Peptic ulcer disease
45
Peptic Ulcer Disease Done by: PROF/GOUDA ELLABBAN SUEZ CANAL UNIVERSITY / EGYPT
-
Upload
scu-hospital -
Category
Health & Medicine
-
view
32 -
download
1
Transcript of Peptic ulcer disease

Peptic Ulcer Disease
Done by:PROF/GOUDA ELLABBAN
SUEZ CANAL UNIVERSITY / EGYPT
ContentDefinitionIncidence & epidemiologyCausesNormal physiologyPathogenesisClinical presentationDifferentialsInvestigationsTreatmentprevention

what is a Peptic Ulcer?
A peptic ulcer is a hole in the gut lining of the Stomach (Gastric ulcer)Duodenum (duodenal ulcer)Esophagus (esophageal ulcer). An ulcer occurs when the lining of these organs is corroded by the acidic digestive juices which are secreted by the stomach cells.


Normal stomach Gastric Ulcer
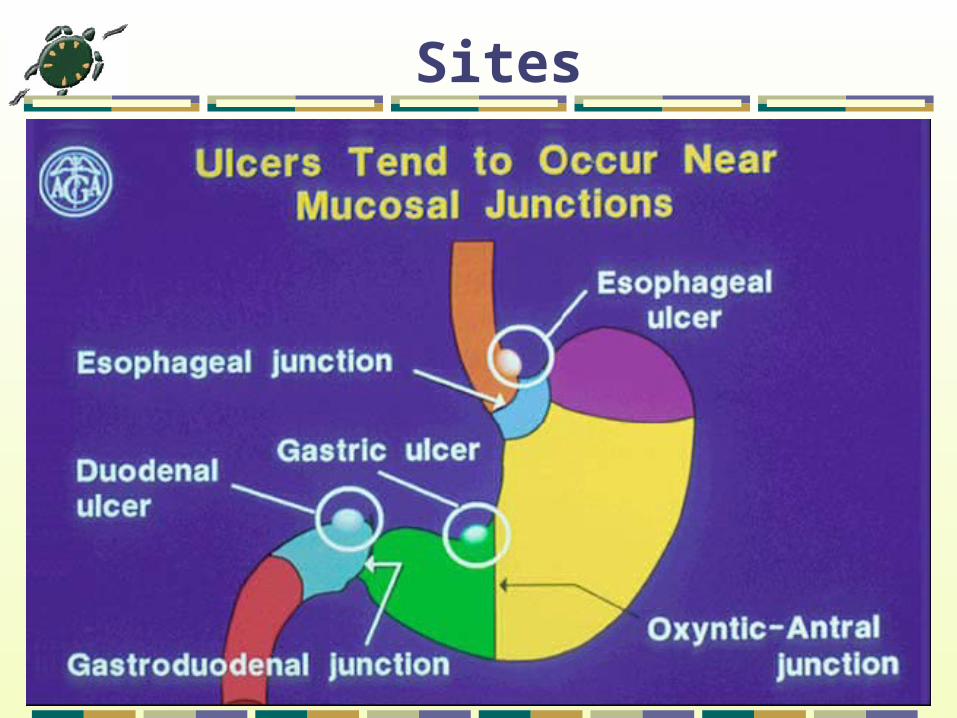
Sites

Incidence & Epidemiology
Frequency: In the US: One-year point prevalence is 1.8%. Lifetime prevalence is approximately 10%. PUD affects approximately 4.5 million people annually.
Internationally: Frequency of PUD is decreasing in the developed world but increasing in developing countries.

H. pylori is found in 50% of people worldwide; 70% of KSA population

Sex: Male-to-female ratio of PUD is approximately 2:1
Age: Duodenal ulcers usually occur in those aged 25-75 years.Gastric ulcer prevalence peaks in those aged 55-65 years.
Mortality/Morbidity: The mortality rate has decreased in the last few decades and is approximately 1 death per 100,000 cases.
The hospitalization rate is approximately 30 patients per 100,000 cases.

What Causes Peptic Ulcers? H pylori (most common cause of ulceration)NSAIDs, aspirinGastrinoma (Zollinger-Ellison syndrome)Heredity (large parietal cell mass, blood group O & blood group antigen)SmokingSevere stress (eg, trauma, burns)AlcoholBile refluxPancreatic enzyme refluxRadiation

H. pylori
gram –ve spirochetal bacteriumfound in the antral and duodenal mucosa.
Mechanism: it is urease +ve split urea and lead to
formation of ammonia alkaline media around the bacteria 2ry high acid ULCER
also it affect the cells through cytotoxin

NSAIDs
Nonsteroidal anti-inflammatory drugs Second most common cause of PUD Addition of steroids potentiates risk Accounts for many H pylori–negative
ulcers


Normal Physiology

Mucosal Defense FactorsTight junctions between epithelial cells which form a physical barrier to diffusing hydrogen ions.
Mucus layer on epithelial cells.
Bicarbonate secreted by epithelial cells.
Adequate blood supply of gastric mucosa, which prevents accumulation of hydrogen ion within mucosal cells.
Competent sphincters(pyloric & lower esophageal) block reflux of bile salts into the stomach & esophagus.



Pathogenesis

Ulcers occur only in the presence of acid & pepsin. Therefore we can say that aggressive factors break the defensive mucosal barrier & then acid, pepsin cause destruction & ulceration.
NSAIDs are non-selective inhibitors of prostaglandins by inhibiting both enzymes cyclooxygenase (COX)1 & 2, so it inflammation & reduce pain along with decreasing the defensive mechanism of gastric mucosa & leave it susceptible to ulcerogenic effect of acid & pepsin

Etiology of PUD
Normal
Increased Attack Hyperacidity
Weak defense Helicobacter pylori* Stress, drugs, smoking

Duodenal Ulcer Gastric UlcerIt usually occurs in the first part of duodenum.It is virtually never malignant.More common 4 times than gastric ulcer.More common in male at age 33-55 years.Risk factors: H pylori, smoking, NSAIDs, COPD,cirrhosis,CRF.
More than 90% of gastric ulcers occur in lesser curvature.It is may be malignant.Less common than duodenal ulcer. More common at age 50-60 years.Most common cause NSAID use, bile reflux &H pylori.

Duodenal Ulcer Gastric Ulcer

Clinical presentaion
Alternating symp. & symp. Free periods
Gnawing,burning epigastric pain
Nocturnal pain➔ early awakening
Duodenal relieved by foods , antacids ,
-if gastric by foods & by vomitting

Clinical presentation ,, cont.
Dyspeptic complaints (belching,bloating,abd.distension)
Weight loss
Epigastric tenderness
Remember .. Heart burn is NOT a sign of PU but of GERD

Clinical presentation in complicated ulcerGI bleeding ➔heme +ve stool , melena ,
hematemesis , anemia
Obstruction ➔ N&V,abd.distension, succussion splash on auscultation
Penetration or perforation ➔ severe abd. Pain , & signs of peritonitis
CA➔ wt loss & anorexia

Non ulcer dyspepsia
CA (gastric , pancreatic , lymphoma)
H.pylori assosciated gastritis
GERD
Chron’s dis
Pancreatitis
Dissecting aneurysm
Billiary colic & acute cholecystitis
Differentials

Investigations A .Routine lab. Tests :
CBC & iron studies➔ can detect anemia (anemia & wt. loss are alarm signs that mandate
endoscopy to know the source of chronic GI bleeding)Serum amylase➔to exclude pancreatitisSerum gastrin➔to exclude zollinger ellisonElectrolytes, BUN, and creatinine ➔in critical-appearing patients who require fluid resuscitation.Type, crossmatch, and screen are indicated if transfusion in unstable or potentially critical patients is needed.

Investigations
B .H.pylori testing:
Urea breath test: very sensitive & specific, if +ve ➔ H.pyloriH.pylori stool antigen test
Blood antibody test for H.pylori (ELIZA)

Investigations ,,, cont.C . Imaging :
Upper GI x-ray with double barium contrast:Helps to confirm or rule out malignancy70-90% accurte in PU Dx.
Chest x-ray ➔ to detect free abdominal air if perforation is suspected


Investigations ,,,imaging .. cont.
Diagnostic endoscopy (Esophagogastrodudenoscopy)Endoscopy ➔the gold standard for accurate diagnosis of peptic ulcer(>95%) & malignancy (>99%), also help in prognosis & sometimes in tttAllows taking biopsies➔culture➔+urease,
+H.pylori


Treatment
Stop orreduce
NSAIDs
Prevent Further flare
ups
Ttt of complications
EliminateOr reducesymptoms
EradicateH.pylori
Goals

Medical Treatment ,,
For eradication of H.pylori :Quadrable therapy(for at least 2 wks) = 2 antibiotics +PPI+bismuth
(clarithromycin , amoxycillin , omeprazole , bismuth subsalicylate )For –ve H.pylori ulcers :PPI , H2 antagonists as cemitidine or ranitidine (zantac)

Medical Treatment ,, cont.
In NSAIDs ulcers :
The same(H2antagonists , cemitidine) + stop NSAIDs
If discontinuing is not possible:
Either give omeprazole concurrently OR specific COX-II anti inflammatory drugs as
celecoxib

Medical Treatment ,,, cont.
Endoscopic therapy :
Indicated in bleeding ulcers with high risk signs(active bleeding, visible vessels, and adherent
clots)
Help determining & evaluating the bleeding & the risk for rebleeding
Several modalities ( injection , coagulation , thermal , hemostatic clips )

Surgical Treatment
Indications for surgery :
1. ulcer perforation,
2. gastric outlet obstruction,
3. giant gastric ulcer, and
4. Failure of medical ttt

Surgical Treatment ,,, cont.
A. Gastric ulcer :
Gastroduodenostomy –billroth I-
Gastrogegunestomy –billroth II-
Both include removal of both the ulcer & the diseased antrum

Surgical treatment ,, cont.
B . Duodenal ulcer :Vagotomy 4 types: Truncal vagotomy➔total abdominal vagal denervation and requires a drainage procedure-pyloroplasty- to prevent gastric stasis. Selective vagotomy➔spares the vagal branches to the liver and small intestine (celiac & hepatic), but produces a total gastric vagotomy. A pyloroplasty is required. Highly selective vagotomy➔diverting innervation of the body only(selective denervation of the parietal cell mass), no pyloroplasty Posterior truncal vagotomy with anterior seromyotomy (Taylor procedure) divides one vagal trunk while preserving the other. This procedure does not require a pyloroplasty.



Prevention
1ry• Stop smoking & Alcohol• Avoid NSAIDs• Low fat diet with Emphasis On 3meals/day• education
2ry• Life style changes will not cure the ulcer but decrease the recurrence &complications incidence

Thank u