Physical Activity and Obesity
10
311 From: Contemporary Endocrinology: Treatment of the Obese Patient Edited by: R. F. Kushner and D. H. Bessesen © Humana Press Inc., Totowa, NJ 16 Physical Activity and Obesity John M. Jakicic, PhD, Amy D. Otto, PhD, RD, LDN, Kristen Polzien, PhD, and Kelli K. Davis, MS CONTENTS INTRODUCTION CONTRIBUTION OF PHYSICAL ACTIVITY TO TOTAL ENERGY EXPENDITURE CAN PHYSICAL ACTIVITY PREVENT WEIGHT GAIN? PHYSICAL ACTIVITY FOR WEIGHT LOSS AND PREVENTION OF WEIGHT REGAIN DEVELOPMENT OF EXERCISE PRESCRIPTION FOR WEIGHT CONTROL CONCLUSION ACKNOWLEDGMENTS REFERENCES Summary There is an increasing prevalence of overweight and obesity in the United States and other developed countries. This can have significant public health implications because of the association of excess body weight with increased risk of chronic diseases. It has been suggested that the increas- ing prevalence of excess body weight (overweight and obesity) and related diseases also has a significant impact on health care costs. Physical activity can significantly affect weight control and can also have an independent effect on associated chronic disease risk factors. However, physical activity participation is less than optimal. Thus, it is important for health care professionals to understand the role of physical activity in weight loss, the prevention of weight gain, and the prevention of weight regain, and to understand how to provide accurate and meaningful information to their patients. Key Words: Exercise; overweight; fitness; weight control. INTRODUCTION Obesity, physical activity, and poor dietary behaviors have been linked to increased health risk, which may contribute to 300,000 to 400,000 additional deaths per year in the United States (1). This may in part be a result of the increasing prevalence of overweight (body mass index [BMI] 25.0 kg/m 2 ) and obesity (BMI 30.0 kg/m 2 ), with these rates estimated to be approx 65% and 30% in adults, respectively (2,3). Moreover, it is esti- mated that 16% of children and adolescents ages 6 to 19 yr are obese (4). The increasing prevalence of overweight and obesity results in associated health risks from an increase
-
Upload
senarath-bandara -
Category
Documents
-
view
8 -
download
0
description
Health
Transcript of Physical Activity and Obesity

Chapter 16 / Physical Activity and Obesity 311
311
From: Contemporary Endocrinology: Treatment of the Obese PatientEdited by: R. F. Kushner and D. H. Bessesen © Humana Press Inc., Totowa, NJ
16 Physical Activity and Obesity
John M. Jakicic, PhD, Amy D. Otto, PhD, RD, LDN,Kristen Polzien, PhD, and Kelli K. Davis, MS
CONTENTS
INTRODUCTION
CONTRIBUTION OF PHYSICAL ACTIVITY TO TOTAL
ENERGY EXPENDITURE
CAN PHYSICAL ACTIVITY PREVENT WEIGHT GAIN?PHYSICAL ACTIVITY FOR WEIGHT LOSS AND PREVENTION
OF WEIGHT REGAIN
DEVELOPMENT OF EXERCISE PRESCRIPTION FOR WEIGHT CONTROL
CONCLUSION
ACKNOWLEDGMENTS
REFERENCES
SummaryThere is an increasing prevalence of overweight and obesity in the United States and other
developed countries. This can have significant public health implications because of the associationof excess body weight with increased risk of chronic diseases. It has been suggested that the increas-ing prevalence of excess body weight (overweight and obesity) and related diseases also has asignificant impact on health care costs. Physical activity can significantly affect weight control andcan also have an independent effect on associated chronic disease risk factors. However, physicalactivity participation is less than optimal. Thus, it is important for health care professionals tounderstand the role of physical activity in weight loss, the prevention of weight gain, and theprevention of weight regain, and to understand how to provide accurate and meaningful informationto their patients.
Key Words: Exercise; overweight; fitness; weight control.
INTRODUCTION
Obesity, physical activity, and poor dietary behaviors have been linked to increasedhealth risk, which may contribute to 300,000 to 400,000 additional deaths per year in theUnited States (1). This may in part be a result of the increasing prevalence of overweight(body mass index [BMI] �25.0 kg/m2) and obesity (BMI �30.0 kg/m2), with these ratesestimated to be approx 65% and 30% in adults, respectively (2,3). Moreover, it is esti-mated that 16% of children and adolescents ages 6 to 19 yr are obese (4). The increasingprevalence of overweight and obesity results in associated health risks from an increase

312 Jakicic et al.
in numerous chronic diseases that include heart disease, diabetes, and various forms ofcancer (1). These increased obesity-related health risks may contribute to more than$100 billion in annual health care costs. Thus, the development and implementation ofinterventions that result in weight loss, prevention of weight gain, and prevention ofweight regain can significantly reduce the health burden and have an impact on publichealth.
It has been demonstrated that a reduction in body weight and an increase in physicalactivity may facilitate the management of body weight and reduce the risk and onset ofobesity-related diseases (1). However, it is estimated that only 20% of adults in theUnited States participate in adequate levels of physical activity to improve their health(5), and it is clear that most children do not participate in adequate amounts of physicalactivity (5). Thus, it is important for health care professionals to understand the role ofphysical activity in the prevention of weight gain, weight loss, and the prevention ofweight regain, and to understand how to provide accurate and meaningful informationto their patients.
CONTRIBUTION OF PHYSICAL ACTIVITY TO TOTAL ENERGYEXPENDITURE
Whether body weight remains stable, increases, or decreases is ultimately dependent onthe balance or imbalance between energy intake (calories consumed) and energy expen-diture. To reduce body weight, energy expenditure must exceed energy intake, whereas toprevent weight gain or to maintain weight loss, energy expenditure must equal energyintake. Thus, the effect of an increase in energy expenditure on body weight is also depen-dent on the relative contribution of energy intake to energy balance. This section will focuson the contribution of the components of energy expenditure on energy balance.
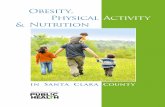
There are three basic component of energy expenditure: resting energy expenditure(REE), thermic effect of food (TEF), and voluntary physical activity (Fig. 1). Although itis recognized that REE can vary among individuals, and there are physiological, meta-bolic, and genetic influences on REE, the REE within a given individual remains rela-tively stable, provided that weight and health status remain stable. Moreover, despite thelarge contribution of REE to total energy expenditure, limited studies have shown theability of lifestyle interventions to increase REE; this is especially true during weightloss when REE tends to decrease (6,7). Thus, it appears that interventions targeting anincrease in REE will have a small and limited impact on total energy expenditure for mostindividuals, which will result in a limited impact on body weight.
TEF is the increase in energy expenditure resulting from the food that is consumed toallow for the necessary components of digestion. Ravussin et al. (8) have suggested thatTEF is approx 10% of total daily energy expenditure. Moreover, TEF is influenced bythe macronutrient content of the food that is consumed. Despite the potential increase inTEF based on dietary composition, this increase in energy expenditure is relatively smallcompared with the total daily energy expenditure. Moreover, this would require a sig-nificant increase in a specific macronutrient content sustained over a relatively longperiod of time to significantly and independently affect body weight. Thus, attemptingto affect body weight solely through an increase in TEF is not practical and will likelyresult in minimal impact. A more detailed discussion of this issue is not within the scopeor focus of this chapter.

Chapter 16 / Physical Activity and Obesity 313
Leisure-time physical activity (LTPA) is the most variable component of energyexpenditure. LTPA can occur in the form of structured exercise, lifestyle activity, orother forms of activity that contribute to an increase in energy expenditure. The amountof the increase in energy expenditure varies based on the amount of LPTA that is per-formed. For example, an individual who is relatively inactive will expend approx 30%more calories above what is expended in REE, with this increasing to approx 50% or 80%for individuals participating in moderate or higher amounts of LTPA, respectively (seeFig, 1). Thus, it is important to understand the contribution of an increase in total dailyenergy expenditure resulting from LTPA on energy balance, which can affect the pre-vention of weight gain, weight loss, the prevention of weight regain following weightloss.
CAN PHYSICAL ACTIVITY PREVENT WEIGHT GAIN?
Close examination of prevalence data indicates the need to focus intervention effortson the prevention of weight gain. If effective, this will decrease the likelihood of atransition from normal weight to overweight or obesity, and decrease the transition fromoverweight to obesity. There is some evidence that LTPA can play a significant role inthe prevention of weight gain; this is mostly likely a result of the increase in energyexpenditure resulting from an increase in LTPA. For example, there are data from pro-spective observation studies that appear to support this hypothesis. Lee and Paffenbarger(9) concluded that participants in the Harvard Alumni Study who reported levels ofphysical activity consistent with approx 30 min of moderate-intensity physical activityhad a lower body weight when compared with individuals reporting lower levels ofphysical activity. When change in cardiorespiratory fitness is used as a surrogate forchange in LTPA, the data reported by DiPietro et al. (10) demonstrate the inverse asso-ciation between change in fitness and change in body weight, which also supports theimportance of physical activity in the prevention of weight gain in adults.
Fig. 1. Contribution of varying levels of leisure-time physical activity (LTPA) to total energyexpenditure (TEE) for a fix resting energy expenditure (REE - 1800 kcal/d) and thermic effectof a metal (TEM = 180 kcal/d).

314 Jakicic et al.
The application of these prospective, observational findings need to be apply to inter-ventions to have a meaningful impact on weight gain prevention. In fact, Sherwood etal. (11) reported that an increase in physical activity was predictive of prevention ofweight gain. Moreover, preliminary data are available from an ongoing clinical trial thatis being conducted in our research center. Results indicated that an increase in physicalactivity (150 to 300 min/wk) resulted in prevention of weight gain or modest weight loss(1–2 kg) in approx 60% of overweight adults (BMI = 25.0–29.9), with change in fitnesspredictive of prevention of weight gain (unpublished data).
These findings are important when considered in context of the recommendations forphysical activity in the prevention of weight gain that appeared in the 2005 US DietaryGuidelines, which stated that to prevent weight gain there is a need for individuals to“engage in approximately 60 minutes of moderate- to vigorous-intensity activity onmost days of the week while not exceeding caloric intake requirements.” Cliniciansshould consider individually tailoring these recommendations based on the response ofthe participant. For example, it has been established that approx 30 min of moderate-intensity physical activity per day on most days of the week can result in a significantreduction in the risk of chronic diseases. Thus, individuals should increase to this levelof activity and determine whether this level of physical activity is sufficient to preventweight gain. If it is not, the recommended level of physical activity can gradually beincreased (e.g, 30 to 35 min/wk, 35 to 40 min/wk, etc.) until weight gain ceases. This isillustrated in the flow chart provided in Fig. 2.
PHYSICAL ACTIVITY FOR WEIGHT LOSS AND PREVENTIONOF WEIGHT REGAIN
Short-Term Weight LossIt has been clearly established that effective behavioral weight-loss interventions
result in approximately a 10% weight loss compared to initial body weight within 6 moof initiating an intervention (12). These results appear to be achievable with the combi-nation of a reduction in energy intake and an increase in energy expenditure (1). How-ever, the contributions of each of these components (reduction in energy intake andincrease in energy expenditure) are not equal, with the majority of weight loss resultingfrom a reduction in energy intake. In response to a 12-wk intervention, Hagan et al. (13)reported a reduction in body weight of 8.4% in males and 5.5% in females, with Winget al. (14) reporting 9.1% in response to a 24-wk intervention, with energy intake rangingfrom 1000 to 1500 kcal/d. The addition of exercise to a reduction in energy intakeresulted in weight loss of 11.4% and 7.5%, respectively in males and females (13), withWing et al. (14) reporting weight loss of 10.4%. In these studies, exercise alone resultedin weight loss of 0.3, 0.6, and 2.1%, respectively (13,14). These findings support theconclusions of the clinical guidelines developed by the National Institutes of Health thatrecommend the combination of a reduction in energy intake and an increase in energyexpenditure to maximize weight loss in response to a behavioral intervention (1).
Long-Term Weight Loss and Weight-Loss MaintenanceDespite the minimal effect of exercise on short-term weight loss, exercise appears to
be an important component of long-term interventions. This is supported by the 2005 USDietary Guidelines (15), the Institute of Medicine (16), and extensive reviews of the

Chapter 16 / Physical Activity and Obesity 315
Fig
. 2. E
xam
ple
of e
xerc
ise
prog
ress
ion
to p
reve
nt w
eigh
t ga
in o
r w
eigh
t re
gain
.

316 Jakicic et al.
literature (17,18). However, a common conclusion that appears to be supported by cross-sectional data, prospective observational data, and data from clinical trials is that physi-cal activity equivalent to �2000 kcal/wk or approx 250 to 300 min/wk is associated withimproved long-term weight loss at 12 to 24 mo (19–24). These results appear to supportthe recommendation of the US Dietary Guidelines that 60 to 90 min/d is required toprevention weight regain following significant weight loss (15).
It appears that adequate levels of physical activity do not act alone to control bodyweight long-term, but rather work in synergy with appropriate levels of energy intake.For example, Jakicic et al. (25) reported that the combination of increased levels ofphysical activity combined with reduced levels of energy intake were predictive of long-term weight-loss outcomes following an 18-mo intervention. Similar findings werereported by McGuire et al. (26) based on data from the National Weight Control Reg-istry. Thus, these data appear to support the importance of maintaining adequate levelsof energy balance (energy intake and energy expenditure) to enhance long-term weightloss and prevent weight regain following weight loss. Thus, it is important for cliniciansto address these components of energy balance equally when providing interventions foroverweight and obese adults.
DEVELOPMENT OF EXERCISE PRESCRIPTIONFOR WEIGHT CONTROL
Exercise ModeThe majority of clinical trials have incorporated aerobic forms of physical activity
(i.e., brisk walking) into the weight loss interventions; overweight/obese individualsreport that walking is the self-selected mode of physical activity for 80 to 90% of activitysessions (20). This may be a result of ease of participation for most individuals, the lowcost of participation, and lack of need for special skills to participate in this form ofphysical activity.
Despite these findings, additional forms of physical activity have been examined forweight control with mixed results. For example, a review of the scientific literaturerevealed no apparent improvement in weight loss with the addition of resistance exercise(27), and preliminary data from our laboratory appear to support this conclusion (35).Moreover, Jannsen et al. (28) reported no significant improvement in risk factors withthe addition of resistance exercise when compared with weight loss resulting from dietalone. However, there is initial evidence, that despite these findings, that resistanceexercise has been associated with a reduction in all-cause mortality (29). Moreover,resistance exercise will improve muscular strength (30,31), which may affect physicalfunction of overweight and obese adults (32). Despite these potential benefits, resistanceexercise has not been shown to be more effective for weight loss or the maintenance ofweight loss compared with other forms of physical activity. Thus, although more re-search is needed to understand the role of resistance exercise for weight control, this formof exercise may be appropriate when used as a complement to other forms of physicalactivity such as walking.
Because of the potential functional limitations of overweight and obese adults, alter-native forms of physical activity may need to be considered. Yoga has been shown toimprove range of motion and physical function, while reducing pain (33,34). However,there are limited data to support the addition of yoga to interventions to improve weight

Chapter 16 / Physical Activity and Obesity 317
loss. Results from a 12-mo weight-loss intervention that included yoga as a complementto aerobic forms of physical activity and a reduction in energy intake demonstrate noimprovement in weight loss when compared with interventions not including yoga (35).Another popular recommendation is to include aquatic forms of physical activity foroverweight adults, as this may overcome functional limitations in overweight and obeseindividuals. Again, the limited data in this area of research do not indicate that weightloss is improved with the addition of aquatic exercise compared with other forms ofphysical activity (36). These factors should be considered by clinicians when recom-mending physical activity to overweight and obese adults when weight loss is the pri-mary outcome, and used to enhance LTPA and energy expenditure for individuals whofind these activities enjoyable.
Physical Activity Intensity vs VolumeCurrent recommendations for physical activity to control body weight appear to
indicate that approx 60 to 90 min/d may be required to prevent weight gain or improvelong-term weight loss (15). Moreover, although the accumulation of at least 10,000 stepsper day, measured using a pedometer, may be associated with improvements in health-related parameters (37), it has been suggested that it may be necessary to progressivelyincrease daily steps to levels above 10,000 steps per day to improve weight loss (38).Thus, clinicians should focus on progressively increasing the total volume of physicalactivity to maximize energy expenditure in overweight and obese adults. This couldinvolve increasing duration by 10 min/d or by 1000 steps/d at approximately 4-wkintervals until the desired level of physical activity is attained.
The total volume of physical activity, expressed as energy expenditure, may be moreimportant for weight control than the intensity of the physical activity that is performed.For example, Duncan et al. (39) have demonstrated that when total volume of physicalactivity is held constant, there is no difference in the effect on body weight acrossdifferent intensities of physical activity. Similar results have been reported by Jakicic etal. (20), who demonstrated that the magnitude of weight loss was affected by volume ofphysical activity rather than the intensity of physical activity within a 12-mo clinicaltrial.
Even though total volume of physical activity may be more important than the inten-sity of physical activity for promoting weight control, this does not suggest that anadequate intensity of physical activity to improve cardiorespiratory fitness is not impor-tant. In fact, there is a growing body of literature to support the need for sufficientimprovements in cardiorespiratory fitness independent of body weight, with higher levelsof fitness reducing health-related risk even in overweight and obese adults (40–43). More-over, this may also result in a reduction in all-cause mortality independent of body weight(44). However, these data appear to only apply to individuals with a BMI <35, as thereare limited data to support the independent effects of physical activity on health-relatedoutcomes and mortality for individuals above this level of BMI.
An additional factor when considering the volume of physical activity is whether thisneeds to be done in a continuous manner to have an effect on the desired outcomes. Infact, there are numerous studies to support that intermittent exercise performed in mul-tiple bouts of at least 10 min in duration can significantly improve desired outcomes.These outcomes can include cardiorespiratory fitness (45–47) and selected risk factors(46). Moreover, intermittent physical activity may provide an effective strategy for

318 Jakicic et al.
improving initial adoption of physical activity in overweight and obese adults (21,47).This may provide a strategy for clinicians when addressing physical activity for indi-viduals who are resistant to traditional forms of physical activity that require continuousexercise for periods ranging from 20 to 60 min per session.
CONCLUSION
Excessive body weight that results in overweight or obesity has been linked to signifi-cant health risks for numerous chronic conditions (1). A continuing challenge for clini-cians is to address the increasing prevalence of weight gain in patients to preventoverweight or obesity, and to prevent weight regain following initial weight loss. How-ever, it appears that physical activity can contribute to a significant increase in energyexpenditure, which will facilitate long-term weight control provided that a sufficientdose of physical activity is performed. It appears that the level of physical activitynecessary for prevention of weight gain and to enhance long-term weight loss mainte-nance ranges from approx 30 to 60 min/d (15,17–20). Therefore, clinicians should encour-age patients to progressively increase physical activity to this range (see Fig. 2) in additionto maintaining a complementary level of energy intake. This may require clinicians toindividually tailor these recommendations to the needs of the patient in a progressive andsystematic manner to enhance both weight control and health-related outcomes in over-weight and obese adults.
ACKNOWLEDGMENTS
The efforts of Dr. Jakicic, Dr. Otto, Dr. Polzien, and Ms. Davis are supported byresearch funding from the National Institutes of Health (HL70257, HL67826,DK066150).
Dr. Jakicic is on the scientific advisory boards for the Coca-Cola Beverage Institutefor Health and Wellness, the Calorie Control Council, and BodyMedia, Inc.
REFERENCES
1. National Institutes of Health, National Heart, Lung and Blood Institute. Clinical Guidelines on theIdentification, Evaluation, and Treatment of Overweight and Obesity in Adults—The Evidence Report.Obes Res 1998;6(suppl.2).
2. Flegal KM, Carroll MD, Ogden CL, et al. Prevalence and trends in obesity among US adults, 1999–2000. JAMA 2002;288(14):1723–1727.
3. Hedley AA, Ogden CL, Johnson CL, et al. Prevalence of overweight and obesity among US children,adolescents, and adults, 1999–2002. JAMA 2004;291:2847–2850.
4. Ogden CL, Flegal KM, Carroll MD, et al. Prevalence and trends in overweight among US children andadolescents, 1999-2000. JAMA 2002;288(14):1728–1732.
5. US Department of Health and Human Services. Physical Activity and Health: A Report of the SurgeonGeneral. US Department of Health and Human Services, Centers for Disease Control and Prevention,National Center for Chronic Disease Prevention and Health Promotion, Atlanta, GA: 1996.
6. Donnelly JE, Pronk NP, Jacobsen DJ, et al. Effects of a very-low-calorie diet and physical-trainingregimenson body composition and resting metabolic rate in obese females. Am J Clin Nutr 1991;54:56–61.
7. Geliebter A, Maher MM, Gerace L, et al. Effects of strength or aerobic training on body composition,resting metabolic rate, and peak oxygen consumption in obese dieting subjects. Am J Clin Nutr1997;66:557–563.

Chapter 16 / Physical Activity and Obesity 319
8. Ravussin E, Bogardus C. Relationship of genetics, age, and physical fitness to daily energy expendi-ture and fuel utilization. Am J Clin Nutr 1989;49:968–975.
9. Lee I-M, Paffenbarger R. Associations of light, moderate, and vigorous intensity physical activity withlongevity: the Harvard Alumni Health Study. Am J Epidemiol 2000;151(3):293–299.
10. DiPietro L, Kohl HW, Barlow CE, Blair SN. Improvements in cardiorespiratory fitness attenuate age-related weight gain in healthy men and women: the Aerobics Center Longitudinal Study. Int J Obes1998;22:55–62.
11. Sherwood NE, Jeffery RW, French SA, et al. Predictors of weight gain in the Pound of Preventionstudy. Int J Obes 2000;24:395–403.
12. Wing RR. Behavioral weight control. In: Wadden TA, Stunkard AJ, eds. Handbook of Obesity Treat-ment. Guilford Press, New York: 2002; pp. 301–316.
13. Hagan RD, Upton SJ, Wong L, et al. The effects of aerobic conditioning and/or calorie restriction inoverweight men and women. Med Sci Sports Exerc 1986;18(1):87–94.
14. Wing RR, Venditti EM, Jakicic JM, et al. Lifestyle intervention in overweight individuals with afamily history of diabetes. Diabetes Care 1998;21(3):350–359.
15. Department of Health and Human Services and Department of Agriculture. Dietary Guidelines forAmericans: www.healthierus.gov/dietaryguidelines; 2005.
16. Institute of Medicine. Dietary Reference Intakes for Energy, Carbohydrates, Fiber, Fat, Protein andAmino Acids (Macronutrients): A Report of the Panel on Macronutrients, Subcommittees on UpperReference Levels of Nutrients and Interpretation and Uses of Dietary Reference Intakes, and theStanding Committee on the Scientific Evaluation of Dietary Reference Intakes. National AcademiesPress, Washington, DC: 2002.
17. Jakicic JM, Clark K, Coleman E, et al. American College of Sports Medicine position stand: appro-priate intervention strategies for weight loss and prevention of weight regain for adults. Med Sci SportsExerc 2001;33(12):2145–2156.
18. Saris WHM, Blair SN, van Baak MA, et al. How much physical activity is enough to prevent unhealthyweight gain? Outcome of the IASO 1st Stock Conference and consensus statement. Obes Rev2003;4:101–114.
19. Jakicic JM, Marcus B, Lang W. Effect of varying doses of exercise on 24-month weight loss inoverweight adults. Obes Res 2005;13(suppl):A24.
20. Jakicic JM, Marcus BH, Gallagher KI, et al. Effect of exercise duration and intensity on weight lossin overweight, sedentary women. A randomized trial. JAMA 2003;290:1323–1330.
21. Jakicic JM, Winters C, Lang W, et al. Effects of intermittent exercise and use of home exerciseequipment on adherence, weight loss, and fitness in overweight women: a randomized trial. JAMA1999;282(16):1554–1560.
22. Jeffery RW, Wing RR, Sherwood NE, et al. Physical activity and weight loss: Does prescribing higherphysical activity goals improve outcome? Am J Clin Nutr 2003;78(4):684–689.
23. Klem ML, Wing RR, McGuire MT, et al. A descriptive study of individuals successful at long-termmaintenance of substantial weight loss. Am J Clin Nutr 1997;66:239–246.
24. Schoeller DA, Shay K, Kushner RF. How much physical activity is needed to minimize weight gainin previously obese women. Am J Clin Nutr 1997;66:551–556.
25. Jakicic JM, Wing RR, Winters-Hart C. Relationship of physical activity to eating behaviors and weightloss in women. Med Sci Sports Exerc 2002;34(10):1653–1659.
26. McGuire MT, Wing RR, Klem ML, et al. What predicts weight regain in a group of successful weightlosers? J Consult Clin Psychol 1999;67(2):177–185.
27. Donnelly JE, Jakicic JM, Pronk NP, et al. Is resistance exercise effective for weight management?Evidence Based Prev Med 2004;1(1):21–29.
28. Jannsen I, Fortier A, Hudson R, et al. Effects of an energy-restrictive diet with or without exercise onabdominal fat, intermuscular fat, and metabolic risk factors in obese women. Diabetes Care2002;25(3):431–438.
29. Jurca R, LaMonte MJ, Church TS, et al. Association of muscle strength and aerobic fitness withmetabolic syndrome in men. Med Sci Sports Exerc 2004;36(8):1301–1307.
30. Kraemer WJ, Volek JS, Clark KL, et al. Physiological adaptations to a weight-loss dietary regimen andexercise programs in women. J Appl Physiol 1997;83(1):270–279.
31. Kraemer WJ, Volek JS, Clark KL, et al. Influence of exercise training on physiological and perfor-mance changes with weight loss in men. Med Sci Sports Exerc 1999;31:1320–1329.

320 Jakicic et al.
32. Jakicic JM. Physical activity considerations for the treatment and prevention of obesity. Am J ClinNutr 2005;82(1 Suppl):226S–229S.
33. Oken BS, Zajdel D, Kishiyama S, et al. Randomized, controlled, six-month trial of yoga in healthyseniors: effects on cognition and quality of life. Altern Ther Health Med 2006;12(1):40–47.
34. Williams KA, Petronis J, Smith D, et al. Effect of iyengar yoga therapy for chronic low back pain. Pain2005;115:107–117.
35. Gallagher KI, Jakicic JM, Otto AD, et al. Examination of twelve month changes in body weight andbody composition following alternative forms of exercise. Med Sci Sports Exerc 2005;37(5(suppl):S339.
36. Nagle EF, Otto AD, Jakicic JM, et al. Effects of aquatic plus walking exercise on weight loss andfunction in sedentary obese females. Med Sci Sports Exerc 2003;35(5 (suppl):S136.
37. Tudor-Locke C, Bassett DR. How many steps/day are enought? Preliminary pedometer indices forpublic health. Sports Med 2004;34(1):1–8.
38. Yamanouchi K, Takashi T, Chikada K, et al. Daily walking combined with diet therapy is a usefulmeans for obese NIDDM patients not only to reduce body weight but also to improve insulin sensi-tivity. Diabetes Care 1995;18(6):775–778.
39. Duncan JJ, Gordon NF, Scott CB. Women walking for health and fitness: how much is enough? JAMA1991;266(23):3295–3299.
40. Barlow CE, Kohl HW, Gibbons LW, et al. Physical activity, mortality, and obesity. Int J Obes 1995;19:S41–S44.
41. Farrell SW, Braun L, Barlow CE, et al. The relation of body mass index, cardiorespiratory fitness, andall-cause mortality in women. Obes Res 2002;10(6):417–423.
42. Lee CD, Blair SN, Jackson AS. Cardiorespiratory fitness, body composition, and all-cause and car-diovascular disease mortality in men. Am J Clin Nutr 1999;69(3):373–380.
43. Wei M, Kampert J, Barlow CE, et al. Relationship between low cardiorespiratory fitness and mortalityin normal-weight, overweight, and obese men. JAMA 1999;282(16):1547–1553.
44. Church TS, LaMonte MJ, Barlow CE, et al. Cardiorespiratory fitness and body mass index as predic-tors of cardiovascular disease mortality among men with diabetes. Arch Intern Med 2005;165:2114–2120.
45. DeBusk R, Stenestrand U, Sheehan M, et al. Training effects of long versus short bouts of exercise inhealthy subjects. Am J Cardiol 1990;65:1010–1013.
46. Ebisu T. Splitting the distances of endurance training: on cardiovascular endurance and blood lipids.Jap J Phys Edu. 1985;30:37–43.
47. Jakicic JM, Wing RR, Butler BA, et al. Prescribing exercise in multiple short bouts versus one con-tinuous bout: effects on adherence, cardiorespiratory fitness, and weight loss in overweight women.Int J Obes 1995;19:893–901.