IDEOLOGICAL WARFARE · Title: IDEOLOGICAL WARFARE Subject: IDEOLOGICAL WARFARE Keywords
description

1
PHM142 Metabolic Biochemistry and Immunology WHITE CELLS
CHEMICAL WARFARE lecture outline1) Molecular mechanisms of leukocyte function (live 2 days)
• Rheumatoid arthritis• Chronic Granulomatous Disease CGD
2) Eosinophils-live 8-12 days when activated (live 8-12 days when not activated). Contain peroxidase, RNase, DNase, lipase
3) Macrophages (greek:big eaters; 21um), amoeboid movement Phagocytose foreign cells AND produce growth factors and
cytokines• But macrophages also induce tissue injury• Cause multiple organ failure, Acute Resp.Distr.Syndr., sepsis

2White (Immune) Cells Type of cell
Red blood cells (erythrocytes)
White blood cells (leukocytes) polymorphonuclear/granular leukocytesNeutrophils (50 60%)Eosinophils (1 4%)
Basophils (0.5 2%)
Mononuclear leukocytes:
Lymphocytes (20 40%)
Monocytes (2 9%)( macrophages in extravascular tissue)Killer cells
Megakaryocytes ( platelets)
Main function
Transport O2 and CO2
Destroy invading bacteria
Phagocytose & kill invading antigensDestroy parasites and modulate allergic inflammatory reactions.Release histamine, serotonin, bradykinin, heparin, and cytokines; converts arachidonic acid to prostaglandins & leukotrienes
(T & B) mediate cytokine release
Phagocytose & kill ingested microbes Kill virally infected cells and tumor cells (offer “natural” immunity as well as adaptive)
Initiate blood clotting; also release histamine and serotonin

3
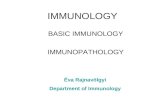
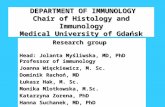
Thin sections of the major types of white blood cells (leukocytes) foundin the circulation, showing the variety of internal structures observed.
12
Macrophage3

4Molecular mechanisms of neutrophil functionAmer J Med. 109, 33-44 (2000)
Neutrophil membrane electron transport
CYTOSOL
PHAGOSOME MEMBRANE
PHAGOSOME VACUOLE
H2O2
H2O
GSH
GSSG
NADP+
NADPH
Glucose
glucose-6-phosphate
glucose-6-phosphatedehydrogenase
6 P gluconic acid
H2O2 O2.-
O2
NADP+
NADPH
Glucose-6-P
Gluconic acid
NADPHoxidase
Intracellularly in white cells
H2O2 + Cl- HOCl Bactericidalmyeloperoxidase
1
2
2
Fe2+

Inflammation or infection
MPO(myeloperoxidase), HOCl(hypochlorite), SOD (superoxide dismutase).
HOCl + red cell GSH = GSH cyclic sulfonamide (biomarker for HOCl formation in vivo that reflects inflammation (oxidant formed by neutrophils))
5
Living with a killer: The effects of hypochlorite/hypobromite on mammalian cells Chem.Res.Toxicol.21,1011-6 (2008)

6
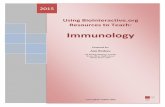
Activation of leukocyte NADPH oxidase (Nox) showing assembly of the enzyme and fusion of the oxidase-containing vesicle with the phagosomal membrane.
Babior, 2000. American Journal of Medicine. 109:33 44.

7
NADPH oxidase (Nox)Activation DON’T MEMORISE!
Proton Channel Function
Medicine 79, 170-200 (2000)
b558
+ H+
ProtonChannel
(phosphorylationby kinase)
gp91phox is b558 with proton channel (or K+?)
phox is “phagocyte oxidase”
membrane
Vacuolar space
b558

8
bact.
• CGD can kill Bacteria that produce H2O2 and have low catalase activity, e.g., streptococci.• But can’t kill bacteria which have high catalase activity or low H2O2 production, e.g., serratia, nocardia, and aspergillus; fungal, staphylococcus, burkholderia (pneumonia, sepsis).
Chronic Granulomatous Disease (CGD)
NADPH OXIDASE DEFICIENCY
White Cell
0.1 M Chloridein blood

• NOX1 – colon > prostate, uterus, breast,macrophage
• NOX2 - phagocyte H2O2 for MPO >> hepatocyte,
B lymphocyte, cardiomyocytes, endothelial cells
• NOX3 inner ear, fetus
• NOX4 kidney, bloodvessels,cardiomyocytes,endoth.
• NOX5 lymphoid tissue,testis
NADPH oxidase family - makes antibacterial H2O2

10
leukocytes
Synovium (synovial fluid)
From Am J Med. (2000). 190:33-44
Rheumatoid Arthritis is an autoimmune inflammatory disease that may affect (skin, blood vessels, heart, lungs, muscles-- but principally attacks joints (proliferative synovitis progressing to cartilage destruction/joint ankylosis.
Pathogenesis (unknown etiology):genetic susceptibility; joint damage mediated by leukocytes or exogenous arthritogen (virus, mycobacteria).
Babior, 2000. American Journal of Medicine. 109:33 44.

NSAID therapy for RA IBUPROPHEN COX-1 inhib. 300mg 3 times perday
Cardiovascular & GI bleeding risk,inhib platelets, kidney/liver tox.
ALEVE (Naproxen) 200mg otc ; lasts 12h
• Inhibits inflammation , COX-I and COX-2 inhibitor
• Decrease pain, temp, muscle pain, menstrual cramps • Lower stroke risk than ibuprofen; high dose risk GI bleed.
VIOXX COX-2 inhibitor for OA,RA 1999 introd.
• 2004 (withdrawn due to heart attack, stroke)
CELEBREX (celecoxib)1998 COX-2 inhib.400mg
• low cardiorenal tox, platelet effects & GI bleeding
11

Side effects of COX-1 inhibitors• e.g. Aspirin may cause stomach bleeding and risk
GI ulcer formation as a result of stomach cell mitochondrial uncoupling and acidosis.
• inhibits COX-1 activity thereby increasing tissue unsat. fatty acid levels and causing acidosis.
• decreases PGE2 levels that protect stomach membr.
• inhibits thromboxane formn. and platelet aggreg. • unsat.fatty acid + PGS(prostaglandin synthase) attacks protective
mucous layer
12

Mechanism of NSAID induced GI toxicity
• Stage I NSAIDs decrease intestinal mucosal prostanoids (PGE,TXB2, 6-keto-PGF)
• Mitochondrial uncouplers (e.g.indomethacin,DNP) compromised intestinal barrier). Resp.inhibited
• Stage 2 mild inflammation + aspirin
• Stage 3 histopathology, ulcers and bleeding
• Rat model: ulcers, intestinal inflammation or gastric permeability induced by indomethacin or DNP + Cox inhib (aspirin).
Aliment Pharmacol. Ther. (2000) 14,639-650
13

14Rheumatoid Arthritis Therapy
Repetitive hypoxia in joints, and endothelial cells
ATP hydrolysis
Hypoxanthine from ATP
ROS
Reperfusion O2 +endothelial cell xanthine oxidase
ALLOPURINOLinhib.
endothelial cell nitric oxide
peroxynitriteDestruction of joint
Uric acidMonosodium urate crystals in joint

15

16
Anti-Inflammation therapy
• ROS Scavenger Therapy SOD, selenomethionine/Vit E, 5-aminosalicylate, penicillamine:Cu • Macrophage inhibitor therapy: Gold thiomalate or auranofin or zinc or copper salicylate• Prostaglandin Synthetase Inhibitors:-(NSAIDS) COX-1 many cells e.g.aspirin,ibuprofen, but GI bleeding,kidney COX-2 inflammatory cells e.g. VIOXX (withdrawn), CELEBREX but
cardiovascular problems.• “Biologics” antibodies that inhibit inflammatory cytokines e.g.TNF-α• Diet: decrease arachidonate intake (meat), increase omega 3 fatty acids (fish)
decreases bad prostaglandins, decrease Fe intake References: Semin. Arthritis Rheum. 27: 366-70 (1998). Autoimmunity Reviews 7,1-7(2007) Anti-inflammatory Biologics

17
EOSINOPHILS: (chemical warfare cont.)
Accumulate in parasite infection, asthma, rheumatoid diseases, Hodgkin’s lymphoma and allergic or inflammatory diseases
1)destroy parasitic worms, tumor cells, fungi and bacteria by forming hypobromite
H2O2 + Br- + H+ HOBr (hypobromite) + H2O
2) cytokine production e.g. PAF, LTC4 unlike neutrophils (leukocytes) .
2
Biochem J. 358, 233-239 (2001),
Journal of Biological Chemistry270 (7) 2905-2913(2000).
MPO

• White blood cells within tissue, have a role in innate and adaptive immunity
• They engulf pathogens and debris via phagocytosis, and move around via amoeboid movement
18

19
MACROPHAGES - chemical warfare function
1) Endocytosis and exocytosis via specific receptors for IgG and C3 coated in bacteria2) H2O2 production by NADPH oxidase to kill mycobacteria3) Arachidonate oxidation to prostaglandin4) Cytokine production - upon activation by PDGF a) lipopolysaccharide (endotoxin) TNF- b) immune system activation BCG infection IL-1 c) inflammation or interferon (IFN-) PAF TGF and arginine nitric oxide kill tumor cells
5) endocytosis and delivery to lysosomes (via scavenger receptor) of oxidised LDL (low density lipoprotein) - can result in transformation to foam cell (the basis of the formation of atherosclerotic plaque)
3

Tumor Necrosis Factor (TNFα) as the primary trigger for
inflammatory response
Macrophages,monocytes,lymphocytes,keratinocyte
• TNFα incr in chronic inflammatory diseases:
rheumatism,arthritis,encephalitis,tumors Rheumatoid arthritis , psoriasis,Crohn’s disease
• Proinflammatory > antiinflammatory cytokines
• DRUG THERAPY: NSAIDs, GC glucocorticoids, Disease Modifying Antirheumatic Drugs (DMARDs).
20

21
Drug induced hepatocyte cytotoxicity caused by activated immune cells releasing cytokines and reactive oxygen species
(Kupffer cells , macrophages ,neutrophils) i
1) Toxic doses of drugs or chemicals injure hepatocytes. Injured hepatocytes release factors that attract Kupffer cells to specificregions of the liver. 2) Additional mononuclear phagocytes are also recruited from blood and bone marrow precursors. 3) Once localised in the liver, the macrophages become activated by hepatocyte-derived factors of endothelial cells. 4) Activated macrophages and endothelial cells release cytokines e.g.TNFα & platelet activating factor prime & activate Kupffer cells which release Reactive Oxygen Species and more cytokines. 5) Some chemoattractants and cytokines can attract and activate neutrophils that also contribute to hepatocyte injury.

22Macrophages and Tissue Injury
Toxicant
Target tissues
Activated macrophagese.g. Kupffer cells
Mediators
Cytotoxicity Amplification
Model for the role of macrophages in tissue injury by generating inflammatory mediators.
Gold thiomalateGadolinium chloride(macrophage inhibitor)
Tissue Injury

Macrophage killing mechanism
• Macrophage oxid.LDL which are then endocytosed by the oxid LDL receptor.
Present antigens to T cells as foreign substances
• Exocytose (via specific receptors) IgC and C3 coated bacteria
• H2O2 kills mycobacteria and form cytokines PDGF,PAF,TNFα & β, IL1
• Unsaturated fatty oxidation to aldehydes causes foam cell formation & plaque formation from macrophages.
23

24 Inflammatory mediators implicated in toxicity Toxicant
Mediator Lung Liver
1) Reactive oxygen intermediates Ozone Endotoxin (H2O2, .OH) Asbestos Acetaminophen
Amiodarone Corynebacterium parvum Reactive nitrogen intermediates Bleomycin (peroxynitrite) Carbon tetrachloride
1,2-dichlorobenzenePhenobarbitalEndotoxin
2) Hydrolytic enzymes Endotoxin (collagenase, elastase) Silica 3) Lipids Hyperoxia (leukotrienes, prostaglandins, thromboxanes)
4) IL-1 Cigarette smoke
5) TNF- (mitochondrial toxin, Cadmium chloride Alcohol reactive oxygen species)
Toxicology 160, 111 8 (2001).Ann. Rev. Pharmacol. Toxicol. 35, 655 (1995).

4. Biologics: anti-cytokine antibodies • TNF blockers 1)Etanercept for RA • 2) Infliximab (remicade)Crohns disease, • drug antigen?, cancer a chimeric human Fab.
3) Adalimumab (Humira) human monoclonal for macular degen.
4)Stelera for psoriasis, 5 shots p.a.$50K • Rituximab kills ANCA-vasculitis NEJM363,221-232(2010) & CD20 B
cell,NH lymphoma,RA, Wegeners ? • Abatacept,fusion protein inhib.T cell costim.RA• Avastin (bevacizumab) inhib.VEGF-A (vascular endoth.growth factor,eye
mac.degen, breastcancer).Withdrawn.
25

B cells named from bursa of fabricius(birds)
• Plasma cells are large B cells exposed to antigens which produce antibodies that bind to microbes. In tissues not plasma.
• Contain rough e.r. & cell rapid apoptosis (short life)
• Memory B cells formed from activ.B cells(long life)
• 23% B-1 cells IgM>IgG in peritoneal & pleural cavities
• B-2 cells
26

Immunosuppressants and anti-inflammatories RA
• B cell depleting agents like rituximab
• human monoclonal antibody against IL-6R cytokine
27

Biomarkers for inflammation diseasePro-inflammatory cytokines
• Elevated cytokines CRP,IL-1B,IL-1B,IL-6,IL-8
• Tumor necrosis factor alpha
• c-ANCA anti-neutrophil cytoplasmic stain Myeloperoxidase is the target antigen,Wegeners
• p-ANCA anti-neutrophil perinuclear stain
Proteinase 3 is the target antigen
• x-ANCA chronic inflammatory bowel disease
28

Biomarkers for determining oxidative stress associated with inflammation diseases
• 1) Plasma lipid hydroperoxide
• 2) Oxidative DNA damage DNA 8-OHdQ
• Urinary 8-OHdQ
• Thymine oxidation HMdU
• DNA strand breaks (Comet assay)
• 3) Protein carbonyls using dinitrophenylhydrazine
• Protein oxidation - cysteine, methionine, histidine
• Protein AGEs
• 4) Fructose oxidation forms toxic glyoxal
29

30