Pharyngeal tumor
37
Pharyngeal tumor Ahmad talalqa Abdullah maaitah
-
Upload
ahmadtalalqa -
Category
Health & Medicine
-
view
522 -
download
0
Transcript of Pharyngeal tumor

Pharyngeal tumor
Ahmad talalqa Abdullah maaitah

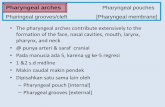
Anatomy of pharynx
The pharynx is a musculomembranous tube that extends from the base of the skull to the level of the sixth cervical vertebra.
Pharynx composed of 3 distinct areas: Nasopharynx : The upper portion of the pharynx, the
nasopharynx, extends from the base of the skull to the upper surface of the soft palate
Oropharynx: located between the soft palate and the superior border of the epiglottis.
Laryngopharynx : located between the superior border of the epiglottis and inferior border of the cricoid cartilage (C6),
Pharyngeal walls composed of superior, middle & inferior pharyngeal constrictor muscles.

Anatomy of pharynx


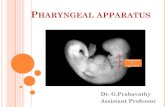
Histology of pharynx
The pharynx is lined by both stratified squamous epithelium and ciliated pseudostratified epithelium with goblet cells (resp. epi.). Different regions are lined by a different type of epithelium. Regions of the pharynx that are likely to be roughened up by food are lined by stratified squamous epithelium. Other regions of the pharynx are lined by ciliated pseudostratified epithelium with goblet cells.

Types
Squamous cell carcinomas most head & neck cancers
Others: Lymphoepithelioma Spindle cell carcinoma Undifferentiated carcinoma Lymphoma (most often widespread non-Hodgkin's lymphoma)

Risk Factors
Smoking or chewing tobacco Alcohol abuse High doses of radiation therapy, particularly in the head or neck
region Exposure to asbestos or certain industrial chemicals Aging (being 65 years or older)

Type-Specific Risk Factors Nasopharyngeal cancers
People of Chinese or Asian descent Epstein-Barr virus (EBV)
Oropharyngeal cancer Drinking maté (an herbal tea drink common in South America) Human papillomavirus (HPV) infection
Hypopharyngeal cancer Nutritional deficiencies
Iron deficiencies (plummer-Vinson syndrome)Alcohol abuse

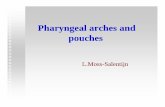
Esophageal web
Plummer-Vinson syndrome :rare disease characterized by difficulty in swallowing, iron deficiency anemia, and esophageal webs. Pre-malignant post cricoid carcinoma.
Treatment with iron supplementation and mechanical widening of the esophagus

Diagnosis
History Depending on the location and extent of the cancer Sore throat A lump in the nose or back of the mouth, throat, or neck A change of voice, or unusual hoarseness Dysphagia Coughing Trouble breathing, or feeling "stuffed up" Ear pain Ringing in the ears A dull pain behind the sternum Headaches Unexplained weight loss

Diagnosis
Physical examination may include visual inspection of the oral and nasal cavities, neck, throat, and tongue using a small mirror and/or lights.
neck mass consisting of painless firm lymph node enlargement Investigation :1. Head, neck and chest X-rays2. Endoscopy3. Ultrasound 4. CT scan5. MRI6. PET scan (Positron Emission Tomography)

arterial blood supplyarterial blood supply of the pharynx include the ascending pharyngeal artery , the ascending palatine branch of the facial artery , the descending palatine and pharyngeal branches of the maxillary artery, and the muscular branch of the superor thyroid artery. the veins of the pharrynx the veins of the pharrynx are similar in name to the arteries and drain into the pterygoid plexus and the internal jugular veinsInnervation pharynx innervated by nerve branches from the pharyngeal plexus supplied by the glossopharyngeal and vagus nerves.

Progression
Spreads by: Local extension and through the destruction of adjacent tissue,
with bony infiltration being a common early finding, can invade the orbit (eye), the skull and the bones of the spinal cord.
Lymphatic invasion with spread to the cervical lymph nodes is common at cancer diagnosis.
Haematogenous spread to distant sites such as the liver, bones, lungs and spleen may also have occured at the time of cancer diagnosis.

Nasopharyngeal tumors
Benign (non-cancerous) & malignant (cancerous). Benign tumors
Rare Occur in children and young adults Include tumors or malformations of the vascular
system, such as angiofibromas and hemangiomas, and benign tumors of the minor salivary glands that are found within the nasopharynx.

Benign but locally aggressive vascular tumor that grows in the back of the nasal cavity. It most commonly affects adolescent males. Patients usually present with one-sided nasal obstruction and recurrent bleeding.

Malignant nasopharyngeal tumors

Presentation Neck mass (most common initial symptom, 70%).
Serous otitis media from eustachian tube obstruction (second most common presentation, 50%).
Nasal obstruction. Cranial nerve palsies (abducent nerve most common cranial nerve palsy) Villaret's
syndrome* Recurrent epistaxis.
Trismus, headache.

Risk Factors:
Regional distribution (Southern China, Northern Africa, Southeast Asia, Alaska, Greenland).
Epstein-Barr Virus (EBV) most immunological finding in nasopharyngeal cancer
Genetic predisposition (genotypes HLA-A2 and HLA-Bsin2).
Nitosamines (smoked meat and salted fish).

World Health Organization (WHO) Classification
WHO Type I: Keratinizing Squamous Cell Carcinoma, squamous differentiation, not associated with EBV, worse prognosis, less sensitive to radiation.
WHO II: Nonkeratinizing Squamous Cell Carcinoma, does not demonstrate definite squamous differentiation, associated with EBV, better prognosis, sensitive to radiation .
WHO III: Undifferentiated (includes lymphoepitheliomas, anaplastic, and clear cell variants): indistinct cell margins, may have lymphocytic stroma (lymphoepitheliomas), associated with EBV, better prognosis, sensitive to radiation

Staging (based on the AJCC Staging) T1: primary tumor confined to nasopharynx T2: primary tumor extension into nasal fossa or oropharynx (without
parapharyngeal extension [T2a], with parapharyngeal extension [T2b])
T3: invasion of bony structures or paranasal sinuses
T4: invasion into intracranium, cranial nerves, infratemporal fossa, hypopharynx, or orbit


Diagnostic Tests
Diagnosis is made by biopsy of the nasopharyngeal mass. Workup includes the following: • Careful visual examination (by fiberoptic endoscopic examination or examination under anesthesia [EUA]). • Documentation of the size and location of the tumor and neck nodes. • Evaluation of cranial nerve function including neuro-ophthalmological evaluation and audiological evaluation. • Computed tomographic (CT) scan or positron emission tomography (PET)-CT scan. • Magnetic resonance imaging (MRI) to evaluate skull base invasion. • Epstein-Barr virus titers.

Oropharyngeal tumor

Benign oropharyngeal tumor Papilloma: usually asymptomatic, surgical excision is the
treatment of choice.(HPV) Haemangioma: may be capillary or cavernous. Treatment is
diathermy coagulation or injection of sclerosing agents. Cryotherapy and laser coagulation is also effective
Pleomorphic adenoma: mostly seen submucosally on the hard or soft palate. It is potentially malignant and should be excised totally.
Mucous cyst: usually seen in vallecula. Surgical excision is the treatment of choice in case of symptomatic cysts
Lipoma

Pleomorphic adenoma Papilloma

Malignant oropharyngeal tumor Squamous cell carcinoma being by far the most common
histologic type. The most important causative factors are prolonged
tobacco and alcohol exposure Potential fascial spaces : • The retropharyngeal space • the parapharyngeal space When invasion does occur, tumors may spread into these potential spaces.

Tonsil and tonsillar fossa (most common) Base of tongue Posterior pharyngeal wall
Common sites of malignancy in oropharynx are:

CARCINOMA TONSIL

Presentation
• Older than 45 years of age • Throat discomfort. • Odynophagia • Otalgia* • Trismus, dysphagia, and dysarthria may develop with deeper invasion. • Bleeding, aspiration, airway obstruction, and weight loss (Late). • Neck mass (most of the patients with oropharyngeal primaries present with cervical adenopathy at the time of diagnosis)

Staging (AJCC)for oropharyngeal carcinoma• TX Primary tumor cannot be assessed • T0 No evidence of primary tumor • Tis Carcinoma in situ • T1 Tumor =2cm in greatest dimension • T2 Tumor >2cm but not more than 4cm in greatest dimension • T3 Tumor >4cm in greatest dimension or extension to lingual surface of the epiglottis T4a Moderately advanced, local disease.Tumor invades the larynx, deep/extrinsic muscle of the tongue, medial pterygoid, hard palate, or mandible T4b Very advanced, local disease.Tumor invades lateral pterygoid muscle, pterygoid plates, lateral nasopharynx, or skull base or encases the carotid artery

Hypopharyngeal tumor
Not common ; 0.5% of all malignancies. Very poor prognosis Almost all of them are SCC Malignant types:
CA. of the piriform fossa in males Post cricoid CA. in females Vast majority of patients present with at least stage III
disease. History of heavy smoking and drinking, hoarsness of voice. Asymptomatic neck mass, dysphagia Surgery followed by Radiation therapy


General Stage Stage I (T1, N0, M0)
Limited to one region Oropharynx or hypopharynx tumour are smaller than a peanut (2 cm) Not spread (M0) beyond its origin.
Stage II (T2, N0, M0) Grown into another region of the pharynx or nearby soft tissues Or may have spread into nearby lymph nodes Not spread (M0) to distant sites.
Stage III (T3, N1, M0): Grown beyond the site of origin May have spread into nearby soft tissues or lymph nodes.
Stage IV: (Any T, Any N, M1) May be any size Spread throughout the body.

Treatment
Surgery Preferred treatment for most oropharyngeal and hypopharyngeal cancers. The cancer is considered localized Tumor is considered surgically resectable . Likely to obtain clean surgical margins
Radiotherapy Postoperative to improve clinical outcomes Higher-stage or larger tumors Local invasion or metastasis May be used by itself or in combination with chemotherapy in cases where
the tumor may be too large to be surgically removed Most cases of nasopharyngeal cancer ((no role for surgery in
treatment)) Useful as palliative treatment

Chemotherapy Sometimes used with radiation in metastatic, unresectable and/or
recurrent tumors. Postsurgically with radiation in late-stage or aggressive cancers. Rarely effective by itself in pharyngeal cancer, but is instead a
valuable part of a multimodality treatment approach. Immunotherapy
In Advanced Nasopharyngeal Cancers, because associated with Epstein-Barr virus (EBV) infection, an immunotherapeutic treatment was designed to target this virus. Investigators isolated T cells from the blood of EBV-positive nasopharyngeal cancer patients, and then modified the T cells to attack the EBV virus.

Prognosis Pharynx cancer tends to grow silently with symptoms of cancer often
not evident until the cancerous disease is quite advanced. The early the diagnosis the better the prognosis Involvement of lymph nodes in the region is associated with a poorer
prognosis of the cancer. 5 year survival rate is between 15-70% However, in some cancer patients the course of pharynx cancer is more
indolent with a long survival rate even if the cancerous disease itself has been controlled but not cured.
Smoking and alcohol worsen the survival rate.

Thank you