
Patient and resource scheduling of multi-step medical...
18
This article was downloaded by: [Texas A&M University Libraries] On: 10 September 2012, At: 07:36 Publisher: Taylor & Francis Informa Ltd Registered in England and Wales Registered Number: 1072954 Registered office: Mortimer House, 37-41 Mortimer Street, London W1T 3JH, UK IIE Transactions on Healthcare Systems Engineering Publication details, including instructions for authors and subscription information: http://www.tandfonline.com/loi/uhse20 Patient and resource scheduling of multi-step medical procedures in nuclear medicine Eduardo Pérez a , Lewis Ntaimo a , Wilbert E. Wilhelm a , Carla Bailey b & Peter McCormack b a Department of Industrial and Systems Engineering, Texas A&M University, 3131 TAMU, College Station, TX, 77843, USA b Scott and White Clinic, 2401 S. 31st Street, Temple, TX, USA Version of record first published: 02 Dec 2011. To cite this article: Eduardo Pérez, Lewis Ntaimo, Wilbert E. Wilhelm, Carla Bailey & Peter McCormack (2011): Patient and resource scheduling of multi-step medical procedures in nuclear medicine, IIE Transactions on Healthcare Systems Engineering, 1:3, 168-184 To link to this article: http://dx.doi.org/10.1080/19488300.2011.617718 PLEASE SCROLL DOWN FOR ARTICLE Full terms and conditions of use: http://www.tandfonline.com/page/terms-and-conditions This article may be used for research, teaching, and private study purposes. Any substantial or systematic reproduction, redistribution, reselling, loan, sub-licensing, systematic supply, or distribution in any form to anyone is expressly forbidden. The publisher does not give any warranty express or implied or make any representation that the contents will be complete or accurate or up to date. The accuracy of any instructions, formulae, and drug doses should be independently verified with primary sources. The publisher shall not be liable for any loss, actions, claims, proceedings, demand, or costs or damages whatsoever or howsoever caused arising directly or indirectly in connection with or arising out of the use of this material.
Transcript of Patient and resource scheduling of multi-step medical...

This article was downloaded by: [Texas A&M University Libraries]On: 10 September 2012, At: 07:36Publisher: Taylor & FrancisInforma Ltd Registered in England and Wales Registered Number: 1072954 Registered office: Mortimer House,37-41 Mortimer Street, London W1T 3JH, UK
IIE Transactions on Healthcare Systems EngineeringPublication details, including instructions for authors and subscription information:http://www.tandfonline.com/loi/uhse20
Patient and resource scheduling of multi-step medicalprocedures in nuclear medicineEduardo Pérez a , Lewis Ntaimo a , Wilbert E. Wilhelm a , Carla Bailey b & Peter McCormack ba Department of Industrial and Systems Engineering, Texas A&M University, 3131 TAMU,College Station, TX, 77843, USAb Scott and White Clinic, 2401 S. 31st Street, Temple, TX, USA
Version of record first published: 02 Dec 2011.
To cite this article: Eduardo Pérez, Lewis Ntaimo, Wilbert E. Wilhelm, Carla Bailey & Peter McCormack (2011): Patientand resource scheduling of multi-step medical procedures in nuclear medicine, IIE Transactions on Healthcare SystemsEngineering, 1:3, 168-184
To link to this article: http://dx.doi.org/10.1080/19488300.2011.617718
PLEASE SCROLL DOWN FOR ARTICLE
Full terms and conditions of use: http://www.tandfonline.com/page/terms-and-conditions
This article may be used for research, teaching, and private study purposes. Any substantial or systematicreproduction, redistribution, reselling, loan, sub-licensing, systematic supply, or distribution in any form toanyone is expressly forbidden.
The publisher does not give any warranty express or implied or make any representation that the contentswill be complete or accurate or up to date. The accuracy of any instructions, formulae, and drug doses shouldbe independently verified with primary sources. The publisher shall not be liable for any loss, actions, claims,proceedings, demand, or costs or damages whatsoever or howsoever caused arising directly or indirectly inconnection with or arising out of the use of this material.

IIE Transactions on Healthcare Systems Engineering (2011) 1, 168–184Copyright C© “IIE”ISSN: 1948-8300 print / 1948-8319 onlineDOI: 10.1080/19488300.2011.617718
Patient and resource scheduling of multi-step medicalprocedures in nuclear medicine
EDUARDO PEREZ1,∗, LEWIS NTAIMO1, WILBERT E. WILHELM1, CARLA BAILEY2
and PETER MCCORMACK2
1Department of Industrial and Systems Engineering, Texas A&M University, 3131 TAMU, College Station, TX 77843, USAE-mail: [email protected] and White Clinic, 2401 S. 31st Street, Temple, TX, USA
Received October 2010 and accepted August 2011.
The rise in demand for specialized medical services in the U.S. has been recognized as one of the contributors to increased health carecosts. Nuclear medicine is a specialized service that uses relatively new technologies and radiopharmaceuticals with a short half-lifefor diagnosis and treatment of diseases. Nuclear medicine procedures are multi-step and have to be performed under restrictive timeconstraints. Consequently, managing patients in nuclear medicine clinics is a challenging problem that has received little researchattention. In this paper, we derive algorithms for scheduling nuclear medicine patients and resources. We validate our algorithmsusing simulation of an actual nuclear medicine clinic based on historical data and compare the performance of our algorithms withthe methods currently used in the clinic. The results we obtain provide useful insights into managing patients and resources in nuclearmedicine clinics. For example, results show that patient throughput can be increased when some clinic resources are reserved toexclusively serve specific procedures on those days when higher demand is expected.
Keywords: Health care, nuclear medicine, patient service, scheduling, simulation
1. Introduction
Nuclear medicine is a sub-specialty of radiology that pro-vides highly specialized services by means of new technol-ogy for diagnosis and treatment of diseases. The increaseddemand for medical diagnostic procedures has been recog-nized as one of the contributors for the rise of health carecosts in the U.S. Physicians are becoming more prone toasking patients to undergo specialized procedures in orderto obtain more accurate diagnoses. Thus, the challenge ofscheduling patients and resources in specialized clinics suchas nuclear medicine is a problem of increasing concern. Thispaper holds two research objectives. The first is to derivealgorithms to assist nuclear medicine managers in schedul-ing patients and resources more efficiently by consideringthe perspectives of both patients and managers. The sec-ond is to evaluate the scheduling algorithms computation-ally using data from an actual clinic to enhance insightsconcerning trade offs in patient and resource schedulingstrategies.
∗Corresponding author
Nuclear medicine procedures (tests) require the adminis-tration of a radiopharmaceutical (radioactive isotope, e.g.,iodine-131) to the patient and typically involve multiplesteps and resources. Images of specific body organs aretaken (i.e., scanned) using gamma cameras that sense ra-diation emitted by the radiopharmaceutical. Since radio-pharmaceuticals have a short half-life (minutes), their decayimposes strict time constraints on scheduling patients andresources in order to get good quality scans. Thus, schedul-ing patients in nuclear medicine requires very strict proce-dure protocols, that, if not followed, can result in a waste oftime, money and resources because the patient might haveto be re-scheduled. Some nuclear medicine tests requireonly a single scan while others involve multiple scans inone day. Each scan takes several minutes to hours to com-plete and must occur within a narrow time window afterradiopharmaceutical administration to assure scan quality.
Multiple resources are required to perform each nu-clear medicine procedure. Resources include technologists;gamma cameras; radiopharmaceuticals; and sometimes, anurse or EKG (electrocardiography) technician. Gammacameras can cost up to a million dollars and thus haveto be used and managed effectively. Since many nuclearmedicine clinics must have radiopharmaceuticals prepared
1948-8300 C© 2011 “IIE”
Dow
nloa
ded
by [
Tex
as A
&M
Uni
vers
ity L
ibra
ries
] at
07:
36 1
0 Se
ptem
ber
2012

Multi-step procedure scheduling 169
by remote radio-pharmacies, scheduling their delivery, pa-tient injection and image acquisition requires lead timeand must be carefully managed. Each radiopharmaceuti-cal may cost as much as several hundred dollars. Resourcesrequired to perform each procedure step must be availableat the scheduled times. Therefore, scheduling patients, re-sources, and radiopharmaceutical preparation and deliveryis a challenging problem for nuclear medicine departments.In fact, practical features that surround the managementof patients and resources in nuclear medicine make it aunique problem with limited research reported in the liter-ature. Consequently, providing a high quality of service tothe patient through the use of mathematical techniques is ofgreat interest to nuclear medicine managers. Furthermore,very few commercial packages are available for patient ser-vice management and those that are available do not in-corporate algorithms for scheduling patients and resourcesefficiently.
We implement our scheduling algorithms in JAVA andtest them using discrete event simulation (Perez et al., 2010).We obtain computational results that provide useful in-sights into managing patient service and resources utiliza-tion in nuclear medicine. While this paper focuses on nu-clear medicine, we believe that results can be applied tosimilar health care settings that may not be as complexas nuclear medicine. For example, our algorithms can beapplied to diagnostic imaging areas such as magnetic reso-nance imaging (MRI) and CT scan scheduling.
The rest of the paper is organized as follows: we re-view closely related work in Section 2 and provide pre-liminaries on nuclear medicine resources and proceduresin Section 3. We derive algorithms for scheduling nuclearmedicine patients and resources in Section 4. We reporton our computational study, which quantifies importanttrade-offs among patient and resource scheduling strate-gies, in Section 5. We also discuss the results and highlightnew insights into the complexity of nuclear medicine pa-tient service management. We end the paper with someconcluding remarks and directions for further research inSection 6.
2. Literature review
Facilities dedicated to the diagnosis and treatment of dis-eases are vital in comprehensive health care systems. Met-tler et al. (2008) found a 5-to-6 fold increase in medical di-agnostic procedures in the U.S. from 1972 to 2005, whereasthe U.S. population increased by approximately 50%. Thisincrease in diagnostic testing has been identified as one ofthe potential causes for increased health care costs in theU.S. (Zhang, 2007). Facilities that are hospital-based suchas radiology clinics are highly specialized at providing dif-ferent types of services to patients. Equipment utilized fordiagnostic procedures is usually expensive and the uniquecharacteristics of radiology procedures make finding an ef-
ficient way of scheduling patients and resources challenging(Vermeulen et al., 2009). A necessary condition for overallhospital efficiency is the effective utilization of medical di-agnostic facilities, which are used by almost every patientthat enters a hospital (O’Kane, 1981).
Operations research techniques such as simulation andmathematical optimization have been shown to be viableapproaches for patient and resource scheduling in the lit-erature. For example, Ho and Lau (1992) and Ho et al.(1995) used simulation to compare the performance of fiftyappointment rules under various operating environments inoutpatient clinics. They concluded that no rule will performwell under all environments and proposed a simple heuristicthat uses the characteristics of the system to select one rule.Wang (1993) considered a single server system with expo-nential service times and used a recursive procedure to pre-scribe optimal appointment time. The author showed thatit is optimal to schedule appointments that require shorterservice times at the start and end of the day and longerones in the middle of the day (dome-shaped). Wang (1997)extended these results to model service times as any phase-ttype distribution. Klassen and Rohleder (1996) used simu-lation to study different strategies for sequencing patientsthat are classified according to their expected service timevariability. They concluded that scheduling patients, whoseservice times have low variances, at the beginning of the dayoutperforms the Ho and Lau (1992) best performing rules.Extending this work, Rohleder and Klassen (2000) consid-ered error in classifying patients. They concluded that evenwith classification errors, their rule still outperformed therules presented by Ho and Lau (1992).
Liu and Liu (1998a) and Liu and Liu (1998b) stud-ied a clinic with multiple doctors where doctors arrivaltimes are random. They identified properties shared bythe best appointment schedules using simulation. Robin-son and Chen (2003) determined optimal patient appoint-ment times when the sequence of patients is given. Theyformulated the problem as a stochastic linear program andused simulation-based techniques to compare the perfor-mances of a variety of heuristic appointment rules. Den-ton and Gupta (2003) presented a two-stage stochasticlinear programming model to determine the optimal ap-pointment times for patients with arbitrarily distributedservice times and showed that the optimal sequence oftime intervals is dome-shaped. Cayirli et al. (2006) stud-ied the scheduling of patients in ambulatory care clinicsand investigated the interaction between patient character-istics and appointment system elements. They concludedthat patient sequencing has a greater effect in the perfor-mance of the system than the choice of an appointmentrule. Gupta and Wang (2008) used a Markov DecisionProcess (MDP) to model a primary care scheduling prob-lem. They considered patient choices and showed that, ifthe clinic is served by one physician, the optimal book-ing policy can be characterized. We refer interested read-ers to recent surveys of outpatient appointment scheduling
Dow
nloa
ded
by [
Tex
as A
&M
Uni
vers
ity L
ibra
ries
] at
07:
36 1
0 Se
ptem
ber
2012

170 Perez et al.
Table 1. Human resources responsibilities in nuclear medicine
Technologists Nurses Physicians Managers
Hydrate patient Hydrate patient Hydrate patient Hydrate patientRadiopharmaceutical Radiopharmaceutical Radiopharmaceutical Radiopharmaceutical preparation
preparation administration administrationImaging Draw doses Draw doses Radiopharmaceutical administration
research by Cayirli and Veral (2003) and Gupta and Denton(2008).
Prior research on patient service management in nuclearmedicine is very limited. However, some research has beenreported in related health care environments such as radiol-ogy, radiotherapy, CT scan and MRI clinics. For example,Conforti et al. (2007) proposed an optimization model foroutpatient scheduling within a radiotherapy departmentwhere patients must visit the treatment center several timesduring the week. Green et al. (2006) studied the problem ofscheduling different types of patients that arrive randomlyduring the week to an MRI facility. They presented a finite-horizon dynamic program for a single server appointmentschedule that allows at most one patient per time period.The problem of managing patients in a CT scan clinic wasaddressed by Patrick and Puterman (2007). They presenteda mathematical formulation that prescribes appointmenttimes to maximize the utilization of resources, subject toan overtime constraint. The authors assumed a pool of pa-tients that can scheduled when time slots become available.They used simulation to show a decrease in patient waitingtime for service. Vermeulen et al. (2009) devised an adap-tive approach to optimize resource schedules in a CT scanfacility. They used simulation for case analysis and demon-strated that their approach makes efficient use of resourcecapacity.
This research differs from earlier studies in a number ofways. First, appointment scheduling in nuclear medicinedeals with lead times required to obtain radiophar-maceuticals. Second, procedures in nuclear medicineinvolve multiple steps, each of which requires the useof two or more resources. Third, procedures in nuclearmedicine follow sequential protocols that impose stricttime constraints on the starting time of each step. Together,these characteristics make the problem of schedulingpatients and resources in nuclear medicine challenging.In fact, Gupta and Denton (2008) identified the problemof scheduling patients in highly constrained health careenvironments as a current research open challenge.
3. Problem description
We consider a nuclear medicine clinic that has a limitednumber of resources to serve patients. Let S be the set ofstations and R be the set of human resources available atthe clinic. Each station contains at least one type of equip-
ment. Stations are classified according to the equipmentthey have. Nuclear medicine equipment include differenttypes of gamma cameras and treadmills for cardiovascu-lar tests. The staff includes four types of human resources:technologists, nurses, physicians, and managers. Each hu-man resource has his/her own expertise and experience, de-termining the set of procedure steps or tasks that they canperform and the amount of time required to complete eachone. Some of the procedure steps that can be performed bythe human resources are listed in Table 1.
Nuclear medicine procedures are requested by the pa-tient’s primary physician. A service request usually includesa procedure type from set P and also a preferred day of theweek q. Patient appointments are scheduled when the re-quest is received and decisions are made without takingfuture requests into account. Unlike patients in generaloutpatient clinics, those in nuclear medicine show up fortheir appointments most of the time.
Nuclear medicine clinics perform |P| different proce-dures, each involving multiple steps or tasks. Table 2presents a list of nuclear medicine procedures along withtheir current procedural terminology (CPT) codes. Proce-dure p ∈ P involves a total number of steps n p. Each stepk of procedure p has an estimated duration βkp and thetotal duration of the procedure is given by
∑n p
k=1 βkp. Atleast one radiopharmaceutical from set A is administeredto the patient at the beginning of each procedure. Radio-pharmaceuticals are requested in advance and they need tobe at the clinic by the time of the patient appointment. Inaddition, each step k of procedure p requires one station
Table 2. Examples of nuclear medicine procedures
CPT Code Name
78465 Cardiovascular Event (CVE)Myocardial Imaging (SP-M)
78815 Positron Emission Tomography (PET)/Computed Tomography (CT) skull to thigh
78306 MSB-bone imaging (whole body)78315 MSC-bone imaging (three phase)78223 GIC-Hepatobiliary imaging78472 CVJ-cardiac blood pool78585 REB-Pulm perfusion/ventilation78006 ENC-Thyroid imaging78195 HEE-Lymphatic imaging78464 CVD-Myocardial imaging (SP-R ORS)
Dow
nloa
ded
by [
Tex
as A
&M
Uni
vers
ity L
ibra
ries
] at
07:
36 1
0 Se
ptem
ber
2012

Multi-step procedure scheduling 171
Table 3. Procedure 78315: MSC-bone imaging (three phase)
Step (k) Task Average time (mins.) Station (Skp) Human Resource (Rkp)
1 Radiopharmaceutical injection 20 Axis; P2000; Meridian; TRT Technologist; Nurse; Manager2 Imaging 15 Axis; P2000; Meridian Technologist; Manager3 Uptake delay 165 Waiting room4 Imaging 45 Axis; P3000; Meridian Technologist; Manager
s ∈ S and at least one human resource r ∈ R to be per-formed.
Table 3 describes the MSC-bone imaging procedure, CPT78315. This procedure has four steps and an average com-pletion time of 245 minutes. Table 3 lists for each procedurestep; the required task, the expected time duration, and theset of feasible stations and human resources. We define setSkp as the set of stations at which step k of procedure pcan be performed. Similarly, let Rkp be the set of humanresources qualified to perform step k of procedure p. Eachtask must be performed by one of the qualified humanresources at one station among the feasible stations Skp.
We evaluate the performance of our scheduling algo-rithms using measures that take into account the perspec-tives of both the clinic patient and the manager. These twoperspectives are relevant to nuclear medicine patient and re-source scheduling. Table 4 describes the performance mea-sures used to quantify the level of patient satisfaction inhealth care clinics, while Table 5 shows performance mea-sures that consider the manager’s perspective.
To provide a unified perspective of all the relevantcomponents, we now give a simple example to illus-trate patient/resource scheduling in nuclear medicine. Fig-ure 1(a) depicts two of the procedures performed in nuclearmedicine. We list for each procedure the corresponding re-quirements of each step as follows: time duration (time),station (s), and human resource (r ). For the purpose ofthis example, only one station and one human resource isassociated with each procedure step. Figure 1(b) depictsa schedule for procedure 78815 (PET/CT skull to thigh)where the patient is assigned to arrive at the beginning ofthe day. The schedule shows that four resources are re-quired at different times of the day to perform this pro-cedure: nurse, technologist, treatment (TRT) station andaxis station. Figure 1(c) shows the schedule for procedure78815 and procedure 78465 (CVE, SP-M). Since some of
the resources are unavailable at the beginning of the day,the second procedure, in dark color, has to be scheduledlater in the day. The schedule shows that for procedure78465 five resources are required namely; EKG technolo-gist, technologist, TRT station, treadmill station, and axisstation. Also, observe that no other procedure can be fittedinto the schedule due to the unavailability of the resourcesat particular times. For instance, an additional procedure78465, represented with dot lines, cannot be scheduled onthis day because the axis station and the technologist areunavailable during the time slots that would be required forthe last step of the procedure.
4. Patient and resource scheduling
We now turn to patient and resource scheduling and derivetwo algorithms: fixed resource (FR) and procedure resourceassignment (PRA). Both algorithms schedule patients fol-lowing a general scheduling structure. The algorithms firstsearch for the patient’s preferred day for the appointment.If the search results in an appointment for which the patienthas to wait more than a month, then an earlier appointmenton an alternate day is considered.
We first derive the FR algorithm, which involves fixingsome of the members of the human resources to specificstations. This algorithm is based on the practical experi-ence of the last two authors of this paper. This algorithmwill provide a benchmark for our methodology using thePRA algorithm which is explained later in subsection 4.2.We assume that no more than one patient can be sched-uled to use the same resource at the same time and thatthe scheduling horizon is long enough so that all patientrequests are satisfied.
For convenience, we list the notation we use to describeour scheduling algorithms in Table 3. In addition, we usethe following symbols:← denotes assignment;== denotes
Table 4. Performance measures for patient’s perspective
Name Description Reference
Waiting time type 1 Waiting time from the time of the procedure request until the time of Rohleder and Klassen (2002),the appointment Robinson and Chen (2003)
Preference ratio Number of times patients are scheduled on the date requested above all Green et al. (2006)patient requests
Cycle time Time patient spends in the system Podgorelec and Kokol (1997),Rohleder and Klassen (2000)
Dow
nloa
ded
by [
Tex
as A
&M
Uni
vers
ity L
ibra
ries
] at
07:
36 1
0 Se
ptem
ber
2012

172 Perez et al.
Table 5. Performance measures for manager’s perspective
Name Description Reference
Equipment utilization The amount of time an equipment is used during Rohleder and Klassen (2002),operating hours Denton et al. (2006)
Human resource utilization The amount of time a human resource is used during Denton et al. (2006)operating hours Centeno et al. (2000)
Patient throughput Number of patients served per day Ramakrishnan et al. (2004)
(equality) comparison, and && denotes logic “and.” Wedefine the set of day and time slot pairs (d, t) for resource ras Ur = {(d, t)| 1 ≤ d ≤ h, 1 ≤ t ≤ τ }. Similarly, we definethe set of day and time slot pairs (d, t) for station s as Vs =
{(d, t)| 1 ≤ d ≤ h, 1 ≤ t ≤ τ }. The sets Ur and Vs includeall the time slots that are already scheduled. The set of dayand time slot pairs (d, t) for patient j schedule is defined asL j = {(d, t)| 1 ≤ d ≤ h, 1 ≤ t ≤ τ }.
Fig. 1. Example showing one and two scheduled procedures (color figure available online).
Dow
nloa
ded
by [
Tex
as A
&M
Uni
vers
ity L
ibra
ries
] at
07:
36 1
0 Se
ptem
ber
2012

Multi-step procedure scheduling 173
Table 6. Scheduling problem sets and parameters
Sets
J : set of patients, indexed jP : set if procedures, indexed pJp: set of patients requesting procedure p, indexed jT : set of time periods tH : set of days, indexed hI : set of resources, indexed iS : set of stations, indexed sR : set of human resources, indexed rP : set of nuclear medicine procedures, indexed pA : set of radiopharmaceuticals, indexed aSkp : set of stations where step k of procedure p can be performedRkp : set of human resources qualified to perform step k of procedure pIkp : set of resources that can be used to perform step k of procedure p, Ikp={Rkp ∪ Skp}Litj : set of appointment star times that require the use of resource i at time-slot t for patient jKitj : set of procedure steps that require the use of resource i at time-slot t for patient jTi j : set of time-slots where resource i could be used to serve patient jTaj : set of time-slots where radiopharmaceutical a could be used to serve patient jL j : Set of day and time slot pairs, (d, t), for patient j .Ur : Set of day and time slot pairs, (d, t), for human resource r schedule.Vs : Set of day and time slot pairs, (d, t), for station s schedule.
Parameters
i : subscript, for the i resourcej : subscript, for the j patienta : subscript, for the a radiopharmaceuticalp : subscript, for the p procedurek : subscript, for the k step of a procedure� : subscript, for the � starting time-slot for a patient appointmentt : subscript, for the t time-slot, incremental timeτ : total number of time-slots in a day, indexed t, . . . , τβkp : number of time-slots required to complete step k of procedure pn p : total number of steps for procedure p, indexed k, . . . , n pρ : variable representing resource r or station sδp : total duration of procedure pω : Number of days in a weekµ : Number of days in a monthm : Number of days before arrival of radiopharmaceutical after placing orderq : day of the week requested by patient, indexed q = 1, . . . ,5, where
1 =Monday, 2 = Tuesday, 3 =Wednesday, 4 = Thursday, 5 = Friday
For ease of exposition, we first describe a function,CheckSchedule(), which is implemented by both the FRand PRA algorithms (Fig. 2). This function checks theavailability of a human resource (when ρ = r ) or a station
CheckSchedule (Gρ, d, t, βkp)1 G ← Gρ;2 for time = t to t + βkp do3 if (d, time) ∈ G then4 return false;5 else6 time ← time + 1;7 end8 end9 return true;
Fig. 2. Pseudocode for CheckSchedule().
(when ρ = s) during a given time interval [t, t + βkp], andreturns a boolean indicating whether (true) or not (false)that time interval is available. If any of the time slots withinthe interval [t, t + βkp] is occupied, meaning the time slotis in the set G, the function returns f alse; otherwise, it re-turns true. The function simply checks whether or not anyof the time slots from time t to t + βkp are included in thecurrent schedule.
The FR and PRA algorithms share the same overallstructure described by the pseudocode in Fig. 3. The indexset of patients J is initialized in line 1. Lines 2 and 3define the time horizon (day and time) over which patientrequests are to be received. Upon arrival (line 4) patientrequests are incorporated in set J as they arrive (line 5).A function called ServeRequest-Algorithm(), whereAlgorithm denotes FR or PRA, uses patient information
Dow
nloa
ded
by [
Tex
as A
&M
Uni
vers
ity L
ibra
ries
] at
07:
36 1
0 Se
ptem
ber
2012

174 Perez et al.
Scheduling-Algorithm1 J ← {∅}, j = 0;2 while d ≤ h do3 while t ≤ τ do4 (pj , q) ← GetPatientRequest(j);5 J ∪ {pj}, dj ← d, tj ← t, j ← j + 1;6 Lj ← ServeRequest-Algorithm (j, pj , dj , tj , q);7 end8 end
Fig. 3. Pseudocode for Scheduling-Algorithm.
(p, q, d, and t) and finds an appointment L j (line 6).The two algorithms differ in the way they implement thisfunction.
4.1. The fixed resource (FR) algorithm
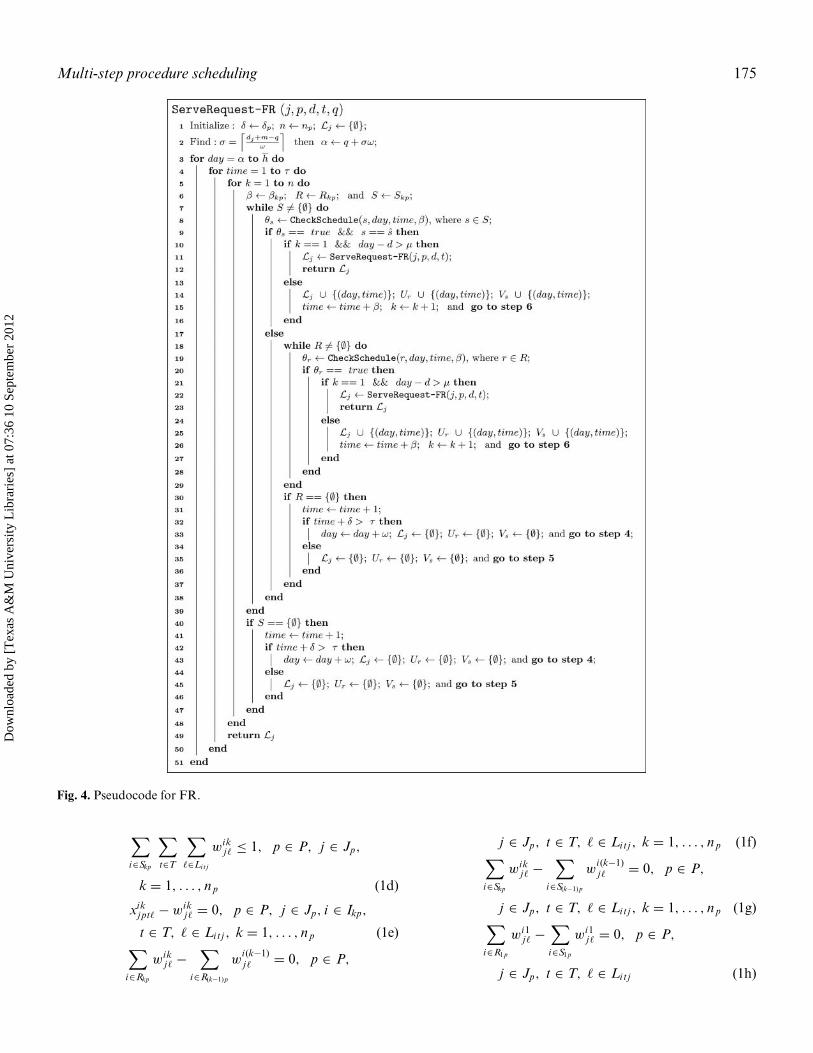
The FR algorithm allows the patient ( j ) to provide a pre-ferred day of the week (q). Using this preferred day, a searchfor an appointment is performed based on the patient’s re-quested procedure p. After the earliest feasible appoint-ment is found, the algorithm determines how long the pa-tient would have to wait. If waiting time is longer than amonth, the algorithm searches for an alternative appoint-ment (different day of the week) with a shorter waiting time.We use a boolean variable θ to store the output returnedby the CheckSchedule() function. Recall that θ takes avalue of true if a resource (human r or station s) is avail-able, and f alse otherwise. In the FR algorithm a groupof human resources (e.g., two technologists) are assignedto always serve patients at specific stations. For example,technologists 1 and 2 must serve all patients whose proce-dures require the use of stations s1 and s2, respectively. Weuse s to denote the stations that may have human resourcesassigned. Figure 4 presents the pseudocode for FR, whichis invoked by the function ServeRequest-FR().
Line 1 of FR initializes parameters. The first day onwhich FR attempts to schedule an appointment is deter-mined in line 2 using the following information: day whenthe request was received (d), patient preferred day (q), andthe number of days (m) needed to obtain the radiopharma-ceutical required for the procedure. The scheduling hori-zon, which ends on day h, is defined in lines 3 and 4. Inline 5 we begin a search for an available combination ofstation and human resource for each procedure step k. Abreadth-first search is conducted to select a station fromset S as well as a human resource from set R (line 6). Weuse breadth-first search to balance work assignments on allresources (load balancing).
Line 9 identifies those stations to which human resourceshave been fixed. A fixed human resource always stays inthe same station. Consequently, when the availability ofa station with a fixed human resource is confirmed, thealgorithm also confirms the availability of the human re-source because they share the same schedule (lines 14–15).
If the station found does not have a fixed human resource,a search is performed to find a qualified human resourcefrom set R (lines 17–19). After finding the resources re-quired for the first step of the procedure, we check that thewaiting for the appointment does not exceed a month (line10 and line 21).
If no station is available for one of the procedure steps(line 31), the current start time for the procedure is in-creased (line 32) by one time slot. Using the new start time,the algorithm checks if the amount of time required toperform the procedure exceeds the remaining time on theday searched (line 33). If the time available in the day isnot enough, the algorithm moves to the following week toperform a new search on the day requested by the patient(line 34). Otherwise, the algorithm begins a new search foran appointment using the new time as a starting time. Thissame process is repeated if no human resource is availablefor one of the procedure steps (lines 30–37). If the waitingtime exceeds a month, we use the same routine to find anappointment but do not take the patient’s preferred dayinto account (lines 11–12 and lines 22–23). In other words,we will schedule the patient in the earliest time availablein the scheduling horizon. The algorithm returns a patientschedule if a combination of human resource and stationis found for each procedure step and if the waiting time forthe appointment is less than a month.
4.2. The procedure resource assignment (PRA) algorithm
We now turn to the derivation of the PRA algorithm. Wewill now assume that the nuclear medicine department ob-serves a high demand pattern for at least one day of theweek (e.g., Friday is usually the day of the week requestedthe most). The idea behind the algorithm is to assign pro-cedures to resources on days with expected high patientdemand based on ‘representative’ historical demand. Wederive an integer programming (IP) model to perform theprocedure-resource assignment. Two binary variables areuse in this problem, xik
j pt� and wikj�. Variable xik
j pt�=1 if pa-tient j requesting procedure p is scheduled to use resourcei at time-slot t when procedure is started at time � for stepk of the procedure, otherwise xik
j pt�=0. Variable wikj�=1 if
resource i is selected to serve patient j in step k when pro-cedure is started at time �, otherwise wik
j�=0. We now statemodel IP:
IP : Max :∑
p∈P
∑
j∈Jp
∑
i∈S1p
∑
t∈T
∑
�∈Litj
wi1j� (1a)
s.t.∑
p∈P
∑
j∈Jp
∑
k∈Kitj
∑
�∈Litj
xikj pt� ≤ 1, i ∈ I, t ∈ T
(1b)∑
i∈Rkp
∑
t∈T
∑
�∈Litj
wikj� ≤ 1, p ∈ P, j ∈ Jp,
k = 1, . . . , n p (1c)
Dow
nloa
ded
by [
Tex
as A
&M
Uni
vers
ity L
ibra
ries
] at
07:
36 1
0 Se
ptem
ber
2012
Multi-step procedure scheduling 175
Fig. 4. Pseudocode for FR.
∑
i∈Skp
∑
t∈T
∑
�∈Litj
wikj� ≤ 1, p ∈ P, j ∈ Jp,
k = 1, . . . , n p (1d)
xikj pt� − wik
j� = 0, p ∈ P, j ∈ Jp, i ∈ Ikp,
t ∈ T, � ∈ Litj , k = 1, . . . , n p (1e)∑
i∈Rkp
wikj� −
∑
i∈R(k−1)p
wi (k−1)j� = 0, p ∈ P,
j ∈ Jp, t ∈ T, � ∈ Litj , k = 1, . . . , n p (1f)∑
i∈Skp
wikj� −
∑
i∈S(k−1)p
wi (k−1)j� = 0, p ∈ P,
j ∈ Jp, t ∈ T, � ∈ Litj , k = 1, . . . , n p (1g)∑
i∈R1p
wi1j� −
∑
i∈S1p
wi1j� = 0, p ∈ P,
j ∈ Jp, t ∈ T, � ∈ Litj (1h)
Dow
nloa
ded
by [
Tex
as A
&M
Uni
vers
ity L
ibra
ries
] at
07:
36 1
0 Se
ptem
ber
2012

176 Perez et al.
xikj pt�, wik
j� ∈ {0, 1} (1i)
Model IP allocates a subset B ⊆ J of the requests to theresource schedules so that their capacities are not exceeded.Each human resource can only serve one patient at a time.The objective function (1a) maximizes the number of pa-tients scheduled during the day. Variables xik
j pt� and wikj�
are connected through constraint (1a) and together theycontrol patient volume. Constraint (1a) assures that eachresource is assigned to at most one patient each time period.Constraints (1a) and (1a) are used to select the staff andstation for each procedure step, respectively, and also todecide the start-time of the appointment for each patient.Constraint (1a) assures that the same resource is scheduledfor the duration of a particular procedure step. Constraints(1a) and (1a) are used to verify that the staff and stations,respectively, selected to serve a patient follow the proceduresequence. Constraint (1a) is used to match a station to astaff member for each step of the procedure requested bythe patient. Finally, constraints (1a) require each variableto be binary.
IP can be solved by a commercial solver but demandfor the day must be known. Since patients make requestsone-at-a-time, actual systems do not provide the decisionsituation supposed by model IP. Therefore, we implementIP using a forecast of demands and now derive a heuristic toprovide good solutions. The key idea behind the heuristic isto choose a “representative peak day” (RPD) h ∈ H froma given demand trace and solve IP corresponding to thisday. Let F ⊆ H be a subset of days containing the day(s)of the week with the highest weekly demand over the en-tire scheduling horizon (i.e., all Fridays in the schedulinghorizon). An RPD is determined by considering the proce-dure demand at each day h ∈ F . The heuristic selects theday with the highest demand in F and solve model IP forthat day. The solution provides the procedure to resourceassignments. These assignments are used to schedule pa-tients online on those days of the week when high demandis expected.
Let xikj pt� denote the patient procedure-resource assign-
ment solution of model IP. Also, let Gp be an indexset comprising all procedure-resource-time triplets (p,i ,t)∈ P × I × T such that (p, i , t) ∈ Gp for xik
j pt�=1. We nowdefine a function, CheckSchedulePRA() which uses set Gpto search for an appointment. Figure 5 gives a pseudocodefor the function. The CheckSchedulePRA() function gets
Fig. 5. Pseudocode for CheckSchedulePRA().
the information of the procedure p requested by the patientand checks if there is a feasible appointment in set Gp. If anappointment is available, the function returns a schedulefor the patient; otherwise, the function returns the emptyset.
Figure 6 gives a pseudocode for PRA, which employsCheckSchedulePRA(). PRA follows the major steps of FRwith two major differences. First, PRA invokes an addi-tional condition (line 4) that checks if the current day isone of the days where a high demand of requests is ex-pected (day ∈ F). If the condition is satisfied, PRA callsthe CheckSchedulePRA() function to find a feasible ap-pointment for the patient. If the condition is not satisfied,PRA proceeds as FR does. The second major difference be-tween these two algorithms is that PRA does not fix humanresources to any of the stations.
5. Application
To test and validate our methodology we applied it to theScott & White Nuclear Medicine Clinic. The algorithmswere implemented in JAVA and tested using the nuclearmedicine department discrete event specification (DEVS)simulator by Perez et al. (2010). A nuclear medicine clinicat an abstract level contains multiple entities which can beclassified as human resources, stations, radiopharmeceuti-cals, and patients. Figure 7 shows the main components ofthe nuclear medicine DEVS simulator. The experimentalframe (EF) allows the modeler to specify the experimentsthat will be performed using the simulation to answer thequestions of interest. The EF contains the call generator(CGENR), scheduler (SCHED), radiopharmaceutical gen-erator (RPGENR), patient generator (PGENR),and thetransducer (TRANSD) models. The CGENR is in chargeof generating random patient appointment requests. TheSCHED model allows for selecting a scheduling algorithmto schedule patients into the system. Patient appointmentinformation is passed from SCHED to RPGENR andPGENR models. RPGENR generates radiopharmaceuti-cal arrivals to clinic at specified times. PGENR generatespatient arrivals to the clinic at their appointment times.The TRANSD computes the performance measures ofinterest. The NMD model is an abstraction of the nu-clear medicine department (NMD) and contains human re-source models (TECH, NURSE, MANGR, PHYSN) andstation models (STATION). Figure 7 only shows modelsfor TECH, NURSE, MANGR, and one STATION dueto space limitations. The EF provides input to the NMDmodel and after entities are served, the NMD providesinput the EF model. The key assumptions of the DEVSsimulation model include Poisson arrivals for patient ap-pointment calls, which is based on historical data; gener-ation of patient procedures is based on an empirical dis-tribution of the number of different procedures performedin a given year; equipment located inside the stations are
Dow
nloa
ded
by [
Tex
as A
&M
Uni
vers
ity L
ibra
ries
] at
07:
36 1
0 Se
ptem
ber
2012

Multi-step procedure scheduling 177
Fig. 6. Pseudocode for PRA.
not subject to failures; and radiopharmaceuticals arrival ontime.
In the next subsection we describe the configuration ofthis actual nuclear medicine clinic and, in Section 5.2, wepresent our experimental setup. We report computationalresults and findings in Section 5.3.
5.1. Real nuclear medicine setting
The Scott & White Nuclear Medicine Clinic is one ofthe largest, fully accredited nuclear medicine clinics inthe country and is located in Temple, Texas. This nuclear
medicine clinic operates nine hours a day, five days a week,and it is not open during weekends. The clinic has 12 sta-tions, each named according to the type of equipment itcomprises. Table 5.1 lists the names of the stations and theequipment at each station.
The staff comprises technologists, nurses, and a manager.There are eight technologists and two EKG technologists atthis clinic. The technologists have several responsibilities,including drawing doses and acquiring images. The nurseassists the technologists in drawing doses. EKG technol-ogists perform stress exams for cardiac tests at treadmillstations. In the absence of one of the staff members, the
Dow
nloa
ded
by [
Tex
as A
&M
Uni
vers
ity L
ibra
ries
] at
07:
36 1
0 Se
ptem
ber
2012

178 Perez et al.
Fig. 7. The nuclear medicine department model components.
division manager can perform that staff member’s tasks(see Table 1). Table 3 shows the procedures that were per-formed more frequently at the clinic during the year of ourstudy.
5.2. Experimental setup
The clinic configuration used for testing and validating ouralgorithms is based on the stations listed in Table 7 and his-torical patient demand data for one year, which was pro-vided by the clinic. The staff comprises twelve members:Technologist(1), Technologist(2), Technologist(3), Tech-nologist(4), Technologist(5), Technologist(6), Technolo-gist(7), Technologist(8), Technologist(9), Technologist(10),Nurse(1), and Manager(1). From this group Technolo-gist(9) and Technologist(10) are EKG Technologists. A
Table 7. Stations of the Scott & White nuclear medicine clinic
Station name Equipment
Axis(1) Philips Axis CameraAxis(2) Philips Axis CameraAxis(3) Philips Axis CameraP2000(1) Philips PRISM 2000 CameraP2000(2) Philips PRISM 2000 CameraP2000(3) Philips PRISM 3000 CameraMeridian(1) Philips Meridian CameraTreadmill(1) TreadmillTreadmill(2) TreadmillTRT(1) Patient preparationTRT(2) Patient preparationTRT(3) Patient preparation
Poisson process was assumed for procedure request ar-rivals based on historical data. The monthly call interarrivaltimes in minutes followed an exponential distribution withthe following means: January, 6.00; February, 6.25; March6.58; April, 6.67; May, 6.75; June, 6.88; July, 6.96; August,7.04; September, 7.10; October, 7.29; November, 7.34; andDecember, 7.44. Empirical distributions based on histori-cal data were used to generate a procedure request and anappointment preferred day for each patient. Procedure timedurations were based on historical data and modeled usingrandom variables. Monday and Friday were identified asthe days of the week requested the most by patients. Sincepatient interarrival times were based on data estimates, ourexperiments considered the impact of having different de-mand patterns. A sensitivity analysis was performed usingthe base demand scenario described above as a benchmarkfor comparison. We considered an alternative scenario inwhich the monthly mean interarrival times are increased byone minute, and another scenario in which the monthly in-terarrival times are decreased by one minute. We call thesescenarios low demand and high demand, respectively.
We conducted experiments to evaluate the robustness ofour scheduling algorithms. In our computational study, weconsidered only the nuclear medicine procedures listed inTable 2. The performance measures listed in Section 3 wereused to quantify service levels based on both patient andmanagement perspectives. In the FR algorithm Technolo-gist(1) and Technologist(2) are fixed to stations Axis(1) andAxis(2).
The experiments involved 100 replications. Each replica-tion was based on one year of operations. To maintain inde-pendence among replications, different seeds were used inthe pseudo random number generators for each simulation
Dow
nloa
ded
by [
Tex
as A
&M
Uni
vers
ity L
ibra
ries
] at
07:
36 1
0 Se
ptem
ber
2012

Multi-step procedure scheduling 179
500
600
700
800
900
1000
1100
1200
1300
1400
1500
Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec
Pa�e
nts
serv
ed
FR Actual clinic
Fig. 8. Patients served per month: FR versus actual (color figureavailable online).
run. All experiments were executed on a DELL OptiplexGX620 with a Pentium D processor running at 3.2GHzwith 3.0GB RAM.
5.3. Computational results
We now report computational results to evaluate the ro-bustness of both FR and PRA algorithms for three patientdemand scenarios: (a) base patient demand, (b) low patientdemand, and (c) high patient demand. Recall that FR is ascheduling algorithm representing current practice and hasbeen validated (Perez et al., 2010). A comparison of the av-erage number of patients served per month using FR versushistorical values is shown in Fig. 8 for a particular year. Itcan be seen that FR is within 10% of historical values.
5.3.1. Base patient demand scenarioTable 8 shows the throughput and computational timesfor both FR and PRA for the base demand scenario. Wereport the mean, standard deviation (Std.Dev.), and a 95%confidence interval for each performance measure. Resultsshow that FR and PRA obtained similar values for theaverage number of patients served during the year. Thecomputation times (CPU seconds) were about the same forboth algorithms.
Table 8. Number of patients served, system throughput andsimulation time
Patients Patients CPU timeAlgorithm Statistic served served/day (secs)
FR Mean 15924.8 49.8 752.5Std. Dev. 73.00 0.23 29.28CI Lower 15912.7 49.7 747.6CI Upper 15936.9 49.8 757.4
PRA Mean 15941.4 49.8 766.2Std. Dev. 69.15 0.22 26.61CI Lower 15929.9 49.8 761.8CI Upper 15952.9 49.9 770.7
Figure 9 shows two graphs that depict the average num-ber of patients served (throughput) per month for bothalgorithms. The first graph on the left shows a decreasingtrend of the average patient throughput as time progresses.This behavior was validated by comparison with the clinic’srecords, which showed that demand declined over the yearstudied. The graph on the right shows the average differ-ence in the number of patients served per month by PRAand FR each month. This graph reveals that PRA is ableto accommodate more patients early in the year (first threemonths) when patient demand is higher. After the thirdmonth, FR begins to schedule more patients per month,which is simply the demand that was pushed into the fu-ture when resource capacity was reached at the beginningof the year. This observation does not impact the overallnumber of patients served over the year. However, it resultsin patients having to wait longer for their appointments.This phenomenon is discussed later in this section.
Figure 10 shows the percentage utilization of the equip-ment and human resources under both algorithms. Thereis an overall increase of 1% in the utilization of both equip-ment and human resources under PRA. This can be ex-plained by the slight increase in the number of patientsserved under this algorithm. Both algorithms exhibit a lowutilization for the TRT (treatment) stations. These stationsare used mainly for patient preparation, which on average
Fig. 9. Patients served per month under base demand scenario.
Dow
nloa
ded
by [
Tex
as A
&M
Uni
vers
ity L
ibra
ries
] at
07:
36 1
0 Se
ptem
ber
2012

180 Perez et al.
Fig. 10. Resources utilization under base demand scenario.
takes around 10 minutes for most of the procedures. FRprovides a more balanced utilization for camera stations.We can see that PRA schedules more procedures at sta-tions Axis(1) and Axis(2). However, PRA is able to providea more balanced distribution of the tasks for the humanresources. FR gives a higher utilization of Technologist(1)and Technologist(2), the human resources assigned to sta-tions Axis(1) and Axis(2), respectively. Based on the uti-lization of the human resources, we argue that providing amore balanced distribution of the tasks is beneficial for thestaff and that PRA performs better than FR, in that respect.
Next, we report performance measures relative to patientperspective, waiting type 1 and preference ratio. Recall thatpatient waiting type 1 is the time a patient must wait frommaking a request to the appointment time, while preferenceratio is the portion of patients scheduled on their requestedday. Table 9 shows results obtained for the two performancemeasures. PRA showed better performance for both per-formance measures. About 9% improvement is obtainedfor patient waiting time, meaning that a patient would waiton average, about a day less under PRA than under FR.In terms of patient preference ratio, PRA shows a sightimprovement over FR.
Table 9. Patient waiting Type 1 and preference satisfaction ratio
Patient waiting Patient preferenceAlgorithm Statistic type 1 satisfaction ratio
FR Mean 5.3 88.2%Std. Dev. 0.04 0.3%CI Lower 5.3 88.1%CI Upper 5.3 88.2%
PRA Mean 4.8 88.4%Std. Dev. 0.01 0.2%CI Lower 4.8 88.4%CI Upper 4.8 88.4%
5.3.2. Low patient demand scenarioTable 10 shows the results for patient throughput and CPUtime when there is low patient demand. As expected, theoverall number of patients is lower compared to the re-sults obtained for the base patient demand scenario (Table8). Consequently, CPU times are also lower for both al-gorithms and the simulation time for FR is less than thatfor PRA. Both algorithms perform similarly relative to theaverage number of patients served over the entire year.
Figure 11 shows the average number of patients servedper month under each algorithm. Even though the aver-age number of patients served per year is about the samefor both algorithms, PRA accommodates more patients atthe beginning of the year. The results for resource utiliza-tion are reported in Fig. 12. PRA gives a higher utiliza-tion compared to the FR algorithm. This can be attributedto the slight increase in the average number of patientsserved per year. Similar to the results obtained for the basecase scenario, FR provides a more balanced utilization ofequipment while PRA gives a more balanced utilization ofhuman resources.
Table 10. Number of patients served, system throughput andsimulation time
Patients Patients CPU timeAlgorithm Statistic served served/day (secs)
FR Mean 14470.8 45.2 559.3Std. Dev. 61.10 0.19 13.47CI Lower 14460.7 45.2 557.1CI Upper 14481.0 45.3 561.5
PRA Mean 14490.1 45.3 581.6Std. Dev. 57.09 0.18 59.17CI Lower 14480.7 45.3 571.8CI Upper 14499.6 45.3 591.4
Dow
nloa
ded
by [
Tex
as A
&M
Uni
vers
ity L
ibra
ries
] at
07:
36 1
0 Se
ptem
ber
2012

Multi-step procedure scheduling 181
Fig. 11. Patients served per month under low demand scenario.
Table 11. Patient waiting Type 1 and preference satisfaction ratio
Patient waiting Patient preferenceAlgorithm Statistic type 1 satisfaction ratio
FR Mean 4.9 92.4%Std. Dev. 0.02 0.4%CI Lower 4.9 92.3%CI Upper 5.0 92.4%
PRA Mean 4.6 92.6%Std. Dev. 0.01 0.5%CI Lower 4.6 92.6%CI Upper 4.6 92.7%
Table 11 show the results relative to patient perspectiveperformance measures. PRA results in a lower average pa-tient waiting time. As for patient preference ratio, the resultsshow that, when lower patient demand is observed at theclinic, both algorithms provide better ratios. This is dueto the fact that, since fewer requests are managed by the
Table 12. Number of patients served, system throughput andsimulation time
Patients Patients CPU timeAlgorithm Statistic served served/day (secs)
FR Mean 16929.8 52.9 744.9Std. Dev. 83.26 0.26 47.15CI Lower 16916.0 52.9 737.1CI Upper 16943.7 52.9 752.8
PRA Mean 17069.2 53.3 861.8Std. Dev. 80.25 0.25 78.88CI Lower 17055.9 53.3 848.7CI Upper 17082.5 53.4 874.9
clinic, there is more flexibility in scheduling patients basedon their preferences.
5.3.3. High patient demand scenarioTable 12 shows patient throughput and CPU times for thehigh patient demand scenario. PRA shows a 1% increase
Fig. 12. Resource utilization under low demand scenario.
Dow
nloa
ded
by [
Tex
as A
&M
Uni
vers
ity L
ibra
ries
] at
07:
36 1
0 Se
ptem
ber
2012

182 Perez et al.
Fig. 13. Patients served per month under high demand scenario.
in the average number of patients served over the year andhas a slightly higher average CPU time. The higher CPUtime can be attributed to the algorithm scheduling andmore patients. Figure 13 reports the average number of pa-tients served per month under each algorithm. Both graphsshow that PRA schedules more patients each month. Ob-serve that, as expected, the number of patients served eachmonth under either algorithm is higher compared to thelow demand and base case scenarios.
Figure 14 shows the results for resource utilization. PRAobtained a 3% higher overall utilization of the resourcescompared to FR. Again, PRA is able to provide a morebalanced utilization of the human resources, especially thetechnologists. In terms of patient perspective performancemeasures, PRA shows better performance. Its patient wait-ing time is about 16% lower, meaning that patients wouldwait about two days less on average compared to the FRalgorithm. As for the patient preference ratio, PRA sched-ules patients on their requested preferred day about 52% ofthe time, which is an improvement of about 48% over theFR algorithm.
Table 13. Patient waiting Type 1 and preference satisfaction ratio
Patient waiting Patient preferenceAlgorithm Statistic Type 1 satisfaction ratio
FR Mean 9.5 35.9%Std. Dev. 0.40 6.0%CI Lower 9.4 34.9%CI Upper 9.5 36.9%
PRA Mean 7.9 52.2%Std. Dev. 0.42 7.9%CI Lower 7.9 50.9%CI Upper 8.0 53.6%
6. Discussion and conclusions
Managing patients in nuclear medicine departments is achallenging problem with limited research reported in theliterature. The complexity involved in this health care set-ting makes this problem unique. In this paper, we de-rive and implement two algorithms for scheduling nuclearmedicine patients and resources. The fixed resource (FR)
Fig. 14. Resources utilization under high demand scenario.
Dow
nloa
ded
by [
Tex
as A
&M
Uni
vers
ity L
ibra
ries
] at
07:
36 1
0 Se
ptem
ber
2012

Multi-Step Procedures Scheduling 183
algorithm is based on the experience of the last two au-thors of this paper and is used as a benchmark against thesecond algorithm named procedure resource assignment(PRA). Both scheduling algorithms take into account thetime constraints imposed by the decay of the radiophar-maceuticals, which are required for most nuclear medicineprocedures. The algorithms were implemented within a sim-ulation framework and experiments are based on historicaldata for an actual clinic.
We report computational results that provide useful in-sights to improve patient service management in nuclearmedicine. We find that the PRA algorithm, which assignsprocedures to resources on those days of the week requestedthe most by the patients, provides better performance formost of the system performance measures under consid-eration. For example, the PRA algorithm provides a morebalanced utilization of human resources, independent ofthe demand. The algorithm is also able to increase thenumber of patients served at the clinic under higher pa-tient demand. In terms of patient perspective performancemeasures, the algorithm is able to provide appointmentswith less waiting time for the patient. For example, underthe high patient demand experiments we observed that pa-tients wait two days less using the PRA algorithm. Thereis some operational differences between FR and PRA interms of how staff do their work. For example, the FR cre-ates task specialization for some of the staff, that is, thosethat are assigned to stations with fixed procedures. Thisspecialization may imply task efficiency for the staff andpatient safety. However, even under PRA with no task spe-cialization, we expect task efficiency and patient safety dueto the fact that the nuclear medicine staff are well-trainedprofessionals.
While this work focuses on nuclear medicine, results canbe easily adopted in other health care settings. For exam-ple, the FR and PRA algorithms can be easily modified toschedule patients and resources in diagnostic clinics thatperform one-step procedures such as MRI and CT scanclinics. Removing the multi-step condition of the nuclearmedicine procedures would simplify the IP model as wellas the algorithms. Also, no other clinics require radiophar-maceuticals, simplifying scheduling even further, since thelead time required to obtain radiopharmaceuticals is nolonger to be considered. Further research along this line ofwork could include extending FR and PRA algorithms tothe stochastic (online) optimization setting in which data,such as stochastic patient arrivals, equipment failures, anddelayed radiopharmaceutical deliveries, are treated explic-itly as stochastic, and where we can estimate costs such asovertime.
Acknowledgments
We are grateful to Mr. Wayne Stockburger (Scott and WhiteHospital) for his interest in this work and for providing ac-
cess to the historical data for validating the models andalgorithms. We also thank the anonymous referees whoprovided valuable comments that helped improve the pre-sentation of this paper.
References
Cayirli, T. and Veral, E. (2003) Outpatient scheduling in health care: Areview of literature. Production and Operations Management, 12(4),519–549.
Cayirli, T., Veral, E. and Rosen, H. (2006) Designing appointmentscheduling systems for ambulatory care services. Health Care Man-agement Science, 9(1), 47–58.
Centeno, M., Albacete, C., Terzano, D., Carrillo, M. and Ogazon, T.(2000) A simulation study of the radiology department at JMH, inProceedings of the 2000 Winter Simulation Conference, Joines, J.A.and Barton, R.R., (eds.), IEEE, pp. 1978–1984.
Conforti, D., Guerriero, F. and Guido, R. (2007) Optimization modelsfor radiotherapy patient scheduling. 4OR: A Quarterly Journal ofOperations Research, 6(3), 263–278.
Denton, B. and Gupta, D. (2003) A sequential bounding approach foroptimal appointment scheduling. IIE Transactions, 35(11), 1003–1016.
Denton, B., Rahman, A., Nelson, H. and Bailey, A. (2006) Simulationof a multiple operating room surgical suite, in Proceedings of the 2006Winter Simulation Conference, Perrone, L.F., Wieland, F.P., Liu, J.,Lawson, B.G., Nicol, D.M., and Fujimoto, R.M., (eds.), IEEE, pp.414–424.
Green, L., Savin, S. and Wang, B. (2006) Managing patient service in adiagnostic medical facility. Operations Research, 54(1), 11–25.
Gupta, D. and Denton, B. (2008) Appointment scheduling in healthcare: Challenges and opportunities. IIE Transactions, 40(9), 800–819.
Gupta, D. and Wang, L. (2008) Revenue management for a primary-careclinic in the presence of patient choice. Operations Research, 56(3),576–592.
Ho, C. and Lau, H. (1992) Minimizing total cost in scheduling outpatientappointments. Management Science, 38(12), 1750–1764.
Ho, C., Lau, H. and Li, J. (1995) Introducing variable-interval appoint-ment scheduling rules in service systems. International Journal ofOperations & Production Management, 15(6), 59–68.
Klassen, K. and Rohleder, T. (1996) Scheduling outpatient appointmentsin a dynamic environment. Journal of Operations Management, 14(2),83–101.
Liu, L. and Liu, X. (1998a) Block appointment systems for outpatientclinics with multiple doctors. Journal of the Operational ResearchSociety, 49(12), 1254–1259.
Liu, L. and Liu, X. (1998b) Dynamic and static job allocation for multi-server systems. IIE Transactions, 30(9), 845–854.
Mettler, F., Bhargavan, M., Thomadsen, B., Gilley, D., Lipoti, J., Ma-hesh, M., McCrohan, J. and Yoshizumi, T. (2008) Nuclear medicineexposure in the United States, 2005–2007: preliminary results, in Sem-inars in Nuclear Medicine, Freeman, L.M. and Blaufox, M.D., (eds.),W.B. Saunders, Philadelphia, PA, pp. 384–391.
O’Kane, P. (1981) A simulation model of a diagnostic radiology depart-ment. European Journal of Operational Research, 6(1), 38–45.
Patrick, J. and Puterman, M. (2007) Improving resource utilization fordiagnostic services through flexible inpatient scheduling: A method forimproving resource utilization. Journal of the Operational ResearchSociety, 58(2), 235–245.
Perez, E., Ntaimo, L., Bailey, C. and McCormack, P. (2010) Modelingand simulation of nuclear medicine patient service management inDEVS. Simulation, 86(8–9), 481–501.
Dow
nloa
ded
by [
Tex
as A
&M
Uni
vers
ity L
ibra
ries
] at
07:
36 1
0 Se
ptem
ber
2012

184 Perez et al.
Podgorelec, V. and Kokol, P. (1997) Genetic algorithm based system forpatient scheduling in highly constrained situations. Journal of MedicalSystems, 21(6), 417–427.
Ramakrishnan, S., Nagarkar, K., DeGennaro, M., Srihari, M., Court-ney, A. and Emick, F. (2004) A study of the CT scan area of ahealthcare provider, in Proceedings of the 2004 Winter SimulationConference, Ingalls, R.G. and Rossetti, M.D., (eds.), IEEE, Washing-ton, DC, pp. 2025–2031.
Robinson, L. and Chen, R. (2003) Scheduling doctors’ appointments:Optimal and empirically-based heuristic policies. IIE Transactions,35(3), 295–307.
Rohleder, T. and Klassen, K. (2000) Using client-variance informationto improve dynamic appointment scheduling performance. Omega,28(3), 293–302.
Rohleder, T. and Klassen, K. (2002) Rolling horizon appointmentscheduling: A simulation study. Health Care Management Science,5(3), 201–209.
Vermeulen, I., Bohte, S., Elkhuizen, S., Lameris, H., Bakker, P. andLa Poutre, H. (2009) Adaptive resource allocation for efficientpatient scheduling. Artificial Intelligence in Medicine, 46(1), 67–80.
Wang, P. (1993). Static and dynamic scheduling of customer arrivals toa single-server system. Naval Research Logistics, 40(3), 345–360.
Wang, P. (1997) Optimally scheduling N customer arrival times for asingle-server system. Computers & Operations Research, 24(8), 703–716.
Zhang, J. (2007, January 9) Growth in U.S. health-care spending slowsagain. The Wall Street Journal, A2.
Dow
nloa
ded
by [
Tex
as A
&M
Uni
vers
ity L
ibra
ries
] at
07:
36 1
0 Se
ptem
ber
2012


















