Penetrating eye injuries: a histopathological review · injury and consisted of spindle cells which...
9
British Journal of Ophthalmology, 1980, 64, 809-817 Penetrating eye injuries: a histopathological review STUART R. WINTHROP, PHILIP E. CLEARY, DONALD S. MINCKLER, AND STEPHEN J. RYAN From the Department of Ophthalmology, University of Southern California, Estelle Doheny Eye Foundation, Los Angeles, California, USA SUMMARY This study reports the histological findings in human eyes after severe penetrating trauma. The findings confirm the high incidence of retinal detachment in eyes with severe penetrating injuries. The retina was detached in 32 out of the 34 eyes examined, with 27 having evidence of traction on the retina. These eyes were characterised histologically by intraocular cellular prolifera- tion producing cyclitic, epiretinal, and retroretinal membranes. Intraocular cellular proliferation was discernible or established within 1 week of injury and typically resulted in a cyclitic membrane at about 6 weeks. Epiretinal and retroretinal membranes were found between 1 and 2 weeks after injury in eyes with a detached retina. The results indicate that a damaged lens, the admixture of lens material and vitreous, and the presence of vitreous haemorrhage were all factors promoting intravitreal fibroblastic proliferation. Vitreous surgery may be a rational method of treatment for these severely injured eyes by removing the stimulus and vitreous scaffold for intravitreal fibro- blastic proliferation. From this series it would appear that vitrectomy should not be delayed beyond the second week of injury, by which time massive cellular ingrowth may already be under way. Ocular trauma is an important cause of blindness,' and in some centres it accounts for half or more of all eyes enucleated.2 Among eye disorders ocular trauma is responsible for a disproportionate eco- nomic problem, as it occurs most commonly in young, otherwise healthy, productive individuals.3 Penetrating injuries of or involving the posterior segment of the eye have a particularly poor visual prognosis because of the high incidence of retinal detachment,4 whereas in penetrating injuries con- fined to the anterior segment of the eye a relatively better visual outcome can be expected.8 Improved results for anterior segment injuries can be attri- buted to the introduction of microsurgical tech- niques, antibiotics, and steroids.9 Recent experience with new surgical techniques such as vitrectomy suggests that it is now also possible to salvage some eyes with severe posterior segment injuries.'0-'3 This study reports the histological findings irn human eyes enucleated after severe penetrating trauma and correlates the occurrence and chrono- logy of various tissue reactions with time after injury. It was of special interest to characterise early changes occurring after injury and to deter- Correspondence to Philip E. Cleary, FRCS, USC School of Medicine, Estelle Doheny Eye Foundation, 1355 San Pablo Street, Los Angeles, California 90033, USA. mine how they might trigger the mechanisms res- ponsible for eventual retinal detachment. Knowledge of the chronology of histopathological events after severe penetrating trauma may help determine a rationale for surgical management of these cases and specifically identify the optimal timing for surgical intervention by pars plana vitrectomy. Material and methods We reviewed case reports from 1970 to 1977 in the pathology files of the Estelle Doheny Eye Founda- tion and retrieved slides on 72 cases with a diagnosis of ruptured globe or penetrating eye injury. Among these were 34 eyes enucleated between 1 day and 3 years after the original injury which could be analysed histologically with reference to: (1) the status of the wound; (2) the presence of damage to the uvea, the lens, the vitreous, or the retina; (3) intraocular cellular proliferation; (4) intraocular inflammation. Multiple sections were examined from each case stained with haemotoxylin-eosin, periodic acid Schiff (PAS), Masson-trichrome, alcian blue with and without digestion by hyaluronidase, and the Prussian blue reaction for iron. The remaining 38 eyes were either enucleated 809 on July 1, 2020 by guest. Protected by copyright. http://bjo.bmj.com/ Br J Ophthalmol: first published as 10.1136/bjo.64.11.809 on 1 November 1980. Downloaded from
Transcript of Penetrating eye injuries: a histopathological review · injury and consisted of spindle cells which...

British Journal of Ophthalmology, 1980, 64, 809-817
Penetrating eye injuries: a histopathological reviewSTUART R. WINTHROP, PHILIP E. CLEARY,DONALD S. MINCKLER, AND STEPHEN J. RYANFrom the Department of Ophthalmology, University of Southern California,Estelle Doheny Eye Foundation, Los Angeles, California, USA
SUMMARY This study reports the histological findings in human eyes after severe penetratingtrauma. The findings confirm the high incidence of retinal detachment in eyes with severe penetratinginjuries. The retina was detached in 32 out of the 34 eyes examined, with 27 having evidence oftraction on the retina. These eyes were characterised histologically by intraocular cellular prolifera-tion producing cyclitic, epiretinal, and retroretinal membranes. Intraocular cellular proliferationwas discernible or established within 1 week of injury and typically resulted in a cyclitic membraneat about 6 weeks. Epiretinal and retroretinal membranes were found between 1 and 2 weeks afterinjury in eyes with a detached retina. The results indicate that a damaged lens, the admixture oflens material and vitreous, and the presence of vitreous haemorrhage were all factors promotingintravitreal fibroblastic proliferation. Vitreous surgery may be a rational method of treatment forthese severely injured eyes by removing the stimulus and vitreous scaffold for intravitreal fibro-blastic proliferation. From this series it would appear that vitrectomy should not be delayed beyondthe second week of injury, by which time massive cellular ingrowth may already be under way.
Ocular trauma is an important cause of blindness,'and in some centres it accounts for half or more ofall eyes enucleated.2 Among eye disorders oculartrauma is responsible for a disproportionate eco-nomic problem, as it occurs most commonly inyoung, otherwise healthy, productive individuals.3Penetrating injuries of or involving the posteriorsegment of the eye have a particularly poor visualprognosis because of the high incidence of retinaldetachment,4 whereas in penetrating injuries con-fined to the anterior segment of the eye a relativelybetter visual outcome can be expected.8 Improvedresults for anterior segment injuries can be attri-buted to the introduction of microsurgical tech-niques, antibiotics, and steroids.9 Recent experiencewith new surgical techniques such as vitrectomysuggests that it is now also possible to salvage someeyes with severe posterior segment injuries.'0-'3
This study reports the histological findings irnhuman eyes enucleated after severe penetratingtrauma and correlates the occurrence and chrono-logy of various tissue reactions with time afterinjury. It was of special interest to characteriseearly changes occurring after injury and to deter-
Correspondence to Philip E. Cleary, FRCS, USC School ofMedicine, Estelle Doheny Eye Foundation, 1355 San PabloStreet, Los Angeles, California 90033, USA.
mine how they might trigger the mechanisms res-ponsible for eventual retinal detachment. Knowledgeof the chronology of histopathological events aftersevere penetrating trauma may help determine arationale for surgical management of these casesand specifically identify the optimal timing forsurgical intervention by pars plana vitrectomy.
Material and methods
We reviewed case reports from 1970 to 1977 in thepathology files of the Estelle Doheny Eye Founda-tion and retrieved slides on 72 cases with a diagnosisof ruptured globe or penetrating eye injury. Amongthese were 34 eyes enucleated between 1 day and3 years after the original injury which could beanalysed histologically with reference to: (1) thestatus of the wound; (2) the presence of damage tothe uvea, the lens, the vitreous, or the retina; (3)intraocular cellular proliferation; (4) intraocularinflammation.
Multiple sections were examined from each casestained with haemotoxylin-eosin, periodic acidSchiff (PAS), Masson-trichrome, alcian blue withand without digestion by hyaluronidase, and thePrussian blue reaction for iron.The remaining 38 eyes were either enucleated
809
on July 1, 2020 by guest. Protected by copyright.
http://bjo.bmj.com
/B
r J Ophthalm
ol: first published as 10.1136/bjo.64.11.809 on 1 Novem
ber 1980. Dow
nloaded from

Stuart R. Winthrop, Philip E. Cleary, Donald S. Minckler, and Stephen J. Rya,r
soon after injury or were too disorganised to permitaccurate evaluation of individual histological fea-tures. They were excluded from the study.
Results (Table l)
THE WOUNDThe site of penetration was limited to the cornea in16 eyes, included the peripheral cornea and adjacentsclera in 13 eyes, and involved the sclera alone in 5.The full extent of the penetrating wound wasdetermined by compiling information from clinicaland operative reports, gross histological descrip-tions, and light microscopy.
Corneal wounds were closed externally by slidingand hyperplasia of epithelial cells within 1 week ofinjury. A fibrous stromal scar was present by 3 to 4weeks in those wounds with good closure where nouveal or vitreous incarceration had occurred.Delayed healing of corneal wounds was commonand could be related to defective wound closure,especially with incarceration of intraocular tissuesin the wound. We judged wound apposition asparticularly poor in 12 eyes, 9 of which had to beenucleated within 2 weeks of injury. Poor woundclosure varied from a wide gap to moderate malap-position of the wound edges. Many corneal woundsshowed posterior wound gape, probably related tosuperficial placement of sutures.
Healing of limbal and scleral wounds was morerapid than in corneal wounds. As early as 4 daysafter injury fibroblastic proliferation had occurredfrom the episclera, and by 1 week it occurred fromthe stroma of the ciliary body and choroid. At 2weeks a mass of vascularised fibrous tissue joinedthe wound edges, and by 4 to 6 weeks a dense
Table 1 Time at which eyes were examined after injury
Time after injury Eyes examined
I day 27 days 512 ,, 314 ,, 53 weeks 14 ,, 16 ,, 3
2 months 54,, 25 ,, 1
6,, 318 ,, 1
2 years 13 ,, 1
fibrous scar had formed. Pigment, both free andwithin macrophages, was scattered throughout thescar tissues.Of the 34 eyes 28 showed prolapsed or incar-
cerated tissues in the wound, including lens material,lens capsule and retina, and most commonly uveaor vitreous. Incarceration of tissues in a cornealwound was consistently associated with a delay inwound healing in eyes enucleated within the first 2weeks of injury, and with the development of fibrousingrowth from the wound in eyes enucleated from3 weeks onward. Incarceration of tissues in limbalor scleral wounds was associated with the formationof granulation tissue in the wound, often extendingintraocularly into the adjacent incarcerated tissue.A single eye with poor closure of a corneal wound
showed an epithelial ingrowth. Fibrous ingrowthfrom the wound occurred in 19 of the 34 eyes. It didnot occur from corneal wounds without incarcera-tion of tissues in the wound, or at least appositionof tissues to the wound, such as a damaged lens oriris. In limbal or scleral wounds fibrous ingrowthoccurred despite good wound closure. These eyes,however, often had obvious vitreous incarcerationin the wound, and they usually showed damage tothe lens and/or vitreous haemorrhage.
THE VITREOUSEarly changes in the structure of the vitreous gelafter injury included separation of the vitreous fromthe posterior retina and condensation of vitreousfibrils over the vitreous base. The vitreous hadseparated from the posterior retina in six of the 13eyes examined between 1 and 2 weeks after injury.Of a total of 22 eyes with a posterior vitreousdetachment 18 had blood loculated in the vitreousgel. In the early weeks after injury, the surface ofthe posterior hyaloid consisted of a discrete layerof condensed vitreous lined by red blood cells andmacrophages, and in 1 eye at 2 months after injuryit also contained fibroblast-like cells.The vitreous did not become detached anteriorly.
Typically, condensed vitreous fibrils remainedattached to the peripheral retina and nonpigmentedciliary epithelium over the vitreous base. Vitreousfibrils often radiated from a limbal or scleral woundin which they were incarcerated, and fibroblastswere typically aligned along these fibrils. In someeyes the vitreous fibrils appeared taut and seemedto account for traction detachment of the peripheralretina 1800 from a penetrating limbal or pars planawound (Fig. 1).Condensed vitreous fibrils were also prominent
in eyes with double perforating injuries due to aforeign body. These fibrils were incarcerated in theentry and exit wound, bridging the vitreous cavity.
810
on July 1, 2020 by guest. Protected by copyright.
http://bjo.bmj.com
/B
r J Ophthalm
ol: first published as 10.1136/bjo.64.11.809 on 1 Novem
ber 1980. Dow
nloaded from

Penetrating eye injuries
INTRAOCULAR INFLAMMATIONIntraocular inflammatory infiltrate was quite vari-able, but was often prominent in the anteriorchamber or vitreous, especially in the presence ofblood. Inflammatory cells, usually mainly mono-cytes, often surrounded the site of rupture of thelens capsule or were present in the penetratingwound or in the incarcerated tissues. The inflamma-tory response was most marked in eyes with lens,vitreous, and blood admixture. Macrophages werepresent in these eyes, surrounding lens fragmentsor at the margins of blood clot within the vitreous.Almost all eyes contained some macrophageseither lining the posterior vitreous separation oraccumulated in areas of subretinal haemorrhage.
INTRAOCULAR CELLULAR PROLIFERATION
Fibroblastic proliferation within the vitreous was
'At'~~~~WVb~ ~ ~ V
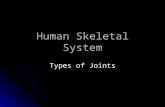
Fig. 1 Photomicrograph showing the appearance ofthe peripheral retina in the vitreous base at 2 monthsafter a penetrating injury. The peripheral retina (R) isdetached and appears to be pulledforward over thepars plana (PP). The vitreous is condensed and vitreousfibrils are incarcerated in a peripheral corneal wound (W).The vitreous was detachedfrom the posterior retina, butremains attached to the peripheral retina over the vitreousbase (VB). (Haematoxylin and eosin, x ?7).
present as early as 1 week after injury and mostoften emanated from the stroma of the ciliary bodyor choroid at a limbal or scieral wound. The invad-ing fibroblasts appeared to extend along the scaffoldprovided by vitreous fibrils or into the blood clotand the vitreous gel behind the lens (Fig. 2). Fibro-blastic proliferation also extended posteriorly overthe pars plana and on to the surface of the peri-pheral retina. Fibrous proliferation within thevitreous resulted in a cyclitic membrane in whichlens material, lens capsule, and detached retina wereoften incorporated. We found cyclitic membranes in17 eyes as early as 2 weeks after injury in 2 eyes thathad a limbal wound and vitreous haemorrhage andprolapse of the lens. The cyclitic membrane was wellestablished in most eyes by 6 to 8 weeks after injury.
Cellular proliferation within the vitreous alsoappeared to originate from the nonpigmentedciliary epithelium. Characteristically these cellsbecame elongated and at 1 week after injury ap-peared to be proliferating into the vitreous cavityalong the vitreous fibrils attached over the vitreousbase (Fig. 2).
Intravitreal fibroblastic proliferation also appearedto occur from the exit wound in eyes with doubleperforating injuries.
THE RETINARetinal detachment was present in 32 out of 34eyes. The 2 eyes without a retinal detachment hadbeen enucleated as blind and painful because ofuncontrolled glaucoma. We found retinal tears inonly 2 eyes, but it was impossible to exclude arhegmatogenous component in the others as we didnot serially section all eyes. Retinal haemorrhageswere present in all 20 eyes enucleated within thefirst 2 months of injury. Choroidal haemorrhageswere also common within the first 2 to 3 weeksafter injury, and ciliary body effusions were frequentin eyes with cyclitic membranes.
Epiretinal membranes were present in 14 eyes.They seemed to originate from the fibrous ingrowthfrom the wound, or from the surface of the opticnerve head, or from the surface of the retina.Epiretinal membranes were present over the peri-pheral retina in 2 eyes examined at 2 weeks afterinjury and consisted of spindle cells which seemedto have their origin in the fibrous ingrowth from anadjacent penetrating wound through the limbus orpars plana (Fig. 3). Similarly, by 12 days afterinjury spindle cells had formed an epiretinal mem-brane over the posterior retina adjacent to an exitwound in an eye with a double perforating injury(Fig. 4). By 4 to 6 weeks after injury multilayeredepiretinal membranes could be found over bothperipheral (Fig. 5) and posterior retina (Fig. 6).
811
on July 1, 2020 by guest. Protected by copyright.
http://bjo.bmj.com
/B
r J Ophthalm
ol: first published as 10.1136/bjo.64.11.809 on 1 Novem
ber 1980. Dow
nloaded from

Stuart R. Winthrop, Philip E. Cleary, Donald S. Minckler, and Stephen J. Ryan
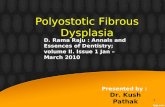
Fig. 2 Photomicrographdemonstrating the peripheralretina and pars plana (PP)1800 from a penetrating woundthrough the parsplana in an-eye enucleated 1 week afterinjury. There is an apparentproliferation of the nonpigmentedciliary epithelium (largearrow). Cellular proliferationhas also occurred along theanterior hyaloid (small arrows).Possibly these cells are derivedfrom the nonpigmented ciliaryepithelium. (Haematoxylin andeosin, x 64).
These membranes also contained pigmented cellsand macrophages and some had connections to thesurface of the retina. In 10 of 16 eyes the epiretinalmembranes were also connected to the surface ofthe optic nerve head. Thick multilayered epiretinalmembranes were often associated with full-thicknessretinal folds.We found retroretinal membranes in 15 eyes.
They were present in 6 of 13 eyes examined between1 and 2 weeks after injury. In the early cases themembranes were delicate, branching, and dendriticin appearance. In late cases they were thickened
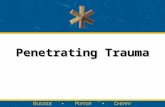
Fig. 3 Photomicrographshowing the appearance of theperipheral retina posterior to a
penetrating wound through thepars plana in an eye enucleated2 weeks after injury. Theperipheral retina appears to bepulledforward over the parsplana. Spindle cells are presenton the surface of the peripheralretina (arrows) and have probablyoriginated from the wound or
from proliferation of the ciliaryepithelium posterior to thewound. (Haematoxylin andeosin, x 86).
and attached to folds in the retina. The pathogenesisof the retroretinal membranes was not clear, butthey were often found in areas of subretinal haemorr-hage (Fig. 7). In 1 eye at 1 week after injury a smallretroretinal membrane composed of nonpigmentedcells was connected to and extended along the outerretina (Fig. 8). In eyes examined at 2 weeks afterinjury prominent retroretinal membranes werepresent and appeared continuous with areas ofproliferation of the retinal pigment epithelium. At2 weeks also, in eyes with choroidal and subretinalhaemorrhage, cellular invasion of the subretinal
,AtJW ~~~~~~~~~~~r4~~~~~~~~~~v ~ N
w. O
4~~~" 9.~~A"
.~~~ ~~*At~~~~~A
812
on July 1, 2020 by guest. Protected by copyright.
http://bjo.bmj.com
/B
r J Ophthalm
ol: first published as 10.1136/bjo.64.11.809 on 1 Novem
ber 1980. Dow
nloaded from

Penetrating eye injuries
Fig. 4 Photomicrographshowing the appearance of aposterior penetrating wound at12 days after injury in an eyewith a double perforating injurydue to an intraocular foreignbody. Spindle cells (arrows) areemanating from the wound (W)on to the surface of the peripheralretina (R), and appear to beinfiltrating the vitreous andblood clot. These spindle cellsmay originate from the choroid,or possibly have their origin inmetaplastic retinal pigmentepithelial cells or in theepisclera. (Haematoxylin andeosin, x 43).
blood clot occurred, apparently from the choroidthrough breaks in Bruch's membrane (Fig. 9).
Discussion
We analysed the histological findings in 34 eyesenucleated after penetrating trauma. These eyeswere characterised histologically by intraocularcellular proliferation leading to the formation ofcyclitic, epiretinal, and retroretinal membranes andby the presence of traction retinal detachment.These findings support clinical studies in whichtraction retinal detachment has been identified as amain cause of loss of vision after a posterior pene-trating injury.47
Immediately after injury an expulsive type ofhaemorrhage may occur with bleeding into thechoroid, under the retina, and into the vitreous. Ifthe expulsive haemorrhage results in prolapse ofthe intraocular contents, there is little potential forvisual recovery.7 In the injured eye an inflammatoryresponse occurs, the extent of which is influencedby various factors, such as vitreous haemorrhage,vitreous-lens admixture, or the presence of a reac-tive intraocular foreign body or of infection. As theinflammation subsides, cellular invasion and pro-liferation within the vitreous occur. Physical altera-tions in the structure of the vitreous may providea more effective scaffold for intravitreal cellularproliferation.'4 The proliferating cells give rise to
Fig. 5 Photomicrograph ofperipheral retina from an eyewith a total retinal detachmentenucleated 6 weeks after apenetrating injury shows anepiretinal membrane 3 layersthick present on the surface ofthe retina. The epiretinalmembrane is artefactuallydetached, revealing an apparentlyintact inner limiting membrane.(Haematoxylin and eosin, x 68).
813
,f,;A--.7
on July 1, 2020 by guest. Protected by copyright.
http://bjo.bmj.com
/B
r J Ophthalm
ol: first published as 10.1136/bjo.64.11.809 on 1 Novem
ber 1980. Dow
nloaded from

Stuart R. Winthrop, Philip E. Cleary, Donald S. Minckler, and Stephen J. Ryan
Fig. 6 Photomicrographshowing a multilayered epiretinalmembrane (ERM) on thesurface of the posterior retinain an eye enucleated 2 monthsafter a penetrating injury. Aposterior vitreous detachment(PVD) is present and blood clotis loculated within the vitreousgel. The posterior hyaloid (PVD)is lined with red cell debris. Theepiretinal membrane lies betweenthe posterior hyaloid and theinner limiting membrane of theretina. In adjacent sectionsfull-thickness retina folds werepresent. (Haematoxylin andeosin, x 37).
cyclitic or trans v-itreal membranes and to epiretinaland retroretinal membranes. Ultimately cells withinthese membranes contract, producing traction on theretina and resulting in traction retinal detachment.'4
In this study intraocular cellular proliferation was
discernible or established within 1 week of injuryand typically resulted in a cyclitic membrane atabout 6 weeks. A cyclitic membrane was present as
early as 2 weeks after injury in eyes with limbal or
scleral wounds associated with incarceration of lensmaterial, vitreous, and blood. The factors asso-
ciated with a vigorous fibrous ingrowth and intra-vitreal fibroblastic proliferation were the site ofthe penetrating wound; the adequacy of woundclosure; the incarceration of tissues in the wound;
Fig. 7 Photomicrograph 4showing the appearance of theposterior retina (R) and opticnerve head (ON) in an eye
enucleated 12 days after a
penetrating injury. A subretinal . ;haemorrhage is present, andspindle cells have formed a
retroretinal membrane (arrows)
in the blood clot. Possibleorigins of this membrane would
include adjacent pigmentepithelial cells, or glial cells ;from the retina, or from the gliallining of the optic nerve. < N(Haematoxylin and eosin, x 43).
the extent of involvement of intraocular tissuesincluding the iris, lens, and vitreous; and thepresence of massive vitreous haemorrhage.
Cellular proliferation within the vitreous appearedto be derived from multiple sources, usually fromthe episclera and from the uvea in the area of aperforating scleral or limbal wound. Proliferationof the nonpigmented ciliary epithelium was also acommon finding. These cells became elongated andextended along the vitreous fibrils into the vitreouscavity, apparently contributing to the formation ofcyclitic membranes. Hyperplasia of the nonpig-mented ciliary epithelium has been observed byothers in a variety of conditions, including traumaand inflammation.215 It is also possible that the
814
.
on July 1, 2020 by guest. Protected by copyright.
http://bjo.bmj.com
/B
r J Ophthalm
ol: first published as 10.1136/bjo.64.11.809 on 1 Novem
ber 1980. Dow
nloaded from

Penetrating eye injuries
Fig. 9 Photomicrograph showing the subretinal spacein an eye enucleated at 2 weeks after penetrating injury.A subretinal blood clot (BC) is present, and fibroblastsare invading the blood clot and su5retinal space througha break in Bruch's membrane (arrow). The retina (R) isdetached and partially necrotic. Bleeding has also occurredin the choroid (C). (Haematoxylin and eosin, x 42).
Fig. 8 Appearance of aretroretinal membrane under theequatorial retina 1 week after apenetrating injury. (Haematoxylinand eosin, x 77).
intravitreal fibroblastic response may have beenderived in part from macrophages or monocytesoriginating in the systemic circulation, though mostof the experimental evidence now supports the viewthat fibroblasts involved in wound healing arederived locally. 1617
Intraocular cellular proliferation also includedthe formation of epiretinal and retroretinal mem-branes which were prominent between 1 and 2weeks after injury. The epiretinal membranes overthe peripheral retina and over the posterior retinaadjacent to exit wounds in eyes with double perfora-tions appeared to be derived from fibroblasticingrowth from the area of the penetrating wound.A similar appearance has been observed in experi-mental animal models of a posterior penetratingeye injury.18 20 On the other hand some epiretinalmembranes were connected to the surface of theretina by bridges of tissue suggesting a glial com-ponent, a feature which has also been described inexperimental animal models.'420 The retroretinalmembrane probably originated from glial cells inthe retina or from proliferation of retinal pigmentepithelial cells. Additionally, in some eyes withchoroidal and subretinal haemorrhage, fibroblastsproliferated from the choroid through breaks inBruch's membrane into the subretinal space.The concept that damaged vitreous forms a
scaffold or matrix for cellular proliferation wassupported by this study. We observed a condensa-tion of the anterior vitreous fibrils in virtually allcases. When vitreous was incarcerated in a pene-trating wound, vitreous strands formed between thewound and the peripheral retina over the vitreousbase, and in those eyes with a double perforatinginjury the vitreous fibrils were aligned between
815
on July 1, 2020 by guest. Protected by copyright.
http://bjo.bmj.com
/B
r J Ophthalm
ol: first published as 10.1136/bjo.64.11.809 on 1 Novem
ber 1980. Dow
nloaded from

Stuart R. Winthrop, Philip E. Cleary, Donald S. Minckler, and Stephen J. Ryan
entry and exit wounds. Ingrowing fibroblasts alongthese vitreous condensations suggest that thevitreous acts as a scaffold for the directed prolifera-tion of cells. In a similar fashion fibroblasts fromthe penetrating wound proliferated along the surfaceof the retina. These findings are in accord withinformation derived from growth of fibroblasts intissue culture, where it has been observed that cellsuse linear structures and scaffolds for directedproliferation."We found evidence of traction on the retina in
27 eyes, either by epiretinal or retroretinal mem-branes or signs suggesting vitreoretinal traction.Retinal tears were observed histologically in only2 eyes, but it was impossible to exclude a rhegmato-genous component in the others, and certainly asevere penetrating injury may result in retinaldialysis or a retinal tear as part of the contusiveeffect. Nevertheless the characteristic configurationof the detached peripheral retina pulled anteriorlyover the pars plana and the presence of retinal foldsrelated to epiretinal and retroretinal membranessuggested that traction mechanisms were importantin the evolution of eventual total retinal detachment.We observed a similar appearance in an experi-mental animal model of a posterior penetrating eyeinjury and proposed that the mechanisms for trac-tion retinal detachment after a penetrating injuryare due to the effects of vitreous traction on theperipheral retina over the vitreous base and con-traction of epiretinal and retroretinal membraneson the peripheral and equatorial retina.'42021 Wehave also noted in this study and in experimentalmodels that with a double perforating injuryanteroposterior vitreous traction may be obser-ved.'822 But, typically, in single perforating woundsthrough the limbus or pars plana the vitreousdetaches from the posterior retina without anysubsequent anteroposterior traction.
In this study fibrous ingrowth occurred fromcorneal wounds only with poor wound closure andwith incarceration of tissues in the wound. Con-versely, with limbal or scleral wounds a fibrousingrowth was common despite good wound closure,but usually associated with damage to the lensand/or vitreous haemorrhage. Development offibrous ingrowth from scleral wounds despite goodwound closure is in accordance with findings fromexperimental animal models of posterior pene-trating eye injuries which emphasised the prognosticsignificance of blood in the vitreous and damage tointraocular structures in severe penetratingtrauma.18 20The clinical implications of this study are numer-
ous. It is clear that the primary surgical repair ofpenetrating wounds must include thorough explora-
tion and debridement with microscopic reapproxi-mation of wound edges. Prolapsed or incarceratedtissue must be excised or reposited. Vitreous incar-ceration in a corneal wound can be avoided, but it isprobably impossible to avoid incarceration ofvitreous in scleral wounds.The results of this study indicate that, with a
posterior penetrating eye injury and in the presenceof retinal detachment, significant cellular prolifera-tion is present within the vitreous and along thesurfaces of the retina as early as 2 weeks afterinjury. The results also indicate that a damagedlens, the admixture of lens material and vitreous,and the presence of a vitreous haemorrhage are allfactors promoting intravitreal fibroblastic prolifera-tion. It has not been possible in this study or inothers to determine the significance of each one ofthese factors in stimulating the intravitreal fibro-blastic response.9 Vitreous surgery may be a rationalmethod of treatment for these eyes by removing thestimulus and vitreous scaffold for intravitrealfibroblastic proliferation. From this series of post-trauma human eyes it would appear that vitrectomyshould not be delayed beyond the second week ofinjury, by which time massive cellular ingrowth mayalready be under way.
This study was supported in part by the National Institutesof Health grant award EY 02061 (Dr Ryan).
References
I Blindness, Facts on the Major Killing and Crippling-Diseases in the United States Today. New York: NationalHealth Education Committee, Inc., 1971: 4-5.
2 Coles WH, Haik GM. Vitrectomy in intraocular trauma:its rationale and its indications and limitations. Arch/Ophthalmol 1972; 87: 621-8.
3 Cox MS, Freeman HM. Retinal detachment due topenetration. I. Clinical characteristics and surgicalresults. Arch Ophthalmol 1978; 95: 1354-61.
4 Roper-Hall MJ. The treatment of ocular injuries. TransOphthalmol Soc UK 1959; 79: 57-69.
5 Johnson S. Perforating injuries: a five-year study.Trans Ophthalmol Soc UK 1971; 91: 895-921.
6 Percival SPB. Late complications from posterior segmentintraocular foreign bodies with particular reference toretinal detachment. Br J Ophthalmol 1972; 56: 462-8.
7 Eagling EM. Perforating injuries involving the posteriorsegment. Trans Ophthalmol Soc UK 1975; 95: 335-9.
8 Eagling EM. Perforating injuries of the eye. Br J Ophthal-mol 1976; 60: 732-6.
9 Faulborn J, Topping TM. Proliferation in the vitreouscavity after perforating injuries: a histopathologic study.Albrecht von Graefes Klin Exp Ophthalmol 1978; 205:157-66.
10 Benson WE, Machemer R. Severe perforating injuriestreated with pars plana vitrectomy. Am J Ophthalmol1976; 81: 728-32.
11 Hutton WL, Synder WB, Vaiser A. Vitrectomy in thetreatment of ocular perforating injuries. Am J Ophthalmol1976; 81: 733-9.
12 Conway BP, Michels RG. Vitrectomy techniques in the
816
on July 1, 2020 by guest. Protected by copyright.
http://bjo.bmj.com
/B
r J Ophthalm
ol: first published as 10.1136/bjo.64.11.809 on 1 Novem
ber 1980. Dow
nloaded from

Penetrating eye injuries
management of selected penetrating ocular injuries.Trans Am Acad Ophthalmol Otolaryngol 1978; 85: 560-83.
13 Ryan SJ, Allen AW. Pars plana vitrectomy in oculartrauma. Am J Ophthalmol 1979; 88: 483-91.
14 Cleary PE, Minckler DS, Ryan SJ. Ultrastructure oftraction retinal detachment in rhesus monkey eyes aftera posterior penetrating eye injury. Am J Ophthalmol inpress.
15 Hogan MJ, Zimmerman LE. Ophthalmic Pathology: AnAtlas and Textbook. Philadelphia: Saunders, 1964.
16 Grillo HC. Derivation of fibroblasts in the healing wound.Arch Surg 1964; 88: 82-8.
17 Peacock EE, VanWinkle W. Surgery and Biology ofWound Repair. Philadelphia: Saunders, 1970.
18 Cleary PE, Ryan SJ. Experimental posterior penetrating
eye injury in the rabbit. 11. Histology of wound, vitreousand retina. Br J Ophthalmol 1979; 63: 312-21.
19 Topping TN, Abrams GW, Machemer R. Experimentaldouble-perforating injury of the posterior segment inrabbit eyes. The natural history of intraocular prolifera-tion. Arch Ophthalmol 1979; 97: 735-42.
20 Cleary PE, Ryan SJ. Method of production and naturalhistory of experimental posterior penetrating eye injuryin the rhesus monkey. Am J Ophthalmol 1979; 88: 221-31.
21 Cleary PE, Ryan SJ. Histology of wound, vitreous, andretina in experimental posterior penetrating eye injuryin the rhesus monkey. Am J Ophthalmol 1979; 88: 212-20.
22 Cleary PE, Ryan SJ. Experimental posterior penetratingeye injury in the rabbit. I. Method of production andnatural history. Br J Ophthalmol 1979; 63: 306-11.
817
on July 1, 2020 by guest. Protected by copyright.
http://bjo.bmj.com
/B
r J Ophthalm
ol: first published as 10.1136/bjo.64.11.809 on 1 Novem
ber 1980. Dow
nloaded from