Physical/Orthopedic Disabilities By: Ashley Mucha EDN 410 Group B June 12th.
34
Physical/ Orthopedic Disabilities By: Ashley Mucha EDN 410 Group B June 12th
-
Upload
morris-gibson -
Category
Documents
-
view
217 -
download
0
Transcript of Physical/Orthopedic Disabilities By: Ashley Mucha EDN 410 Group B June 12th.

Physical/Orthopedic Disabilities
By: Ashley MuchaEDN 410 Group B June 12th
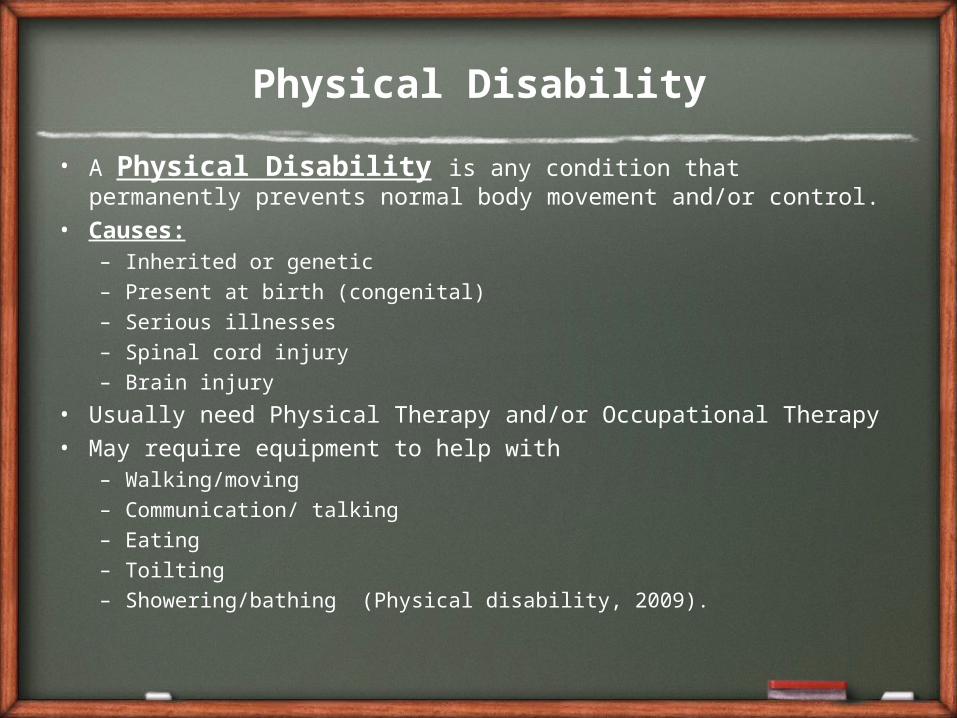
Physical Disability
• A Physical Disability is any condition that permanently prevents normal body movement and/or control.
• Causes:– Inherited or genetic– Present at birth (congenital)– Serious illnesses– Spinal cord injury– Brain injury
• Usually need Physical Therapy and/or Occupational Therapy• May require equipment to help with
– Walking/moving– Communication/ talking– Eating– Toilting– Showering/bathing (Physical disability, 2009).

List of Physical Disabilities
• Spina Bifida• Cerebral Palsy
• Multiple Sclerosis (MS)• Muscular Dystrophy (MD)
• Paralysis• Traumatic Brain Injury
Images from Google

Spina Bifida
• Spina bifida is a birth defect that involves the incomplete development of the spinal cord or its coverings.
• The term spina bifida comes from Latin and literally means "split" or "open" spine.
• Spina bifida occurs at the end of the first month of pregnancy when the two sides of the embryo's spine fail to join together, leaving an open area.
• In some cases, the spinal cord or other membranes may push through this opening in the back. The condition usually is detected before a baby is born and treated right away
• Children with spina bifida often have problems with bowel and bladder control, and some may have attention deficit hyperactivity disorder (ADHD) or other learning difficulties, such as hand-eye coordination problems.(Kids Health)

Spina Bifida: Types
• “1. Spina Bifida Occulta: There is an opening in one or more of the vertebrae (bones) of the spinal column without apparent damage to the spinal cord.
• 2. Meningocele: The meninges, or protective covering around the spinal cord, has pushed out through the opening in the vertebrae in a sac called the “meningocele.” However, the spinal cord remains intact. This form can be repaired with little or no damage to the nerve pathways.
• 3. Myelomeningocele: This is the most severe form of spina bifida, in which a portion of the spinal cord itself protrudes through the back. In some cases, sacs are covered with skin; in others, tissue and nerves are exposed. Generally, people use the terms “spina bifida” and “myelomeningocele” interchangeably” (Disability Fact Sheet, No. 12, 2004).
Image from: http://www.ncbi.nlm.nih.gov/pubmedhealth/PMH0002525/

Spina Bifida: Statistics
• Spina bifida occurs in seven of out every 10,000 live births in the United States.
• Spina Bifida Association of America estimates that more than 70,000 people in the United States are living with this birth defect.
• Women of childbearing age can reduce their risk of having a child with spina bifida by taking 400 micrograms (mcg) of folic acid every day since half of all pregnancies in the United States are unplanned. Women who have experienced a pregnancy affected by a NTD like spina bifida need a larger prescription dose of 4000 (mcg) of folic acid daily when planning a pregnancy.

Spina Bifida: In School
• Spina Bifida is usually dealt with when a child is very young, in school there would need to be accommodations for those children who have problems with:– Bowel and bladder control
• More frequent bathroom breaks or different bathroom privileges would need to be given to these children.
– ADHD– Learning Disabilities– Problems with hand-eye coordination
– They may also have occupational therapy if needed.

Cerebral Palsy• Affects:
– Muscle tone– Movement– Motor skills– Can also lead to:
• Hearing impairment• Vision impairment• Speech impairment• Learning disabilities
• One of the most common congenital (exists before or at birth) disorders.
• Causes of most are unknown: usually ->– Pregnancy complication
• Infections• Maternal heath
complications• anything that interferes
with brain development
– Premature birth– Brain damage in infancy
or early childhood
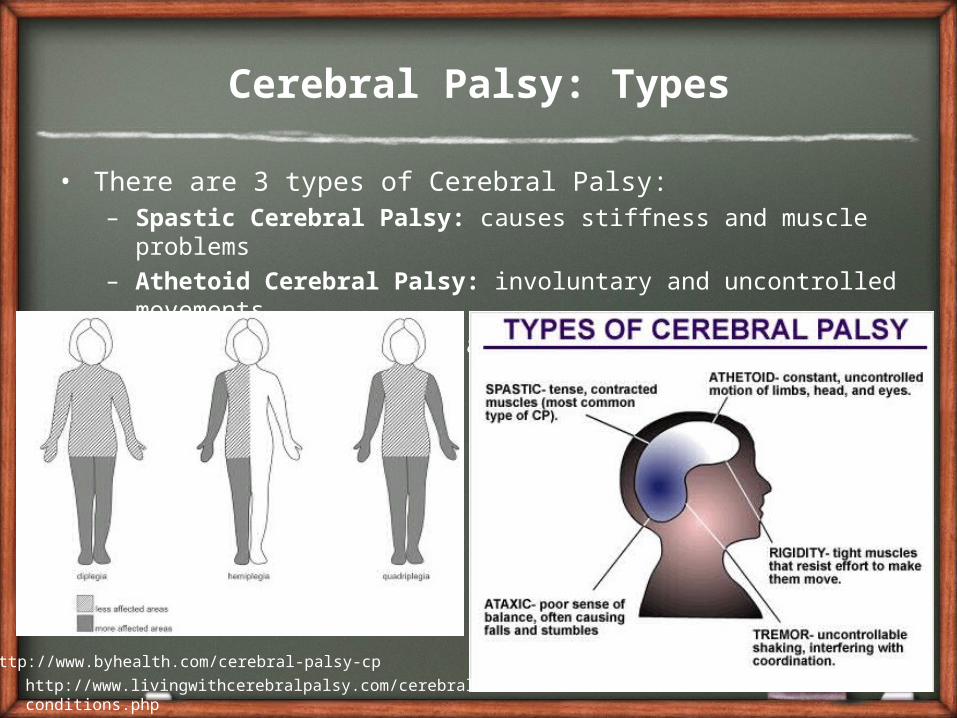
Cerebral Palsy: Types
• There are 3 types of Cerebral Palsy:– Spastic Cerebral Palsy: causes stiffness and muscle
problems– Athetoid Cerebral Palsy: involuntary and uncontrolled
movements– Ataxic Cerebral Palsy: affects balance and depth perception
http://www.byhealth.com/cerebral-palsy-cp
http://www.livingwithcerebralpalsy.com/cerebral-conditions.php

Cerebral Palsy: Statistics
• About 10,000 babies per year in the U.S. will develop cerebral palsy
• An estimated 800,000 people have cerebral palsy in US
• About 2-3 children per 1,000 have cerebral palsy
• Two-thirds of children with cerebral palsy will be mentally impaired
• (4 My Child: Help and Hope for Life)

Cerebral Palsy: In School
• Assistive technology is great for children with cerebral palsy.
• Many children with cerebral palsy have average intelligence and some have higher than average. As teachers we must remember that and give them every opportunity possible.
• Depending on what part of the brain is affected the child may have learning disabilities as well.
• Be sure that there is a clear communication line between parents and teachers. This makes a world of difference for any child with special needs, especially physical disabilities.
• No two children with cerebral palsy are alike. The disability can affect them mildly, moderately, or severely and as teachers we must be continually challenging their abilities.
Multiple Sclerosis (MS) • An autoimmune disease that affects the central nervous
system• The immune system mistakenly attacks the body’s own
tissues, usually the myelin that coats nerve cells• The scars that are produced from the attacks cause the nerve
impulses to be slow or interrupted. • The disease is VERY unpredictable.• Can cause visual disturbances, weakness, and other invisible
symptoms• It is a chronic illness • Pediatric MS is very uncommon and not well understood.• Many children with MS have difficulties in at least one major
cognitive domain. Therefore, cognitive testing and evaluation of school progress is essential.
• Causes are still unknown
Multiple Sclerosis: Statistics
• Estimates suggest that 8,000-10,000 children (defined as up to 18 years old) in the United States have multiple sclerosis, and another 10,000-15,000 have experienced at least one symptom suggestive of MS.
• Studies suggest 2 to 5% of all people with MS have a history of symptom onset before age 18.
• Increasing evidence suggests a slower disease course in children with MS, but significant disability can accumulate at an earlier age compared to individuals with adult onset MS.
• A similar frequency of girls to boys under the age of 10 years, but more girls than boys in the above 10 year old group.
• http://www.nationalmssociety.org/about-multiple-sclerosis/pediatric-ms/index.aspx

Multiple Sclerosis: In Schools
• Bladder symptoms requiring frequent, urgent trips to the bathroom
• Difficulty navigating stairs due to weakness, fatigue or poor balance
• A change in academic placement due to cognitive changes• Visual changes that, unknown to others, may come and go, and
interfere with classroom functioning• Depression or mood disorder• Inconsistent level of empathy and support from school staff • Isolation • Could cause frequent missed days from school which could
cause them to become behind. They will need extra support to help keep up in school.
• In some students, their memory, language, visual perceptions, motor functions, and cognitive abilities may be affected.
MS: In Schools (cont.)
• It is important to be flexible with students with MS, as their symptoms and abilities may change from week to week.
• Help to keep the child organized and be flexible with the homework load
• Be a support system: students with MS may lose an academic skill once it has been mastered. They will need more support though they may seem “normal”
• Students with MS may be considered Otherwise Health Impaired (OHI)
• Very low prevalence in children.
Helm, S., Karpinski, M., Milazzo, M., Rodriquez, E., Shaffer, C., Smith, L.L.,& Timmel, G.L. (2009)
Muscular Dystrophy (MD)
• Caused by a genetic disorder that weakens the muscles that help the body move.
• A person with MD has incorrect or missing information in their genes– This missing info prevents the person from making proteins for
healthy muscles
• People are born with this problem it it not contagious.• Muscles weaken over time. People gradually lose their ability
to walk or sit up.• Life expectancy depends on the type and severity of muscle
weakening• Affects the lungs and heart• No cure for MD- doctors are currently working to fix defective
genes• Physical and occupational therapy can work to help muscles
(Kids Health: Muscular Dystrophy, 2011)
Muscular Dystrophy: Types• Duchenne Muscular Dystrophy: most common type, problem with the
gene that makes dystrophin (helps muscles keep their strength and shape), affects boys, symptoms start between age 2-6.
• Becker Muscular Dystrophy: affects boys, similar to DMD, symptoms start later and are less severe, causes breathing, heart, bone, muscle and joint problems.
• Emery- Dreifuss Muscular Dystrophy: starts in late childhood, affects mostly boys, affects muscles in the shoulders, upper arms and chins.
• Limb-girdle Muscular Dystrophy: affects boys and girls equally, progresses slowly, many different types.
• Facioscapulohumeral Muscular Dystrophy: affects guys and girls in teen years, affects muscles in the face, shoulder and lower legs, can be very mild.
• Myotonic Dystrophy: a form of MD where muscles have problems relaxing• Congenital Muscular Dystrophy: Term for all types of MD that show signs
in babies and young children. Occurs in both boys and girls. Varies on how quick it progresses and weakens muscles.

Muscular Dystrophy: Statistics
• A quarter of a million kids and adults are living with the disease (Kids Health)
• 500 - 600 male newborns are diagnosed with muscular dystrophy each year in the US, Duchenne and Becker types (Wrong Diagnosis)
Muscular Dystrophy: In School
• Students with MD may need• physical therapy and bracing to improve flexibility• power wheelchairs and scooters to improve mobility• a ventilator to support breathing• robotics to help your child perform routine daily tasks• Flexibility with attendance• Teachers should use adaptive equipment to convey lessons
(Kids Health: Muscular Dystrophy, 2011)• Teachers must be careful not to pull on limbs, dislocation
could occur• Wheelchair accessible classrooms will be needed as most
children between 10-14 must use one.• Teachers need to be alert for signs of fatigue.• Teachers should always be promoting use of muscles
Paralysis• Loss of muscle function in part of your body.• Also called:
– Hemiplegia– Palsy– Paraplegia– Quadraplegia
• Caused when something goes wrong with the way messages pass between brain and muscles.– Main causes are stroke, spinal cord injury, or broken neck– Also caused by:
• Amyotrophic lateral sclerosis: Nerve diseases• Auto immune disease such as Guillain- Barre Syndrome• Bell’s palsy- affects facial muscles
• Polio was a past cause but no longer happens in the US (Paralysis: Medline, 2010).
http://www.nlm.nih.gov/medlineplus/paralysis.html

Paralysis: Types
• Can be complete or partial.• Can be on one side of your body or both• Can occur in just one area.
• Paraplegia: Lower half of your body.• Quadraplegia: affects the arms and legs

Paralysis: Statistics• The average age of those who reported being paralyzed was 52.• The average age of those who reported being paralyzed due to a
spinal cord injury was 48.• The average length of time since the paralysis occurred was 15.6
years.• The average length of time since the spinal cord injury occurred
was 14 years.• 54% of those who reported being paralyzed were males, while 46%
were females.• 61% of those who reported being paralyzed due to a spinal cord
injury were males, while 39% were females.• Males were nearly twice as likely (1.77) to incur a spinal cord injury as
females.• Causes: 29% Stroke, 23% Spinal cord injury, 17% Multiple sclerosis,
7% Cerebral Palsy, 5% Post- Polio Syndrome, 4% Neurofibromatosis, 4% Traumatic Brain Injury, 2% Unspecified Birth Defect (Paralysis Facts and Figures, n.d.)
Paralysis: In Schools
• Don’t lean on a student’s wheelchair (if used)• Make sure to keep crutches or canes near the
student’s desk• Ask the custodian to use non-skid polish• Plan field trips in advanced• Arrange room in a way that the student can
successfully move about the room• Allow student extra time to get where they need to go• Tape lectures as a student with paralysis may not be
able to write• Make sure the student has a desk with enough leg
room

Traumatic Brain Injury (TBI)
• May occur any time during the brain development stages.• The most frequent cause of disability and death in children• Injury to the brain by external force• Most frequent causes are from
– Automobile accidents– Falls– Sports– Abuse or assult
• Could cause:– Physical impairments: speech, language, hearing, headaches,
paralysis– Cognitive impairments: long and short term memory, short attention,
show thinking, concentration problems, learning disabilities– Psychosocial, behavioral, or emotional impairments: fatigue, mood
swings, anxiety, depression, low emotional control, difficulty relating to others

Traumatic Brain Injury: Statistics
• More than one million children sustain brain injuries every year and approximately 165,000 require hospitalization.
• Children aged 0 to 4 years, older adolescents aged 15 to 19 years, and adults aged 65 years and older are most likely to sustain a TBI.
• Almost half a million (473,947) emergency department visits for TBI are made annually by children aged 0 to 14 years.
• In every age group, TBI rates are higher for males than for females.
• Males aged 0 to 4 years have the highest rates of TBI-related emergency department visits, hospitalizations, and deaths. (Center of Disease control and Prevention)
Traumatic Brain Injury: In Schools
• Some students that have TBI have been incorrectly diagnosed as having learning disabilities, emotional disturbance, or mental retardation.
• Most students with TBI return to school after the incident that causes the injury. Their emotional needs may be very different than before.
• Teachers need to work hard to help them readjust to school.• They may know how they obtained their injury and could have
serious problems dealing with the sudden onset and change in their life.
• Teachers should also be a support for the family as this affects them drastically as well. Students need the most support as they are the ones having to change their life so suddenly.
• Teachers may need to supervise this student at all times.• Students with TBI need repetition and consistency, the least
amount of distractions, many rest breaks.(Traumatic Brain Injury Fact Sheet)
Universal Design for Learning
• Make sure to have wide hallways, ramps, elevators and doors that open easily or have handicap accessible capabilities.
• Use technology for extended access to class resources• Have assignments available online and through computer
programs• Use all different types of lessons that use many of the
multiple intelligences to present the information• Allow students to make choices about how they complete
assignments, learn the material, where they work in the classroom, and any other feasible choices that you can tolerate.
• Ask the child what he or she is needs for assistance
(Curry, 2003)
Assistive Technology
• Software that is built into the operating system
• Text-to-Speech software• Speech- to- Text Software• Portable word processers• Handwriting recognition programs• Electronic white boards• (Curry, 2003)

Physical Environment Accommodations: For All Physical
Disabilities
– Provide a second set of books to be kept at home; helps reduce fatigue
– Seat student near the teacher – Stand near the student when giving directions or presenting
lessons – Avoid distracting stimuli (high traffic area, etc.) – Seat student near door to allow easy exit – Allow student to leave classroom early to have extra time to
get to next classroom – Allow student to have water at his/her desk – Allow student time out of seat to stretch to avoid spasms – Allow use of bathroom pass if student has bowel or bladder
difficulties
Helm, S., Karpinski, M., Milazzo, M., Rodriquez, E., Shaffer, C., Smith, L.L.,& Timmel, G.L.

Lesson Presentation Accommodations:For All Physical Disabilities – Pair students to check work
– Provide written outline before class – use visual cues such as writing key points on the board – let student tape record lessons; assists in recall and processing
deficits– Provide peer tutoring– Have student review key points orally – Provide visual aids – Teach through multi-sensory modes – Provide peer note taker or provide a scribe – Use of Assistive Technology – Special computers depending on the specific child’s needs.– Enlarge notes for students with visual problems– Include a variety of activities during each lesson – Break longer presentations into shorter segments
Helm, S., Karpinski, M., Milazzo, M., Rodriquez, E., Shaffer, C., Smith, L.L.,& Timmel, G.L.

Test Taking:For All Physical Disabilities
– Allow open book exams– Allow extra time for exams (if not contraindicated due to
fatigue) – do not time exams – Give exams orally – Give take-home tests – Use more objective items and fewer essay responses – Allow student to give test answers on tape recorder – Continued individual or one on one assessments of learning– Special testing accommodations in other rooms, with someone
reading or helping to actually see what the student knows.
Helm, S., Karpinski, M., Milazzo, M., Rodriquez, E., Shaffer, C., Smith, L.L.,& Timmel, G.L.

Tips for Teachers• Be sure that there is a clear
communication line between parents and teachers. This makes a world of difference for any child with special needs, especially physical disabilities
• Be Flexible and understanding
• Always be an advocate for the child.
Informational Links• http://kidshealth.org/parent/system/ill/spina_bifida.html#
– Spina Bifida
• http://www.advocacyinstitute.org/UDL/index.shtm– Universal Design for Learning
• http://sped.wikidot.com/pe-for-the-physically-disabled– Physical Education for the Physically Disabled
• http://sped.wikidot.com/physical-disabilities– Information about Physical Disabilities
• http://www.as.wvu.edu/~scidis/motor.html– Strategies for working with students with Physical Disabilities

ReferencesCAST. (2008). Universal design for learning questions and answers. The advocacy institute. Retrieved
from http://www.advocacyinstitute.org/UDL/faqs.shtml.Curry, C. Universal design: Accessibility for all learners. (2003). Educational Leaders, 61(2). Retrieved
from http://www.ascd.org/ASCD/pdf/journals/ed_lead/el200310_curry.pdfKids health: Spina bifida, muscular dystrophy, multiple sclerosis, cerebral palsy . (2011). The
Nemours Foundation. Retrieved from http://kidshealth.org/parent/system/ill/spina_bifida.html.Pediatric MS. (n.d.). National Multiple Sclerosis Society. Retrieved from
http://www.nationalmssociety.org/about-multiple-sclerosis/pediatric-ms/index.aspxPhysical Disability. (2009). Parenting and child- Health topics. Retrieved from
http://www.cyh.com/HealthTopics/HealthTopicDetails.aspx?p=114&np=306&id=1874Pralysis. (2010). Paralysis: MedLine Plus. Retrieved from
http://www.nlm.nih.gov/medlineplus/paralysis.htmlPralysis facts and figures. (n.d.). Christopher and dana reeves foundation. Retrieved from
http://www.christopherreeve.org/site/c.mtKZKgMWKwG/b.5184189/k.5587/Paralysis_Facts__Figures.htm
Spina bifida: Disability fact sheet, no. 12. (2004). National Dissemination Center for Children with Disabilities.
Spina bifida statistics. (2011). Spina bifida association of america. Keller, E. (2005). Strategies for teaching students with motor/orthopedic impairments. Retrieved from
http://www.as.wvu.edu/~scidis/motor.htmlHelm, S., Karpinski, M., Milazzo, M., Rodriquez, E., Shaffer, C., Smith, L.L.,& Timmel, G.L.
(2009).Students with ms and the academic setting: A handbook for school personnel. National Multiple Sclerosis Society.
The state of cerebral palsy: Facts and figures. (n.d.). 4MyChild. Retrieved from http://www.cerebralpalsy.org/what-is-cerebral-palsy/statistics.
Traumatic brain injury fact sheet. (1997). National information center for children and youth with disabilities. Retrieved from http://www.theteachersguide.com/TraumBrainInjuryFactSheet.html










![ALFONS MUCHA - old · 3 Alphonse Mucha. The Master of Art Nouveau. Text by Ji ří Mucha. Translated [z češ. do angl.] by Geraldine Thomsen. P., Artia 1966. 291, [1] s.](https://static.fdocuments.in/doc/165x107/5b0879997f8b9a51508be6ca/alfons-mucha-alphonse-mucha-the-master-of-art-nouveau-text-by-ji-r-mucha-translated.jpg)