
Challenges in the diagnosis & treatment of miliary ... · Key words Complications - diagnosis -...
28
Challenges in the diagnosis & treatment of miliary tuberculosis Surendra K. Sharma, Alladi Mohan * & Abhishek Sharma ** Department of Medicine, All India Institute of Medical Sciences, New Delhi, * Division of Pulmonary, Critical Care & Sleep Medicine, Department of Medicine, Sri Venkateswara Institute of Medical Sciences, Tirupati, India & ** University of Medicine, Pleven, Bulgaria Received August 2, 2011 Miliary tuberculosis (TB) is a potentially lethal disease if not diagnosed and treated early. Diagnosing miliary TB can be a challenge that can perplex even the most experienced clinicians. Clinical manifestations are nonspecific, typical chest radiograph findings may not be evident till late in the disease, high resolution computed tomography (HRCT) shows randomly distributed miliary nodules and is relatively more sensitive. Ultrasonography, CT and magnetic resonance imaging (MRI) are useful in discerning the extent of organ involvement by lesions of miliary TB in extra-pulmonary locations. Fundus examination for choroid tubercles, histopathological examination of tissue biopsy specimens, conventional and rapid culture methods for isolation of Mycobacterium tuberculosis, drug-susceptibility testing, along with use of molecular biology tools in sputum, body fluids, other body tissues are useful in confirming the diagnosis. Although several prognostic markers have been described which predict mortality, yet untreated miliary TB has a fatal outcome within one year. A high index of clinical suspicion and early diagnosis and timely institution of anti-tuberculosis treatment can be life-saving. Response to first-line anti-tuberculosis drugs is good but drug-induced hepatotoxicity and drug-drug interactions in human immunodeficiency virus/ acquired immunodeficiency syndrome (HIV/AIDS) patients pose significant problems during treatment. However, sparse data are available from randomized controlled trials to define the optimum regimen and duration of treatment in patients with drug-sensitive as well as drug-resistant miliary TB, including those with HI/AIDS. Key words Complications - diagnosis - human immunodeficiency virus - miliary tuberculosis - treatment 703 Review Article Introduction In 1700, John Jacob Manget 1 described a form of disseminated tuberculosis (TB) and likened the tiny tubercles evident on gross pathological examination to that of innumerable millet seeds in size and appearance. He coined the term miliary TB (derived from the Latin word miliarius, meaning related to millet seed) to denote this fatal form of disseminated TB. Miliary TB results from a massive lymphohaematogeneous dissemination from a Mycobacterium tuberculosis- laden focus 2-4 (Fig. 1). Miliary TB still remains a perplexing disease that continues to elude the most erudite and experienced clinicians and is a diagnostic and therapeutic challenge. Mortality from this disease has remained high despite effective therapy being available. The myriad clinical Indian J Med Res 135, May 2012, pp 703-730
-
Upload
nguyenliem -
Category
Documents
-
view
216 -
download
0
Transcript of Challenges in the diagnosis & treatment of miliary ... · Key words Complications - diagnosis -...
Challengesinthediagnosis&treatmentofmiliarytuberculosis
SurendraK.Sharma,AlladiMohan*&AbhishekSharma**
Department of Medicine, All India Institute of Medical Sciences, New Delhi, *Division of Pulmonary, Critical Care & Sleep Medicine, Department of Medicine, Sri Venkateswara Institute of Medical Sciences, Tirupati, India & **University of Medicine, Pleven, Bulgaria
ReceivedAugust2,2011
Miliary tuberculosis (TB) is a potentially lethal disease if not diagnosed and treated early. Diagnosing miliary TB can be a challenge that can perplex even the most experienced clinicians. Clinical manifestations are nonspecific, typical chest radiograph findings may not be evident till late in the disease, high resolution computed tomography (HRCT) shows randomly distributed miliary nodules and is relatively more sensitive. Ultrasonography, CT and magnetic resonance imaging (MRI) are useful in discerning the extent of organ involvement by lesions of miliary TB in extra-pulmonary locations. Fundus examination for choroid tubercles, histopathological examination of tissue biopsy specimens, conventional and rapid culture methods for isolation of Mycobacterium tuberculosis, drug-susceptibility testing, along with use of molecular biology tools in sputum, body fluids, other body tissues are useful in confirming the diagnosis. Although several prognostic markers have been described which predict mortality, yet untreated miliary TB has a fatal outcome within one year. A high index of clinical suspicion and early diagnosis and timely institution of anti-tuberculosis treatment can be life-saving. Response to first-line anti-tuberculosis drugs is good but drug-induced hepatotoxicity and drug-drug interactions in human immunodeficiency virus/acquired immunodeficiency syndrome (HIV/AIDS) patients pose significant problems during treatment. However, sparse data are available from randomized controlled trials to define the optimum regimen and duration of treatment in patients with drug-sensitive as well as drug-resistant miliary TB, including those with HIV/AIDS.
Key words Complications-diagnosis-humanimmunodeficiencyvirus-miliarytuberculosis-treatment
703
Review Article
Introduction
In1700,JohnJacobManget1describedaformofdisseminated tuberculosis (TB) and likened the tinytuberclesevidentongrosspathologicalexaminationtothatofinnumerablemilletseedsinsizeandappearance.He coined the term miliary TB (derived from theLatinwordmiliarius,meaningrelated tomilletseed)todenotethisfatalformofdisseminatedTB.Miliary
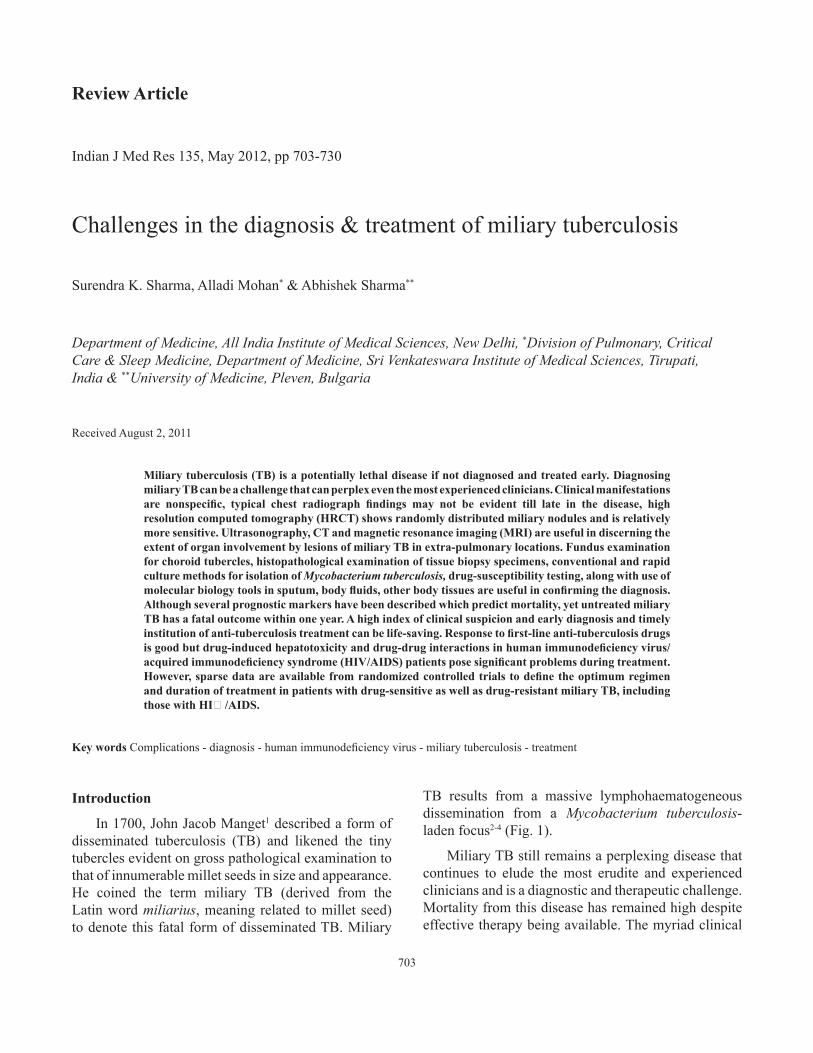
TB results from a massive lymphohaematogeneousdissemination from a Mycobacterium tuberculosis-ladenfocus2-4(Fig.1).
MiliaryTBstillremainsaperplexingdiseasethatcontinues to elude themost erudite and experiencedcliniciansandisadiagnosticandtherapeuticchallenge.Mortalityfromthisdiseasehasremainedhighdespiteeffectivetherapybeingavailable.Themyriadclinical
IndianJMedRes135,May2012,pp703-730
704 INDIANJMEDRES,May 2012
denominatorsused, lackof a“gold standard” for thediagnosisandvariationinthenatureofinvasivemethodsusedforsecuringtissuetoconfirmthediagnosis,sparseautopsydataregardingmiliaryTBinchildrencertainconclusionscanbedrawnregardingtheepidemiologyof miliary TB. Among immunocompetent adults,miliaryTBaccountsforlessthan2percentofallcasesofTB and up to 20 per cent of all extra-pulmonaryTB(EPTB)casesinvariousclinicalstudies5-12.InlateHIV infection,EPTB accounts formore than 50 percent of all cases of TB4. In autopsy studies13-19, thecorresponding figures have been higher; miliary TBaccountsfor0.3 to13.3percentofallautopsiesand11.9 to 40.5 per cent of all cases ofTB. In the pre-antibioticera,miliaryTBwaspredominantlyadiseaseof infants and children20,21. Currently, two peaks areevident- one involving adolescents and young adultsandanotherlaterinlifeamongelderlypersons4,9,11,22-44.MalesseemtobemorefrequentlyaffectedbymiliaryTBinpaediatricaswellasadultseries4,9,11,22-44.Afewrecent adult series on miliary TB9,19,29,33 describe afemale preponderance probably reflecting increasedawarenessandutilizationofhealthservicesbywomen. In USA, a higher incidence ofmiliary TB has beendescribedinAfricanAmericansinsomeoftheearlierpublications though such a trend is not evident fromrecentdata4,24,34.
Predisposing, associated conditions
Severalpredisposingorassociatedconditionshavebeen described in patients with miliary TB. These
Fig. 1.Chestradiograph(postero-anteriorview)(A) andchestCT(lungwindow)(B)showingclassicalmiliarypattern.
manifestations, atypical radiographic findings anddifficulties in establishing TB as the aetiologicaldiagnosis, among others, are challenges in diagnosisandtreatmentofmiliaryTB(TableI).
In this review, we first provide an overviewregarding the epidemiology, current understandingof key pathogenetic mechanisms, molecular basis ofdissemination,predisposingandassociatedconditions,the varied clinical manifestations that have beendocumentedinmiliaryTB,andthenthechallengesinthediagnosisandtreatmentofmiliaryTBareaddressed.
Burden of the problem
Mortality from this disease has remained highdespite effective therapy being available. For along time, miliary TB has been considered to be achildhood disease. However, during the last threedecades, it is increasinglybeing recognized inadultsaswell.Severalreasonsarethoughttoberesponsiblefor this changing epidemiological trend. Theseinclude: human immunodeficiency virus/acquiredimmunodeficiency syndrome (HIV/AIDS), everincreasing list of causes of immunosuppression,such as use of biologicals and immunosuppressivedrugs for treatment of various medical disorders,increasingoccurrenceoforgantransplantation,chronichaemodialysisprogramme,amongothers.
Interpretation of published epidemiological dataonmiliaryTBishamperedbycertainmethodologicalissues.Evenaftergivingallowancefornon-availabilityofcommunitybaseddataontheprevalence,different
includechildhoodinfections,malnutrition,HIV/AIDS,alcoholism,diabetesmellitus,chronickidneydisease,dialysis, post-gastrectomy, organ transplantation,connective tissue disorders, pregnancy, postpartum,presenceofanunderlyingmalignancy,andsilicosis4.However,theirpathogeneticsignificanceisnotclear.
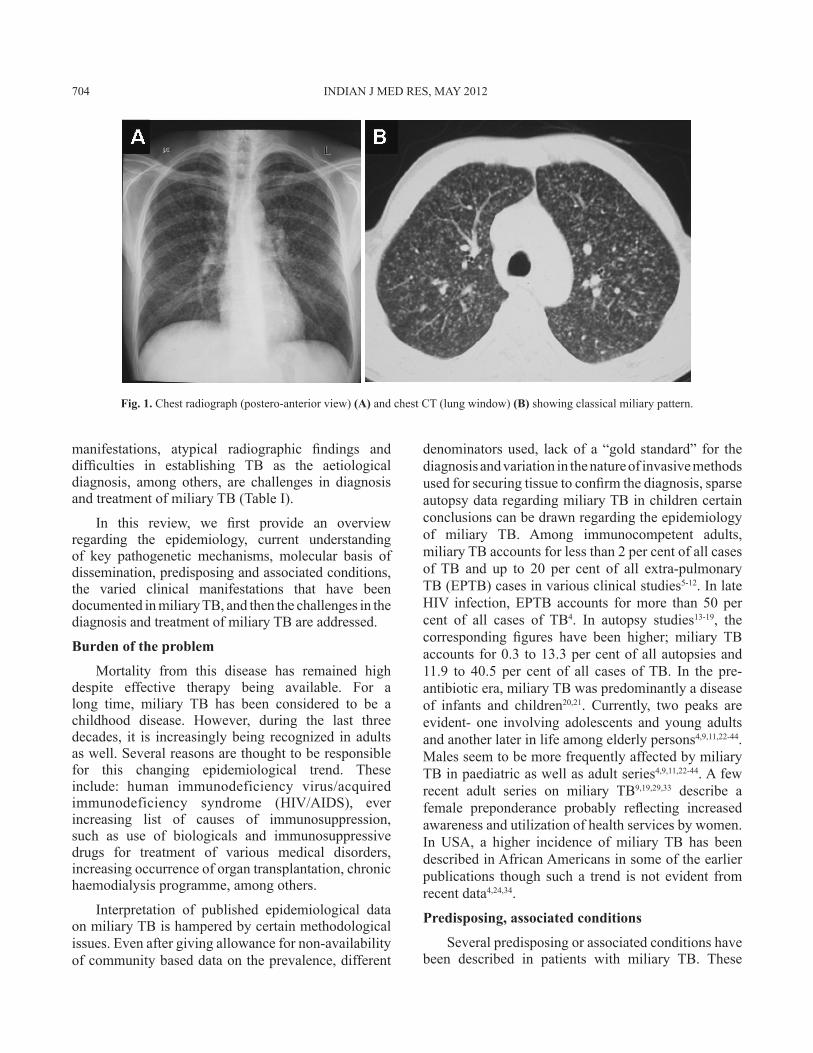
Inadditiontocorticosteroids,immunosuppressiveand cytotoxic drugs are known to predispose to thedevelopmentofmiliaryTB,useofimmunomodulatordrugs(biologicals)hasbeendocumentedtocausefatalTB including miliary TB in rheumatoid arthritis45-48.Theseincludeanti-tumournecrosisfactor(TNF)agentsinfliximab48,etanercept47,andadalimumab46.Inarecentprospective study amongpatientswho received anti-TNF therapy45, EPTB constituted 62 per cent of allcasesofTB;disseminatedandmiliaryTBaccountedfor27.5percentofallTBcases,44percentofextra-pulmonaryTB. The rate of development of TBwashigher for adalimumab and infliximab than foretanercept.ThemediantimetodevelopmentofTBwaslowest for infliximab compared with etanercept andadalimumab (Table II). Patients with non-white
ethnicityhada6-foldhigherriskofTBcomparedwithwhitepatients45.
Several procedures and interventions have beenimplicatedinthecausationofmiliaryTB.Theseincludeureteral catheterization, extracorporeal shockwavelithotripsy, laser lithotripsy, cardiac valve homograftreplacement, intravesical bacille Calmette-Guerin(BCG)therapyforurinarybladdercarcinoma49-53.
Table II. RiskofdevelopingmiliaryTBwiththeuseofanti-TNFagentsinpatientswithrheumatoidarthritisVariable Infliximab Adalimumab Etanercept
RateofdevelopmentofmiliaryTB(events/100,000person-years)
136 144 39
MediantimetodevelopmentofTB(months)
5.5 18.5 13.4
TB,tuberculosis;TNF,tumournecrosisfactorDatafromreference45
Table I.WhymiliaryTBisachallengefordiagnosisandtreatment?Cliniciansmaynotbefamiliarwiththeatypicalpresentation(s),suchas,presentationwithnormalchestradiograph,abnormal•behaviourinTBmeningitis,hyponatraemia,ARDS,andskinmanifestations,etc.Fundusexaminationfollowingmydriaticadministrationmaynotbearoutinepracticeinhealthcarefacilities.•Patientsmaybetoosicktoundergovariousinvestigations.•Patientsgenuinely arenot able toproduce sputum,bodyfluidsmaybe absent,maynothavemeningitis; sometimes, sputum•specimenmaybenegative,bodyfluids,tissuespecimensmaybedifficulttoprocure;stateof-the-artfacilitiesandexpertisemaynotbeavailableexceptintertiarycarecenters.Qualityassured,periodicallyaccreditedlaboratoryinfrastructuremaynotbeavailableforcarryingoutmycoabcterialcultureand•drug-susceptibilitytestingandmoleculardiagnosis.Evenwhenappropriatespecimensaresubmitted,especiallyinHIV-negativemiliaryTB,thesespecimensmayyieldgenuinely•negativeresultsbecauseEPTBisapaucibacillarydisease.Treatment:choosingtherightanti-tuberculosisdrugregimen,additionofsteroids,durationofanti-tuberculosistreatment,lackof•laboratorymonitoringfacilities,difficultiesinthemanagementofcomplications(especiallyinperipheralcentresduetolackofexpertise)arealltherapeuticchallenges.Notassessingtheextentoforgansysteminvolvementinitially(e.g.,TBmeningitis)mayresultinsub-optimaldurationoftherapy.WhiletreatingTB,drugsshouldbegenuinewithgoodbioavailabilitywhichmaynotbethecaseinresource-constrainednations•wherethediseaseismostprevalent.Insomesituations,especiallyinHIVco-infectedpatients,despiteregularanti-tuberculosisdrugintake,adequateplasmalevels•maynotbeachievedduetomalabsorptionproblems.ART andATT: several issues that are still not clear, like adequate staff training for recognition of adverse effects and close•monitoringofco-drugtoxicities,scarcityofqualityassuredlaboratoryfacilitieswherethediseaseiscommon,IRISdiagnosis(adequateeducationofthepatientsforrecognitionofdrugtoxicities,drugadherenceissues).
TB,tuberculosis;HIV,humanimmunodeficiencyvirus;EPTB,extra-pulmonarytuberculosis;ART,anti-retroviraltreatment;ATT,anti-tuberculosistreatment;IRIS,immunereconstitutioninflammatorysyndrome
SHARMAet al:DIAGNOSIS&TREATMENTOFMILIARYTB 705
Immunopathogenesis
The inadequacy of effector T-cell response incontainment of M. tuberculosis is thought to beresponsible for the development of miliary TB54-57.The abundance ofTh1 andTh2 polarized effectorT(Teff) cells in the peripheral blood and local diseasesite(s) among patients with miliary TB suggest thatmiliary TB probably represents the Th2 end of thespectrum56,57. Interleukin-4 (IL-4), with its ability todownregulateinduciblenitricoxidesynthase(iNOS),toll-likereceptor2(TLR2)andmacrophageactivation,mayplayanimportantroleintheeventsthatdeterminewhethertheinfectionbecomeslatentorprogressive4,54,55.M. tuberculosis caneitherfailtoevoketheprotectiveresponseorcandrive theprotectivemechanismsandthendeliberately‘sabotage’themleadingtoprogressivedisease55-57. InmiliaryTB, frequencyof regulatoryT(Treg) cells (CD4+CD25+FoxP3+) andhigher levelsofFoxP3mRNAweresignificantlyincreasedinlocaldisease site specimens57. Further, FoxP3+ Treg cellsobtained from the bronchoalveolar lavage (BAL)fluid of patients with miliary TB predominantlyproduced interleukin-10 (IL-10) and could suppressthe autologousT-cell proliferation in response toM. tuberculosisantigen56.InmiliaryTB,theattemptbythehosttoselectivelyrecruittheTeffcellsatthepathologicsite, however, fails to provide an adequate level ofeffector immunity at the disease site due to efficientandcomparablehomingofTregcells(FoxP3+),whichinhibitthefunctionoftheTeffcellsthathaveinfiltratedthedisease site. Ithasbeenpostulated thatwhen thebalanceofhomingofTregandTeffcellsshiftstowardtheformer,thereisastateoflocalimmunosuppressionleadingtodiseasedissemination4,56,57.
Observationsregardingthecellularcharacteristicsof BAL fluid in patients with miliary TB haveyielded conflicting results58-60.Though the diagnosticsignificance of thesefindings is not clear, thesemayfacilitate the understanding of the pathogenesis ofmiliary TB. The proportion and absolute numberof lymphocytes are substantially increased in BALfluid.A raised CD4+/CD8+ T-lymphocyte ratio andB-lymphocytesaswellasadecrease inCD4+/CD8+T-lymphocyteratiohaveearlierbeenreportedinBALfluid61,62. Polyclonal hypergammaglobulinaemia withincreaseinimmunoglobulin(Ig)G,IgA,andIgMwasobserved in peripheral blood andBALfluid61.Thesefindingsprobablyresultfromincreasedlocalsynthesisby activated B-lymphocytes. Increased BAL fluidfibronectinandserumC3levelsreflectanacutephaseresponse to ongoing inflammation61,62. Lymphocyticalveolitis and increased IgG and IgA levels havepersistedfollowingantituberculosistreatment61.
Molecular basis of dissemination
Several molecular mechanisms have beenimplicated in the development ofmiliaryTB.Theseincludeimpairedexpansionofγ/δT-cells63,failuretogenerateadequatecell-mediatedimmunity64,presenceof HLA-Bw1565, HLA-DRB1*15/16, DRB1*13, andDQB1*060266,absenceofHLA-Cw6,HLA-DRB1*10,andDQB1*050166, impairedMHCclass II restrictedtargetcelllysis,andover-exuberantlysisoftargetcellmacrophages67andLTA+368G/Apolymorphisms68.
Clinical manifestations
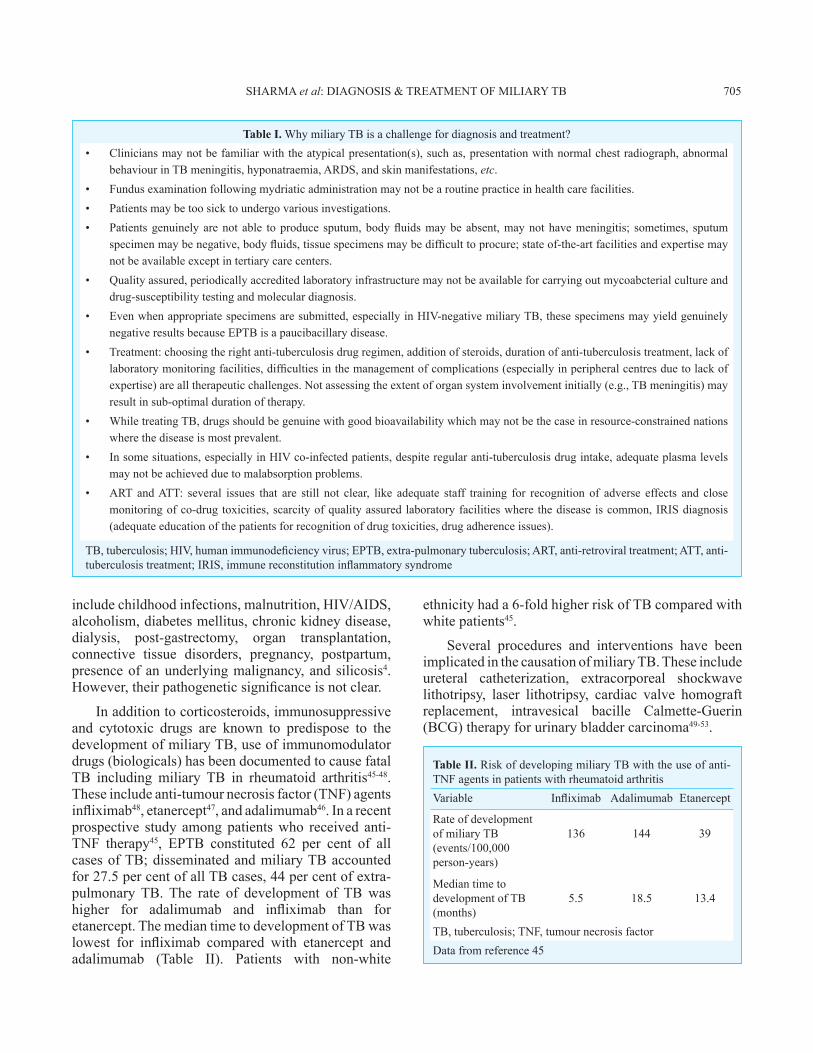
TheclinicalmanifestationsofmiliaryTBinadultsareprotean,non-specificandcanbeobscuretilllateinthedisease(Fig.2).
Fig. 2. Median prevalence of symptoms and signs at initial presentation in adult patients with miliary tuberculosis. Datafromreferences9,18,24-27,29,31-34,36,37,39-42,44.
706 INDIANJMEDRES,May 2012

Fig. 3. Clinicalphotographofachildshowingcutaneouslesionsofmiliarytuberculosis(Kind courtesy:DrM.Ramam,DepartmentofDermatology,AllIndiaInstituteofMedicalSciences,NewDelhi,India).
Constitutional symptoms: Patients with miliary TBclassically present with fever with evening rise oftemperature of several weeks duration, anorexia,weight loss, weakness and cough3,4. Occurrence ofdailymorning temperature spikes69 is reported to becharacteristic ofmiliaryTB.However, fevermaybeabsentand thepatientsmaypresentwithprogressivewasting strongly mimicking a metastatic carcinoma(cryptic miliary TB)70. Since its initial description,crypticmiliaryTBisincreasinglybeingreportedintheelderlypopulation20,21.
Chills and rigors, described in patients withmalaria, or, sepsis and bacteraemia, have often beendescribed in adult patients withmiliary TB3,4. Nightsweats are common.A “damp shadow” sign (wheresweat engraved the patient’s silhouette on the bed,closely resembling a body’s shadow) has also beendescribedinmiliaryTB71.
Systemic involvement: SincemiliaryTB can involvemanyorgans,patientspresentwithsymptomsandsignsreferredtovariousorgansystems(Fig.2).Drycoughanddyspnoeaareoftenpresent.Sputummaybescanty.Haemoptysiscanoccurrarely.Cutaneouslesionsmayoffer a valuable clue to the diagnosis ofmiliaryTB(Fig. 3). These include erythematous macules andpapules(tuberculosis miliaria cutis)4.
Choroidaltubercleswhenpresentinanappropriateclinicalsetting,provideavaluablecluetothediagnosisofmiliaryTB.Thepresenceofchoroidaltuberclesisconsidered to be pathognomonic of miliary TB3,4,39.Choroidal tubercles are bilateral, pale, gray-white or
yellowishlesionsusuallylessthanonequarterof thesizeoftheopticdiscandarelocatedwithin2cmoftheopticnerve.Thesearemorecommonlyseeninchildren.Therefore,asystematicophthalmoscopicexaminationisrecommendedaftermydriatricadministrationinallpatientswithsuspectedmiliaryTB(Fig.4).
TB meningitis (TBM) has been describedin 10 to 30 per cent adult patients with miliary TB9,18,22-27,29,30,32-39,41,42; conversely, about one-thirdof patients presenting with TB meningitis haveunderlying miliary TB72. In a recently publishedstudy73, the spectrumof neurological involvement inadultpatientswithmiliaryTBincludedTBmeningitiswithandwithouttuberculoma;andthoracictransversemyelopathy.
Beforetheadventofmodernimagingmodalities,such as CT, MRI and echocardiography, clinicallyevident cardiac or renal involvement was seldomdocumentedinpatientswithmiliaryTB.OvertadrenalinsufficiencymanifestingasAddison’sdiseaseatinitialpresentation,orduringanti-tuberculosistreatmenthasalsobeendescribedinmiliaryTB74,75.
Children
Thereareonlyafewpublishedseriesonchildhoodmiliary TB6-8,22-38. Miliary TB develops less often inchildren who have received the BCG vaccination4.Compared with adults, chills and night sweats,haemoptysis, productive cough are less common;peripherallymphadenopathyandhepatosplenomegalyaremorefrequentinchildrenwithmiliaryTB.Alargerproportion of children with miliary TB (20-40%) suffer from TBM6-8,22-38 compared to adults (15-30%)9,18,22-27,29,31-34,36-42,44.
Miliary tuberculosis in immunosuppressed individuals
The prevalence of miliary TB in persons withearly HIV infection (CD4+ cell counts >200 cells/mm3)issimilartothatobservedinimmunocompetentindividuals.Withprogressionof immunosuppression,in late, advanced stage ofHIV infection (CD4+ cellcounts <200 cells/mm3), miliary TB is seen moreoften4,58,76. Table III shows a comparison of variousaspectsofmiliaryTB in late advanced stageofHIVinfectionand in immunocompetent individuals, earlyHIVinfection4,41,58,76-82.Cutaneousinvolvement,arareclinicalmanifestationinHIV-seronegativepatientswithmiliaryTB,ismorecommonlyseeninlateHIVinfectionwith severe immunosuppression4,58,76-82. The skinmanifestationsincludetinypapulesorvesiculopapules,
SHARMAet al:DIAGNOSIS&TREATMENTOFMILIARYTB 707
(tuberculosis cutis miliaris disseminata, tuberculosis cutis acuta generalisita),anddisseminatedtuberculosisoftheskin(Fig.3).Sometimes,macular,pustular,orpurpuric lesions, indurated ulcerating plaques, andsubcutaneousabscesseshavebeenreported83.
In miliary TB patients co-infected with HIV,especiallyinthosewithprofoundimmunosuppression,intrathoracic lymphadenopathyand tuberculinanergyaremorecommon;sputumsmearsareseldompositive
and blood culture may grow M. tuberculosis4,58,76-82 (TableIII).Theseobservationsseemtobeapplicabletoothercausesofimmunosuppressionaswell84.
Uncommon clinical manifestations and complications Several uncommon clinical manifestations andcomplications have been observed in patients withmiliaryTB(TableIV).Insomepatients,complicationslikeARDS ormyocarditismay in fact be the initial
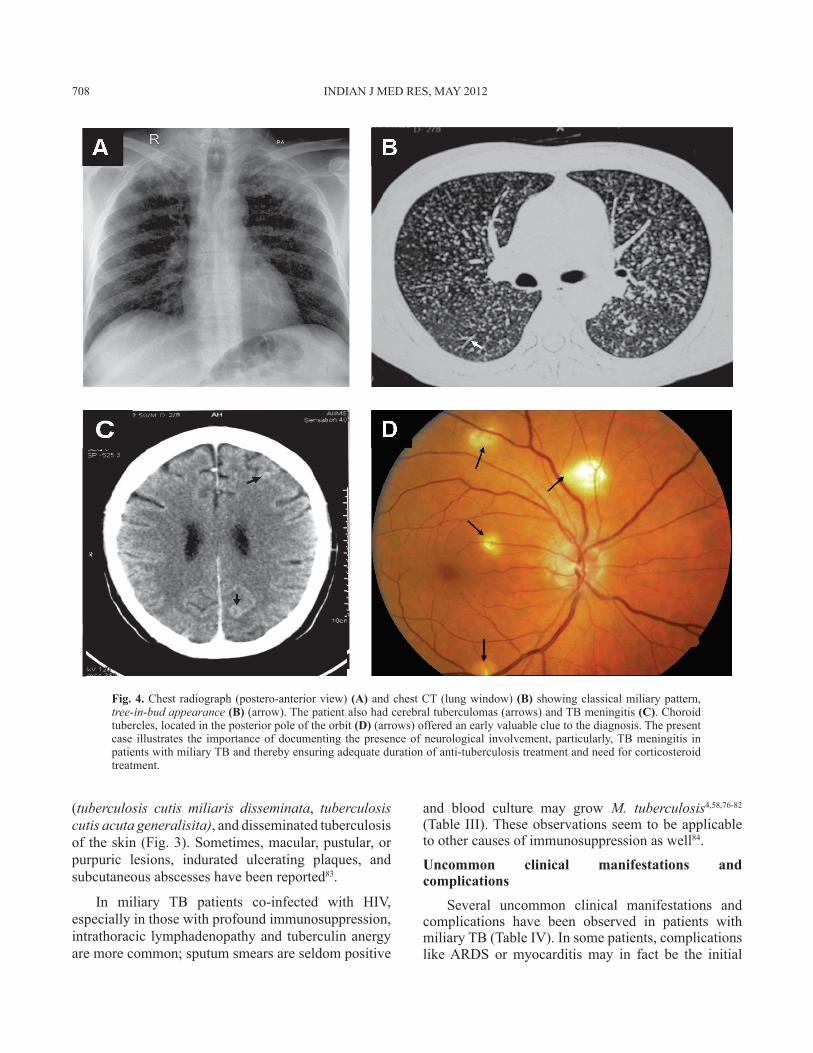
Fig. 4. Chestradiograph(postero-anteriorview)(A)andchestCT(lungwindow)(B)showingclassicalmiliarypattern,tree-in-bud appearance (B) (arrow).Thepatientalsohadcerebraltuberculomas(arrows)andTBmeningitis(C).Choroidtubercles,locatedintheposteriorpoleoftheorbit (D)(arrows)offeredanearlyvaluablecluetothediagnosis.Thepresentcase illustrates the importanceofdocumenting thepresenceofneurological involvement,particularly,TBmeningitis inpatientswithmiliaryTBandtherebyensuringadequatedurationofanti-tuberculosistreatmentandneedforcorticosteroidtreatment.
708 INDIANJMEDRES,May 2012
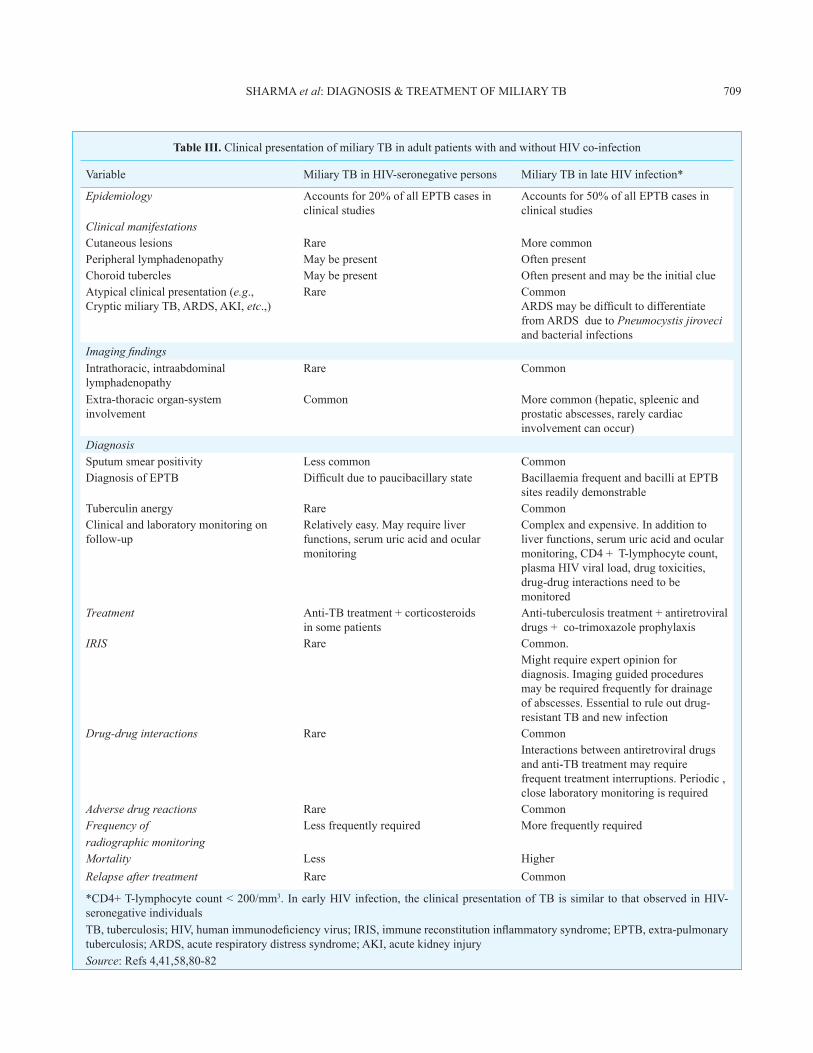
Table III. ClinicalpresentationofmiliaryTBinadultpatientswithandwithoutHIVco-infection
Variable MiliaryTBinHIV-seronegativepersons MiliaryTBinlateHIVinfection*
Epidemiology Accountsfor20%ofallEPTBcasesinclinicalstudies
Accountsfor50%ofallEPTBcasesinclinicalstudies
Clinical manifestationsCutaneouslesions Rare MorecommonPeripherallymphadenopathy Maybepresent OftenpresentChoroidtubercles Maybepresent OftenpresentandmaybetheinitialclueAtypicalclinicalpresentation(e.g., CrypticmiliaryTB,ARDS,AKI,etc.,)
Rare CommonARDSmaybedifficulttodifferentiatefromARDSduetoPneumocystis jiroveci andbacterialinfections
Imaging findingsIntrathoracic,intraabdominallymphadenopathy
Rare Common
Extra-thoracicorgan-system involvement
Common Morecommon(hepatic,spleenicandprostaticabscesses,rarelycardiacinvolvementcanoccur)
DiagnosisSputumsmearpositivity Lesscommon CommonDiagnosisofEPTB Difficultduetopaucibacillarystate BacillaemiafrequentandbacilliatEPTB
sitesreadilydemonstrableTuberculinanergy Rare CommonClinicalandlaboratorymonitoringonfollow-up
Relativelyeasy.Mayrequireliverfunctions,serumuricacidandocularmonitoring
Complexandexpensive.Inadditiontoliverfunctions,serumuricacidandocularmonitoring,CD4+T-lymphocytecount,plasmaHIVviralload,drugtoxicities,drug-druginteractionsneedtobemonitored
Treatment Anti-TBtreatment+corticosteroids insomepatients
Anti-tuberculosistreatment+antiretroviraldrugs+co-trimoxazoleprophylaxis
IRIS Rare Common.Mightrequireexpertopinionfordiagnosis.Imagingguidedproceduresmayberequiredfrequentlyfordrainageofabscesses.Essentialtoruleoutdrug-resistantTBandnewinfection
Drug-drug interactions Rare CommonInteractionsbetweenantiretroviraldrugsandanti-TBtreatmentmayrequirefrequenttreatmentinterruptions.Periodic,closelaboratorymonitoringisrequired
Adverse drug reactions Rare CommonFrequency of Lessfrequentlyrequired Morefrequentlyrequiredradiographic monitoring Mortality Less HigherRelapse after treatment Rare Common
*CD4+T-lymphocytecount<200/mm3.InearlyHIVinfection, theclinicalpresentationofTBissimilar to thatobservedinHIV-seronegativeindividualsTB,tuberculosis;HIV,humanimmunodeficiencyvirus;IRIS,immunereconstitutioninflammatorysyndrome;EPTB,extra-pulmonarytuberculosis;ARDS,acuterespiratorydistresssyndrome;AKI,acutekidneyinjurySource:Refs4,41,58,80-82
SHARMAet al:DIAGNOSIS&TREATMENTOFMILIARYTB 709
presentation.AtypicalclinicalpresentationoftendelaysthediagnosisandtreatmentandmiliaryTBisoftena“misseddiagnosis”.
Acute respiratory distress syndrome
AlthoughARDSmaydevelopanytimeduringthecourseofmiliaryTB,itisusuallyseenatthetimeofinitialpresentation(Fig.5);ARDSmaydevelopasacomponent of the multiorgan dysfunction syndrome(MODS)due toTBorasamanifestationof immunereconstitutioninflammatorysyndrome(IRIS)85-89.InastudyfromtwolargeteachinghospitalsatNewDelhiandTirupatiinIndia89,amongpatientswithTB,prolonged
illness, miliary TB, absolute lymphocytopaenia andelevated alanine aminotransferase (ALT)were foundtobe independentlyassociatedwith thedevelopmentof ARDS. In another study90 from Korea, higherC-reactiveproteinlevelsandanincreasingnutritionalrisk scorewere found to be independent risk factorsforthedevelopmentofARDSinpatientswithmiliaryTB.
Air-leak syndromes
Pneumothorax,whichmaysometimesbebilateral,may be the presenting feature or may sometimesdevelopwhilethepatientisreceivinganti-tuberculosistreatment3,4,91,92.Classicalmiliaryshadowsmaynotbediscernible initially and may become apparent oncelung expands. Intrapulmonary rupture of alveoli andconsequentair-leakthattraversesintothemediastinumafterspreadingalongthevascularsheathcanresultinpneumomediastinum with subcutaneous emphysemawhich may be fatal93. Rarely, pneumothorax maydevelop as a complication in TB-ARDS patientsreceivingmechanicalventilation(Fig.5E).
Acute kidney injury
InadditiontobeingapartofMODS,acutekidneyinjury(AKI)mayoccurduetodirectrenalparenchymalinvolvementinpatientswithmiliaryTB4,94.InHIVco-infectedpatientswithmiliaryTB,AKIcanalsodevelopasamanifestationofIRIS95.Uncommonly,renalfailurecandevelopasaconsequenceofobstructiveuropathycausedbythediseaseprocess58.
Hepatic and gastrointestinal manifestations
Fulminant hepatic failure may rarely be thepresenting manifestation in miliary TB. In some ofthesepatientsthecharacteristicpulmonarylesionsthatconstitute thehallmarkofmiliaryTBareabsent96,97.This could probably be the result of extrapulmonaryfocus discharging the tubercle bacilli into the portalcirculation,resultinginhepaticmiliaryTB.Peritonealinvolvementmaybeevidentbythepresenceofascites.Somepatientsmaymanifestdiarrhoeaoralteredbowelhabit suggestive of intestinal involvement. Smallintestinal perforations at the site of granulomatousinvolvement have been described in some patientswhileontreatment98.
Lesions located elsewhere in the body
Thoracic and abdominal lymphadenopathy:Patients with miliary TB, especially those co-infected with HIV manifest associated intrathoracic
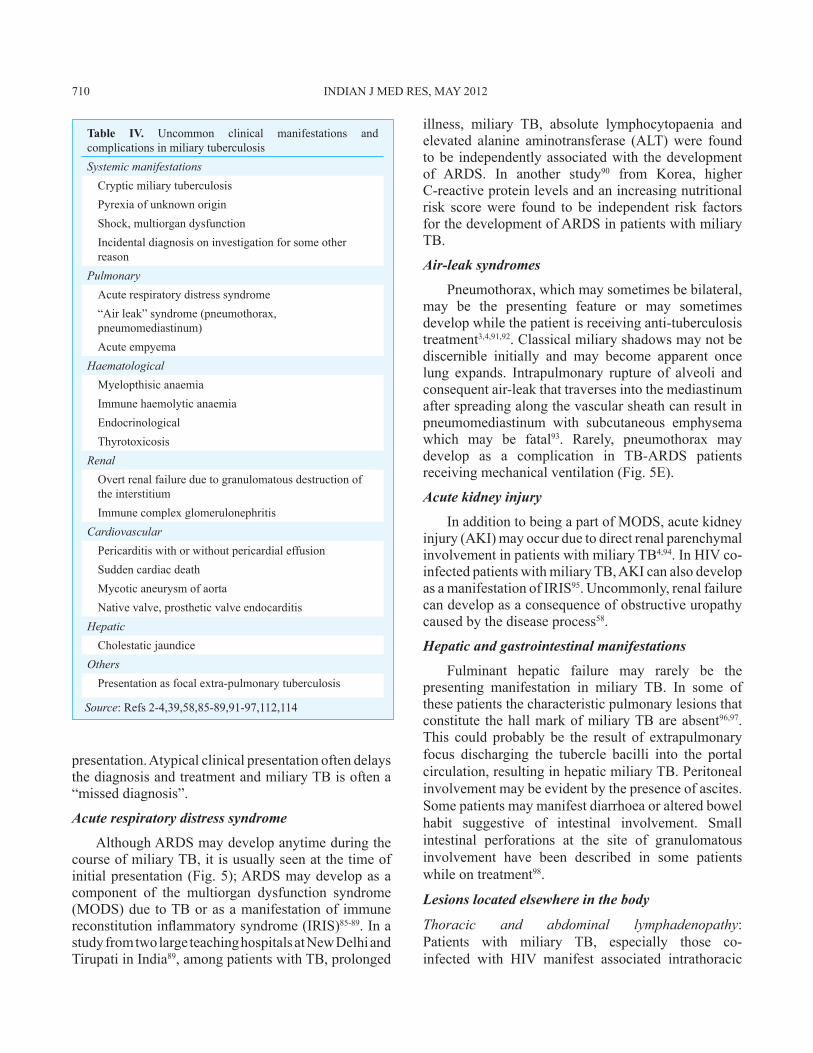
Table IV. Uncommon clinical manifestations andcomplicationsinmiliarytuberculosisSystemic manifestations CrypticmiliarytuberculosisPyrexiaofunknownoriginShock,multiorgandysfunctionIncidentaldiagnosisoninvestigationforsomeotherreason
Pulmonary Acuterespiratorydistresssyndrome“Airleak”syndrome(pneumothorax,pneumomediastinum)Acuteempyema
HaematologicalMyelopthisicanaemiaImmunehaemolyticanaemiaEndocrinologicalThyrotoxicosis
RenalOvertrenalfailureduetogranulomatousdestructionoftheinterstitiumImmunecomplexglomerulonephritis
Cardiovascular PericarditiswithorwithoutpericardialeffusionSuddencardiacdeathMycoticaneurysmofaortaNativevalve,prostheticvalveendocarditis
HepaticCholestaticjaundice
OthersPresentationasfocalextra-pulmonarytuberculosis
Source:Refs2-4,39,58,85-89,91-97,112,114
710 INDIANJMEDRES,May 2012

Fig. 5. Chestradiograph(postero-anteriorview)ofapregnantwomanwhopresentedwithprolongedpyrexiashowingaclassicalmiliarypattern(A).FundusexaminationfollowingmydriaticadministrationinboththeeyesrevealedchoroidtuberclesandhadraisedthesuspicionofmiliaryTB.ThepatientdevelopedARDSduring thecourseofher illness.Chest radiograph (antero-posteriorview),obtainedwithaportableX-raymachine,bed-sideshowingbilateralfrontalopacitiessuggestiveofARDS (B).CTchestobtainedatthesametimerevealsair-spaceconsolidation(C and D);air-bronchogram(arrow)(D).Whileassistedventilationwasbeingadministered,thepatientdevelopedpneumothorax(asterisk)ontherightside;collapsedlungborderisalsoevident(arrow)(E).Thepatientrequiredtubethoracostomyandunderwatersealdrainage.Eventuallythepatientwasweanedofftheventilatorandtheintercostaltubewasremovedfollowingresolutionofthepneumothorax.Thechestradiographobtainedthereaftershowssignificantimprovementinthelesions(F).Thepatientsurvivedtheturbulentin-hospitalcourse,wentontocompletefull-termofpregnancyandwassuccessfullydeliveredalivebaby.ARDS,acuterespiratorydistresssyndrome;CT,computedtomography;TB,tuberculosis.
SHARMAet al:DIAGNOSIS&TREATMENTOFMILIARYTB 711
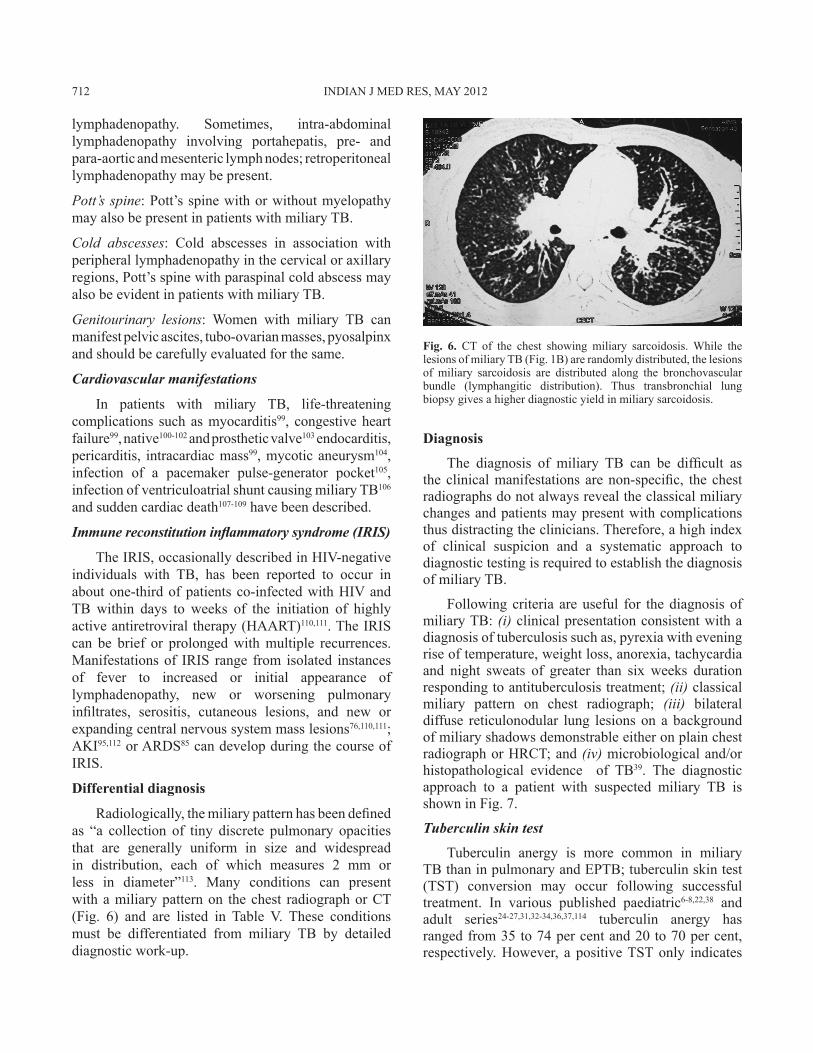
Fig. 6. CT of the chest showing miliary sarcoidosis.While thelesionsofmiliaryTB(Fig.1B)arerandomlydistributed,thelesionsof miliary sarcoidosis are distributed along the bronchovascularbundle (lymphangitic distribution). Thus transbronchial lungbiopsygivesahigherdiagnosticyieldinmiliarysarcoidosis.
lymphadenopathy. Sometimes, intra-abdominallymphadenopathy involving portahepatis, pre- andpara-aorticandmesentericlymphnodes;retroperitoneallymphadenopathymaybepresent.
Pott’s spine:Pott’sspinewithorwithoutmyelopathymayalsobepresentinpatientswithmiliaryTB.
Cold abscesses: Cold abscesses in association withperipherallymphadenopathyinthecervicaloraxillaryregions,Pott’sspinewithparaspinalcoldabscessmayalsobeevidentinpatientswithmiliaryTB.
Genitourinary lesions: Women with miliary TB canmanifestpelvicascites,tubo-ovarianmasses,pyosalpinxandshouldbecarefullyevaluatedforthesame.
Cardiovascular manifestations
In patients with miliary TB, life-threateningcomplications suchasmyocarditis99, congestiveheartfailure99,native100-102andprostheticvalve103endocarditis,pericarditis, intracardiacmass99,mycoticaneurysm104,infection of a pacemaker pulse-generator pocket105,infectionofventriculoatrialshuntcausingmiliaryTB106 andsuddencardiacdeath107-109havebeendescribed.
Immune reconstitution inflammatory syndrome (IRIS)
TheIRIS,occasionallydescribedinHIV-negativeindividuals with TB, has been reported to occur inaboutone-thirdofpatientsco-infectedwithHIVandTB within days to weeks of the initiation of highlyactiveantiretroviraltherapy(HAART)110,111.TheIRIScan be brief or prolongedwithmultiple recurrences.Manifestationsof IRIS range from isolated instancesof fever to increased or initial appearance oflymphadenopathy, new or worsening pulmonaryinfiltrates, serositis, cutaneous lesions, and new orexpandingcentralnervoussystemmasslesions76,110,111;AKI95,112orARDS85candevelopduringthecourseofIRIS.
Differential diagnosis
Radiologically,themiliarypatternhasbeendefinedas “a collection of tiny discrete pulmonary opacitiesthat are generally uniform in size and widespreadin distribution, each of which measures 2 mm orless in diameter”113. Many conditions can presentwithamiliarypatternon thechest radiographorCT (Fig. 6) and are listed in Table V. These conditionsmust be differentiated from miliary TB by detaileddiagnosticwork-up.
Diagnosis
The diagnosis of miliary TB can be difficult astheclinicalmanifestationsarenon-specific, thechestradiographsdonotalwaysrevealtheclassicalmiliarychangesandpatientsmaypresentwithcomplicationsthusdistractingtheclinicians.Therefore,ahighindexof clinical suspicion and a systematic approach todiagnostictestingisrequiredtoestablishthediagnosisofmiliaryTB.
Followingcriteria areuseful for thediagnosisofmiliaryTB:(i)clinicalpresentationconsistentwithadiagnosisoftuberculosissuchas,pyrexiawitheveningriseoftemperature,weightloss,anorexia,tachycardiaand night sweats of greater than six weeks durationrespondingtoantituberculosistreatment;(ii) classical miliary pattern on chest radiograph; (iii) bilateraldiffuse reticulonodular lung lesionson abackgroundofmiliaryshadowsdemonstrableeitheronplainchestradiographorHRCT;and(iv)microbiologicaland/orhistopathological evidence of TB39. The diagnosticapproach to a patient with suspected miliary TB isshowninFig.7.
Tuberculin skin test
Tuberculin anergy is more common in miliaryTBthaninpulmonaryandEPTB;tuberculinskintest (TST) conversion may occur following successfultreatment. In various published paediatric6-8,22,38 and adult series24-27,31,32-34,36,37,114 tuberculin anergy hasrangedfrom35to74percentand20to70percent, respectively.However, a positiveTSTonly indicates
712 INDIANJMEDRES,May 2012
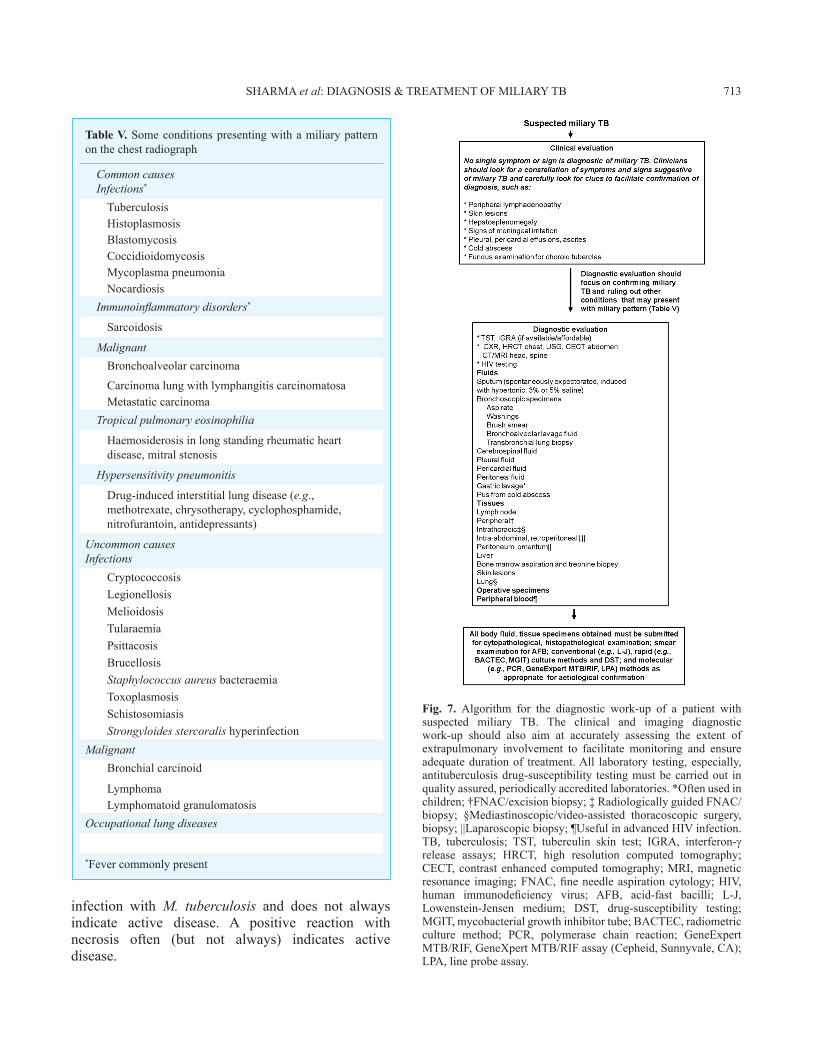
Fig. 7. Algorithm for the diagnostic work-up of a patient withsuspected miliary TB. The clinical and imaging diagnosticwork-up should also aim at accurately assessing the extent ofextrapulmonary involvement to facilitate monitoring and ensureadequatedurationof treatment.All laboratory testing,especially,antituberculosisdrug-susceptibility testingmustbecarriedout inqualityassured,periodicallyaccreditedlaboratories.*Oftenusedinchildren;†FNAC/excisionbiopsy;‡RadiologicallyguidedFNAC/biopsy; §Mediastinoscopic/video-assisted thoracoscopic surgery,biopsy;||Laparoscopicbiopsy;¶UsefulinadvancedHIVinfection.TB, tuberculosis; TST, tuberculin skin test; IGRA, interferon-γ release assays; HRCT, high resolution computed tomography;CECT,contrastenhancedcomputed tomography;MRI,magneticresonance imaging;FNAC,fineneedleaspirationcytology;HIV,human immunodeficiency virus; AFB, acid-fast bacilli; L-J,Lowenstein-Jensen medium; DST, drug-susceptibility testing;MGIT,mycobacterialgrowthinhibitortube;BACTEC,radiometricculture method; PCR, polymerase chain reaction; GeneExpertMTB/RIF,GeneXpertMTB/RIFassay(Cepheid,Sunnyvale,CA);LPA,lineprobeassay.
Table V. Someconditionspresentingwithamiliarypatternonthechestradiograph
Common causes Infections*
TuberculosisHistoplasmosisBlastomycosisCoccidioidomycosisMycoplasmapneumoniaNocardiosis
Immunoinflammatory disorders*
Sarcoidosis
MalignantBronchoalveolarcarcinoma
CarcinomalungwithlymphangitiscarcinomatosaMetastaticcarcinoma
Tropical pulmonary eosinophilia
Haemosiderosisinlongstandingrheumaticheartdisease,mitralstenosis
Hypersensitivity pneumonitis
Drug-inducedinterstitiallungdisease(e.g.,methotrexate,chrysotherapy,cyclophosphamide,nitrofurantoin,antidepressants)
Uncommon causesInfections
CryptococcosisLegionellosisMelioidosisTularaemiaPsittacosisBrucellosisStaphylococcus aureusbacteraemiaToxoplasmosisSchistosomiasisStrongyloides stercoralishyperinfection
MalignantBronchialcarcinoid
LymphomaLymphomatoidgranulomatosis
Occupational lung diseases
*Fevercommonlypresent
infection with M. tuberculosis and does not alwaysindicate active disease. A positive reaction with necrosis often (but not always) indicates activedisease.
SHARMAet al:DIAGNOSIS&TREATMENTOFMILIARYTB 713

Interferon-gamma release assays
Newer in vitro T-cell based interferon-gammarelease assays (IGRAs) available in the enzymelinked immunosorbent assay (ELISA) and enzymelinked immunospot (ELISPOT) formats appear to bepromisingindetectinglatentTBinfection(LTBI)andhaveseveraladvantagesovertheTST.Thesetestsmaybe particularly useful in children, BCG vaccinatedindividuals and in HIV infection andAIDS115,116.AswithTST, apositive IGRA test result, however,doesnot distinguishbetweenLTBI and activedisease, butanegativeIGRAresultmaybehelpfulinruling-outadiagnosisofTB116.Thesetestsarecostlyandonthebasisofavailableevidencetheirroutineuseisnotindicated.
Haematological and biochemical abnormalities
A number of haematological and biochemicalabnormalities are known to occur in miliary TB (Table VI)6-9,18,22,23,24-27,29,31,32-36,36-42,44 but theirsignificance is controversial. Disseminatedintravascularcoagulation(DIC)86,89hasbeendescribedin patients with miliary TB in the setting ofARDSandMODS and is associated with a high mortality.
Table VI. LaboratoryabnormalitiesinmiliaryTBHaematologicalAnaemiaLeucocytosisNeutrophiliaLymphocytosisMonocytosisThrombocytosisLeucopeniaLymphopeniaThrombocytopeniaLeukaemoidreactionHaemophagocytosisElevatedESR,CRPlevels
BiochemicalHyponatraemiaHypoalbuminaemiaHypercalcaemiaHypophosphatemiaHyperbilirubinaemiaElevatedserumtransaminasesElevatedserumalkalinephosphataseElevatedserumferritinlevels
ESR,erythrocytesedimentationrate;CRP,C-reactiveproteinSource:Refs2-4,39,114
Immune mechanisms have been implicated to causebonemarrowsuppressionandmiliaryTBhasalsobeenimplicated as a cause of pancytopenia, hypoplasticanaemia4,117.HypercalcaemiahasbeendocumentedinmiliaryTB,butisuncommon118.
HyponatraemiainmiliaryTBcanoccurduetoanacquired disturbance of neurohypophyseal functionresulting in unregulated antidiuretic hormone (ADH)release; an antidiuretic principle in the lung tissueaffectedbyTBthatmayeitherproduceADHorabsorbaninappropriatelyreleasedhormonefromtheposteriorpituitary119-121. Hyponatraemia may indicate thepresenceofTBmeningitis34andmayalsobeapredictorofmortality39inpatientswithmiliaryTB.Rifampicin-inducedadrenalcrisisinapatientwithmiliaryTBandAddison’sdiseasewhodevelopedgeneralizedmalaiseandhyponatraemiawhileinitiatedonantituberculosistreatmenthasalsobeendescribed75.
Imaging studies
Miliary pattern on the chest radiograph is oftenthefirstcluesuggestiveofmiliaryTB.Severalotherimaging modalities, such as, ultrasonography, CT,MRI, positron emission tomography (PET) helpto assess the extent of organ involvement and are alsouseful inevaluatingresponse to treatment (Figs.8and9).
Chest radiograph: The chest radiographic abnormalities in miliary TB are depicted in TableVII4,114.Miliarypatternonchestradiograph3,4,113 is thehallmarkofmiliaryTBand isevident inamajorityofpatients.Classically,subtlemiliarylesionsarebestdelineatedinslightlyunderpenetratedfilmsespeciallywhenthediamondshapedareasofthelunginbetweentheribsarecarefullyscrutinizedusingbrightlight122,123.However,in10percentofthecases,thenodulesmaybegreaterthan3mmindiameter124.Beforetheadventof CT, it was observed that classicalmiliary patternwouldnotbeevidentinthechestradiographinupto50percentofthepatientsandwouldbedetectedonlyatthetimeofautopsy14,17,18,24,34,124.
When caseous material, collagen or both arepresent inthetubercles, thesebecamevisibleonthechest radiograph122. Classicalmiliary pattern on thechestradiographrepresentssummationofdensitiesofthetuberclesthatareperfectlyalignedandimperfectlyaligned tubercles result in curvilinear densitiesand a reticulonodular pattern125. Rarely, lymphaticobstruction or infiltration can result in ground glass
714 INDIANJMEDRES,May 2012
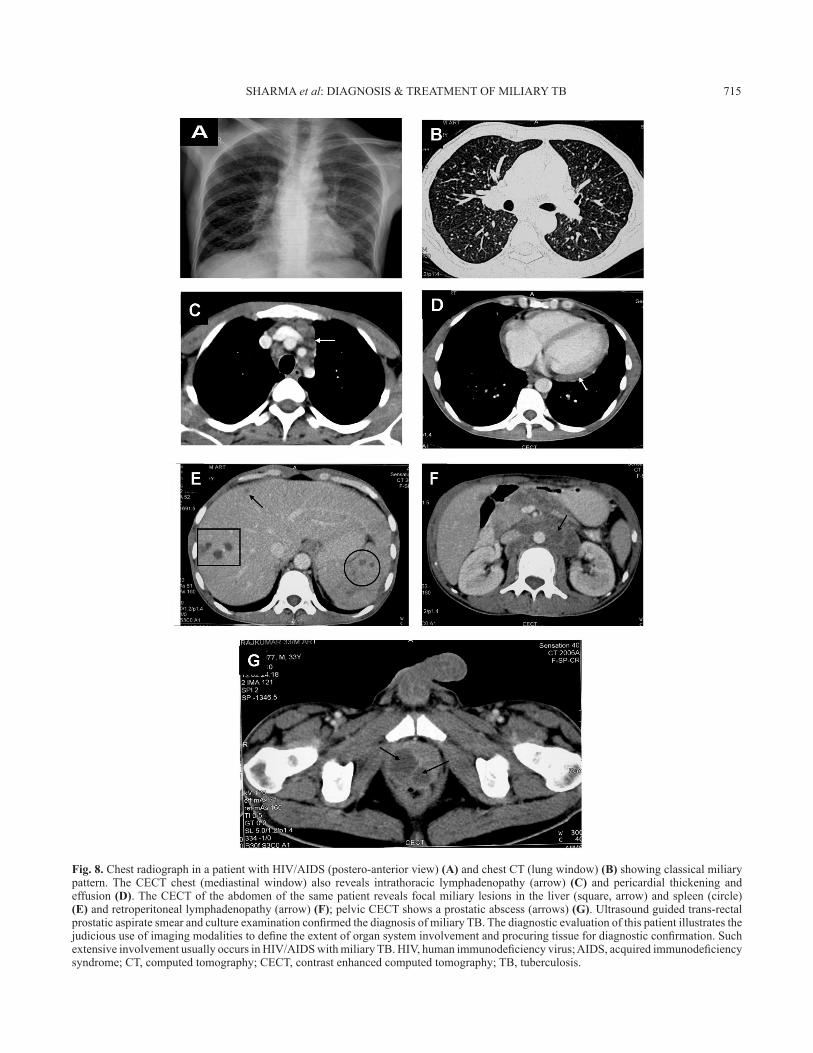
Fig. 8. ChestradiographinapatientwithHIV/AIDS(postero-anteriorview)(A)andchestCT(lungwindow)(B) showingclassicalmiliarypattern.TheCECT chest (mediastinalwindow) also reveals intrathoracic lymphadenopathy (arrow) (C) and pericardial thickening andeffusion(D).TheCECToftheabdomenofthesamepatientrevealsfocalmiliarylesionsintheliver(square,arrow)andspleen(circle)(E)andretroperitoneallymphadenopathy(arrow)(F);pelvicCECTshowsaprostaticabscess(arrows)(G).Ultrasoundguidedtrans-rectalprostaticaspiratesmearandcultureexaminationconfirmedthediagnosisofmiliaryTB.Thediagnosticevaluationofthispatientillustratesthejudicioususeofimagingmodalitiestodefinetheextentoforgansysteminvolvementandprocuringtissuefordiagnosticconfirmation.SuchextensiveinvolvementusuallyoccursinHIV/AIDSwithmiliaryTB.HIV,humanimmunodeficiencyvirus;AIDS,acquiredimmunodeficiencysyndrome;CT,computedtomography;CECT,contrastenhancedcomputedtomography;TB,tuberculosis.
SHARMAet al:DIAGNOSIS&TREATMENTOFMILIARYTB 715
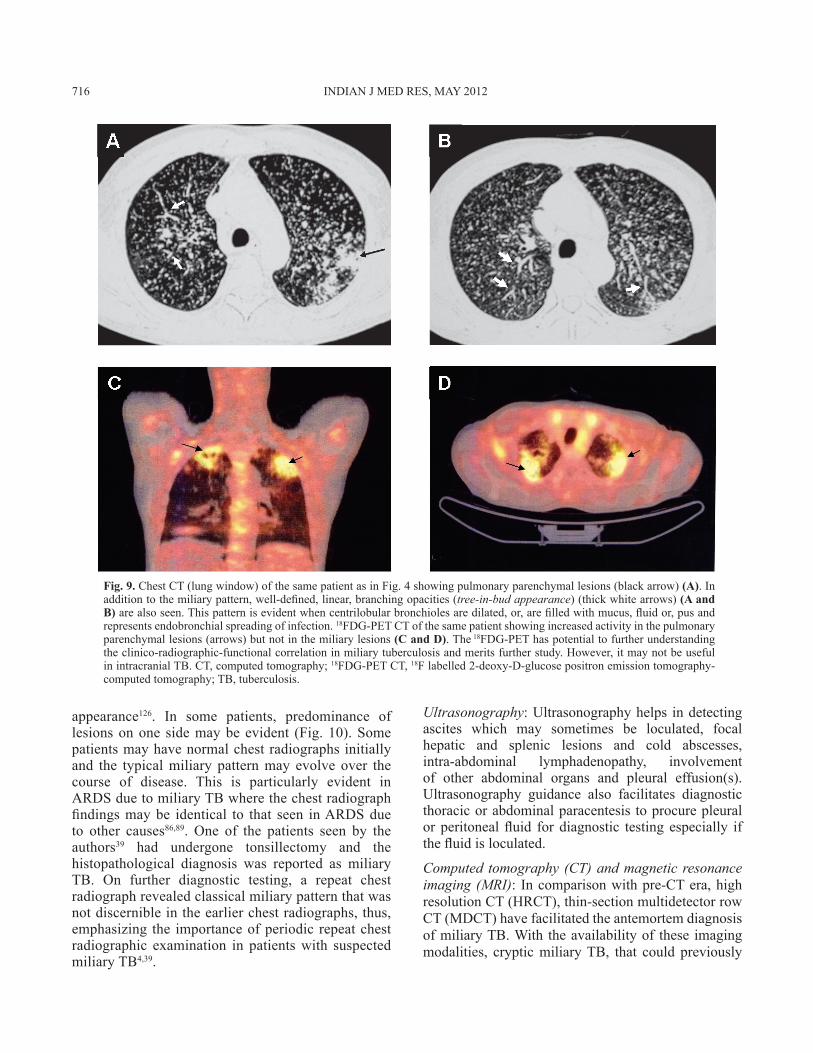
Fig. 9. ChestCT(lungwindow)ofthesamepatientasinFig.4showingpulmonaryparenchymallesions(blackarrow)(A).Inadditiontothemiliarypattern,well-defined,linear,branchingopacities(tree-in-bud appearance)(thickwhitearrows)(A and B)arealsoseen.Thispatternisevidentwhencentrilobularbronchiolesaredilated,or,arefilledwithmucus,fluidor,pusandrepresentsendobronchialspreadingofinfection.18FDG-PETCTofthesamepatientshowingincreasedactivityinthepulmonaryparenchymallesions(arrows)butnotinthemiliarylesions(C and D).The18FDG-PEThaspotentialtofurtherunderstandingtheclinico-radiographic-functionalcorrelationinmiliarytuberculosisandmeritsfurtherstudy.However,itmaynotbeusefulinintracranialTB.CT,computedtomography;18FDG-PETCT,18Flabelled2-deoxy-D-glucosepositronemissiontomography-computedtomography;TB,tuberculosis.
appearance126. In some patients, predominance oflesionsonone sidemaybeevident (Fig.10).Somepatientsmayhavenormalchestradiographsinitiallyand the typicalmiliary patternmay evolve over thecourse of disease. This is particularly evident inARDSduetomiliaryTBwherethechestradiographfindingsmaybe identical to that seen inARDSdueto other causes86,89. One of the patients seen by theauthors39 had undergone tonsillectomy and thehistopathological diagnosis was reported as miliaryTB. On further diagnostic testing, a repeat chestradiographrevealedclassicalmiliarypatternthatwasnotdiscernibleintheearlierchestradiographs,thus,emphasizing the importanceofperiodicrepeatchestradiographic examination in patientswith suspectedmiliaryTB4,39.
Ultrasonography:Ultrasonographyhelps indetectingascites which may sometimes be loculated, focalhepatic and splenic lesions and cold abscesses,intra-abdominal lymphadenopathy, involvementof other abdominal organs and pleural effusion(s).Ultrasonography guidance also facilitates diagnosticthoracicorabdominalparacentesis toprocurepleuralor peritonealfluid for diagnostic testing especially ifthefluidisloculated.
Computed tomography (CT) and magnetic resonance imaging (MRI): Incomparisonwithpre-CTera,highresolutionCT(HRCT),thin-sectionmultidetectorrowCT(MDCT)havefacilitatedtheantemortemdiagnosisofmiliaryTB.With theavailabilityof these imagingmodalities, crypticmiliaryTB, that could previously
716 INDIANJMEDRES,May 2012
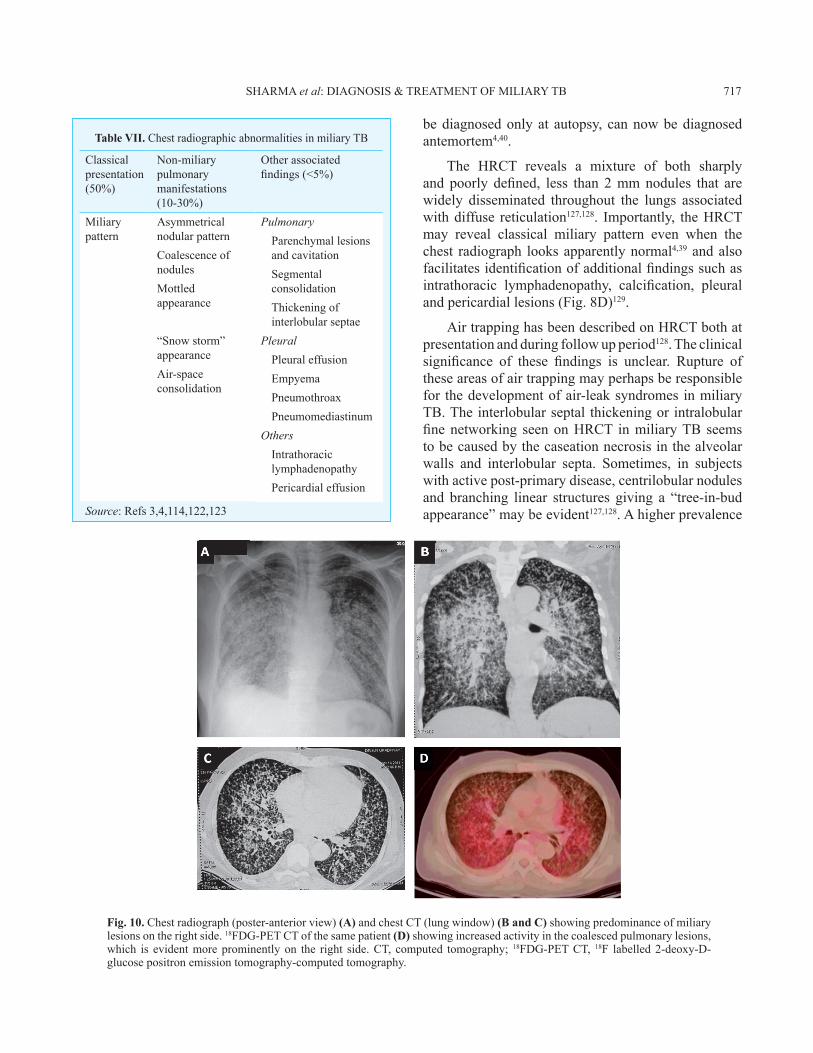
Fig. 10. Chestradiograph(poster-anteriorview)(A)andchestCT(lungwindow)(B and C)showingpredominanceofmiliarylesionsontherightside.18FDG-PETCTofthesamepatient(D)showingincreasedactivityinthecoalescedpulmonarylesions,which is evidentmoreprominentlyon the right side.CT, computed tomography; 18FDG-PETCT, 18F labelled2-deoxy-D-glucosepositronemissiontomography-computedtomography.
Table VII. ChestradiographicabnormalitiesinmiliaryTB
Classicalpresentation(50%)
Non-miliarypulmonarymanifestations (10-30%)
Otherassociatedfindings(<5%)
Miliarypattern
AsymmetricalnodularpatternCoalescenceofnodulesMottledappearance
“Snowstorm”appearanceAir-spaceconsolidation
Source:Refs3,4,114,122,123
PulmonaryParenchymallesionsandcavitationSegmentalconsolidationThickeningofinterlobularseptae
PleuralPleuraleffusionEmpyemaPneumothroaxPneumomediastinum
OthersIntrathoraciclymphadenopathyPericardialeffusion
bediagnosedonlyat autopsy, cannowbediagnosedantemortem4,40.
The HRCT reveals a mixture of both sharplyand poorly defined, less than 2mmnodules that arewidely disseminated throughout the lungs associatedwithdiffuse reticulation127,128. Importantly, theHRCTmay reveal classical miliary pattern even when thechest radiograph looksapparentlynormal4,39andalsofacilitatesidentificationofadditionalfindingssuchasintrathoracic lymphadenopathy, calcification, pleuralandpericardiallesions(Fig.8D)129.
AirtrappinghasbeendescribedonHRCTbothatpresentationandduringfollowupperiod128.Theclinicalsignificance of these findings is unclear. Rupture oftheseareasofairtrappingmayperhapsberesponsiblefor thedevelopmentofair-leaksyndromesinmiliaryTB.Theinterlobularseptal thickeningorintralobularfinenetworking seenonHRCT inmiliaryTB seemstobecausedbythecaseationnecrosisinthealveolarwalls and interlobular septa. Sometimes, in subjectswithactivepost-primarydisease,centrilobularnodulesand branching linear structures giving a “tree-in-budappearance”maybeevident127,128.Ahigherprevalence
SHARMAet al:DIAGNOSIS&TREATMENTOFMILIARYTB 717

per cent23,31,32,37,39,131. In patientswith dry coughBALfluidobtainedthroughfiberopticbronchoscopyshouldbe submitted for mycobacterial smear, culture andmolecularmethods(iffacilitiesexist).
Laparascopy
Laparascopyprovidesanopportunity tovisualisethe lesions, facilitates biopsy from the liver, spleen,peritoneum, omentum, mesenteric lymph nodes fordiagnosticconfirmation132.Whenassociatedabdominalinvolvement is present, laparascopy should beconsideredforprocuringtissuefordiagnostictesting.
Body fluids and tissue examination
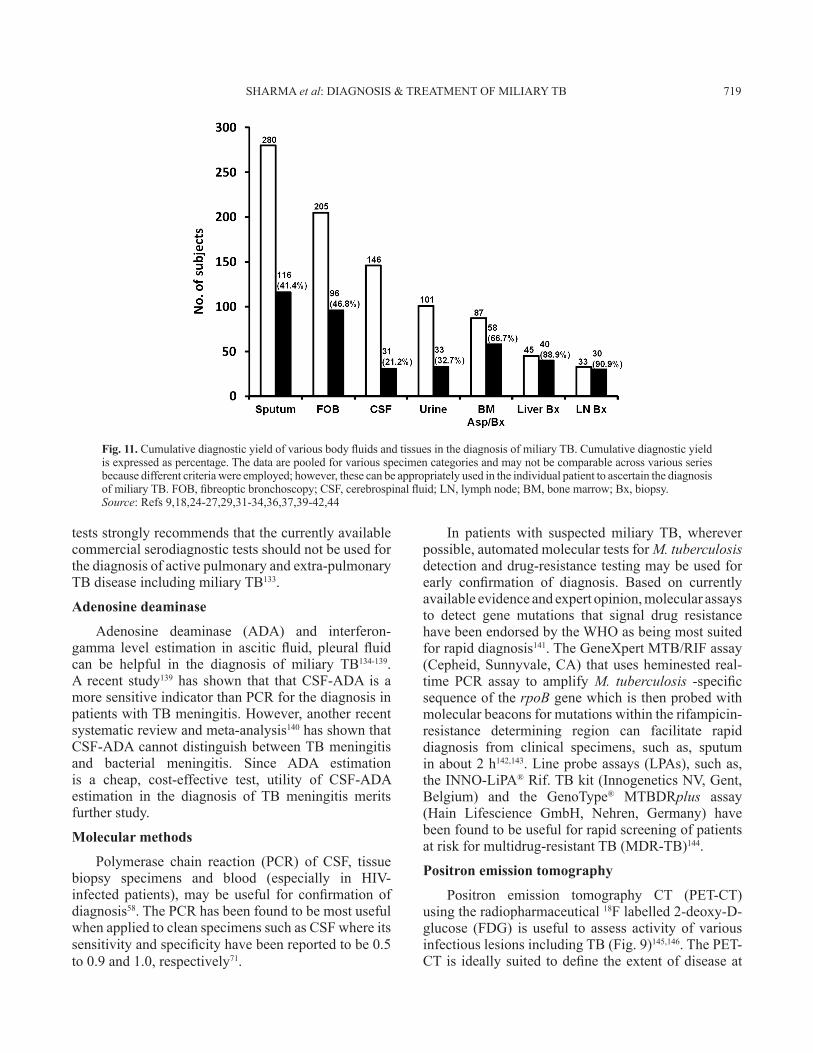
InpatientswithsuspectedmiliaryTB,dependingontheextentoforgansysteminvolvement,appropriatetissue and body fluid samples must be obtained toconfirm histopathological microbiological diagnosis.Elevated serum alkaline phosphatase levels indicatediffuse liver involvement; needle biopsy of the livercanbeusefulinconfirmingthediagnosis.BonemarrowaspirationandneedlebiopsyhavealsobeenfoundtobeusefulforthediagnosisofmiliaryTB.Pleuralfluid,pericardialfluid,asciticfluid,CSF,urine,bronchoscopicsecretions,bloodandtissuebiopsyspecimenshaveallbeenemployedtoconfirmthediagnosisofdisseminatedandmiliaryTB.Thediagnosticyieldofvarioustissueandbodyfluidspecimenshasbeenvariable6-9,18,22-27,29,31-34,36-41,42,44(Fig.11).
Whenimagingstudiesrevealfocallesionsinorgans(e.g., liver, spleen prostate), intrathoracic or intra-abdominal lymphadenopathyor cold abscess, image-guidedFNACortru-cutbiopsycanbecarriedoutandsubjected to histopathological and microbiologicalevaluationtoconfirmtheaetiologicaldiagnosis.
Mycobacterial culture and drug-susceptibility testing (DST)
Mycobacterial culture and drug susceptibilitytesting of sputum, body fluids and tissue specimenscarried out in an accredited laboratorywith externalquality assurance can facilitate identification andappropriatemanagement of drug-resistantTB.RapidculturemethodssuchastheBACTEC-460radiometricmethod,mycobacterialgrowthindicatortube(MGIT),andmolecularmethodsmaybeusefulforrapiddrug-susceptibilitytesting4.
Serodiagnostic methods
TherecentlypublishedWorldHealthOrganization(WHO)policystatementontheuseofserodiagnostic
ofinterlobularseptalthickening,necroticlymphnodesand extrathoracic involvement has been observed inHIV-seropositivepatientswithmiliaryTB80.
CT and MRI have been useful in identifyingmiliary lesions at extra-pulmonary sites. AbdominalCThasbeenusefulinidentifyinglesionsintheliver,spleen,intestine,mesentery,peritoneum,adrenalsandlymphnodes,andalsodetectscoldabscesses4.UnliketheCTofthechestwheretheclassicallessthan2mmnodularlesionsareevident,miliarylesionsintheliverandspleenmayappearasdiscretehypodense lesions(Fig.8E)afewofwhichmaybeconfluent,sometimeswithirregularperipheralrimenhancement130.
TheMRIofbrainandspineisveryuseful in theevaluation of patients with miliary TB and TBM,and spinal TB. The MRI is particularly helpful inidentificationanddelineatingtheextentoftuberculomasand cold abscesses and monitoring the response totreatment4.
Pelvic evaluation with all imaging modalitiesshould be routinely done in all female patients fordefining the extent of involvement. Tubo-ovarianmasses,hydro-andpyosalpinx,fluidcollectioninthepouchofDouglasmaybecomeobvious.Imageguidedradiologicalproceduressuchasfineneedleaspirationforcytologicalexamination(FNAC)andbiopsyunderCTorMRIguidanceareuseful forprocuring tissue/bodyfluidsfordiagnostictesting.
Sputum examination
ThoughnotallpatientswithmiliaryTBmanifestproductive cough, when available, sputum mustbe subjected to smear and mycobacterial cultureexamination.SputumsmearmicroscopyusingZiehl-Neelsen stain is useful in detecting acid-fast bacilli(AFB).Fluorescent stainingmayalso facilitate rapiddiagnosis. Sputum mycobacterial culture and drugsusceptibility testing carried out in an accreditedlaboratorywithexternalqualityassurancecanfacilitateidentification and appropriate management of drug-resistantTB.
Bronchoscopy
Fibreoptic bronchoscopy, BAL, bronchoscopicaspirate,brushings,washings,andtransbronchiallungbiopsy(TBLB)areusefulinconfirmingthediagnosisof miliary TB. The cumulative diagnostic yield forvariousbronchoscopicspecimensbysmearandculturemethodsinpublishedstudieshasbeenfoundtobe46.8
718 INDIANJMEDRES,May 2012
testsstronglyrecommendsthatthecurrentlyavailablecommercialserodiagnostictestsshouldnotbeused forthediagnosisofactivepulmonaryandextra-pulmonaryTBdiseaseincludingmiliaryTB133.
Adenosine deaminase
Adenosine deaminase (ADA) and interferon-gamma level estimation in ascitic fluid, pleural fluidcan be helpful in the diagnosis of miliary TB134-139.A recent study139 has shown that thatCSF-ADA is amoresensitiveindicatorthanPCRforthediagnosisinpatientswithTBmeningitis.However,anotherrecentsystematicreviewandmeta-analysis140hasshownthatCSF-ADAcannotdistinguishbetweenTBmeningitisand bacterial meningitis. Since ADA estimationis a cheap, cost-effective test, utility of CSF-ADAestimation in the diagnosis of TB meningitis meritsfurtherstudy.
Molecular methods
Polymerase chain reaction (PCR) of CSF, tissuebiopsy specimens and blood (especially in HIV-infected patients),may be useful for confirmation ofdiagnosis58.ThePCRhasbeenfoundtobemostusefulwhenappliedtocleanspecimenssuchasCSFwhereitssensitivityandspecificityhavebeenreportedtobe0.5to0.9and1.0,respectively71.
In patients with suspectedmiliaryTB, whereverpossible,automatedmoleculartestsforM. tuberculosis detectionanddrug-resistancetestingmaybeusedforearly confirmation of diagnosis. Based on currentlyavailableevidenceandexpertopinion,molecularassaysto detect gene mutations that signal drug resistancehavebeenendorsedbytheWHOasbeingmostsuitedforrapiddiagnosis141.TheGeneXpertMTB/RIFassay(Cepheid,Sunnyvale,CA) thatusesheminestedreal-time PCR assay to amplifyM. tuberculosis -specificsequenceoftherpoB genewhichisthenprobedwithmolecularbeaconsformutationswithintherifampicin-resistance determining region can facilitate rapiddiagnosis from clinical specimens, such as, sputuminabout2h142,143.Lineprobeassays(LPAs),suchas,theINNO-LiPA®Rif.TBkit(InnogeneticsNV,Gent,Belgium) and the GenoType® MTBDRplus assay(Hain Lifescience GmbH, Nehren, Germany) havebeenfoundtobeusefulforrapidscreeningofpatientsatriskformultidrug-resistantTB(MDR-TB)144.
Positron emission tomography
Positron emission tomography CT (PET-CT)usingtheradiopharmaceutical18Flabelled2-deoxy-D-glucose (FDG) is useful to assess activityof variousinfectiouslesionsincludingTB(Fig.9)145,146.ThePET-CTis ideallysuited todefinetheextentofdiseaseat
Fig. 11. CumulativediagnosticyieldofvariousbodyfluidsandtissuesinthediagnosisofmiliaryTB.Cumulativediagnosticyieldisexpressedaspercentage.Thedataarepooledforvariousspecimencategoriesandmaynotbecomparableacrossvariousseriesbecausedifferentcriteriawereemployed;however,thesecanbeappropriatelyusedintheindividualpatienttoascertainthediagnosisofmiliaryTB.FOB,fibreopticbronchoscopy;CSF,cerebrospinalfluid;LN,lymphnode;BM,bonemarrow;Bx,biopsy.Source:Refs9,18,24-27,29,31-34,36,37,39-42,44
SHARMAet al:DIAGNOSIS&TREATMENTOFMILIARYTB 719

thetimeofinitialpresentation.TheutilityofPET-CTin assessing the activity of lesions thatmight persistfollowingantituberculosistreatmentinmiliaryTBalsomeritsfurtherstudy.
Pulmonary function, gas exchange abnormalities and cardiopulmonary exercise testing
Miliary TB is associated with abnormalitiesof pulmonary function typical of interstitial lungdisease.Impairmentofdiffusionisthemostcommonabnormalityandmaysometimesbesevere59,147.Otherabnormalities include, amild reduction in flow ratessuggestiveofperipheralairwaysinvolvement59.Duringtheacutestage,arterialhypoxaemiaduetowideningofthe alveolar-arterial oxygen gradient and hypocapniadue to tachypnoea are also observed148. Often, thepulmonary function and gas exchange abnormalitiesmaybeofagreatermagnitudethanmightbeexpectedfromthechestradiograph61,148-150.
Abnormalcardiopulmonaryexerciseperformancehas been described in patientswithmiliaryTB.Thesalient abnormalities included lower maximumoxygen consumption, maximal work rate, anaerobicthreshold, peak minute ventilation, breathingreserve, and low maximal heart rate4,114,148,150. Otherabnormalities included higher respiratory frequency,peakminuteventilationatsubmaximalwork,andhighphysiologicaldeadspace/tidalvolume.Ademonstrablefallinoxygensaturation(to4%ormore)withexercisewas observed.Following successful anti-tuberculosistreatment,theseabnormalitiesreversedinamajorityofthepatients148,150.
Treatment
PatientswithmiliaryTBmustbepromptlytreatedwithstandardanti-tuberculosistreatmentasthediseaseisuniformlyfatalifnottreated3,4.However,thereisnoconsensusregardingtheoptimumdurationoftreatment.There are no published randomized controlled trialsassessingtheefficacyofthestandardWHOtreatmentregimens that have been widely used in nationaltuberculosiscontrolprogrammesworldwide151.
The American Thoracic Society (ATS), theCenters forDiseaseControl andPrevention (CDC),theInfectiousDiseaseSocietyofAmerica(IDSA)152 and National Institute for Health and ClinicalExcellence (NICE)153 guidelines fromUKstate thatsixmonthsoftreatment(2-monthintensivephasewithisoniazid,rifampicin,pyrazinamide,andethambutolorstreptomycin,followedbya4-monthcontinuation
phase with isoniazid and rifampicin) , whereas theAmericanAcademyofPediatrics(AAP)154advocatesninemonthsoftreatmentfornewlydiagnosedcasesofmiliaryTBwithoutmeningealinvolvement.WhenTB meningitis is present, it is suggested that thetreatmentbeextendedfor12months136-138.Inseveralparts of the world, patients with miliary TB gettreatedundernationalTBcontrolprogrammes,withDOTSusingshort-courseintermittent,thrice-weeklytreatment151.
IntheWHOguidelinesforthetreatmentofTB155,patientsarecategorizedas“newpatients”or“previouslytreated patients”. In these guidelines, miliary TB isclassifiedaspulmonaryTBbecause thereare lesionsin the lungs.NewpatientswithmiliaryTBreceive6monthsofdailyorintermittenttreatmentasdescribedabove. The guidelines mention that some expertsrecommend 9 to 12 months of treatment when TBmeningitisispresentgiventheseriousriskofdisabilityandmortality;and9monthsof treatmentwhenboneandjointTBisalsopresent.
For previously treated patients, the guidelinesadvocate that specimens for culture andDST shouldbe obtained at or before the start of treatment. TheDST should be performed for at least isoniazid andrifampicinandinsettingswhererapidmolecular-basedDSTresultsareavailable,theresultsshouldguidethechoiceofregimen.
These observations highlight the importanceof accurately assessing the extent of involvementclinically and radiologically. Thus, if underlyingTBmeningitis remains undiagnosed in a patient withmiliaryTB,suchapatienthasariskofreceivinganti-tuberculosistreatmentonlyfor6monthswhichmaybesub-optimal.Therefore,thoughthestandarddurationoftreatmentmaybesufficientformany,eachpatientneedsto be assessed individually, and wherever indicated,treatmentdurationmayhavetobeextended.
Other issues such as quality of anti-tuberculosisdrugs and their bio-availability are important inresource-poornations.EspeciallyinHIV-seropositivepatients,considerationmustalsobegiventoinadequateplasma levels of anti-tuberculosis drugs in spite ofregularintakeinadequatedosageduetomalabsorptionproblem.
Monitoring for adverse drug reactions
PatientswithmiliaryTBreceivinganti-tuberculosistreatment should be carefully monitored for adverse
720 INDIANJMEDRES,May 2012

drug reactions, especially, anti-tuberculosis drug-induced hepatotoxicity (DIH). Asymptomatic risein hepatic transaminases is common in patientswithmiliaryTB and unless definitive evidence ofDIH ispresent156-159,anti-tuberculosistreatmentshouldnotbewithheldonthisevidencealone.Inthisscenario,liverfunctionsshouldbeperiodicallymonitored.Intropicalcountries, acute viral hepatitis must be ruled out inpatientswhodevelopantituberculosisDIH160,161.
When patients with miliary TB develop anti-tuberculosis DIH, the potentially hepatotoxic drugs(rifampicin, isoniazid and pyrazinamide) should bestopped158. These patients should be treated withnon-hepatotoxic anti-tuberculosis drugs, such asethambutol, streptomycin and a fluoroquinolone, tillthe liver functions normalize. In patients who havedevelopedanti-tuberculosisDIH,itisusuallypossibleto reintroduce the same hepatotoxic drugs that havebeen implicated in the causation of DIH once theliverfunctionsnormalize.However,tillrecently,therehas been a lack of consensus regarding the optimalsequence and dosage schedule for reintroduction.Arecentlypublishedprospectiverandomizedcontrolledstudy162, provides useful data on this topic. In thisstudy from India, 175 patients with a diagnosis ofantituberculosis DIH were randomized to receiveone of three different pre-defined reintroductionregimensofanti-tuberculosisdrugsandwereevaluatedprospectively. The recurrence rate of DIH was notsignificantly different between the groups receivingisoniazid, rifampicin, andpyrazinamide administeredsimultaneously at full dosage from day 1; and thegroups receiving reintroduction regimens based ontheATS158andBritishThoracicSocietyguidelines163.Furtherstudiesarerequiredtoclarifytheissue.
Corticosteroids
Only limited published data are availablespecifically evaluating the role of adjunctcorticosteroid treatment in patients with miliaryTB and the results have been conflicting.While abeneficialresponsewasobservedinsomestudies164,such a benefit could not be observed in others165.Associated adrenal insufficiency is an absoluteindication for the administration of adjunctivecorticosteroid treatment. However, in patients withmiliary TB, adjunctive corticosteroid treatment isconsidered to be beneficial with TB meningitis,large pericardial effusion, IRIS, ARDS, immunecomplex nephritis, and histiocyticphagocytosissyndrome4,85,166.
Antiretroviral drugs
The efficacy of standard anti-tuberculosistreatmentregimensinthetreatmentofHIV,miliaryTBco-infectionhasnotbeenstudiedindetailinthefieldsetting under programme conditions. Treatment ofmiliaryTB inpatientsco-infectedwithHIVrequirescareful consideration of drug-drug interactionsbetweenanti-tuberculoisandanti-retroviraldrugs167,168.Co-administration of rifampicin, by inducing thehepatic cytochrome P450 pathway, may result indangerously low levels of anti-retroviral agents.Rifabutinispreferredoverrifampicinespeciallywhenproteaseinhibitorsareusedbutiscostly.Efavirenzispreferredovernevirapinebutshouldbeavoidedduringpregnancy. Pregnancy test needs to be done whilefemale patients are on efavirenz.A closemonitoringof laboratory parameters is required to detect drug-drug interaction when patients are receiving bothtreatments. Recently, there has been a change in theWHO revised recommendations167 based onGradingof Recommendations Assessment, Development andEvaluation(GRADE)system169 regardingthe timeofstartinganti-retroviraldrugs, thechoiceofdrugsandthetimeofinitiationinrelationtoinstitutionofanti-tuberculosis treatment. The algorithm for treatmentandmonitoringofpatientswithmiliaryTBisshowninFigs.12AandB.
In peripheral hospitals in endemic areas whereHIVandTBarecommon,qualityassured laboratoryfacilitiesforHIVELISA,CD4+T-lymphocytecountsand plasma HIV viral load estimation may not beavailable. Timing of initiation and antiretroviraltreatment (ART),choiceofARTandantituberculosistreatmentregimens,drug-druginteractions,allrequirecarefulconsideration.AhighdegreeofsuspicionandappropriatetrainingofthestaffisrequiredtoidentifyIRIS, recognize adverse drug reactions and drugtoxicities,drugadherenceissues.
Mechanical ventilation
Intensivecare,assistedmechanicalventilationandotherinterventionsmayberequiredforthemanagementof patients withmiliaryTB-ARDS86,89. Patients withmiliaryTB receiving assistedmechanical ventilationshouldbecarefullywatchedforcomplicationssuchaspneumothorax(Fig.5F).
Interventional radiology
Image-guidedpigtailcatheterdrainagefordrainingpsoasabscess,coilorgelfoamembolizationfortreating
SHARMAet al:DIAGNOSIS&TREATMENTOFMILIARYTB 721
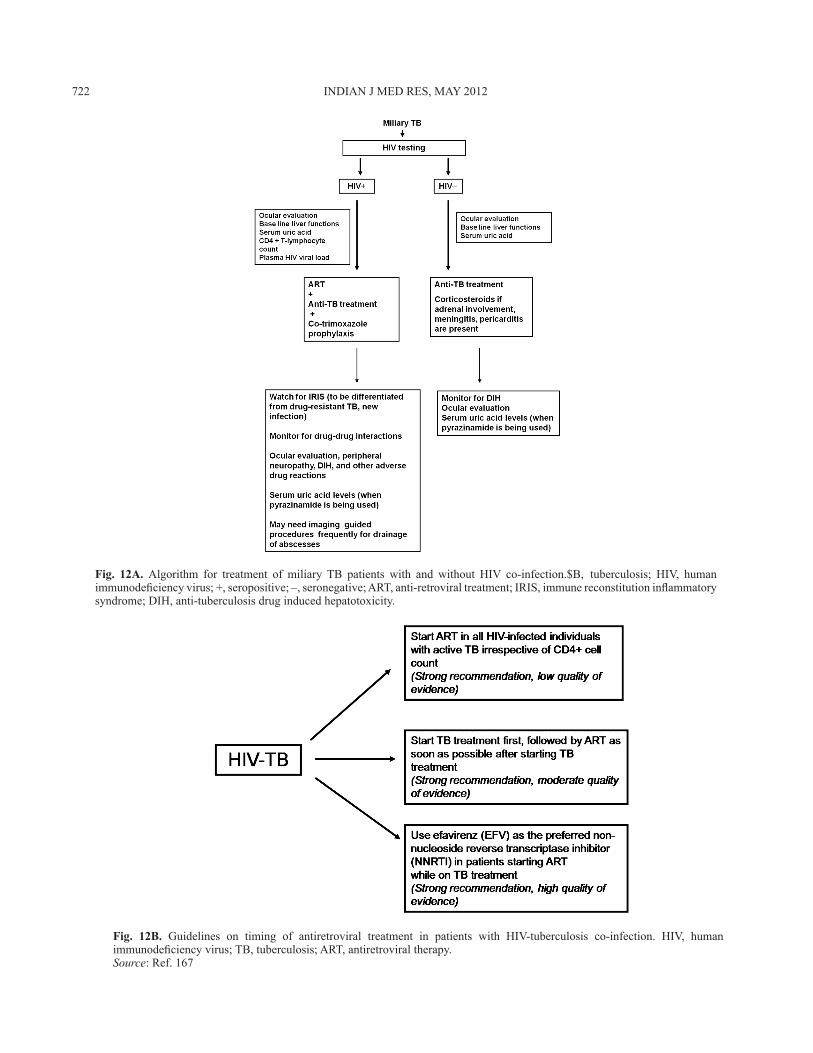
Fig. 12A. Algorithm for treatment of miliary TB patients with and without HIV co-infection.TB, tuberculosis; HIV, humanimmunodeficiencyvirus;+,seropositive;–,seronegative;ART,anti-retroviraltreatment;IRIS,immunereconstitutioninflammatorysyndrome;DIH,anti-tuberculosisdruginducedhepatotoxicity.
Fig. 12B. Guidelines on timing of antiretroviral treatment in patients with HIV-tuberculosis co-infection. HIV, humanimmunodeficiencyvirus;TB,tuberculosis;ART,antiretroviraltherapy.Source:Ref.167
722 INDIANJMEDRES,May 2012

issuesinthediagnosisandmanagementofmiliaryTBarelistedinTableIX.Astheclinicalsymptomatologyandphysical signsarenon-specific,cliniciansshouldhave a low threshold for suspecting miliary TB.Carefulphysicalexaminationfordiagnosticcluessuchasperipheral lymphadenopathy, coldabscess,pleuraleffusion,ascites,amongotherswillhelpinprocuringtissue and body fluids for confirming the diagnosis.Fundus examination for detecting choroid tuberclesmust be done in all patients with suspected miliaryTBastheirpresenceispathognomonicofmiliaryTB.SpecificeffortsshouldalsobedirectedatdocumentingthepresenceofTBmeningitisas thishas therapeuticsignificance.
Imaging modalities such as CT and MRI areuseful toestablish themiliarypattern.Inconjunction
Table VIII. Predictors of poor outcome in patients withmiliaryTBVariables PredictorsofpooroutcomeDemographicparameters Increasingage,femalegender,
malegenderCo-morbidconditions Presenceofanyunderlying
co-morbiddisease,cirrhosisofliver,Presenceofoneormorepredisposingconditions
Symptoms Historyofcough,nightsweats,dyspnoea,chills
Signs Alteredmentalstatus,meningismus,temperature>39.3°C,icterus,hepatomegaly
Laboratoryabnormalities Hyponatraemia,hypoalbuminaemiaelevatedtransaminaselevels,elevatedserumalkalinephosphataseLeucopenia,leucocytosis,Lymphopenia,Thrombocytopenia
Others Presenceofatypicalchestradiographicpatterns,treatmentdelay,highnutritionalriskscore*
*afour-pointnutritionalriskscorewasdefinedaccordingtothepresenceoffournutritionalfactors:lowbodymassindex(<18.5kg/m2),hypoalbuminaemia(serumalbumin<30g/l),hypocholesterolaemia(serumcholesterol<2.33mmol/l)andsevere lymphocytopenia (<7×105 cells/l).Each risk factorwasassignedavalueof1 ifpresentor0 ifabsent.Patientswith three or four points were classified as having a highnutritionalriskscore90TB,tuberculosisSource:Refs9,18,24-27,29,31-34,36-42,44,90
haemoptysis,amongothersareusefuladjunctsforthemanagementofcomplicationsinpatientswithmiliaryTB.
Surgery
Surgery is often required to procure specimensfordiagnostictestingandtoamelioratecomplications,such as small bowel perforation where it may belifesaving.Surgerymaybeindicatedwhenpatientsfailtorespondtochemotherapywithevidenceofongoinginfectionandforreliefofspinalcordcompressionwithpersistence or recurrence of neurological deficits, orinstabilityofthespine.
Mortality
The mortality related to miliary TB is about 15to 20 per cent in children and is slightly higher inadults (25 to 30%)24-27,31-34,36,37. Delay in diagnosisand consequently, delayed initiation of specific anti-tuberculosistreatmentappearstobethemostimportantfactorresponsibleformortalityinmiliaryTB.
Prognostic factors
Several factorshavebeen identifiedaspredictorsof poor outcome in patients with miliary TB (TableVIII). In patients with miliary TB-ARDS89, acutephysiologicalandchronichealthevaluation(APACHEII)score>18;APACHEIIscore≤18inthepresenceofhyponatraemiaandarterialoxygentensiontofractionofinspiredoxygen(PaO2/FIO2)ratio≤108.5havebeenidentified to be predictors of death. Identification ofthesefactorscanalertthecliniciansmanagingpatientswithmiliaryTB.
Prevention
TheBCGvaccinationiseffectiveinreducingtheincidence of miliary TB, especially in children170.However, it isnoteffective in individualswhohavelatent TB infection and should not be administeredto immunosuppressed hosts, such as, HIV infectedinfants. Targeted tuberculin testing is practised incountries with low prevalence of TB such as theUSA152,171, but anti-TB drug-induced hepatotoxicityis a potential risk with this intervention. Ongoingresearch172,173 is likely to provide a more effectivevaccinethanBCG.
Lessons learnt
MiliaryTB remainsanelusivediagnosiseven inareaswhereTBishighlyendemic.Thekeypractical
SHARMAet al:DIAGNOSIS&TREATMENTOFMILIARYTB 723
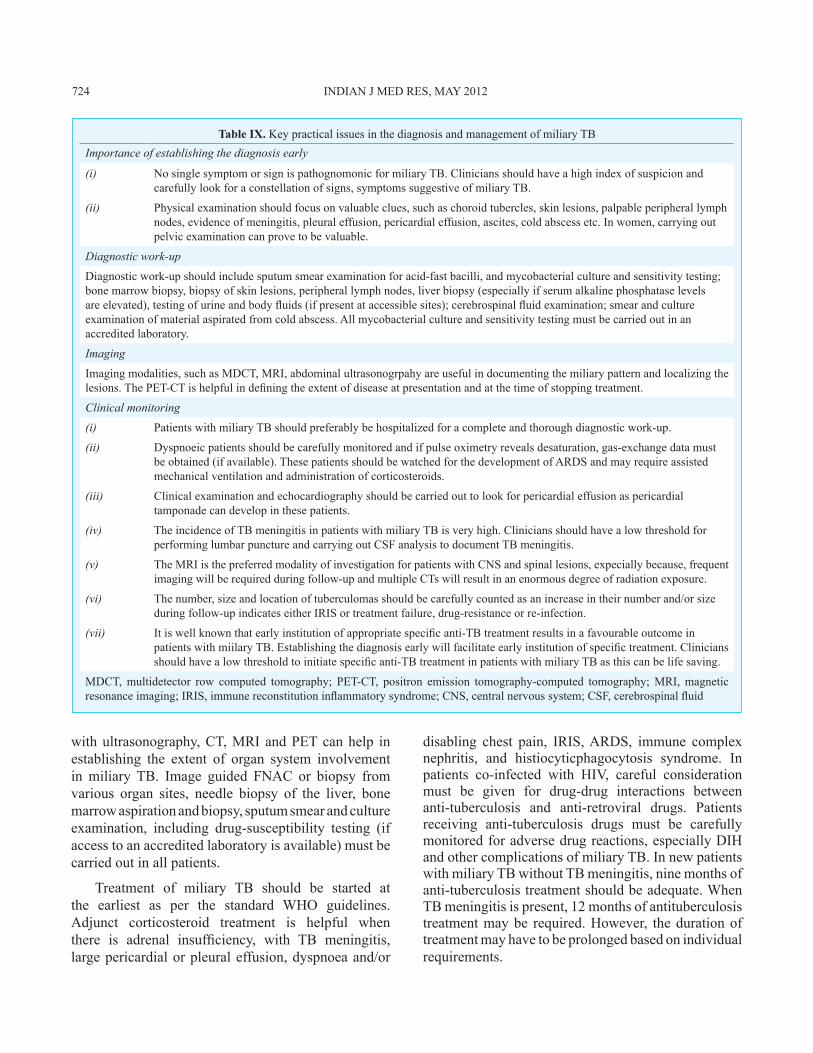
Table IX. KeypracticalissuesinthediagnosisandmanagementofmiliaryTBImportance of establishing the diagnosis early
(i) NosinglesymptomorsignispathognomonicformiliaryTB.Cliniciansshouldhaveahighindexofsuspicionandcarefullylookforaconstellationofsigns,symptomssuggestiveofmiliaryTB.
(ii) Physicalexaminationshouldfocusonvaluableclues,suchaschoroidtubercles,skinlesions,palpableperipherallymphnodes,evidenceofmeningitis,pleuraleffusion,pericardialeffusion,ascites,coldabscessetc.Inwomen,carryingoutpelvicexaminationcanprovetobevaluable.
Diagnostic work-up
Diagnosticwork-upshouldincludesputumsmearexaminationforacid-fastbacilli,andmycobacterialcultureandsensitivitytesting;bonemarrowbiopsy,biopsyofskinlesions,peripherallymphnodes,liverbiopsy(especiallyifserumalkalinephosphataselevelsareelevated),testingofurineandbodyfluids(ifpresentataccessiblesites);cerebrospinalfluidexamination;smearandcultureexaminationofmaterialaspiratedfromcoldabscess.Allmycobacterialcultureandsensitivitytestingmustbecarriedoutinanaccreditedlaboratory.
Imaging
Imagingmodalities,suchasMDCT,MRI,abdominalultrasonogrpahyareusefulindocumentingthemiliarypatternandlocalizingthelesions.ThePET-CTishelpfulindefiningtheextentofdiseaseatpresentationandatthetimeofstoppingtreatment.
Clinical monitoring
(i) PatientswithmiliaryTBshouldpreferablybehospitalizedforacompleteandthoroughdiagnosticwork-up.
(ii) Dyspnoeicpatientsshouldbecarefullymonitoredandifpulseoximetryrevealsdesaturation,gas-exchangedatamustbeobtained(ifavailable).ThesepatientsshouldbewatchedforthedevelopmentofARDSandmayrequireassistedmechanicalventilationandadministrationofcorticosteroids.
(iii) Clinicalexaminationandechocardiographyshouldbecarriedouttolookforpericardialeffusionaspericardialtamponadecandevelopinthesepatients.
(iv) TheincidenceofTBmeningitisinpatientswithmiliaryTBisveryhigh.CliniciansshouldhavealowthresholdforperforminglumbarpunctureandcarryingoutCSFanalysistodocumentTBmeningitis.
(v) TheMRIisthepreferredmodalityofinvestigationforpatientswithCNSandspinallesions,expeciallybecause,frequentimagingwillberequiredduringfollow-upandmultipleCTswillresultinanenormousdegreeofradiationexposure.
(vi) Thenumber,sizeandlocationoftuberculomasshouldbecarefullycountedasanincreaseintheirnumberand/orsizeduringfollow-upindicateseitherIRISortreatmentfailure,drug-resistanceorre-infection.
(vii) Itiswellknownthatearlyinstitutionofappropriatespecificanti-TBtreatmentresultsinafavourableoutcomeinpatientswithmiilaryTB.Establishingthediagnosisearlywillfacilitateearlyinstitutionofspecifictreatment.Cliniciansshouldhavealowthresholdtoinitiatespecificanti-TBtreatmentinpatientswithmiliaryTBasthiscanbelifesaving.
MDCT,multidetector row computed tomography; PET-CT, positron emission tomography-computed tomography;MRI,magneticresonanceimaging;IRIS,immunereconstitutioninflammatorysyndrome;CNS,centralnervoussystem;CSF,cerebrospinalfluid
withultrasonography,CT,MRIandPETcanhelp inestablishing the extent of organ system involvementinmiliary TB. Image guided FNAC or biopsy fromvarious organ sites, needle biopsy of the liver, bonemarrowaspirationandbiopsy,sputumsmearandcultureexamination, including drug-susceptibility testing (ifaccesstoanaccreditedlaboratoryisavailable)mustbecarriedoutinallpatients.
Treatment of miliary TB should be started atthe earliest as per the standard WHO guidelines.Adjunct corticosteroid treatment is helpful whenthere is adrenal insufficiency, with TB meningitis,largepericardialorpleuraleffusion,dyspnoeaand/or
disabling chest pain, IRIS,ARDS, immune complexnephritis, and histiocyticphagocytosis syndrome. Inpatients co-infected with HIV, careful considerationmust be given for drug-drug interactions betweenanti-tuberculosis and anti-retroviral drugs. Patientsreceiving anti-tuberculosis drugs must be carefullymonitoredforadversedrugreactions,especiallyDIHandothercomplicationsofmiliaryTB.InnewpatientswithmiliaryTBwithoutTBmeningitis,ninemonthsofanti-tuberculosistreatmentshouldbeadequate.WhenTBmeningitisispresent,12monthsofantituberculosistreatmentmaybe required.However, thedurationoftreatmentmayhavetobeprolongedbasedonindividualrequirements.
724 INDIANJMEDRES,May 2012
InlightofthecontinuingHIV/AIDSepidemicandincreasing use of immunosuppressive and cytotoxicdrugs, the burden of miliary TB will continue torise.TheutilityofnewerdiagnosticmethodssuchasIGRAsneedstobeclarified.Eventhoughclinical trials ofafewnewanti-tuberculosisdrugsareongoing,noothernewanti-tuberculosisdrugsappeartobeonthethresholdofbeingintroducedintopractice.Therefore,judicious use of available drugs to ensure regular,complete and adequate treatment is imperative. Therole of adjunctive corticosteroid therapy needs to beelucidated in future studies.The scope andutility ofPET-CTinassessingtheactivityoflesionsthatmightpersistfollowinganti-tuberculosistreatmentinmiliaryTBneedstobestudiedfurther.Thequestforabettervaccine than BCG is still on and more data on thecandidatevaccines thatarecurrentlybeingevaluatedislikelytoemerge.
References
1. Manget JJ. Sepulchretum sive anatomica practica. Vol. 1.ObservatioXLVII (3 vols). London:Cramer and Perachon;1700.
2. SahnSA,NeffTA.Miliarytuberculosis.Am J Med1974;56:494-505.
3. SharmaSK,MohanA.Miliarytuberculosis.In:SchlossbergD, editor. Tuberculosis and nontuberculous mycobacterial infections. 6th ed. Washington: American Society forMicrobiologyPress;2011.p.415-35.
4. Sharma SK, Mohan A, Sharma A, Mitra DK. Miliarytuberculosis:new insights intoanolddisease.Lancet Infect Dis2005;5:415-30.
5. Alvarez S, McCabe WR. Extrapulmonary tuberculosisrevisited: a review of experience at Boston City and otherhospitals.Medicine (Baltimore)1984;63:25-55.
6. Gurkan F, BosnakM,Dikici B, BosnakV,YaramisA,TasMA, et al.Miliarytuberculosisinchildren:aclinicalreview.Scand J Infect Dis1998;30:359-62.
7. Hussey G, Chisholm T, Kibel M. Miliary tuberculosis inchildren:areviewof94cases.Pediatr Infect Dis J1991;10:832-6.
8. Kim PK, Lee JS, Yun DJ. Clinical review of miliarytuberculosis inKoreanchildren.84casesand reviewof theliterature.Yonsei Med J1969;10:146-52.
9. LongR,O’Connor R, PalayewM,Hershfield E,ManfredaJ. Disseminated tuberculosis with and without a miliarypattern on chest radiograph: a clinical-pathologic-radiologiccorrelation.Int J Tuberc Lung Dis1997;1:52-8.
10. Alsoub H, Al Alousi FS. Miliary tuberculosis in Qatar: areviewof32adultcases.Ann Saudi Med2001;21:16-20.
11. Somu N, Vijayasekaran D, Ravikumar T, BalachandranA,SubramanyamL,ChandrabhushanamA.Tuberculousdiseasein a pediatric referral centre: 16 years experience. Indian Pediatr1994;31:1245-9.
12. UdaniPM,BhatUS,BhaveSK,EzuthachanSG,ShettyVV.Problem of tuberculosis in children in India: epidemiology,morbidity,mortalityandcontrolprogramme. Indian Pediatr 1976;13:881-90.
13. AnsariNA,KombeAH,KenyonTA,HoneNM,TapperoJW,NyirendaST, et al.Pathologyandcausesofdeathinagroupof 128 predominantly HIV-positive patients in Botswana,1997-1998.Int J Tuberc Lung Dis2002;6:55-63.
14. Chapman CB, Whorton CM. Acute generalised miliarytuberculosis in adults.A clinicopathological study based onsixty threecasesdiagnosedatautopsy.N Engl J Med1946;235:239-48.
15. Jacques J, Sloan TM. The changing pattern of miliarytuberculosis.Thorax1970;25:237-40.
16. JagirdarJ,ZagzagD.Pathologyandinsightsintopathogenesisof tuberculosis. In: Rom WN, Garay SM, editors. Tuberculosis. Philadelphia: LippincottWilliams &Wilkins;2004.p.323-44.
17. LewisonM,FrelichEB,RaginsOB.Correlationof clinicaldiagnosisandpathologicaldiagnosiswithspecialreferencetotuberculosis: analysis of autopsy findings in 893 cases.Am Rev Tuberc1931;24:152-71.
18. Slavin RE, Walsh TJ, Pollack AD. Late generalizedtuberculosis: a clinical pathologic analysis and comparisonof100casesinthepreantibioticandantibioticeras. Medicine (Baltimore)1980;59:352-66.
19. Vasankari T, Liippo K, Tala E. Overt and cryptic miliarytuberculosismisdiagnoseduntil autopsy.Scand J Infect Dis 2003;35:794-6.
20. Anonymous.Miliarytuberculosis:achangingpattern.Lancet 1970;1:985-6.
21. Braun MM, Cote TR, Rabkin CS. Trends in death withtuberculosisduringtheAIDSera.JAMA1993;269 :2865-8.
22. AdereleWI.Miliary tuberculosis inNigerianchildren.East Afr Med J1978;55:166-71.
23. Al-Jahdali H, Al-Zahrani K, Amene P, Memish Z, Al-ShimemeriA,MoamaryM, et al.ClinicalaspectsofmiliarytuberculosisinSaudiadults.Int J Tuberc Lung Dis2000;4:252-5.
24. Biehl JP.Miliary tuberculosis; a reviewof sixty-eight adultpatients admitted to a municipal general hospital. Am Rev Tuberc1958;77:605-22.
25. CampbellIG.MiliarytuberculosisinBritishColumbia.Can Med Assoc J 1973;108:1517-9.
26. Gelb AF, Leffler C, Brewin A, Mascatello V, Lyons HA.Miliary tuberculosis. Am Rev Respir Dis 1973; 108 : 1327-33.
27. GriecoMH,ChmelH.Acutedisseminated tuberculosisasadiagnostic problem.A clinical study based on twenty-eightcases.Am Rev Respir Dis1974;109:554-60.
28. JacobJT,MehtaAK,LeonardMK.Acuteformsoftuberculosisinadults.Am J Med2009;122:12-7.
29. Hussain SF, Irfan M, Abbasi M, Anwer SS, Davidson S,Haqqee R, et al. Clinical characteristics of 110 miliarytuberculosispatientsfromalowHIVprevalencecountry.Int J Tuberc Lung Dis 2004;8:493-9.
SHARMAet al:DIAGNOSIS&TREATMENTOFMILIARYTB 725
30. MonieRD,HunterAM,RocchiccioliKM,WhiteJP,CampbellIA,KilpatrickGS.RetrospectivesurveyofthemanagementofmiliarytuberculosisinSouthandWestWales,1976-8.Thorax 1983;38:369-72.
31. Kim JH, Langston AA, Gallis HA. Miliary tuberculosis:epidemiology,clinicalmanifestations,diagnosis,andoutcome.Rev Infect Dis1990;12:583-90.
32. MaartensG,WillcoxPA,Benatar SR.Miliary tuberculosis:rapid diagnosis, hematologic abnormalities, and outcome in109treatedadults.Am J Med1990;89:291-6.
33. MertA,BilirM,TabakF,OzarasR,OzturkR,SenturkH,et al.Miliarytuberculosis:clinicalmanifestations,diagnosisandoutcomein38adults.Respirology2001;6:217-24.
34. MuntPW.Miliarytuberculosisinthechemotherapyera:withaclinicalreviewin69Americanadults.Medicine (Baltimore) 1972;51:139-55.
35. Noertjojo K, Tam CM, Chan SL, Chan-Yeung MM.Extrapulmonaryandpulmonary tuberculosis inHongKong.Int J Tuberc Lung Dis2002;6:879-86.
36. OnadekoBO,DickinsonR,SofoworaEO.Miliarytuberculosisof the lung in Nigerian adults.East Afr Med J 1975; 52 :390-5.
37. ProutS,BenatarSR.Disseminatedtuberculosis.Astudyof62cases.S Afr Med J1980;58:835-42.
38. Rahajoe NN. Miliary tuberculosis in children. A clinicalreview.Paediatr Indones1990;30:233-40.
39. Sharma SK, MohanA, Pande JN, Prasad KL, Gupta AK,KhilnaniGC.Clinical profile, laboratory characteristics andoutcomeinmiliarytuberculosis.Q J Med 1995;88:29-37.
40. FedereleMP(Editor-in-Chief).Theyearbookofdiagnosticradiology,St.Louis:Mosby-YearBook,Inc;1997.p.91-3.
41. SwaminathanS,PadmapriyadarsiniC,PonnurajaC,SumathiCH,RajasekaranS,AmerandranVA, et al.Miliarytuberculosisin human immunodeficiency virus infected patients not onantiretroviral therapy: clinical profile and response to shortcoursechemotherapy.J Postgrad Med2007;53:228-31.
42. TekluB,ButlerJ,OstrowJH.Miliarytuberculosis.Areviewof 83 cases treated between 1950 and 1968.Ethiop Med J 1977;15:39-48.
43. UdaniPM,BhatUS,BhaveSK,EzuthachanSG,ShettyVV.Problem of tuberculosis in children in India: epidemiology,morbidity,mortalityandcontrolprogramme. Indian Pediatr 1976;13:881-90.
44. El Shamy AS, Al Saidi F, Baidas G, Al Bader M, SawyM, Hakkim R. Miliary tuberculosis in Kuwait: clinicalpresentation,diagnosisandtreatmentoutcome.Kuwait Med J 2008;40:288-92.
45. Dixon WG, Hyrich KL, Watson KD, Lunt M, GallowayJ, Ustianowski A; BSR BR Control Centre Consortium,SymmonsDP;B.S.R.BiologicsRegister.Drug-specific riskof tuberculosis in patients with rheumatoid arthritis treatedwith anti-TNF therapy: results from the British Society forRheumatologyBiologicsRegister(BSRBR).Ann Rheum Dis 2010;69:522-8.
46. Malipeddi AS, Rajendran R, Kallarackal G. Disseminatedtuberculosisafteranti-TNFalphatreatment.Lancet2007;369 :162.
47. ToussirotE,StreitG,WendlingD. Infectiouscomplicationswithanti-TNFalphatherapyinrheumaticdiseases:areview.Recent Pat Inflamm Allergy Drug Discov2007;1:39-47.
48. UthmanI,KanjN,El-SayadJ,BizriAR.MiliarytuberculosisafterinfliximabtherapyinLebanon.Clin Rheumatol2004;23 :279-80.
49. Anyanwu CH, Nassau E, Yacoub M. Miliary tuberculosisfollowing homograft valve replacement.Thorax 1976; 31 :101-6.
50. MoranoAmadoLE,AmadorBarcielaL,RodriguezFernandezA,Martinez-SapinaLlamasI,VazquezAlvarezO,FernandezMartinJ.Extracorporealshockwavelithotripsycomplicatedwithmiliarytuberculosis.J Urol1993;149:1532-4.
51. Rabe J,NeffKW,LehmannKJ,MechtersheimerU,GeorgiM. Miliary tuberculosis after intravesical bacille Calmette-Guerinimmunotherapyforcarcinomaofthebladder.AJR Am J Roentgenol1999;172:748-50.
52. Silverblatt A, DeSimone JA, Babinchak TJ. Acute miliarytuberculosisfollowinglaserlithotripsy.Infect Med2002;19 :80-2.
53. Yekanath H, Gross PA, Vitenson JH. Miliary tuberculosisfollowingureteralcatheterization.Urology1980;16:197-8.
54. CollinsHL,KaufmannSH.Themanyfacesofhostresponsestotuberculosis.Immunology2001;103:1-9.
55. Rook GA, Hernandez-Pando R, Dheda K, Teng Seah G.IL-4intuberculosis:implicationsforvaccinedesign.Trends Immunol2004;25:483-8.
56. SharmaPK,SahaPK,SinghA,SharmaSK,GhoshB,MitraDK. FoxP3+ regulatory T cells suppress effector T-cellfunctionatpathologicsiteinmiliarytuberculosis.Am J Respir Crit Care Med2009;179:1061-70.
57. SharmaSK,MitraDK,BalamuruganA,PandeyRM,MehraNK.Cytokinepolarizationinmiliaryandpleuraltuberculosis.J Clin Immunol 2002;22:345-52.
58. SharmaSK,MohanA.Extrapulmonarytuberculosis.Indian J Med Res2004;120 :316-53.
59. Ainslie GM, Solomon JA, Bateman ED. Lymphocyte andlymphocytesubsetnumbersinbloodandinbronchoalveolarlavage and pleural fluid in various forms of pulmonarytuberculosis at presentation and during recovery. Thorax 1992;47:513-8.
60. Sharma SK, Pande JN, Verma K. Bronchoalveolar lavage(BAL)inmiliarytuberculosis.Tubercle1988;69:175-8.
61. SharmaSK,PandeJN,SinghYN,VermaK,KathaitSS,KhareSD,et al.Pulmonaryfunctionandimmunologicabnormalitiesinmiliarytuberculosis.Am Rev Respir Dis1992;145:1167-71.
62. PrabhakaranD,SharmaSK,VermaK,PandeJN.Estimationof fibronectin in bronchoalveolar lavage fluid in variousdiffuseinterstitiallungdiseases.Am Rev Respir Dis1990;141 :A51.
63. BarnesPF,GrissoCL,AbramsJS,BandH,ReaTH,ModlinRL. Gamma delta T lymphocytes in human tuberculosis. J Infect Dis1992;165:506-12.
64. Ellner JJ. The immune response in human tuberculosis-implicationsfortuberculosiscontrol.J Infect Dis1997;176:1351-9.
726 INDIANJMEDRES,May 2012
65. Al-Arif LI, Goldstein RA,Affronti LF, Janicki BW. HLA-Bw15andtuberculosisinaNorthAmericanblackpopulation.Am Rev Respir Dis1979;120:1275-8.
66. BalamuruganA. HLA-DR restriction of Th1/Th2 cytokineprofile in tuberculosis: impact of genetic diversity. Ph.D.Thesis.NewDelhi:All India InstituteofMedicalSciences;2002.
67. KumararatneDS,PithieAS,DrysdaleP,GastonJS,KiesslingR, Iles PB, et al. Specific lysis of mycobacterial antigen-bearingmacrophagesbyclassIIMHC-restrictedpolyclonalTcelllinesinhealthydonorsorpatientswithtuberculosis.Clin Exp Immunol1990;80:314-23.
68. Taype CA, Shamsuzzaman S, Accinelli RA, Espinoza JR,ShawMA.Genetic susceptibility to different clinical formsoftuberculosisinthePeruvianpopulation.Infect Genet Evol 2010;10:495-504.
69. Cunha BA, Krakakis J,McDermott BP. Fever of unknownorigin (FUO) caused by miliary tuberculosis: diagnosticsignificanceofmorningtemperaturespikes.Heart Lung2009;38:77-82.
70. ProudfootAT,AkhtarAJ,DouglasAC,HorneNW.Miliarytuberculosisinadults. BMJ1969;2:273-6.
71. Flores-FrancoRA,Ríos-OrtizLA.The"dampshadow"sign:anotherclinicalindicatorofmiliarytuberculosis.Heart Lung 2010;39:87-8.
72. Thwaites GE, Nguyen DB, Nguyen HD, Hoang TQ, DoTT,NguyenTC, et al.Dexamethasone for the treatment oftuberculousmeningitis in adolescents and adults.N Engl J Med2004;351:1741-51.
73. Garg RK, Sharma R, KarAM,Kushwaha RA, SinghMK,Shukla R, et al. Neurological complications of miliarytuberculosis.Clin Neurol Neurosurg2010;112:188-92.
74. BraidyJ,PothelC,AmraS.Miliarytuberculosispresentingasadrenalfailure.J Can Med Assoc1981;82:254-6.
75. Yokoyama T, Toda R, Kimura Y, Mikagi M, Aizawa H.Addison's disease induced by miliary tuberculosis and theadministration of rifampicin. Intern Med 2009; 48 : 1297-300.
76. SharmaSK,MohanA,KadhiravanT.HIV-TBco-infection:epidemiology,diagnosisandmanagement.Indian J Med Res 2005;121:550-67.
77. Sharma SK, Mohan A. Co-infection of humanimmunodeficiency virus (HIV) and tuberculosis: Indianperspective.Indian J Tuberc2004;51:5-16.
78. SharmaSK,MohanA,GuptaR,KumarA,GuptaAK,SinghalVK, et al.ClinicalpresentationoftuberculosisinpatientswithAIDS: an Indian experience. Indian J Chest Dis Allied Sci 1997;39:213-20.
79. LadoLadoFL,BarrioGomezE,CarballoArceoE,CabarcosOrtizdeBarronA.Clinicalpresentationoftuberculosisandthedegreeof immunodeficiency inpatientswithHIV infection.Scand J Infect Dis1999;31:387-91.
80. Kim JY, JeongYJ,KimKI,Lee IS, ParkHK,KimYD,et al.Miliarytuberculosis:acomparisonofCTfindingsinHIV-seropositiveandHIV-seronegativepatients.Br J Radiol2010;83:206-11.
81. ZumlaA,MalonP,HendersonJ,GrangeJM.ImpactofHIVinfectionontuberculosis.Postgrad Med J2000;76:259-68.
82. HarriesA,MaherD,GrahamS. TB/HIV: a clinical manual.2nd ed. WHO/HTM/TB/2004. Geneva: World HealthOrganization;2004.p.329.
83. delGiudiceP,BernardE,PerrinC,BernardinG,FouchéR,BoissyC,et al.Unusualcutaneousmanifestationsofmiliarytuberculosis.Clin Infect Dis2000;30:201-4.
84. Shao C, Qu J, He L. A comparative study of clinicalmanifestationscausedbytuberculosisinimmunocompromisedand non-immunocompromised patients.Chin Med J (Engl) 2003;116 :1717-22.
85. GoldsackNR,AllenS,LipmanMC.Adultrespiratorydistresssyndromeasasevereimmunereconstitutiondiseasefollowingthecommencementofhighlyactiveantiretroviraltherapy.Sex Transm Infect2003;79:337-8.
86. MohanA,SharmaSK,PandeJN.Acute respiratorydistresssyndrome in miliary tuberculosis: a 12-year experience.Indian J Chest Dis Allied Sci 1996;38:147-52.
87. KimJY,ParkYB,KimYS,KangSB,ShinJW,ParkIW,et al.Miliarytuberculosisandacuterespiratorydistresssyndrome.Int J Tuberc Lung Dis2003;7:359-64.
88. Penner C, Roberts D, Kunimoto D, Manfreda J, Long R.Tuberculosisasaprimarycauseofrespiratoryfailurerequiringmechanicalventilation.Am J Respir Crit Care Med1995;151 :867-72.
89. SharmaSK,MohanA,BangaA,SahaPK,GuntupalliKK.Predictorsofdevelopmentandoutcomeinpatientswithacuterespiratorydistresssyndromeduetotuberculosis.Int J Tuberc Lung Dis2006;10:429-35.
90. KimDK,KimHJ,KwonSY,YoonHI,LeeCT,KimYW, et al.Nutritionaldeficitasanegativeprognosticfactorinpatientswithmiliarytuberculosis.Eur Respir J2008;32:1031-6.
91. Gupta PP, Mehta D, Agarwal D, Chand T. Recurrentpneumothoraxdevelopingduring chemotherapy in apatientwithmiliarytuberculosis.Ann Thorac Med2007;2:173-5.
92. Lakin BD, Riordan FA, John CM. Air leak in miliarytuberculosis.Am J Trop Med Hyg2009;80:325.
93. Krishnaswami KV. Mediastinal emphysema in miliarytuberculosis.JAMA1977;69:227-9.
94. MallinsonWJ, Fuller RW, Levison DA, Baker LR, CattellWR.Diffuseinterstitialrenaltuberculosis-anunusualcauseofrenalfailure.Q J Med1981;50:137-48.
95. SalliotC,GuichardI,DaugasE,LagrangeM,VerineJ,MolinaJM. Acute kidney disease due to immune reconstitutioninflammatory syndrome in an HIV-infected patient withtuberculosis. J Int Assoc Physicians AIDS Care (Chic Ill) 2008;7 :178-81.
96. AsadaY,HayashiT,SumiyoshiA,AburayaM,ShishimeE.Miliary tuberculosis presenting as fever and jaundice withhepaticfailure.Hum Pathol1991;22:92-4.
97. HussainW,MutimerD,HarrisonR,HubscherS,NeubergerJ.Fulminanthepaticfailurecausedbytuberculosis.Gut 1995;36:792-4.
98. SeabraJ,CoelhoH,.BarrosH,AlvesJO,GoncalvesV,Rocha-MarquesA.Acutetuberculousperforationofthesmallbowel
SHARMAet al:DIAGNOSIS&TREATMENTOFMILIARYTB 727
duringantituberculosistherapy.J Clin Gastroenterol1993;16 :320-2.
99. RoseAG.Cardiactuberculosis.Astudyof19patients.Arch Pathol Lab Med1987;111:422-6.
100.TheuerCP,HopewellPC,EliasD,SchecterGF,RutherfordGW,ChaissonRE.Humanimmunodeficiencyvirusinfectionintuberculosispatients.J Infect Dis1990;162:8-12.
101.Cope AP, Heber M, Wilkins EG. Valvular tuberculousendocarditis:acasereportandreviewoftheliterature.J Infect 1990;21:293-6.
102.WainwrightJ.Tuberculousendocarditis:areportof2cases.S Afr Med J1979;56:731-3.
103.YamaneH,FujiwaraT,DokoS,InadaH,NogamiA,MasakiH, et al.Twocasesofmiliarytuberculosisfollowingprostheticvalvereplacement.Kokyu To Junkan1989;37:803-5.
104.Felson B, Akers PV, Hall GS, Schreiber JT, Greene RE,Pedrosa CS.Mycotic tuberculous aneurysm of the thoracicaorta.JAMA1977;237:1104-8.
105.DohertyJG,RankinR,KerrF.Miliarytuberculosispresentingasinfectionofapacemakerpulse-generatorpocket. Scott Med J1996;41:20-1.
106.Shibolet S, Dan M, Jedwab M, Goldhammer Y, BaumGL. Recurrent miliary tuberculosis secondary to infectedventriculoatrialshunt.Chest1979;76:328-30.
107.Tseng HL, Roulet F. Cardiac involvement in miliarytuberculosis. Am Rev Tuberc1953;68:771-4.
108.BiedrzyckiOJ,BaithunSI.TB-relatedsuddendeath(TBRSD)duetomyocarditiscomplicatingmiliaryTB:acasereportandreviewoftheliterature.Am J Forensic Med Pathol2006;27:335-6.
109.Wallis PJ,BranfootAC,EmersonPA.Suddendeath due tomyocardialtuberculosis.Thorax1984;39:155-6.
110.Meintjes G, Lawn SD, Scano F, Maartens G, FrenchMA,Worodria W, et al; International Network for the Studyof HIV-associated IRIS. Tuberculosis-associated immunereconstitution inflammatory syndrome: case definitions foruse in resource-limited settings.Lancet Infect Dis2008;8 :516-3.
111.Sharma SK, Dhooria S, Barwad P, Kadhiravan T, RanjanS, Miglani S, et al. A study of TB-associated immunereconstitution inflammatory syndrome using the consensuscase-definition.Indian J Med Res2010;131:804-8.
112.JehleAW,KhannaN,SigleJP,Glatz-KriegerK,BattegayM,SteigerJ,et al.Acuterenalfailureonimmunereconstitutionin an HIV-positive patient with miliary tuberculosis. Clin Infect Dis2004;38:e32-5.
113.TuddenhamWJ. Glossary of terms for thoracic radiology:recommendations of the Nomenclature Committee of theFleischner Society.AJR Am J Roentgenol 1984;143 : 509-17.
114.SharmaSK,MohanA.Disseminatedandmiliarytuberculosis.In:SharmaSK,MohanA,editors.Tuberculosis.2nded.NewDelhi: Jaypee Brothers Medical Publishers; 2009. p. 493-518.
115.Mori T. Usefulness of interferon-gamma release assays fordiagnosingTB infection and problemswith these assays. J Infect Chemother2009;15:143-5.
116 Pai,M,JoshiR,KalantriSP.Diagnosisoflatenttuberculosisinfection: recentadvancesand futuredirections, In:SharmaSK,MohanA,editors.Tuberculosis.2nded.NewDelhi:JaypeeBrothersMedicalPublishers;2009.p.186-99.
117.SinghKJ,AhluwaliaG, SharmaSK, SaxenaR,ChaudharyVP,AnantM.Significanceofhaematologicalmanifestationsinpatientswithtuberculosis. J Assoc Physicians India2001;49:790-4.
118.Chan CH, ChanTY, ShekAC,MakTW, Lui SF, Lai KN.Severehypercalcaemiaassociatedwithmiliary tuberculosis.J Trop Med Hyg1994;97:180-2.
119.ShalhoubRJ,AntoniouLD.Themechanismofhyponatremiainpulmonary tuberculosis.Ann Intern Med1969;70 :943-62.
120.Vorherr H, Massry SG, Fallet R, Kaplan L, Kleeman CR.Antidiureticprinciple in tuberculous lung tissueofapatientwith pulmonary tuberculosis and hyponatremia.Ann Intern Med1970;72:383-7.
121.WinklerAW,CrankshawDF.ChloridedepletioninconditionsotherthanAddison’sdisease.J Clin Invest1938;17:1-6.
122.Steiner PE. The histopathological basis for the X-raydiagnosability of pulmonary miliary tuberculosis. Am Rev Tuberc1937;36:692-705.
123.KwongJS,CarignanS,KangEY,MullerNL,FitzgeraldJM.Miliarytuberculosis.Diagnosticaccuracyofchestradiography.Chest1996; 110:339-42.
124.LeeKS,KimTS,HanJ,HwangJH,YoonJH,KimY,et al.Diffuse micronodular lung disease: HRCT and pathologicfindings.J Comput Assist Tomogr1999;23:99-106.
125. JamiesonDH,CreminBJ.High resolutionCTof the lungsinacutedisseminated tuberculosisandapediatric radiologyperspectiveoftheterm“miliary”.Pediatr Radiol1993;23 :380-3.
126.PriceM.Lymphangitisreticularistuberculosa.Tubercle1968;49:377-84.
127.McGuinnessG,NaidichDP,JagirdarJ,LeitmanB,McCauleyDI. High resolution CT findings in miliary lung disease. J Comput Assist Tomogr1992;16:384-90.
128.SharmaSK,MukhopadhyayS,AroraR,VermaK,PandeJN,KhilnaniGC.Computedtomographyinmiliarytuberculosis:comparison with plain films, bronchoalveolar lavage,pulmonaryfunctionsandgasexchange.Australasian Radiol 1996;40:113-8.
129.PipavathSN,SharmaSK,SinhaS,MukhopadhyayS,Gulati.MS. High resolution CT (HRCT) in miliary tuberculosis(MTB)ofthelung:correlationwithpulmonaryfunctiontests&gasexchangeparametersinnorthIndianpatients.Indian J Med Res2007;126:193-8.
130.Yu RS, Zhang SZ,Wu JJ, Li RF. Imaging diagnosis of 12patients with hepatic tuberculosis. World J Gastroenterol 2004;10:1639-42.
131 WillcoxPA,PotgieterPD,BatemanED,BenatarSR.Rapiddiagnosis of sputumnegativemiliary tuberculosis using theflexiblefibreopticbronchoscope.Thorax1986;41:681-4.
132.IbrarullahM,MohanA, SarkariA, SrinivasM,MishraA,SundarTS.Abdominaltuberculosis:diagnosisbylaparoscopyandcolonoscopy.Trop Gastroenterol2002;23:150-3.
728 INDIANJMEDRES,May 2012
133.WorldHealthOrganization.Commercialserodiagnostictestsfordiagnosisof tuberculosis:policystatement.WHO/HTM/TB/2011.5.Geneva:WorldHealthOrganization;2011.
134.RiquelmeA, CalvoM, Salech F,Valderrama S, PattilloA,ArellanoM,et al.Valueof adenosinedeaminase (ADA) inascetic fluid for the diagnosis of tuberculous peritonitis: ameta-analysis.J Clin Gastroenterol2006;40:705-10.
135.SharmaSK,SureshV,MohanA,KaurP,SahaP,KumarA,et al.Aprospectivestudyofsensitivityandspecificityofadenosinedeaminaseestimationinthediagnosisoftuberculosispleuraleffusion.Indian J Chest Dis Allied Sci2001;43:149-55.
136.SharmaSK,BangaA.DiagnosticutilityofpleuralfluidIFNgammaintuberculosispleuraleffusion.J Interferon Cytokine Res2004;24:213-7.
137.Sharma SK, Banga A. Pleural fluid interferon-gamma andadenosinedeaminaselevelsintuberculosispleuraleffusion:acost-effectivenessanalysis.J Clin Lab Anal2005;19:40-6.
138.SharmaSK,TahirM,MohanA,Smith-RohrbergD,MishraHK, PandeyRM.Diagnostic accuracy of ascitic fluid IFN-gamma and adenosine deaminase assays in the diagnosisof tuberculousascites.J Interferon Cytokine Res2006;26 :484-8.
139.RanaSV,ChackoF,LalV,AroraSK,ParbhakarS,SharmaSK,et al.TocompareCSFadenosinedeaminase levelsandCSF-PCRfortuberculousmeningitis.Clin Neurol Neurosurg 2010;112:424-30.
140.TuonFF,HigashinoHR,LopesMI,LitvocMN,AtomiyaAN,AntonangeloL,et al.Adenosinedeaminaseandtuberculousmeningitis-a systematic reviewwithmeta-analysis.Scand J Infect Dis2010;42:198-207.
141.World Health Organization. Policy statement. Molecularline probe assays for rapid screening of patients at risk ofmultidrug-resistant tuberculosis (MDR-TB). June 27, 2008.Available from: http://www.who.int/tb/features_archive/policy.pdf,accessedonApril19,2012.
142.Boehme CC, Nabeta P, HillemannD, NicolMP, Shenai S,KrappF,et al.Rapidmoleculardetectionoftuberculosisandrifampinresistance. N Engl J Med2010;363:1005-15.
143.World Health Organization. Rapid implementation of theXpert MTB/RIF diagnostic test: technical and operational‘How-to’; practical considerations. WHO/HTM/TB/2011.2.Geneva:WorldHealthOrganization;2011.
144.Ling DI, Zwerling AA, Pai M. Rapid diagnosis of drug-resistantTBusinglineprobeassays:fromevidencetopolicy.Expert Rev Respir Med2008;2:583-8.
145.Goo JM, Im JG, Do KH,Yeo JS, Seo JB, KimHY, et al.Pulmonary tuberculoma evaluated by means of FDG PET:findingsin10cases.Radiology2000;216:117-21.
146.Ichiya Y, Kuwabara Y, Sasaki M, Yoshida T, Akashi Y,Murayama S, et al. FDG-PET in infectious lesions: Thedetection and assessment of lesion activity.Ann Nucl Med 1996;10:185-91.
147.Williams NH Jr, Kane C,Yoo OH. Pulmonary function inmiliarytuberculosis.Am Rev Respir Dis1973;107:858-60.
148.SharmaSK,AhluwaliaG.Effectofantituberculosistreatmenton cardiopulmonary responses to exercise in miliarytuberculosis.Indian J Med Res2006;124:411-8.
149.McClement JH,Renzetti JrAD,CarrollD,HimmelsteinA,Cournand A. Cardiopulmonary function in hematogenouspulmonarytuberculosisinpatientswithstreptomycintherapy.Am Rev Tuberc1951;64:588-601.
150.Sharma, SK, Ahluwalia G. Exercise testing in miliarytuberculosis–some facts. Indian J Med Res 2007; 125 :182-3.
151.World Health Organization. Treatment of tuberculosis:Guidelines for National Programmes. 3rd ed. WHO/CDS/TB/2003.313.Geneva:WorldHealthOrganization;2003.
152.BlumbergHM,BurmanWJ,ChaissonRE,DaleyCL,EtkindSC,FriedmanLN,et al;AmericanThoracicSociety,Centersfor Disease Control and Prevention and the InfectiousDiseases Society. American Thoracic Society/Centers forDiseaseControl and Prevention/InfectiousDiseases SocietyofAmerica.Treatmentoftuberculosis.Am J Respir Crit Care Med2003;167:603-62.
153.NationalInstituteforHealthandClinicalExcellence,NationalCollaborating Centre for Chronic Conditions. Managementof non-respiratory tuberculosis. In: Tuberculosis: clinical diagnosis and management of tuberculosis, and measures for its prevention and control. London: Royal College ofPhysicians;2006.p.63-76.
154.AmericanAcademy of Pediatrics Committee on InfectiousDiseases. Chemotherapy for tuberculosis in infants andchildren.Pediatrics1992;89:161-5.
155.World Health Organization. Treatment of tuberculosis.Guidelines.4thed.WHO/HTM/TB/2009.420.Geneva:WorldHealthOrganization;2009.
156.Sharma SK, Mohan A. Antituberculosis treatment inducedhepatotoxicity:frombenchtobed-side.In:GuptaSB,editor.Medicine update.Mumbai:AssociationofPhysiciansofIndia;2005.p.479-84.
157.SharmaSK.Antituberculosisdrugsandhepatotoxicity.Infect Genet Evol2004;4:167-70.
158.SaukkonenJJ,CohnDL,JasmerRM,SchenkerS,JerebJA,NolanCM,et al.AnofficialATSstatement:Hepatotoxicityofanti tuberculosis therapy.Am J Respir Crit Care Med2006;174:935-52.
159. SinglaR,SharmaSK,MohanA,MakhariaG,SreenivasV,Jha B, et al. Evaluation of risk factors for antituberculosistreatment induced hepatotoxicity. Indian J Med Res 2010; 132 :81-6.
160.Sarda P, Sharma SK, MohanA, Makharia G, JayaswalA,PandeyRM.Role of acute viral hepatitis as a confoundingfactor in antituberculosis treatment induced hepatotoxicity.Indian J Med Res2009;129:64-7.
161.SharmaSK,SinglaR,SreenivasV,KumarS,JhaB,RathoredJ, et al.Acuteviralhepatitisasaconfoundingfactorinpatientswithantituberculosistreatmentinducedhepatotoxicity.Indian J Med Res2009;130:200-1.
162.Sharma SK, Singla R, Sarda P, Mohan A, Makharia G,JayaswalA,et al.Safetyof3differentreintroductionregimensofantituberculosisdrugsafterdevelopmentofantituberculosistreatment-inducedhepatotoxicity.Clin Infect Dis 2010;50 :833-9.
163.JointTuberculosisCommitteeoftheBritishThoracicSociety.ChemotherapyandmanagementoftuberculosisintheUnitedKingdom:recommendations.Thorax1998;53:536-48.
SHARMAet al:DIAGNOSIS&TREATMENTOFMILIARYTB 729

164.SunTN,YangJY,ZhengLY,DengWW,SuiZY.Chemotherapyand its combination with corticosteroids in acute miliarytuberculosis inadolescents andadults: analysisof55cases.Chin Med J (Engl)1981;94:309-14.
165.MassaroD,KatzS, SachsM.Choroidal tubercles.A clue tohematogenoustuberculosis.Ann Intern Med1964;60:231-41.
166.MaraisS,WilkinsonRJ,PepperDJ,MeintjesG.Managementof patients with the immune reconstitution inflammatorysyndrome.Curr HIV/AIDS Rep2009;6:162-71.
167.World Health Organization. Rapid advice. AntiretroviraltherapyforHIVinfectioninadultsandadolescents.Geneva:WorldHealthOrganization;2009.
168.PozniakAL,CoyneKM,MillerRL,LipmanMCI,FreedmanAR, Ormerod LP, et al; BHIVA Guidelines Subcommittee.BritishHIVAssociationguidelines for the treatmentofTB/HIVcoinfection2011.HIV Med2011;12:517-24.
Reprint requests:DrSurendraK.Sharma,Professor&Head,DepartmentofMedicine,AllIndiaInstituteofMedicalSciences AnsariNagar,NewDelhi110029,India
e-mail:[email protected]
169.Guyatt GH, OxmanAD, Vist GE, Kunz R, Falck-Ytter Y,Alonso-CoelloP,et al;GRADEWorkingGroup.GRADE:anemergingconsensusonratingqualityofevidenceandstrengthofrecommendations. BMJ2008;336:924-6.
170.Trunz BB, Fine P, Dye C. Effect of BCG vaccination onchildhood tuberculous meningitis and miliary tuberculosisworldwide: a meta-analysis and assessment of cost-effectiveness.Lancet2006;367:1173-80.
171.AmericanThoracic Society.Targeted tuberculin testing andtreatment of latent tuberculosis infection.MMWR Recomm Rep2000;49:1-51
172.Kaufmann SH, Hussey G, Lambert PH. New vaccines fortuberculosis.Lancet2010;375:2110-9.
173.ParidaSK,KaufmannSH.Noveltuberculosisvaccinesonthehorizon.Curr Opin Immunol2010;22:374-84.
730 INDIANJMEDRES,May 2012


















