Gastritis & Peptic Ulcer Disease
47
Peptic Ulcer Disease
-
Upload
silvestri-purba -
Category
Documents
-
view
76 -
download
21
description
Gastritis
Transcript of Gastritis & Peptic Ulcer Disease

Peptic Ulcer Disease

Definitions
Ulcer:A lesion on an epithelial surface (skin or mucous membrane) caused by superficial loss of tissue
Erosion:A lesion on an epithelial surface (skin or mucous membrane) caused by superficial loss of tissue which is limited to the mucosa.

Definitions
Peptic UlcerAn ulcer of the alimentary tract mucosa,
stomach duodenumrarely in the lower esophagus
Where ?
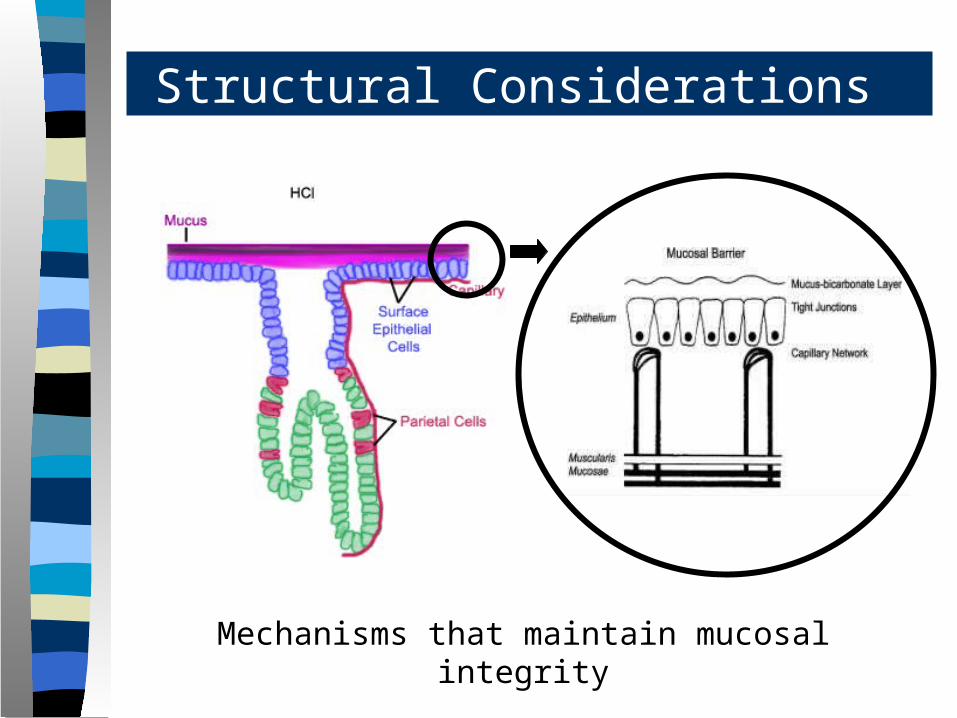
Structural Considerations
Mechanisms that maintain mucosal integrity

5

66
The inside of the stomach is bathed in about two liters of gastric juice every day.
Gastric juice is composed of digestive enzymes and concentrated HCL , which can readily tear apart the toughest food or microorganism.
The gastroduodenal mucosal integrity is determined by protective (defensive) and damaging (aggressive) factors.
Gastric Mucosa & Secretions


99
The defensive forces– Bicarbonate– Mucus layer– Mucosal blood flow– Prostaglandins– Growth factors
Gastric Mucosa & Secretions
The aggressive forces– Helicobacter pylori– HCl acid– Pepsins– NSAIDs– Bile acids– Ischemia and hypoxia. – Smoking and alcohol
VS

The two most common causes of PUD are:
– Helicobacter pylori infection– Non-steroidal anti-inflammatory drugs (NSAIDS)
Other uncommon causes include:
– Gastrinoma (Gastrin secreting tumor)– Stress ulceration (trauma, burns, critical illness)– Viral infections– Vascular insufficiency
Etiology

12
Clinical Features
Gastric Ulcer• Worse by/unrelated to
food• Anorexia• Weight Loss• Food Aversion
Duodenal Ulcer• 90 min – 3 hr after
meal• >> Nocturnal• Relieved by food

Helicobacter pylori

Helicobacter pylori as a cause of PUD
The majority of PUD patients are H. pylori infected.
Studies show that about 95% of patients with DU and 85% with GU are infected with H. pylori
Cure of H. pylori infection reduces ulcer recurrence.
Etiology – Helicobacter pylori

Helicobacter pylori as a cause of PUD
Over a 10 year period 1 out of 133 (0.75%) individuals without H. pylori developed a peptic ulcer, compared with 35 out of 321 (11%) with H. pylori infection.
The incidence of peptic ulcers in H.pylori infected people is about 1% per year.
Etiology – Helicobacter pylori
16

Etiology – NSAIDS

Non-steroidal anti-inflammatory drugs (NSAIDs)
Symptomatic GI ulceration occurs in 2% to 4% of patients treated with NSAIDs for 1 year.
In view of the million of people who take NSAIDs annually, these small percentages translate into a large number of symptomatic ulcers.
The effects of aspirin and NSAIDs on the gastric mucosa ranges from mucosal hemorrhages to erosions and acute ulcers.
Etiology – NSAIDs

Etiology – NSAIDS
Effect of NSAIDS
All NSAIDs reduce the mucosal production of prostaglandins from precursor membrane fatty acids.
The drugs also generate oxygen-free radicals and products of the lipoxygenase pathway that may contribute to ulceration.

Etiology – NSAIDS
Users of NSAIDs are at approximately 3 times greater relative risk of serious adverse gastrointestinal events than nonusers.
Additional risk factors include: – Age greater than 60 years– Smoking – Previous history of GI events – Concomitant corticosteroid use. In terms of serious
complications, the combination of steroids and NSAIDs leads to a 10-fold increase in GI bleeding and a 20-fold increase in GI-related death.

Etiology – NSAIDS
Type of NSAID and Risk of Ulcer
Risk Group Drug Relative Risk
Low Ibuprofen 2.0Diclofenac 4.2
Medium Naproxen 9.1Indomethacin 11.3Piroxicam 13.7
High Ketoprofen 23.7Azapropazone 31.5

Etiology: NSAIDS + H. pylori = ??
Are patients on NSAIDs who are also infected with H. pylori more likely than those who are not infected to have dyspepsia, mucosal damage, or ulcers?

PUD – Clinical Presentation

Symptoms of PUD
Pain– Epigastric pain– Hunger pain– Nocturnal pain
Other symptoms– Waterbrash– Heartburn– Vomiting
Asymptomatic – 1% - 3% adults endoscopy volunteers– 20% of complicated ulcers present without previous
symptoms
PUD – Clinical Presentation

Peptic Ulcer Disease - Diagnosis
Diagnosis of ulcer Diagnosis of H. pylori
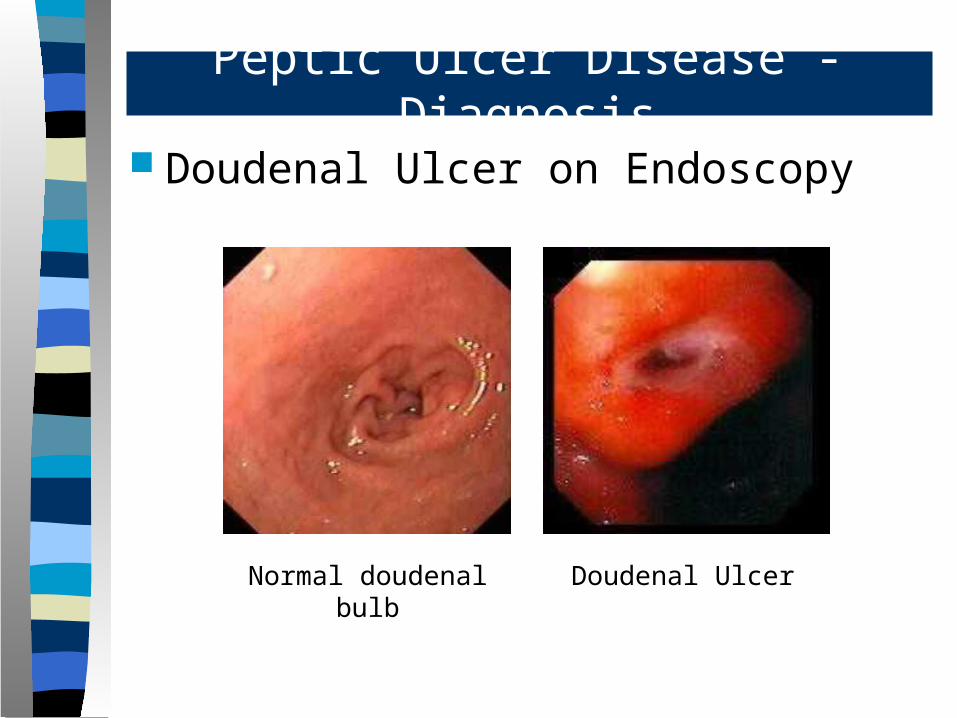
Doudenal Ulcer on Endoscopy
Normal doudenal bulb
Doudenal Ulcer
Peptic Ulcer Disease - Diagnosis

Gastric Ulcer on Endoscopy
Peptic Ulcer Disease - Diagnosis
Chronic Gastric Ulcers

Duodenal Ulcer on Barium meal
Peptic Ulcer Disease - Diagnosis
Duodenal Ulcer

Gastric Ulcer on Barium meal
Peptic Ulcer Disease - Diagnosis
Gastric Ulcer

Tests for Helicobacter pylori
Non-invasive C13 or C14 Urea Breath Test Stool antigen test H. pylori IgG titer (serology)
Invasive Gastric mucosal biopsy Rapid Urease test
Diagnosis of H. pylori

Tests for Helicobacter pylori
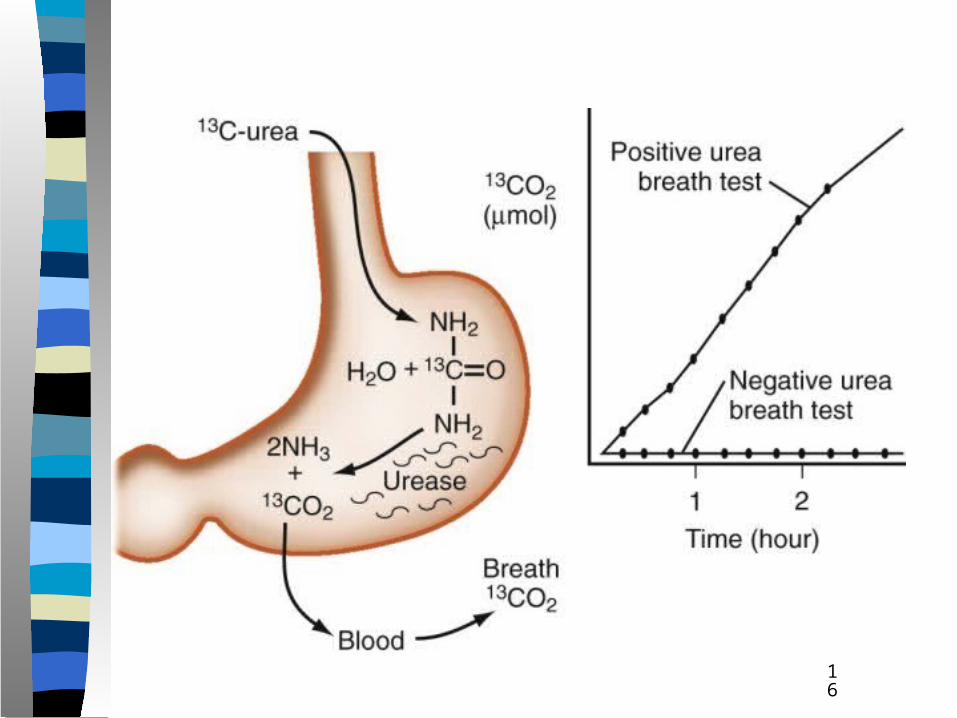
C13 or C14 Urea Breath Test
Diagnosis of H. pylori

Tests for Helicobacter pylori
Stool Antigen test
Diagnosis of H. pylori

Tests for Helicobacter pylori
Mucosal Biopsy
Diagnosis of H. pylori

Tests for Helicobacter pylori
Rapid Urease Test
This test is based on the urease enzyme present in the H. pylori
Urea is split into NH3 and CO2
The change in pH causes a color change in the medium
Diagnosis of H. pylori

PUD – Complications

Complications of PUD
Bleeding
Perforation
Gastric outlet or duodenal obstruction
Chronic anemia
PUD – Complications
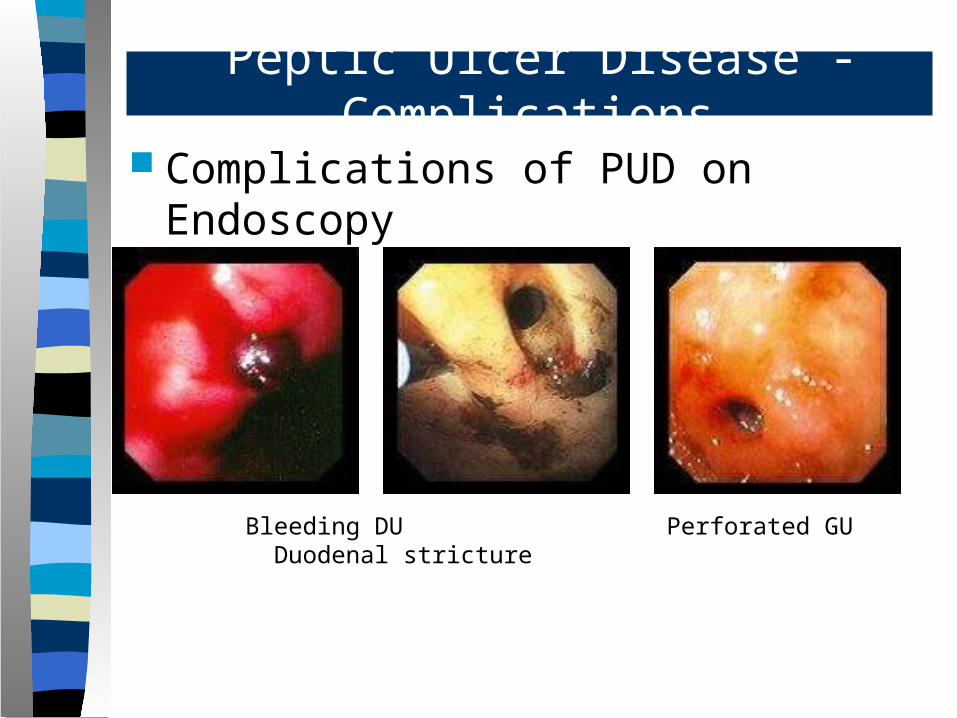
Complications of PUD on Endoscopy
Peptic Ulcer Disease - Complications
Bleeding DU Perforated GU Duodenal stricture

Peptic Ulcer Disease - Treatment
Medical Treatment Endoscopic Treatment Surgical Treatment
Medical Treatment of Peptic Ulcer Disease
Pharmacologic intervention can speed healing of peptic ulcers as well as delay and reduce the rate of recurrent peptic ulceration.
The major aims of peptic ulcer therapy have been expanded accordingly to include: – Rapid symptom resolution – Effective ulcer healing – H. pylori eradication – Prevention of ulcer relapse
Peptic Ulcer Disease - Treatment

Medical Treatment of Peptic Ulcer Disease
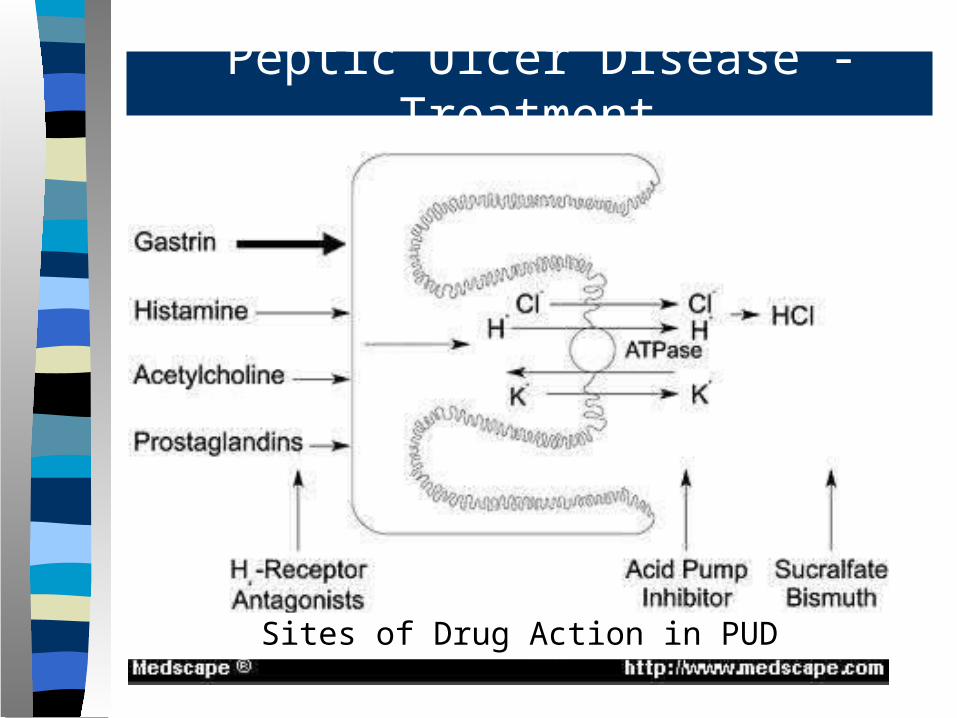
The major agents in the current armamentarium against peptic ulcer disease are – H2-receptor antagonists – H+,K+-ATPase (acid/proton pump) inhibitors – Sucralfate – Antacids – Bismuth compounds
Peptic Ulcer Disease - Treatment
Peptic Ulcer Disease - Treatment
Sites of Drug Action in PUD
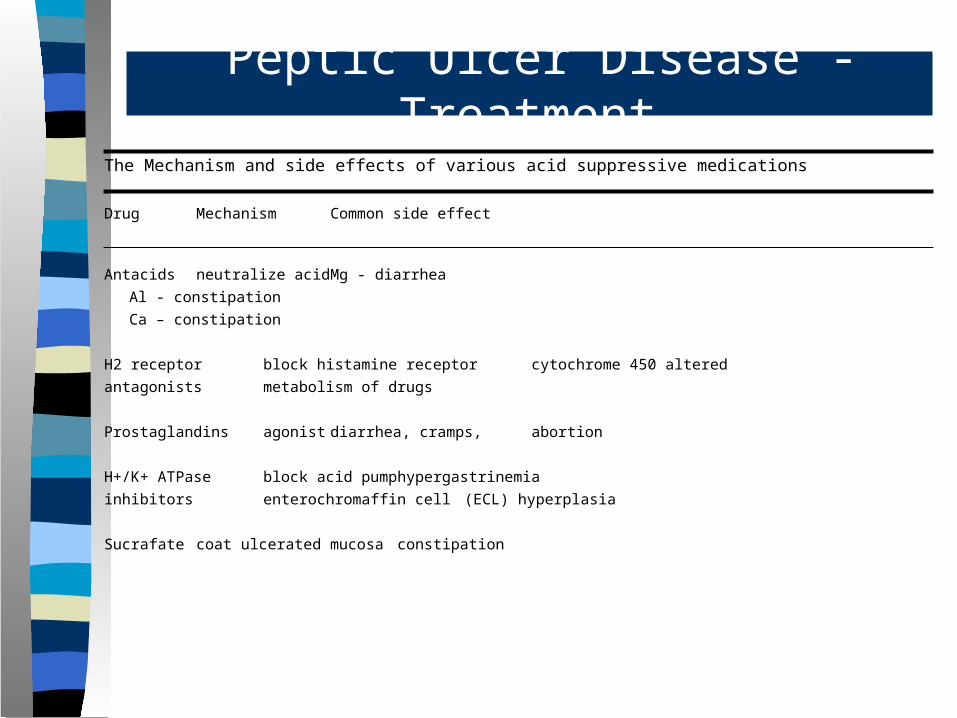
The Mechanism and side effects of various acid suppressive medications
Drug Mechanism Common side effect
Antacids neutralize acid Mg - diarrhea
Al - constipation
Ca – constipation
H2 receptor block histamine receptor cytochrome 450 altered
antagonists metabolism of drugs
Prostaglandins agonist diarrhea, cramps, abortion
H+/K+ ATPase block acid pump hypergastrinemia
inhibitors enterochromaffin cell (ECL) hyperplasia
Sucrafate coat ulcerated mucosa constipation
Peptic Ulcer Disease - Treatment

Misoprostol
Synthetic prostaglandin E1 analog
Inhibits gastric acid secretion
Protects the gastric mucosa – Increases bicarbonate and mucous production– Decreases pepsin levels during basal conditions
Used in prevention of NSAIDS induced gastric ulcers
Does not prevent development of duodenal ulcers
May also stimulate uterine contractions that may endanger pregnancy
Peptic Ulcer Disease - Treatment
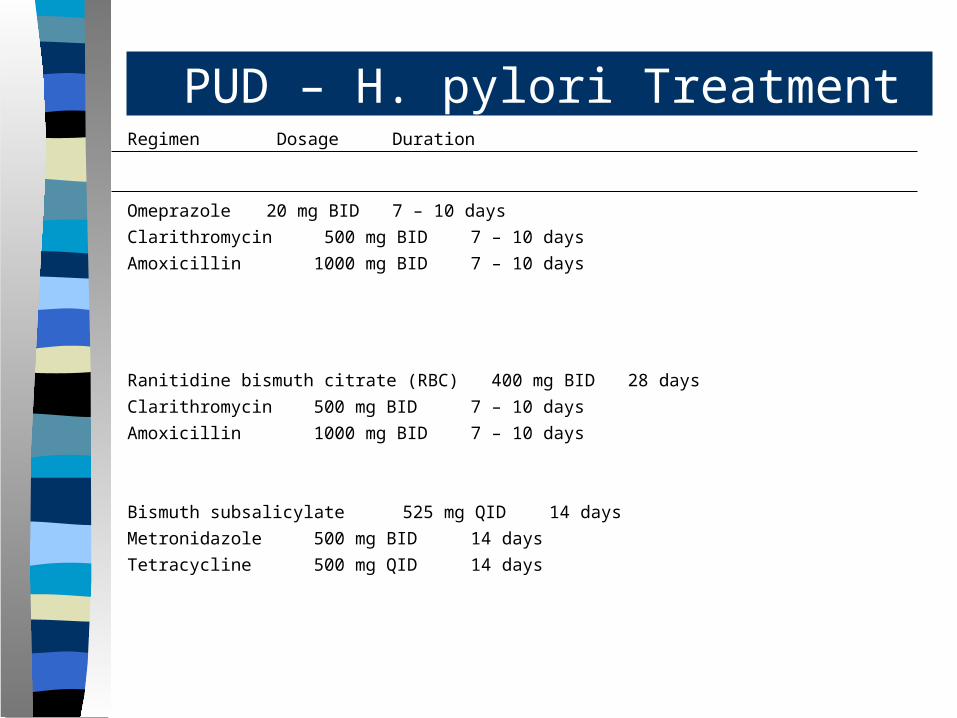
Regimen Dosage Duration
Omeprazole 20 mg BID 7 – 10 days
Clarithromycin 500 mg BID 7 – 10 days
Amoxicillin 1000 mg BID 7 – 10 days
Ranitidine bismuth citrate (RBC) 400 mg BID 28 days
Clarithromycin 500 mg BID 7 – 10 days
Amoxicillin 1000 mg BID 7 – 10 days
Bismuth subsalicylate 525 mg QID 14 days
Metronidazole 500 mg BID 14 days
Tetracycline 500 mg QID 14 days
PUD – H. pylori Treatment

Gastritis
Gastritis Inflammation of the gastric mucosa caused by any
of several conditions, including infection (Helicobacter pylori), drugs (NSAIDs, alcohol), and autoimmune phenomena (atrophic gastritis).
Many cases are asymptomatic, but dyspepsia and GI bleeding sometimes occur.
Diagnosis is by endoscopy.
Treatment is directed at the underlying cause but often includes acid suppression and, for H. pylori infection, antibiotics.

Gastritis