Pharynx Anatomy and conditions
45
Pharynx Anatomy and conditions
Transcript of Pharynx Anatomy and conditions

Pharynx Anatomy and conditions

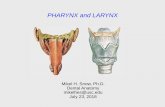
• The pharynx is a fibromuscular tube that is semicircular in cross section and is situated directly anterior to the vertebral column.

Nasopharynx
Behind the nose and above the soft palate.
In front it communicates through choanae with the nasal cavities
The lateral wall contains the pharyngeal ostium of the ET.
The pharyngeal recess (fossa of Rosenmüller)
Posterosuperior wall (Basisphenoid)
Pharyngobasilar fascia (Ant. To Atlas)


Oropharynx
• communicates anteriorly with the oral cavity proper .
• superiorly by the undersurface of the soft palate and inferiorly by the root of the posterior tongue and the epiglottis.

• The posterior root of the tongue exhibits numerous follicles that contain lymphatic tissue, which are known collectively as lingual tonsils.

• the palatoglossal arch and the palatopharyngeal arch .. the tonsillar fossa, which contains the palatine tonsils .

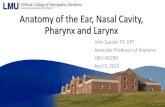
Laryngopharynx ( hypopharynx)
• its superior border is the epiglottis and oropharynx and its inferior border is the posterior surface of the cricoid cartilage of the larynx.

On either side of
the laryngeal
orifice is a recess,
termed the sinus
pyriformis, which is
bounded medially
by the
aryepiglottic fold,
laterally by the
thyroid cartilage
and hyothyroid
membrane .

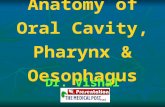
Nerve supply of the pharynx
• Pharyngeal Plexus
• Situated in the buccopharyngeal fascia surrounding the pharynx
• Supplies most innervation to pharynx; composed of CN IX (sensory), CN X (motor) & sympathetics from superior cervical ganglion .
• except the stylopharyngeus ( derives motor innervation from the glossopharyngeal nerve)

Blood supply of the pharynx
1) Ascending pharyngel a. 2) Facial a. (ascending
palatine & tonsillar branches).
3) Maxillary a. (greater palatine & pterygoid branches).
4) Superior thyroid a. Venous drainage through
the pharyngeal plexus to the internal jugular & anterior facial veins.


Adenotonsillar disease
• Adenoids : – They develop from a subepithelial infiltration of
lymphocytes in the 16th week of gestation.
– One component of the waldeyer ring .
– present at birth and then begin to enlarge. They, along with the tonsils, continue to grow until individuals are aged 5-7 years.
– The adenoids can become infected and harbor pathogenic bacteria, which may lead to the development of disease of the ears, nose, and sinuses .


• Presentation :
• nasal airway obstructive symptoms (eg, nasal congestion, snoring, sleeping with open mouths) adenoid facies
• Recurrent sinusitis , otitis media ,

Chronic mouth breathing changes
• Dull facial expression
• Dilated and flattened nose
• Open mouth
• High vaulted palate
• Protruding upper incisor teeth


Treatment
• Antibiotics (may not have much value)
• Nasal corticosteroid
• Adenoidectomy Complications:
• Hemorrhage
• Otitis media
• Regrowth of residual adenoid tissue
• Rhinolalia aperta (nasal speech)

Tonsillitis
• inflammation of the palatine tonsils.
• Most cases of bacterial tonsillitis are caused by group A beta-hemolytic Streptococcus pyogenes (GABHS).


• Signs and symptoms • Fever • Sore throat • Foul breath • Dysphagia (difficulty swallowing) • Odynophagia (painful swallowing) • Tender cervical lymph nodes • Airway obstruction may manifest as mouth
breathing, snoring, sleep-disordered breathing, nocturnal breathing pauses, or sleep apnea.

• Diagnosis
• clinical diagnoses
• throat cultures are the criterion standard for detecting GABHS.

Peritonsillar abscess (Quinsy)
• Definition: - collection of pus forming outside the capsule of the tonsil in close
relationship to its upper pole.
• Etiology: GABH in 50% of cases.
The infection spreads to the peritonsillar area (peritonsillitis). This region comprises loose connective tissue susceptible to formation of abscess. Both aerobic and anaerobic bacteria can be causative. Commonly involved species include streptococci, staphylococci and hemophilus.
• Epidemiology: - occur as complication of acute tonsillitis.
- more in adults (15-30) than in children.

Clinical features
• Fever, dehydration.
• severe dysphagia
• Edema of soft palate
• Uvular deviation (downward and medially)
• Involvement of motor branch of CN V increased salivation and trismus (Persistent contraction of
the masseter muscles due to failure of central inhibition)
• Hot potato voice
• Unilateral referred otalgia


• Etiology of pseudomembranous tonsillitis
– Epstein–Barr virus (mononucleosis)
– Candidiasis
– Vincent’s angina
– Neisseria gonorrhea
– Syphilis
– Corynebacterium diphtheria
– Group A β-hemolytic Streptococcus

Infectious mononucleosis (glandular fever)
• usually presents as severe membranous tonsillitis.
• EBV spread by close contact.
• The node enlargement is marked and malaise is more severe than expected from tonsillitis.
• Diagnosis confirmed by lymphocytosis within a week monospot test positive ( less sensitive in < 2 years of age ) .

Diphtheria • Corynebacterium diphtheriae • Very rare • insidious onset • characterized by a grey membrane
(difficult to remove) on the tonsils, fauces and uvula.
• Pyrexia usually low and diagnosis is confirmed by examination and culture of a swab.
• Hx of recent travel.


• Complications of adenotonsillectomy
• Postoperative hemorrhage: 0.5–10 %
• °Postoperative pulmonary edema: due to loss of auto-PEEP from chronic obstruction and
• VPI (velopharyngeal insufficiency )
• Nasopharyngeal stenosis
• Atlantoaxial subluxation (Grisel’s syndrome )
laxity of anterior transverse ligament; Down syndrome children more prone to this
Diagnosis: MRI or CT C-spine
Treatment: muscle relaxants, benzodiazepines, spine consultation/traction, cervical collar, NSAIDs
• Malodorous breath (most common complaint)

Obstructive Sleep Apnea Syndrome
• OSA : Recurrent episodes of partial or complete airway obstruction during sleep in the presence of breathing effort, necessitating recurrent awakenings or arousals to reestablish airway patency, often with oxygen desaturation.

Epidemiology
• Relatively common disorder .
• 3% to 7% in adult men and 2% to 5% in adult women .
• The prevalence increases with age.
• 1% of OSAHS patients are receiving appropriate treatment.

Consequences of Untreated Obstructive Sleep Apnea
• Significant increase in mortality • Effect on the cardiovascular system, including
hypertension, coronary heart disease, congestive heart failure, arrhythmias, sudden death, pulmonary hypertension, and stroke.
• Increase the risk of fatal and nonfatal motor vehicle accidents by 2.5-fold .
• independent risk factor for insulin resistance. • The prevalence of gastroesophageal reflux
disease (GERD) in OSA patients is significantly higher than in the general population.

Pathophysiology
• OSA is caused by soft tissue collapse in the pharynx.
• mechanism of collapse is multifactorial :
Anatomic factors : decrease in the cross-sectional area of the upper airway and/or increase the pressure surrounding the airway.
Neuromuscular factors .

• Nasal obstruction : contributes to increased airway resistance and may worsen OSA, but it is rarely the sole cause.
• Adenotonsillar hypertrophy : major cause of obstructive sleep apnea in children not in adult .

• Obesity :
• The increased fat deposition is postulated to narrow and compress the upper airway .
• effects on metabolism, ventilation, and lung volume.

• RISK FACTORS: • age, male gender, obesity, and craniofacial or upper
airway soft tissue abnormalities. • smoking, nasal congestion, menopause, and family
history. • medical conditions, such as pregnancy, end-stage renal
disease, congestive heart failure, chronic lung disease, stroke
• Acromegaly • Hypothyroidism • polycystic ovary syndrome

Diagnosis
• Symptoms :
• Daytime sleepiness
• Snoring
• Morning headaches

• Polysomnography :
• gold-standard diagnostic test for OSA .
• night-to-night variability in polysomnography results.

• DISEASE SPECTRUM • classified as having mild, moderate or severe disease
on the basis of symptoms and the apnea-hypopnea index (AHI).
• Mild :AHI between 5 and 15 respiratory events. • Moderate:AHI between 15 and 30 respiratory events
per hour of sleep. • Severe:AHI greater than 30 respiratory events per hour
of sleep and/or an oxyhemoglobin saturation below 90 percent for more than 20 percent of the total sleep time.

Treatment
• Medical Treatment
1. Weight loss :
should be recommended for all overweight patients with OSA.
bariatric surgery and morbidly obese.

2) Continuous positive airway pressure (CPAP):
Gold standard treatment for moderate to severe OSA .
Reduction in AHI, improvement in objective and subjective sleepiness, improvement in overall quality of life, reduction in risk of cardiovascular events, and reduction of the risk of motor vehicle accidents.
Patient adherence remains a significant obstacle.

• Surgical Treatment :
• According to patient’s wishes, CPAP tolerance, severity of symptoms, severity of disease, patient comorbidities, and site and severity of upper airway collapse.

• The site of obstruction must be determined in each patient to determine the type and extent of surgical intervention .

Tracheotomy
• the traditional gold standard of surgical management of OSA.
• considered in patients :
• failed all other OSA treatments,
• patients who have life-threatening OSA and are unable to tolerate CPAP,
• neurodevelopmentally impaired.