Patient-centered drug delivery system: Use of big data for ...€¦ · Patient-centered drug...
46
Patient-centered drug delivery system: Use of big data for clinical unmet needs Beom-Jin Lee, Ph.D. Professor and Dean of College of Pharmacy Ajou University Suwon, Korea
Transcript of Patient-centered drug delivery system: Use of big data for ...€¦ · Patient-centered drug...

Patient-centered drug delivery system:
Use of big data for clinical unmet
needs
Beom-Jin Lee, Ph.D.
Professor and Dean of College of Pharmacy
Ajou University
Suwon, Korea

Platform technology A few successful case: OROS, OCAS, SODAS, Geomatrix.. Sensitive to system design, drug type, formulation and excipients,
races and patient pathophysiology Therapeutically acceptable to satisfy clinical unmet needs from
patients
Evolution of Drug Delivery Technology
Patient-centered (therapeutic-based) DDS according to patient medical unmet needs: pathophysiology, clinical benefits and treatments
Material basis and formulation

The number of older adults
(aged over 65years)
• In Europe, 87 million in
2010 -> 123 million in
2030
• In the UK, older adults aged
80+ will represent 9% of the
population in 2050 compared
with 4.8% in 2012
Americans have been living
longer, meaning that the
demarcation of 65 as "old" is
more distant from the
average life expectancy.
www.ajou.ac.kr
Population of geriatric patient
Figure. Age composition of american

Physiological changes on aging(ADME in the geriatrics)
Absorption Distribution Metabolism Elimination
Amount of saliva ↓ Cardiac output ↓ Liver function (through
decrease in blood flow) ↓
Kidney size ↓
Gastric acid production ↓ Renal blood flow ↓ Cyp P450 enzyme levels ↓ Renal blood flow ↓
Gastro-intestinal surface ↓ Hepatic blood flow ↓ Overall drug metabolism ↓ Number of functional
nephrons ↓
Active transport
mechanism ↓
Albumin water levels ↓ Tubular secretion ↓
Gastric pH ↑ Volume of distribution for
water soluble drugs ↓
Overall glomerular filtration
rate (GFR) ↓
Gastric emptying time ↑ Body fat/water ratio ↑
Learning from practice to meet patient centricity
2015-10-27
• The Guidance for Industry Q8(R2) Pharmaceutical Development”
request: “In all cases, the product should be designed to meet
patients’ needs and the intended product performance”
• Lack of suitable formulations, pharmaceutical packs and
administration devices to meet their needs.
A. Swallowing considerations
B. Dosage form and pharmaceutical product design Dosage form design: The size, shape, color, surface structure, taste
and smell of the product should be considered to improve the ease of
swallowing
Packaging and labelling: Tamper-resistant product
C. Medication schedule and management factors Dosing frequency: Controlled release system
Dealing with polypharmacy: Fixed-dose combination
Medicines requirement for pediatrics & geriatrics

Patient-centric drug delivery
The development of drug products that address unmet needs within
specific target populations.
Patient-centric formulations and dosage forms can positively impact
the quality life of patients Improving or maintaining therapeutic efficacy
Diminishing the negative aspects of taking medication
Patient populations
Geriatric Pediatric Dysphasic Those affected by debilitating
mental or physical illnesses Life-threatening diseases (CV,
cancer, DM)
Primary objectives
Ease of administration Improved compliance to the dosing
regimen Improved palatability Optimized dosage form needs Reduction in the number of daily doses Satisfaction of clinical unmet needs

Specialized Patient Needs
[Expected levels of concern for patients]
Optimal patient
dosing needs
Geriatric Pediatric Dysphasic Mentally III
Ease of swallowing ++++ ++++
++++
++++
Reduced pill
burden
++++
++
++
++
Convenient dosage
form
++ ++++
+ +
Pleasant taste ++
++++
+ +
Identification, mix-
up prevention
++++
++
+ ++
Moynihan, H., Crean, A. (2009) Physicochemical Basis of Pharmaceuticals. Chapter 1, Oxford University Press.
Higher ++++>+++>++>+ Lower
2015-10-27

Big Data in Pharma Industry
Definition: Big data is a set of techniques and technologies that require new forms of integration to uncover large hidden values from large datasets that are diverse, complex, and of a massive scale. Big Data is used in the singular and refers to a collection of data sets so large and complex, it’s impossible to process them with the usual databases and tools. Because of its size and associated numbers in complexity, Big Data is hard to capture, store, search, share, analyze and visualize. The phenomenon came about in recent years due to the sheer amount of machine data being generated today – thanks to mobile devices, tracking systems, RFID (definition to follow), sensor networks, social networks, Internet searches, automated record keeping, video archives, e-commerce, etc.
Big Data : Raising the Table Stakes for Master Data Management, IMS Health
“We swim in a sea of data … and the sea level is rising rapidly.” Pew Research Center’s Internet & American Life Project - July 2012

Big Data Advantages in Pharma R&D
• Better disease understanding • Better design of products, trials &
treatments • Real-world patient data • Customized drug development • Identification of undiagnosed patients • Detection of serious adverse events • Prediction of hospital re-admissions • Improved HO & medical forecasting
• Comparative effectiveness • Track of patient pathway & drug
switches • Prediction of disease trends & locations • Patient sentiments & feedbacks • Improved communications • Healthy pipeline & better products • Reduced cost, enhanced quality &
efficiency
Detecting adverse/side effects and finding clinical unmet needs for patient centricity
• Cases using big data in Korea : Accessibility of EMR in general hospital (Ajou University Hospital); Drug safety monitoring (adverse effects) and decision making in drug discovery & development
• History - Use of big data for evidence-based drug safety monitoring and decision making: Detecting adverse effects of medicines (thalidomide, cisapride, rofecoxib)

10
Next-Gen Pharma R&D with Big data
Pharmaceutical and life sciences companies that focus on research, clinical trials,
and managing the business historically use data warehouses and business
intelligence tools to report on and analyze this data.
- Big Data solutions help improve the efficiency of the drug discovery and
development process and to provide support for transnational approaches to
research(discovery, non-clinical safety, PK/PD, clinical data)
Accelerated Clinical Trials and
Drug Discovery
Monitoring and Improving
Patient Adherence
Improving Operational
Efficiency
By combining shared research data from
the marketplace with clinical data,
genetic / genomic profiles, patient
adherence, and population data,
research outcomes can be recognized
faster, clinical trials can become
streamlined, and new medicines can be
discovered faster and at lower cost. Once
consumers have access to the drugs,
social media can be monitored to better
understand drug effectiveness and
possible side effects.
When drugs are prescribed by
physicians, there is often a question
of how often the prescriptions are
filled and whether they are taken in
the way that the drug was designed
for and as the physician intended.
As sensors become more prevalent in
drugs and monitoring devices, the
industry is becoming better
equipped to monitor patient
adherence.
Predictive analytics has typically been
applied to data residing in a data
warehouse. Applying analytics to a Big
Data solution enables us to analyze a
wider variety of data sources thus
improving the accuracy of our
predictions.
Predicting the success of a drug trial
early is critical to determining if a
drug’s development should be
continued and can greatly reduce
wasted time and cost.

Linkage of big data and patient centricity
BA improvement, durability
Better response, tolerance
Taste, route & frequency
of administration
Pricing, Cost,
patent, Treatment
GI irritation,
toxicity (heart, kidney)
Bleeding, Sugar level
Technology (CR, Sol, BBB)
Dosage forms
(Nano, beads, matrix)
Big Data
(Collection &
Analysis)

Korea United Pharm. Brief History
1987 Establishment 1992 Acquired KGMP approval for the plant
2000 Established API Plant 2001 10 Mil. Dollar Export Award
2004 Completed Korea United Pharm Int’l, JSC. in Vietnam 2004 Completed United Douglas Pharm. Inc. in Alabama
2009 / 2010 Forbes Asia’s 200 Best Under a billion for 2 years
2011 Established New Plant (cGMP) 2012 Designated Korea Innovative Pharmaceutical Company
2013
Out-licensing of IMDs to other companies 2014 Selected on the list of World Class 300 project

Globally Registered Countries & Products
Number of Exported products : 416 Number of registered countries : 32
Hongkong Indonesia Malaysia Mongolia Pakistan
Singapore Thailand
Uzbekistan India
Costa Rica El Salvador
Ecuador Guatemala Nicaragua
Peru Chile Cuba
Colombia Uruguay
Venezuela Honduras
Dominica
Panama
Nigeria Kenya Egypt Ghana Yemen Syria Iran
Belarus Georgi
144
132
49
60
31

Product Partner Business Region
License Out Russia Kazakhstan Ukraine
Uzbekistan Belarus Venezuela
License Out China
Co-marketing S. Korea
Co-marketing S. Korea
IMDs Partnering

Case I: Aceclofenac
: Physicochemical & biopharmaceutical properties
Molecular formula C16H13Cl2NO4
Molecular weight 354.19
Dose 100 mg
Protein binding >99%
Peak time after oral
administration 1 ~ 3 h
Elimination half life Approximately 4 h
Solubility Insoluble in water, soluble in alcohol
Major route of eliminat
ion About two-thirds of a dose is excreted in the
urine mainly as hydroxymetabolites
Adverse effect Gastro-intestinal disturbances,
nausea, diarrhoea
Aceclofenac : 89796-99-66
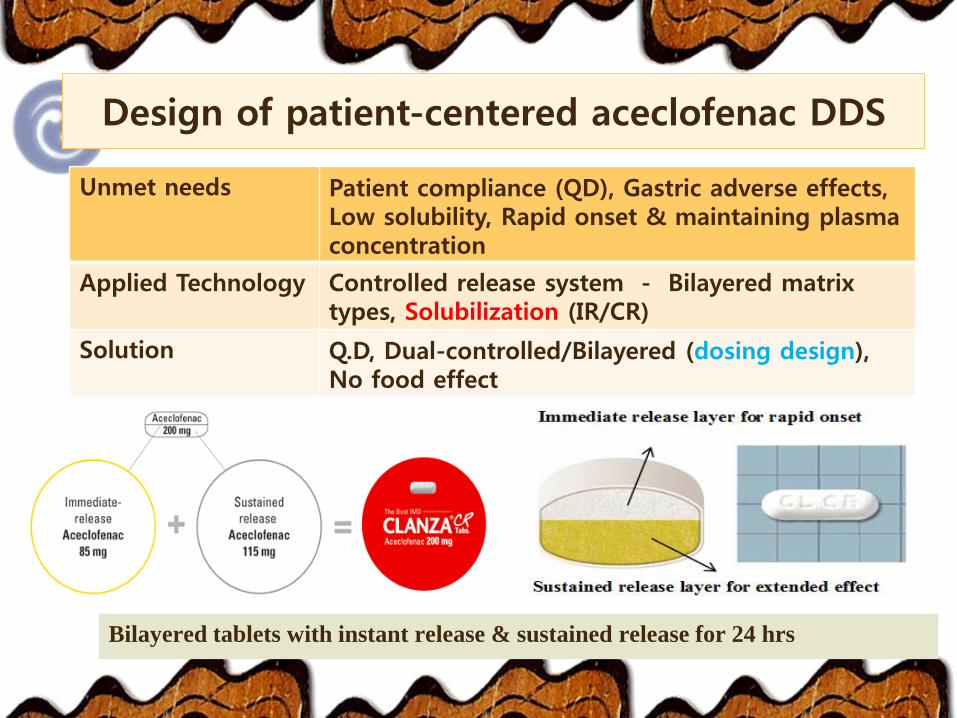
Unmet needs Patient compliance (QD), Gastric adverse effects, Low solubility, Rapid onset & maintaining plasma concentration
Applied Technology Controlled release system - Bilayered matrix types, Solubilization (IR/CR)
Solution Q.D, Dual-controlled/Bilayered (dosing design), No food effect
Design of patient-centered aceclofenac DDS
Bilayered tablets with instant release & sustained release for 24 hrs

Generations in Solubility Enhancement
Beom-Jin Lee et al., EJPB (2013)
Aceclofenac
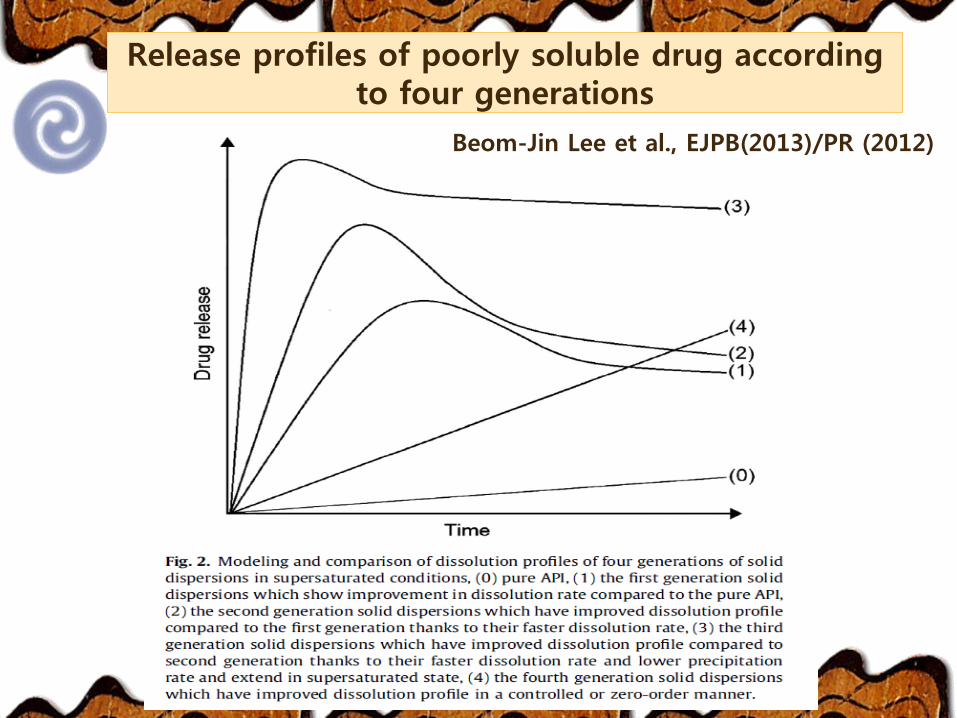
Release profiles of poorly soluble drug according to four generations
Beom-Jin Lee et al., EJPB(2013)/PR (2012)

Modulation of micro-environmental pH and controlled release system

Formulations & dissolution profiles
Time (min)
0 15 30 45 60
Dis
solu
tion r
ate
(%
)
0
20
40
60
80
100F25
F26
F27
F28
F29
Time (min)
0 15 30 45 60
Dis
solu
tion r
ate
(%
)
0
20
40
60
80
100F30
F31
F32
F33
F34
Time (min)
0 15 30 45 60
Dis
so
lutio
n r
ate
(%
)
0
20
40
60
80
100
F35
F36
F37
F38
F39
F40
Time (min)
0 15 30 45 60
Dis
solu
tion r
ate
(%
)
0
20
40
60
80
100
F41
F42
F43
F44
F45
Time (hr)
0 5 10 15 20 25
Diss
olut
ion
rate
(%)
0
20
40
60
80
100
120
F8
F9
F10
F11
F12
Time (hr)
0 5 10 15 20 25
Diss
olut
ion
rate
(%)
0
20
40
60
80
100
120
F13
F14
F15
F16
Time (hr)
0 5 10 15 20 25
Diss
olutio
n ra
te (%
)
0
20
40
60
80
100
120
F27
F28
F29
F30
SR layer IT layer

Time (h)
0 5 10 15 20 25
Dis
solu
tio
n A
mo
un
t (m
g)
0
50
100
150
200
Airtal
Clanza CR
Time (hr) 1 12 24
Airtal® 92.3
Clanza® CR 86.3 137.4 195
Amount of drug dissolved (mg)
Dissolution Profile of optimized formulation

Alkalizer (Na2CO3)
Hydrogen ion
(pHm) controlled system
(Electronic microscopy image, x
5000000) (pHm) images in dissolution media
pH 1.2
pH 6.8
Release-modulating mechanism: Microenvironmental pH (pHm) and swelling system

Preclinical Test in Beagle Dogs
0
20
40
60
80
100
0 4 8 12 16 20 24 28 32
Pla
sma
level
( ㎍
/mL
)
Time (h)
mean (n = 6)
AIRTAL® TAB 100 mg
CLANZA CR TAB 200 mg
0.1
100.0
0 4 8 12 16 20 24 28 32Pla
sma
level
( ㎍
/mL
)
Time (h)
mean (n = 6) AIRTAL TAB 100 mg
CLANZA CR TAB 200 mg
Reference Test
Cmax 54.47 ± 6.86 60.65 ± 25.34
Tmax 1.64 ± 1.34 3.750 ± 4.168
t1/2 4.44 ± 0.79 4.191 ± 0.720
AUC(0-t) 258.99 ± 60.18 428.7 ± 163.6
AUC(0-inf) 263.93 ± 60.75 433.9 ± 164.2
AUC(0-t)/AUC(0-inf),% 98.1 98.5
F* (%) - 82.2
Confirming the SR pattern
* F : Relative Bioavailability to Airtal® 200mg; Bioavailabity (%) = (AUC∞ , Test / AUC∞ Ref x 2 ) x 100

Single Dose and Food Effect Study Multiple Dose Study
Study Design 3 treatment, 3 period 2x2 cross-over
Study Purpose
To Assess the Pharmacokinetics and Food Effect
of Aceclofenac Controlled Release Tablets
Following Sing-Dose Administration Compared
with the Immediate Release Tablets in Healthy
Male Subjects
To Assess the Pharmacokinetics of
Aceclofenac Controlled Release Tablets
Following Multiple-Dose
Administration Compared with the
Immediate Release Tablets in Healthy
Male Subjects
Subjects 42 healthy male adults 30 healthy male adults
Dosing Groups 6 groups of 7 people 2 groups of 15 people
Dose, Route
- Clanza® CR 200mg qd for 1day (fasted), po
- Clanza® CR 200mg qd for 1day (fed, High fat), po
- Airtal 100 mg bid for 1 day (fasted), po
- Clanza® CR 200 mg qd for 7 days,
po
- Airtal® 100 mg bid for 7 days, po
Primary Endpoint PK parameters: Cmax, AUCt
Safety Parameters AE, Vital Sign, EKG, Physical examination, Clinical Laboratory test
Start date August 24, 2009 October 7, 2009
End date October 13, 2009 November 16, 2009
PK analysis center & CRO for Clinical Trial: Hopkins Bio Research Center
Summary of Clinical Study Synopsis

2015-10-27 25
Clanza® CR tablet - Clinical Trials in humans
• Clinical equivalence between Clanza® CR (q.d.) vs. Airtal® (b.i.d., Almiral)
• All clinical data requirements are fulfilled
Single dosing PK and food effects study
Randomized, open-label, single dose, 3-treatment, 3-period
Repeated (multiple) dosing PK study
Randomized, open-label, repeated dose, 2-Way crossover
Post-marketing comparative clinical trials
Patients with chronic back pain and chronic knee
osteoarthritis
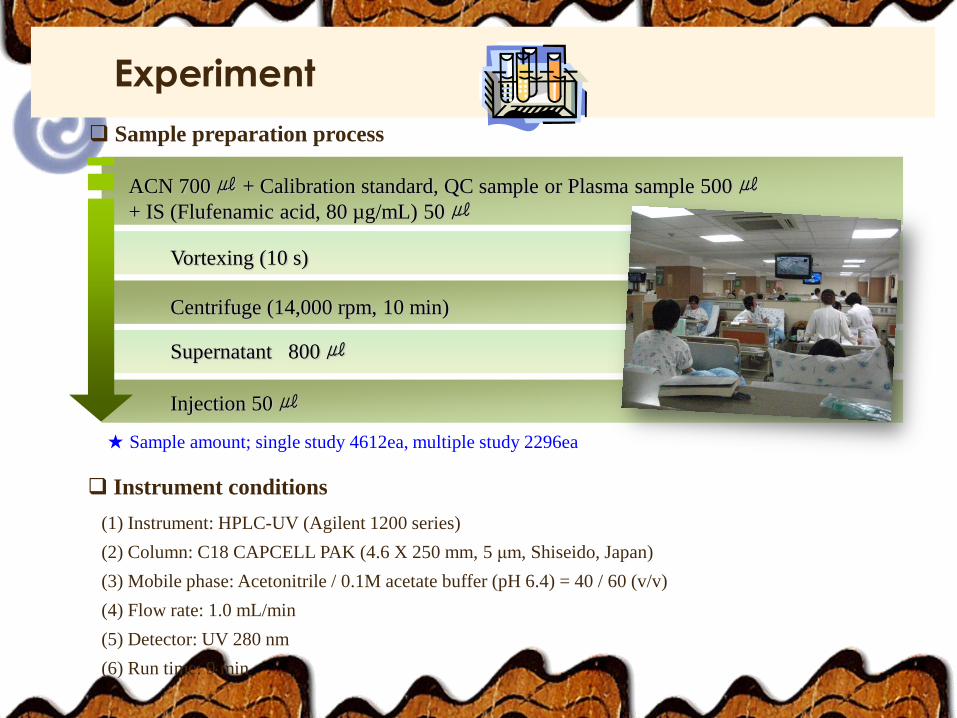
Experiment
Sample preparation process
Centrifuge (14,000 rpm, 10 min)
Supernatant 800 ㎕
Injection 50 ㎕
ACN 700 ㎕ + Calibration standard, QC sample or Plasma sample 500 ㎕
+ IS (Flufenamic acid, 80 µg/mL) 50 ㎕
Vortexing (10 s)
Instrument conditions
(1) Instrument: HPLC-UV (Agilent 1200 series)
(2) Column: C18 CAPCELL PAK (4.6 X 250 mm, 5 μm, Shiseido, Japan)
(3) Mobile phase: Acetonitrile / 0.1M acetate buffer (pH 6.4) = 40 / 60 (v/v)
(4) Flow rate: 1.0 mL/min
(5) Detector: UV 280 nm
(6) Run time: 9 min
★ Sample amount; single study 4612ea, multiple study 2296ea

Total average n=41
0
1
10
100
0 4 8 12 16 20 24
Tim e (h)
Plasma level ( g/mL)
Reference drug (fasted)
Test drug (fasted)
Mean Plasma Concentrations Following Single Oral Administration
Bioequivalence Test (Single Dose, Fasting State)
Items AUCt Cmax
90% confidence interval log 0.9975 ≤ δ ≤ log 1.0634 log 0.9144 ≤ δ ≤ log 1.0280
PK parameters Reference
(fasted)
Test
(fasted)
Cmax (μg/mL) 10.26 ± 1.81 10.61 ± 2.07
AUCt (h∙μg/mL) 42.33 ± 8.35 41.05 ± 7.66
AUC∞ (h∙μg/mL) 43.22 ± 8.62 43.31 ± 7.89
Tmax (h) 1.7 ± 0.7 1.5 ± 0.7
Λz (1/h) 0.39 ± 0.14 0.16 ± 0.07
T1/2 (h) 2.1 ± 0.9 5.0 ± 2.1
Confirming the SR pattern

Total average n=41
0
1
10
100
0 4 8 12 16 20 24
Time (h)
Pla
sma leve
l (g/m
L)
Test drug (fasted)
Test drug (fed)
Mean Plasma Aceclofenac Concentrations Following Single Oral Administration
Bioequivalence Test (Single Dose, Fed State)
Items AUCt Cmax
90% confidence interval log 0.9566 ≤ δ ≤ log 1.0198 log 0.9733 ≤ δ ≤ log 1.0942
PK parameters Test drug
(fasted)
Test drug
(fed)
Cmax (μg/mL) 10.61 ± 2.07 10.34 ± 2.27
AUCt (h∙μg/mL) 41.05 ± 7.66 41.61 ± 7.71
AUC∞ (h∙μg/mL) 43.31 ± 7.89 43.22 ± 7.69
Tmax (h) 1.5 ± 0.7 2.7 ± 1.2
Λz (1/h) 0.16 ± 0.07 0.21 ± 0.06
T1/2 (h) 5.0 ± 2.1 3.9 ± 2.5
No food effect

Items AUCt Cmax
90% confidence interval log 0.890 ≤ δ ≤ log 0.938 log 1.060 ≤ δ ≤ log 1.123
Mean Plasma Concentrations Following Single Oral Administration
PK parameters Reference drug
(fasted)
Test drug
(fasted)
Cmax (μg/mL) 3.24 ± 0.42 3.55 ± 0.56
AUCt (h∙μg/mL) 31.57 ± 4.51 29.10 ± 5.62
AUC∞ (h∙μg/mL) 34.87 ± 5.46 32.18 ± 6.59
Tmax (h) 2.61 ± 0.77 2.48 ± 0.78
Λz (1/h) 0.18 ± 0.03 0.12 ± 0.03
T1/2 (h) 3.86 ± 0.60 6.14 ± 1.46
Metabolic Bioequivalence Test (Single Dose)
Total average n=41
0
1
10
0 4 8 12 16 20 24
Tim e (h)
Plasma level (
g/mL)
Referene drug (fasted)
Test drug (fasted)
Active Metabolite (4-OH Aceclofenac)

Bioequivalence Test with Multiple Dosing
Items AUCt Cmax
90% confidence interval log 0.929 ≤ δ ≤ log 1.015 log 0.932 ≤ δ ≤ log 1.105
PK parameters Reference drug Test drug
Css,max (μg/mL) 10.00 ± 2.25 10.08 ± 1.96
Css,min (μg/mL) 0.02 ±0.07 0.07 ±0.11
AUCt (h∙μg/mL) 39.28 ± 6.68 37.99 ± 5.88
AUC∞ (h∙μg/mL) 39.60 ± 6.83 39.79 ± 5.93
Tmax (h) 1.8 ± 0.9 1.7 ± 0.9
Λz (1/h) 0.46 ± 0.15 0.16 ± 0.07
T1/2 (h) 1.7 ± 0.7 5.1 ± 2.4
Total average n=29
0
1
10
100
0 4 8 12 16 20 24
Time (h)
Pla
sm
a level (g/m
L)
Reference drug
Test drug
Mean Plasma Concentrations Following Multiple Dosing Administration

Bioequivalence Test (Multiple Dose, Metabolite)
Pharmacokinetic
parameters
Reference
drug Test drug
Css,max (μg/mL) 2.89 ± 0.78 3.17 ± 0.68
Css,min (μg/mL) 0.27 ± 0.18 0.08 ± 0.13
AUCt (h∙μg/mL) 26.53 ± 7.17 22.56 ± 5.73
AUC∞ (h∙μg/mL) 28.41 ± 8.09 24.53 ± 6.07
Tmax (h) 5.4 ± 5.4 2.4 ± 0.9
Λz (1/h) 0.22 ± 0.05 0.13 ± 0.04
T1/2 (h) 3.3 ± 0.7 5.6 ± 1.6
Total average n=29
0
1
10
100
0 4 8 12 16 20 24
Time (h)
Pla
sm
a level (g/m
L)
Reference drug
Test drug
Items AUCt Cmax
90% confidence interval log 0.817 ≤ δ ≤ log 0.890 log 1.043 ≤ δ ≤ log 1.177
Mean Plasma Concentrations Following Multiple Dosing Administration
Active Metabolite (4-OH Aceclofenac)

Information synopsis of Clanza® CR tablet
•World’s first once daily formulation of aceclofenac (200mg film coated),
satisfying medical unmet needs
•Best choice for the treatment of chronic pain management
•Improved patient compliance, taking once daily with and without food
: Reach MEC rapidly and maintain effective plasma concentration over
24 hrs due to the modified drug release profile from two-layered tablet
•Safety and efficacy
: Reduced side effects of upper gastrointestinal bleeding and
cardiovascular system
: Rapid onset of pain relief and safety for long term therapy
•Approval from Korea FDA on Apr. 14, 2010

Case II: Cilostazol Advanced Antiplatelet agent with reduced adverse events
Composition Cilostazol 200mg
Description White, oblong, controlled release tablet
Indication It is used in the treatment of ischemic symptoms including ulcer, pain and coldness of the extremities in chronic arterial occlusion. It is also indicated in preventing recurrence of cerebral infarction except cardiogenic cerebral embolism
Dosage & Administration
Adults: The recommended dose is 200 mg daily, taken as one dose(every 24 hours) Take this drug in the fasted state
Unmet Needs • Improved drug compliance by taking once-a-day tablet. • Designing double-controlled release tablet with improved dissolution • Reduced adverse events of cilostasol by maintain a plasma concentration in a
controlled manner

34
Cilostasol
Drug Information / Patient profile
• Patient compliance is the key issue for the target patient
60 years old and above: > 76%
Daily dosing regimen: Mostly 2 tablets per day (> 68%)
Concomitant drugs: Mostly once daily regimen
1st Statins (44%), 2nd Aspirin (32%), 3rd Metformin (24%), 4th
ARB (24%), 5th CCB (24%)
Co-morbidity: Diabetes (14%), Stroke (13%), Hypertension (10%)

Time (min)
0 200 400 600 800 1000 1200 1400
Dis
solu
tion (
%)
0
20
40
60
80
100
C5 (Carbomer)
F5 (Carbomer + HPMC)
H5 (HPMC)
Time (min)
0 200 400 600 800 1000 1200 1400
Dis
solu
tion (
%)
0
50
100
150
200
Reference drug (Pletal(R))
Tested drug (F5)
Time (min)
0 200 400 600 800 1000 1200 1400
Sw
ell
ing
(%
)
0
200
400
600
800
1000
1200
1400
1600
H5 (HPMC)
F5 (HPMC + Carbomer)
Formulations & dissolution profiles
Dissolution rate of reference drug and tested drug in SLS 0.3%(w/v) in water

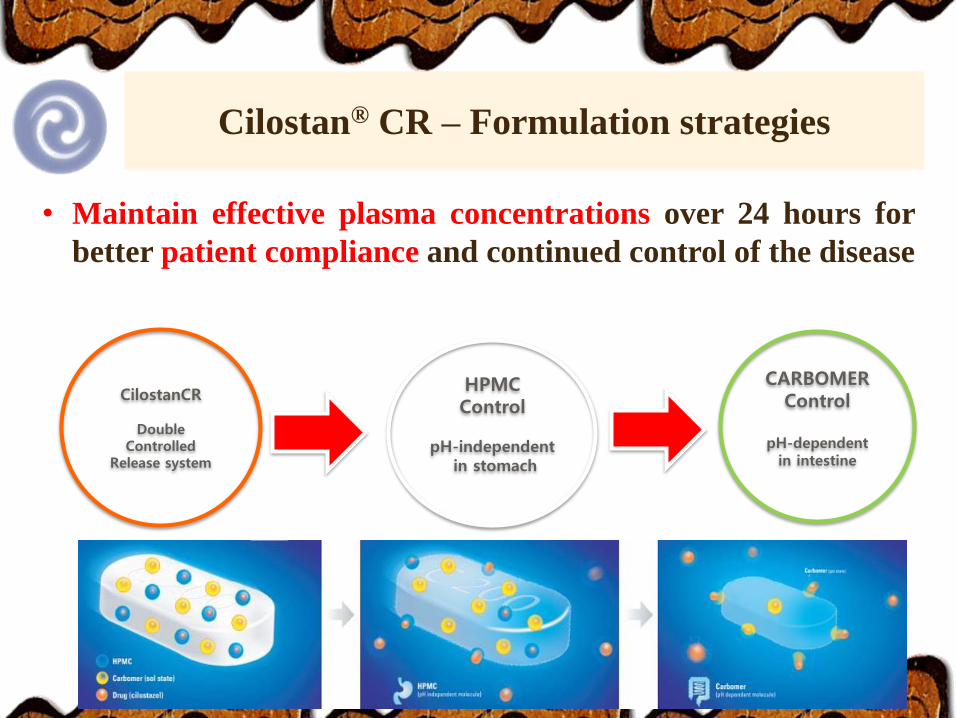
Carbomer Gastric fluid (pH 1.0~2.0)
Intestinal fluid
(pH 6.0~8.0)
Cilostazol
HPMC
HPMC Control Carbomer Control
Erosion Diffusion
Water Uptake
Sol state Gel state
Swelling
Neutralized
Sol-gel transition of carbormer according to pH value
Release-modulating mechanism: Sol-Gel proces
37
Cilostan® CR – Formulation strategies
• Maintain effective plasma concentrations over 24 hours for
better patient compliance and continued control of the disease
HPMC Control
pH-independent
in stomach
CARBOMER Control
pH-dependent
in intestine
CilostanCR
Double Controlled
Release system

Reference drug Test drug
Cmax /dose (ng/mL) 0.87 ± 0.28 0.62 ± 0.12
Tmax (h) 2.75 ± 0.61 4.17 ± 0.41
T1/2 (h) 7.25 ± 6.18 8.34 ± 1.56
AUCt (h∙ng/mL) 307.63 ± 86.14 683.77 ± 90.68
AUC∞ (h∙ng/mL) 333.72 ± 88.73 720.93 ± 95.01
AUC(0-t)/AUC(0-inf),% 92.41 ± 7.59 94.88 ± 3.28
F* (%) - 108.0
* F : Relative Bioavailability to Pletaal® 200mg
Bioavaility (%) = (AUC∞ , Test / AUC∞ Ref x 2 ) x 100 Concentration-time profile of Aceclofenac after oral administration at a
dose of tablet of test (Cilostan® CR TAB 200 mg) and reference (Pletaal®
TAB 100 mg) formulation to male beagle dogs
mean (n =6)
0
50
100
150
0 6 12 18 24 30 36 42 48
Time (h)
Pla
sm
a level (n
g/m
L)
.
Pletaal TAB 100mg
CILOSTAN CR TAB 200mg
Preclinical Test in Beagle Dogs (Oral)
Enhanced bioavailability due to the solubility and controlled release

39
Cilostan® CR – Clinical trial
Clinical equivalence between Cilostan CR® (q.d.) vs. Pletaal
(b.i.d., Otsuka)
All clinical data requirements are fulfilled
• Single Dose Pharmacokinetic Study: Randomized, Open-label, Single
dose, 2-Treatment, 2-Period, 2-Way Crossover
•Repeated Dose Pharmacokinetic Study: Randomized, Open-label,
Repeated dose, 2-Treatment, 2-Period, 2-Way Crossover
•Food Effect Study: Randomized, Open-label, Single dose, 2-Treatment,
2-Period, 2-Way Crossover Study under fed conditions

Mean Plasma Concentrations Following Single Oral Administration
Items AUCt Cmax
90% confidence interval log 0.8087 ≤ δ ≤ log 1.0791 log 0.8217 ≤ δ ≤ log 1.2195
PK parameters Reference drug
(fasted)
Test drug
(fasted)
Cmax (ng/mL) 1512 ± 498 1569 ± 697
AUCt (h∙ng/mL) 30031 ± 15604 27764 ± 15501
AUC∞ (h∙ng/mL) 31195 ± 17064 30710 ± 19639
Tmax (h) 3.70 ± 1.88 4.03 ± 1.59
Λz (1/h) 0.14 ± 0.05 0.10 ± 0.05
T1/2 (h) 8.96 ± 5.25 12.95 ± 8.10
Cilostazol
10
100
1000
10000
0 12 24 36 48 60 72
Pla
sm
a l
evel (n
g/m
L)
.
Time (h)
Total average, n=30
Reference drug
Test drug
Bioequivalence Test (Single Dose, Fasting State)
Highly improved and sustained over a 24-
hour period in a controlled manner.
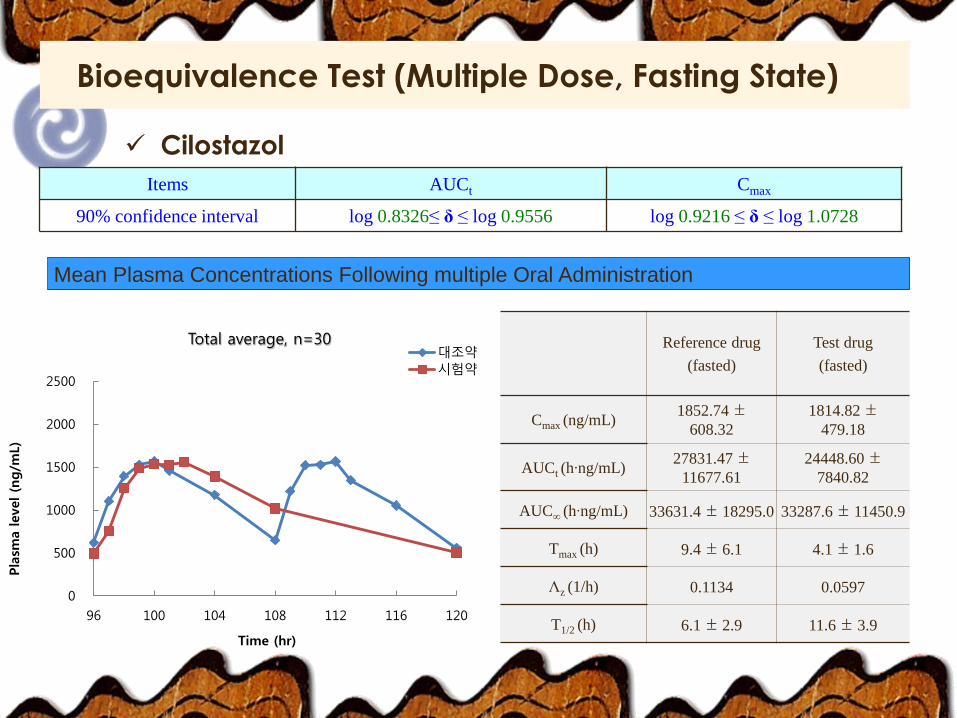
Mean Plasma Concentrations Following multiple Oral Administration
Items AUCt Cmax
90% confidence interval log 0.8326≤ δ ≤ log 0.9556 log 0.9216 ≤ δ ≤ log 1.0728
Reference drug
(fasted)
Test drug
(fasted)
Cmax (ng/mL) 1852.74 ±
608.32
1814.82 ±
479.18
AUCt (h∙ng/mL) 27831.47 ±
11677.61
24448.60 ±
7840.82
AUC∞ (h∙ng/mL) 33631.4 ± 18295.0 33287.6 ± 11450.9
Tmax (h) 9.4 ± 6.1 4.1 ± 1.6
Λz (1/h) 0.1134 0.0597
T1/2 (h) 6.1 ± 2.9 11.6 ± 3.9
Cilostazol
0
500
1000
1500
2000
2500
96 100 104 108 112 116 120
Pla
sma level (n
g/m
L)
Time (hr)
Total average, n=30 대조약
시험약
Bioequivalence Test (Multiple Dose, Fasting State)

Mean Plasma Concentrations Following single Oral Administration
Items AUCt Cmax
90% confidence interval log 0.7777 ≤ δ ≤ log 0.8787 log 1.2834 ≤ δ ≤ log 1.4332
PK parameters Reference drug
(fasted)
Test drug
(fasted)
Cmax (ng/mL) 1968.6 ± 25.1 2715.4 ±758.9
AUCt (h∙ng/mL) 31686.8 ±
10327.8
26933.2 ±
10491.1
AUC∞ (h∙ng/mL) 31923.8 ± 10352.7 27424.5 ± 10526.5
Tmax (h) 9.5 ± 6.2 5.0 ± 1.1
Λz (1/h) 0.1193 0.0769
T1/2 (h) 5.8 ± 1.9 9.0 ± 4.2
Cilostazol
0
1000
2000
3000
0 12 24 36 48 60 72
Pla
sma level (n
g/m
L)
Time (hr)
Total average, n=30 대조약
시험약
Bioequivalence Test (Single Dose, Fed State)

• Formulation strategies: Dual-controlled release cilostazol tablet which
exhibits a stable release pattern without any variation in the percentage
eluted depending on the pH in the stomach in addition to an effect
whereby release of the drug is delayed, by using a release-controlling
polymer consisting of a mixture of hydrophilic polymer and a pH-
dependent polymer
• Dual-controlled release system prevents the rapid release of API in the
tablet to ensure a long retention time and avoid adverse effects such as
headache, flushing
• No significant PK difference in AUCi / dose, Cmax / dose and t 1 / 2 but
significant difference in Tmax

44
• The World’S One and Only
Cilostazol controlled release 200mg tablet (white elliptical /
oval)
•Improved patient compliance
One 200mg tablet, once daily (Pletaal, twice daily)
•Safe and Effective
Reduced side effects of headache & tachycardia
•Korea FDA Approval
Approval from Korea FDA on Feb. 28, 2013
• Approved indications
Peripheral Artery Occlusive Disease (PAOD) Cerebral
Infarction
Cilostan® CR - Drug Information / Patient profile

Summary and Conclusions
• Patient-centric drug products have been designed to meet the clinical unmet
needs for geriatric and pediatric patients who have different pathophysiology,
taking into account their specific characteristics in terms of age, physiology,
morbidity/comorbidity and functional impairments.
• Patient-centric drug product development provides more medical & clinical
benefits for targeted patient population and their specific needs with a safe and
patient-friendly administration and good quality management.
• Patient-centric drug products are based on the combination of existing or new
formulation and drug delivery technologies, along with efficient, highly flexible,
and innovative manufacturing technologies and platforms
• In the meanwhile, use of big data gives a privilege for patient centricity and
pharma industry to help improve the efficiency of the drug discovery and
development process.

Thank you for your kind attention!

![Bimodal Gastroretentive Drug Delivery Systems of ......a gastroretentive floating drug delivery system[12]. The drug concentrations can be controlled by formulating bimodal drug delivery](https://static.fdocuments.in/doc/165x107/5e6f0293269d113bd9170da6/bimodal-gastroretentive-drug-delivery-systems-of-a-gastroretentive-floating.jpg)