa3–5 (Fig 1).
For example, diseases such as sarcoidosis thatlocalize within or adjacent to lymphatics predomi-
*From the Division of Pulmonary and Critical Care Medicine(Drs. Raoof and Amchentsev), New York Methodist Hospital,Brooklyn, NY; the Department of Radiology (Drs. Vlahos andNaidich), Tisch Hospital, New York University Medical Center,New York, NY; and the Department of Radiology (Dr. Goud),Brigham and Women’s Hospital, Boston, MA.No financial or other potential conflicts of interest exist for any ofthe authors.Manuscript received January 9, 2006; revision accepted January14, 2006.Reproduction of this article is prohibited without written permissionfrom the American College of Chest Physicians (www.chestjournal.org/misc/reprints.shtml).Correspondence to: Suhail Raoof, MD, FCCP, Chief, Pulmonaryand Critical Care Medicine, Medical Director, Respiratory Ther-apy Department, New York Methodist Hospital, PulmonaryDivision, 506 Sixth St, Brooklyn, NY 11215; e-mail:[email protected]
CHEST Chest Imaging for Clinicians
www.chestjournal.org CHEST / 129 / 3 / MARCH, 2006 805
Copyright © 2006 by American College of Chest Physicians on April 15, 2008 chestjournal.orgDownloaded from

nate in those regions in which lymphatics are mostextensive, specifically along the pleural and fissuralsurfaces, within the interlobular septae, and alongthe peribronchovascular axial interstitium (Fig 2).Diseases that are primarily hematogenous in origin,such as miliary infections or hematogenous metasta-ses, give rise to nodules that are randomly distrib-uted throughout the secondary lobule, with thegreatest profusion in the lung bases (Fig 3). Thesepatterns are clearly separate from nodules that resultfrom inhalational disorders such as occur in patientswith endobronchial spread of infection or hypersen-sitivity pneumonitis (HP), in which nodules arepredominantly centrilobular in distribution, sparingthe lobular periphery (Fig 4, 5).
Morphologic Characterization
This includes assessing a number of characteristicsincluding whether nodules are as follows: uniform orvariable in size; sharply or poorly marginated6–8;solid or subsolid in density (so-called ground-glassopacities) [Fig 5]5; or have a so-called tree-in-budappearance (Fig 4).9 Additionally, nodules may ei-ther be calcified, as occurs in fungal disease, orcavitary, as is seen, for example, in patients withseptic emboli, metastatic disease, or Langerhans cellhistiocytosis (LCH).10
It should be emphasized that many of thesecharacteristics are best evaluated on high-resolutionCT scan images. With the introduction of multide-tector CT scanners, it is now possible to routinely,prospectively reconstruct both thick and thin sec-tions through the lungs after a single breathhold,provided that the initial data are acquired usingappropriately thin collimation. This approach alsoenables the use of high-definition, multiplanar re-constructions, the use of which may be of value infurther characterizing lung nodules.11
Multinodular HRCT Algorithm: A Step-Wise Approach
The use of this algorithm begins by dividing CTscans into two broad arms based on the presence(group 1) or absence (group 2) of pleural or perifis-sural involvement (Table 1).
Step 1
Group 1: Those cases in which a striking propor-tion of nodules demonstrate pleural or perifissuralinvolvement characterize nodules as predominantlyperilymphatic or lymphohematogenous in origin,constituting a separate arm of the algorithm (Table1). The explanation for this pattern lies in the greaterdensity of lymphatic channels seen in the interlobu-
Figure 1. Secondary lobular anatomy. A side-by-side diagram-matic representation of two normal secondary pulmonary lobules.Secondary lobules represent fundamental anatomic units of thelung and are defined by centrilobular structures, includingpulmonary arteries/arterioles and their accompanying bronchi/bronchioles, and peripheral structures, including the pulmonaryveins and lymphatics within the interlobular septae. As shown,most of these structures are � 1 mm in size and therefore, withthe exception of the centrilobular arteries, lie below the resolu-tion of even HRCT scans. Most importantly, note that centri-lobular structures do not extend to the pleural or interlobularseptal surfaces. As will be illustrated, knowledge of basic lobularanatomy is the key to differentiating between different etiologiesof diffuse pulmonary nodules.
Figure 2. Perilymphatic disease. A diagrammatic representationof the characteristic distribution of lung nodules in patients withperilymphatic disease. Note that nodules are preferentially sub-pleural, peribronchovascular within the axial interstitium, oralong lobular septae. While this appearance is especially charac-teristic of nodular sarcoidosis, less commonly a similar patternmay also be seen in patients with silicosis or coal-workerspneumoconiosis.
806 Chest Imaging for Clinicians
Copyright © 2006 by American College of Chest Physicians on April 15, 2008 chestjournal.orgDownloaded from

lar septa and subpleural regions, including along thefissures.
Step 2
Once nodules are characterized as predominantlyperilymphatic or lymphohematogenous in origin,further assessment requires determining whether ornot nodules are distributed diffusely or are patchy orclustered, with particular attention paid to the pres-ence or absence of the extent of axial interstitialinvolvement. It is recalled that the axial interstitiumenvelops the main pulmonary vessels and bronchiextending from the hilum outward toward the lungperiphery.12
Step 3
If nodules prove to be clustered in a predomi-nantly subpleural/axial distribution, they are deemedto be perilymphatic in distribution (Fig 2). In thiscategory, the main disease to be considered is sar-coidosis (Fig 6, 7).2,13,14 This diagnosis is furthersuggested by nodules that are typically ill-defined,frequently measuring only a few millimeters in size.Clusters of these nodules often have a “grainy”appearance and when sufficiently profuse may resultin an appearance of poorly defined nodules ormasses on corresponding chest radiographs (so-
Figure 4. Bronchiolar disease. A diagrammatic representation ofthe typical appearance of bronchiolar inflammation resulting inso-called tree-in-bud opacities. These characteristically result inclusters of ill-defined nodules “attached” to adjacent branching ortubular structures due to extensive bronchiolar mucoid impac-tion. Most importantly, note that, unlike the situation in patientswith either perilymphatic disease or random nodules, mucoidimpacted bronchioles do not extend to the pleural, fissural, orseptal surface. This pattern is nearly always due to infectedsecretions resulting from virtually any cause of acute or subacutebronchiolar infection.
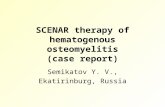
Figure 3. Random nodules. A diagrammatic representation ofthe characteristic distribution of randomly distributed nodules inpatients with lymphohematogenous disease. Note that in distinc-tion with patients having predominantly perilymphatic disease,random nodules may been seen adjacent to all secondary lobularstructures. Some nodules may also appear to be attached topulmonary arterial branches (so-called feeding vessels). Randomnodules are most commonly due to metastatic disease, and mayvary considerably in size and edge characteristics. The differentialdiagnosis most importantly includes miliary infection. Lym-phangitic carcinomatosis, while hematogenous in origin, is easilydistinguished from random metastatic nodules by the presence ofcharacteristically thickened interlobular septae, preferentiallyinvolving the lung bases, and usually associated with asymmetrichilar adenopathy and pleural effusions.
Figure 5. Centrilobular disease. A diagrammatic representationof the distribution of diseases that predominantly affect thecentrilobular portion of secondary lobules, excluding those dis-eases that result in predominantly mucoid impaction due toinfected secretions. The most common cause of diffuse centri-lobular disease is subacute HP. This characteristically results inpoorly defined, poorly marginated ground-glass opacities. Similarto tree-in-bud opacities, these rarely involve the pleural orfissural surfaces. While a number of different entities may resultin predominantly centrilobular opacities, the differential diagno-sis most often includes RB/RB-ILD. In distinction with subacuteHP, RB in particular is less extensive, typically upper lobe indistribution, and almost always occurs in smokers.
www.chestjournal.org CHEST / 129 / 3 / MARCH, 2006 807
Copyright © 2006 by American College of Chest Physicians on April 15, 2008 chestjournal.orgDownloaded from

called alveolar sarcoid). When coalescent, these maysimulate progressive massive fibrosis. Ancillary find-ings include a predominant upper lobe distribution,focal air-trapping due to bronchiolar obstruction,and diffuse adenopathy, often calcified. Calcifiednodules may also be present in later stages of thedisease.
The most important differential diagnoses for thispattern of disease are silicosis and coal workerpneumoconiosis.15,16 In both of these occupationaldiseases, perilymphatic nodules are the primary ab-normality, typically involving the mid and upper lungfields. While these entities may simulate the appear-ance of sarcoidosis, they are usually easily diagnosedwhen correlated with clinical history.15 This includesother rare occupational lung disease, for example,siderosis, that may also simulate the appearance ofsarcoidosis.17
While lymphangitic carcinomatosis may result inperilymphatic nodules, in fact, CT scan findings aremost often characterized by markedly thickenednodular interlobular septae usually asymmetricallyinvolving the lower lobes and usually associated withadenopathy and effusions.18 Nodules, when present,tend more often to be well-defined and are oftenassociated with discrete feeding vessels, furtheridentifying them as hematogenous in origin. Lym-phangitic carcinomatosis rarely mimics findings thatare characteristic of sarcoidosis.
Step 4
If nodules prove to be diffuse instead of clustered,they are properly considered to be random in distri-bution (Table 1). By definition, true random distri-bution will lead to nodules being identified alongpleural and fissural surfaces as well as along the axial
Figure 6. Perilymphatic disease: sarcoidosis. An HRCT scan ofa 1-mm section at the level of the carina shows innumerableill-defined small nodules clustered in the mid-portions of bothlungs with relative sparing of the anterior aspects of both upperlobes. Note that these preferentially involve the left major fissure(arrow on left lung) as well as the walls of the peripheral airways(curved arrow on right lung).
Table 1—HRCT Algorithm for Multinodular Disease*
* CWP � coal workers pneumoconiosis; MAI � M avium intracellulare; MTB � M tuberculosis; PMF � progressive massive fibrosis.
808 Chest Imaging for Clinicians
Copyright © 2006 by American College of Chest Physicians on April 15, 2008 chestjournal.orgDownloaded from

interstitium. However, in distinction from primarilyperilymphatic disease, random nodules may also beidentified in even greater numbers when dispersedrandomly throughout the lungs.
Included in this category most importantly arehematogenous metastases.19 Unlike nodules in pa-tients with sarcoidosis, metastatic nodules tend to besmooth, well-defined lesions (Fig 8, 9).8 However, awide variety of morphologic appearances has beennoted. In a study20 comparing the HRCT scanfeatures of pulmonary metastatic lesions with au-topsy findings, while nodules most often proved tohave well-defined margins (38% of cases), noduleswith well-defined irregular margins, poorly definedsmooth margins, and poorly defined irregular mar-gins could be identified in 16%, 16%, and 30% ofcases, respectively. While nodules range from a few
millimeters to � 1 cm, they are frequently similar insize. A basilar predominance is typically noted due topreferential blood flow to the lung bases. Individualnodules may have “feeding vessels” consistent withtheir hematogenous origin. On HRCT scans, a con-nection between nodules and the adjacent pulmo-nary vessels (ie, the mass-vessel sign) may be seen inapproximately 75% of cases.21 Nodules may also beeither cavitary or surrounded by a “halo” of ground-glass attenuation, which is typical of hemorrhagicmetastases such as those due to choriocarcinoma.22
Features of lymphangitic cancer may also be present,which again is consistent with a hematogenous originof disease.19
It should be noted that the reported incidence ofmalignant disease as a cause of multiple pulmonarynodules has been shown to vary greatly, from as lowas 10% to as high as 58% in some surgical series.23 In133 patients with a known malignancy who under-went video-assisted thoracoscopy for multiple pul-monary nodules, 64% proved to have at least onemalignant nodule.24 A number of malignancies canresult in a miliary pattern, rendering differentialdiagnosis more problematic. This includes tumors,such as renal cell carcinoma, head and neck cancers,and testicular tumors, that have their primary venousdrainage in the lungs.25
The differential diagnosis includes a number ofadditional entities that result in random nodules. Themost important of these is miliary infection (Fig10).26,27 In fact, while differentiation between miliaryinfection and a miliary tumor may be impossible todetermine by imaging features alone, in general,close correlation with the clinical history rendersthese diagnoses relatively straightforward. Miliarymetastases are frequently due to metastatic thyroidcancer, renal cancer, and melanoma, among othercancers, while larger less profuse metastases tend tobe adenocarcinomas in adults, typically originatingfrom the lung, breast, or the GI tract.19,28 Lesscommonly, diffuse nodules may be identified inpatients with septic emboli, invasive fungal infec-tions, and pulmonary vasculitides.29 These entitiesfrequently result in cavitary nodules, some with adistinct “halo” of ground-glass attenuation,22 andhave even been described in patients with organizingpneumonia.30 Despite similarities between these en-tities and routine metastatic disease, it should beemphasized that the numbers of nodules identifiedin these cases usually fail to meet the criterion of “toomany nodules to count,” with the differential diag-nosis again further aided by close clinical correlation.
Step 5Group 2: In distinction with the patterns de-
scribed in patients in group 1, group 2 includes those
Figure 7. Perilymphatic disease: sarcoidosis. An HRCT scan ofa 1-mm section through the right mid-lung in a different patientthan the one in Figure 6 shows evidence of innumerableill-defined small nodules. Note that these tend to be clusteredwith relative sparing of the right upper lobe anteriorly and clearlypreferentially lie adjacent to the right major fissure (arrow), alongpleural surfaces, and along central vascular structures (arrow-heads). This distribution of nodules is rarely seen in any otherdisease.
www.chestjournal.org CHEST / 129 / 3 / MARCH, 2006 809
Copyright © 2006 by American College of Chest Physicians on April 15, 2008 chestjournal.orgDownloaded from

patients in whom no or very few nodules are perifis-sural or subpleural in distribution. Anatomically,these nodules are grouped together as being centri-lobular in distribution.4 By definition, these entitiesprimarily involve centrilobular bronchioles and/ortheir accompanying pulmonary artery branches. An-atomically, these structures taper peripherally, stop-ping 5 to 10 mm short of the pleural or interlobularseptal surfaces and consequently fail to involve pleu-ral and fissural surfaces (Table 1). As will be dis-cussed, these nodules typically fall into the followingtwo broad categories: those with a “tree-in-bud”configuration; and those that appear as amorphous“ground-glass” nodules.
Step 6
Once nodules are characterized as being primarilycentrilobular in distribution, further assessment re-quires determining whether or not these have atree-in-bud configuration. Tree-in-bud opacities arecharacterized by the appearance of centrilobularmicronodular branching structures that end severalmillimeters distant from nearby pleural or fissuralsurfaces (Fig 11).31
Tree-in-bud opacities are nearly always the result
of inspissated (ie, frequently aspirated) secretionslodged within centrilobular bronchioles, accountingfor a branching configuration when coursing parallelto the CT scan plane.9,32,33 Normal bronchioles,which have a diameter of � 1 mm and a wallthickness of � 0.1 mm, are below the limit of HRCTscan spatial resolution.34 The presence of inspissatedsecretions results in bronchiolar distension and in-creased density, allowing their direct visualization.Not surprisingly, in many cases there is also evidenceof coexisting bronchiectasis. Another frequently en-countered finding in patients with bronchiolar dis-ease is so-called mosaic attenuation.33 In these cases,bronchiolar occlusion results in air-trapping, hypoxiaof the poorly ventilated lung units with resultantreflex vasoconstriction and air-trapping. This combi-nation of findings causes decreased attenuation ofthe affected areas of the lung with blood flowredistributed to normal lung. The hypoattenuateddiseased lung is therefore surrounded by hyperat-tenuated, overperfused normal lung, resulting inheterogeneous-appearing mosaic attenuation.
While classically described in patients with anendobronchial spread of tuberculosis, in fact, tree-in-bud opacities can be identified in virtually any
Figure 8. Random nodules: hematogenous metastases. An HRCT scan of a 1-mm section through thelower lobes shows innumerable sharply defined nodules throughout both lungs. Note that while manyof these lie along pleural and fissural surfaces, or less commonly appear related to adjacent vessels(arrows), most are unattached to adjacent structures. When sufficiently well defined and generallyuniform in size, this pattern of diffuse nodularity is easily separable from that resulting fromperilymphatic disease.
810 Chest Imaging for Clinicians
Copyright © 2006 by American College of Chest Physicians on April 15, 2008 chestjournal.orgDownloaded from

type of infectious bronchiolitis. This includes Myco-bacterium tuberculosis, Mycobacterium avium-intra-cellulare, bacterial, viral, and fungal infections, andallergic bronchopulmonary mycosis. This pattern isalso frequently encountered in patients with AIDS inwhom recurrent episodes of bronchial infection arefrequent.35 Differential diagnosis also includes follic-ular bronchiolitis, an entity that is characterized bythe presence of hyperplastic lymphoid follicles andgerminal centers occurring along the bronchovascu-lar bundles.36
Most often, infectious bronchiolitis results in clus-ters of tree-in-bud opacities. When they are wide-spread and diffuse, the differential diagnosis in-cludes “Asiatic panbronchiolitis.”37,38 This entity hasa well-established predilection in Japanese, Chinese,and Korean populations, appears to show a geneticpredisposition, and is usually seen in association withchronic sinusitis. Diffuse tree-in-bud opacities arealso frequently encountered in patients with cysticfibrosis and viral bronchiolitis.
It cannot be overemphasized that in the vastmajority of cases the finding of tree-in-bud opacitiesshould be taken as being indicative of bronchiolarinfection. While tree-in-bud opacities have beendescribed39 as occurring in patients with pulmonaryvascular tumor emboli, in our experience this entity
is exceedingly rare. As noted in one retrospectivestudy9 of 141 patients with a variety of airwaydiseases, including bronchiolitis obliterans, bronchi-olitis obliterans-organizing pneumonia, HP, respira-tory bronchiolitis (RB), and pneumonia, among oth-ers, the finding of tree-in-bud opacities wasidentified in association only with pneumonia and/orbronchiectasis in 17% and 25% of cases, respectively.Even in patients with panbronchiolitis, while noconsistent infectious agent has been associated withthis disease, interestingly, most individuals respond,at least initially, to low-dose erythromycin thera-py.38,40 Some authors41 have suggested that thetherapeutic efficacy of macrolide agents may ema-nate from their inhibition of proinflammatory cyto-kines, and from mucus and water secretion fromairway epithelial cells.
Step 7
Those cases in which centrilobular nodules arepresent in patients in the absence of tree-in-budopacities constitute the last part of this CT scanalgorithm (Table 1). Included in this category are avariety of diseases or “mixed” entities that have incommon localization to the centrilobular portion ofthe secondary lobule. This includes diseases that
Figure 9. Random nodules: metastatic thyroid cancer. An HRCT scan of a 1-mm section through themid-thorax shows innumerable small nodules. Note that, in addition to unattached nodules, many ofthese lie along both the minor and right major fissures (arrows), as well as along the proximal middlelobe pulmonary artery (arrowheads). Although there are fewer nodules than shown in Figure 8, in theappropriate clinical stetting this pattern is again consistent with metastatic disease.
www.chestjournal.org CHEST / 129 / 3 / MARCH, 2006 811
Copyright © 2006 by American College of Chest Physicians on April 15, 2008 chestjournal.orgDownloaded from

primarily affect the centrilobular bronchiole, as wellas those that are either primarily peribronchiolar orperivascular in origin.2,4,5
Most often, this group of diseases results in apattern of diffuse, poorly defined ground-glass nod-ules, which are typically the result of a primarilyperibronchiolar distribution. The classic example ofthis appearance is subacute HP (Fig 12).42,43 Thisdiagnosis is frequently first suggested on the basis ofCT scan findings and is usually established by acombination of exposure history, clinical symptomsof a flu-like illness, the presence of specific serumantibodies when those data are available, increasednumbers of lymphocytes and neutrophils in BALfluid, and, when feasible, clinically significant im-provement in symptoms when the patient is removedfrom the offending environmental agent.44
The differential diagnosis encompasses a numberof important disease entities, most importantly in-cluding RB, lymphocytic interstitial pneumonitis(LIP), and LCH. RB/RB-interstitial lung disease(ILD) are smoking-related disorders that may alsoresult in poorly defined centrilobular nodules.45,46
RB typically results in far fewer ground-glass nodulesthan the number in patients with subacute HP andgenerally display a distinctly upper lobe predomi-nance. RB-ILD is associated with widespreadground-glass attenuation and reticular opacities,which are findings that are not seen in patients withsubacute HP.45,46
Also included in the differential diagnosis of indi-viduals with diffuse centilobular nodules are diseasesrelated to bronchiolar lymphatics. This includes mu-
Figure 10. Random nodules: miliary tuberculosis. A magnifiedHRCT scan image through the right upper lobe shows innumer-able tiny nodules throughout the lungs extensively involving thepleural surfaces (black arrowheads) and along bronchovascularstructures (arrows). Numerous unattached nodules are also iden-tifiable. This pattern is typical of a random, miliary distribution.While typically resulting from either metastatic disease or infec-tion, clinical correlation is usually diagnostic. Case courtesy ofNestor Muller, MD, Vancouver, BC, Canada.
Figure 11. Bronchiolar disease: infectious bronchiolitis. A mag-nified HRCT scan image through the middle and lower lobesshows numerous nodules associated with linear/branching densi-ties throughout the lungs (arrows). These tree-in-bud opacitiesare the result of infected mucoid impacted peripheral airwaysand hence have a distinctly centrilobular pattern of distribution.Note that none of these peripherally is in contact with eitherpleural or fissural surfaces. Classically the result of the endobron-chial spread of tuberculosis, this pattern may be seen in virtuallyany patient in whom there is infection of the peripheral airways.Not surprisingly, tree-in-bud opacities tend to be clustered ratherthan truly diffuse and frequently are associated with CT scanevidence of bronchiectasis.
812 Chest Imaging for Clinicians
Copyright © 2006 by American College of Chest Physicians on April 15, 2008 chestjournal.orgDownloaded from

cosa-associated lymphoid tissue lymphoma (malto-mas) and, in particular, LIP. LIP is most often seenin patients with underlying immunologic abnormal-ities, especially Sjogren syndrome and AIDS, and ischaracterized histologically by diffuse hyperplasia ofbronchus-associated lymphatic tissue, resulting in adiffuse, polyclonal lymphoid cell infiltrate surround-ing the airways and expanding the lung intersti-tium.47,48 As reported by Johkoh et al,48 in a study of22 patients with documented LIP, while subpleuralnodules could be identified in 86% of cases, likelyreflecting subpleural lymphatic involvement, poorlydefined centrilobular nodules could be seen in 100%of cases. Additional imaging features include thepresence of thickened bronchovascular bundles and,
in particular, the presence of randomly distributedthin-walled cysts.47 Poorly defined centrilobular nod-ules may also be seen early in the course of LCH.49,50
However, these most often are associated with char-acteristic bizarrely shaped, thick walled cysts, someof which represent cavitary nodules with character-istic sparing of the lung bases.51
Conclusion
The finding of multiple lung nodules is a charac-teristic that encompasses a number of disparateparenchymal diseases. Although inexact, the use ofanatomic and morphologic features to characterizenodules based on HRCT scan findings may help tosimplify the differential diagnosis. Most importantly,the use of this imaging algorithm can prove to be anaid in standardizing the clinical approach to differ-ential diagnosis. In a study reported by Gruden etal,4 four experienced chest radiologists indepen-dently evaluated HRCT scan images in 58 patientswith diffuse nodular disease. In each case, observerswere asked to place nodules in one of the followingfour possible anatomic locations or categories: peri-lymphatic; random; associated with small airwaysdisease (ie, cases in which the primary abnormalitywas tree-in-bud opacities); or centrilobular disease.There was agreement among all four observers in79% of cases, while three of four observers agreed onan additional 17%. Observers were correct (based onsubsequent histologic/clinical correlation) in 218 of232 localizations (94%) in the 58 cases. These datasuggest that this algorithm, which has been elabo-rated on in the present report, represents a repro-ducible method for categorizing patients with diffusepulmonary nodules.
It should also be noted that, in individual cases,HRCT scan findings may be sufficiently characteris-tic, especially when coupled with close clinical cor-relation, to obviate the need to perform a biopsy.Patients with classic HRCT scan findings of sarcoid-osis, as well as those with subacute HP for whichbiopsy confirmation may not be required, should beincluded in this category. In patients with a knownhistory of smoking, the finding of scattered, tiny,ill-defined centrilobular upper lobe nodules is suffi-ciently characteristic to warrant a clinical diagnosis ofRB, obviating the need for more invasive diagnosticprocedures, while the finding of scattered centri-lobular opacities associated with bizarrely shapedcysts predominantly involving the upper lobes spar-ing the lung bases is characteristic of LCH. Similarly,the finding of characteristic tree-in-bud opacities inthe appropriate clinical setting may be taken asdiagnostic of small airway-bronchiolar infection. In
Figure 12. Centrilobular disease: subacute HP. A magnifiedHRCT scan section through the right upper lobe shows innu-merable poorly defined, hazy ground-glass nodules throughoutthe lung (arrows). In addition to a uniform distribution, none ofthese nodules lies adjacent to the visualized pleural surfaces.Note as well the lack of any tree-in-bud opacities that wouldsuggest the presence of mucoid impacted airways (compare withFig 11). Few entities besides subacute HP result in this patternof ill-defined nodules. Differential diagnoses includes RB, typi-cally causing fewer nodules restricted to the upper lobes inknown smokers, and LIP, which is usually associated with eitherSjogren syndrome or AIDS.
www.chestjournal.org CHEST / 129 / 3 / MARCH, 2006 813
Copyright © 2006 by American College of Chest Physicians on April 15, 2008 chestjournal.orgDownloaded from

distinction, the appearance of diffuse, poorly definedcentrilobular nodules in the absence of a clinicalhistory of established antigen exposure, infection, ora history of smoking generally requires open-lungbiopsy for definitive evaluation. Given the widediversity of potential causes for this appearance, theuse of an HRCT scan algorithm should be consid-ered an important, if not fundamental, component ofclinical assessment in these cases.
References1 Webb WR, Muller NL, Naidich DP. 3rd ed. Philadelphia,
PA: Lippincott, Williams and Wilkins, 20012 Colby TV, Swensen SJ. Anatomic distribution and histopatho-
logic patterns in diffuse lung disease: correlation with HRCT.J Thorac Imaging 1996; 11:1–26
3 Bergin C, Roggli V, Coblentz C, et al. Secondary pulmonarylobule: normal and abnormal CT appearance. AJR Am JRoentgenol 1988; 151:21–25
4 Gruden JF, Webb WR, Warnock M. Centrilobular opacitieson HRCT: diagnosis and differential diagnosis with patho-logic correlation. AJR Am J Roentgenol 1994; 162:569–574
5 Murata K, Itoh H, Todo G, et al. Centrilobular lesions of thelung: demonstration by high resolution CT and pathologiccorrelation. Radiology 1986; 161:641–645
6 Muller NL, Kullnig P, Miller RR. The CT findings ofpulmonary sarcoidosis: analysis of 25 patients. AJR Am JRoentgenol 1989; 152:1179–1182
7 Lee KS, Song KS, Lim TH, et al. Adult onset of pulmonarytuberculosis: findings on chest radiographs and CT scans. AJRAm J Roentgenol 1993; 160:753–758
8 Hirikata K, Nakata H, Haratake J. Appearance of pulmonarymetastases on high-resolution CT scans: comparison withhistopathologic findings from autopsy specimens. AJR Am JRoentgenol 1993; 161:37–43
9 Aquino SL, Gamsu G, Webb WR, et al. Tree-in-bud pattern:frequency and significance on thin-section CT. J ComputAssist Tomogr 1996; 20:594–599
10 Moore AD, Godwin JD, Muller NL, et al. Pulmonary histio-cytosis X: comparison of radiographic and CT findings.Radiology 1989; 172:249–254
11 Revel M-P, Lefort C, Bissery A, et al. Pulmonary nodules:preliminary experience with three-dimensional evaluation.Radiology 2004; 231:459–466
12 Weibel ER, Taylor CR. Design and structure of the humanlung. In: Weibel ER, Taylor CR, eds. Pulmonary diseases anddisorders. New York, NY: McGraw-Hill, 1988; 11–60
13 Brauner MW, Grenier P, Mompoint D, et al. Pulmonarysarcoidosis: evaluation with high-resolution CT. Radiology1989; 172:467–471
14 Nishimura K, Itoh H, Kitaichi M, et al. Pulmonary sarcoid-osis: correlation of CT and histopathologic findings. Radiol-ogy 1993; 172:467–471
15 Remy-Jardin M, Remy J, Farre L, et al. Computed tomo-graphic evaluation of silicosis and coal worker’s pneumoconi-osis. Radiol Clin North Am 1992; 30:115–1176
16 Ooi GC, Tsang KWT, Cheung TF, et al. Silicosis in 76 men:qualitative and quantitative CT evaluation- clinical-radiologiccorrelation study. Radiology 2003; 228:816–825
17 Kim KI, Kim CW, Lee MK, et al. Imaging of occupationallung disease. Radiographics 2001; 21:1371–1391
18 Johkoh T, Icfhikado Kea J, Tomiyama N, et al. CT findings inlymphangitic carcinomatosis of the lung: correlation with
histologic findings and pulmonary function tests. AJR Am JRoentgenol 1992; 158:1217–1222
19 Aquino SL. Imaging of metastatic disease to the thorax.Radiol Clin North Am 2005; 43:481–495
20 Hirakata K, Nakata H, Haratake J. Appearance of pulmonarymetastases on high-resolution CT scans: comparison withhistopathologic findings from autopsy specimens. AJR Am JRoentgenol 1993; 161:37–43
21 Milne ENC, Zerhouni EA. Blood supply of pulmonarymetastases. J Thorac Imaging 1987; 2:15–23
22 Gaeta M, Blandino A, Scribano E, et al. Computed tomog-raphy halo sign of pulmonary nodules: frequency and diag-nostic value. J Thorac Imaging 1999; 14:109–113
23 Benjamin MS, Drucker EA, McLoud T, et al. Small pulmo-nary nodules: detection at chest CT and outcome. Radiology2003; 226:489–493
24 Ginsberg MS, Griff SK, Go BD, et al. Pulmonary nodulesresected at video-assisted thorascopic surgery: etiology in 426patients. Radiology 1999; 213:277–282
25 Patz EF, Fidler J, Knelson M, et al. Significance of percuta-neous needle biopsy in patients with multiple pulmonarynodules and a single known primary malignancy. Chest 1995;107:601–604
26 Muller NL, Fraser RS, Lee KS, et al. Pulmonary infection. In:Diseases of the lung. Philadelphia, PA: Lippincott, Williamsand Wilkins, 2003; 17–75
27 McGuinness G, Naidich DP, Jagardar J, et al. High resolutionCT findings in miliary lung disease. J Comput Assist Tomogr1992; 16:384–390
28 Seo JB, Im J-G, Goo JM, et al. Atypical pulmonary metasta-ses: spectrum of radiologic findings. Radiographics 2001;21:403–417
29 Silva CIS, Muller NL, Fujimoto K, et al. Churg-Strausssyndrome: high resolution CT and pathologic findings. J Tho-rac Imaging 2005; 20:74–80
30 Haro M, Vizcaya M, Texido A, et al. Idiopathic bronchiolitisobliterans organizing pneumonia with multiple cavitary nod-ules. Eur Respir J 1995; 8:1975–1977
31 Collins J, Blankenbaker D, Stern EJ. CT patterns of bron-chiolar disease: what is “tree-in-bud”? AJR Am J Roentgenol1998; 171:365–370
32 Colby TV. Bronchiolitis: pathologic considerations. Am J ClinPathol 1998; 109:101–109
33 Hartman TE, Primack SL, Lee KS, et al. CT of bronchial andbronchiolar disease. Radiographics 1994; 14:991–1003
34 Webb WR, Muller NL, Naidich DP. Normal lung anatomy.In: High-resolution CT of the lung. Philadelphia, PA: Lippin-cott, Williams and Wilkins, 2001; 49–70
35 McGuinness G, Gruden JF, Bhalla M, et al. AIDS-relatedairways disease. AJR Am J Roentgenol 1997; 168:67–77
36 Ryu JH, Myers JH, Swensen SJ. Bronchiolar disorders: stateof the art. Am J Respir Crit Care Med 2003; 168:1277–1292
37 Akira M, Kitatani F, Lee YS, et al. Diffuse panbronchiolitis:evaluation with high resolution CT. Radiology 1988; 168:433–438
38 Nishimura K, Kitaichi M, Izumi T, et al. Diffuse panbronchi-olitis: correlation of high resolution CT and pathologic find-ings. Radiology 1992; 184:779–785
39 Shepard JO, Moore EH, Templeton PA, et al. Pulmonaryvascular tumor emboli: dilated and beaded peripheral pulmo-nary arteries at CT. Radiology 1993; 187:797–801
40 Kudoh S. Erythromycin treatment in diffuse panbronchiolitis.Curr Opin Pulm Med 1998; 4:116–121
41 Baz MA, Kussin PS, Van Trigt P, et al. Recurrence of diffusepanbronchiolitis after lung transplantation. Am J Respir CritCare Med 1995; 151:895–898
42 Lynch DA, Rose CS, Way D, et al. Hypersensitivity pneumo-
814 Chest Imaging for Clinicians
Copyright © 2006 by American College of Chest Physicians on April 15, 2008 chestjournal.orgDownloaded from

nitis: sensitivity of high resolution CT in a population-basedstudy. AJR Am J Roentgenol 1992; 159:469–472
43 Hansell DM, Wells AU, Padley SP, et al. Hypersensitivitypneumonitis: correlation of individual CT patterns with func-tional abnormalities. Radiology 1996; 199:123–128
44 Selman M. Hypersensitivity pneumonitis: a multifaceted de-ceiving disorder. Clin Chest Med 2004; 25:531–547
45 Yousem SA, Colby TV, Gaensler EA. Respiratory bronchioli-tis-associated interstitial lung disease and its relationship todesquamative interstitial pneumonia. Mayo Clin Proc 1989;64:1373–1380
46 Heyneman LE, Ward S, Lynch DA, et al. Respiratorybronchiolitis, respiratory bronchiolitis-associated interstitialpneumonia: different entities or part of the spectrum of thesame disease? AJR Am J Roentgenol 1999; 173:1617–1622
47 Honda O, Johkoh T, Icfhikado K, et al. Differential diagnosisof lymphocytic interstitial pneumonia and malignant lym-phoma on high-resolution CT. AJR Am J Roentgenol 1999;173:71–74
48 Johkoh T, Muller NL, Pickford HA, et al. Lymphocyticinterstitial pneumonia: thin section CT findings in 22 patients.Radiology 1999; 212:567–572
49 Brauner MW, Grenier P, Mouelhi MM, et al. Pulmonaryhistiocytosis X: evaluation with high-resolution CT. Radiology1989; 172:255–258
50 Kulwiec EL, Lynch DA, Aguayo SM, et al. Imaging ofpulmonary histiocytosis X. Radiographics 1992; 12:515–526
51 Howarth DM, Gilchrist GS, Mullan BP, et al. Langerhans cellhistiocytosis: natural history, management, and outcome.Cancer 1999; 85:2278–2290
www.chestjournal.org CHEST / 129 / 3 / MARCH, 2006 815
Copyright © 2006 by American College of Chest Physicians on April 15, 2008 chestjournal.orgDownloaded from

DOI 10.1378/chest.129.3.805 2006;129;805-815 Chest
Naidich Suhail Raoof, Alexey Amchentsev, Ioannis Vlahos, Ajay Goud and David P.
Diagnostic AlgorithmPictorial Essay: Multinodular Disease: A High-Resolution CT Scan
This information is current as of April 15, 2008
& ServicesUpdated Information
http://chestjournal.org/cgi/content/full/129/3/805high-resolution figures, can be found at: Updated information and services, including
References
http://chestjournal.org/cgi/content/full/129/3/805#BIBLfor free at: This article cites 47 articles, 33 of which you can access
Citations
http://chestjournal.org/cgi/content/full/129/3/805articles: This article has been cited by 1 HighWire-hosted
Permissions & Licensing
http://chestjournal.org/misc/reprints.shtml(figures, tables) or in its entirety can be found online at: Information about reproducing this article in parts
Reprints http://chestjournal.org/misc/reprints.shtml
Information about ordering reprints can be found online:
Email alerting service
online article. article sign up in the box at the top right corner of the Receive free email alerts when new articles cite this
Images in PowerPoint format
format. See any online article figure for directions. downloaded for teaching purposes in PowerPoint slide Figures that appear in CHEST articles can be
Copyright © 2006 by American College of Chest Physicians on April 15, 2008 chestjournal.orgDownloaded from