Neonatal/Pediatric Cardiopulmonary Care Resuscitation.
58
Neonatal/Pediatric Neonatal/Pediatric Cardiopulmonary Cardiopulmonary Care Care Resuscitation Resuscitation
-
Upload
brett-rice -
Category
Documents
-
view
235 -
download
0
Transcript of Neonatal/Pediatric Cardiopulmonary Care Resuscitation.
Neonatal/Pediatric Neonatal/Pediatric Cardiopulmonary CareCardiopulmonary Care
ResuscitationResuscitation
2
When To Resuscitate
Need usually related
Combination of
Can occur in
3
Causes of Fetal Asphyxia
4
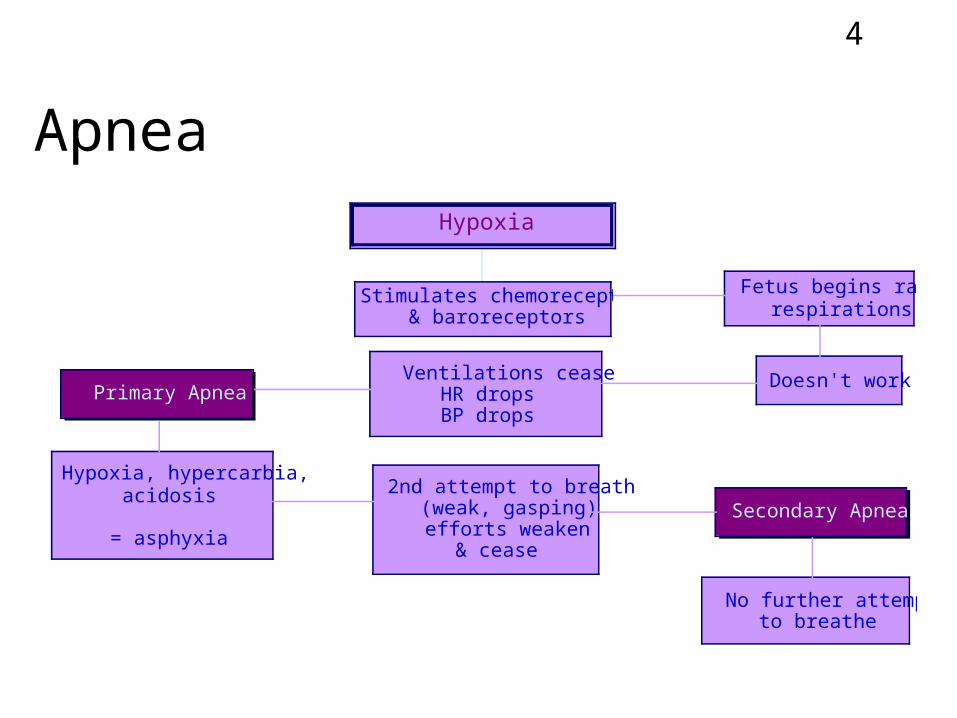
Apnea
Doesn't work
Fetus begins rapidrespirations
Ventilations ceaseHR dropsBP drops
Primary Apnea
Hypoxia, hypercarbia,acidosis
= asphyxia
2nd attempt to breath (weak, gasping) efforts weaken
& cease
Secondary Apnea
No further attemptto breathe
Stimulates chemoreceptors& baroreceptors
Hypoxia
5
Effect of Asphyxia on Lungs
Initial adaption to extra-uterine life requires 2 steps:
–
–
6
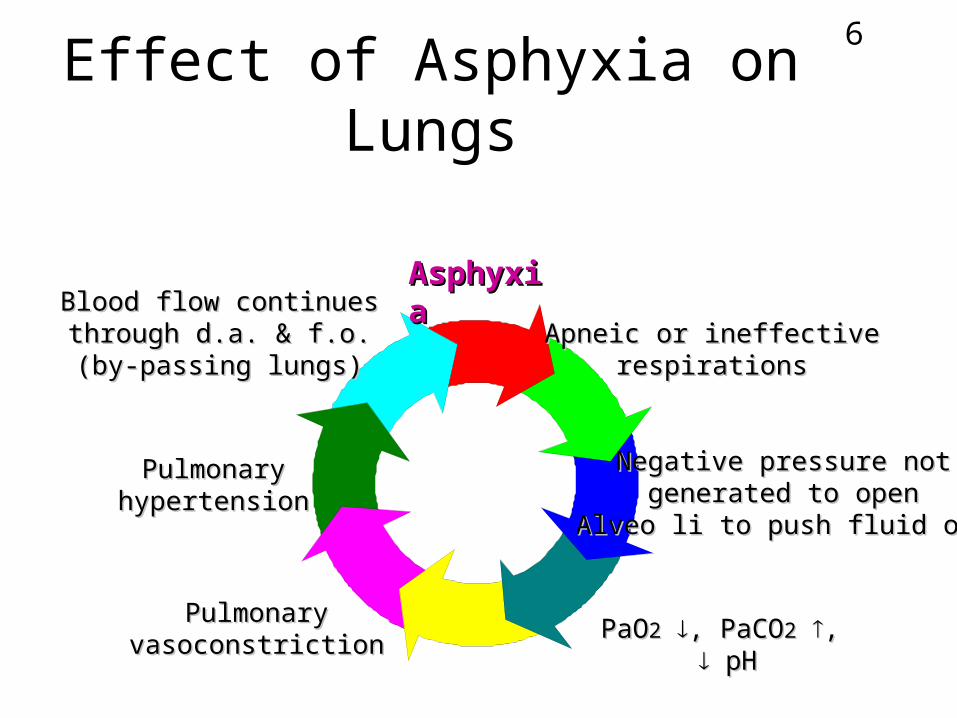
Effect of Asphyxia on Lungs
AsphyxiaAsphyxia
Apneic or ineffectiveApneic or ineffectiverespirationsrespirations
Negative pressure notNegative pressure notgenerated to opengenerated to open
Alveo li to push fluid outAlveo li to push fluid out
PaOPaO22 , PaCO, PaCO22 ,, pHpH
PulmonaryPulmonaryvasoconstrictionvasoconstriction
PulmonaryPulmonaryhypertensionhypertension
Blood flow continuesBlood flow continuesthrough d.a. & f.o.through d.a. & f.o.(by-passing lungs)(by-passing lungs)
7
Effect of Asphyxia on Lungs
If asphyxia severe with lactic acidosis
Ventilation alone will not change
acid-base imbalance
8
Effect of Asphyxia on Lungs
In severe cases - might be beneficial to give HCO3
- to
–
–
–

9
Effect of Asphyxia on Lungs
NOTE:
Adequate ventilation must be maintained when bicarb
given!!!
Why??
10
Effect of Asphyxia on Lungs
11
Preparation For Resuscitation
12
Basics of Neonatal Resuscitation
A -
B -
C -
3 steps:3 steps:
13
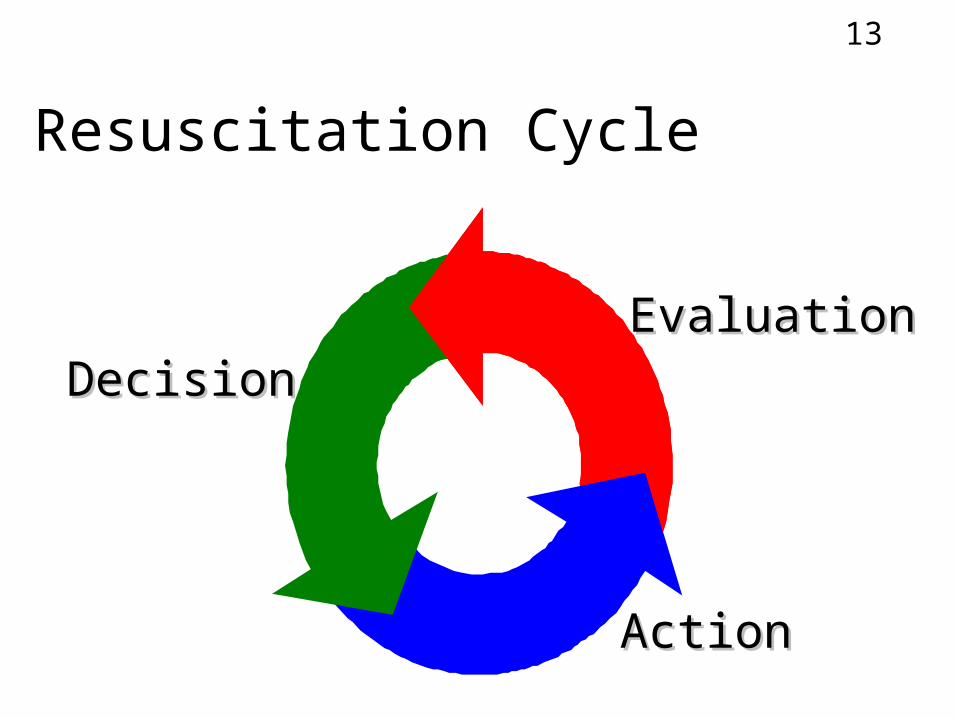
Resuscitation Cycle
EvaluationEvaluationDecisionDecision
ActionAction
14
Steps in Resuscitation
1st step =
15
Mechanisms of Heat Loss
Radiation– Loss to
Conduction– Loss to
Evaporation– Loss when
Convection– Loss to
16
Causes of Heat Loss
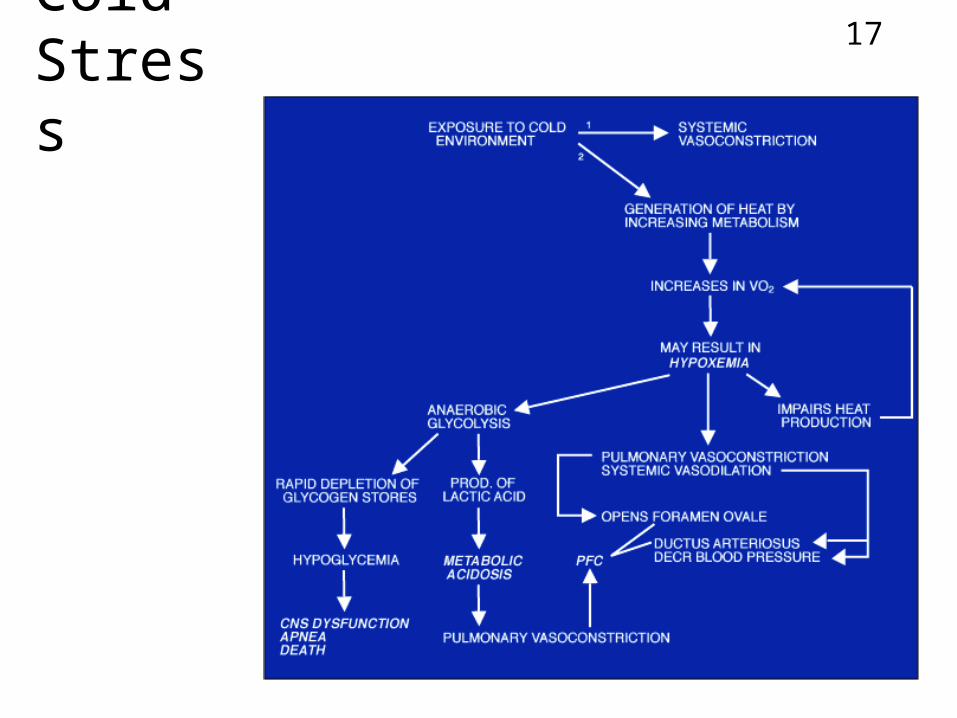
17ColdStress
18
Steps in Resuscitation
Next Step = Open airwayNext Step = Open airway
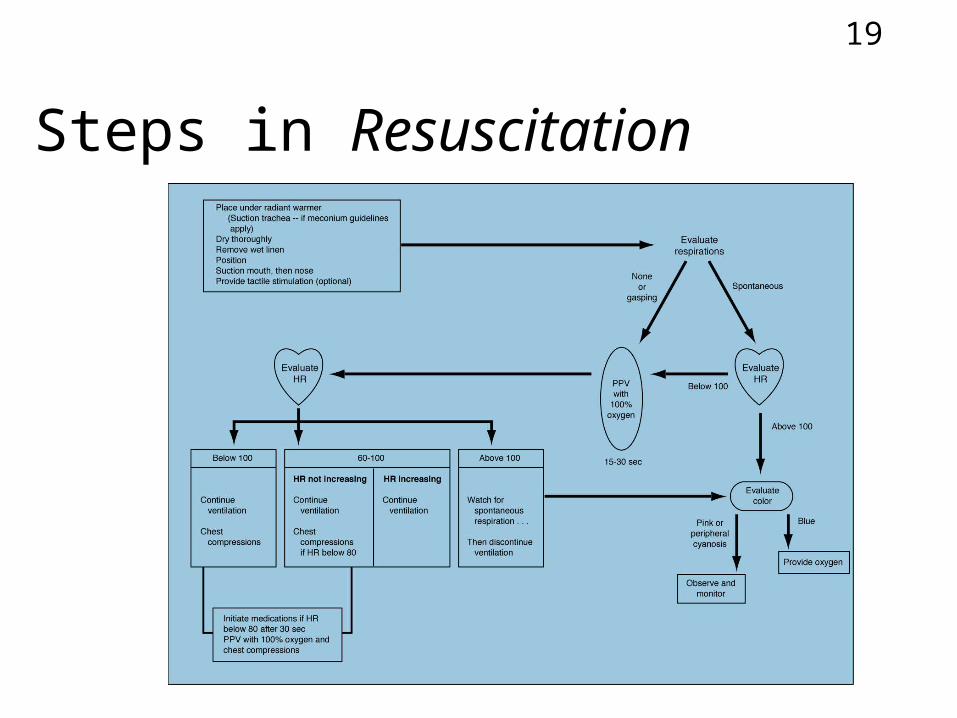
19
Steps in Resuscitation
20
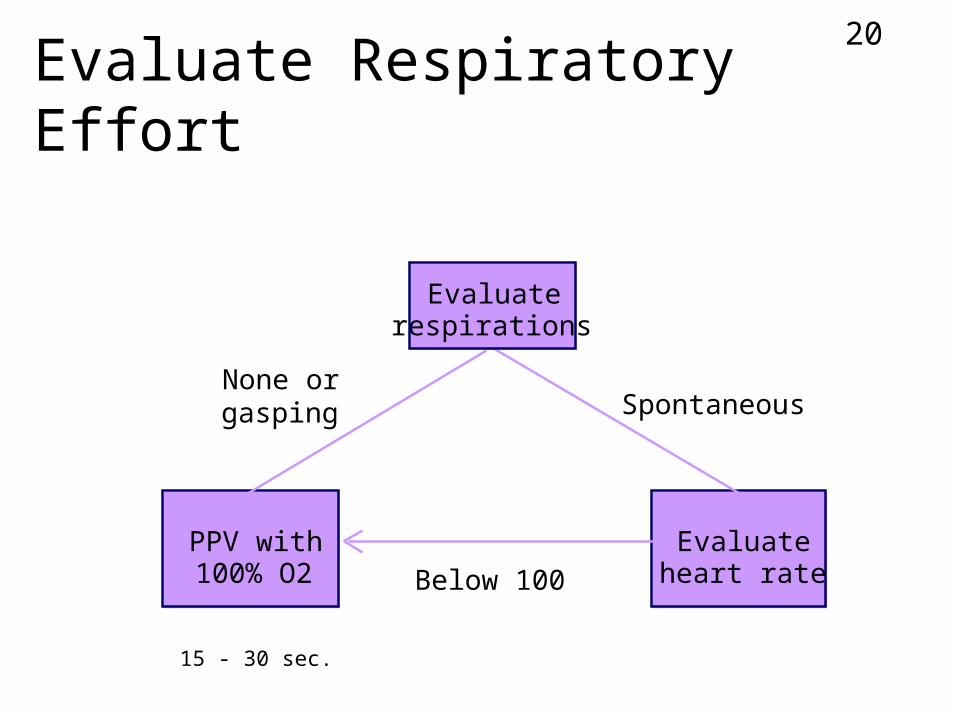
Evaluate Respiratory Effort
Evaluateheart rate
PPV with100% O2
None orgasping Spontaneous
Below 100
15 - 30 sec.
Evaluaterespirations
21
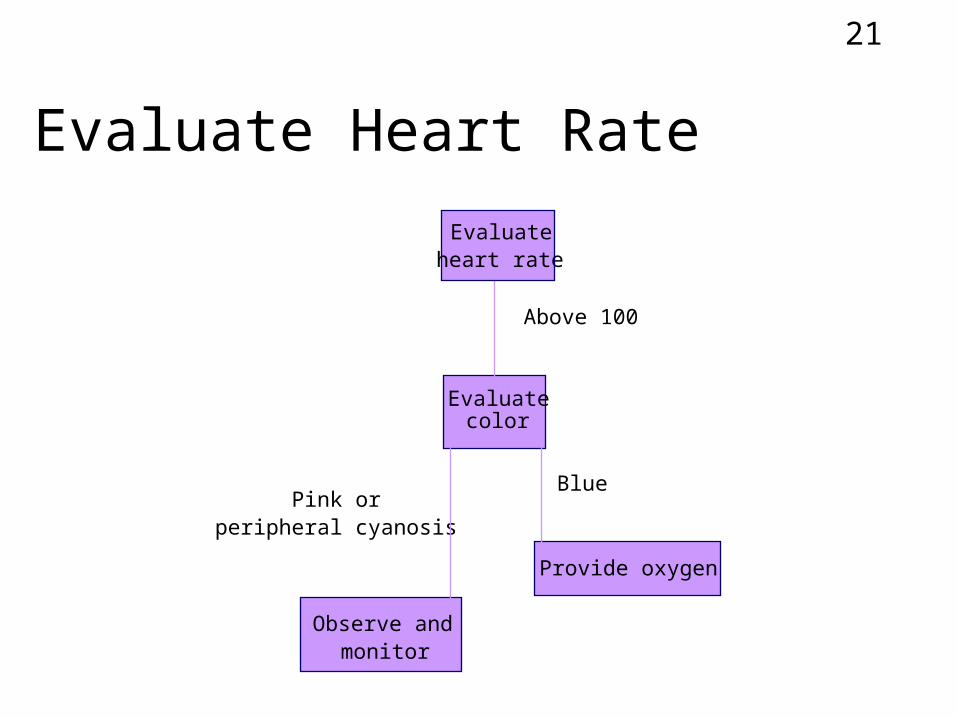
Evaluate Heart Rate
Above 100
Evaluatecolor
Provide oxygen
Observe andmonitor
Pink orperipheral cyanosis
Blue
Evaluateheart rate
22
Indications for PPV
23
Positive Pressure Ventilation
Flow-inflating bag
Self-inflating bag
Pressure gauge
Oxygen flow 5-8 lpm
Pop-off at 30-40 cmH2O
24
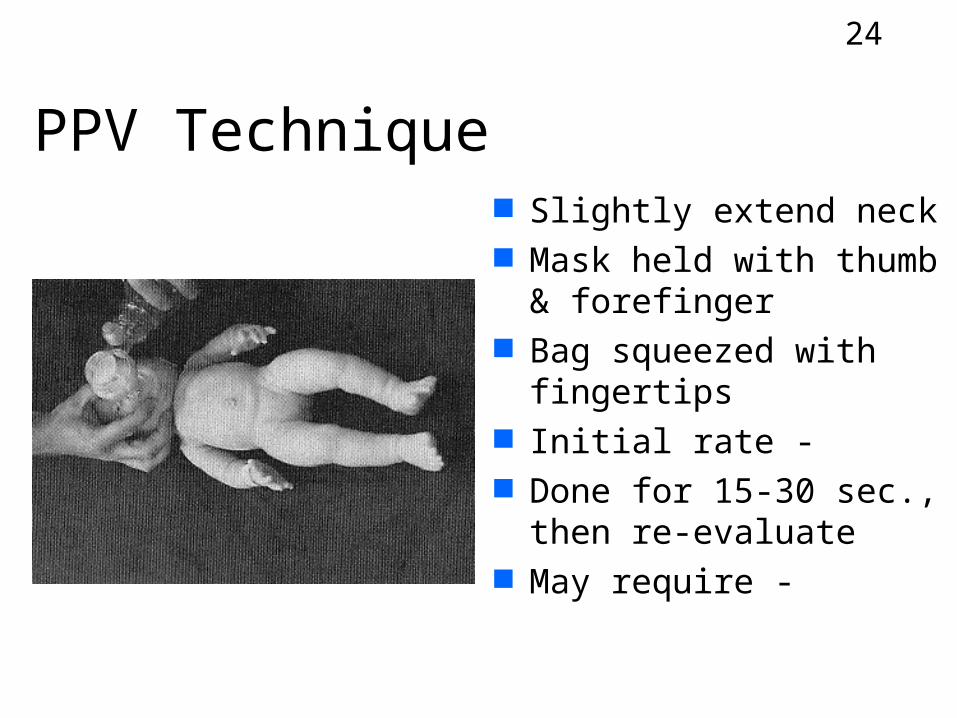
PPV Technique Slightly extend neck Mask held with thumb &
forefinger Bag squeezed with
fingertips Initial rate - Done for 15-30 sec.,
then re-evaluate May require -
25
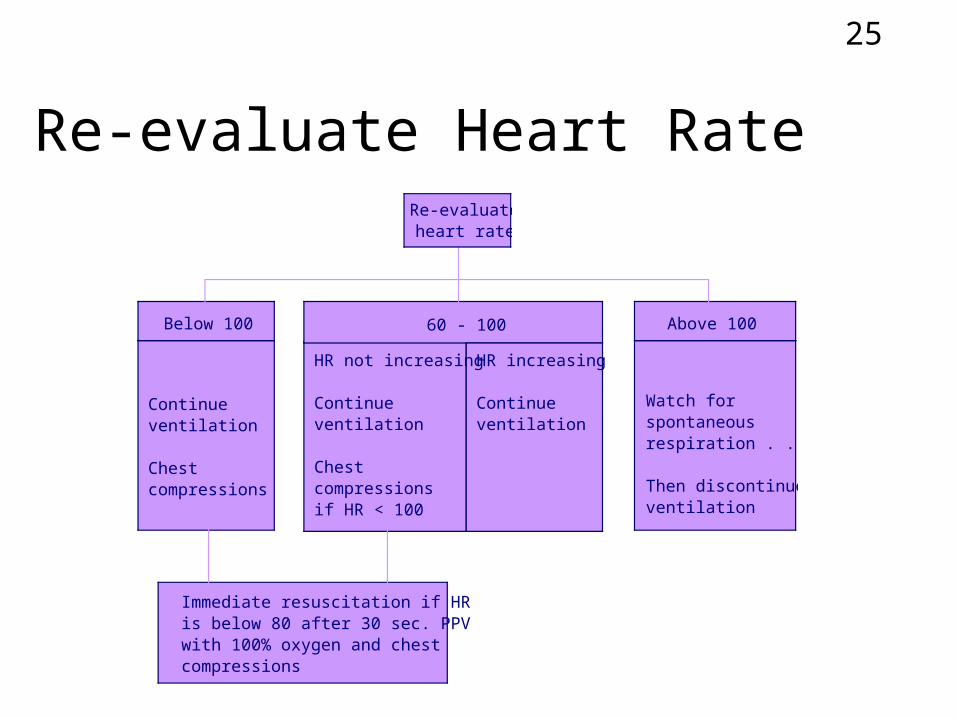
Re-evaluate Heart Rate
Below 100
Continueventilation
Chestcompressions
60 - 100
HR not increasing
Continueventilation
Chestcompressionsif HR < 100
HR increasing
Continueventilation
Above 100
Watch forspontaneousrespiration . . .
Then discontinueventilation
Immediate resuscitation if HRis below 80 after 30 sec. PPVwith 100% oxygen and chestcompressions
Re-evaluateheart rate
26
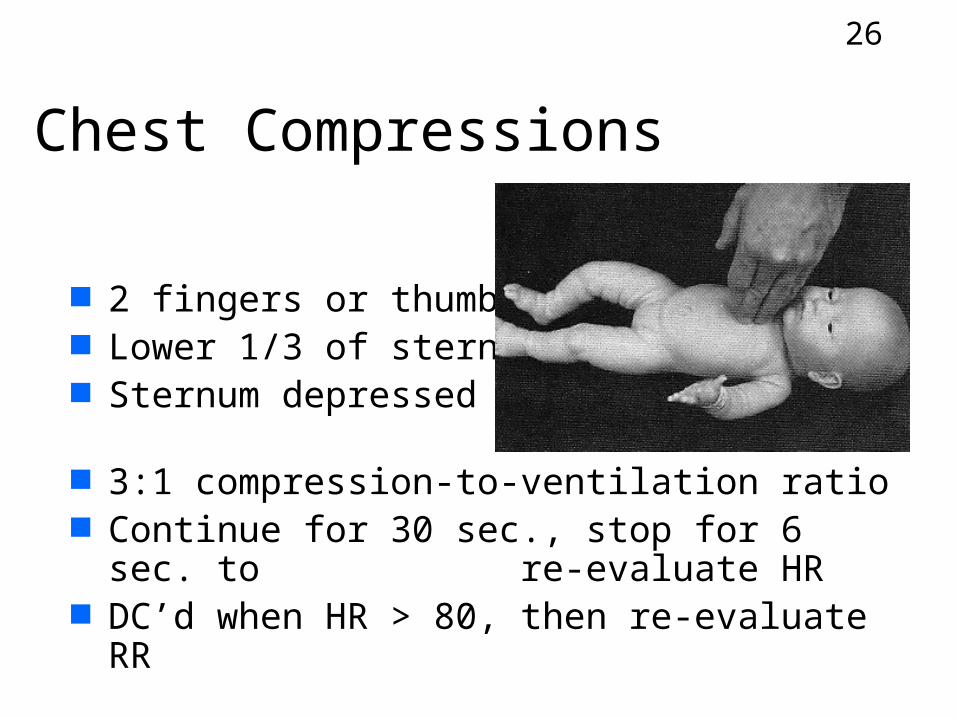
Chest Compressions
2 fingers or thumbs Lower 1/3 of sternum Sternum depressed
1/2-3/4 inches 3:1 compression-to-ventilation ratio Continue for 30 sec., stop for 6 sec. to
re-evaluate HR DC’d when HR > 80, then re-evaluate RR
27
Indications for Intubation
Bag/mask ventilation is difficult or ineffective
Prolonged PPV is required Thick meconium is present in amniotic
fluid Suspicion of diaphragmatic hernia
28
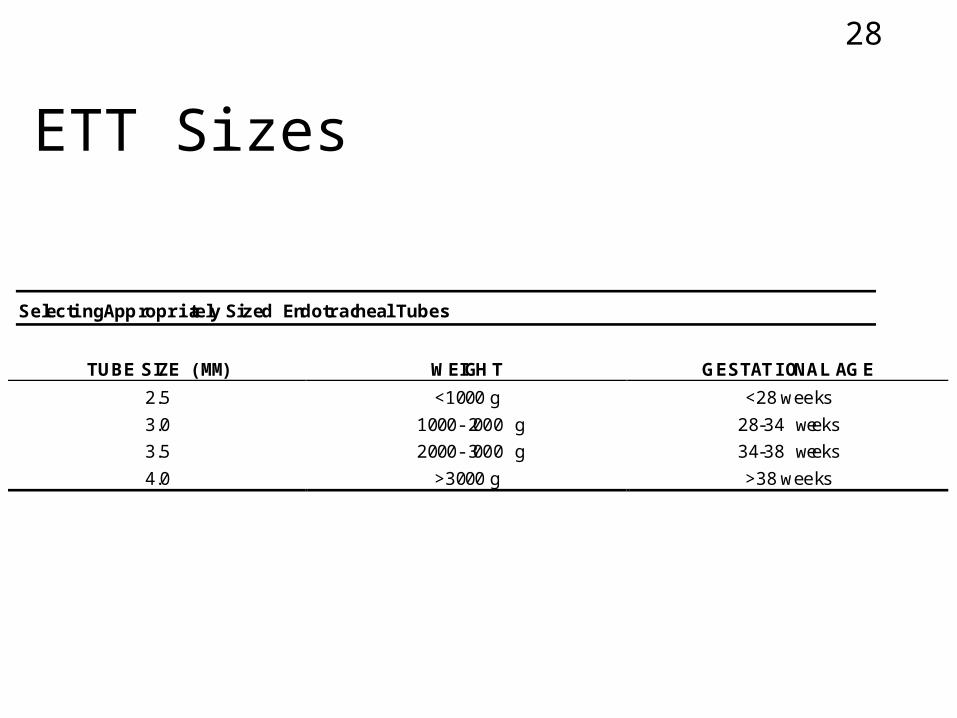
ETT Sizes
Selecting Appropriately Sized Endotracheal Tubes
TUBE SIZE (MM) WEIGHT GESTAT IONAL AGE
2.5 <1000 g <28 weeks
3.0 1000-2000 g 28-34 weeks
3.5 2000-3000 g 34-38 weeks
4.0 >3000 g >38 weeks
29
Laryngoscope Blades
Size 1 for
Size 0 for
30
Intubation Technique
Same as adult
Limit attempts to -
Provide blow-by oxygen at -
ETT tip midway between carina &
clavicles
Cut ETT to leave -
31
Medications - Uses
32
Medications - Routes
33
Instillation Into ETT
N N A A V V E E L L
OO22
34
Medications - Indications
HR < 80 despite PPV and chest compressions for at least 30 sec.
HR is 0
35
Epinephrine
Powerful sympathomimetic
–
–
– 1st drug given IV or ETT, delivered rapidly Repeated q3-5’ until HR -
36
Volume Expanders
Given if hypovolemic BP– Pallor with adequate oxygenation– HR > 100 with weak pulses– Failure to respond to resuscitation
Whole blood, 5% albumin, plasma expanders, NS
IV, may be repeated as needed
37
Sodium Bicarbonate
Prolonged arrest & not responding
Alkaline to buffer metabolic acidosis
Only given when ventilation is adequate
IV
38
Narcan (naloxone)
Reversal of narcotic depression– Demerol (meperidine)– Morphine sulfate– Fentanyl (Sublimaze)
IV, IM, sub-q, ETT
Given rapidly
39
Dopamine
40
APGAR Scoring
41
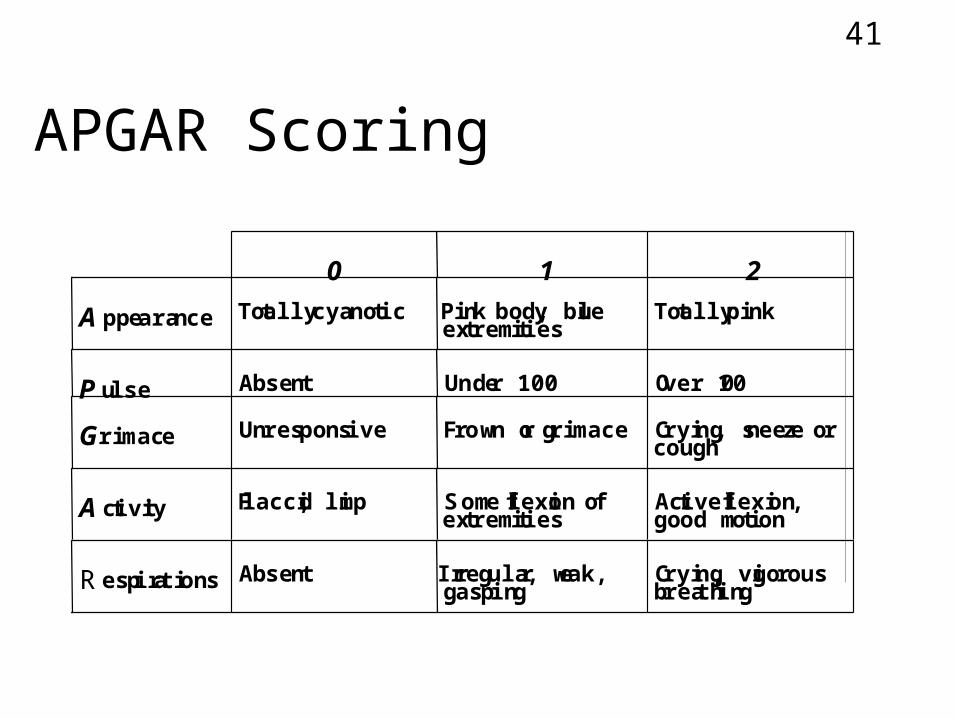
APGAR Scoring
0 1 2
A ppearance Totally cyanotic Pink body, blueextremities
Totally pink
P ulse Absent Under 100 Over 100
G rimace Unresponsive Frown or grimace Crying, sneeze orcough
A ctivity Flaccid, limp Some flexion ofextremities
Active flexion,good motion
R espirations Absent Irregular, weak,gasping
Crying, vigorousbreathing
42
Serum Glucose
Nutritional needs of fetus supplied by Mom & regulated by placenta
Fetus prepares for postnatal life by energy stores & developing enzyme-dependant processes for usage of stored energy
Sources
43
Serum Glucose
Glycogen– –
Triglycerides (brown fat)– –
Energy Storage
44
Serum Glucose
At 2 hours -
By 3 days -
Post-delivery
45
Serum Glucose
Term -
Preterm -
Hypoglycemia
46
Hypoglycemia - Signs
Tremors Irritability orMoro reflex Apnea/tachypnea Cyanosis Seizures
Lethargy Hypothermia Weak/high-pitched cry Poor feeding Vomiting CV failure
47
Hypoglycemia
CNS dysfunction Apnea Death
Hypoglycemia
48
Hypoglycemia - Causes
Hyperinsulinism Prematurity IUGR Starvation Sepsis Shock Asphyxia
Hypothermia Glucogen Storage Disease Galactosemia Adrenal insufficiency Polycythemia Congenital heart defects Iatrogenic causes
49
Hyperinsulinism
Fetus of diabetic Mom
Rh incompatibility
Insulin-producing tumors
Maternal tocolytic therapy (ritodrine,
terbutaline)
50
Glucose Measurement
Glucose Test Strip “Dextrostik”
“One Touch”
Lab sample (blood glucose)
51
Hypoglycemia Treatment
Early feeding (oral) D10W
– 200 mg/kg bolus over 1-3 minutes– Con’t IV, 4-8 mg/kg/min. until feedings
started Treat cause
52
Umbilical Blood Sampling
53
Umbilical Vein Catheter (UVC)
Usually placed in -
Drug administration during -
54
Umbilical Artery Catheter (UAC)
Indications
55
Umbilical Artery Catheter (UAC)
5 Fr. catheter (>1250 g), 3.5 Fr. catheter (<1250 g)
Sterile procedure Heparinized-filled catheter Tip L3-4 for low catheter, T8 for high
catheter (in aorta below renal a., above bifurcation of femoral a.)
PlacementPlacement

56
UAC
57
Umbilical Artery Catheter
Complications
58
Umbilical Artery Catheter
Sampling Technique