Emergencies in Pediatric Oncology
65
Emergencies in Pediatric Oncology Katarzyna Muszynska-Roslan Department of Pediatric Oncology and Hematology Medical University of Bialystok
Transcript of Emergencies in Pediatric Oncology

Emergencies in Pediatric Oncology
Katarzyna Muszynska-Roslan
Department of Pediatric Oncology and Hematology Medical University of Bialystok

Pediatric oncologic Emergencies
??

Pediatric oncologic Emergencies
4 major types
Metabolic emergencies (hypercalcemia,
hyponatremia, hypoglycemia, adrenal failure, lactic acidosis)
Hematologic emergencies (hyperleukocytosis, DIC, thrombosis, bleeding)
Infectious / Inflammatory emergencies(enetrocolitis, pancreatitis, hemorrhagic cystitis , sepsis)
Mechanical emergencies (cerebral herniation/status epilepticus, cardiac tamponade, SVC syndrome, spinal cord compression )

Objectives
Tumor lysis syndrome
Hyperleukocytosis
Mediastinal masses/superior vena cava syndrome
Spinal cord compression
CNS events
SIADH
VOD
Infections

Tumor Lysis Syndrome - who gets it?

Tumor Lysis Syndrome - who gets it?
Patients with rapidly growing tumors and/or bulky disease
Most common with Burkitt’s lymphoma,
T-cell leukemia/lymphoma, B-cell leukemia

Tumor Lysis Syndrome
Can occur at diagnosis, but more common early after start of chemotherapy

Pathogenesis of TLS
???

Pathogenesis of TLS
Rapid death of tumor cells > cells breakdown releaseof large amounts of metabolities (potasssium, phosphate, nucleic acids, urate and other purinemetabolities) into extracellular space
impaired excretion by the kidneys (uric acid is
relatively insoluble, especially at low pH and mayprecipitate in concentrated urine)
urate accumulation
acute renal failure + electrolyte imbalance


Biochemical and clinical consequences of tumor lysis
syndrome
??

Biochemical and clinical consequences of tumor lysis
syndromeHyperkalemia weakness, arrhythmia
Hyperphosphatemia hypocalcemia
Hyperuricemia “uric acid nephropathy”
Hypocalcemia tetany, mental status changes, seizures
Renal failure

“The best treatment is prevention”
It is directed at maximizing the excretion of releasedintracelluar contents and minimizing the production of uricacid
Fluid intake = 2-3 L/m2/day
enhances uric acid excretion, phosphate excretion
Exact fluid balance (fluid intake = urine output)
limitation of potassium and phosphate intake

“The best treatment is prevention”
Urine alkalinization – iv. administration of sodium bicarbonate
Uric acid more soluble at urine pH = 7.0 vs 5.0
Goal of urine specific gravity 1.015 and pH
7.0 - 7.5
Caution! - hypoxanthine and Ca-PO4 stones possible if urine pH > 7.5

Allopurinol –
Decrease production of uric acid
competitive inhibitor of xanthine oxidase which decreases conversion of purine metabolites to uric acid

Recombinant Urate oxidase
Decrease production of uric acid, promotes catabolism of uric acid
Catalyzes conversion of uric acid to allantoin
Allantoin more soluble, easily excreted by kidneys
Urine alkalinization unnecessary if used

Observations
Blood tests every 6 - 8 h: Blood gases Complete blood count Sodium, potassium, calcium, magnesium, phosphorus Urea, creatinine, uric acid
Vital signs (pulse, blood pressure, respiratory rate, temperature), Twice daily weight, diuresis, evidence of oedema, signs of electrolyte
abnormality, ECG
Dialysis


Clinical Indications for Dialysis
oliguria, anuria,
volume overload
weakness,
severe cardiac rhythm abnormalities,
seizures,

Biochemical Indications for Hemodialysis

Pathogenesis of ARF in pediatric oncology
???

Pathogenesis of ARF in pediatric oncology

Hyperleukocytosis
5-20% of children with new Dx of leukemia have WBC count >100,000/mm3
These patients are at risk of severe complications
from hyperviscosity of blood

Hyperleukocytosis
Blasts interact with endothelium to form aggregates, thrombi in microcirculation
Most problems in CNS, pulmonary and renal circulation
More common with AML than ALL
Myeloblasts and monoblasts larger, less deformible, “stickier”

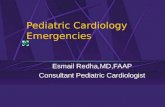
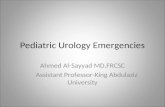
Pulmonary leukostasis
Pulmonary arteriole with leukostatic thrombus in patient with AML and hyperleukocytosis

Pulmonary leukostasis
Sx: dyspnea, tachypnea, hypoxemia, acidosis,
CXR: diffuse interstitial infiltrates
Problems with gas exchange
Acute respiratory failure

CNS leukostasis
Headache, mental status changes, seizures, coma in spectrum of Sx
blurred vision, confusion, delirium, papilledema
High risk of intracranial hemorrhage and/or thrombosis, especially with AML and thrombocytopenia

Genitourinary leukostasis
Clinical features:
oliguria, anuria,
priapism

Hyperleukocytosis
Diagnosis:
WBC
CNS CT: hemorrhage, leukemic plaques
Chest radiograph/ CT: pneumonitis, leukemic emboli

Therapy for symptomatic hyperleukocytosis
To decrease blood viscosity (directly related to morbidity)
Induction chemotherapy
Carefull hydration
AVOID use of diuretics
AVOID RBC transfusion
(Hb goal < 10 gm/dL for viscosity)

Urine alkalinization, adequate hydratation as with tumor lysis syndrome
Consider leukapheresis
PICU - supportive care - mechanical ventilation, hemodynamic support, etc

Apheresis: a process in which blood of
a patient is passed through a medical device, which separates one or more components of blood

Mediastinal masses

Most common types of mediastinal tumors in children
Anterior
Non-Hodgkin’s lymphoma
Hodgkin’s disease
Teratoma
Middle
Lymphoma
Posterior
Neuroblastoma

Pathophysiology of SVCS or SMS
Displacement or obstruction of:
Tracheobronchial tree
Heart and great vessels
SVCS
Superior mediastinal syndrome


SVC syndrome - plethora, oedema of face & upper extremities; dilatation of veins in area

Presentation and symptoms
Often a subacute hx of cough, low-grade fever, dyspnea, ± orthopnea, ± weight loss
Signs/symptoms of airway obstruction and/or SVC syndrome demand emergency evaluation
Airway obstruction - stridor, dyspnea, anxiety, “position of comfort”

Diagnosis:
Chest radiograph – anterior mediastinal mass
Chest CT – mediastinal mass and compression of trachea and bronchi,
Tissue diagnosis e.g. lymph node biopsy, bone marrow aspiration, pleurocentesis, thoracocentesis
Hist-pat examination

Diagnosis:
Blood tests:
blood gas analysis,
complete blood count with differential
sodium, potassium, calcium, magnesium,
urea, creatinine,phosphorus, uric acid,
lactate dehydrogenase (LDH)

Evaluation – problems…
Inability to tolerate supine position !!!
May result from weight of tumor compressing not only airway, but great vessels and heart (especially RV outflow tract)
If can tolerate anesthesia should be performed biopsy

Evaluation of the child with mediastinal mass
Management/diagnostic decisions difficult and controversial –
emergency treatment vs definitive Dx
Significant stridor, dyspnea usually not present unless airway cross-sectional area narrowed by >50%

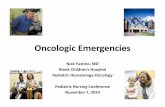
CT Scan of Mediastinal Mass Showing Tracheal Compression at Carina
Carina
Mass

Emergent Management
Keep child in sitting, left lateral decubitus position - -helps “lift” mass off airway and RVOT
IV access (lower extremities preferable due to SVC obstruction)
Face mask O2, non-invasive PEEP
Heli-ox possibly helpful due to large airway obstruction decreases airway resistance

Therapy
Urgent radiotherapy since most lymphomas are radiosensitive. (-)
Chemotherapy, including steroids or cyclophosphamide, is a possible alternative to irradiation, especially in children.

Spinal cord compression
Occurs in 3-5% of children with cancer, often at diagnosis.
Can occur with any tumor type, but mostly with neuroblastoma, sarcoma, leukemia, lymphoma, medulloblastoma.

Presentation
Back Pain !:
suspect cord compression when . . . pain not relieved in supine position or back pain has a radicular component!!!
Weakness, sensory abnormalities, and paresis
Paraplegia and quadriplegia can occur rapidly !!@
Urinary and fecal incontinence.

Diagnosis
MRI is the imaging procedure of choice

Treatment
Sx of cord dysfunction:
give dexamethasone bolus of 1-2 mg/kg and obtain MRI
Decompression: surgery, radiation, chemotherapy.
Surgery indicated if tumor type is not known or symptoms progress despite management
Chemotherapy is appropriate for patients with spinal cord compression due to lymphoma, leukemia, and neuroblastoma.

Emergencies related to brain tumors
Hemorrhage:
ICP, Altered consciousness.
Peri-tumor brain edema:
Rx: dexamethasone ± furosemide
Hydrocephalus:
occurs mostly with posterior fossa and midline supratentorial tumors
Rx: urgent CSF shunting

Sepsis in Pediatric Cancer Patients
diagnostic criteria:
Fever/hypothermia
Tachycardia
Tachypnea
Hypoperfusion
Acidosis
Hypotension
Common etiologies:
Gram (+) cocci
-hemolytic Strep
Staph. Epi
Staph aureus
Gram (-) rodsPseudomonas
Enterobacter
E. coli
Fungi
Viruses

Therapy for Sepsis in Pediatric CancerPatients
Empiric broad-spectrum Abx
Early consideration of antifungals
Usual PICU supportive care is nedeed:
Mechanical vent.
Fluids/inotropes
Parenteral nutrition/blood products, etc
Consider aggravated cardiac dysfunction if hx of high-dose anthracyclines, radiation
Beware risk of adrenal suppression in pts with steroid Rx hx
Granulocyte transfusion reportedly helpful in fungal/bacterial sepsis
Ig substitution

Pulmonary infections in childhood cancers - etiology
Bacteria:
-hemolytic Strept.
Staph. Aureus
Pseudomonas
Klebsiella
E coli
others
Pneumocystis carinii
Mycoplasma pneumonia
Fungi: Aspergillus and Candida
Viruses: CMV, herpes simplex, varicella-zoster virus, adenovirus

Risk factors for acute lung injury
Multiple blood products transfusion
Radiation
Sepsis
Amphotericin B
SIRS (systemic inflammatory response syndrom) from other causes(treatment agents, pancreatitis, etc)

Hepatic sinusoidal obstruction syndrome/veno-occlusive disease (SOS/VOD) is a life-threatening complication of HCT - identified as transplant-related, systemic endothelial diseases.
Veno-occlusive disease


Syndrome of Inappropriate Antidiuretic Hormone (SIADH) and Abnormal Sodium Metabolism
Serum sodium level below 120mmol/l
Etiology in pediatric oncology:
The use of vincristine or cyclophosphamide
after CNS irradiation

Pathophysiology of SIADH:
???

Pathophysiology:
Continuous release of ADH without any relation to plasma osmolality
→ the kidneys conserve water and concentrate the urine
→ hyponatremia and water intoxication

Symptoms:
Fatigue
Weight gain
Lethargy, confusion, seizures, coma
Diagnosis:
Urine /plasma osmolality
Serum sodium level

Treatment
Fluid restriction !!!
In case of seizures or coma:
Hydratation with hypertonic saline
200ml/m2 1.5%NaCl - 6 -8h,
than more slowly to normal level- 24 -72h
Diuresis – furosemide 1mg/kg
Risk of demielinisation and brain injury!!

Hematological emergencies
anemia
trombocytopenia
granulocytopenia
with their consequences
RBC, platelets, granulocytes transfusion as substitution therapy

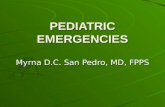
Timeline of non-infectious complications in organ and hematopoietic stem cell transplantation transplantation.
Lama Elbahlawan et al. Respir Care 2017;62:765-775
(c) 2012 by Daedalus Enterprises, Inc.

Conclusions
Pediatric oncology patients experience a broad variety of critical illnesses related to both disease and therapy
Monitoring, prevention and tretament (using ICU care)can benefit children with malignancies

Thanks for your attention