Pediatric Oncology - CAPhO. Mark Diachins… · Pediatric Oncology Or why cancers should fear...
48
Pediatric Oncology Or why cancers should fear little children Mark Diachinsky, BScPharm Clinical Practice Leader, AHS Pharmacy Services University of Alberta / Stollery Children’s Hospital Edmonton, AB 1
Transcript of Pediatric Oncology - CAPhO. Mark Diachins… · Pediatric Oncology Or why cancers should fear...

Pediatric Oncology
Or why cancers should fear little children
Mark Diachinsky, BScPharmClinical Practice Leader, AHS Pharmacy ServicesUniversity of Alberta / Stollery Children’s HospitalEdmonton, AB
1

Disclosure Slide
I have no conflict of interests to declare
2

Learning Objectives
1. Understand common childhood malignancies;
2. Recognize the importance of collaboration and research in the success of childhood cancer;
3. Identify unique challenges associated with the treatment of adolescent and young adults with cancer; and
4. Discuss the late effects of treatment on survivors of childhood cancer.
3

A look at the landscape
4

Some Canadian Statistics
• Each year, on average approximately 880 children under the age of 15 and 412 adolescents (15 – 19 years) are diagnosed with cancer.• 150 children and 74 adolescents will die from the disease.
• Childhood cancer is the second leading cause of death by disease among Canadian children.
Health Canada Statistics, 2012 5

What is the most common childhood cancer
A. Leukemias
B. CNS Tumours
C. Lymphomas
D. Soft tissue cancers (e.g rhabdomyosarcoma)
E. Bone Cancers (e.g osteosarcoma)
6

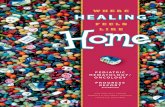
Incidences of cancer types
7

Statistics Canada, 2015 8

Statistics Canada 2015, CCRN 2013 9

What is the approximate overall survival of childhood cancers?A. 50 %
B. 60 %
C. 75 %
D. 80 %
E. 90 %
10

• Over the last 30 years, childhood cancer incidence rate increased by an average approximately 0.4% annually
• Fortunately, survival rates have improved substantially• 71% in the late 1980s to 82% in the early 2000s• 5-year survival rates have increased for several types of childhood cancers.
Statistics Canada, 2015 11

CCRN 2013, Ward 201412

The Importance of Research
• C17 Council Reports that 27% of new patients seen in pediatric cancer centers were enrolled in clinical trials• VS ~5% of adults
• All Canadian sites are members of the Children’s Oncology Group (COG)• Over 200 institutions in Australia, Canada, New Zealand, several European
countries and MOSTLY the US
• In 2013 there were 72 COG trials open in Canada
CPAC 201213

Teamwork makes Dreamwork!
• Who is this guy?
• Have you read this?
• I’m from the binging era, so have you watched this?
• What is co-operative group research?
14

Co-operation Around the World
• Recognition of the value of inter and multidisciplinary care
• Numbers, numbers, numbers!
• Outcomes
• Funding, funding, funding!
15

A glimpse into the world of pediatric oncology
www.childrensoncologygroup.org16

Question #3
A parent comes in with their 5 year old boy to the emergency department. The parent has noted that they have noted unusual bruising on the child’s upper extremities, and the child is much more tired than usual. The parents report the child has had 2 colds in the past 2 months, and currently has a fever. Bloodwork is taken and reported HgB 63 g/L, WBC 55 x109/L, and platelets 25 000 /mm3.
What is the most likely cancer diagnosis?
A. Osteosarcoma
B. Wilms tumor
C. Acute Lymphoblastic Leukemia
D. Rhabdomyosarcoma
17

Childhood Leukemia
• Most common childhood cancers
• Acute Lymphoblastic Leukemia (ALL) and Acute Myeloid Leukemia (AML) are the most common, however many other leukemias and bone marrow disorders affect children• Ex: Acute Promyelocytic Leukemia (APL
or APML), Juvenile MyelomonocyticLeukemia (JMML), Chronic Myelogenous Leukemia (CML), Myelodysplastic Syndromes (MDS)
PDQ AML 2018, PDQ ALL 2018 18

Acute Leukemias
• Presentation: usually pretty non specific.• bruising/bleeding, bone pain, generic flu-like symptoms, night sweats, infections.
• Treatments and intensity of treatment are chosen based on many factors:• Tumor biology
• Immunophenotype (B- vs T- leukemia) and• cytogenetics
• Intensity of response minimal residual disease (MRD)• Initial presentation
• WBC count and patient age• Rapidity of response• Presence of extramedullary disease
• CNS or Testicular Dx
• Diagnosis usually from BM aspirate and/or peripheral blood samples.
PDQ AML 2018, PDQ ALL 2018 19

Treatment of Acute Leukemias
• Acute Lymphoblastic Leukemia• 2-3 years of systemic chemoterapy, and sometimes radiation (CNS-disease).• 4 phases – induction, consolidation, delayed intensification, maintenance.• Rarely may require bone marrow transplant (BMT) for cure (for refractory, relapsed
disease)• Survival rate approximately 90% for children younger than 15 years and 75% for
adolescents aged 15 to 19 years.
• Acute Myeloid Leukemia (20% of childhood leukemias)• Usually about 6 months of intensive chemotherapy• Often requiring BMT for cure.• High risk of complications (neutropenia, infections, side effects)• Survival rate approximately 68% for children less than 15 years and 57% for
adolescents aged 15 to 19 years
PDQ AML 2018, PDQ ALL 2018 20

Central Nervous System (CNS)tumours.• Many different CNS tumors
• Atypical Teratoid/Rhabdoid (ATRT), Embryonal, Germ Cell, Gliomas, etc.
• Very common childhood cancer
• May present very differently depending on location of the tumor• Seizures or neurologic issues• Endocrinologic issues • Neuro-psychologic issues, etc
• Classified based on their histology and location• Classically as infratentorial, supratentorial, parasellar and spinal cord tumors
PDQ CNS 2017 21

Treatment of CNS tumours
• Surgery and Radiation are the mainstay of most brain tumors but some are responsive to chemotherapy• Advent of increased knowledge of tumor genetics is starting to change this.
• Adverse effects of treatment mean complex team care• neurosurgery, neuropathology, radiation oncology, pediatric oncology, neuro-
oncology, neurology, rehabilitation, neuroradiology, endocrinology, and psychology,
PDQ CNS 2017 22

Wilms Tumour
• Wilm’s tumor is most common kidney tumor of childhood. (~90%)• Usually in younger children• Other childhood renal tumors include renal cell carcinomas, rhabdoid tumors, clear
cell sarcomas and others
• Presentation:• Hypertension, lumps, pain or swelling in abdomen, fever, loss of appetite, weight
loss, blood in the urine.
• Risk determines treatment intensity.• Metastasis• Tumor size• Bilateral/unilateral• Tumor biology and histiology• Patient age
PDQ Wilms 2018 23

Treatment of Wilms tumours
• Treatment mainstay is:• Nephrectomy and chemotherapy
• +/- radiation
• Treatment intensity increases with disease risk• Addition of anthracyclines, radiation, additional chemotherapy
• Differing treatment strategies in Europe and NA especially wrt low risk patients.
• 5-year survival rates 88% (above 90% in patients with favorable histology)
PDQ Wilms 2018 24

Retinoblastoma
• 2 forms • Heritable - ~ 25% - RB1 gene• Non-heritable
• Presentation:• Eyes looking in different directions (strabismus, or
“lazy eye”)• Pain or redness• Infection in eye• Eyeball larger than normal• Leukocoria -"cat's eye reflex" most common
• “white pupil” - pupil looks white instead of red when you shine a light (camera flash)
• Treatment – risk based (one or both eyes involved, large or small tumor, metastasis or progression.• enucleation (removal of eye)• Radiation• laser surgery (photocoagulation)• Cryotherapy• Chemotherapy
• Many patients get adjuvant chemotherapy here then sent to HSC in Toronto.
PDQ Retinoblastoma 2018 25

Neuroblastoma
• Most common extracranial solid tumor of childhood.• Originates in the adrenal medulla and paraspinal or periaortic regions
where sympathetic nervous system tissue is present
• Presentation• Proptosis• Abdominal distension• Bone pain• Fever, hypertension, anemia• Paralysis• Blueberry muffins• Rarely opsoclonus myoclonus syndrome (dancing eyes –dancing legs)• https://www.youtube.com/watch?v=UCiAz8YA0iY
• MIBG (iodine-123 meta-iodobenzylguanidine)
PDQ Neuroblastoma 2018 26

Treatment of Neuroblastoma
• Based on prognostic risk
• Age
• Tumor histology, and differentiation
• Stage
• Tumor genetics
• MYCN amplification, 11q aberration, ploidy
• New International Neuroblastoma Risk Group Stratification now used.
• Complicated
• Low risk, • Surgery +/- Chemo +/- rads
• Intermediate risk, • Surgery +/- Chemo +/- rads
• High risk• chemo., surgery, myeloablative chemo with stem cell
rescue then immunotherapy then maintenance with retinoic acid derivatives
• Stage 4S• Observation or chemotherapy
• 5-year survival rate 95% for children younger than 1 year and 68% for children aged 1 to 14 years
PDQ Neuroblastoma 2018 27

Rhabdomyosarcoma
• Soft tissue tumor arising from rhabdomyoblasts – primitive muscle cells that should become striated muscle• Embryonal ~60%
• Mostly young boys 0-4 years• Alveolar ~25%
• Girls and boys 0-19• Other (mixed) ~15%
• Prognosis variable based on many factors:• Age (1> & <9 y/o =better)• Site of origin (orbit better than abdomen)• Tumor size (≤5 cm = better)• Resectability• Subtype embryonal>alveolar• Tumor genetics• Metastasis at diagnosis
• Presentation• Depends on site could have pain in a
limb, painful lump, bulging eyes, urinary retention, headaches, blood in urine, constipation.
• Treatment varies based on prognostic risk• Compressed chemotherapy regimens
with colony stimulating factor rescue.• Radiotherapy and surgery
• General idea is to try for total resection either initially or with adjuvant chemo first.
• Continue chemotherapy and if residual dx or metastasis may add radiotherapy.
PDQ Rhabdomyosarcoma 201828

Ewing’s Sarcoma
• Tumour derived from mesenchymal stem cells• >(osteoblasts, myocytes,
chondrocytes,adipocytes)
• Presentation: depends on location. • May be osseous or extra-
osseous
• Often takes a while before diagnosed – 25% have metastasis on Dx
• Prognosis• Pretreatment
• Good
• Distal location, extra skeletal primary, smaller size, age < 15y, being a girl, lower LDH, no mets,
• Bad
• Opposite of above, previous cancer, cytogenetics
• Response to therapy• Having total resection =good
• Treatment• Chemotherapy, radiation and surgery.
PDQ Ewing Sarcoma 2018 29

Osteosarcoma (the disease of the 715 million dollar man)• Usually starts in osteoblasts.
• Most common in teenagers and usually forms in ends of long bones – often near knee. Can be extra osseous.
• Presentation:• Knee pain, mistaken for sports
injuries, pathologic fractures, etc.
• Prognostic factors:• Haven’t been helpful in
choosing treatments• Good
• distal primary, smaller tumors, localized dx (one lung involvement and few lung mets better), adequate resection, necrosis after neo-adjuvant chemo
• Bad – opposite
• Treatment:• Chemotherapy and surgery.
PDQ Osteosarcoma 2018 30

Question #4
The 5 year old boy receives a bone marrow aspirate that confirms acute lymphoblastic leukemia. Treatment with 4 drug induction has been ordered to start that night. What is the most urgent oncologic emergency to monitor for in this pediatric patient?
A. Febrile Neutropenia
B. Tumour Lysis Syndrome
C. Disseminated intravascular coagulation
D. Bowel perforation
E. Spinal cord compression
31

Pediatric Oncological Emergencies
• Mechanical• Airway obstruction, superior vena cava syndrome (SVCS), spinal cord compression,
cerebral herniation, intussusception, bowel perforation, altered stool patterns, GI infection (typhlitis or necrotizing neutropenic enterocolitis)
• Hematological• Anemia, thrombocytopenia, thrombosis, disseminated intravascular coagulation
(DIC), hyperleukocytosis.
• Metabolic• Tumour Lysis Syndrome (TLS), SIADH
• Infectious• Infection, febrile neutropenia
• Neurologic• Seizures, cerebrovascular accidents (uncommon)
32

Risk Stratification
Adverse effects / late effects
survival
33

Question #5
• A 15 year old female is currently receiving her fourth cycle of chemotherapy for Hodgkin lymphoma. Her family asks what the most likely long-term side effects that may occur after her treatment. Her treatment consists of prednisone, doxorubicin, bleomycin, vincristine and cyclophosphamide. What are possible long-term effects?
A. Reproductive issues
B. Secondary cancer
C. Cardiovascular disease
D. Decreased pulmonary function
E. C and D
F. All of the above
35

Late effects of Treating Childhood cancer.
• 60% to more than 90% develop one or more chronic health conditions.
• 20% to 80% experience severe or life-threatening complications during adulthood.
• Late effects in childhood cancer survivors may include:• Growth and development.
• Thinking, learning and memory
• Organ, tissue and body function
• Reproductive capacity
• Secondary neoplasms
• Psychosocial sequelae related to the primary cancer, its treatment, or maladjustment associated with the cancer experience• Anxiety, depression, PTSD, socialization problems PDQ Late Effects of Treatment for Childhood Cancer 2018
36

Childhood Cancer Survivor Study
• About 24000 survivors and ~ 4000 siblings cohort identified over a 30 year period being followed longitudinally.
• Findings from the ongoing study include:• 4x greater risk of breast cancer with chest radiotherapy
• 2.4x greater risk of thyroid cancer with alkylating agents
• Increase risk of cardiac risk factors in survivors
• Survivors offspring are not at an increased risk of birth defects.
(https://www.cancer.gov/types/childhood-cancers/ccss) 37

Fertility & Offspring effects
• Infertility remains one of the most common life-altering treatment effects experienced by long-term childhood survivors. • Decreased gonadal function• Acute ovarian failure• Premature menopause
• Survivors have significantly decreased likelihood of siring or having a pregnancy• 38% of survivors vs 62% of siblings
• Survivors less likely to have live births, more likely to have medical abortions, and more likely to have low-birth-weight babies than were siblings.• 63% live births, 1% stillbirths, 15% miscarriages, and 17% abortions
• Children of cancer survivors NOT at significantly increased risk for congenital anomalies
PDQ Late Effects of Treatment for Childhood Cancer 201838

Fertility Preservation
• Progress in reproductive endocrinology has resulted in the availability of several options for preserving or permitting fertility in patients about to receive potentially toxic chemotherapy or radiation therapy.• Males: cryopreservation of spermatozoa before treatment is an effective
method to circumvent the sterilizing effect of therapy.
• Females: harvesting and banking the postpubertal patient’s oocytes and cryopreserving unfertilized oocytes or embryos before gonadotoxic therapy.
39

Factors that affect the risk of late effects
• Tumor-related factors• Cancer type and location.
• Treatment-related factors• Treatment modalities, chemotherapy agents used, cumulative amounts,
transfusions.
• Patient-related factors• Gender, development at time of treatment, other comorbidities, family history,
genetics, hormonal changes, health habits
• In general, the risk of having late effects increases over time as survivors are living longer due to successful treatments• Most common causes of death are relapse, secondary neoplasm or heart and lung
damage
41PDQ Late Effects of Treatment for Childhood Cancer 2018

Follow-up!
• Long term follow-up clinics• Multidisciplinary approach
• Regular follow-up by practitioners that are familiar with the late effects of cancer treatment
• Long term follow-up guidelines• http://www.survivorshipguidelines.org/
42

Survivorship guidelineshttp://www.survivorshipguidelines.org/
43

Drug use in Children with Cancer
• Drugs used for treatment• Regimens have very robust data to support
• Regimens extensively tested usually via cooperative group trials
• Drugs used in supportive care• Many medications have limited good quality literature to support use
• Most are “off-label’ with Health Canada
44

Other factors to consider in children
• Drug formulations
• Compliance/Adherence issues
• Self-reporting of symptoms
• Family/Caregiver involvement
• Decision-making
45

Examples of current research questions.
46

47

48

References• Canadian Cancer Research Alliance. Investment in Research on Childhood and Adolescent Cancers,. Toronto; 2013.
• Ward E, DeSantis C, Robbins A, Kohler B, Jemal A. Childhood and adolescent cancer statistics, 2014. CA Cancer J Clin [Internet]. 2014 [cited 2014 Oct 24];64(2):83–103. Available from: http://www.ncbi.nlm.nih.gov/pubmed/24488779
• Canadian Cancer Society’s Steering Committee on Cancer Statistics. Canadian Cancer Statistics, 2012. Toronto; 2012.
• Canadian Partnership Against Cancer. The 2012 Cancer System Performance Report. Toronto; 2012.
• PDQ Pediatric Treatment Editorial Board. Childhood Acute Myeloid Leukemia/Other Myeloid Malignancies Treatment (PDQ®): Health Professional Version. 2018 July 6. [Internet]. 2002 [cited 2018 Aug 21]. Available from: https://www.cancer.gov/types/leukemia/patient/child-aml-treatment-pdq
• PDQ Pediatric Treatment Editorial Board. Childhood Acute Lymphoblastic Leukemia Treatment (PDQ®): Health Professional Version. 2018 Aug 17. [Internet]. 2002 [cited 2018 Aug 21]. Avaiable from: https://www.cancer.gov/types/leukemia/hp/child-all-treatment-pdq
• PDQ Pediatric Treatment Editorial Board. Wilms Tumor and Other Childhood Kidney Tumors Treatment (PDQ®): Health Professional Version. 2018 Apr 2 [Internet]. PDQ Cancer Information Summaries [Internet]. 2002 [cited 2018 Aug 21]. Available from: https://www.cancer.gov/types/kidney/hp/wilms-treatment-pdq /
• PDQ Pediatric Treatment Editorial Board. Retinoblastoma Treatment (PDQ®): Health Professional Version. 2018 Aug 22. [Internet]. PDQ Cancer Information Summaries [Internet]. 2002 [cited 2018 Aug 22]. Available from: https://www.cancer.gov/types/retinoblastoma/hp/retinoblastoma-treatment-pdq
• PDQ Pediatric Treatment Editorial Board. Neuroblastoma Treatment (PDQ®): Health Professional Version. 2018 Aug 17. [Internet]. PDQ Cancer Information Summaries [Internet]. 2002 [cited 2018 Aug 22]. Available from: https://www.cancer.gov/types/retinoblastoma/hp/retinoblastoma-treatment-pdq
• PDQ Pediatric Treatment Editorial Board. Childhood Rhabdomyosarcoma Treatment (PDQ®): Health Professional Version. 2018 Apr 4. [Internet]. PDQ Cancer Information Summaries [Internet]. 2002 [cited 2018 Aug 22]. Available from: https://www.cancer.gov/types/soft-tissue-sarcoma/hp/rhabdomyosarcoma-treatment-pdq
• Board. PPTE. Osteosarcoma and Malignant Fibrous Histiocytoma of Bone Treatment (PDQ®): Health Professional Version. 2018 June 11 [Internet]. PDQ Cancer Information Summaries [Internet]. 2002 [cited 2018 Aug 27]. Available from: https://www.cancer.gov/types/bone/hp/osteosarcoma-treatment-pdq
• Board. PPTE. Ewing Sarcoma Treatment (PDQ®): Health Professional Version. 2018 Aug 17. [Internet]. PDQ Cancer Information Summaries [Internet]. 2002 [cited 2018 Aug 27]. Available from: https://www.cancer.gov/types/bone/hp/ewing-treatment-pdq
• Prusakowski MK, Connone D. Pediatric Oncologic Emergencies. Hematol Oncol Clin N Am 31 (2017) 959–980.
49

Acknowledgements
• I would like to thank Marcel Romanick, BScPharm, for contributing content to the material presented today.
50