PEDIATRICS is the official journal of the American Academy ... · Neonatal Resuscitation: 2010...
28
DOI: 10.1542/peds.2010-2972B 2010;126;e1319-e1344; originally published online Oct 18, 2010; Pediatrics COLLABORATORS CHAPTER Sithembiso Velaphi and on behalf of the NEONATAL RESUSCITATION Sam Richmond, Wendy M. Simon, Nalini Singhal, Edgardo Szyld, Masanori Tamura, Chameides, Jay P. Goldsmith, Ruth Guinsburg, Mary Fran Hazinski, Colin Morley, Jeffrey M. Perlman, Jonathan Wyllie, John Kattwinkel, Dianne L. Atkins, Leon Recommendations Resuscitation and Emergency Cardiovascular Care Science With Treatment Neonatal Resuscitation: 2010 International Consensus on Cardiopulmonary http://www.pediatrics.org/cgi/content/full/126/5/e1319 located on the World Wide Web at: The online version of this article, along with updated information and services, is rights reserved. Print ISSN: 0031-4005. Online ISSN: 1098-4275. Grove Village, Illinois, 60007. Copyright © 2010 by the American Academy of Pediatrics. All and trademarked by the American Academy of Pediatrics, 141 Northwest Point Boulevard, Elk publication, it has been published continuously since 1948. PEDIATRICS is owned, published, PEDIATRICS is the official journal of the American Academy of Pediatrics. A monthly . Provided by Health Internetwork on December 13, 2010 www.pediatrics.org Downloaded from
Transcript of PEDIATRICS is the official journal of the American Academy ... · Neonatal Resuscitation: 2010...

DOI: 10.1542/peds.2010-2972B 2010;126;e1319-e1344; originally published online Oct 18, 2010; Pediatrics
COLLABORATORS CHAPTERSithembiso Velaphi and on behalf of the NEONATAL RESUSCITATION
Sam Richmond, Wendy M. Simon, Nalini Singhal, Edgardo Szyld, Masanori Tamura,Chameides, Jay P. Goldsmith, Ruth Guinsburg, Mary Fran Hazinski, Colin Morley,
Jeffrey M. Perlman, Jonathan Wyllie, John Kattwinkel, Dianne L. Atkins, Leon Recommendations
Resuscitation and Emergency Cardiovascular Care Science With Treatment Neonatal Resuscitation: 2010 International Consensus on Cardiopulmonary
http://www.pediatrics.org/cgi/content/full/126/5/e1319located on the World Wide Web at:
The online version of this article, along with updated information and services, is
rights reserved. Print ISSN: 0031-4005. Online ISSN: 1098-4275. Grove Village, Illinois, 60007. Copyright © 2010 by the American Academy of Pediatrics. All and trademarked by the American Academy of Pediatrics, 141 Northwest Point Boulevard, Elkpublication, it has been published continuously since 1948. PEDIATRICS is owned, published, PEDIATRICS is the official journal of the American Academy of Pediatrics. A monthly
. Provided by Health Internetwork on December 13, 2010 www.pediatrics.orgDownloaded from

Special Report—Neonatal Resuscitation:2010 International Consensus on CardiopulmonaryResuscitation and Emergency Cardiovascular CareScience With Treatment Recommendations
Note From the Writing Group: Throughout this article, the reader willnotice combinations of superscripted letters and numbers (eg, “Peripar-tum SuctioningNRP-011A, NRP-012A”). These callouts are hyperlinked toevidence-basedworksheets, whichwere used in the development of thisarticle. An appendix of worksheets, applicable to this article, is locatedat the end of the text. The worksheets are available in PDF format andare open access.
Approximately 10% of newborns require some assistance to beginbreathing at birth, and�1% require extensive resuscitation (LOE 41,2).Although the vast majority of newborn infants do not require interven-tion to make the transition from intrauterine to extrauterine life, thelarge number of births worldwide means that many infants requiresome assistance to achieve cardiorespiratory stability. Newborn in-fants who are born at term and are breathing or crying and have goodtone must be dried and kept warm. These actions can be provided withthe baby lying on themother’s chest and should not require separationof mother and baby.
All others need to be assessed to determine their need for one or moreof the following actions in sequence:
A. Initial steps in stabilization (dry and provide warmth, position,assess the airway, stimulate to breathe)
B. Ventilation
C. Chest compressions
D. Medications or volume expansion
Progression to the next step is initially based on simultaneous assess-ment of 2 vital characteristics: heart rate and respirations. Progres-sion occurs only after successful completion of the preceding step.Approximately 30 seconds is allotted to complete each of the first 2steps successfully, reevaluate, and decide whether to progress to thenext (see Figure: Newborn Resuscitation Algorithm).
Since publication of the 2005 International Consensus on CPR and ECCScience With Treatment Recommendations,3,4 several controversialneonatal resuscitation issues have been identified. The literature wasresearched and a consensus was reached on the assessment of oxy-genation and role of supplementary oxygen, peripartum managementof meconium, ventilation strategies, devices to confirm placement ofan advanced airway (eg, tracheal tube or laryngeal mask airway), med-
Jeffrey M. Perlman, Co-Chair*, Jonathan Wyllie, Co-Chair*,John Kattwinkel, Dianne L. Atkins, Leon Chameides, Jay P.Goldsmith, Ruth Guinsburg, Mary Fran Hazinski, ColinMorley, Sam Richmond, Wendy M. Simon, Nalini Singhal,Edgardo Szyld, Masanori Tamura, Sithembiso Velaphi, onbehalf of the NEONATAL RESUSCITATION CHAPTERCOLLABORATORS
KEY WORDSarrhythmia, cardiopulmonary resuscitation, pediatrics,resuscitation
The American Heart Association requests that this document becited as follows: Perlman JM, Wyllie J, Kattwinkel J, Atkins DL,Chameides L, Goldsmith JP, Guinsburg R, Hazinski MF, Morley C,Richmond S, Simon WM, Singhal N, Szyld E, Tamura M, Velaphi S;on behalf of the Neonatal Resuscitation Chapter Collaborators.Part 11: neonatal resuscitation: 2010 International Consensus onCardiopulmonary Resuscitation and Emergency CardiovascularCare Science With Treatment Recommendations. Circulation.2010;122(suppl 2):S516–S538.
*Co-chairs and equal first co-authors.
(Circulation. 2010;122[suppl 2]:S516–S538.)
© 2010 American Heart Association, Inc., European ResuscitationCouncil, and International Liaison Committee on Resuscitation.
Circulation is available at http://circ.ahajournals.org
doi:10.1542/peds.2010-2972B
FROM THE AMERICAN ACADEMY OF PEDIATRICS
PEDIATRICS Volume 126, Number 5, November 2010 e1319. Provided by Health Internetwork on December 13, 2010 www.pediatrics.orgDownloaded from

ications, maintenance of body temper-ature, postresuscitation management,and considerations for withholding anddiscontinuing resuscitation. Educationaltechniques for teaching, assessing, andmaintaining resuscitation knowledge
and skills and issues regarding the per-sonnel needed at cesarean sectionswere also debated. The following are themajor new recommendations:
● Progression to the next step fol-lowing the initial evaluation is now
defined by the simultaneous as-sessment of 2 vital characteristics:heart rate and respirations. Oxime-try should be used for evaluation ofoxygenation because assessment ofcolor is unreliable.
FIGURE.Newborn Resuscitation Algorithm.
e1320 FROM THE AMERICAN ACADEMY OF PEDIATRICS. Provided by Health Internetwork on December 13, 2010 www.pediatrics.orgDownloaded from

● For babies born at term it is best tobegin resuscitation with air ratherthan 100% oxygen.
● Administration of supplementary oxy-gen should be regulated by blendingoxygen and air, and the concentra-tion delivered should be guided byoximetry.
● The available evidence does notsupport or refute the routine endo-tracheal suctioning of infants bornthrough meconium-stained amni-otic fluid, even when the newborn isdepressed.
● The chest compression-ventilationratio should remain at 3:1 for neo-nates unless the arrest is knownto be of cardiac etiology, in whichcase a higher ratio should beconsidered.
● Therapeutic hypothermia should beconsidered for infants born at termor near-term with evolving mod-erate to severe hypoxic-ischemicencephalopathy, with protocol andfollow-up coordinated through a re-gional perinatal system.
● It is appropriate to consider dis-continuing resuscitation if therehas been no detectable heart ratefor 10 minutes. Many factors con-tribute to the decision to continuebeyond 10 minutes.
● Cord clamping should be delayedfor at least 1 minute in babies whodo not require resuscitation. Evi-dence is insufficient to recommenda time for clamping in those who re-quire resuscitation.
INITIAL ASSESSMENTAND INTERVENTION
Assessment of CardiorespiratoryTransition and Need forResuscitationNRP-001A, NRP-001B, NRP-014A, NRP-014B
Consensus on ScienceA prompt increase in heart rate re-mains the most sensitive indicator ofresuscitation efficacy (LOE 55). Of the
clinical assessments, auscultation ofthe heart is the most accurate, withpalpation of the umbilical cord less so.However, both are relatively insensi-tive (LOE 26 and LOE 47). Several studieshave addressed the accuracy of pulseoximetry in measuring heart rate inthe delivery room and have shown thefeasibility of pulse oximetry duringnewborn resuscitation. However, noneof these studies examined the impactof these measurements on resuscita-tion outcomes (LOE 47,8). Pulse oxime-try (SpO2) and heart rate can be mea-sured reliably after 90 seconds frombirthwith a pulse oximeter designed toreduce movement artifact and a neo-natal probe (LOE 49,10). Preductal val-ues, obtained from the right wrist orhand, are higher than postductal val-ues.8,11 Applying the oximeter probe tothe subject before connecting it to theinstrument will produce reliable re-sults more quickly (LOE 410).
There is clear evidence that an in-crease in oxygenation and improve-ment in color may take many minutesto achieve, even in uncompromised ba-bies. Furthermore, there is increasingevidence that exposure of the newlyborn to hyperoxia is detrimental tomany organs at a cellular and func-tional level. For this reason color hasbeen removed as an indicator of oxy-genation or resuscitation efficacy. Theoximeter can be used to adjust the in-crease in oxygenation to that of the un-compromised baby born at term.
Treatment RecommendationsHeart rate should remain the primaryvital sign by which to judge the needfor and efficacy of resuscitation. Aus-cultation of the precordium should re-main the primary means of assessingheart rate. There is a high likelihoodof underestimating heart rate withpalpation of the umbilical pulse, butthis is preferable to other palpationlocations.
For babies who require ongoing resus-citation or respiratory support orboth, the goal should be to use pulseoximetry. The sensor should be placedon the baby’s right hand or wrist be-fore connecting the probe to the in-strument. Because of concerns aboutthe ability to consistently obtain accu-rate measurements, pulse oximetryshould be used in conjunction with andshould not replace clinical assess-ment of heart rate during newbornresuscitation.
Use of SupplementaryOxygenNRP-013A, NRP-013B, NRP-014A, NRP-014B
Consensus on ScienceIn term infants receiving resuscitationwith intermittent positive-pressureventilation, 100% oxygen conferred noadvantage over air in the short termand resulted in increased time to firstbreath or cry or both (LOE 212,13). Meta-analyses of these studies showed a de-crease in mortality with the group forwhom resuscitation was initiated withair.14,15
There is evidence in newborn animalmodels of asphyxia that exposure tohigh concentrations of oxygen at re-suscitation does not confer any clinicaladvantage and is potentially harmfulat the cellular level.16,17 Two animal mod-els of hypoxia-ischemia and persistentbradycardia found that those resusci-tatedwith roomair rather than 100%ox-ygen developed untoward biochemicalchanges in the brain (LOE 518,19).
In preterm infants at�32 weeks’ ges-tation, if attempting to mimic the grad-ual rise in oxygen saturation of healthyterm babies in the first 10 minutes af-ter birth by titrating the concentrationto the baby’s saturation, initial use ofair or 100% oxygen is more likely toresult in hypoxemia or hyperoxemia,respectively, than initiation of resus-citation with 30% or 90% oxygen andtitration to oxygen saturation (LOE 211,20).There is insufficient evidence in babies
FROM THE AMERICAN ACADEMY OF PEDIATRICS
PEDIATRICS Volume 126, Number 5, November 2010 e1321. Provided by Health Internetwork on December 13, 2010 www.pediatrics.orgDownloaded from

born at 32 to 37 weeks’ gestation todefine the appropriate oxygen admin-istration strategy.
Treatment RecommendationIn term infants receiving resuscitationat birth with positive-pressure ventila-tion, it is best to begin with air ratherthan 100% oxygen. If despite effectiveventilation there is no increase inheart rate or if oxygenation (guided byoximetry) remains unacceptable, useof a higher concentration of oxygenshould be considered.
Because many preterm babies of�32weeks’ gestation will not reach targetsaturations in air, blended oxygen andairmay be given judiciously and ideallyguided by pulse oximetry. Both hyper-oxemia and hypoxemia should beavoided. If a blend of oxygen and air isnot available, resuscitation should beinitiated with air.
Peripartum SuctioningNRP-011A, NRP-012A
Peripartum suctioning was examinedfrom 2 perspectives: (1) suctioning ofthe airway in depressed neonatesborn through clear amniotic fluid and(2) tracheal suctioning in depressedneonates born through meconium-stained amniotic fluid.
Suctioning of the Upper Airway
Consensus on ScienceThere is no evidence to support or re-fute suctioning of the mouth and noseof depressed neonates at birth whenthe infant is born through clear am-niotic fluid. In healthy neonates suc-tioning of the mouth and nose isassociated with cardiorespiratorycomplications (LOE 121,22). In infantswho are intubated, sedated, or para-lyzed following resuscitation, endotra-cheal suctioning in the absence of se-cretions may result in a decrease inoxygenation, an increase in cerebralblood flow and intracranial pressure,and a decrease in compliance (LOE523).
Treatment RecommendationRoutine intrapartum oropharyngealand nasopharyngeal suctioning for in-fants born with clear or meconium-stained amniotic fluid is no longerrecommended.
Tracheal Suctioning
Consensus on ScienceDepressed infants born throughmeconium-stained amniotic fluid areat increased risk of developing meco-nium aspiration syndrome (LOE 424,25).Although these infants are at in-creased risk of developing meconiumaspiration syndrome, the use of tra-cheal suctioning has not been associ-ated with a reduction in the incidenceof meconium aspiration syndrome ormortality (LOE 426; LOE 527). No random-ized controlled studies have comparedintubation and tracheal suctioning andno tracheal suctioning in depressedinfants.
Treatment RecommendationThe available evidence does not sup-port or refute the routine endotra-cheal suctioning of depressed infantsborn throughmeconium-stained amni-otic fluid.
VENTILATION STRATEGIESNRP-028A, NRP-028B
Ventilation strategies were examinedfrom 4 perspectives: (1) characteris-tics of the initial assisted breaths andthe role of positive end-expiratorypressure (PEEP), (2) continuous posi-tive airway pressure (CPAP) during orfollowing resuscitation, (3) devices toassist ventilation, and (4) strategieswhen resources are limited.
Initial Breaths
Consensus on ScienceBoth longer and shorter inspiratorytimes are in clinical use for initial ven-tilation in term infants, but there areno randomized controlled trials com-paring these 2 approaches. In a smallcase series in term infants, a pro-
longed initial inflation of 5 secondsproduced a 2-fold increase in func-tional residual capacity comparedwith historic controls (LOE 428). A singlerandomized controlled trial in preterminfants of a 10-second sustained infla-tion followed by nasal CPAP comparedwith face mask ventilation demon-strated decreased need for intubationin the first 72 hours, shorter durationof ventilatory support, and reducedbronchopulmonary dysplasia (LOE 129).Two other randomized controlled tri-als failed to showabenefit fromdeliveryroomapplication of a sustained initial in-flation followedbynasal CPAP (LOE130,31).Multiple variables among the 3 random-ized controlled trials, including mode ofintervention (nasopharyngeal tube ver-sus face mask, T-piece versus self-inflating bag), as well as the use of CPAPin the delivery room make it difficult todetermine the effect of the initial sus-tained inflation on establishing a func-tional residual capacity in very preterminfants.
PressureThere is no evidence to support the useof inflation pressures higher thanthose that are necessary to achieve im-provement in heart rate or chest ex-pansion. This can usually be achievedin term infants with an inflation pres-sure of 30 cm H2O (LOE 428,32) and inpreterm infants with pressures of 20to 25 cm H2O (LOE 433). Occasionallyhigher pressures are required (LOE434). In immature animals, ventilationat birth with high tidal volumes asso-ciated with the generation of highpeak inflation pressures for a fewminutes causes lung injury, impairedgas exchange, and reduced lungcompliance (LOE 535).
Positive End-Expiratory PressureThere is no evidence to support or re-fute the value of PEEP during resusci-tation of term infants. In preterm in-fants 1 small study did not show a
e1322 FROM THE AMERICAN ACADEMY OF PEDIATRICS. Provided by Health Internetwork on December 13, 2010 www.pediatrics.orgDownloaded from

benefit from PEEP during initial stabili-zation in reducing the number of in-fants who required intubation in thedelivery room (LOE 136). In studies ofintubated immature animals the use ofPEEP during initial stabilization afterbirth improved functional residual ca-pacity, oxygenation, and lung compli-ance and reduced lung injury (LOE537,38), but high levels of PEEP (8 to 12cm H2O) may reduce pulmonary bloodflow and increase the risk of pneumo-thorax (LOE 539,40).
Treatment RecommendationTo establish initial lung inflation in ap-neic newborn infants, initiation of in-termittent positive-pressure ventila-tion at birth can be accomplished witheither shorter or longer inspiratorytimes. Initial peak inflating pressuresnecessary to achieve an increase inheart rate or movement of the chest arevariable and unpredictable and shouldbe individualized with each breath. Ifpressure is being monitored, an initialinflation pressure of 20 cm H2O may beeffective in preterm babies, but a pres-sure of 30 to 40 cm H2O may be neces-sary in some term babies. If pressure isnot being monitored, the minimal infla-tion required to achieve an increase inheart rate should be used. Providersshould avoid creation of excessive chestwall movement during ventilation of pre-term infants immediately after birth.
Although measured peak inflation pres-sure does not correlatewellwith volumedelivered in the context of changing re-spiratorymechanics,monitoringof infla-tion pressure may help provide consis-tent inflations and avoid unnecessarilyhigh pressures. If positive-pressure ven-tilation is required, an initial inflationpressure of 20 to 25 cm H2O is adequatefor most preterm infants. If prompt im-provement in heart rate or chest move-ment is not obtained, then higher pres-sures to achieve effective ventilationmay be needed. PEEP is likely to be bene-ficial during initial stabilization of apneic
preterm infants who require positive-pressure ventilation and should be usedif suitable equipment is available.
Continuous Positive AirwayPressureNRP-002A, NRP-002B
Consensus on ScienceFor spontaneously breathing preterminfants at �25 weeks’ gestation whohave signs of respiratory distress,there is no significant difference be-tween starting CPAP or intubation andmechanical ventilation in the deliveryroom when considering death or oxy-gen requirement at 36weeks postmen-strual age. In spontaneously breathinginfants at 25 to 28 weeks’ gestation,CPAP compared with intubation re-duced the rates of mechanical ventila-tion from 100% to 46% and surfactantuse from 77% to 38% (LOE 141). In thesame trial infants on CPAP had a signif-icantly increased rate of pneumotho-rax (9% versus 3%) (LOE 141). There isno evidence to support or refute theuse of CPAP in the term baby.
For very preterm infants, a multifacetedintervention, including PEEP, giving asustained inflation and starting CPAP inthe delivery room reduces the need forintubation and rate of mechanical venti-lation within 72 hours and reduces inci-dence of bronchopulmonary dysplasiacompared with positive-pressure venti-lation with a self-inflating bag via a facemask (LOE 129). When comparedwith his-toric controls, use of delivery roomCPAPfor very premature infants was associ-ated with a decrease in the requirementfor intubation, days onmechanical venti-lation, and use of postnatal steroids (LOE433), althoughasmall underpowered fea-sibility trial of delivery room CPAP/PEEPversus no CPAP/PEEP did not show a sig-nificant difference in immediate out-comes (LOE 136).
Treatment RecommendationSpontaneously breathing preterm in-fants who have respiratory distressmay be supported with CPAP or intuba-
tion and mechanical ventilation. Themost appropriate choice may be guidedby local expertise and preferences.
Assisted VentilationDevicesNRP-015A, NRP-015B, NRP-015C, NRP-017A,NRP-017B
Consensus on ScienceThere are no clinical studies in new-borns requiring positive pressure dur-ing resuscitation to support or refutethe superiority of the T-piece resus-citator over bag-mask ventilation in im-proving outcome. In mechanical modelstarget inflation pressures are deliv-ered more consistently when usingT-piece resuscitators than with self-inflating bags or flow-inflating bags(LOE 542,43). In mechanical models PEEPis maintained more consistently withT-piece resuscitators compared withself-inflating bags or flow-inflatingbags (LOE 544). In mechanical modelsthe ability to deliver a sustained infla-tion is better with either a T-piece re-suscitator or flow-inflating bag thanwith a self-inflating bag (LOE 542,45).
Treatment RecommendationVentilation of the newborn can be per-formed effectively with a flow-inflatingbag, a self-inflating bag, or a pressure-limited T-piece resuscitator.
Laryngeal Mask AirwayNRP-017A, NRP-017B
Consensus on ScienceIn 1 randomized controlled trial (LOE146) providers had similar success pro-viding effective ventilation with eitherthe laryngeal mask airway or facemask among newborns in the deliveryroom. In 1 retrospective cohort study(LOE 247) and 3 large case series (LOE448) effective ventilation was achievedquickly using a laryngeal mask airwayin newborns weighing �2000 g or de-livered at �34 weeks’ gestation. In 1randomized controlled trial (LOE 149)and 1 retrospective cohort study (LOE250) providers had similar success pro-viding effective ventilation using either
FROM THE AMERICAN ACADEMY OF PEDIATRICS
PEDIATRICS Volume 126, Number 5, November 2010 e1323. Provided by Health Internetwork on December 13, 2010 www.pediatrics.orgDownloaded from

the laryngeal mask airway or endo-tracheal tube among newborns in thedelivery room. Although a single co-hort study (LOE 250) suggests thatnewborns resuscitated with a laryn-geal mask may require less respi-ratory support after initial resusci-tation, this conclusion is subject tosignificant selection bias. In multiplesmall case reports effective ventila-tion was achieved with a laryngealmask airway when both face maskventilation and endotracheal intuba-tion were unsuccessful. There is lim-ited evidence to evaluate the effective-ness of the laryngeal mask airway fornewborns weighing �2000 g, deliv-ered at �34 weeks’ gestation, in thesetting of meconium-stained amnioticfluid, during chest compressions, orfor administration of emergency intra-tracheal medications.
Treatment RecommendationThe laryngeal mask airway shouldbe considered during resuscitation ofthe newborn if face mask ventilationis unsuccessful and tracheal intuba-tion is unsuccessful or not feasible.The laryngeal mask airway may beconsidered as an alternative to aface mask for positive-pressure venti-lation among newborns weighing�2000 g or delivered at �34 weeks’gestation. There is limited evidence,however, to evaluate its use for new-borns weighing �2000 g or deliveredat �34 weeks’ gestation. The laryn-geal mask airway may be consid-ered as an alternative to endotra-cheal intubation as a secondaryairway for resuscitation among new-borns weighing�2000 g or deliveredat �34 weeks’ gestation. The laryn-geal mask airway has not been eval-uated in the setting of meconium-stained amniotic fluid, during chestcompressions, or for administration ofemergency intratrachealmedications.
Upper Airway InterfaceDevicesNRP-003A, NRP-003B
Consensus on ScienceWithin classes of interfaces, reportsconflict about the ability to maintain aseal with an anatomically shapedmask compared with a soft roundmask (LOE 551,52). Delivery of positive-pressure ventilation via nasal prongshas been shown to be superior to de-livery via a triangular face mask foroutcomes of chest compressions andintubation (LOE 253). It is likely that dif-ferences in clinical outcomes that havebeen reported in several studies maybe attributable to the targeted inter-vention (ie, CPAP versus intermittentpositive-pressure ventilation) ratherthan the interface. Nasal prongs maybe a more effective device than facemasks for providing respiratory sup-port after birth (LOE 253). There is insuf-ficient evidence to support or refutethe use of one type of mask over an-other for achieving clinical outcome,except that the Rendell-Baker stylemask is suboptimal in achieving an ad-equate seal when used for newborns(LOE 554).
Treatment RecommendationsNasal prongs are an alternative way ofgiving respiratory support.Whichever in-terface is used, providers should ensurethat they are skilled in using the inter-face devices available at the institution.Differentmasksmustbeheld indifferentways to appropriately reduce leak.
Exhaled Air VentilationNRP-004A, NRP-004B
Consensus on ScienceMouth-to-mouth ventilation is less effec-tive than a self-inflating bag or tube andmask in improving survival rates in new-borns with birth asphyxia (LOE 355). Useof mouth-to-mask ventilation at 30 insuf-flations perminute is as effective as self-inflatingbag-mask ventilation in increas-ing heart rate in the first 5minutes afterbirth (LOE 256). Mask-to-tube ventilation
may cause infection in newborn infants(LOE 557). Two studies (LOE 558,59) demon-strated that tube-to-mask ventilation canbe easily taught and acceptable breathsdelivered. However, tube-to-mask venti-lation was more difficult to use (LOE 560;LOE 355).
Treatment RecommendationBag-mask ventilation is preferable tomouth-to-mask ventilation or tube-to-mask ventilation during neonatal re-suscitation, but one of the latter twoshould be used when bag-mask de-vices are not available. Precautionsmust be taken becausemouth-to-maskand mouth tube–to-mask ventilationare less comfortable and more tiringthan bag-mask ventilation for the new-born at birth and may be associatedwith increased risk of infection in theinfant and healthcare provider.
MONITORING DURING ANDAFTER INTUBATION
Gas Monitoring Devices
Measurement of TidalVolumeNRP-005A, NRP-005B, NRP-005C
Consensus of ScienceThere are no studies that compareclinical outcomes in newborns afterresuscitation with or without monitor-ing of tidal volume. In preterm animalmodels the tidal volume used duringinitial ventilation after birth may altersubsequent lung function and induceinflammation, but other factors, in-cluding the use and level of PEEP, ap-pear to interact with tidal volume indetermining specific effects (LOE561,62). It is unclear whether the abso-lute tidal volumes used affected out-comes. Studies in manikins and ani-mals (LOE 563,64) suggest that providerscannot maintain constant pressuresor assess delivered volume duringmanual ventilation. The position of themask and degree of leak may be im-proved by the use of a volume monitor(LOE 565).
e1324 FROM THE AMERICAN ACADEMY OF PEDIATRICS. Provided by Health Internetwork on December 13, 2010 www.pediatrics.orgDownloaded from

Treatment RecommendationsVentilation during newborn resuscita-tion should aim to adequately inflatethe lung while avoiding overinfla-tion. There is insufficient evidence torecommend routine use of tidal vol-ume monitoring in neonates receivingpositive-pressure ventilation duringresuscitation.
Use of Exhaled CO2 Detectors toConfirm Tracheal TubePlacementNRP-016A
Consensus on ScienceStudies (LOE 266–68) suggest that detec-tion of exhaled CO2 confirms trachealintubation in neonates with cardiacoutput more rapidly and accuratelythan clinical assessment alone. False-negative readings have been reportedduring cardiac arrest (LOE 469) despitemodels suggesting efficacy (LOE 570).False-positive readingsmay occurwithcolorimetric devices contaminatedwith epinephrine (adrenaline), surfac-tant, and atropine (LOE 571). Neonatalstudies have excluded infants whoneed extensive resuscitation. There isno comparative information to recom-mend any one method for detection ofexhaled CO2 in the neonatal population.
Treatment RecommendationDetection of exhaled CO2 in addition toclinical assessment is recommendedas themost reliablemethod to confirmendotracheal placement in neonateswith spontaneous circulation.
Colorimetric CO2 Detection toAssess Ventilation in NonintubatedPatientsNRP-018A, NRP-018B, NRP-018C
Consensus on ScienceThe use of colorimetric exhaled CO2 de-tectors during face mask ventilation ofsmall numbers of preterm infants in theintensive care unit (LOE 472) and the de-livery room (LOE 473) has been reportedand may help identify airway obstruc-tion. It is unclear whether the use ofexhaled CO2 detectors during face mask
ventilation confers additional benefitover clinical assessment alone. No risksattributed to the use of exhaled CO2 de-tectors have been identified. The use ofexhaled CO2 detectors with other inter-faces (eg, nasal airways, laryngealmasks) during positive-pressure ventila-tion in the delivery room has not beenreported.
Treatment RecommendationThere is insufficient evidence to recom-mend routine use of colorimetric ex-haled CO2 detectors duringmask ventila-tion of newborns in the delivery room.
CIRCULATORY SUPPORT
ChestCompressionsNRP-006A, NRP-006B, NRP-007A, NRP-007B
Consensus on ScienceIn animal studies of asphyxial modelsof cardiac arrest, piglets resusci-tated with a combination of chestcompressions and ventilations hadbetter outcomes than those resusci-tated with ventilations or compres-sions alone (LOE 574,75). A further studyin piglets suggested that sustainedchest compressions had a deleteriouseffect on myocardial and cerebral per-fusion, especially during prolongedresuscitation.76
A physiologic mathematical modelingstudy suggested that using highercompression-ventilation ratios wouldresult in underventilation of asphyxi-ated infants (LOE 577). The model pre-dicts that between 3 and 5 compres-sions to 1 ventilation should be mostefficient for newborns.
Manikin studies confirm that the 3:1compression-ventilation ratio providesmore ventilations perminutewhen com-pared with higher ratios, but the resus-citation is perceived asbeingmorephys-ically taxing, especially when performedby a lone rescuer (LOE 578,79). Adult man-ikin studies using 2 rescuers haveshown that a 5:1 ratio provides better-quality chest compressions than a 15:2
ratio (LOE 580) but can result in moremissed ventilations per cycle (LOE 581).A pediatric manikin study of mouth-to-mouth ventilation by a lone lay rescuerfound equivalent minute ventilation forboth the 15:2 and 5:1 ratios, but the15:2 ratio produced more chest com-pressions per minute (LOE 582). With2-rescuer CPR provided by nursing stu-dents, however, minute ventilation andcompressions per minute were in-creasedwith the5:1 ratiocomparedwiththe 10:2 and 15:2 ratios (LOE 583). Whenthe 15:2 ratio was compared with the30:2 ratio in a 1-rescuer model of medi-cal personnel using adolescent, child,and infant manikins, more compressioncycles could be achieved with the 30:2ratio on all manikins with no apparenteffect on quality of compressions (LOE584). Effect on ventilation, however, wasnot assessed. One study in children sug-gested that CPR with rescue breathingis preferable to CPR alone when the ar-rest is of noncardiac etiology (LOE 585).There are no data regarding the opti-mum compression-ventilation ratios inneonates or neonatal models of primarycardiac versus predominantly asphyxialarrest.
Evidence from randomized studies inswine models (LOE 586,87), manikin stud-ies (LOE 584,88), small case series (LOE489), and cadavers (LOE 590) support thecurrent practice of favoring the 2thumb–encircling hands technique ofchest compressions when comparedwith the 2-finger technique. The formermethod produces higher blood pres-sure, can sustain a consistent quality ofcompressions for a longer time, and isperceived as easier and less tiring forthe provider. One manikin study involv-ing a variety of medical or quasimedicalpersonnel (LOE 591) found no differencein a number of qualitative measures be-tween the 2 techniques other than signif-icantly fewer compressionswere judgedas too shallow with the 2-thumb tech-nique. One small case series in new-
FROM THE AMERICAN ACADEMY OF PEDIATRICS
PEDIATRICS Volume 126, Number 5, November 2010 e1325. Provided by Health Internetwork on December 13, 2010 www.pediatrics.orgDownloaded from

borns found higher systolic blood pres-suregeneratedwith the2-finger techniquewhen compared with the 2 thumb–encir-cling hands technique (LOE 492). Both tech-niques, however, generated comparableandadequatediastolicpressures, amoreimportant determinant of coronary per-fusion. Compressions should be cen-teredover the lower thirdof the sternumrather than the mid-sternum (LOE 593,94).Chest compression depth should favorone third the external anterior-posteriordiameterof thechest rather thandeepercompressions (LOE 595).
Treatment RecommendationThere isnoevidence fromqualityhuman,animal, manikin, or mathematical mod-eling studies to warrant a change fromthe current compression-ventilation ra-tio of 3:1. Strategies should be consid-ered for optimizing the quality of com-pressions and ventilations with as fewinterruptions as possible. Because venti-lation is critical to reversal of newbornasphyxial arrest, any higher ratio thatdecreases minute ventilation should beintroduced with caution. If the arrest isknown to be of cardiac etiology, a highercompression-ventilation ratio should beconsidered (eg, 15:2).
Chest compressions in the newbornshould be delivered by the 2 thumb–en-circling hands method as the preferredoption. Compressions should be cen-teredover the lower thirdof the sternumand should compress the chest onethird the anterior-posterior diameter.Any chest compressions should be per-formed in combinationwith adequate in-flation breaths.
MEDICATIONS ANDFLUID ADMINISTRATION
Epinephrine
Route and Dose ofEpinephrineNRP-008A, NRP-008B, NRP-009A, NRP-009B
Consensus on ScienceDespite the widespread use of epineph-rine during resuscitation, no controlled
clinical trials have directly compared en-dotracheal and intravenous administra-tion of epinephrine among neonateswith a heart rate of �60 beats perminute despite adequate ventilation andchest compressions. Limited evidencefrom neonatal case series or case re-ports (LOE 496,97) indicates that epineph-rine administered by the endotrachealroute using awide range of doses (0.003mg/kg to 0.25 mg/kg) may result in re-turn of spontaneous circulation (ROSC)or an increase in heart rate when intra-venous access is not available. Thesecase series are limited by inconsistentstandards for epinephrine administra-tion and are subject to both selectionand reporting bias.
Evidence from 1 case series using rigor-ously defined standards for epinephrineadministration and outcomes reportingindicates that endotracheal administra-tion of epinephrine (0.01 mg/kg) is likelyto be less effective than intravenous ad-ministration of the same dose (LOE 42).This is consistent with evidence extrapo-lated from neonatal animal models indi-cating that higher doses (0.05 mg/kg to0.1 mg/kg) of endotracheal epinephrinemay be required to achieve increasedblood epinephrine concentrations and ahemodynamic response equivalent to in-travenous administration (LOE 598,99). Ev-idence extrapolated from adult animalmodels indicates that blood concentra-tions of epinephrine are significantlylower following endotracheal adminis-tration (LOE 5100,101), and endotrachealdoses ranging from 0.05 mg/kg to 0.1mg/kg may be required to achieve ROSC(LOE 5102).
Although it has been widely assumedthat epinephrine can be administeredfaster by the endotracheal route thanby the intravenous route, no clinicaltrials have evaluated this hypothesis.Two studies have reported cases of in-appropriate early use of endotrachealepinephrine before airway and breath-ing are established (LOE 496,97). One
case series describing in-hospital pe-diatric cardiac arrest suggested thatsurvival was higher among infantswho received their first dose of epi-nephrine by the endotracheal route;however, the time required for firstdose administration using the endo-tracheal and intravenous routes wasnot provided (LOE 5103).
Despite the widespread use of epineph-rine during resuscitation, no controlledclinical trials have evaluated the idealdose of epinephrine among neonateswith a heart rate of �60 beats perminute despite adequate ventilation andchest compressions. Evidence extrapo-lated from pediatric studies that in-cluded infants �1 year of age (LOE5104,105) indicate no benefit from intrave-nous epinephrine doses �0.03 mg/kg.This is in contrast to a single pediatriccase series using historic controls thatindicated a marked improvement inROSC using high-dose intravenous epi-nephrine (0.1 mg/kg) among childrenwho had not responded to 2 doses ofstandard epinephrine (0.01 mg/kg) (LOE5106). Further extrapolative evidencefrom a meta-analysis of 5 adult clinicaltrials indicates that high-dose intrave-nous epinephrine may increase ROSCbut offers no benefit in survival to hospi-tal discharge (LOE 5107). Evidence from aplanned secondary analysis of a pediat-ric randomized controlled trial suggestsan increased risk of mortality amongchildren receiving high-dose intrave-nous epinephrine (0.1 mg/kg) (LOE 5104).Additional evidence from 2 pediatric ani-mal studies (LOE 5108,109) indicates thatintravenous epinephrine �0.1 mg/kgincreased risk of postresuscitationmortality and interfered with cerebralcortical blood flow and cardiac output.There are no published studies compar-ing standard- and high-dose endotra-cheal epinephrine in the neonatal popu-lation with hypoxic-hypercarbic arrest,and the ideal dose for endotrachealadministration is unknown. Data from
e1326 FROM THE AMERICAN ACADEMY OF PEDIATRICS. Provided by Health Internetwork on December 13, 2010 www.pediatrics.orgDownloaded from

neonatal case series and animal modelssuggest that higherdoses (0.05mg/kg to0.1 mg/kg) of endotracheal epinephrinemay be required to achieve increasedblood epinephrine concentrations and ahemodynamic response equivalent to in-travenous administration (LOE 42,96).
Treatment RecommendationIf adequate ventilation and chest com-pressions have failed to increase theheart rate to�60beats perminute, thenit is reasonable to use epinephrine de-spite the lack of human neonatal data. Ifepinephrine is indicated, a dose of 0.01to 0.03 mg/kg should be administeredintravenously as soon as possible. If ad-equate ventilation and chest compres-sions have failed to increase the heartrate to�60 beats per minute and intra-venous access is not available, then it isreasonable to administer endotrachealepinephrine. If epinephrine is adminis-tered by the endotracheal route, it islikely that a larger dose (0.05 mg/kg to0.1mg/kg)will be required to achieve aneffect similar to that of the 0.01 mg/kgintravenous dose. Higher intravenousdoses cannot be recommended andmaybe harmful.
VolumeExpansionNRP-029A, NRP-029B, NRP-029C
Consensus on ScienceMultiple case series support the use ofvolume expansion in babies with a his-tory of blood loss, including some whoare unresponsive to chest compres-sions (LOE 4110). Many with pallor andtachycardia responded to volumeexpan-sion without having received chest com-pressions. In the absence of a history ofblood loss there is limited evidence ofbenefit from administration of volumeduring resuscitation unresponsive tochest compressions/epinephrine (LOE4111) and some suggestion of potentialharm from animal studies (LOE 5112,113).
Treatment RecommendationEarly volume replacementwith crystal-loid or red cells is indicated for babies
with blood loss who are not respond-ing to resuscitation. There is insuffi-cient evidence to support the routineuse of volume administration in theinfant with no blood loss who is re-fractory to ventilation, chest com-pressions, and epinephrine. Becauseblood loss may be occult, a trial of vol-ume administration may be consid-ered in babies who do not respond toresuscitation.
Other DrugsVery rarely a narcotic antagonist (nalox-one), sodium bicarbonateNRP-021A, NRP-021B,or vasopressors may be useful afterresuscitation.
NaloxoneNRP-022A, NRP-022B
Consensus on ScienceThere are no data comparing naloxonewith positive-pressure ventilation asthe main intervention for opioid-exposed newborn infants who are ap-neic at birth. For newborns who arevigorous in the delivery room despitematernal use of opioids, naloxone sub-tly increases ventilation parameters(such as increased alveolar ventilationand improved CO2 response curves)for a short time, but the clinical rele-vance of these observations is question-able (LOE 4114). Several other studiesfound no difference between vigoroustreatment with naloxone and placeboor no drug treatment for newbornswith outcomes of pH, PCO2, Apgarscores, and neurologic outcomes (LOE5115). Studies examining naloxone haveconsistently demonstrated that it isfrequently misused (LOE 4116). Nalox-one given to a baby born to an opioid-addicted mother has been associatedwith seizures (LOE 5117). There are con-cerns about short- and long-termsafety of naloxone in neonates (LOE5118). Naloxone is absorbed more effec-tively when given intravenously buthas a shorter half-life compared withintramuscular administration.
Treatment RecommendationNaloxone is not recommended as partof the initial resuscitation for new-borns with respiratory depression inthe delivery room. For the clinicalsituation of a newborn with respira-tory depression after maternal opiateexposure, the focus needs to remainon effective ventilation and airwaysupport for the persistently apneicnewborn.
Vascular AccessNRP-020A
Consensus on ScienceMultiple clinical series and case re-ports suggest that fluids and medica-tions can be successfully delivered bythe intraosseous route during resusci-tation of neonates when equipment orpersonnel skilled in establishing ve-nous access are not available or ifother vascular access sites (especiallyintravenous) cannot be successfullyestablished within several minutes(LOE 4119,120).
Treatment RecommendationTemporary intraosseous access toprovide fluids and medications to re-suscitate critically ill neonates may beindicated following unsuccessful at-tempts to establish intravenous vascu-lar access or when caregivers aremore skilled at securing intraosseousaccess.
SUPPORTIVE THERAPY
Temperature Control
Maintenance of BodyTemperatureNRP-023A
Consensus on ScienceA large body of evidence supports thewrapping of newborn infants of �28weeks’ gestation in polythene wrapsor bags at birth without drying to re-duce heat loss (LOE 1121,122). Some ofthese infants were hyperthermic onadmission to the neonatal intensivecare unit, but it is unclear whether thisis because they were born hot or be-
FROM THE AMERICAN ACADEMY OF PEDIATRICS
PEDIATRICS Volume 126, Number 5, November 2010 e1327. Provided by Health Internetwork on December 13, 2010 www.pediatrics.orgDownloaded from

cause they became overheated duringstabilization and transfer. In the ab-sence of polythene wrapping, use ofexothermic mattresses maintainedthe temperature of newborn infantsweighing �1500 g within the normalrange (LOE 2123). A combination of exo-thermic mattresses and polythenewrapping during resuscitation is themost effective strategy to avoid hypo-thermia but may increase the risk ofhyperthermia (LOE3124). Delivery roomtemperatures of at least 26°C for new-borns at�28weeks’ gestation in combi-nation with polythene wraps or bagsmaintained temperatures most effec-tively (LOE 4125; LOE 3126).
Treatment RecommendationNewborn infants of�28 weeks’ gesta-tion should be completely covered in apolythene wrap or bag up to theirnecks without drying immediately af-ter birth and then placed under a radi-ant heater and resuscitated or stabi-lized in a standard fashion. Infantsshould be kept wrapped until admis-sion and temperature check. Hyper-thermia should be avoided. Deliveryroom temperatures should be at least26°C for infants of �28 weeks’gestation.
POSTRESUSCITATION MANAGEMENT
Temperature
HyperthermiaNRP-031A, NRP-031B
Consensus on ScienceInfants born to febrile mothers havebeen reported to have a higher inci-dence of perinatal respiratory de-pression, neonatal seizures, cerebralpalsy, and increased risk of mortality(LOE 4127,128). There is no evidence todetermine whether the fever or thecause of the fever increases the risk tothe baby. In 1 study, neonatal fever atbirth resolved spontaneously within60 minutes (LOE 4129). Adult animaltrials show decreased central nervoussystem injury with antipyretic therapyfor hyperthermia (LOE 5130). In a ran-
domized study high-dose corticoste-roids lowered maternal temperaturebut were associated with an increasednumber of cases of asymptomatic bac-teremia in neonates (LOE 2131).
Treatment RecommendationThere is insufficient evidence to sup-port or refute the routine use of inter-ventions to lower maternal fever to re-duce neonatalmorbidity andmortality.There should be an increased aware-ness that the presence of maternalhyperthermia may lead to a need forneonatal resuscitation. The goal is toachieve normothermia and avoid iat-rogenic hyperthermia.
TherapeuticHypothermiaNRP-024A, NRP-024B
Consensus on ScienceA large body of evidence from 3 largerandomized studies (LOE 1132–134) and2 small randomized trials (LOE 1135,136)demonstrated that induced hypother-mia (33.5° to 34.5°C) implementedwithin 6 hours of birth in term infantsat highest risk for brain injury (as de-fined by specific protocols) and withfurther treatment in neonatal inten-sive care units is associated with sig-nificantly fewer deaths and less neuro-developmental disability at 18-monthfollow-up. The number needed to treatis 9.137 Both cooling methods (systemicversus selective head cooling) wereshown to be effective, but none of thestudies compared them directly. Therandomized trials produced remark-ably consistent results despite usingdifferent methods of cooling.138
Treatment RecommendationsNewly born infants born at or near-term with evolving moderate to se-vere hypoxic-ischemic encephalopathyshould be offered therapeutic hypo-thermia. Whole body cooling and selec-tive head cooling are both appropriatestrategies. Cooling should be initiatedand conducted under clearly defined
protocols with treatment in neonatalintensive care facilities and with thecapability for multidisciplinary care.Treatment should be consistent withthe protocols used in the randomizedclinical trials (ie, begin within 6 hoursof birth, continue for 72 hours afterbirth, and rewarmover at least 4 hours).Carefully monitor for known adverse ef-fects of cooling, eg, thrombocytopeniaand hypotension. All treated infantsshould be followed up longitudinally.
General Supportive Care
GlucoseNRP-019A, NRP-019B
Consensus on ScienceNewborns with lower blood glucose lev-els have a higher incidence of brain in-jury and adverse outcomes after ahypoxic-ischemic insult, although nospecific level associated with worse out-come has been identified (LOE 4139; LOE3140). Increased glucose levels after hyp-oxia-ischemia do not appear to have ad-verse effects in studies of pediatric pa-tients (LOE 5141) or in animal studies (LOE5142) and may be protective (LOE 5143).However, no randomized controlled tri-als have examined this question. Due tothepaucity of data, nospecific target glu-cose concentration range can be identi-fied at present.
Treatment RecommendationIntravenous glucose infusion shouldbe considered as soon as practicalafter resuscitation, with the goal ofavoiding hypoglycemia.
Timing of CordClampingNRP-030A, NRP-030B, NRP-030C, NRP-030D
Consensus on ScienceFor the uncomplicated birth at termthere is evidence of a benefit to delayingcord clamping for aminimum time rang-ing from 1 minute until the cord stopspulsating after delivery. Those with de-layedclampinghad improved ironstatusthrough early infancy but were morelikely to receive phototherapy (LOE 1144).
e1328 FROM THE AMERICAN ACADEMY OF PEDIATRICS. Provided by Health Internetwork on December 13, 2010 www.pediatrics.orgDownloaded from

For an otherwise uncomplicated pre-term birth, there is evidence of a benefitto delaying cord clamping for a mini-mum time ranging from 30 seconds to 3minutes after delivery. Those who expe-rienced delayed clamping in this grouphad higher blood pressures during sta-bilization and a lower incidence of intra-ventricular hemorrhage (LOE 1145) andreceived fewer blood transfusions145
but were more likely to receive photo-therapy (LOE 2144). There are limiteddata on the hazards or benefits of de-layed cord clamping in the nonvigor-ous infant.146,147
Treatment RecommendationDelay in umbilical cord clamping for atleast 1minute is recommended for new-born infants not requiring resuscita-tion. There is insufficient evidence tosupport or refute a recommendation todelay cord clamping in babies requiringresuscitation.
WITHHOLDING ORDISCONTINUING RESUSCITATIVEEFFORTSNRP-025A, NRP-025B, NRP-025C, NRP-026A, NRP-026B,NRP-026C, NRP-027A, NRP-027B
Noninitiation of Resuscitation
Consensus on ScienceFor neonates at the margins of viabilityor those with conditions which predict ahigh risk of mortality or morbidity, atti-tudes and practice vary according to re-gion and availability of resources (LOE4148). Social science studies indicate thatparents would like a larger role in thedecisions to start resuscitation and con-tinue life support of severely compro-mised newborns. Opinions among neo-natal providers vary widely regardingthe benefits and disadvantages of ag-gressive therapies in such newborns(LOE 4149,150). Some data are available tohelp identify conditions associatedwith high mortality and poor outcome(LOE 4151,152). Such conditions may in-clude extreme prematurity and anom-alies that predict extrememorbidity or
early death. Treatment and outcome ofinfants at the margins of viability maybe influenced by factors in addition togestational age and birthweight.153
Noninitiation of resuscitation andwith-drawal of cardiorespiratory supportare ethically equivalent.154
Treatment RecommendationWhen gestation, birth weight, or congen-ital anomalies are associated with al-most certain early death and an unac-ceptably high morbidity is likely amongthe rare survivors, resuscitation is notindicated. In conditions associated witha high rate of survival and acceptablemorbidity, resuscitation is nearly alwaysindicated. In conditions associated withuncertain prognosis, when there is bor-derline survival anda relatively high rateof morbidity and when the burden to thechild is high, theparents’ viewsonresus-citation should be supported. Thereshould be a consistent and coordinatedapproach from the obstetric and neona-tal teams in applying these guidelinesand in communicating with the parentsin developing an agreed-upon manage-ment plan when possible. Once resusci-tation is initiated it may be appropriateto subsequently decide to discontinuecardiorespiratory support and offercomfort care.
Discontinuation of Resuscitation
Consensus on ScienceAvailable evidence, albeit from relativelysmall numbers of babies, suggests thatbabiesbornwithoutaheart rate thathasnot returned by 10 minutes of age arelikely to either die or have severe neuro-logic disability (LOE 4155,156). It is notknownwhether therewas significant se-lection bias inmany of these studies, norindeed that the babies included in thesestudies did receive “good-quality resus-citation.” One study with a large contem-porary cohort of infants (some random-ized to postresuscitation hypothermia)indicates that in babies born without adetectable heart rate, the lack of ROSC
after 10 minutes of age is associatedwith survival without severe neurologicdeficit in a small numberof the survivors(LOE 4157). Data are not available regard-ing the number of infants who weredeemed too sick for study entry or whodied before enrollment. These factorsmay have resulted in a significant over-estimation of the rate of intact survivalamong infants with an Apgar score of 0at 10 minutes. In all reported series thecause of the asphyxia and the efficacy ofthe resuscitation process were notelucidated.
The evidence from 7 LOE 5 studies157,158
is insufficient to support or refute anyrecommendation regarding howmuchtime should elapse with a heart rate of�60 but �0 beats per minute beforediscontinuing resuscitative efforts.
Treatment RecommendationIn a newly born baby with no detectableheart rate which remains undetectablefor 10 minutes, it is appropriate to thenconsider stopping resuscitation. The de-cision to continue resuscitation effortswhen the infant has a heart rate of 0 forlonger than 10 minutes is often complexandmay be influenced by issues such asthe presumed etiology of the arrest, ges-tation of the baby, potential reversibilityof the situation, and the parents’ previ-ously expressed feelings about accept-able risk of morbidity.
The evidence of outcomewhen the heartrate is �60 beats per minute at birthand persists after 10 or 15 minutes ofcontinuous and adequate resuscitative ef-forts at delivery is insufficient to guide de-cisionsas towhether towithholdor tocon-tinue resuscitation.
Personnel Needs at ElectiveCesarean SectionsNRP-010A, NRP-010B,NRP-010C
Consensus on ScienceRetrospective studies show that deliveryby cesarean section at term under re-gional anesthesia is associated with a
FROM THE AMERICAN ACADEMY OF PEDIATRICS
PEDIATRICS Volume 126, Number 5, November 2010 e1329. Provided by Health Internetwork on December 13, 2010 www.pediatrics.orgDownloaded from

small increase in risk of receiving as-sisted ventilation during neonatal resus-citation compared with unassisted vagi-nal birth. The number needed to treatequals 35 (LOE 4159,160). Five retrospectivestudies showed that delivery by cesar-ean section at termunder regional anes-thesia did not increase the risk ofrequirement for intubation during neo-natal resuscitation comparedwith unas-sisted vaginal birth (LOE 4161,162). There isno evidence addressing this question inbabies born at 34 to 36weeks’ gestation.
Treatment RecommendationsWhen an infant without antenatally iden-tified risk factors is delivered at term bycesarean section under regional anes-thesia, a provider capable of performingassisted ventilation should be present atthe delivery. It is not necessary for a pro-vider skilled in neonatal intubation to bepresent at that delivery.
EDUCATIONAL TECHNIQUES FORTEACHING, ASSESSING, ANDMAINTAINING RESUSCITATIONKNOWLEDGE AND SKILLS
SimulationNRP-032A, NRP-032B, NRP-032C, EIT-019A, EIT-019B
Consensus on ScienceThere is a lack of uniformity in the def-inition of simulation as a learning
methodology, determination of rele-vant outcomes, and use of appropriatemeasurement tools. Use of simulationas an adjunct to traditional educationmethodologies may enhance perfor-mance of healthcare professionals inactual clinical settings (LOE 1163; LOE3164) and simulated resuscitations (LOE1165; LOE 2166). Some studies did notshow any difference in performancebetween standard training and simu-lation training in a clinical setting (LOE1167) or using other means of evalua-tion (LOE 1168). No studies were foundthat revealed simulation-based train-ing produced inferior results com-pared with traditional methodologies.
Treatment RecommendationsSimulation should be used as a meth-odology in resuscitation education.The most effective interventions andevaluation methodologies remain tobe defined.
Briefings andDebriefingsNRP-033A, NRP-033B, EIT-001A, EIT-001B
Consensus on ScienceEvidence from 1 prospective random-ized controlled study (LOE 1169) and 17other studies (LOE 3 to 4) of briefingsand debriefings document improve-ment in the acquisition of content
knowledge, technical skills, or behav-ioral skills required for effective andsafe resuscitation. Only a single study(LOE 4170) revealed no effect of brief-ing/debriefing on performance, and nostudies indicated that the use of brief-ings and debriefings had any negativeeffects.
Treatment RecommendationsIt is reasonable to recommend the useof briefings and debriefings duringlearning activities while caring forsimulated patients and during clinicalactivities.
ACKNOWLEDGMENTSWe thank the following individuals (theNeonatal Resuscitation Chapter Col-laborators) for their collaborations onthe worksheets contained in this sec-tion: Khalid Aziz; David Boyle; StevenByrne; Peter Davis; William A. Engle;Marilyn B. Escobedo; Maria Fernandade Almeida; David Field; Judith Finn;Louis P. Halamek; Jane E. McGowan;Douglas D. McMillan; Lindsay Milden-hall; Rintaro Mori; Susan Niermeyer;Colm O’Donnell; Yacov Rabi; Steven A.Ringer; Jasmeet Soar; Benjamin J.Stenson; Enrique Udaeta; DharmapuriVidyasagar; Michael Watkinson; GaryM. Weiner; and Myra H. Wyckoff.
REFERENCES
1. Perlman JM, Risser R. Cardiopulmonaryresuscitation in the delivery room: associ-ated clinical events. Arch Pediatr AdolescMed. 1995;149:20–25
2. Barber CA, Wyckoff MH. Use and efficacy ofendotracheal versus intravenous epi-nephrine during neonatal cardiopulmo-nary resuscitation in the delivery room.Pediatrics. 2006;118:1028–1034
3. 2005 International Consensus on Cardio-pulmonary Resuscitation and EmergencyCardiovascular Care Science With Treat-ment Recommendations. Part 7: NeonatalResuscitation. Resuscitation. 2005;67:293–303
4. 2005 International Consensus on Cardio-pulmonary Resuscitation and EmergencyCardiovascular Care Science With Treat-ment Recommendations. Part 7: Neonatal
Resuscitation. Circulation. 2005;112:III-91–III-99
5. Dawes GS. Foetal and neonatal physiology.Chicago, IL: Year Book Medical Publishers;1968:149
6. Owen CJ, Wyllie JP. Determination of heartrate in the baby at birth. Resuscitation.2004;60:213–217
7. Kamlin CO, Dawson JA, O’Donnell CP,Morley CJ, Donath SM, Sekhon J, DavisPG. Accuracy of pulse oximetry mea-surement of heart rate of newborn in-fants in the delivery room. J Pediatr.2008;152:756 –760
8. Dawson JA, Kamlin CO, Wong C, Te Pas AB,O’Donnell CP, Donath SM, Davis PG, MorleyCJ. Oxygen saturation and heart rate dur-ing delivery room resuscitation of infants�30 weeks’ gestation with air or 100% ox-
ygen. Arch Dis Child Fetal Neonatal Ed.2009;94:F87–F91
9. Altuncu E, Ozek E, Bilgen H, Topuzoglu A,Kavuncuoglu S. Percentiles of oxygen sat-urations in healthy term newborns in thefirst minutes of life. Eur J Pediatr. 2008;167:687–688
10. O’Donnell CP, Kamlin CO, Davis PG, MorleyCJ. Obtaining pulse oximetry data inneonates: a randomised crossover studyof sensor application techniques. Arch DisChild Fetal Neonatal Ed. 2005;90:F84–F85
11. Wang CL, Anderson C, Leone TA, Rich W,Govindaswami B, Finer NN. Resuscitationof preterm neonates by using room air or100% oxygen. Pediatrics . 2008;121:1083–1089
12. Vento M, Asensi M, Sastre J, Garcia-Sala F,Pallardo FV, Vina J. Resuscitation with
e1330 FROM THE AMERICAN ACADEMY OF PEDIATRICS. Provided by Health Internetwork on December 13, 2010 www.pediatrics.orgDownloaded from

room air instead of 100% oxygen preventsoxidative stress in moderately asphyxi-ated term neonates. Pediatrics. 2001;107:642–647
13. Saugstad OD, Rootwelt T, Aalen O. Resusci-tation of asphyxiated newborn infantswith room air or oxygen: an internationalcontrolled trial: the RESAIR 2 study. Pediat-rics. 1998;102:e1
14. Davis PG, Tan A, O’Donnell CP, Schulze A.Resuscitation of newborn infants with100% oxygen or air: a systematic reviewand meta-analysis. Lancet. 2004;364:1329–1333
15. Rabi Y, Rabi D, Yee W. Room air resuscita-tion of the depressed newborn: a system-atic review and meta-analysis. Resuscita-tion. 2007;72:353–363
16. Lakshminrusimha S, Russell JA, SteinhornRH, Swartz DD, Ryan RM, Gugino SF, WynnKA, Kumar VH, Mathew B, Kirmani K, MorinFC III. Pulmonary hemodynamics in neona-tal lambs resuscitated with 21%, 50%, and100% oxygen. Pediatr Res. 2007;62:313–318
17. Solberg R, Andresen JH, Escrig R, Vento M,Saugstad OD. Resuscitation of hypoxicnewborn piglets with oxygen induces adose-dependent increase in markers ofoxidation. Pediatr Res. 2007;62:559–563
18. Solas AB, Kutzsche S, VinjeM, Saugstad OD.Cerebral hypoxemia-ischemia and reoxy-genation with 21% or 100% oxygen in new-born piglets: effects on extracellular levelsof excitatory amino acids and microcircu-lation. Pediatr Crit Care Med. 2001;2:340–345
19. Presti AL, Kishkurno SV, Slinko SK, RandisTM, Ratner VI, Polin RA, Ten VS. Reoxygen-ation with 100% oxygen versus room air:late neuroanatomical and neurofunc-tional outcome in neonatal mice withhypoxic-ischemic brain injury. Pediatr Res.2006;60:55–59
20. Escrig R, Arruza L, Izquierdo I, Villar G,Saenz P, Gimeno A, Moro M, Vento M.Achievement of targeted saturation valuesin extremely low gestational age neonatesresuscitated with low or high oxygenconcentrations: a prospective, random-ized trial. Pediatrics. 2008;121:875–881
21. Gungor S, Kurt E, Teksoz E, Goktolga U, Cey-han T, Baser I. Oronasopharyngeal suctionversus no suction in normal and term in-fants delivered by elective cesareansection: a prospective randomized con-trolled trial. Gynecol Obstet Invest. 2006;61:9–14
22. Waltman PA, Brewer JM, Rogers BP, MayWL. Building evidence for practice: a pilotstudy of newborn bulb suctioning at birth.
J Midwifery Womens Health. 2004;49:32–38
23. Simbruner G, Coradello H, Fodor M, Hav-elec L, Lubec G, Pollak A. Effect of trachealsuction on oxygenation, circulation, andlung mechanics in newborn infants. ArchDis Child. 1981;56:326–330
24. Usta IM, Mercer BM, Sibai BM. Risk factorsfor meconium aspiration syndrome. Ob-stet Gynecol. 1995;86:230–234
25. Rossi EM, Philipson EH, Williams TG, KalhanSC. Meconium aspiration syndrome: intra-partum and neonatal attributes. Am J Ob-stet Gynecol. 1989;161:1106–1110
26. Al Takroni AM, Parvathi CK, Mendis KB, Has-san S, Reddy I, Kudair HA. Selective tra-cheal suctioning to prevent meconium as-piration syndrome. Int J Gynaecol Obstet.1998;63:259–263
27. Gupta V, Bhatia BD, Mishra OP. Meconiumstained amniotic fluid: antenatal, intrapar-tum and neonatal attributes. Indian Pedi-atr. 1996;33:293–297
28. Vyas H, Milner AD, Hopkin IE, Boon AW.Physiologic responses to prolonged andslow-rise inflation in the resuscitation ofthe asphyxiated newborn infant. J Pediatr.1981;99:635–639
29. Te Pas AB, Walther FJ. A randomized, con-trolled trial of delivery-room respiratorymanagement in very preterm infants. Pe-diatrics. 2007;120:322–329
30. Lindner W, Hogel J, Pohlandt F. Sustainedpressure-controlled inflation or intermit-tent mandatory ventilation in preterm in-fants in the delivery room? A randomized,controlled trial on initial respiratory sup-port via nasopharyngeal tube. Acta Paedi-atr. 2005;94:303–309
31. Harling AE, Beresford MW, Vince GS, BatesM, Yoxall CW. Does sustained lung inflationat resuscitation reduce lung injury in thepreterm infant? Arch Dis Child Fetal Neo-natal Ed. 2005;90:F406–F410
32. Boon AW, Milner AD, Hopkin IE. Lung expan-sion, tidal exchange, and formation of thefunctional residual capacity during resus-citation of asphyxiated neonates. J Pedi-atr. 1979;95:1031–1036
33. Lindner W, Vossbeck S, Hummler H,Pohlandt F. Delivery room management ofextremely low birth weight infants: spon-taneous breathing or intubation? Pediat-rics. 1999;103:961–967
34. Upton CJ, Milner AD. Endotracheal resus-citation of neonates using a rebreathingbag. Arch Dis Child. 1991;66:39–42
35. Hillman NH, Moss TJ, Kallapur SG, Bachur-ski C, Pillow JJ, Polglase GR, Nitsos I,Kramer BW, Jobe AH. Brief, large tidal vol-
ume ventilation initiates lung injury and asystemic response in fetal sheep. Am J Re-spir Crit Care Med. 2007;176:575–581
36. Finer NN, Carlo WA, Duara S, Fanaroff AA,Donovan EF, Wright LL, Kandefer S, PooleWK. Delivery room continuous positive air-way pressure/positive end-expiratorypressure in extremely low birth weightinfants: a feasibility trial. Pediatrics. 2004;114:651–657
37. Siew ML, Te Pas AB, Wallace MJ, KitchenMJ, Lewis RA, Fouras A, Morley CJ, DavisPG, Yagi N, Uesugi K, Hooper SB. Positiveend-expiratory pressure enhances devel-opment of a functional residual capacity inpreterm rabbits ventilated from birth.J Appl Physiol. 2009;106:1487–1493
38. Te Pas AB, Siew M, Wallace MJ, Kitchen MJ,Fouras A, Lewis RA, Yagi N, Uesugi K, Do-nath S, Davis PG, Morley CJ, Hooper SB.Establishing functional residual capacityat birth: the effect of sustained inflationand positive end-expiratory pressure in apreterm rabbit model. Pediatr Res. 2009;65:537–541
39. Polglase GR, Hooper SB, Gill AW, Allison BJ,McLean CJ, Nitsos I, Pillow JJ, Kluckow M.Cardiovascular and pulmonary conse-quences of airway recruitment in pretermlambs. J Appl Physiol. 2009;106:1347–1355
40. Probyn ME, Hooper SB, Dargaville PA, Mc-Callion N, Crossley K, Harding R, Morley CJ.Positive end expiratory pressure duringresuscitation of premature lambs rapidlyimproves blood gases without adverselyaffecting arterial pressure. Pediatr Res.2004;56:198–204
41. Morley CJ, Davis PG, Doyle LW, Brion LP,Hascoet JM, Carlin JB. Nasal CPAP or intu-bation at birth for very preterm infants.N Engl J Med. 2008;358:700–708
42. Oddie S, Wyllie J, Scally A. Use of self-inflating bags for neonatal resuscitation.Resuscitation. 2005;67:109–112
43. Hussey SG, Ryan CA, Murphy BP. Compari-son of threemanual ventilation devices us-ing an intubated mannequin. Arch Dis ChildFetal Neonatal Ed. 2004;89:F490–F493
44. Finer NN, Rich W, Craft A, Henderson C.Comparison of methods of bag and maskventilation for neonatal resuscitation. Re-suscitation. 2001;49:299–305
45. Bennett S, Finer NN, Rich W, Vaucher Y. Acomparison of three neonatal resuscita-tion devices. Resuscitation. 2005;67:113–118
46. Singh R. Controlled trial to evaluate theuse of LMA for neonatal resuscitation.J Anaesth Clin Pharmacol . 2005;21:303–306
47. Trevisanuto D, Micaglio M, Pitton M, Maga-
FROM THE AMERICAN ACADEMY OF PEDIATRICS
PEDIATRICS Volume 126, Number 5, November 2010 e1331. Provided by Health Internetwork on December 13, 2010 www.pediatrics.orgDownloaded from

rotto M, Piva D, Zanardo V. Laryngeal maskairway: is themanagement of neonates re-quiring positive pressure ventilation atbirth changing? Resuscitation. 2004;62:151–157
48. Gandini D, Brimacombe JR. Neonatal re-suscitation with the laryngeal mask air-way in normal and low birth weight in-fants. Anesth Analg. 1999;89:642–643
49. Esmail N, Saleh M, et al. Laryngeal maskairway versus endotracheal intubation forApgar score improvement in neonatal re-suscitation. Egypt J Anesthesiol. 2002;18:115–121
50. Zanardo V, Simbi AK, Savio V, Micaglio M,Trevisanuto D. Neonatal resuscitation bylaryngeal mask airway after elective ce-sarean section. Fetal Diagn Ther. 2004;19:228–231
51. Palme C, NystromB, Tunell R. An evaluationof the efficiency of face masks in the re-suscitation of newborn infants. Lancet.1985;1:207–210
52. O’Donnell CP, Davis PG, Lau R, DargavillePA, Doyle LW, Morley CJ. Neonatal resusci-tation 2: an evaluation of manual ventila-tion devices and face masks. Arch Dis ChildFetal Neonatal Ed. 2005;90:F392–F396
53. Capasso L, Capasso A, Raimondi F, Ven-demmia M, Araimo G, Paludetto R. A ran-domized trial comparing oxygen deliveryon intermittent positive pressure with na-sal cannulae versus facial mask in neona-tal primary resuscitation. Acta Paediatr.2005;94:197–200
54. Wood FE, Morley CJ, Dawson JA, Kamlin CO,Owen LS, Donath S, Davis PG. Assessing theeffectiveness of two round neonatal resus-citation masks: study 1. Arch Dis Child Fe-tal Neonatal Ed. 2008;93:F235–F237
55. Bang AT, Bang RA, Baitule SB, Reddy HM,Deshmukh MD. Management of birth as-phyxia in home deliveries in ruralGadchiroli: the effect of two types of birthattendants and of resuscitating withmouth-to-mouth, tube-mask or bag-mask.J Perinatol. 2005;25 suppl 1:S82–S91
56. Massawe A, Kilewo C, Irani S, Verma RJ,Chakrapam AB, Ribbe T, Tunell R, FischlerB. Assessment of mouth-to-mask ventila-tion in resuscitation of asphyxic newbornbabies. A pilot study. Trop Med Int Health.1996;1:865–873
57. Roberts RB, Day RL. Mouth-to-tube resusci-tation of the neonate, II: the transmissionof bacteria through endotracheal tubesand its prevention. Anesth Analg. 1973;52:242–245
58. Milner AD, Stokes GM, Tunell R, McKeughM, Martin H. Laboratory assessment of
Laerdal mouth tube mask prototype re-suscitation device. Med Biol Eng Comput.1992;30:117–119
59. Terndrup TE, Kanter RK, Cherry RA. A com-parison of infant ventilation methods per-formed by prehospital personnel. AnnEmerg Med. 1989;18:607–611
60. Coffey PS, Kelly K, Tsu V. Preferences andpractices: use of neonatal resuscitationdevices in low-resource settings. J TropPediatr. 2007;53:415–419
61. Polglase GR, Hillman NH, Pillow JJ, CheahFC, Nitsos I, Moss TJ, Kramer BW, IkegamiM, Kallapur SG, Jobe AH. Positive end-expiratory pressure and tidal volume dur-ing initial ventilation of preterm lambs. Pe-diatr Res. 2008;64:517–522
62. Probyn ME, Hooper SB, Dargaville PA, Mc-Callion N, Harding R, Morley CJ. Effects oftidal volume and positive end-expiratorypressure during resuscitation of very pre-mature lambs. Acta Paediatr. 2005;94:1764–1770
63. Kattwinkel J, Stewart C, Walsh B, Gurka M,Paget-Brown A. Responding to compliancechanges in a lung model during manualventilation: perhaps volume, rather thanpressure, should be displayed. Pediatrics.2009;123:e465–e470
64. Resende JG, Zaconeta CA, Ferreira AC,Silva CA, Rodrigues MP, Rebello CM, Ta-vares P. Evaluation of peak inspiratorypressure, tidal volume and respiratoryrate during ventilation of prematurelambs using a self-inflating bag. J Pediatr(Rio J). 2006;82:279–283
65. Wood FE, Morley CJ, Dawson JA, Kamlin CO,Owen LS, Donath S, Davis PG. Improvedtechniques reduce face mask leak duringsimulated neonatal resuscitation: study 2.Arch Dis Child Fetal Neonatal Ed. 2008;93:F230–F234
66. Hosono S, Inami I, Fujita H, Minato M, Taka-hashi S, Mugishima H. A role of end-tidalCO(2) monitoring for assessment of tra-cheal intubations in very low birth weightinfants during neonatal resuscitation atbirth. J Perinat Med. 2009;37:79–84
67. Repetto JE, Donohue P-CP, Baker SF, Kelly L,Nogee LM. Use of capnography in the deliv-ery room for assessment of endotrachealtube placement. J Perinatol. 2001;21:284–287
68. Roberts WA, Maniscalco WM, Cohen AR, Lit-man RS, Chhibber A. The use of capnogra-phy for recognition of esophageal intuba-tion in the neonatal intensive care unit.Pediatr Pulmonol. 1995;19:262–268
69. Aziz HF, Martin JB, Moore JJ. The pediat-ric disposable end-tidal carbon dioxide
detector role in endotracheal intubationin newborns. J Perinatol. 1999;19:110–113
70. Garey DM, Ward R, Rich W, Heldt G, Leone T,Finer NN. Tidal volume threshold for color-imetric carbon dioxide detectors availablefor use in neonates. Pediatrics. 2008;121:e1524–e1527
71. Hughes SM, Blake BL, Woods SL, LehmannCU. False-positive results on colorimetriccarbon dioxide analysis in neonatalresuscitation: potential for serious patientharm. J Perinatol. 2007;27:800–801
72. Leone TA, Lange A, RichW, Finer NN. Dispos-able colorimetric carbon dioxide detectoruse as an indicator of a patent airway dur-ing noninvasive mask ventilation. Pediat-rics. 2006;118:e202–e204
73. Finer NN, Rich W, Wang C, Leone T. Airwayobstruction during mask ventilation ofvery low birth weight infants during neo-natal resuscitation. Pediatrics. 2009;123:865–869
74. Berg RA, Hilwig RW, Kern KB, Babar I, EwyGA. Simulated mouth-to-mouth ventilationand chest compressions (bystander car-diopulmonary resuscitation) improvesoutcome in a swine model of prehospitalpediatric asphyxial cardiac arrest. CritCare Med. 1999;27:1893–1899
75. Berg RA, Hilwig RW, Kern KB, Ewy GA. “By-stander” chest compressions and as-sisted ventilation independently improveoutcome from piglet asphyxial pulseless“cardiac arrest.” Circulation. 2000;101:1743–1748
76. Dean JM, Koehler RC, Schleien CL, AtchisonD, Gervais H, Berkowitz I, Traystman RJ.Improved blood flow during prolongedcardiopulmonary resuscitation with 30%duty cycle in infant pigs. Circulation. 1991;84:896–904
77. Babbs CF, Nadkarni V. Optimizing chestcompression to rescue ventilation ratiosduring one-rescuer CPR by professionalsand lay persons: children are not just littleadults. Resuscitation. 2004;61:173–181
78. Srikantan SK, Berg RA, Cox T, Tice L, Nad-karni VM. Effect of one-rescuer compression/ventilation ratios on cardiopulmonary re-suscitation in infant, pediatric, and adultmanikins. Pediatr Crit Care Med. 2005;6:293–297
79. Whyte SD, Sinha AK, Wyllie JP. Neonatalresuscitation–a practical assessment. Re-suscitation. 1999;40:21–25
80. Greingor JL. Quality of cardiac massagewith ratio compression-ventilation 5/1and 15/2. Resuscitation. 2002;55:263–267
81. Wik L, Steen PA. The ventilation/compressionratio influences the effectiveness of two res-
e1332 FROM THE AMERICAN ACADEMY OF PEDIATRICS. Provided by Health Internetwork on December 13, 2010 www.pediatrics.orgDownloaded from

cuer advanced cardiac life support on amanikin. Resuscitation. 1996;31:113–119
82. Dorph E, Wik L, Steen PA. Effectiveness ofventilation-compression ratios 1:5 and2:15 in simulated single rescuer paediat-ric resuscitation. Resuscitation. 2002;54:259–264
83. Kinney SB, Tibballs J. An analysis of the effi-cacy of bag-valve-mask ventilation and chestcompression during different compression-ventilation ratios in manikin-simulated pae-diatric resuscitation. Resuscitation. 2000;43:115–120
84. Haque IU, Udassi JP, Udassi S, Theriaque DW,Shuster JJ, Zaritsky AL. Chest compressionquality and rescuer fatigue with increasedcompression to ventilation ratio during sin-gle rescuer pediatric CPR. Resuscitation.2008;79:82–89
85. Kitamura T, Iwami T, Kawamura T, Nagao K,Tanaka H, Nadkarni VM, Berg RA, Hiraide A.Conventional and chest-compression-onlycardiopulmonary resuscitation by by-standers for children who have out-of-hospital cardiac arrests: a prospective,nationwide, population-based cohortstudy. Lancet. 2010;375:1347–1354
86. Houri PK, Frank LR, Menegazzi JJ, Taylor R.A randomized, controlled trial of two-thumb vs two-finger chest compression ina swine infant model of cardiac arrest.Prehosp Emerg Care. 1997;1:65–67
87. Menegazzi JJ, Auble TE, Nicklas KA, HosackGM, Rack L, Goode JS. Two-thumb versustwo-finger chest compression during CPRin a swine infant model of cardiac arrest.Ann Emerg Med. 1993;22:240–243
88. Udassi JP, Udassi S, Theriaque DW, Shus-ter JJ, Zaritsky AL, Haque IU. Effect of alter-native chest compression techniques ininfant and child on rescuer performance.Pediatr Crit Care Med. 2009;10:328–333
89. DavidR. Closedchest cardiacmassage in thenewborn infant. Pediatrics. 1988;81:552–554
90. Thaler MM, Stobie GH. An improved tech-nique of external caridac compression ininfants and young children. N Engl J Med.1963;269:606–610
91. Whitelaw CC, Slywka B, Goldsmith LJ. Com-parison of a two-finger versus two-thumbmethod for chest compressions by health-care providers in an infant mechanicalmodel. Resuscitation. 2000;43:213–216
92. Moya F, James LS, Burnard ED, Hanks EC.Cardiac massage in the newborn infantthrough the intact chest. Am J Obstet Gy-necol. 1962;84:798–803
93. Orlowski JP. Optimum position for exter-nal cardiac compression in infants and
young children. Ann Emerg Med. 1986;15:667–673
94. Phillips GW, Zideman DA. Relation of infantheart to sternum: its significance in car-diopulmonary resuscitation. Lancet. 1986;1:1024–1025
95. Braga MS, Dominguez TE, Pollock AN, NilesD, Meyer A, Myklebust H, Nysaether J, Nad-karni V. Estimation of optimal CPR chestcompression depth in children by usingcomputer tomography. Pediatrics. 2009;124:e69–e74
96. Jankov RP, Asztalos EV, Skidmore MB.Favourable neurological outcomes follow-ing delivery room cardiopulmonary resus-citation of infants � or �750 g at birth.J Paediatr Child Health. 2000;36:19–22
97. O’Donnell AI, Gray PH, Rogers YM. Mortalityand neurodevelopmental outcome for in-fants receiving adrenaline in neonatalresuscitation. J Paediatr Child Health.1998;34:551–556
98. Crespo SG, Schoffstall JM, Fuhs LR, SpiveyWH. Comparison of two doses of endotra-cheal epinephrine in a cardiac arrestmodel. Ann Emerg Med. 1991;20:230–234
99. Jasani MS, Nadkarni VM, Finkelstein MS,Mandell GA, Salzman SK, Norman ME. Ef-fects of different techniques of endo-tracheal epinephrine administration inpediatric porcine hypoxic-hypercarbiccardiopulmonary arrest. Crit Care Med.1994;22:1174–1180
100. Mielke LL, Frank C, Lanzinger MJ, WilhelmMG, Entholzner EK, Hargasser SR, Hipp RF.Plasma catecholamine levels followingtracheal and intravenous epinephrine ad-ministration in swine. Resuscitation. 1998;36:187–192
101. Roberts JR, Greenberg MI, Knaub MA, Ken-drick ZV, Baskin SI. Blood levels followingintravenous and endotracheal epineph-rine administration. JACEP. 1979;8:53–56
102. Hornchen U, Schuttler J, Stoeckel H, Eich-elkraut W, Hahn N. Endobronchial instilla-tion of epinephrine during cardiopulmo-nary resuscitation. Crit Care Med. 1987;15:1037–1039
103. Guay J, Lortie L. An evaluation of pediatricin-hospital advanced life support interven-tionsusing thepediatric utstein guidelines: areview of 203 cardiorespiratory arrests. CanJ Anaesth. 2004;51:373–378
104. Perondi MB, Reis AG, Paiva EF, NadkarniVM, Berg RA. A comparison of high-doseand standard-dose epinephrine in chil-dren with cardiac arrest. N Engl J Med.2004;350:1722–1730
105. PattersonMD, Boenning DA, Klein BL, FuchsS, Smith KM, Hegenbarth MA, Carlson DW,
Krug SE, Harris EM. The use of high-doseepinephrine for patients with out-of-hospital cardiopulmonary arrest refrac-tory to prehospital interventions. PediatrEmerg Care. 2005;21:227–237
106. Goetting MG, Paradis NA. High-dose epi-nephrine improves outcome from pediat-ric cardiac arrest. Ann Emerg Med. 1991;20:22–26
107. Vandycke C, Martens P. High dose versusstandard dose epinephrine in cardiac ar-rest—a meta-analysis. Resuscitation. 2000;45:161–166
108. Berg RA, Otto CW, Kern KB, Hilwig RW, Sand-ers AB, Henry CP, Ewy GA. A randomized,blinded trial of high-dose epinephrine ver-sus standard-dose epinephrine in a swinemodel of pediatric asphyxial cardiac ar-rest. Crit Care Med. 1996;24:1695–1700
109. Burchfield DJ, Preziosi MP, Lucas VW, FanJ. Effects of graded doses of epinephrineduring asphxia-induced bradycardia innewborn lambs. Resuscitation. 1993;25:235–244
110. Kirkman HN, Riley HD Jr. Posthemor-rhagic anemia and shock in the newborndue tohemorrhageduringdelivery: report of8 cases. Pediatrics. 1959;24:92–96
111. Wyckoff MH, Perlman JM, Laptook AR.Use of volume expansion during deliveryroom resuscitation in near-term and terminfants. Pediatrics. 2005;115:950–955
112. Wyckoff M, Garcia D, Margraf L, Perlman J,Laptook A. Randomized trial of volume in-fusion during resuscitation of asphyxiatedneonatal piglets. Pediatr Res. 2007;61:415–420
113. Mayock DE, Gleason CA. Cerebrovasculareffects of rapid volume expansion in pre-term fetal sheep. Pediatr Res. 2004;55:395–399
114. Box D, Cochran D. Safe reduction in admin-istration of naloxone to newborn infants:an observational study. Acta Paediatr.2006;95:1083–1086
115. Bonta BW, Gagliardi JV, Williams V, War-shaw JB. Naloxone reversal of mild neu-robehavioral depression in normal new-born infants after routine obstetricanalgesia. J Pediatr. 1979;94:102–105
116. Gill AW, Colvin J. Use of naloxone duringneonatal resuscitation in australia: com-pliance with published guidelines. J Paedi-atr Child Health. 2007;43:795–798
117. Gibbs J, Newson T, Williams J, Davidson DC.Naloxone hazard in infant of opioid abuser.Lancet. 1989;2:159–160
118. Van Woerkom R, Beharry KD, Modanlou HD,Parker J, Rajan V, Akmal Y, Aranda JV. In-fluence of morphine and naloxone on en-
FROM THE AMERICAN ACADEMY OF PEDIATRICS
PEDIATRICS Volume 126, Number 5, November 2010 e1333. Provided by Health Internetwork on December 13, 2010 www.pediatrics.orgDownloaded from

dothelin and its receptors in newborn pig-let brain vascular endothelial cells: clinicalimplications in neonatal care. Pediatr Res.2004;55:147–151
119. Ellemunter H, Simma B, Trawoger R, Mau-rer H. Intraosseous lines in preterm andfull term neonates. Arch Dis Child FetalNeonatal Ed. 1999;80:F74–F75
120. Glaeser PW, Hellmich TR, Szewczuga D,Losek JD, Smith DS. Five-year experience inprehospital intraosseous infusions in chil-dren and adults. Ann Emerg Med. 1993;22:1119–1124
121. Cramer K, Wiebe N, Hartling L, Crumley E,Vohra S. Heat loss prevention: a system-atic review of occlusive skin wrap for pre-mature neonates. J Perinatol. 2005;25:763–769
122. Vohra S, Roberts RS, Zhang B, Janes M,Schmidt B. Heat loss prevention (help) inthe delivery room: a randomized con-trolled trial of polyethylene occlusive skinwrapping in very preterm infants. J Pedi-atr. 2004;145:750–753
123. Almeida PG, Chandley J, Davis J, HarriganRC. Use of the heated gel mattress and itsimpact on admission temperature of verylow birth-weight infants. Adv NeonatalCare. 2009;9:34–39
124. Singh A, Duckett J, Newton T, Watkinson M.Improving neonatal unit admission tem-peratures in preterm babies: exothermicmattresses, polythene bags or a tradi-tional approach? J Perinatol. 2010;30:45–49
125. Knobel RB, Wimmer JE Jr, Holbert D. Heatloss prevention for preterm infants in thedelivery room. J Perinatol. 2005;25:304–308
126. Kent AL, Williams J. Increasing ambient op-erating theatre temperature and wrap-ping in polyethylene improves admissiontemperature in premature infants. J Pae-diatr Child Health. 2008;44:325–331
127. Petrova A, Demissie K, Rhoads GG, SmulianJC, Marcella S, Ananth CV. Association ofmaternal fever during labor with neonataland infant morbidity and mortality. ObstetGynecol. 2001;98:20–27
128. Lieberman E, Eichenwald E, Mathur G, Rich-ardson D, Heffner L, Cohen A. Intrapartumfever and unexplained seizures in term in-fants. Pediatrics. 2000;106:983–988
129. Shalak LF, Perlman JM, Jackson GL, LaptookAR. Depression at birth in term infants ex-posed to maternal chorioamnionitis: doesneonatal fever play a role? J Perinatol. 2005;25:447–452
130. Coimbra C, Boris-Moller F, Drake M, Wie-loch T. Diminished neuronal damage in therat brain by late treatment with the antipy-
retic drug dipyrone or cooling followingcerebral ischemia. Acta Neuropathol.1996;92:447–453
131. Goetzl L, Zighelboim I, Badell M, Rivers J,Mastrangelo MA, Tweardy D, Suresh MS.Maternal corticosteroids to prevent intra-uterine exposure to hyperthermia andinflammation: a randomized, double-blind,placebo-controlled trial. Am J Obstet Gy-necol. 2006;195:1031–1037
132. Gluckman PD, Wyatt JS, Azzopardi D, Bal-lard R, Edwards AD, Ferriero DM, Polin RA,Robertson CM, Thoresen M, Whitelaw A,Gunn AJ. Selective head cooling with mildsystemic hypothermia after neonatalencephalopathy: multicentre randomisedtrial. Lancet. 2005;365:663–670
133. Shankaran S, Laptook AR, Ehrenkranz RA,Tyson JE, McDonald SA, Donovan EF, Fan-aroff AA, Poole WK, Wright LL, Higgins RD,Finer NN, Carlo WA, Duara S, Oh W, CottenCM, Stevenson DK, Stoll BJ, Lemons JA,Guillet R, Jobe AH. Whole-body hypother-mia for neonates with hypoxic-ischemicencephalopathy. N Engl J Med. 2005;353:1574–1584
134. Azzopardi DV, Strohm B, Edwards AD, DyetL, Halliday HL, Juszczak E, Kapellou O, Lev-ene M, Marlow N, Porter E, Thoresen M,Whitelaw A, Brocklehurst P. Moderate hy-pothermia to treat perinatal asphyxial en-cephalopathy. N Engl J Med. 2009;361:1349–1358
135. Eicher DJ, Wagner CL, Katikaneni LP, HulseyTC, Bass WT, Kaufman DA, Horgan MJ, Lan-guani S, Bhatia JJ, Givelichian LM, Sanka-ran K, Yager JY. Moderate hypothermia inneonatal encephalopathy: efficacy out-comes. Pediatr Neurol. 2005;32:11–17
136. Lin ZL, Yu HM, Lin J, Chen SQ, Liang ZQ,Zhang ZY. Mild hypothermia via selectivehead cooling as neuroprotective therapyin term neonates with perinatal asphyxia:an experience from a single neonatal in-tensive care unit. J Perinatol. 2006;26:180–184
137. Edwards AD, Brocklehurst P, Gunn AJ, Hal-liday H, Juszczak E, Levene M, Strohm B,Thoresen M, Whitelaw A, Azzopardi D. Neu-rological outcomes at 18 months of ageafter moderate hypothermia for perinatalhypoxic ischaemic encephalopathy: syn-thesis andmeta-analysis of trial data. BMJ.2010;340:c363
138. Jacobs S, Hunt R, Tarnow-Mordi W, Inder T,Davis P. Cooling for newborns with hypoxicischaemic encephalopathy. Cochrane Da-tabase Syst Rev. 2007:CD003311
139. SalhabWA,WyckoffMH, Laptook AR, PerlmanJM. Initial hypoglycemia and neonatal brain
injury in term infants with severe fetal aci-demia. Pediatrics. 2004;114:361–366
140. Ondoa-Onama C, Tumwine JK. Immediateoutcome of babies with low Apgar score inMulago hospital, Uganda. East Afr Med J.2003;80:22–29
141. Klein GW, Hojsak JM, Schmeidler J, Rapa-port R. Hyperglycemia and outcome in thepediatric intensive care unit. J Pediatr.2008;153:379–384
142. LeBlanc MH, Huang M, Patel D, Smith EE,Devidas M. Glucose given after hypoxic is-chemia does not affect brain injury in pig-lets. Stroke. 1994;25:1443–1447; discus-sion 1448
143. Hattori H, Wasterlain CG. Posthypoxic glu-cose supplement reduces hypoxic-ische-mic brain damage in the neonatal rat. AnnNeurol. 1990;28:122–128
144. McDonald SJ, Middleton P. Effect of timingof umbilical cord clamping of term infantson maternal and neonatal outcomes. Coch-rane Database Syst Rev. 2008:CD004074
145. Rabe H, Reynolds G, Diaz-Rossello J. A sys-tematic review and meta-analysis of abrief delay in clamping the umbilical cordof preterm infants. Neonatology. 2008;93:138–144
146. Aladangady N, McHugh S, Aitchison TC,Wardrop CA, Holland BM. Infants’ blood vol-ume in a controlled trial of placental trans-fusion at preterm delivery. Pediatrics.2006;117:93–98
147. Mercer JS, Vohr BR, McGrath MM, PadburyJF, Wallach M, Oh W. Delayed cord clamp-ing in very preterm infants reduces the in-cidence of intraventricular hemorrhageand late-onset sepsis: a randomized, con-trolled trial . Pediatrics . 2006;117:1235–1242
148. De Leeuw R, Cuttini M, Nadai M, Berbik I,Hansen G, Kucinskas A, Lenoir S, Levin A,Persson J, Rebagliato M, Reid M, SchroellM, de Vonderweid U. Treatment choices forextremely preterm infants: an interna-tional perspective. J Pediatr. 2000;137:608–616
149. Sanders MR, Donohue PK, Oberdorf MA,Rosenkrantz TS, Allen MC. Perceptions ofthe limit of viability: neonatologists’ atti-tudes toward extremely preterm infants.J Perinatol. 1995;15:494–502
150. Kopelman LM, Irons TG, Kopelman AE. Neo-natologists judge the ‘Baby Doe’ regula-tions. N Engl J Med. 1988;318:677–683
151. Costeloe K, Hennessy E, Gibson AT, MarlowN, Wilkinson AR. The epicure study: out-comes to discharge from hospital for in-fants born at the threshold of viability. Pe-diatrics. 2000;106:659–671
e1334 FROM THE AMERICAN ACADEMY OF PEDIATRICS. Provided by Health Internetwork on December 13, 2010 www.pediatrics.orgDownloaded from

152. Field DJ, Dorling JS, Manktelow BN, DraperES. Survival of extremely premature ba-b ies in a geographica l l y definedpopulation: prospective cohort study of1994–9 comparedwith 2000–5. BMJ. 2008;336:1221–1223
153. Tyson JE, Parikh NA, Langer J, Green C, Hig-gins RD. Intensive care for extremeprematurity–moving beyond gestationalage. N Engl J Med. 2008;358:1672–1681
154. Paris JJ. What standards apply to resusci-tation at the borderline of gestational age?J Perinatol. 2005;25:683–684
155. Casalaz DM, Marlow N, Speidel BD. Out-come of resuscitation following unex-pected apparent stillbirth. Arch Dis ChildFetal Neonatal Ed. 1998;78:F112–F115
156. Jain L, Ferre C, Vidyasagar D, Nath S, Shef-tel D. Cardiopulmonary resuscitation ofapparently stillborn infants: survival andlong-term outcome. J Pediatr. 1991;118:778–782
157. Laptook AR, Shankaran S, Ambalavanan N,Carlo WA, McDonald SA, Higgins RD, Das A.Outcome of term infants using Apgarscores at 10 minutes following hypoxic-is-chemic encephalopathy. Pediatrics. 2009;124:1619–1626
158. Chamnanvanakij S, Perlman JM. Outcomefollowing cardiopulmonary resuscitation inthe neonate requiring ventilatory assis-tance. Resuscitation. 2000;45:173–180
159. Annibale DJ, Hulsey TC, Wagner CL, South-gate WM. Comparative neonatal morbidityof abdominal and vaginal deliveries afteruncomplicated pregnancies. Arch PediatrAdolesc Med. 1995;149:862–867
160. Atherton N, Parsons SJ, Mansfield P. Atten-dance of paediatricians at elective caesar-ean sections performed under regionalanaesthesia: is it warranted? J PaediatrChild Health. 2006;42:332–336
161. Gordon A, McKechnie EJ, Jeffery H. Pediat-ric presence at cesarean section: justifiedor not? Am J Obstet Gynecol. 2005;193:599–605
162. Parsons SJ, Sonneveld S, Nolan T. Is a pae-diatrician needed at all caesarean sec-tions? J Paediatr Child Health. 1998;34:241–244
163. KnudsonMM, Khaw L, BullardMK, Dicker R,Cohen MJ, Staudenmayer K, Sadjadi J,Howard S, Gaba D, Krummel T. Traumatraining in simulation: translating skillsfrom SIM time to real time. J Trauma. 2008;64:255–263; discussion 263–254
164. Wayne DB, Didwania A, Feinglass J, FudalaMJ, Barsuk JH, McGaghie WC. Simulation-based education improves quality of careduring cardiac arrest team responses atan academic teaching hospital: a case-control study. Chest. 2008;133:56–61
165. Schwid HA, Rooke GA, Michalowski P, RossBK. Screen-based anesthesia simulation
with debriefing improves performance ina mannequin-based anesthesia simulator.Teach Learn Med. 2001;13:92–96
166. Kory PD, Eisen LA, Adachi M, Ribaudo VA,Rosenthal ME, Mayo PH. Initial airwayman-agement skills of senior residents: simula-tion training compared with traditionaltraining. Chest. 2007;132:1927–1931
167. Shapiro MJ, Morey JC, Small SD, LangfordV, Kaylor CJ, Jagminas L, Suner S, Salis-bury ML, Simon R, Jay GD. Simulationbased teamwork training for emergencydepartment staff: does it improve clinicalteamperformancewhen added to an exist-ing didactic teamwork curriculum? QualSaf Health Care. 2004;13:417–421
168. Cherry RA, Williams J, George J, Ali J. Theeffectiveness of a human patient simula-tor in the ATLS shock skills station. J SurgRes. 2007;139:229–235
169. Savoldelli GL, Naik VN, Park J, Joo HS, ChowR, Hamstra SJ. Value of debriefing duringsimulated crisis management: oral versusvideo-assisted oral feedback. Anesthesiol-ogy. 2006;105:279–285
170. Blum RH, Raemer DB, Carroll JS, DufresneRL, Cooper JB. A method for measuringthe effectiveness of simulation-basedteam training for improving communica-tion skills. Anesth Analg. 2005;100:1375–1380
FROM THE AMERICAN ACADEMY OF PEDIATRICS
PEDIATRICS Volume 126, Number 5, November 2010 e1335. Provided by Health Internetwork on December 13, 2010 www.pediatrics.orgDownloaded from

DISCLOSURES
CoSTR Part 11: Writing Group DisclosuresWriting GroupMember
Employment Research Grant OtherResearchSupport
Speakers’ Bureau/Honoraria
OwnershipInterest
Consultant/Advisory Board Other
Jeffrey M.Perlman
Weill Cornell Medical College—Professor ofPediatrics
†NIH funding-Co-Investigator—Improvingantimicrobial
prescribing practicesin the NICU
None *University of Miami,and Cook CountyChicago
None None None
Jonathan Wyllie South Tees Foundation NHS Trust HealthService Provider NHS UK ConsultantNeonatologist and Clinical Director of
Neonatology
None None None None *Volunteer ICC Newborn Life Support ERCVolunteer author European Newborn LifeSupport Guidelines Volunteer author UKNewborn Resuscitation Guidelines
Volunteer co-author Advanced PaediatricLife support Guidelines Volunteermember Advanced Life Support GroupUK. Volunteer acting chair Newborn LifeSupport Working Group for RC(UK)
Volunteer British Association of PerinatalMedicine Neonatal Services and staffing
working group
None
John Kattwinkel University of Virginia—Professor ofPediatrics
*American Academy ofPediatrics researchgrant to studyresuscitatorsdetection of
compliance whileadministering positivepressure ventilationby resuscitation bag
None None None None *Curley vs Gordonet al, Boston, MA(still active)
Dianne L. Atkins University of Iowa; Prof.†I am a compensated worksheet editor forAHA 2010 Guidelines process. Thecompensation is divided: 2/3 to myinstitution and 1/3 directly to me. Theamount paid to my institution does not
alter my salary
None None None None None None
Leon Chameides Emeritus Director, Pediatric Cardiology;Clinical Professor, University of Connecticut
None None None None None None
Jay P.Goldsmith
Pediatrix Medical Group: Single specialtymulti-site group practice—Neonatologist
None None None None None None
Ruth Guinsburg Federal University of Sao Paulo—FullProfessor of Pediatrics
None None None None None None
Mary FranHazinski
Vanderbilt University School of Nursing—Professor; AHA ECC Product Development—
Senior Science Editor†the significant AHA compensation isdesigned to provide protected time forediting and writing responsibilities. I have asignificant relationship with the AHA tosupport the mission of the AHA with theproduction of CoSTR and AHA Guidelines for
CPR and ECC
None None None None None None
Colin Morley Retired Professor of Neonatal Medicine None None Honoraria*Japanese Neonatal
Society*Neonatal Ventilationand Resuscitation-Zagreb, Croatia*UK MiddlesboroughNeonatal Symposium
None *Drager Medical about equip design*Education video on neonatal CPAP
None
Sam Richmond UK National Health Service—ConsultantNeonatologist
None None None None None None
Wendy M. Simon American Academy of Pediatrics—Directorof Life Support Programs
None None None None None None
Nalini Singhal University of Calgary—Professor *AAP grant looking ateffect of PEEP withand with oxygen onresuscitation.Developing a
International programfor resuscitation,Helping Babies Breath
None None None None None
Edgardo Szyld Fundasamin, Foundation for Womens andInfant Health—Executive Director of a non
profit institution (NGO)
None None None None None None
(Continued)
e1336 FROM THE AMERICAN ACADEMY OF PEDIATRICS. Provided by Health Internetwork on December 13, 2010 www.pediatrics.orgDownloaded from

CoSTR Part 11: Worksheet Collaborator DisclosuresWorksheetCollaborator
Employment Research Grant Other ResearchSupport
Speakers’ Bureau/Honoraria OwnershipInterest
Consultant/AdvisoryBoard
Other
Khalid Aziz University of Alberta—AssociateProfessor
None None None None None None
David Boyle Indiana University School of Medicine,Associate Professor of Pediatrics;University Pediatric Associates, Staff
Neonatologist
None None None None None None
Steven Byrne South Tees Hospital Foundation NHSTrust: National Health Service Trust
None None None None None None
Peter Davis The Royal Women’s Hospital,Melbourne, Australia—Staff
Neonatologist
None None None None None None
William A.Engle
Indiana University School of MedicineProfessor of Pediatrics
None None None None None None
MarilynEscobedo
University of Oklahoma—Professor ofPediatrics
None None None None None None
MariaFernandadeAlmeida
Federal University of Sao Paulo: Fulltime work (40 h/week) at NeonatalDivision—Department of Pediatrics—Assoc. Prof; Brazilian PediatricSociety: Voluntary work at BrazilianNeonatal Resuscitation Program–NRPSteering Committee—Co-chair
None None None None None None
David Field University of Leicester: Highereducational institution—UK
Government funded—Professor ofNeonatal Medicine
None None None None None None
Judith Finn University of Western Australia—Professor
†Multiple National Health andMedical Research Grants (NH& MRC), National HeartFoundation Australia andState Government grants of�$10 000 since 1999. A—Nomoney came to me—allcame to my University toemploy research staff andmeet research expenses. Nogrants were directly relatedto any topic on which I amundertaking a Worksheet andnone involved the trialing of acommercial product
None *Less than $1000 from theJapanese Resuscitation Councilto speak at their JRC Conference
in Osaka in 2009
None None None
(Continued)
CoSTR Part 11: Writing Group Disclosures, ContinuedWriting GroupMember
Employment Research Grant OtherResearchSupport
Speakers’ Bureau/Honoraria
OwnershipInterest
Consultant/Advisory Board Other
MasanoriTamura
Saitama Medical Center, Saitama MedicalUniversity—Professor and Chairman,
Department of Pediatrics
None None None None None None
SithembisoVelaphi
Univ of the Witwatersrand Univ-lecturer;Chris Hani Baragwanath hosp Govt hosp,
principal specialist
None None None None None None
This table represents the relationships of writing group members that may be perceived as actual or reasonably perceived conflicts of interest as reported on the Disclosure Questionnaire, whichall members of the writing group are required to complete and submit. A relationship is considered to be “significant” if (a) the person receives $10 000 or more during any 12-month period, or 5%or more of the person’s gross income; or (b) the person owns 5% or more of the voting stock or share of the entity, or owns $10 000 or more of the fair market value of the entity. A relationship isconsidered to be “modest” if it is less than “significant” under the preceding definition.*Modest.†Significant.
FROM THE AMERICAN ACADEMY OF PEDIATRICS
PEDIATRICS Volume 126, Number 5, November 2010 e1337. Provided by Health Internetwork on December 13, 2010 www.pediatrics.orgDownloaded from

CoSTR Part 11: Worksheet Collaborator Disclosures, ContinuedWorksheetCollaborator
Employment Research Grant Other ResearchSupport
Speakers’ Bureau/Honoraria OwnershipInterest
Consultant/AdvisoryBoard
Other
Louis P.Halamek
Stanford University—AssociateProfessor
†Source: Laerdal Foundation Iwas the Principal Investigatoron 3 year grant (2006–2009)funded by the Laerdal
Foundation in the amount of$450 000 USD that was givento the simulation center Idirect, the Center forAdvanced Pediatric andPerinatal Education at
Packard Children’s Hospitalat Stanford. This grant ended2009-07-31. This grant wasnot a source of support for
my salary
None None None *I provideconsultation servicesregarding simulationproduct design andfunction to LaerdalMedical, Inc., andAdvanced MedicalSimulation, Inc.
*I provide medicolegalconsultation services totrial attorneys in theU.S., advising onquestions relating toneonatal intensive care
Jane E.McGowan
St Christopher’s Pediatric Associates:Practice Group for Children’s
Hospital—part of Tenet Healthcare—Attending Neonatologist
None None *Received honorarium for givingat talk for the March of Dimeson “NRP and the Preterm Infant”
None None None
Douglas D.McMillan
Dalhousie University and AcademicPediatrics Incorporated: Universityand Department of PediatricsFinancial group—Professor andHead, Division of Neonatal Perinatal
medicine
None None †Medical Legal consulting feesfor different hospitals and theCanadian Medical ProtectiveAssociation (occasionally for theplaintiff)—presently “remitted”to Academic Pediatrics
Incorporated *Consulting feesfor program reviews related tonewborn care and associatededucation programs—presently“remitted” to AcademicPediatrics Incorp.
None *Consulting fees forprogram reviewsrelated to newborncare and associatededucation
programs—pres-ently “remitted” toAcademic PediatricsIncorporated
*Medical Legalconsulting fees fordifferent hospitals andthe Canadian MedicalProtective Association(occasionally for theplaintiff)—presently“remitted” to AcademicPediatrics Incorporated
LindsayMildenhall
Counties Manukau District HealthBoard Auckland New Zealand: PublicHealth Care Provider—Consultant
Neonatologist
None None None None None None
Rintaro Mori Osaka Medical Center and ResearchInstitute for Maternal and ChildHealth: a public children’s hosp. runby a local government—DivisionDirector of Strategic Planning &
Collaboration
None None None None None None
SusanNiermeyer
University of Colorado Denver Schoolof Medicine: professor, clinicalneonatologist—Professor of
Pediatrics
†Editorship, Helping BabiesBreathe, American Academyof Pediatrics 2008–2009Salary support throughcontract with University ofColorado Denver School of
Medicine
None None None None None
ColmO’Donnell
The National Maternity Hospital,Holles Street, Dublin 2, Ireland—Con-sultant Neonatologist; Our Lady’sChildren’s Hospital, Crumlin, Dublin
12, Ireland—ConsultantNeonatologist; University CollegeDublin, Ireland: University medicalschool—Clinical Lecturer
None None *I have received honoraria fromChiesi Pharma (makers ofCurosurf) for speaking at 2educational courses and 3scientific meetings (ie. on 5occasions) in the last 2 years.The combined total of thesehonoraria is less than 1000
euros
None None None
Yacov Rabi Alberta Health Services: Provideemployment income for my role as aneonatologist—Physician; Universityof Calgary: Provides income for myrole as an Assistant Professor of
Medicine
None *Supply of modifiedNeopuff circuits fora randomizedcontrol trial byFisher Paykell
None None None None
Steven A.Ringer
Brigham and Women’s Hospital: Non-profit Hospital—Chief, Newborn
Medicine
None None *Vermont Oxford NeonatalNetwork Annual Meeting
None *Alere HealthcareAdvisory Board
Consulting on ClinicalCare guidelines.Nothing relevant totopics with which Iam involved
†Expert Witness inmedical legalproceedings
(Malpractice cases). Anumber of differentattorneys/
insurance companiesMoney comes directly tome. Nothing relevant toquestions underconsideration
JasmeetSoar
North Bristol NHS Trust: GovernmentHospital in UK—Consultant inAnesthetics & Intensive Care
Medicine
None None None None None None
(Continued)
e1338 FROM THE AMERICAN ACADEMY OF PEDIATRICS. Provided by Health Internetwork on December 13, 2010 www.pediatrics.orgDownloaded from

APPENDIXCoSTR Part 11: Worksheet AppendixTask Force WS ID PICO Title Short Title Authors URL
EIT EIT-001A For resuscitation teams (P), dobriefings/debriefings (I), when compared to nobriefings/debriefings (C), improve performance
or outcomes (O)? (INTERVENTION)
Debriefing of CPRperformance
Dana P. Edelson,Trevor Yuen
http://circ.ahajournals.org/site/c2010/eit-001a.pdf
EIT EIT-001B For resuscitation teams (P), dobriefings/debriefings (I), when compared to nobriefings/debriefings (C), improve performance
or outcomes (O)? (INTERVENTION)
Debriefing of CPRperformance
Jasmeet Soar http://circ.ahajournals.org/site/c2010/eit-001b.pdf
(Continued)
CoSTR Part 11: Worksheet Collaborator Disclosures, ContinuedWorksheetCollaborator
Employment Research Grant Other ResearchSupport
Speakers’ Bureau/Honoraria OwnershipInterest
Consultant/AdvisoryBoard
Other
Benjamin J.Stenson
United Kingdom Public Health Service-Consultant Neonatologist
None None None None None None
EnriqueUdaeta
Medica Sur Lomas: Private MaternityHospital—Director Department of
Neonatology
None None None None None None
DharmapuriVidyasagar
University of Illinois Professoremeritus Progfessor emeritus
None None None None None None
MichaelWatkinson
NHS Heart of England FoundationTrust, Birmingham, UK This is an NHShospital in England Consultant
neonatologist
None None None None None None
Gary M.Weiner
St. Joseph Mercy Hospital—AttendingNeonatologist
None †Received equipmenton-loan (3resuscitation
mannequins, 2 sets ofvideo recordingequipment) fromLaerdalMedicalCorporation to beused to complete aresearch projectevaluating
educationalmethodsfor teaching neonatalresuscitation. Thevalue of the on-loanequipment isapproximately$35000
None None None None
Myra H.Wyckoff
UT Southwestern Medical Center atDallas—Associate Professor of
Pediatrics
†PI, American Academy ofPediatrics. Neonatal
Resuscitation Program. Theergonomics of neonatal
cardiac compressions. $71 030January 2008–2009 Thefunding comes to theinstitution *Co-Investigator(Mentor), American Academyof Pediatrics Neonatal
Resuscitation Program YoungInvestigator Grant.
Effectiveness of Plastic HeadCoverings for HypothermiaPrevention in PretermNewborns. January 2009–January 2010, $10 000 Thefunding comes to theinstitution
None Feb 5, 2009 Pediatric GrandRounds. University of OklahomaHealth Sciences Center. OKC, OK
None None None
This table represents therelationshipsofworksheet collaboratorsmembers thatmaybeperceivedasactual or reasonablyperceivedconflictsof interestas reportedon theDisclosureQuestionnaire,which all worksheet collaborators are required to complete and submit. A relationship is considered to be “significant” if (a) the person receives $10 000 ormore during any 12-month period, or 5%or more of the person’s gross income; or (b) the person owns 5% or more of the voting stock or share of the entity, or owns $10 000 or more of the fair market value of the entity. A relationship isconsidered to be “modest” if it is less than “significant” under the preceding definition.*Modest.†Significant.
FROM THE AMERICAN ACADEMY OF PEDIATRICS
PEDIATRICS Volume 126, Number 5, November 2010 e1339. Provided by Health Internetwork on December 13, 2010 www.pediatrics.orgDownloaded from

CoSTR Part 11: Worksheet Appendix, ContinuedTask Force WS ID PICO Title Short Title Authors URL
EIT EIT-019A In participants undergoing BLS/ALS courses (P),does the inclusion of more realistic techniques(eg. high fidelity manikins, in-situ training) (I), asopposed to standard training (eg. low fidelity,education centre) (C), improve outcomes (eg.skills performance on manikins, skillsperformance in real arrests, willingness to
perform etc.) (O)?
High fidelity training Jordan Duval-Arnould, Elizabeth A.
Hunt
http://circ.ahajournals.org/site/c2010/eit-019a.pdf
EIT EIT-019B In participants undergoing BLS/ALS courses (P),does the inclusion of more realistic techniques(eg. high fidelity manikins, in-situ training) (I), asopposed to standard training (eg. low fidelity,education centre) (C), improve outcomes (eg.skills performance on manikins, skillsperformance in real arrests, willingness to
perform etc.) (O)?
High fidelity training Judith Finn http://circ.ahajournals.org/site/c2010/eit-019b.pdf
NRP NRP-001A For neonates requiring resuscitation (P), is anyadjunct measure (eg. CO2 detection, pulseoximeter) as effective as the usual clinicalfindings (eg. heart rate, chest movement)effective to improve outcome (O)?
Adjuncts: CO2detection, pulseoximeter
John Kattwinkel http://circ.ahajournals.org/site/c2010/nrp-001a.pdf
NRP NRP-001B For neonates requiring resuscitation (P), is anyadjunct measure (eg. CO2 detection, pulseoximeter) as effective as the usual clinicalfindings (eg. heart rate, chest movement)effective to improve outcome (O)?
Adjuncts: CO2detection, pulseoximeter
Yacov Rabi http://circ.ahajournals.org/site/c2010/nrp-001b.pdf
NRP NRP-002A In the neonates infant (preterm and term)receiving respiratory support (P), does the use ofCPAP(I) versus no-CPAP or IPPV(C) improve
outcome—specify (O)?
CPAP and IPPV Colm O’Donnell http://circ.ahajournals.org/site/c2010/nrp-002a.pdf
NRP NRP-002B In the neonates infant (preterm and term)receiving respiratory support (P), does the use ofCPAP(I) versus no-CPAP or IPPV(C) improve
outcome—specify (O)?
CPAP and IPPV Douglas D. McMillan http://circ.ahajournals.org/site/c2010/nrp-002b.pdf
NRP NRP-003A In neonates receiving respiratory support (P)does the use of face mask interface (I) versusCPAP, NPCPAP, NC (C) (excluding intubation
improve outcome) (O)?
Face mask interfacevs CPAP etc
Colin Morley http://circ.ahajournals.org/site/c2010/nrp-003a.pdf
NRP NRP-003B In neonates receiving respiratory support (P)does the use of face mask interface (I) versusCPAP, NPCPAP, NC (C) (excluding intubation)
improve outcome (O)?
Face mask interfacevs CPAP etc
Yacov Rabi http://circ.ahajournals.org/site/c2010/nrp-003b.pdf
NRP NRP-004A In neonates receiving resuscitation (P) does theuse of mouth-to-mouth, mouth-to-mask, mouthtube to mask (I) as compared to a self-inflatingbag (C) give equivalent outcomes (stablespontaneous breathing) (O), when devices for
delivering PPV are not available?
Self-inflating bag vsmouth techniques
Nalini Singhal http://circ.ahajournals.org/site/c2010/nrp-004a.pdf
NRP NRP-004B In neonates receiving resuscitation (P) does theuse of mouth-to-mouth, mouth-to-mask, mouthtube to mask (I) as compared to a self-inflatingbag (C) give equivalent outcomes (stablespontaneous breathing) (O), when devices for
delivering PPV are not available?
Self-inflating bag vsmouth techniques
Maria Fernanda deAlmeida
http://circ.ahajournals.org/site/c2010/nrp-004b.pdf
NRP NRP-005A In neonates receiving positive pressureventilation (P) does the use of gas volume
monitoring (I) versus clinical assessment with orwithout pressure monitoring (C) improve clinical
outcome (O)?
Ventilation volumemonitoring
Steven A. Ringer http://circ.ahajournals.org/site/c2010/nrp-005a.pdf
NRP NRP-005B In neonates receiving positive pressureventilation (P) does the use of gas volume
monitoring (I) versus clinical assessment with orwithout pressure monitoring (C) improve clinical
outcome (O)?
Ventilation volumemonitoring
Khalid Aziz http://circ.ahajournals.org/site/c2010/nrp-005b.pdf
NRP NRP-005C In neonates receiving positive pressureventilation (P) does the use of gas volume
monitoring (I) versus clinical assessment with orwithout pressure monitoring (C) improve clinical
outcome (O)?
Ventilation volumemonitoring
Jane E. McGowan http://circ.ahajournals.org/site/c2010/nrp-005c.pdf
NRP NRP-006A In neonates receiving chest compressions (P) doother ratios (5:1, 15:2) (I) versus a 3:1 (C) improve
outcomes (O)?
Compressionventilation ratio
Lindsay Mildenhall http://circ.ahajournals.org/site/c2010/nrp-006a.pdf
NRP NRP-006B In neonates receiving chest compressions (P) doother ratios (5:1, 15:2) (I) versus a 3:1 (C) improve
outcomes (O)?
Compressionventilation ratio
Myra H. Wyckoff http://circ.ahajournals.org/site/c2010/nrp-006b.pdf
(Continued)
e1340 FROM THE AMERICAN ACADEMY OF PEDIATRICS. Provided by Health Internetwork on December 13, 2010 www.pediatrics.orgDownloaded from
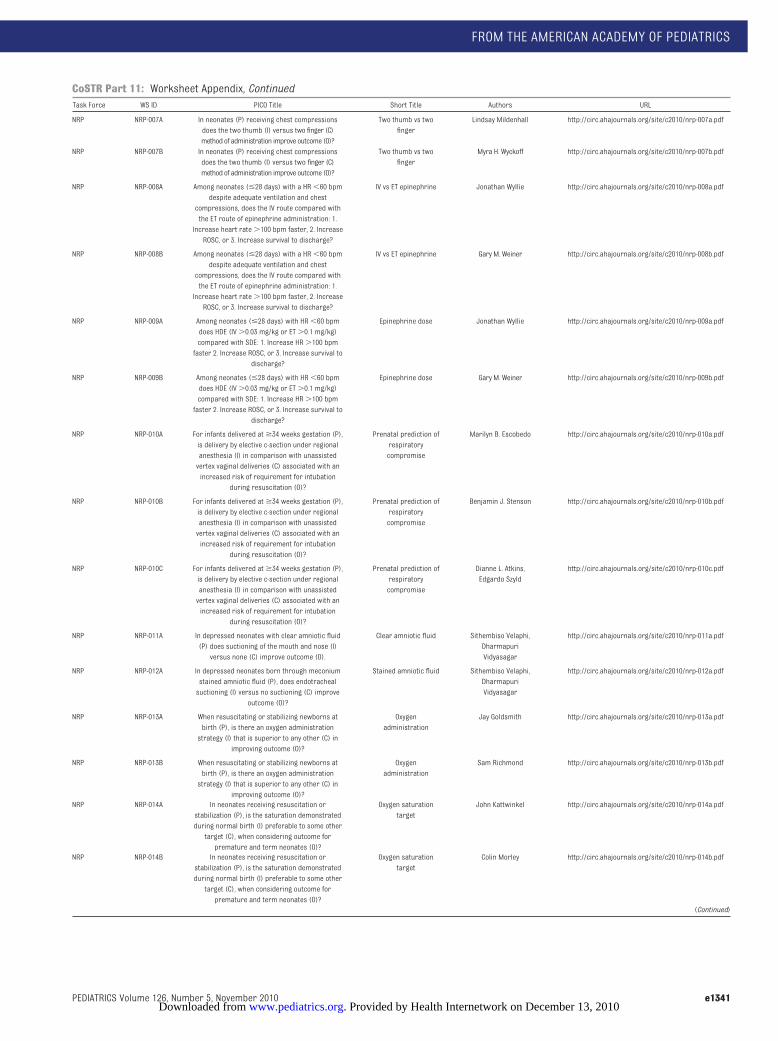
CoSTR Part 11: Worksheet Appendix, ContinuedTask Force WS ID PICO Title Short Title Authors URL
NRP NRP-007A In neonates (P) receiving chest compressionsdoes the two thumb (I) versus two finger (C)method of administration improve outcome (O)?
Two thumb vs twofinger
Lindsay Mildenhall http://circ.ahajournals.org/site/c2010/nrp-007a.pdf
NRP NRP-007B In neonates (P) receiving chest compressionsdoes the two thumb (I) versus two finger (C)method of administration improve outcome (O)?
Two thumb vs twofinger
Myra H. Wyckoff http://circ.ahajournals.org/site/c2010/nrp-007b.pdf
NRP NRP-008A Among neonates (�28 days) with a HR�60 bpmdespite adequate ventilation and chest
compressions, does the IV route compared withthe ET route of epinephrine administration: 1.Increase heart rate�100 bpm faster, 2. IncreaseROSC, or 3. Increase survival to discharge?
IV vs ET epinephrine Jonathan Wyllie http://circ.ahajournals.org/site/c2010/nrp-008a.pdf
NRP NRP-008B Among neonates (�28 days) with a HR�60 bpmdespite adequate ventilation and chest
compressions, does the IV route compared withthe ET route of epinephrine administration: 1.Increase heart rate�100 bpm faster, 2. IncreaseROSC, or 3. Increase survival to discharge?
IV vs ET epinephrine Gary M. Weiner http://circ.ahajournals.org/site/c2010/nrp-008b.pdf
NRP NRP-009A Among neonates (�28 days) with HR�60 bpmdoes HDE (IV�0.03 mg/kg or ET�0.1 mg/kg)compared with SDE: 1. Increase HR�100 bpmfaster 2. Increase ROSC, or 3. Increase survival to
discharge?
Epinephrine dose Jonathan Wyllie http://circ.ahajournals.org/site/c2010/nrp-009a.pdf
NRP NRP-009B Among neonates (�28 days) with HR�60 bpmdoes HDE (IV�0.03 mg/kg or ET�0.1 mg/kg)compared with SDE: 1. Increase HR�100 bpmfaster 2. Increase ROSC, or 3. Increase survival to
discharge?
Epinephrine dose Gary M. Weiner http://circ.ahajournals.org/site/c2010/nrp-009b.pdf
NRP NRP-010A For infants delivered at�34 weeks gestation (P),is delivery by elective c-section under regionalanesthesia (I) in comparison with unassistedvertex vaginal deliveries (C) associated with anincreased risk of requirement for intubation
during resuscitation (O)?
Prenatal prediction ofrespiratorycompromise
Marilyn B. Escobedo http://circ.ahajournals.org/site/c2010/nrp-010a.pdf
NRP NRP-010B For infants delivered at�34 weeks gestation (P),is delivery by elective c-section under regionalanesthesia (I) in comparison with unassistedvertex vaginal deliveries (C) associated with anincreased risk of requirement for intubation
during resuscitation (O)?
Prenatal prediction ofrespiratorycompromise
Benjamin J. Stenson http://circ.ahajournals.org/site/c2010/nrp-010b.pdf
NRP NRP-010C For infants delivered at�34 weeks gestation (P),is delivery by elective c-section under regionalanesthesia (I) in comparison with unassistedvertex vaginal deliveries (C) associated with anincreased risk of requirement for intubation
during resuscitation (O)?
Prenatal prediction ofrespiratorycompromise
Dianne L. Atkins,Edgardo Szyld
http://circ.ahajournals.org/site/c2010/nrp-010c.pdf
NRP NRP-011A In depressed neonates with clear amniotic fluid(P) does suctioning of the mouth and nose (I)versus none (C) improve outcome (O).
Clear amniotic fluid Sithembiso Velaphi,DharmapuriVidyasagar
http://circ.ahajournals.org/site/c2010/nrp-011a.pdf
NRP NRP-012A In depressed neonates born through meconiumstained amniotic fluid (P), does endotrachealsuctioning (I) versus no suctioning (C) improve
outcome (O)?
Stained amniotic fluid Sithembiso Velaphi,DharmapuriVidyasagar
http://circ.ahajournals.org/site/c2010/nrp-012a.pdf
NRP NRP-013A When resuscitating or stabilizing newborns atbirth (P), is there an oxygen administrationstrategy (I) that is superior to any other (C) in
improving outcome (O)?
Oxygenadministration
Jay Goldsmith http://circ.ahajournals.org/site/c2010/nrp-013a.pdf
NRP NRP-013B When resuscitating or stabilizing newborns atbirth (P), is there an oxygen administrationstrategy (I) that is superior to any other (C) in
improving outcome (O)?
Oxygenadministration
Sam Richmond http://circ.ahajournals.org/site/c2010/nrp-013b.pdf
NRP NRP-014A In neonates receiving resuscitation orstabilization (P), is the saturation demonstratedduring normal birth (I) preferable to some othertarget (C), when considering outcome forpremature and term neonates (O)?
Oxygen saturationtarget
John Kattwinkel http://circ.ahajournals.org/site/c2010/nrp-014a.pdf
NRP NRP-014B In neonates receiving resuscitation orstabilization (P), is the saturation demonstratedduring normal birth (I) preferable to some othertarget (C), when considering outcome forpremature and term neonates (O)?
Oxygen saturationtarget
Colin Morley http://circ.ahajournals.org/site/c2010/nrp-014b.pdf
(Continued)
FROM THE AMERICAN ACADEMY OF PEDIATRICS
PEDIATRICS Volume 126, Number 5, November 2010 e1341. Provided by Health Internetwork on December 13, 2010 www.pediatrics.orgDownloaded from

CoSTR Part 11: Worksheet Appendix, ContinuedTask Force WS ID PICO Title Short Title Authors URL
NRP NRP-015A In neonates (P) receiving positive pressure duringresuscitation, is positive pressure ventilation byT-piece resuscitator (I) superior to bag ventilation(C) for improving outcome—specify (O)?
T-piece resuscitator David Boyle http://circ.ahajournals.org/site/c2010/nrp-015a.pdf
NRP NRP-015B In neonates (P) receiving positive pressure duringresuscitation, is positive pressure ventilation byT-piece resuscitator (I) superior to bag ventilation(C) for improving outcome—specify (O)?
T-piece resuscitator Benjamin J. Stenson http://circ.ahajournals.org/site/c2010/nrp-015b.pdf
NRP NRP-015C In neonates(P) receiving positive pressure duringresuscitation, is positive pressure ventilation byT-piece resuscitator (I) superior to bag ventilation(C) for improving outcome—specify (O)?
T-piece resuscitator David Field http://circ.ahajournals.org/site/c2010/nrp-015c.pdf
NRP NRP-016A For neonates (P) following attemptedendotracheal intubation, is CO2 detection (I)
superior to clinical assessment (C) for confirmingendotracheal location (O)?
CO2 detection Jonathan Wyllie http://circ.ahajournals.org/site/c2010/nrp-016a.pdf
NRP NRP-017A For neonates requiring positive pressureventilation (P), is LMA (I) an effective alternativeto mask or endotracheal ventilation (C) forimproving outcome (O)? (achieving stable vitalsigns and reducing the need for subsequent
endotracheal intubation)?
LMA Gary M. Weiner http://circ.ahajournals.org/site/c2010/nrp-017a.pdf
NRP NRP-017B For neonates requiring positive pressureventilation (P), is LMA (I) an effective alternativeto mask or endotracheal ventilation (C) forimproving outcome (O)? (achieving stable vitalsigns and reducing the need for subsequent
endotracheal intubation)?
LMA Enrique Udaeta http://circ.ahajournals.org/site/c2010/nrp-017b.pdf
NRP NRP-018A For non intubated bradycardic neonates (P)requiring positive pressure ventilation, is the CO2monitoring device (I) more effective than chestrise, color (C) for assessing adequate ventilation (O)?
Bradycardia and CO2monitoring
Colm O’Donnell http://circ.ahajournals.org/site/c2010/nrp-018a.pdf
NRP NRP-018B For non intubated bradycardic neonates (P)requiring positive pressure ventilation, is the CO2monitoring device (I) more effective than chestrise, color (C) for assessing adequate ventilation (O)?
Bradycardia and CO2monitoring
Masanori Tamura http://circ.ahajournals.org/site/c2010/nrp-018b.pdf
NRP NRP-018C For non intubated bradycardic neonates (P)requiring positive pressure ventilation, is the CO2monitoring device (I) more effective than chestrise, color (C) for assessing adequate ventilation (O)?
Bradycardia and CO2monitoring
Steven A. Ringer http://circ.ahajournals.org/site/c2010/nrp-018c.pdf
NRP NRP-019A In neonates requiring resuscitation, (P) will theearly use of supplemental glucose (I) during and/or following delivery room resuscitation, versusnone (C) improve outcome (i.e. avoidance ofhypoglycemia, reduced long-term neurologic
morbidity) (O)?
Supplemental glucose Jane E. McGowan http://circ.ahajournals.org/site/c2010/nrp-019a.pdf
NRP NRP-019B In neonates requiring resuscitation, (P) will theearly use of supplemental glucose (I) during and/or following delivery room resuscitation, versusnone (C) improve outcome (i.e. avoidance ofhypoglycemia, reduced long-term neurologic
morbidity) (O)?
Supplemental glucose Jeffrey Perlman http://circ.ahajournals.org/site/c2010/nrp-019b.pdf
NRP NRP-020A In neonates requiring resuscitation, does theadministration of emergency medications (P) byintraosseous infusion (I) versus the intravenous
route improve outcome (O)?
IO vs IV William A. Engle http://circ.ahajournals.org/site/c2010/nrp-020a.pdf
NRP NRP-021A In neonates requiring resuscitation and notresponding to CPR (P), does the administration ofsodium bicarbonate (I) versus no bicarbonate (C)
improve outcome (O)?
Sodium bicarbonate Jeffrey Perlman http://circ.ahajournals.org/site/c2010/nrp-021a.pdf
NRP NRP-021B In neonates requiring resuscitation and notresponding to CPR (P), does the administration ofsodium bicarbonate (I) versus no bicarbonate (C)
improve outcome (O)?
Sodium bicarbonate Dianne L. Atkins, SamRichmond
http://circ.ahajournals.org/site/c2010/nrp-021b.pdf
NRP NRP-022A In apneic neonates suspected of narcoticdepression (P), does naloxone (I) when comparedto effective ventilation without naloxone (C)
improve outcome (O)?
Nalaxone Ruth Guinsburg http://circ.ahajournals.org/site/c2010/nrp-022a.pdf
NRP NRP-022B In apneic neonates suspected of narcoticdepression (P), does naloxone (I) when comparedto effective ventilation without naloxone (C)
improve outcome (O)?
Nalaxone Myra H. Wyckoff http://circ.ahajournals.org/site/c2010/nrp-022b.pdf
(Continued)
e1342 FROM THE AMERICAN ACADEMY OF PEDIATRICS. Provided by Health Internetwork on December 13, 2010 www.pediatrics.orgDownloaded from

CoSTR Part 11: Worksheet Appendix, ContinuedTask Force WS ID PICO Title Short Title Authors URL
NRP NRP-023A In preterm neonates under radiant warmers (P),does increased room temperature, thermalmattress, or other intervention (I) as comparedto plastic wraps alone (C) improve outcome (O)?
Warming adjuncts Marilyn B. Escobedo,Michael Watkinson
http://circ.ahajournals.org/site/c2010/nrp-023a.pdf
NRP NRP-024A In term neonates at risk for hypoxic-ischemicencephalopathy secondary to intra-partum hypox-ia (P) does selective/whole body cooling (I) versusstandard therapy (C), result in improved outcome
(O)?
Hypothermia(induced)
Jeffrey Perlman http://circ.ahajournals.org/site/c2010/nrp-024a.pdf
NRP NRP-024B In term neonates at risk for hypoxic-ischemicencephalopathy secondary to intra-partum hypox-ia (P) does selective/whole body cooling (I) versusstandard therapy (C), result in improved outcome
(O)?
Hypothermia(induced)
Peter Davis http://circ.ahajournals.org/site/c2010/nrp-024b.pdf
NRP NRP-025A In term neonates without a detectable heart rateand no other signs of life (P) is ten minutes (I) asopposed to 15 minutes or longer (C) of effectiveresuscitation a reliable measure of outcome(abnormal neurologic examination and/or death)
(O)?
Duration of CPR withasystole and outcome
Steve Byrne http://circ.ahajournals.org/site/c2010/nrp-025a.pdf
NRP NRP-025B In term neonates without a detectable heart rateand no other signs of life (P) is ten minutes (I) asopposed to 15 minutes or longer (C) of effectiveresuscitation a reliable measure of outcome(abnormal neurologic examination and/or death)
(O)?
Duration of CPR withasystole and outcome
Jay Goldsmith http://circ.ahajournals.org/site/c2010/nrp-025b.pdf
NRP NRP-025C In term neonates without a detectable heart rateand no other signs of life (P) is ten minutes (I) asopposed to 15 minutes or longer (C) of effectiveresuscitation a reliable measure of outcome(abnormal neurologic examination and/or death)
(O)?
Duration of CPR withasystole and outcome
Ruth Guinsburg http://circ.ahajournals.org/site/c2010/nrp-025c.pdf
NRP NRP-026A In term neonates with a heart rate�60 and noother signs of life (P), is ten minutes (I) as
opposed to 15 minutes or longer (C) of effectiveresuscitation a reliable measure of outcome(abnormal neurologic examination and/or death) (O)?
Duration of CPR withbradycardia andoutcome
Steve Byrne http://circ.ahajournals.org/site/c2010/nrp-026a.pdf
NRP NRP-026B In term neonates with a heart rate�60 and noother signs of life (P), is ten minutes (I) as
opposed to 15 minutes or longer (C) of effectiveresuscitation a reliable measure of outcome(abnormal neurologic examination and/or death) (O)?
Duration of CPR withbradycardia andoutcome
Jay Goldsmith http://circ.ahajournals.org/site/c2010/nrp-026b.pdf
NRP NRP-026C In term neonates with a heart rate�60 and noother signs of life (P), is ten minutes (I) as
opposed to 15 minutes or longer (C) of effectiveresuscitation a reliable measure of outcome(abnormal neurologic examination and/or death) (O)?
Duration of CPR withbradycardia andoutcome
Ruth Guinsburg http://circ.ahajournals.org/site/c2010/nrp-026c.pdf
NRP NRP-027A In neonates at the limits of viability or anomaliesassociated with lethal outcomes (P) does the noninitiation (I) versus initiation (C) of resuscitationresult in an outcome that is ethically justified (O).
Futile resuscitationrules
Steve Byrne http://circ.ahajournals.org/site/c2010/nrp-027a.pdf
NRP NRP-027B In neonates at the limits of viability or anomaliesassociated with lethal outcomes (P) does the noninitiation (I) versus initiation (C) of resuscitationresult in an outcome that is ethically justified (O).
Futile resuscitationrules
Jay Goldsmith http://circ.ahajournals.org/site/c2010/nrp-027b.pdf
NRP NRP-028A In depressed neonates requiring positivepressure ventilation (P) does the administrationof longer inspiratory times, higher inflationpressures, use of PEEP (I) as compared to
standard management (C) improve outcome (O)?
Ventilation times andpressures
David Boyle http://circ.ahajournals.org/site/c2010/nrp-028a.pdf
NRP NRP-028B In depressed neonates requiring positivepressure ventilation (P) does the administrationof longer inspiratory times, higher inflationpressures, use of PEEP (I) as compared to
standard management (C) improve outcome (O)?
Ventilation times andpressures
Benjamin J. Stenson http://circ.ahajournals.org/site/c2010/nrp-028b.pdf
NRP NRP-029A In neonates requiring resuscitation andunresponsive to chest compressions/epinephrine(P) does the administration of volume (I) versus
no volume (C) improve outcome (O).
Volume resuscitationwith CPR
Susan Niermeyer http://circ.ahajournals.org/site/c2010/nrp-029a.pdf
NRP NRP-029B In neonates requiring resuscitation andunresponsive to chest compressions/epinephrine(P) does the administration of volume (I) versus
no volume (C) improve outcome (O).
Volume resuscitationwith CPR
Douglas D. McMillan http://circ.ahajournals.org/site/c2010/nrp-029b.pdf
(Continued)
FROM THE AMERICAN ACADEMY OF PEDIATRICS
PEDIATRICS Volume 126, Number 5, November 2010 e1343. Provided by Health Internetwork on December 13, 2010 www.pediatrics.orgDownloaded from

CoSTR Part 11: Worksheet Appendix, ContinuedTask Force WS ID PICO Title Short Title Authors URL
NRP NRP-029C In neonates requiring resuscitation andunresponsive to chest compressions/epinephrine(P) does the administration of volume (I) versus
no volume (C) improve outcome (O).
Volume resuscitationwith CPR
Masanori Tamura http://circ.ahajournals.org/site/c2010/nrp-029c.pdf
NRP NRP-030A In neonates (P), does delayed cord clamping cordor milking of the cord (I) versus standardmanagement (C), improve outcome (O).
Umbilical cordclamping and milking
Susan Niermeyer http://circ.ahajournals.org/site/c2010/nrp-030a.pdf
NRP NRP-030B In neonates (P), does delayed cord clamping cordor milking of the cord (I) versus standardmanagement (C), improve outcome (O).
Umbilical cordclamping and milking
Dianne L. Atkins,Nalini Singhal
http://circ.ahajournals.org/site/c2010/nrp-030b.pdf
NRP NRP-030C In neonates (P), does delayed cord clamping cordor milking of the cord (I) versus standard
management (C), improve outcome (O) (milkingof the cord).
Umbilical cordclamping and milking
Gary M. Weiner http://circ.ahajournals.org/site/c2010/nrp-030c.pdf
NRP NRP-030D In neonates (P), does delayed cord clamping cordor milking of the cord (I) versus standardmanagement (C), improve outcome (O)?
Umbilical cordclamping and milking
Rintaro Mori http://circ.ahajournals.org/site/c2010/nrp-030d.pdf
NRP NRP-031A In neonates born to febrile mothers (P) doesintervention to normalize temperature (I),compared to standard care (C) improve
outcome (O)?
Maternal fever Jeffrey Perlman http://circ.ahajournals.org/site/c2010/nrp-031a.pdf
NRP NRP-031B In neonates born to febrile mothers (P) doesintervention to normalize temperature (I),compared to standard care (C) improve
outcome (O).
Maternal fever Steven A. Ringer http://circ.ahajournals.org/site/c2010/nrp-031b.pdf
NRP NRP-032A In participants undergoing resuscitation courses(P), does the inclusion of more realistictechniques (eg. high fidelity manikins, in-situtraining) (I), as opposed to standard training (eg.low fidelity, education centre) (C), improveoutcomes (eg. skills performance) (O).
Impact of realistictraining on skillsperformance
Jane E. McGowan http://circ.ahajournals.org/site/c2010/nrp-032a.pdf
NRP NRP-032B In participants undergoing resuscitation courses(P), does the inclusion of more realistictechniques (eg. high fidelity manikins, in-situtraining) (I), as opposed to standard training (eg.low fidelity, education centre) (C), improveoutcomes (eg. skills performance) (O).
Impact of realistictraining on skillsperformance
Louis P. Halamek http://circ.ahajournals.org/site/c2010/nrp-032b.pdf
NRP NRP-032C In participants undergoing resuscitation courses(P), does the inclusion of more realistictechniques (eg. high fidelity manikins, in-situtraining) (I), as opposed to standard training (eg.low fidelity, education centre) (C), improveoutcomes (eg. skills performance) (O).
Impact of realistictraining on skillsperformance
Khalid Aziz http://circ.ahajournals.org/site/c2010/nrp-032c.pdf
NRP NRP-033A For hospital resuscitation teams (P), do teambriefings/debriefings (I), when compared to nobriefings/debriefings (C), improve teamperformance (O)? (INTERVENTION)
Impact of debriefingon team performance
Dianne L. Atkins,Nalini Singhal
http://circ.ahajournals.org/site/c2010/nrp-033a.pdf
NRP NRP-033B For hospital resuscitation teams (P), do teambriefings/debriefings (I), when compared to nobriefings/debriefings (C), improve teamperformance (O)? (INTERVENTION)
Impact of debriefingon team performance
Louis P. Halamek http://circ.ahajournals.org/site/c2010/nrp-033b.pdf
e1344 FROM THE AMERICAN ACADEMY OF PEDIATRICS. Provided by Health Internetwork on December 13, 2010 www.pediatrics.orgDownloaded from

DOI: 10.1542/peds.2010-2972B 2010;126;e1319-e1344; originally published online Oct 18, 2010; Pediatrics
COLLABORATORS CHAPTERSithembiso Velaphi and on behalf of the NEONATAL RESUSCITATION
Sam Richmond, Wendy M. Simon, Nalini Singhal, Edgardo Szyld, Masanori Tamura,Chameides, Jay P. Goldsmith, Ruth Guinsburg, Mary Fran Hazinski, Colin Morley,
Jeffrey M. Perlman, Jonathan Wyllie, John Kattwinkel, Dianne L. Atkins, Leon Recommendations
Resuscitation and Emergency Cardiovascular Care Science With Treatment Neonatal Resuscitation: 2010 International Consensus on Cardiopulmonary
& ServicesUpdated Information
http://www.pediatrics.org/cgi/content/full/126/5/e1319including high-resolution figures, can be found at:
References
http://www.pediatrics.org/cgi/content/full/126/5/e1319#BIBLfree at: This article cites 167 articles, 49 of which you can access for
Citations
cleshttp://www.pediatrics.org/cgi/content/full/126/5/e1319#otherartiThis article has been cited by 1 HighWire-hosted articles:
Permissions & Licensing
http://www.pediatrics.org/misc/Permissions.shtmltables) or in its entirety can be found online at: Information about reproducing this article in parts (figures,
Reprints http://www.pediatrics.org/misc/reprints.shtml
Information about ordering reprints can be found online:
. Provided by Health Internetwork on December 13, 2010 www.pediatrics.orgDownloaded from