Pediatrics Controlling Asthma at School Fadel Ruiz MD Pediatric Pulmonary Baylor College of Medicine...
75
Pediatrics Controlling Asthma at School Fadel Ruiz MD Fadel Ruiz MD Pediatric Pulmonary Pediatric Pulmonary Baylor College of Medicine Baylor College of Medicine Texas Children’s Hospital Texas Children’s Hospital
-
Upload
stewart-wells -
Category
Documents
-
view
216 -
download
1
Transcript of Pediatrics Controlling Asthma at School Fadel Ruiz MD Pediatric Pulmonary Baylor College of Medicine...
Pediatrics
Controlling Asthma at School
Fadel Ruiz MDFadel Ruiz MD
Pediatric PulmonaryPediatric Pulmonary
Baylor College of MedicineBaylor College of Medicine
Texas Children’s HospitalTexas Children’s Hospital
Page 2
xxx00.#####.ppt 04/19/23 12:56 PMPediatrics
ObjectivesObjectives• Review basic facts about asthma•Understand basics of asthma treatment •Review how to recognize control and uncontrolled asthma
•Review goals and policies for the management of asthma in the school setting
•Review proper use of inhalers and spacers•Practical (hands/on) review of use of inhalers and spacers
Page 3
xxx00.#####.ppt 04/19/23 12:56 PMPediatrics
Epidemiology•Asthma is the most common chronic health problem in childhood. (7.1 million children ≤18 year) ,10% of children
•4.1 million had an asthma episode or attack within the previous year in 2011
•Most common reason for school absence(12.8 million school days and costs caretakers $726.1 million because of work absence.)
•$ 3.2 billion per year to treat childhood asthma
http://www.cdc.gov/healthyyouth/asthma/(2009) and 2010)
ALA ; asthma & children fact sheet: October 2012

Page 4
xxx00.#####.ppt 04/19/23 12:56 PMPediatrics
Epidemiology
•Life- threatening disease‐3388 deaths attributed to asthma in 2009
•3rd leading cause of hospitalizations <15 years age
•400,000 to 1 million children with worse asthma due to 2nd hand smoke exposure
ALA ; asthma & children fact sheet: October 2012

Page 5
xxx00.#####.ppt 04/19/23 12:56 PMPediatrics
3 or more children are likely to have asthma
In a classroom of 30 children,
Page 6
xxx00.#####.ppt 04/19/23 12:56 PMPediatrics
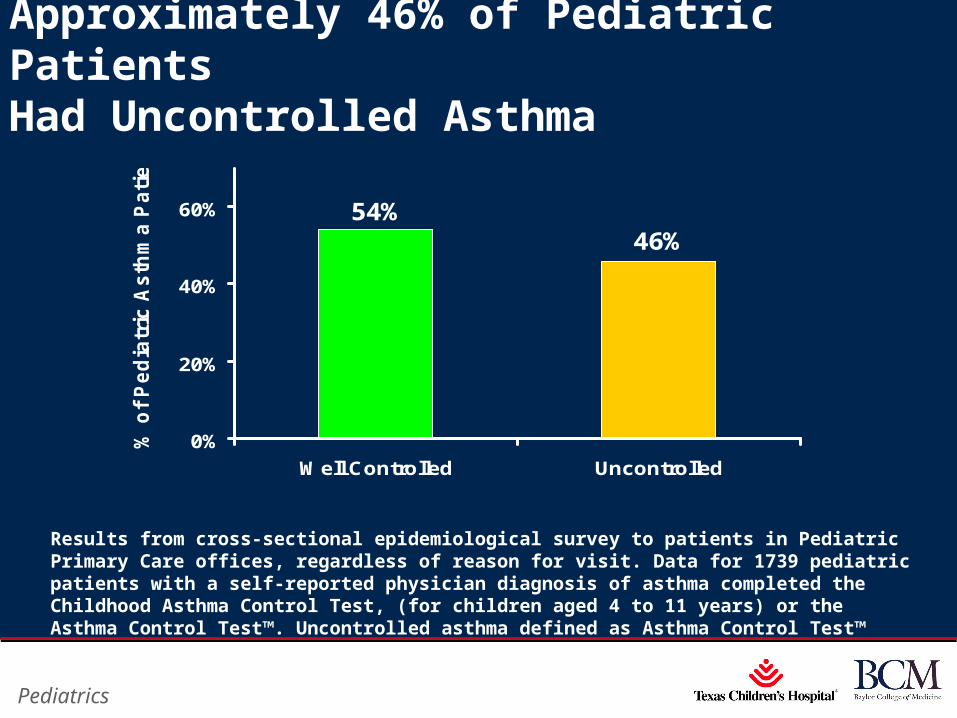
Approximately 46% of Pediatric Patients Had Uncontrolled Asthma
46%54%
0%
20%
40%
60%
Well Controlled Uncontrolled
% o
f P
ed
iatr
ic A
sth
ma
Pa
tie
nts
Results from cross-sectional epidemiological survey to patients in Pediatric Primary Care offices, regardless of reason for visit. Data for 1739 pediatric patients with a self-reported physician diagnosis of asthma completed the Childhood Asthma Control Test, (for children aged 4 to 11 years) or the Asthma Control Test™. Uncontrolled asthma defined as Asthma Control Test™ ≤19. Asthma Control Test is a trademark of QualityMetric Incorporated.
Page 7
xxx00.#####.ppt 04/19/23 12:56 PMPediatrics
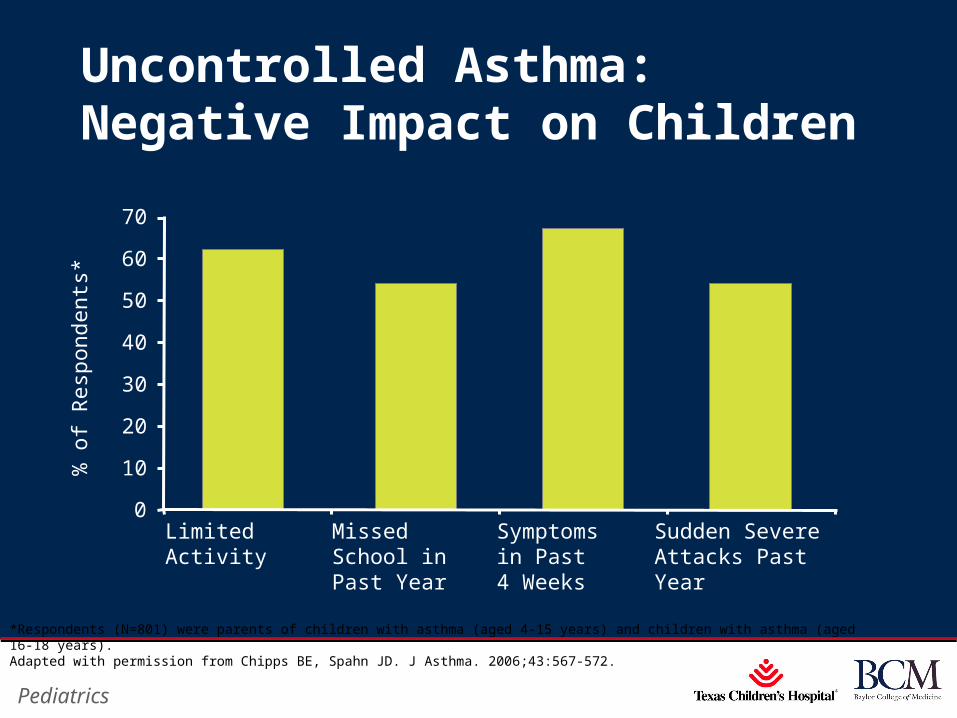
Uncontrolled Asthma: Negative Impact on Children
0
10
20
30
40
50
60
70
Limited Activity Symptomsin Past4 Weeks
MissedSchool inPast Year
Sudden Severe Attacks PastYear
% o
f Res
pond
ents
*
*Respondents (N=801) were parents of children with asthma (aged 4-15 years) and children with asthma (aged 16-18 years).Adapted with permission from Chipps BE, Spahn JD. J Asthma. 2006;43:567-572.
Page 9
xxx00.#####.ppt 04/19/23 12:56 PMPediatrics
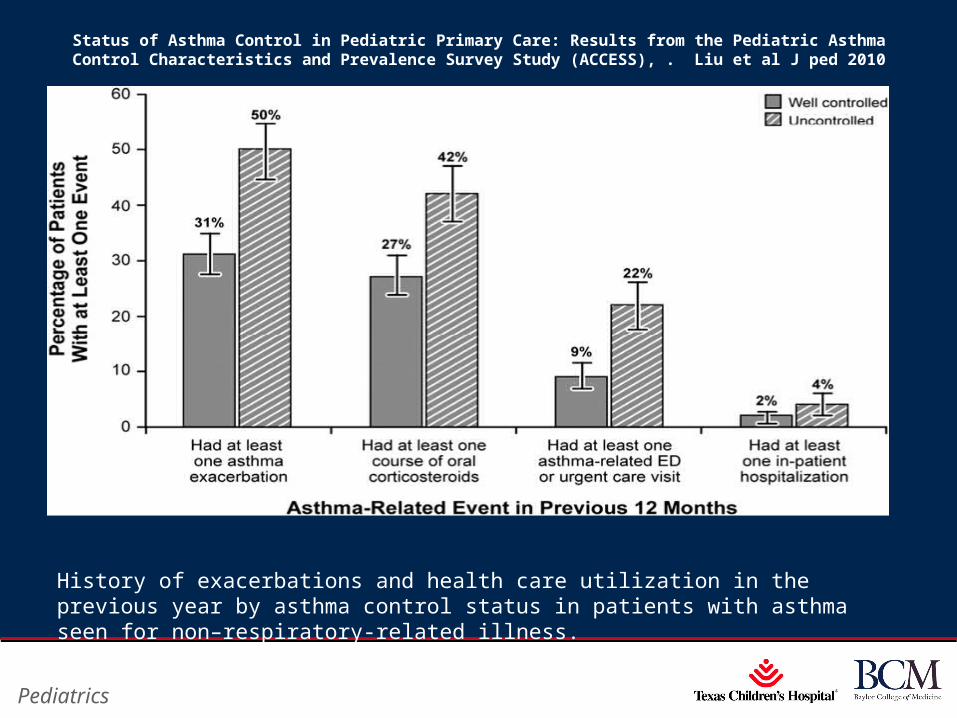
History of exacerbations and health care utilization in the previous year by asthma control status in patients with asthma seen for non–respiratory-related illness.
Status of Asthma Control in Pediatric Primary Care: Results from the Pediatric Asthma Control Characteristics and Prevalence Survey Study (ACCESS), . Liu et al J ped 2010
Page 10
xxx00.#####.ppt 04/19/23 12:56 PMPediatrics
What is Asthma?
A disease that:
‐ Is chronic
‐ Produces recurring episodes of breathing problems
• Coughing
• Wheezing
• Chest tightness
• Shortness of breath
‐ Cannot be cured, but can be controlled
Page 11
xxx00.#####.ppt 04/19/23 12:56 PMPediatrics
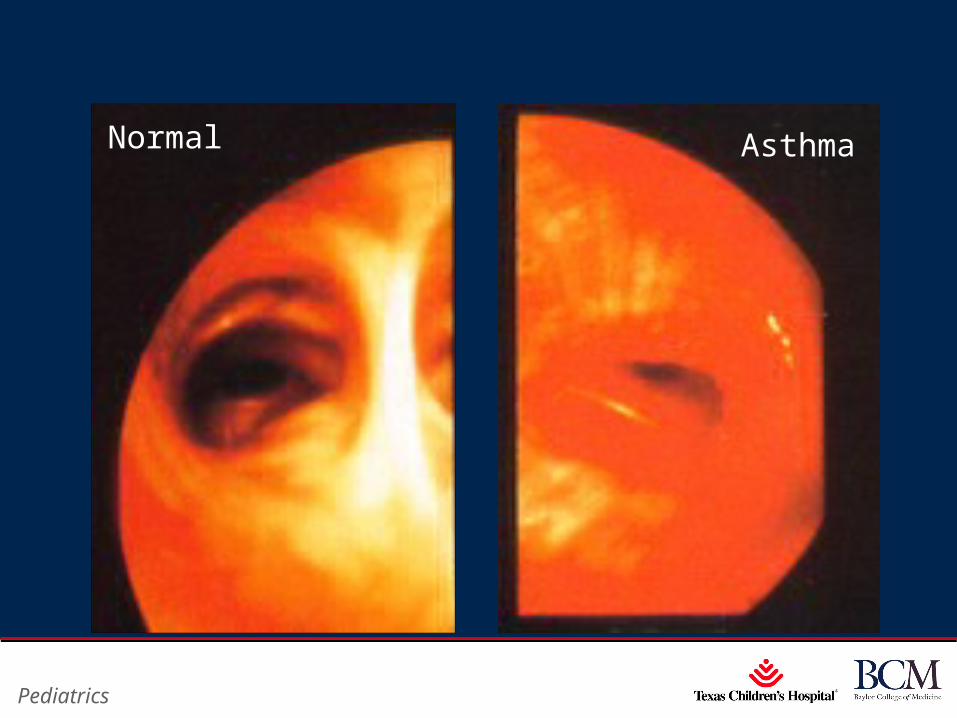
AsthmaNormal

Page 12
xxx00.#####.ppt 04/19/23 12:56 PMPediatrics
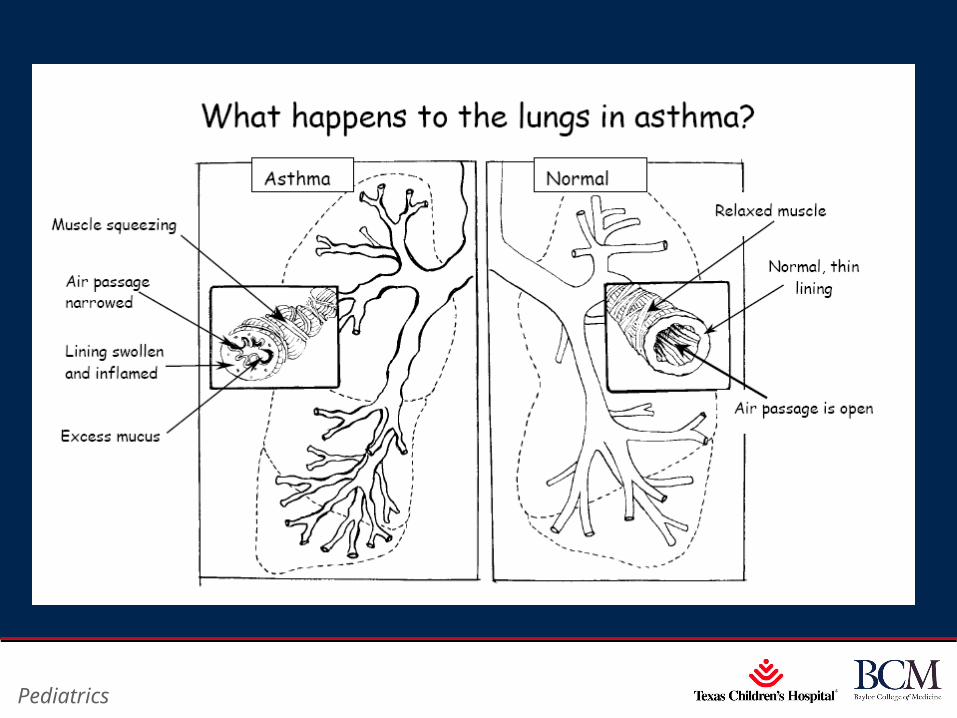
Pathophysiology of Asthma
Inflammation Bronchoconstriction
Reduced airway opening
Muscle Layer
Excess Mucus
BRONCHIOLE
Tightened muscle
Alveolus filled with trapped air
Page 13
xxx00.#####.ppt 04/19/23 12:56 PMPediatrics
Page 14
xxx00.#####.ppt 04/19/23 12:56 PMPediatrics
What Happens During an Episode of Asthma?•The lining of the airways becomes swollen (inflamed)
•The airways produce a thick mucus
•The muscles around the airways tighten and make airways narrower
Page 15
xxx00.#####.ppt 04/19/23 12:56 PMPediatrics
What are the Symptoms of Asthma?
‐Shortness of breath
‐Wheezing
‐Tightness in the chest
‐Coughing at night or after physical activity; cough that lasts more than a week
‐Waking at night with asthma symptoms (a key marker of uncontrolled asthma)

Page 16
xxx00.#####.ppt 04/19/23 12:56 PMPediatrics
Evaluation in Children: History
•“Noisy symptoms”
‐ Wheezing
• Timing and pattern
• Age of onset
• Acute or chronic
• Associated factors
‐ Cough
• “Quiet” symptoms
‐ Chest tightness
‐ Chest pain
‐ Fatigue with exertion
‐ Irritability
• Symptom frequency & severity
‐ Limitation of physical activity
‐ Interference with sleep
‐ ED visits/hospitalizations
• Course
‐ Intermittent vs chronic
‐ Recurrent
• Past medical history
‐ β-Adrenergic responsiveness
‐ Family history
‐ Atopy
‐ Social/environmental historyNational Asthma Education and Prevention Program. Expert Panel Report 2: Guidelines for the Diagnosis and Management of Asthma. National Heart, Lung, and Blood Institute, National Institutes of Health; July 1997. NIH publication 97-4051.
Page 17
xxx00.#####.ppt 04/19/23 12:56 PMPediatrics
Evaluation in Children: Physical Examination
•Physical examination maybe normal
•Skin
‐Atopic dermatitis
•HEENT
‐Allergic facies
‐Pharyngeal cobblestoning
‐Nasal voice
‐Mouth breathing
‐Pale/swollen nasal mucosa
‐Clear nasal discharge
•Chest/lungs (at rest and with forced expiration)
‐Tachypnea
‐ Inspiratory vs expiratory
‐Prolonged expiratory phase
‐Decreased air entry
‐Wheeze/cough
•During exacerbations only‐Accessory muscle use
‐Hyperexpansion of thorax
‐Cyanosis
•Not associated with asthma‐Digit clubbing
‐ Isolated “crackles”
‐Stridor without wheeze
HEENT = head, ears, eyes, nose, throat.National Asthma Education and Prevention Program. Expert Panel Report 2: Guidelines for the Diagnosis and Management of Asthma. National Heart, Lung, and Blood Institute, National Institutes of Health; July 1997. NIH publication 97-4051.
Page 18
xxx00.#####.ppt 04/19/23 12:56 PMPediatrics
Asthma Imitators
‐Cystic fibrosis
‐Gastroesophageal reflux
‐Chronic lung disease of prematurity
‐Aerodigestive foreign body
‐Congenital airway anomaly
‐Immunodeficiency
‐Congenital heart disease
‐Vocal cord dysfunction
Page 19
xxx00.#####.ppt 04/19/23 12:56 PMPediatrics
Goals of Asthma Care
No asthma symptoms. No cough. No wheeze. No chest tightness.
No limitation of exercise.
No asthma attacks: daytime or nighttime!
No need for urgent or emergency care.
Page 20
xxx00.#####.ppt 04/19/23 12:56 PMPediatrics
3 lines of defense
•1) Manage THE ENVIRONMENT
Keep asthma triggers away. ‐Irritants
•smoke, strong chemicals, and cold viruses
‐ Allergens
•dusts, molds, pollens, furry or feathered pets, cockroaches, and rodents

Page 21
xxx00.#####.ppt 04/19/23 12:56 PMPediatrics
Asthma Triggers
•Allergens‐Warm-blooded pets (including dogs, cats, birds, and small rodents)
‐House dust mites
‐Cockroaches
‐Pollens from grass and trees
‐Molds (indoors and outdoors)

Page 22
xxx00.#####.ppt 04/19/23 12:56 PMPediatrics
Control of TriggersControl of Triggers
Oak Timothy
Mites Fungi Cockroach
Mountain cedar Ragweed
Cat

Page 23
xxx00.#####.ppt 04/19/23 12:56 PMPediatrics
Asthma Triggers
•Irritants‐Cigarette smoke and wood smoke
‐Scented products such as hair spray, cosmetics, and cleaning products
‐Strong odors from fresh paint or cooking
‐Automobile fumes and air pollution
‐Chemicals such as pesticides and lawn treatments
•Infections ‐Colds & Flu
Page 24
xxx00.#####.ppt 04/19/23 12:56 PMPediatrics
Asthma Triggers

Page 25
xxx00.#####.ppt 04/19/23 12:56 PMPediatrics
Asthma Triggers
Page 26
xxx00.#####.ppt 04/19/23 12:56 PMPediatrics
Asthma Triggers

Page 27
xxx00.#####.ppt 04/19/23 12:56 PMPediatrics
Asthma Triggers
Page 28
xxx00.#####.ppt 04/19/23 12:56 PMPediatrics
3 lines of defense
•2) Protect THE BREATHING TUBES
‐Long acting asthma controller medicine taken every day.
‐Rule of 2’s for well controlled asthma
•Needs quick relief inhaler < 2x/week
•Sleep interrupted from asthma <2x/month

Page 29
xxx00.#####.ppt 04/19/23 12:56 PMPediatrics
ACT ( Asthma Control Test)•Reliable, valid, and responsive to changes in asthma control over time
•A cutoff score of 19 or less identifies patients with poorly controlled asthma.
•Useful tool to identify patients with uncontrolled asthma and to follow progress with treatment.
Schatzet al J Allergy Clin Immunol 2006;117:549-56.
Page 30
xxx00.#####.ppt 04/19/23 12:56 PMPediatrics
Pharmacotherapy
Long-Term ControlLong-Term Control
•Corticosteroids
•Leukotriene modifiers
•Long-acting beta2-agonists
•Methylxanthines
•Cromolyn/nedocromil
Quick ReliefQuick Relief
•Short-acting inhaled beta2-agonists
•Anticholinergics
•Systemic corticosteroids
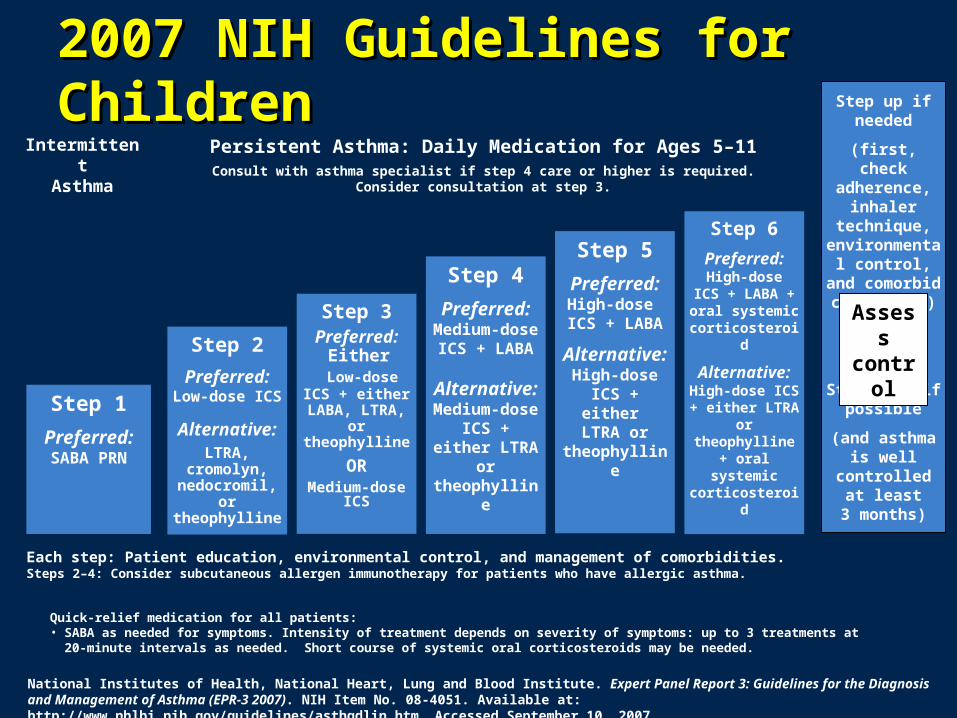
IntermittentAsthma
Persistent Asthma: Daily Medication for Ages 5–11Consult with asthma specialist if step 4 care or higher is required.
Consider consultation at step 3.
Step 1
Preferred:SABA PRN
Step 2
Preferred:Low-dose ICS
Alternative:LTRA,
cromolyn, nedocromil, or theophylline
Step 3Preferred:
Either Low-dose ICS + either LABA,
LTRA, or theophylline
ORMedium-dose
ICS
Step 5
Preferred:High-dose
ICS + LABA
Alternative:High-dose ICS
+ either LTRA or
theophylline
Step 6
Preferred:High-dose
ICS + LABA + oral systemic corticosteroid
Alternative:High-dose ICS + either LTRA or theophylline + oral systemic corticosteroid
Step up if needed
(first, check adherence,
inhaler technique, environmental
control, and comorbid
conditions)
Step down if possible
(and asthma is well controlled at
least3 months)
Each step: Patient education, environmental control, and management of comorbidities.Steps 2–4: Consider subcutaneous allergen immunotherapy for patients who have allergic asthma.
Step 4
Preferred:Medium-dose ICS + LABA
Alternative:Medium-dose ICS + either LTRA or theophylline
Assess control
Quick-relief medication for all patients:• SABA as needed for symptoms. Intensity of treatment depends on severity of symptoms: up to 3 treatments at 20-
minute intervals as needed. Short course of systemic oral corticosteroids may be needed.
National Institutes of Health, National Heart, Lung and Blood Institute. Expert Panel Report 3: Guidelines for the Diagnosis and Management of Asthma (EPR-3 2007). NIH Item No. 08-4051. Available at: http://www.nhlbi.nih.gov/guidelines/asthgdlin.htm. Accessed September 10, 2007.
2007 NIH Guidelines for Children2007 NIH Guidelines for Children

Page 32
xxx00.#####.ppt 04/19/23 12:56 PMPediatrics
Daily Albuterol Users Not on a Controller Experience More Frequent Activity Limitation
12%
36%
0
20
40
60
Daily Albuterol Not Daily Albuterol
% o
f S
ub
jects
Lim
itin
g
Ph
ysic
al
Acti
vit
y
Q3c: How much do exercise – or exertion-related asthma symptoms limit your participation in sports or other vigorous activities – some or a lot?

Page 33
xxx00.#####.ppt 04/19/23 12:56 PMPediatrics
1 in 4 Daily Albuterol Users Not on a Controller Said “Asthma Controls Me and My Life”
6
25
0
20
40
Daily Albuterol Not Daily Albuterol
% o
f S
ub
jects
Q20: Please indicate how strongly you agree or disagree with the following statement:Asthma controls me and my life.
%
%
Page 34
xxx00.#####.ppt 04/19/23 12:56 PMPediatrics
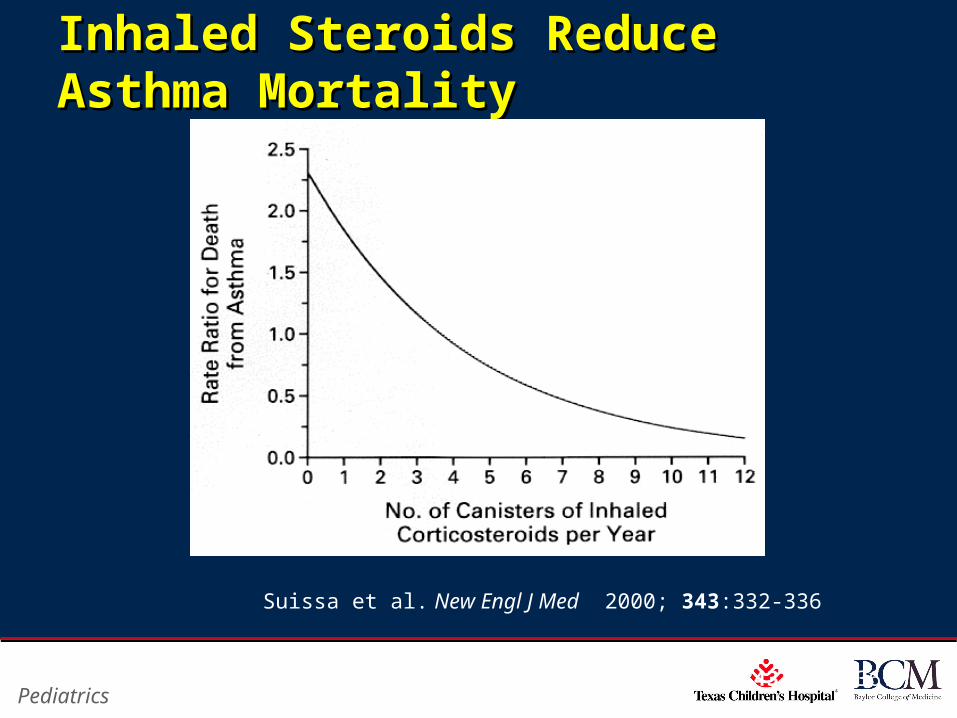
Inhaled Steroids Reduce Asthma Inhaled Steroids Reduce Asthma MortalityMortality
Suissa et al. New Engl J Med 2000; 343:332-336.
Suissa et al. New Engl J Med 2000; 343:332-336

Page 35
xxx00.#####.ppt 04/19/23 12:56 PMPediatrics
Relative Risk of Asthma Hospitalization in the United States
Donahue et al. JAMA. 1997;277:887-891.
Prescriptions per person-year
RelativeRisk
None 1-2 2-3 3-5 5-8 8+0-1
2-agonists
Total
ICS
0
1
2
3
4
5
6
7
8
Age 0-17Age 18-44Age 45+
TotalAge 0-17Age 18-44Age 45+

Page 36
xxx00.#####.ppt 04/19/23 12:56 PMPediatrics
Before and After 3 Months of Treatment With an ICS
Reprinted with permission from Laitinen LA et al. J Allergy Clin Immunol. 1992;90:32-42. Copyright (1992), with permission from the American Academy of Allergy, Asthma and Immunology.
Effects of Inhaled Corticosteroids on Inflammation
Before After
Epithelium
BasementMembrane
Eosinophil
Lymphocytes
Mast Cells
Epithelium
BasementMembrane

Page 37
xxx00.#####.ppt 04/19/23 12:56 PMPediatrics
Benefits of ICSBenefits of ICS• Reduces symptom severity
• Improves pulmonary function
• Reduces bronchial hyperreactivity and airway inflammation
• Reduces rescue inhaler use
• Reduces exacerbations, hospitalizations and asthma-related mortality
• The safety of these agents when used correctly is well-established in all age groups.
Guidelines for the Diagnosis and Management of Asthma. 1997. NIH Publication No. 97-4051
Guidelines for the Diagnosis and Management of Asthma. 1997. NIH Publication No. 97-4051.
Page 38
xxx00.#####.ppt 04/19/23 12:56 PMPediatrics
3 lines of defense
•3) Anticipate THE FLARE UPS‐Know the early signs of asthma.
‐Doctors should provide a written asthma action plan (also called a green, yellow, red zone plan) for each child with asthma.

Page 39
xxx00.#####.ppt 04/19/23 12:56 PMPediatrics
Good asthma care providers give Written Asthma Action Plans
Page 40
xxx00.#####.ppt 04/19/23 12:56 PMPediatrics
Recognizing Symptoms
Page 41
xxx00.#####.ppt 04/19/23 12:56 PMPediatrics
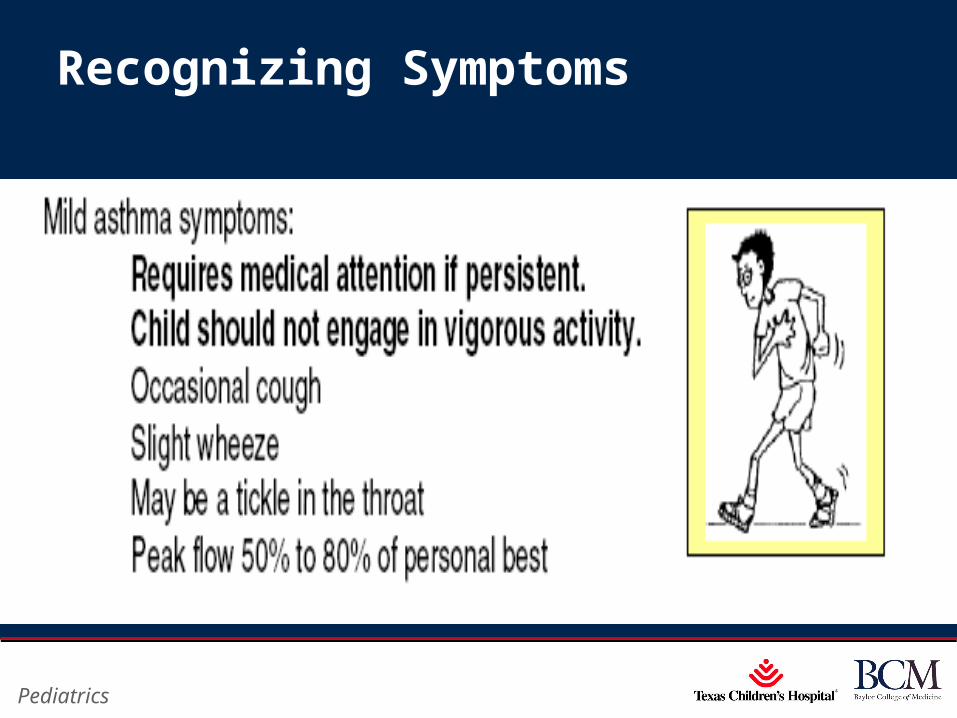
Recognizing Symptoms
Page 42
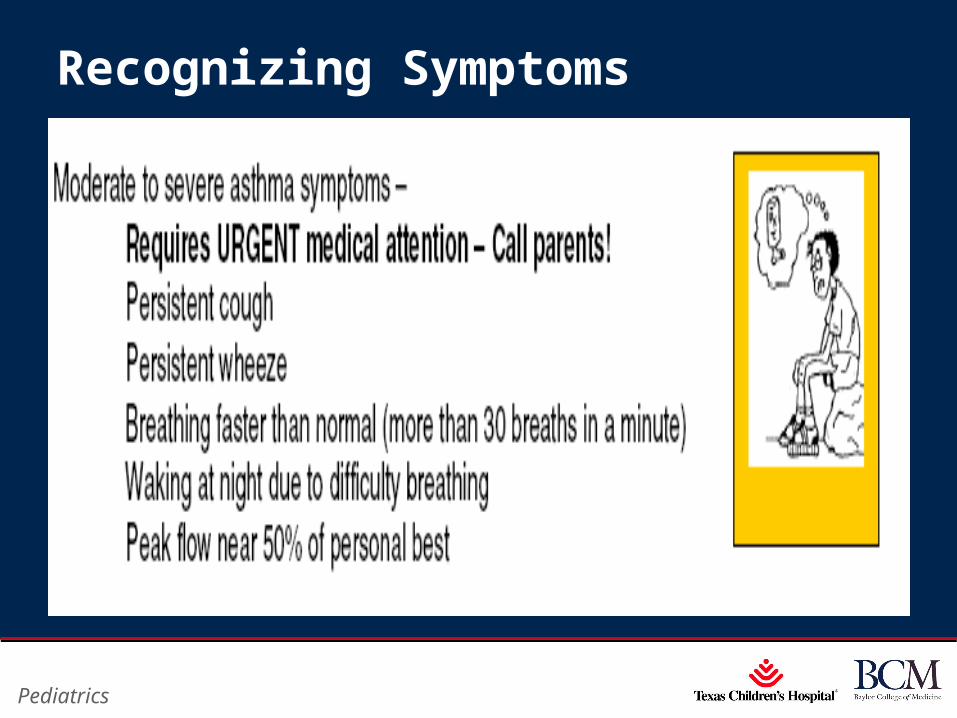
xxx00.#####.ppt 04/19/23 12:56 PMPediatrics
Recognizing Symptoms
Page 43
xxx00.#####.ppt 04/19/23 12:56 PMPediatrics
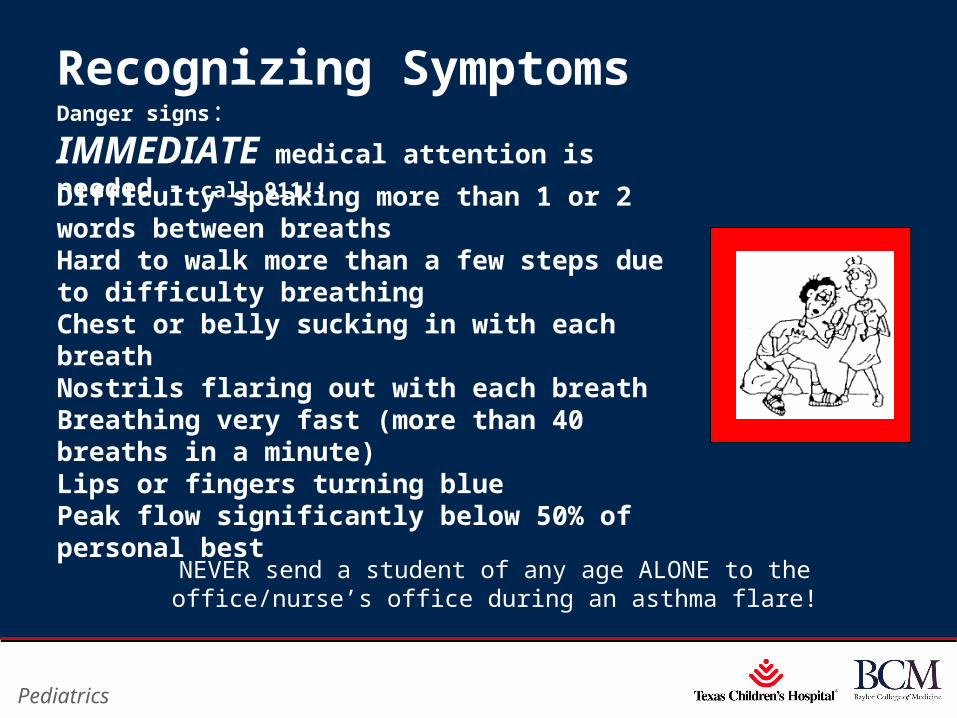
Recognizing Symptoms
NEVER send a student of any age ALONE to the office/nurse’s office during an asthma flare!
Danger signs:
IMMEDIATE medical attention is needed – call 911!!
Difficulty speaking more than 1 or 2 words between breathsHard to walk more than a few steps due to difficulty breathingChest or belly sucking in with each breathNostrils flaring out with each breathBreathing very fast (more than 40 breaths in a minute)Lips or fingers turning bluePeak flow significantly below 50% of personal best
Page 44
xxx00.#####.ppt 04/19/23 12:56 PMPediatrics
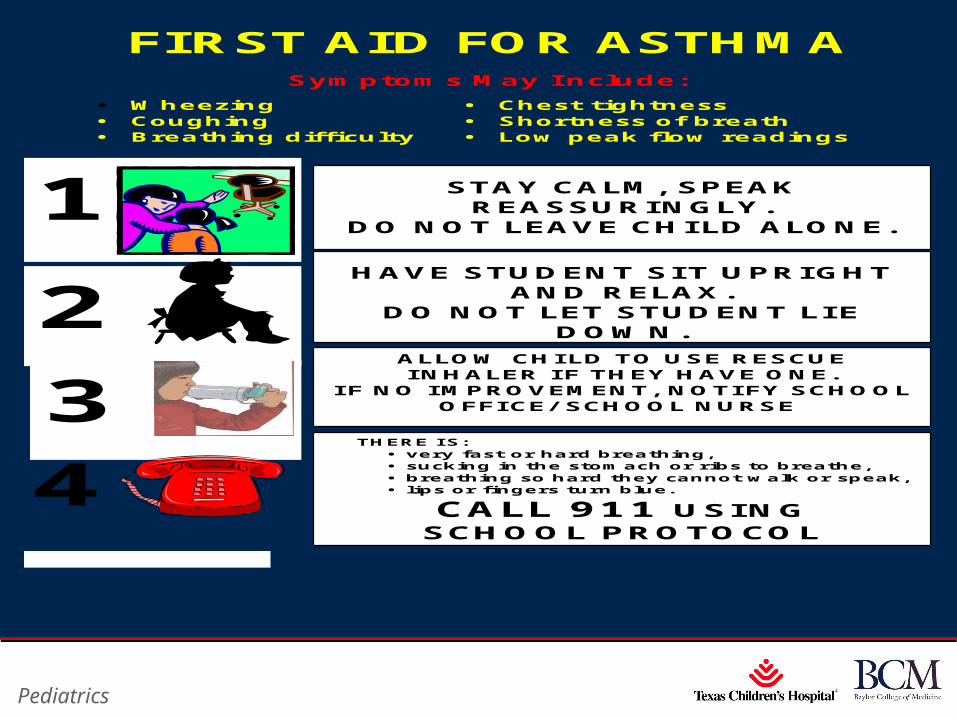
FIRST AID FOR ASTHMA
Symptoms May Include:
• Wheezing • Chest tightness • Coughing • Shortness of breath • Breathing difficulty • Low peak flow readings
4
1
STAY CALM, SPEAK REASSURINGLY.
DO NOT LEAVE CHILD ALONE.
3
2
HAVE STUDENT SIT UPRIGHT AND RELAX.
DO NOT LET STUDENT LIE DOWN.
ALLOW CHI LD TO USE RESCUE I NHALER I F THEY HAVE ONE.
I F NO I MPROVEMENT, NOTI FY SCHOOL OFFI CE/ SCHOOL NURSE.
I F THERE IS: • very fast or hard breathing, • sucking in the stomach or ribs to breathe, • breathing so hard they cannot walk or speak, • lips or fingers turn blue.
CALL 911 USING SCHOOL PROTOCOL
Page 45
xxx00.#####.ppt 04/19/23 12:56 PMPediatrics
Control of Environmental FactorsControl of Environmental Factors
•House-dust mites‐Encase mattress and pillow in impermeable cover
‐Wash bedding weekly in hot water‐Reduce indoor humidity < 50 %‐Remove dust “collectors” from room
•Animal Dander‐Remove animal from house‐Keep out of patient’s bedroom and off fabric furniture
‐Filter on bedroom air duct
Page 46
xxx00.#####.ppt 04/19/23 12:56 PMPediatrics
Control of Environmental Factors‐Indoor Mold
• Fix leaky faucets and pipes
• Avoid humidifiers
• Reduce humidity < 50 %
‐Cockroaches
• Traps
• Preventative measures
Page 47
xxx00.#####.ppt 04/19/23 12:56 PMPediatrics
Precipitating / Sustaining Factorsfor Asthma
‐Allergen exposure
‐Allergic Rhinitis
‐Exercise
‐Viral URI’s
‐Rhinosinusitis
‐GERD
‐Cigarette smoke
‐Environmental exposures (eg, pollution, fumes)
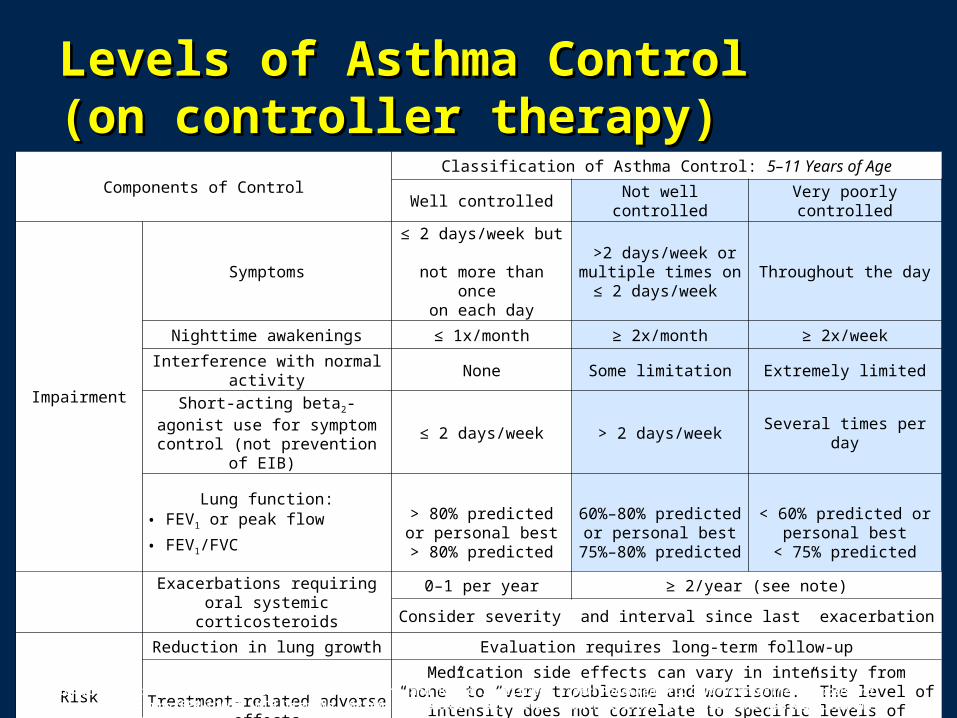
Levels of Asthma Control Levels of Asthma Control (on controller therapy)(on controller therapy)
Components of ControlClassification of Asthma Control: 5–11 Years of Age
Well controlled Not well controlled Very poorly controlled
Impairment
Symptoms≤ 2 days/week but not more than once
on each day
>2 days/week or multiple times on ≤ 2 days/week
Throughout the day
Nighttime awakenings ≤ 1x/month ≥ 2x/month ≥ 2x/week
Interference with normal activity None Some limitation Extremely limited
Short-acting beta2-agonist use for symptom control (not prevention of
EIB) ≤ 2 days/week > 2 days/week Several times per day
Lung function:• FEV1 or peak flow
• FEV1/FVC
> 80% predicted or personal best
> 80% predicted
60%–80% predicted or personal best
75%–80% predicted
< 60% predicted or personal best
< 75% predicted
Exacerbations requiring oral systemic corticosteroids
0–1 per year ≥ 2/year (see note)
Consider severity and interval since last exacerbation
Risk
Reduction in lung growth Evaluation requires long-term follow-up
Treatment-related adverse effectsMedication side effects can vary in intensity from “none” to “very troublesome and worrisome.” The level of intensity does not correlate to specific levels of control but
should be considered in the overall assessment of risk
National Institutes of Health, National Heart, Lung and Blood Institute. Expert Panel Report 3: Guidelines for the Diagnosis and Management of Asthma (EPR-3 2007). NIH Item No. 08-4051. Available at: http://www.nhlbi.nih.gov/guidelines/asthgdlin.htm. Accessed September 10, 2007.
Page 49
xxx00.#####.ppt 04/19/23 12:56 PMPediatrics
What are the main reasons for poor control of asthma?
•Misdiagnosis•Under treatment with anti inflammatory meds•Over reliance on short acting B-agonist•Presence of other coexisting conditions
‐GERD (gastroesophageal reflux)‐Sinusitis‐Allergic rhinitis‐Vocal cord dysfunction
•Wrong diagnosis •Continuous exposure to allergens
Page 50
xxx00.#####.ppt 04/19/23 12:56 PMPediatrics
Achieving the GoalAchieving the GoalThe Components of Good Asthma CareThe Components of Good Asthma Care
Assessment and monitoring‐Assess asthma severity to initiate treatment
‐Assess asthma control frequently, measure lung function annually, and adjust therapy as needed
Asthma education‐Disease process, medication use, environmental avoidance, and symptom monitoring
‐Provide written asthma action plans
Page 51
xxx00.#####.ppt 04/19/23 12:56 PMPediatrics
When Asthma Control is Elusive‐Do I have the correct diagnosis?
‐Have I prescribed the proper medication?
‐What do I know about the patient’s adherence?
‐Are there concerns about aerosol delivery?
‐Do undiagnosed co-morbidities exist?
‐Are there persistent environmental allergens / irritants?

Page 52
xxx00.#####.ppt 04/19/23 12:56 PMPediatrics
Fort Bend ISD

Page 53
xxx00.#####.ppt 04/19/23 12:56 PMPediatrics
Promoting asthma Health in Schools
•Asthma is #1 cause for absence from school.
•School nurses identify asthma as the most common disease they must address.
•Asthma in school affects teachers, administrators, nurses ,coaches, and maintenance personnel
Adapted from CDC
Page 54
xxx00.#####.ppt 04/19/23 12:56 PMPediatrics
Challenges in the Schools
•To recognize and appropriately intervene with a child having an asthma flare-up.
•To reduce asthma triggers in the school
•To recognize and refer children with poorly controlled asthma.
Page 55
xxx00.#####.ppt 04/19/23 12:56 PMPediatrics
Asthma Resources For Schools• Control Your Child’s Asthma: A Breakthrough Program
for the Treatment and Management of Childhood Asthma. By Harold J. Farber, MD (Henry Holt, 2001)
• National Asthma Education and Prevention Program (NAEPP) Website and Materials
• Start at www.nhlbi.nih.gov
• Check out health information for lung diseases
• Indoor Air Quality: Tools for Schools
• http://www.epa.gov/iaq/schools/index.html
Page 56
xxx00.#####.ppt 04/19/23 12:56 PMPediatrics
Asthma Goals For SchoolHealth•Healthy school environment
•Health services in school
•Asthma education
•Supportive policies
•Sound communication
Page 57
xxx00.#####.ppt 04/19/23 12:56 PMPediatrics
Goal: Healthy School Environment
‐ Enforce no-smoking policies
‐ Reduce exposures to triggers: tobacco smoke, chemical vapors, furry or feathered animals, mites, cockroaches, chalk dust, mold
‐ Keep temperature and humidity at appropriate settings
‐ Maintain HVAC systems
‐ Dry up damp and wet areas within 1-2 days
Page 58
xxx00.#####.ppt 04/19/23 12:56 PMPediatrics
Goal: Health Services in School
•Provide full-time nursing services
•Include nursing assessments, care plans in student records
•Teach and monitor correct inhaler techniques, peak flow meter use
•Train, supervise and delegate to health assistants and education staff, as appropriate
Page 59
xxx00.#####.ppt 04/19/23 12:56 PMPediatrics
Goal: Asthma Education
•Provide asthma awareness for all students
•Teach asthma management to students with asthma
•Provide asthma education for faculty and staff
•Teach parents how to manage asthma
Page 60
xxx00.#####.ppt 04/19/23 12:56 PMPediatrics
Goal: Supportive Policies
‐ Identify students with asthma
‐ Provide quick, reliable access to medications
‐ Establish individualized student asthma management plan
‐ Establish individualized student emergency plan for asthma episodes
‐ Promote safe and full participation in all school activities
‐ Monitor students’ asthma
Page 61
xxx00.#####.ppt 04/19/23 12:56 PMPediatrics
Supportive Policies
Identify Students
•Review student health records
•Interview parents
•Interview school health staff

Page 62
xxx00.#####.ppt 04/19/23 12:56 PMPediatrics
Supportive Policies
Provide Access to Medication
•Ensure reliable access to medication for all school activities
•Allow self-administration as appropriate
•Provide for nebulizer treatment as needed
Page 63
xxx00.#####.ppt 04/19/23 12:56 PMPediatrics
Supportive Policies
Establish Student Asthma Management Plan
‐ Address triggers
‐ Record personal best peak flow
‐ Specify routine medications
‐ Outline signs and symptoms of worsening asthma
‐ Specify medications required for emergencies and how to monitor response to them.
‐ Indicate emergency contacts
‐ Place plan in student’s health record
• Make copies for off-campus activities
Page 64
xxx00.#####.ppt 04/19/23 12:56 PMPediatrics
Supportive Polices
Establish Plan for Asthma Episodes
• Develop school wide emergency plans/procedures‐ Include respiratory distress treatment protocols
‐ Include plan for someone without an individualized plan
• Include an emergency plan for asthma episodes in the individualized student asthma management plan.
Page 65
xxx00.#####.ppt 04/19/23 12:56 PMPediatrics
Supportive Policies
Promote Participation in All Activities, including Physical Activities
‐ Encourage student participation
‐ Allow pretreatment and or warm-up before physical activity
‐ Allow access to quick relief medication
‐ Modify activity or substitute with less strenuous option

Page 66
xxx00.#####.ppt 04/19/23 12:56 PMPediatrics
Supportive Policies
Monitor Students’ Asthma
•Watch for symptoms of uncontrolled asthma
•Monitor absenteeism due to asthma
•Refer for home teaching as needed
Page 67
xxx00.#####.ppt 04/19/23 12:56 PMPediatrics
Goal: Sound Communication
‐ Form linkages among school, home and health care providers
‐ Observe and report symptoms, medication use
‐ Review difficulties student may have with daily school management plan
‐ Resolve problems with school performance related to asthma
‐ Encourage active student participation in school activities

Page 68
xxx00.#####.ppt 04/19/23 12:56 PMPediatrics
Using InhalersProperly
Page 69
xxx00.#####.ppt 04/19/23 12:56 PMPediatrics
Page 70
xxx00.#####.ppt 04/19/23 12:56 PMPediatrics
Scope of Problem
•28 – 63% of patients do not use their pMDI or DPI well enough to get benefit
‐More than 500 million pMDIs or DPIs are produced each year
‐At an average retail cost of $50/inhaler total retail of $25 Billion
•$7 – 15.7 Billion wasted
•Increased ER visits and hospital admissions
•Increased morbidity and mortality

Page 71
xxx00.#####.ppt 04/19/23 12:56 PMPediatrics
pMDI +Valved Holding Chamber
‐Most studies report equal or better efficacy and less side effects
‐Improved patient adherence to therapy
‐Immediate use with little preparation
‐Can be used in many settings
‐Treatment effect can be titrated
‐Significant cost benefit
Page 72
xxx00.#####.ppt 04/19/23 12:56 PMPediatrics
Valved Holding Chambers vs Nebulizers for B2-Agonist Treatment of Acute Asthma?
•2001 analyzed 1076 children and 444 adults who were included in 22 trials
•MDI’s with holding chambers produced outcomes that were at least equivalent to those of nebulizer delivery
•In children with acute asthma, holding chambers have advantages compared with nebulizers
Osmond M, Diner B. Ann Emerg Med 2004;43:413-415 Cates CJ, Rowe B, Bara A. 2003 Cochrane Review

Page 73
xxx00.#####.ppt 04/19/23 12:56 PMPediatrics
Poor Inhalation Technique Even After Instruction in Children with Asthma
‐66 newly referred children with asthma
•60 / 66 had received instruction from PCP
•58% performed all steps correctly
•97% thought they had proper technique
‐29 control patients followed in asthma clinic
•93% performed all steps correctly
‐Major difference was extent of training
•PCP relied on verbal instruction for 5 mins
•Asthma clinic used demonstration til correct (30 mins)
Kamps AWA, et al. Pediatr Pulmonol 2000;29:39-42.
Page 74
xxx00.#####.ppt 04/19/23 12:56 PMPediatrics
Instruction of Hospitalized Patients by Respiratory Therapists on MDI/VHC use Leads to Decrease in Patient Errors
‐58 patients was observed by a physician while performing 2 actuations of their MDI and the number of errors they committed‐After a program of MDI instruction (which included encouragement to use a VHC) by an RT was performed, group of hospitalized patients was again observed‐This improvement in proper use went from 27.6% to 91.7%‐Instruction of hospitalized patients with obstructive lung disease by an RT improves their correct use of MDI and VHC
Song WS, et al. Respir Care. 2005 Aug;50(8):1040-5.
Page 75
xxx00.#####.ppt 04/19/23 12:56 PMPediatrics
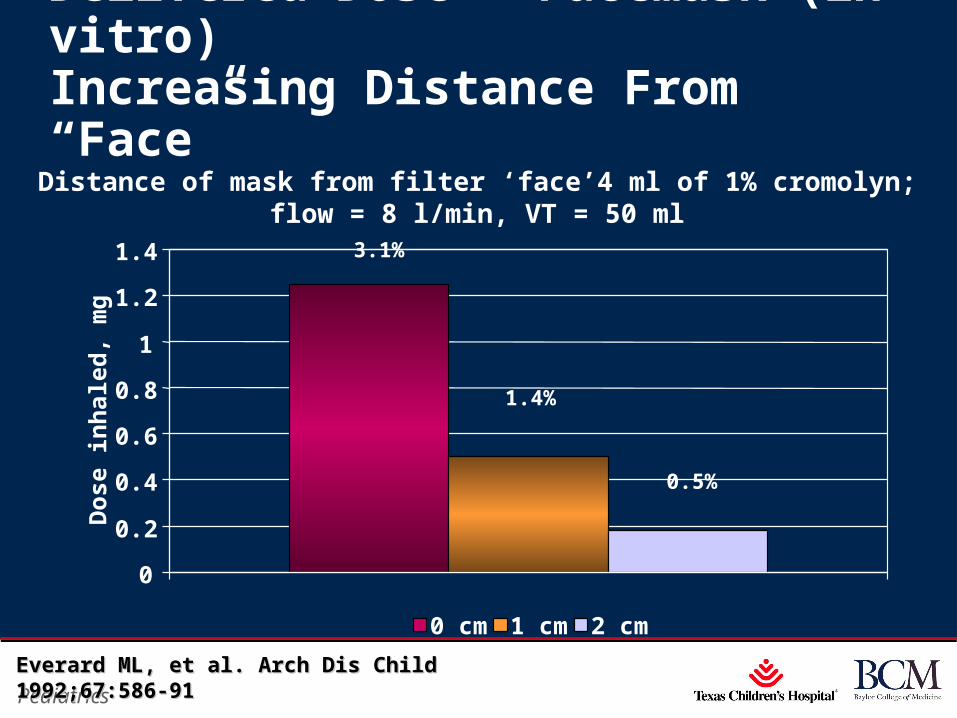
Delivered Dose – Facemask (in vitro)Increasing Distance From “Face”
Distance of mask from filter ‘face’4 ml of 1% cromolyn; flow = 8 l/min, VT = 50 ml
0.5%
1.4%
3.1%
0
0.2
0.4
0.6
0.8
1
1.2
1.4
Dos
e in
hale
d, m
g
0 cm 1 cm 2 cm
Everard ML, et al. Arch Dis Child 1992;67:586-91Everard ML, et al. Arch Dis Child 1992;67:586-91

Page 76
xxx00.#####.ppt 04/19/23 12:56 PMPediatrics
Conclusions
‐Asthma is a leading cause of morbidity in childhood.
‐Asthma control can be achieved with proper evaluation and treatment
‐Proper policies, education and involvement of key personnel in the school system help decreased the impact of asthma.
‐Using inhalers and spacer correctly is a key aspect in the management of asthma