Pathophysiology of polytrauma · Pathophysiology of polytrauma Marius Keel*, Otmar Trentz ......
19
REVIEW Pathophysiology of polytrauma Marius Keel * , Otmar Trentz Division of Trauma Surgery, University Hospital Zurich, Raemistrasse 100, CH-8091 Zurich, Switzerland Accepted 14 December 2004 Contents Introduction ................................................................ 692 Two-hit theory .............................................................. 693 Hyperinflammation–—SIRS ....................................................... 694 Injury, Int. J. Care Injured (2005) 36, 691—709 www.elsevier.com/locate/injury KEYWORDS Trauma; Injury; Pathophysiology; Host defence response; Systemic inflammatory response syndrome (SIRS); Compensatory anti- inflammatory response syndrome (CARS); Apoptosis; Necrosis; Multiple organ dysfunction syndrome (MODS); Multiple organ failure (MOF); Damage control; Mortality Summary Immediate and early trauma deaths are determined by primary brain injuries, or significant blood loss (haemorrhagic shock), while late mortality is caused by secondary brain injuries and host defence failure. First hits (hypoxia, hypotension, organ and soft tissue injuries, fractures), as well as second hits (e.g. ischaemia/ reperfusion injuries, compartment syndromes, operative interventions, infections), induce a host defence response. This is characterized by local and systemic release of pro-inflammatory cytokines, arachidonic acid metabolites, proteins of the contact phase and coagulation systems, complement factors and acute phase proteins, as well as hormonal mediators: it is defined as systemic inflammatory response syndrome (SIRS), according to clinical parameters. However, in parallel, anti-inflammatory mediators are produced (compensatory anti-inflammatory response syndrome (CARS). An imbalance of these dual immune responses seems to be responsible for organ dysfunction and increased susceptibility to infections. Endothelial cell damage, accumulation of leukocytes, disseminated intravascular coagulation (DIC) and microcirculatory disturbances lead finally to apoptosis and necrosis of parenchymal cells, with the development of multiple organ dysfunction syndrome (MODS), or multiple organ failure (MOF). Whereas most clinical trials with anti-inflammatory, anti-coagulant, or antioxidant strategies failed, the implementa- tion of pre- and in-hospital trauma protocols and the principle of damage control procedures have reduced post-traumatic complications. However, the development of immunomonitoring will help in the selection of patients at risk of post-traumatic complications and, thereby, the choice of the most appropriate treatment protocols for severely injured patients. # 2005 Elsevier Ltd. All rights reserved. * Corresponding author. Tel.: +41 1 255 3657; fax: +41 1 255 4406. E-mail address: [email protected] (M. Keel). 0020–1383/$ — see front matter # 2005 Elsevier Ltd. All rights reserved. doi:10.1016/j.injury.2004.12.037
Transcript of Pathophysiology of polytrauma · Pathophysiology of polytrauma Marius Keel*, Otmar Trentz ......

Injury, Int. J. Care Injured (2005) 36, 691—709
www.elsevier.com/locate/injury
REVIEW
Pathophysiology of polytrauma
Marius Keel *, Otmar Trentz
Division of Trauma Surgery, University Hospital Zurich, Raemistrasse 100, CH-8091 Zurich, Switzerland
Accepted 14 December 2004
KEYWORDSTrauma;Injury;Pathophysiology;Host defence response;Systemic inflammatory
response syndrome(SIRS);
Compensatory anti-inflammatoryresponse syndrome(CARS);
Apoptosis;Necrosis;Multiple organ
dysfunctionsyndrome (MODS);
Multiple organ failure(MOF);
Damage control;Mortality
Summary Immediate and early trauma deaths are determined by primary braininjuries, or significant blood loss (haemorrhagic shock), while late mortality is causedby secondary brain injuries and host defence failure. First hits (hypoxia, hypotension,organ and soft tissue injuries, fractures), as well as second hits (e.g. ischaemia/reperfusion injuries, compartment syndromes, operative interventions, infections),induce a host defence response. This is characterized by local and systemic release ofpro-inflammatory cytokines, arachidonic acid metabolites, proteins of the contactphase and coagulation systems, complement factors and acute phase proteins, as wellas hormonal mediators: it is defined as systemic inflammatory response syndrome(SIRS), according to clinical parameters. However, in parallel, anti-inflammatorymediators are produced (compensatory anti-inflammatory response syndrome(CARS). An imbalance of these dual immune responses seems to be responsible fororgan dysfunction and increased susceptibility to infections.
Endothelial cell damage, accumulation of leukocytes, disseminated intravascularcoagulation (DIC) and microcirculatory disturbances lead finally to apoptosis andnecrosis of parenchymal cells, with the development of multiple organ dysfunctionsyndrome (MODS), or multiple organ failure (MOF). Whereas most clinical trials withanti-inflammatory, anti-coagulant, or antioxidant strategies failed, the implementa-tion of pre- and in-hospital trauma protocols and the principle of damage controlprocedures have reduced post-traumatic complications. However, the developmentof immunomonitoring will help in the selection of patients at risk of post-traumaticcomplications and, thereby, the choice of the most appropriate treatment protocolsfor severely injured patients.# 2005 Elsevier Ltd. All rights reserved.
Contents
Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 692Two-hit theory . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 693Hyperinflammation–—SIRS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 694
* Corresponding author. Tel.: +41 1 255 3657; fax: +41 1 255 4406.E-mail address: [email protected] (M. Keel).
0020–1383/$ — see front matter # 2005 Elsevier Ltd. All rights reserved.doi:10.1016/j.injury.2004.12.037

692 M. Keel, O. Trentz
Hypoinflammation–—CARS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 695Activation of plasmatic cascade system . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 696Acute phase reaction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 697Leukocyte recruitment . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 698Proteases, oxidative stress and capillary leakage . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 698Microcirculatory disturbances . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 699Ischaemia/reperfusion injury . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 699Neuroendocrine reaction and metabolic alterations . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 700Multiple organ dysfunctions or failure . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 701Therapeutic strategies for multiply injured patients . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 702References. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 703
Table 1 Clinical parameters of systemic inflammatoryresponse syndrome (SIRS)
1. Heart rate > 90/min2. Breathing rate > 20/min, respectively,
hyperventilation with decrease of thearterial CO2 partial pressure (PaCO2)under 32 mmHg
3. Temperature > 38 8C or < 36 8C4. Number of leukocytes > 12,000/mm3
or < 4000/mm3 or � 10% juvenileneutrophil granulocytes
For the definition of SIRS, two or more parameters must befulfiled. Sepsis is defined as SIRS with detection of bacteremiaor bacterial focus.6
Introduction
Despite improved traffic and occupational safety,as well as significant advances in pre- and in-hospital management, severe trauma representsthe most frequent cause of death in people belowthe age of 40 years.4,38,60,128,149,168 Immediate andearly trauma deaths are determined by severeprimary brain injuries, or significant blood loss(haemorrhagic shock) after blunt, or penetrating,trauma.4,38,60,70,128,149,158,168,173,181,194 Late mor-tality is caused by secondary brain injuries andhost defence failure.4,70,158,168,173,194 Direct, orindirect, mechanical forces induce organ and softtissue injuries, or fractures. However, these firsthits represent a greater challenge, as local tissuedamage, such as contusions or lacerations, hypoxiaand hypotension, induce further local and systemichost responses, to preserve the immune integrityand stimulate reparative mechanisms.164 This sys-temic inflammation was defined in 1991, throughthe consensus conference of the American Collegeof Chest Physicians/Society of Critical Care Med-icine (ACCP/SCCM), as systemic inflammatoryresponse syndrome (SIRS).6 At least two of thefour clinical parameters (Table 1) must be fulfiledfor the diagnosis of SIRS.6 It is characterized by thelocal and systemic production and release of dif-ferent mediators, such as pro-inflammatory cyto-kines, complement factors, proteins of the contactphase and coagulation systems, acute phase pro-teins, neuroendocrine mediators and an accumu-lation of immunocompetent cells at the local siteof tissue damage (Fig. 1).17,18,40,91,163,169,195 Inaddition, this systemic inflammation is augmentedby second hits, such as ischaemia/reperfusioninjuries, surgical interventions or infections(two-hit theory).163,164
However, different clinical trials and animalmodels have shown that, in parallel with avoidthe autodestructive effects of immunocompetentcells (Fig. 1).19,88,91,120,195 An imbalance betweenthese dual immune responses, with an overwhelm-
ing release of pro- or anti-inflammatory mediators,seems to be responsible for organ dysfunctionand increased susceptibility to infections andsepsis.19,116,118,155 Endothelial cell damage, accu-mulation of leukocytes, disseminated intravascularcoagulation (DIC) and microcirculatory dysfunctionfinally lead to programmed cell death (apoptosis)and necrosis of parenchymal cells (microenviron-ment theory) with the development of multipleorgan dysfunction syndrome (MODS) or multipleorgan failure (MOF).67,91,92,95,107,117,153,159,195 Inaccordance with these pathophysiological mechan-isms and definition of SIRS, the term polytraumacan be defined as a syndrome of combinedinjuries with an injury severity score (ISS) > 17and consequent SIRS for at least 1 day, leading todysfunction, or failure, of remote organs and vitalsystems, which themselves had not directly beeninjured.76,193
This review is planned to give an insight into thetriggers and the mechanisms of the post-traumatic‘‘cardiovascular shock, homeostasis, apoptosis,organ dysfunctions and immune suppression’’(CHAOS) as coined by Bone.19 In addition, it shouldelucidate the pathophysiological basis for thedamage control concept in the surgical manage-ment of multiple injured patients, reasons for the

Pathophysiology of polytrauma 693
Figure 1 Host defence response after trauma. See text for details and explanations. APC: antigen presenting cells. TH,T-helper cells (lymphocytes); SIRS, systemic inflammatory response syndrome; CARS, compensatory anti-inflammatoryresponse syndrome; PMNL, polymorphonuclear leukocytes; MODS, multiple organ dysfunction syndrome; MOF, multipleorgan failure.
failure of clinical trials with immunotherapies inthe past two decades and the significance forthe development of post-traumatic immunomoni-toring.
Two-hit theory
The complex cascade of the host defence response isstimulated by primary and secondary insults (two-hit theory).163,164 The trauma impact determinesprimary organ, or soft tissue, injuries and fractures(first hit; trauma load) with local tissue damage aswell as an activation of the systemic inflammatoryresponse.118,135,163,164,179 In addition, secondaryendogenous and exogenous factors play a crucialrole in the initiation and severity of post-traumaticcomplications.164,179,202 Typical endogenous (anti-genic load) second hits are respiratory distress withhypoxia, repeated cardiovascular instability, meta-bolic acidosis, ischaemia/reperfusion injuries, deadtissue, contaminated catheters, or tubes, and infec-tions.46,50 Surgical interventions with severe tissuedamage, hypothermia or blood loss, inadequate, ordelayed, surgical, or intensive care, after neglectedor missed injuries, as well as massive transfusions,represent exogenous second hits (interventionalload or surgical load).46,81,202
The severity of organ injuries, varying from con-tusions to complete lacerations, and the remainingorgan perfusion influence the post-traumatic sys-temic inflammatory response. The highest incidencefor the development of SIRS can be observed afterisolated or combined severe head injuries.55,155
Primary focal or diffuse and secondary braindamages including ischemia/reperfusion injuries,cerebral oedema or intracranial hypertension deter-mine the cerebral outcome and themortality as wellas the incidence and severity of post-traumaticcomplications.169,176,181 Although the central ner-vous system has been defined historically as an‘‘immunologically privileged organ’’, due to itsseparation from the peripheral circulation by theblood—brain barrier (BBB), different studies haveshown that the brain acts as a target and as aneffector organ.87,104,169 Glial cells, astrocytesand neurons are potent producers of pro- andanti-inflammatory mediators and their receptors,leading to local tissue damage and a systemicresponse.104,132,169 In addition, systemic mediatorsreleased by peripheral immune, endothelial, or par-enchymal cells influence the integrity of the BBB,leading to a bi-directional communication of theinflammatory mediators.104,132,169 Primary epiduralhematoma, or cerebral oedema, as well as post-traumatic secondary oedema, induced by local and

694 M. Keel, O. Trentz
systemic inflammatory processes, are responsiblefor the development of a cerebral compartmentsyndrome, which is lethal without intervention.173
Thoracic injuries, with multiple rib fractures,lung contusions, or lacerations, are often compli-cated by local and systemic inflammation, with orwithout manifestation of pneumonia, acute lunginjury (ALI), or acute respiratory distress syndrome(ARDS).9,120,137 Injuries of intra-abdominal organscause haemorrhagic shock (liver, spleen, vascularinjuries) and aseptic, or septic, peritonitis (pancrea-tic or hollow organ injuries).11 Severe intra-abdom-inal or retroperitoneal haemorrhage, after vascular,renal, or pelvic injuries, as well as systemic inflam-matory processes in septic patients, can lead to anabdominal compartment syndrome with systemiccomplications.59,125
Soft tissue injuries of the extremities, espe-cially in patients with haemorrhagic shock, areoften complicated by decreased perfusion (low-flow hypoxia), with a high risk for ischaemia/reperfusion injuries and secondary infections.Furthermore, severe muscle crushing injuries pre-dispose to a compartment syndrome with musclenecrosis, rhabdomyolysis and finally acute renalfailure (crush kidney).159 Fractures of the femur,multiple long bone fractures and unstable pelvicring fractures are characterized by a high bloodloss and contribute to the inflammatory acti-vity.22,49,53 Additionally, fat embolism syndromeis an infrequent clinical consequence with thetypical triad of pulmonary distress, mentalchanges and petechial rash, 24—48 h after pelvicor long-bone fractures.148
The incidence of septic complications hasincreased during the last decade.122 Closed woundswith large soft tissue damage and open wounds,or fractures, as well as neglected soft tissueinjuries, represent portal of entry for microorgan-isms.205,210 Central venous catheters, intratra-cheal tubes, chest tubes and bladder cathetersare often contaminated and raise the infection riskin severely injured patients.32 The most commonreasons for sepsis after trauma are hospitalacquired pneumonia, catheter infections, intra-abdominal and wound infections.9,140,179 Further-more, ischaemic lesions of the gastrointestinaltract after haemorrhagic shock seem to be respon-sible for bacterial translocation into the circulation(gut hypothesis).103,130
Hyperinflammation–—SIRS
Tissue damage induces in commensurate with theseverity of trauma (trauma load), genetic factors
(gene polymorphism), the general condition of thehost and the type of antigens (antigenic load), bothlocal and systemic release of pro-inflammatorycytokines and phospholipids.40,88,143,171,190 Poly-morphonuclear leukocytes (PMNL), monocytes, tis-sue macrophages (e.g. alveolar macrophages),lymphocytes, natural killer cells, and parenchymalcells are involved in a complex network of this hostdefence response.195 An overwhelming pro-inflam-matory response (hyperinflammation) leads to theclinical manifestation of SIRS and finally to hostdefence failure (MODS, MOF).55,71,135,195
Cytokines are polypeptides and act in a para- orautocrine manner.40 They are capable of exertingmany effects on an array of cell types (pleiotropy).40
Besides hyperacute pro-inflammatory cytokines,such as tumor necrosis factor-a (TNF-a), or inter-leukin-1b (IL-1b), with an effect after 1—2 h, thereexist subacute (secondary) cytokines such as IL-6,IL-8 (neutrophil activating peptide (NAF)), macro-phage migratory factor (MMF), high motility groupprotein -1 (HMG-1), as well as IL-12 and IL-18,two interferon-g (IFN-g)-modulating cytokines(Fig. 1).40,71 Increased TNF-a, IL-1b or IL-8 serumlevels are observed in patients with systemic inflam-mation, as well as in bronchoalveolar lavage fluids ofpatients with thoracic trauma, or acute respiratorydistress syndrome.42,43,100,121,187 In addition, IL-6serum levels correlate with the ISS, the incidenceof MODS, ARDS, or sepsis and with outcome.15,121,166
Through the influence of antigens, T-helper lym-phocytes (TH cells, CD4
+ cells) differentiate into twophenotypes, the TH1 and TH2 lymphocytes.146 TH1cells support the pro-inflammatory cascade throughsecretion of IL-2, interferon-g and TNF-b, whereasTH2 cells are important producers of anti-inflam-matory mediators. Monocytes/macrophages areinvolved in the differentiation of TH1 cells, viathe secretion of IL-12. Depressed IL-12 productionafter trauma correlated with a shift of the TH1/TH2ratio towards the TH2-type pattern, with an adverseclinical outcome.146
Pro-inflammatory cytokines activate the recruit-ment and phagocytosis activity of PMNL (priming),the immune cells of the first hours (the first defenceline), and stimulate PMNL to release proteases andfree oxygen radicals (respiratory burst, oxidativestress) (Fig. 1).21 Furthermore, PMNL are influencedby colony-stimulating factors, such as granulocyte-colony stimulating factor (G-CSF) and granulocytemacrophage-colony stimulating factor (GM-CSF).20,31,51,189 They enhance monocyte- or granu-locytopoiesis, on the one hand and reduce thespontaneous programmed cell death (apoptosis) ofPMNL during SIRS or sepsis, on the other hand.20,31,51
Other pro-inflammatory mediators contribute addi-

Pathophysiology of polytrauma 695
tionally to the reduction of neutrophil apoptosis,with an accumulation of PMNL at the site of localtissue damage.16,47,54,78,97,102,109,124
Mechanical and hypoxic cellular damage leadsfurther to an increase of intracellular Ca++ levelswith an activation of phospholipase A2 (PLA2) andphospholipase C (PLC).163 These enzymes catalysethe release of arachidonic acids from membranephospholipids. Through the activation of cyclooxy-genase and 5-lipooxygenase prostaglandine E2(PGE2) leucotriene B4 (LTB4) and thromboxane A2(TXA2), respectively, are produced (Fig. 1).165 Thesemetabolites are involved in the recruitment ofinflammatory cells, regulation of vascular perme-ability and motility, as well as the aggregation ofthrombocytes.163 Additionally, PLA2 induces therelease of the platelet activating factor (PAF).212
It supports the activation of macrophages, theirinteraction with endothelial cells and the activationand aggregation of thrombocytes.212
Hypoinflammation–—CARS
Depending on the severity of injury and the post-traumatic course, anti-inflammatory mediators arealso produced. TH2-cells and monocytes/macro-phages release IL-4, IL-10, IL-13, or transforminggrowth factor-b (TGF-b) (Fig. 1).30,33,57 In addition,different cytokines (e.g. IL-6) have shown a dualeffect with pro- and anti-inflammatory activities.The serum levels of IL-10 correlate with ISS and post-traumatic complications, such as MODS, ARDS, orsepsis.88,138 In addition, natural inhibitors of recep-tors, such as soluble TNF-receptors (TNF-RI (55 kD)and TNF-RII (75 kD)), or IL-1 receptor antagonist(IL-1ra) are detectable in the sera of injuredpatients, correlating also with the ISS and the inci-dence of post-traumatic complications.52,88,99
Furthermore, the readiness of blood monocytesfrom injured patients to release pro-inflammatorycytokines was decreased in in vitro studiesafter stimulation with Gram-negative (endotoxin,lipopolysaccharide (LPS)), or Gram-positive (e.g.peptidoglycan, lipoteichonic acid), bacterial pro-ducts and correlated with the post-traumaticcourse.25,56,84,85,101,203 The mechanisms of this‘‘endotoxin tolerance’’ are still incompletelyunderstood.203 It seems that anti-inflammatorymediators, like IL-10, depress the activity of intra-cellular transcription factors, such as nuclearfactor-kappa B (NF-kB), which are essential forthe synthesis of pro-inflammatory cyto-kines.24,69,84,101,116,197,198,203 The expression ofthe LPS-receptor CD14 on monocytes is decreasedafter trauma, combined with an increase of the
soluble CD14 (sCD14), through shedding of the mem-brane-bound CD14.203 However, the decreasedexpression of CD14, as well as expression altera-tions of the pattern-recognition receptors for bac-terial products, the toll-like receptors, seem not tobe responsible for ‘‘endotoxin tolerance’’.83 Bycontrast, the expressions of the toll-like receptorsfor Gram-positive (TLR2) and Gram-negative (TLR4)bacterial products are increased on monocytes,or PMNL, during systemic inflammation.80 Further-more, antigen-presenting cells (APC), such asmonocytes/macrophages, showed a depressedexpression of the MHC (major histocompatibilitycomplex) class II molecule HLA-DR (human leuko-cyte antigen) that correlated with post-traumaticinfections.71
During the early phase of the post-traumaticcourse, a lymphocytopaenia has been observ-ed.22,92,111,195 This lymphocyte depletion was asso-ciated with morbidity and outcome after trauma.195
It may be related to increased apoptosis, triggeredby stress hormones (steroids) and cell death pro-teins.39,111,117,145,153 Apoptosis is characterizedmorphologically by cell shrinking, with cytoplas-matic condensation (apoptotic bodies), nuclear con-densation (pycnosis) and DNA-fragmentation (DNAladdering).134,153 The cell membranes stay primarilyintact and no surrounding inflammatory signs can beobserved, in contrast to necrosis.153
Typical cell death proteins are TNF-a or Fas ligand(CD95 ligand).5,134 They induce cell death afterbinding with their receptors, respectively, TNF-RIand Fas antigen (CD95 antigen) and activationof complex intracellular cascades and effectorenzymes, such as intracellular proteases (e.g.calpains, caspases).5,39,75,111,134,156 The cellularexpressionsofTNF-RI andFasantigen,or their solublemolecules, were elevated in serum from injuredpatients, postoperatively or during sepsis.37,145
An overwhelming anti-inflammatory response(hypoinflammation) seems to be responsible forpost-traumatic immunosuppression, with a highsusceptibility to infections and septic complica-tions.19,171,195 This immunological status is calledcompensatory anti-inflammatory response syn-drome.19 However, it does not look like a compen-satory mechanism in a biphasic model; as only a fewhours after trauma anti-inflammatory mediators(e.g. IL-10) were detectable in the serum of injuredpatients.138 It seems that the host defence responsetries to strike a fine balance between SIRS and CARS,to induce reparative mechanisms and limit entryor overload of microorganisms, on the one hand, andto avoid autoaggressive inflammation, with second-ary tissue damage and susceptibility to infections,on the other hand. These mixed inflammatory

696 M. Keel, O. Trentz
Figure 2 Plasmatic cascade system. Proinflammatory mediators and toxins stimulate the plasmatic cascade systemwith activtion of complement factors, kallikrein—kinin system and coagulation cascade. These mechanisms play a crucialrole in endothelial and parenchymal cell death as well in the disseminated intravascular coagulation (DIC). See text fordetails and explanations.
mechanisms are called mixed antagonistic responsesyndrome (MARS).19
Activation of plasmatic cascade system
Pro-inflammatory mediators (cytokines, arachidonicacid metabolites) and toxins activate the plasmaticcascade system, consisting of the complement cas-cade, the kallikrein—kinin system and the coagula-tion cascade (Fig. 2). The classical pathway ofcomplement activation is induced by antigen—anti-body complexes (immunoglobulins M or G (IgM,IgG)), or activated coagulation factor XII (FXIIa),whereas bacterial products (e.g. LPS) activate thealternative pathway (Fig. 2).66,129,182 Cleavages ofC3, by C3 convertase, and C5, by C5 convertase,lead to the formation of opsonins, anaphylatoxinsand, finally, the membrane attack complex(MAC).66,129,182 The opsonins C3b and C4b areinvolved in the phagocytosis of cell detritus, andespecially bacteria, by covalent binding of pathogensurfaces (opsonization).66,129 The anaphylatoxinsC3a and C5a support different inflammatorymechanisms, the recruitment (chemotaxis) andactivation of phagocytic cells (PMNL, monocytes,macrophages), the enhancement of the hepaticacute phase response, the degranulation of mastcells and basophils, with release of vasoactive med-
iators, such as histamine, as well as the adhesionof leukocytes to endothelial cells, leading toincreased vascular permeability with oedema.129,169
In addition, apoptosis and cell lysis (necrosis) ofparenchymal cells, or bacteria, are induced byC5a, through the C5a receptor (C5aR) and theMAC (C5b-9) .129,169,182 In clinical studies, elevatedserum levels of different complement components,or their expression in injured tissue, were observedafter trauma, or during sepsis.42,86,165,169,182,211
Similarly to some cytokines, C3a and C5a showeddual effects with activation of reparative mechan-isms too.129 Furthermore, during systemic inflam-mation, serum levels of the C1-inhibitor, producedby hepatocytes, endothelial cells, monocytes andmacrophages, were decreased through a degrada-tion by PMNL-elastases. C1-inhibitor regulates theclassical complement pathway through inactivationof the active subunits C1s and C1r.129
The plasma proteins FXII, prekallikrein, kinino-gen and the factor XI (FXI) represent the contactphase system (Fig. 2).185 They are characterized bythe fact, that they can be activated by negatively-charged cellular surfaces (contact activation).185
FXII and prekallikrein activate mutually and formFXIIa and kallikrein. FXIIa stimulates the com-plement cascade along the classical pathway.185
Kallikrein induces the fibrinolysis through conver-sion of plasminogen to plasmin, or activation of
Pathophysiology of polytrauma 697
the urokinase-like plasminogen activator (u-PA)(Fig. 2). The tissue-plasminogen activator (t-PA)works as a cofactor, whereas natural inhibitors ofthe fibrinolytic system are a2-antiplasmin (a2AP),a2-macroglobulin (a2MG) and the plasminogen-activator-inhibitor 1 (PAI-1). In addition, kallikreinstimulates the formation of bradykinin fromkininogen. Kinins are vasodilators, increase thevascular permeability and inhibit the functionsof thrombocytes.185
The intrinsic coagulation system is linked to thecontact activation system through the formationof FIXa by FXIa (Fig. 2). During the host defenceresponse, a consumption of FXII, prekallikrein andFXI has been observed, whereas plasma levels ofenzyme—inhibitor complexes, such as FXIIa—C1-inhibitor or kallikrein—C1-inhibitor, were increas-ed.1 C1-inhibitor and a1-protease-inhibitor (a1PI)represent the inhibitors of the intrinsic coagulationsystem (Fig. 2).1,94
However, the coagulation system is initially acti-vated over the extrinsic pathway with an increasedexpression of the tissue factor (TF) on endothelialcells and monocytes, induced by bacterial cell wallfragments and pro-inflammatory cytokines (TNF-a,IL-1b) (Fig. 2).61,68,94 The FVII—TF complex stimu-lates the coagulation cascade, with the formation ofFXa and finally thrombin (FIIa), from prothrombin(FII). Thrombin activates FV, FVIII and FXI, leading toenhanced formation of thrombin. After cleavage offibrinogen by thrombin, fibrin monomers polymerizeto form stable fibrin clots, via support of FXIIIa.1,94
To control the consumption of coagulation factors,antithrombin (ATIII) produced by hepatocytes inhi-bits thrombin and FXa, through the formation of athrombin—antithrombin complex.1 This effect canbe enhanced by heparin. Furthermore, ATIII inhibitsthe factors IXa, XIa and XIIa. Further inhibitors arethe tissue factor pathway inhibitor (TFPI) and theactivated protein C, in combination with the freeprotein S.160 However, the plasma level of freeprotein S is decreased during systemic inflamma-tion, through binding to the C4b binding protein(C4bBP).1,160
Disseminated intravascular coagulation canoccur after trauma (Fig. 2).1,68,94,113 After the initialphase, with increased thrombin formation andreduced fibrinolytic cascade, intra- and extra-vascular (e.g. intra-alveolar in ARDS) fibrin clots(hypercoagulability) and increased interactionbetween endothelial cells and leukocytes wasobserved.1,61,94,113 The consumption of coagulationfactors (hypocoagulability) and dysfunction ofthrombocytes are responsible for diffuse bleed-ing (haemorrhagic diathesis).1,68 The intravascularfibrin clots lead finally to microcirculatory distur-
bances with hypoxia-induced cellular damage.1,94
The consumption of coagulation factors is furtherenhanced through the proteolysis of fibrin clotsto fibrin fragments by the protease plasmin(fibrinolysis).94,115
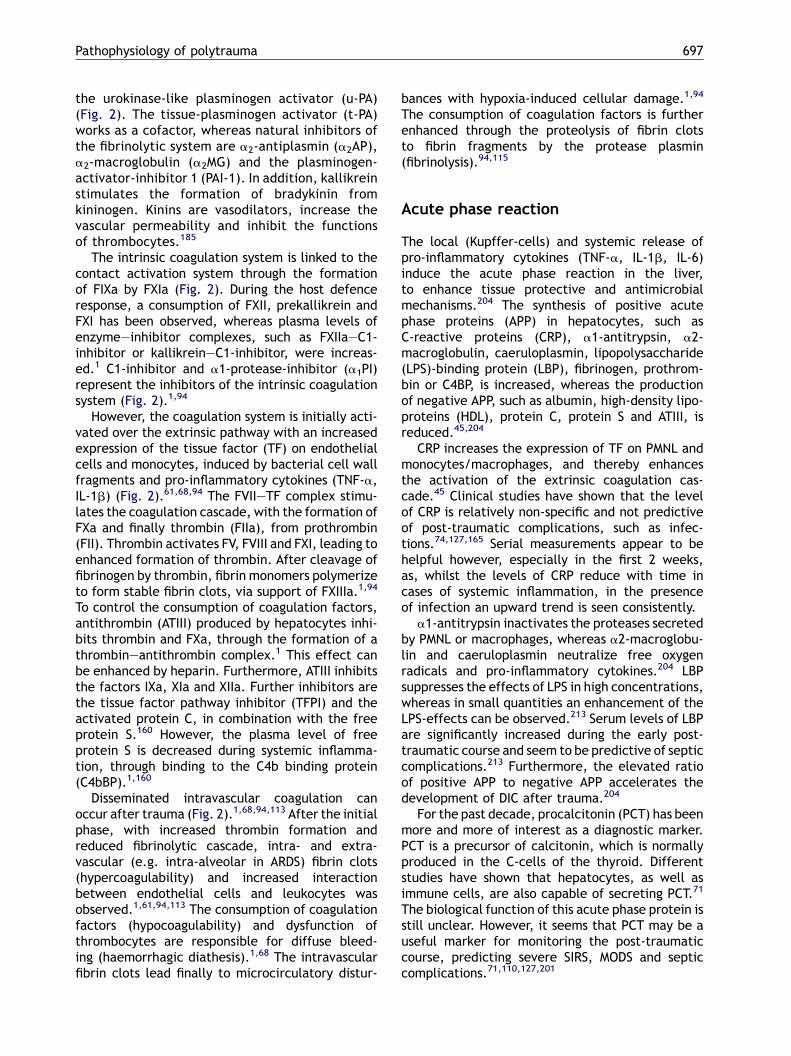
Acute phase reaction
The local (Kupffer-cells) and systemic release ofpro-inflammatory cytokines (TNF-a, IL-1b, IL-6)induce the acute phase reaction in the liver,to enhance tissue protective and antimicrobialmechanisms.204 The synthesis of positive acutephase proteins (APP) in hepatocytes, such asC-reactive proteins (CRP), a1-antitrypsin, a2-macroglobulin, caeruloplasmin, lipopolysaccharide(LPS)-binding protein (LBP), fibrinogen, prothrom-bin or C4BP, is increased, whereas the productionof negative APP, such as albumin, high-density lipo-proteins (HDL), protein C, protein S and ATIII, isreduced.45,204
CRP increases the expression of TF on PMNL andmonocytes/macrophages, and thereby enhancesthe activation of the extrinsic coagulation cas-cade.45 Clinical studies have shown that the levelof CRP is relatively non-specific and not predictiveof post-traumatic complications, such as infec-tions.74,127,165 Serial measurements appear to behelpful however, especially in the first 2 weeks,as, whilst the levels of CRP reduce with time incases of systemic inflammation, in the presenceof infection an upward trend is seen consistently.
a1-antitrypsin inactivates the proteases secretedby PMNL or macrophages, whereas a2-macroglobu-lin and caeruloplasmin neutralize free oxygenradicals and pro-inflammatory cytokines.204 LBPsuppresses the effects of LPS in high concentrations,whereas in small quantities an enhancement of theLPS-effects can be observed.213 Serum levels of LBPare significantly increased during the early post-traumatic course and seem to be predictive of septiccomplications.213 Furthermore, the elevated ratioof positive APP to negative APP accelerates thedevelopment of DIC after trauma.204
For the past decade, procalcitonin (PCT) has beenmore and more of interest as a diagnostic marker.PCT is a precursor of calcitonin, which is normallyproduced in the C-cells of the thyroid. Differentstudies have shown that hepatocytes, as well asimmune cells, are also capable of secreting PCT.71
The biological function of this acute phase protein isstill unclear. However, it seems that PCT may be auseful marker for monitoring the post-traumaticcourse, predicting severe SIRS, MODS and septiccomplications.71,110,127,201

698 M. Keel, O. Trentz
Leukocyte recruitment
The infiltration and accumulation of PMNL representa crucial event for the development of secondaryorgan and tissue damage (theory of neutrophil-mediated tissue injury).21,28,67,180 Pro-inflammatorymediators and toxins induce a leukocyte/endothe-lial cell interaction (adherence) through upregula-tion of adhesion molecules on these cells.112,144,172
During the initial phase of adherence, selectins onleukocytes (L-selectin, leukocyte adhesion mole-cule (LAM-1)) and endothelial cells (E-selectin,endothelial leukocyte adhesion molecule (ELAM-1)and P-selectin (platelet)) are responsible for the‘‘rolling’’ of PMNL.172 In the second step, upregula-tion of integrins on PMNL such as CD11a/CD18 (leu-kocyte function associated molecule-1 or LFA-1),CD11b/CD18 (macrophage antigen-1 or Mac-1),CD11c/CD18 and intercellular adhesion molecules(ICAM-1), or vascular cell adhesion molecules(VCAM-1) on endothelial cells can be observed aftertrauma.172 The interaction of these adhesion mole-cules leads to a stable cell-to-cell contact with aPMNL-attachment, so-called ‘‘sticking’’ of PMNL.Through shedding increased levels of adhesionreceptors (selectins, soluble ICAM-1 (sICAM-1), orsVCAM-1) are detectable in serum of injuredpatients, with a predictive value for the develop-ment of post-traumatic complications.108 Finally,the migration (‘‘diapedesis’’), accumulation andactivation of leukocytes into tissue are mediatedby chemoattractant factors, such as chemokinesand complement anaphylatoxins (C3a, C5a), afterbinding to their corresponding receptors (chemo-taxis).169 Chemokine subfamilies are distinguishedby the position of the first two conserved cysteins,which are either separated by one to three aminoacids, such as CXC chemokine IL-8 (CXCL8), or adja-cent, such as CC chemokine macrophage inflamma-tory protein (MIP)-1a (CCL3).169 Chemokines andC3a or C5a were detectable in increased local con-centrations at sites of injury, as well as systemi-cally.169 In addition, the accumulation of PMNL issupported by reduced spontaneous apoptosis, asdescribed above.82,97,109
Proteases, oxidative stress andcapillary leakage
Infiltrated PMNL and tissue macrophages are respon-sible for the phagocytosis of microorganisms andcellular detritus. However, activated PMNL have aJanus face (Janus, the mythological gate-keeperhas two faces, looking in opposite directions).142
They are also able to induce secondary tissue and
organ damage by degranulation of extracellularproteases (elastase, metalloproteinase) and forma-tion of reactive oxygen species (ROS, oxygen radi-cals), the so-called respiratory burst, or oxidativestress (Fig. 3).28,67,73,123,152,180 Elastases have thecapacity to degrade most proteins in the extracel-lular matrix and important plasma proteins. Theirproteolytic activity is regulated by endogenousprotease inhibitors (PI), such as a1-antitrypsin,a2-macroglobulin, or a1-protease-inhibitor. Inaddition, neutrophil elastase induces the releaseof pro-inflammatory cytokines. Elevated levels ofelastase, or elastase—a1-protease-inhibitor com-plex (Ea1PI), were detectable in multiply injuredpatients depending on the injury severity and thepost-traumatic course.165 In the same manner,metalloproteinases seem to be involved in thedegradation of important structural proteins aftertrauma.23,115,133,152,199
Oxidative cell injury involves the modification ofcellular macromolecules by ROS, often leading tocell death.98,114,123 Superoxide anions (O2
��) aregenerated by membrane associated nicotinamideadenine dinucleotide phosphate (NADPH)-oxidase,which is activated by pro-inflammatory cytokines,arachidonic acid metabolites, complement factorsand bacterial products.77,206 Thereafter, superoxideanions are reduced in the Haber-Weiss reaction tohydrogen peroxide (H2O2) by superoxide dismutasein cytosol (SOD 1), mitochondrion (SOD 2), or cellmembrane (SOD 3). H2O2 is the substrate for themyeloperoxidase that forms the highly toxic andbactericidal hypochloric acid (HOCL). In addition,accumulated H2O2 is transformed to hydroxyl ions(OH��) in the Fenton reaction. The free ROS inducelipid peroxidation, cell membrane disintegrationand DNA-damage of endothelial and parenchymalcells.98,105,175 Furthermore, oxygen radicals andHOCL activate PMNL to release proteases and col-lagenase and to inactivate protease-inhibitors(PI).114 In addition, the capacity of non-enzymaticantioxidants, such as vitamins E or C (scavenger), orenzymatic antioxidants, such as SOD, katalase, orglutathione peroxidase, is reduced during systemicinflammation.136,175
In addition, reactive nitrogen species (RNS)are involved in the pathogenesis of trauma-inducedtissue damage.107 Nitric oxide (NO) is generatedfrom the amino acid L-arginine by inducible nitricoxide synthase (iNOS) in PMNL, or vascular musclecells, and by endothelial nitric oxide synthase(eNOS) in endothelial cells (Fig. 3).107 NO inducesvasodilatation, through increase of guanosine 30,50-cyclic monophosphate (cGMP) by activation of theguanylate cyclase. The activity of iNOS is stimulatedby cytokines and toxins, whereas eNOS is stimulated

Pathophysiology of polytrauma 699
Figure 3 Oxidative stress and capillary leakage. Activated polymorphonuclear leukocytes (PMNL) release reactiveoxygen (ROS) and reactive nitrogen species (RNS). These metabolites in combination with proteases are responsible forendothelial cell damages and the development of a capillary leakage. See text for details and explanations.
by mechanical shearing forces, or by acetylcho-line.107,178 Additional metabolites emerging fromthe interaction of superoxide anions and NO, suchas peroxynitrite (ONOO�) have been shown to med-iate cellular cytotoxicity.107 The results of the vas-cular dysfunction caused by ROS and RNS are ageneralized oedema, clinically manifest as capillaryleakage syndrome, with a disturbance of nutritionaland metabolic exchange, cell swelling and cellulardysfunctions.107
Microcirculatory disturbances
The microcirculation as functional unity, consistingof terminal arterioles, capillaries and venules, reg-ulates nutritional and metabolic exchange in organsand tissues.12,126 Microcirculatory disturbances dur-ing haemorrhagic shock and systemic inflammationare primarymediated through the sympathetic-adre-nal reaction leading to a vasoconstrictionof arteriolesand venules. However, through decreased catechola-mine effect on arterioles, a reduced capillary flowwith an increased hydrostatic pressure can beobserved.12 This microcirculatory alteration, in com-bination with the cytokine and NOmediated capillaryleakage, are responsible for a secondary hypovolae-mia and haemoconcentration, with agglutinationof erythrocytes (red sludge) and thrombocytes (white
sludge).12 The sludge phenomenon leads to anobstruction of the microcirculation with a failure ofthe transcapillary exchange. The cellular oxygendeficiency and the accumulation of metabolites (hid-den acidosis) are finally responsible for tissue andcell damage. In addition, NO (vasodilatation) andendothelin (vasoconstriction) induce a shock-specificmicrocirculatory change with a shunting of someorgan or tissue areas, enhancing their damage.12
Ischaemia/reperfusion injury
Systemic hypoxaemia and hypotension during theresuscitative period after trauma, as well as localhypoperfusion through contusions, lacerations, vas-cular injuries, or compartment syndromes lead to anoxygen deficit in endothelial, parenchymal, orimmune competent cells, which is partially compen-sated for by the intracellular degradation of theenergy-store adenosine triphosphate (ATP) to ade-nosine diphosphate (ADP) and adenosine monopho-sphate (AMP).177 As a result of the ATP-consumption,disturbances of membrane permeability andenergy-dependent Na+/K+-ATPase-pump arise, withan intracellular Na+ increase and cellular swelling.Finally, the generation of hypoxanthine leads to adeficit of the cellular second messenger cyclic AMP(cAMP). The ATP-deficit is further responsible
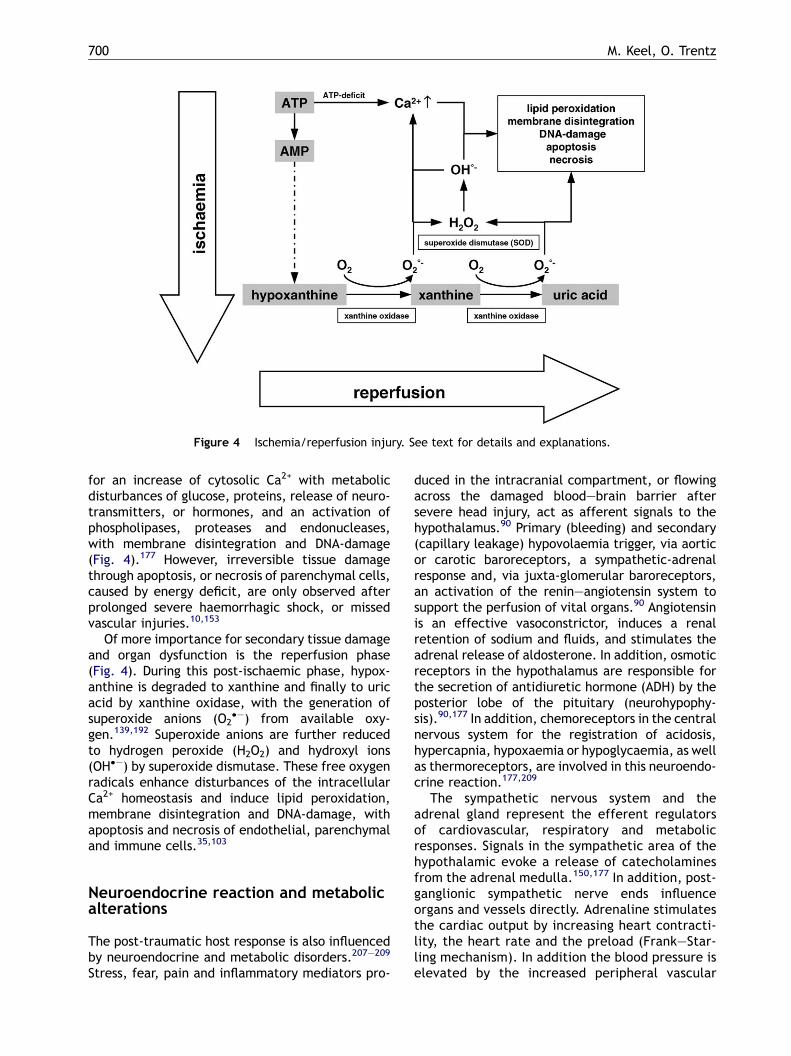
700 M. Keel, O. Trentz
Figure 4 Ischemia/reperfusion injury. See text for details and explanations.
for an increase of cytosolic Ca2+ with metabolicdisturbances of glucose, proteins, release of neuro-transmitters, or hormones, and an activation ofphospholipases, proteases and endonucleases,with membrane disintegration and DNA-damage(Fig. 4).177 However, irreversible tissue damagethrough apoptosis, or necrosis of parenchymal cells,caused by energy deficit, are only observed afterprolonged severe haemorrhagic shock, or missedvascular injuries.10,153
Of more importance for secondary tissue damageand organ dysfunction is the reperfusion phase(Fig. 4). During this post-ischaemic phase, hypox-anthine is degraded to xanthine and finally to uricacid by xanthine oxidase, with the generation ofsuperoxide anions (O2
��) from available oxy-gen.139,192 Superoxide anions are further reducedto hydrogen peroxide (H2O2) and hydroxyl ions(OH��) by superoxide dismutase. These free oxygenradicals enhance disturbances of the intracellularCa2+ homeostasis and induce lipid peroxidation,membrane disintegration and DNA-damage, withapoptosis and necrosis of endothelial, parenchymaland immune cells.35,103
Neuroendocrine reaction and metabolicalterations
The post-traumatic host response is also influencedby neuroendocrine and metabolic disorders.207—209
Stress, fear, pain and inflammatory mediators pro-
duced in the intracranial compartment, or flowingacross the damaged blood—brain barrier aftersevere head injury, act as afferent signals to thehypothalamus.90 Primary (bleeding) and secondary(capillary leakage) hypovolaemia trigger, via aorticor carotic baroreceptors, a sympathetic-adrenalresponse and, via juxta-glomerular baroreceptors,an activation of the renin—angiotensin system tosupport the perfusion of vital organs.90 Angiotensinis an effective vasoconstrictor, induces a renalretention of sodium and fluids, and stimulates theadrenal release of aldosterone. In addition, osmoticreceptors in the hypothalamus are responsible forthe secretion of antidiuretic hormone (ADH) by theposterior lobe of the pituitary (neurohypophy-sis).90,177 In addition, chemoreceptors in the centralnervous system for the registration of acidosis,hypercapnia, hypoxaemia or hypoglycaemia, as wellas thermoreceptors, are involved in this neuroendo-crine reaction.177,209
The sympathetic nervous system and theadrenal gland represent the efferent regulatorsof cardiovascular, respiratory and metabolicresponses. Signals in the sympathetic area of thehypothalamic evoke a release of catecholaminesfrom the adrenal medulla.150,177 In addition, post-ganglionic sympathetic nerve ends influenceorgans and vessels directly. Adrenaline stimulatesthe cardiac output by increasing heart contracti-lity, the heart rate and the preload (Frank—Star-ling mechanism). In addition the blood pressure iselevated by the increased peripheral vascular

Pathophysiology of polytrauma 701
resistance (vasoconstriction of arterioles) and acentralization of the blood in favour of vitalorgans, such as heart and brain, establishedthrough a decrease of the perfusion of splanchnicarea, kidneys and muscles.159
Furthermore, catecholamines influence the post-traumatic metabolism with an increase in theenergy expenditure, hepatic glycogenolysis andgluconeogenesis (glucose-lactate (Cori-cycle) andglucose-alanin cycles), as well as release of freefatty acids.90,150,209 Early hyperglycaemia (gluco-se � 200 mg/dL) after trauma was associated withsignificantly higher infection and mortality rates.106
The natural post-traumatic insulin secretion is toolow to cope with this post-traumatic hyperglycae-mia. In addition, insulin secretion is partiallysuppressed by catecholamines, mediated by a-receptors, whereas glucagon release is elevatedby b-receptor stimulation, contributing to hepaticglycogenolysis and gluconeogenesis.90 A peripheralinsulin resistance has also been observed.177 Differ-ent cytokines (TNF-a, IL-1b) increase the expressionof glucose transport systems (insulin-like activity).The increased intracellular glucose is oxidized topyruvate and finally reduced to lactate (stress lac-tate acidosis), which contributes to the elevatedlactate levels caused primarily by the metaboliclactic acidosis (cellular hypoxia).150 Different stu-dies have shown that early increased serum levels oflactate, or base deficit, are reliable markers for apoor outcome in severely injured patients.3,36
Pain, stress and fear cause the hypothalamus torelease corticotropin-releasing hormone (CRH),leading to a secretion of adrenocorticotropic hor-mone (corticotropin, ACTH) from the anterior lobeof pituitary (adenohypophysis).62,177 ACTH stimu-lates the adrenal cortex to release glucocorticoids(cortisol), or mineralocorticoids (aldosterone).Withinminutes after trauma, increased serum levelsof steroids are detectable.62,177 Glucocorticoidshave different effects on the metabolism, such ashepatic gluconeogenesis, glycogenesis, inhibition ofprotein synthesis, increase of protein degradation inmuscles and mobilization of free fatty acids bylipolysis.90,177 In addition they limit inflammatoryprocesses of mononuclear cells and suppress theproduction of antibodies.90 In contrast, the sponta-neous apoptosis of PMNL is reduced by cortisol.34
Aldosterone increases the renal resorption ofsodium-associated by fluid retention.
The metabolic disorders after trauma are initiallycharacterized by a reduced metabolism for about24 h (acute, shock or ebb phase).90,150,177 This isfollowed by a flow phase with a catabolic metabo-lism for some days to 2 weeks and a final reparativephase with a turnover from a catabolic to an ana-
bolic metabolism.90,150,177 In the second phase, allenergy stores, such as glucose, fat acids and pro-teins, are made available for the host defenceresponse. The increase of the energy expenditurereaches a maximum after 5—10 days.62,90,150,177 Theincreased levels of amino acids are needed for thesynthesis of acute phase proteins in the liver andinflammatory mediators in mononuclear cells. Inaddition, glutamate represents a neurotransmitterand is the most important substrate for the meta-bolic processes of enterocytes and immune cells,conserving the immune integrity of the intestinalwall to avoid bacterial translocation during thesystemic inflammation.90
Multiple organ dysfunctions or failure
The evolution of the physiological and reversiblesystemic inflammation after trauma (host defenceresponse) to a host defence failure, which is asso-ciated with irreversible organ defects and high mor-tality, can be described as an overload of primaryand secondary hits and an imbalance of pro- andanti-inflammatory mechanisms.18,19,118,159,177,188 Inaddition, natural protective factors such as antiox-idants or protease inhibitors are consumed.1
Endothelial cell damage, dysfunction of vascularpermeability with capillary leakage, microcircula-tory disturbances with cellular hypoxia and finallyapoptosis of parenchymal cells by cell-associated,or free, cell death proteins and/or necrosis ofparenchymal cells, are involved in the multipleorgan dysfunctions syndrome or multiple organfailure.18,27,58,79,92,117,153,159,200 Depending on theresponsible insults (primary or secondary) MODScan be classified in primary, or early, MODS andsecondary, or late, MODS.18,27,50,95,157,159,202 Exam-ples of early organ dysfunction are the primarycerebral oedema after head injury, or the primaryARDS after thoracic injury.15,18,95,120,137 The clinicalmanifestation of secondary MODS varies in affectedorgans and dysfunction severities. Therefore, dif-ferent scores, such as the MOF score (Goris score),MODS score (Marshall score), or sequential organfailure assessment (SOFA) score are available todescribe dysfunctions of seven systems: respiratory,cardiovascular, renal, hepatic, gastrointestinal,haematological and central nervous sys-tems.8,63,73,119 For the diagnosis of acute lung injury(ALI), or acute respiratory distress syndrome, bilat-eral lung infiltrations on thoracic X-ray and adecrease of the Horowitz ratio must be observed(PaO2/ FiO2 ratio < 300 corresponds to an ALI,< 200to an ARDS).137 Renal and gastrointestinal systemsare very sensitive to microcirculatory disorders,

702 M. Keel, O. Trentz
leading to a necrosis of renal tubules with increaseof serum creatinine concentrations and oliguria(< 0.5 ml/kg KG/h) or anuria, and to necrosis ofintestinal villi.103,159 The alteration of the intestinalmucosa seems to be responsible for a bacterialtranslocation and explains the high rate of bacter-aemia in the absence of a detectable infective focusin lethal septic complications after trauma (guthypothesis).103,130,159 The gastrointestinal tractoften represents the source for the developmentof secondary multiple organ failure after trauma,whereas the liver represents the engine, with anacute phase and cytokine response, and decreasedfunction of hepatocytes (increase of serum bilirubinconcentration).130,157,162 Repeated scoring is help-ful for identifying categories of injured patients atmajor risk of death, or complications, after surgicalinterventions.8
Therapeutic strategies for multiplyinjured patients
Hypoxia and severe haemorrhagic shock correlatewith high mortality rates, as well as with an highincidence of SIRS, sepsis and organ dysfunction.95 Toreduce these high mortality and morbidity rates inthe post-traumatic course, early ‘‘preventive’’interventions are necessary. According to the guide-lines of advanced trauma life support (ATLS#), earlyoxygenation therapy by intubation and controlledassisted ventilation and an adequate volume ther-apy with crystalloids, colloids and/or blood productsare essential.29 However, the large-volume loadingscheme is the subject of controversial debate insevere haemorrhagic shock.131,174 Patients withblood loss > 2 l should not be overwhelmed bycrystalloids or colloids until surgical managementof bleeding is undertaken, whereas in septic shockearly, goal-directed, high volume therapy is success-ful.161 In contrast, small volume resuscitation insevere traumatic shock seems to avoid a reducedO2 transport capacity, coagulopathy, and infusion-induced hypothermia.131,174
After the primary survey, with basic imaging,multiply injured patients are graded as non-respon-ders, ‘‘borderlines’’ and responders, according tothe initial response to volume therapy, or pharma-ceutical resuscitation.29 Life saving surgical proce-dures, such as decompressing pneumothorax,cardiac tamponade or acute epidural haematoma,and surgical control of massive haemorrhage in thethoracic or abdominal cavities and from pelvic frac-tures, or traumatic amputations are carried outwithout delay.29,53,60,154 These early interventionsseem to limit the systemic inflammation and
decrease the early and late mortality.13 Patientswith a borderline state after primary survey, orpatients with a high trauma impact, or at risk ofadverse outcome, such as head injury, bilateral lungcontusions, multiple long bone fractures, coagulo-pathy, hypothermia or a presumed operationtime > 6 h, should be supplied with a stagedsequential surgical management as damage control,after the further work up in the secondary survey, toavoid or limit the influence of second hits (inter-ventional or antigenic loads).147,202 Damage controlincludes haemorrhage control through tamponade,vascular repair or vessel ligation, and organ resec-tions.59 In addition, a reduction of contaminationafter hollow organ injuries, or open fractures, aswell as decompression of compartment syndromesof the extremities by fasciotomy, or of the abdomenby decompressive laparotomy, should contribute tothe limitation of secondary inflammatory pro-cesses.11,49,89,154 Furthermore, the temporary sta-bilization of pelvic and long bone fractures, ordislocations of large joints, by rapidly assembledand applied external fixators seem to be benefi-cal.49,53,89,141,147,154 This concept decreases the sys-temic release of pro- and anti-inflammatorymediators, in comparison with definitive interven-tions, such as reamed nailing (early total care).147
Debridement of open wounds and fractures, withresection of non-viable tissues, temporary closureby vacuum assisted closure therapy and second lookinterventions, contribute to a limited antigenicload, with a decrease in septic complications.89,186
However, the early stabilization of major skeletalinjuries (early total care) represents still theconcept for patients with isolated fractures and inthe absence of high traumatic impact and the riskfactors mentioned above.147
With regard to strategies for post-traumaticintensive care, only supportive therapies are estab-lished to avoid secondary organ damage and hits.95
Secondary brain injuries, with elevated intracranialpressure (ICP) due to cerebral oedema, or ischae-mia/reperfusion injuries, can be limited by applyingdifferent neuroprotective strategies, such as con-trolled hyperventilation, moderate hypothermia,and release of cerebrospinal fluid (CSF).167,183
Whenever these therapeutic regimens fail to reduceICP, intravenous administration of barbiturate maybecome necessary.183 The beneficial effect of bar-biturates, in terms of lowering elevated ICP, isthought to be due to decreased cerebral metabolismand blood flow.41 Other supportive therapies includemechanical ventilation, inotropes and haemofiltra-tion for renal failure.159,177 Furthermore, a singleshot of an antibiotic (cephalosporin) after traumareduces the post-traumatic wound infection rate.196

Pathophysiology of polytrauma 703
Further antibiotics should only be given accordingto an antibiogram of an infectious focus.196 Earlyenteral nutrition, via gastric or duodenal tubes,reduces the accumulation of pathogenic bacteriain the intestinal tract and avoids atrophy of intest-inal mucosa,.177,184 Additional arginine, glutamine,nucleotides, or unsaturated omega-3-fatty acids(‘‘immune-enhanced enteral nutrition’’ (IEEN)) re-duce post-traumatic hypermetabolism and improveimmune competence.26
Despite thorough insights into the pathophysio-logical mechanisms of post-traumatic systemicinflammation and hopeful results of animal studies,multiple prospective clinical trials performed in thepast decades, especially in patients with sepsis,have failed to provide a benefit of anti-inflamma-tory, anti-coagulant, or antioxidant strategieswith regard to the mortality, whereas the incidenceof post-traumatic complications, such as infections,or multiple organ dysfunctions, has partiallydecreased.2,13,33,64,65,72,91,113,136,151 However, themagic bullet is still not found. Reasons for theseequivocal results may include individual injury pat-terns, inappropriate timing of drug administration,or suboptimal drug levels at the target site.35,65 Inaddition, the study protocols have focused onsingle mechanisms only, whereas the immunenetwork is more complex and individual (genepolymorphism, sexual dimorphism), as describedabove.13,64,65,93,151 Nevertheless, some successfulclinical studies are available, especially for septicpatients, although the underlying mechanisms havenot been clearly defined.91 Trauma patients receiv-ing high doses of intravenous immunoglobulinsexhibit a reduction in septic complications andan improvement in serum bactericidal activity.44
Treatment with recombinant human activated pro-tein C (drotrecogin alfa activated) showed a sig-nificant reduction of mortality in patients withsevere sepsis.14 However, criticisms concern dataconsistence, unclear mechanism of action and theincreased risk of bleeding, which restricts its use ininjured patients, especially with severe head inju-ries.14,48 Although the effects of steroids in patientswith sepsis are controversial, low doses of corti-costeroids seem to reduce the mortality rate inpatients with septic complications.7,191 Insulinhas recently been shown to decrease mortalityand to prevent the incidence of multiple organfailure in critically ill patients.96 It seems thatinsulin attenuates the inflammatory response bydecreasing the pro-inflammatory, and increasingthe anti-inflammatory, cascades, thus restoringsystemic homeostasis, which has been shownto be critical for organ function and survival incritically ill patients.96
Although some successful progress in clinicaltrials is obvious, better understanding of the patho-logical mechanisms at local site of injury wouldidentify exact primary targets for drug interven-tions. However, progress in diagnostic tools forthe monitoring of the immune status (beside immu-nomonitoring) may become more successful for themanagement of severely injured patients in the nearfuture. Parallel monitoring of pro- (e.g. IL-6) andanti-inflammatory (e.g. IL-10) cytokines, as well asacute phase proteins (e.g. CRP, procalcitonin), orother factors, could help us in the decision makingfor optimal secondary operative interventions tolimit second hits.71,170 However, more prospectivediagnostic studies have to be conducted, to under-stand the kinetics and significance of these factorsin order to optimize the concept of damagecontrol.
References
1. Abraham E. Coagulation abnormalities in acute lung injuryand sepsis. Am J Respir Cell Mol Biol 2000;22:401—4.
2. Abraham E, Reinhart K, Opal S, et al., OPTIMIST Trail StudyGroup. Efficacy and safety of tifacogin (recombinant tissuefactor pathway inhibitor) in severe sepsis: a randomizedcontrolled trial. JAMA 2003;290:256—8.
3. Abramson D, Scalea TM, Hitchcock R, et al. Lactateclearance and survival following injury. J Trauma 1993;35:584—9.
4. Acosta JA, Yang JC, Winchell RJ, et al. Lethal injuries andtime to death in a level I trauma center. J Am Coll Surg1998;186:528—33.
5. Alderson MR, Tough TW, Davis-Smith T, et al. Fas ligandmediates activation-induced cell death in human T lympho-cytes. J Exp Med 1995;181:71—7.
6. Definitions for sepsis and organ failure and guidelines for theuse of innovative therapies in sepsis.In: American College ofChest Physicians/Society of Critical Care Medicine Consen-sus Conference. Crit Care Med 1992;20:864—74.
7. Annane D, Sebille V, Charpentier C, et al. Effect of treat-ment with low doses of hydrocortisone and fludrocortisoneon mortality in patients with septic shock. JAMA 2002;288:862—71.
8. Antonelli M, Moreno R, Vincent JL, et al. Application of SOFAscore to trauma patients. Sequential organ failure assess-ment. Intensive Care Med 1999;25:389—94.
9. Antonelli M, Moro ML, Capelli O, et al. Risk factors for earlyonset pneumonia in trauma patients. Chest 1994;105:224—8.
10. Arundine M, Tymianski M. Molecular mechanisms of calcium-dependent neurodegeneration in excitotoxicity. Cell Cal-cium 2003;34:325—37.
11. Asensio JA, McDuffie L, Petrone P, et al. Reliable variables inthe exsanguinated patient which indicate damage controland predict outcome. Am J Surg 2001;182:743—51.
12. Bateman RM, Sharpe MD, Ellis CG. Bench-to-bedside review:microvascular dysfunction in sepsis–—hemodynamics, oxy-gen transport, and nitric oxide. Crit Care Med 2003;7:359—73.

704 M. Keel, O. Trentz
13. Baue AE, DurhamR, Faist E. Systemic inflammatory responsesyndrome (SIRS), multiple organ dysfunction syndrome(MODS), multiple organ failure (MOF): are we winning thebattle? Shock 1998;10:79—89.
14. Bernard GR, Vincent JL, Laterre PF, et al. Recombinanthuman protein C worldwide evaluation in severe sepsis(PROWESS) study group. Efficacy and safety of recombinanthuman activated protein C for severe sepsis. N Engl J Med2001;344:699—709.
15. Bhatia M, Moochhala S. Role of inflammatory mediators inthe pathophysiology of acute respiratory distress syndrome.J Pathol 2004;202:145—56.
16. Biffl WL, Moore EE, Moore FA, et al. Interleukin-6 delaysneutrophil apoptosis. Arch Surg 1996;131:24—30.
17. Bone RC. Toward an epidemiology and natural history ofSIRS (systemic inflammatory response syndrome). JAMA1992;268:3452—5.
18. Bone RC. Immunologic dissonance: a continuing evolution inour understanding of the systemic inflammatory responsesyndrome (SIRS) and the multiple organ dysfunction syn-drome (MODS). Ann Intern Med 1996;125:680—7.
19. Bone RC. Sir Isaac Newton, sepsis, SIRS, and CARS. Crit CareMed 1996;24:1125—8.
20. Brach MA, deVos S, Gruss H-J, Herrmann F. Prolongation ofsurvival of human polymorphonuclear neutrophils by gran-ulocyte-macrophage colony-stimulating factor is causedby inhibition of programmed cell death. Blood 1992;80:2920—4.
21. Botha AJ, Moore FA, Moore EE, et al. Postinjury neutrophilpriming and activation: an early vulnerable window. Surgery1995;118:358—65.
22. Buzdon MM, Napolitano LM, Shi HJ, et al. Femur fractureinduces site-specific changes in T-cell immunity. J Surg Res1999;82:201—8.
23. Carney DE, McCann UG, Schiller HJ, et al. Metalloproteinaseinhibition prevents acute respiratory distress syndrome. JSurg Res 2001;99:245—52.
24. Cassatella MA, Meda L, Bonora S, et al. Interleukin-10 (IL-10)inhibits the release of pro-inflammatory cytokines fromhuman polymorphonuclear leukocytes. Evidence for anautocrine role of tumor necrosis factor and IL-1b in mediat-ing the production of IL-8 triggered by lipopolysaccharide. JExp Med 1993;178:2207—11.
25. Cavaillon JM, Adrie C, Fitting C, Adib-Conquy M. Endotoxintolerance: is there a clinical relevance? J Endotoxin Res2003;9:101—7.
26. Chuntrasakul C, Siltharm S, Sarasombath S, et al.Metabolic and immune effects of dietary arginine, gluta-mine and omega-3 fatty acids supplementation in immu-nocompromised patients. J Med Assoc Thai 1998;81:334—43.
27. Ciesla DJ, Moore EE, Johnson JL, et al. Multiple organdysfunction during resuscitation is not postinjury multipleorgan failure. Arch Surg 2004;139:590—4.
28. Cochrane CG. Immunologic tissue injury mediated by neu-trophilic leukocytes. Adv Immunol 1968;9:97—162.
29. Collicott PE, Hughes I. Training in advanced trauma lifesupport. JAMA 1980;243:1156—9.
30. Collighan N, Giannoudis PV, Kourgeraki O, et al. Interleukin13 and inflammatory markers in human sepsis. Br J Surg2004;91:762—8.
31. Colotta F, Re F, Polentarutti N, et al. Modulation of granu-locyte survival and programmed cell death by cytokines andbacterial products. Blood 1992;80:2012—20.
32. Coopersmith CM, Zack JE, Ward MR, et al. The impact ofbeside behavior on catheter-related bacteremia in theintensive care unit. Arch Surg 2004;139:131—6.
33. Cox G. IL-10 enhances resolution of pulmonary inflammationin vivo by promoting apoptosis of neutrophils. Am J Physiol1996;271:L566—71.
34. Cox G. Glucocorticoid treatment inhibits apoptosis in humanneutrophils: separation of survival and activation outcomes.J Immunol 1995;154:4719—25.
35. Cristofori L, Tavazzi B, Gambin R, et al. Early onset of lipidperoxidation after human traumatic brain injury: a fatallimitation for the free radical scavenger pharmacologicaltherapy? J Investig Med 2001;49:450—8.
36. Davis JW, Parks SN, Kaups KL, et al. Admission base deficitpredicts transfuion requirements and risk of complications.J Trauma 1996;41:769—74.
37. De Freitas I, Fernandez-Somoza M, Essenfeld-Sekler E, Car-dier JE. Serum levels of the apoptosis-associatedmolecules,tumor necrosis factor-alpha/tumor necrosis factor type-Ireceptor and Fas/FasL, in sepsis. Chest 2004;125:2238—46.
38. Demetriades D, Murray J, Charalambides K, et al. Traumafatalities: time and location of hospital deaths. J Am CollSurg 2004;198:20—6.
39. Dhein J, Walczak H, Baumler C, et al. Autocrine T-cellsuicide mediated by APO-1/(Fas/CD95). Nature 1995;373:438—41.
40. Dinarello CA. Proinflammatory cytokines. Chest 2000;118:503—8.
41. Donegan JH, Traystman FJ, Koehler RC, et al. Cerebrovas-cular hypoxic and autoregulatory responses during reducedbrain metabolism. Am J Physiol 1985;249:H421—9.
42. Donnelly TJ, Meade P, Jagels M, et al. Cytokine, comple-ment, and endotoxin profiles associated with the develop-ment of the adult respiratory distress syndrome after severeinjury. Crit Care Med 1994;22:768—76.
43. Donnelly SC, Strieter RM, Kunkel SL, et al. Interleukin-8 anddevelopment of adult respiratory distress syndrome in at-risk patient groups. Lancet 1993;341:643—7.
44. Douzinas EE, Pitaridis MT, Louris G, et al. Prevention ofinfection in multiple trauma patients by high-dose intrave-nous immunoglobulins. Crit Care Med 2000;28:8—15.
45. Du Clos TW. Function of C-reactive protein. Ann Med2000;32:274—8.
46. Dunham CM, Damiano AM, Wiles CE, Cushing BM. Post-traumatic multiple organ dysfunction syndrome–—infectionis an uncommon antecedent risk factor. Injury 1995;26:373—8.
47. Dunican AL, Leuenroth SJ, Grutkoski P, et al. TNFalpha-induced suppression of PMN apoptosis is mediated throughinterleukin-8 production. Shock 2000;14:284—8.
48. Eichacker PQ, Natanson C. Recombinant human activatedprotein C in sepsis: inconsistent trial results, an unclearmechanism of action and safety concerns resulted in label-ing restrictions and the need for phase IV trials. Crit CareMed 2003;31(Suppl. 1):594—6.
49. Ertel W, Eid K, Keel M, Trentz O. Therapeutical strategiesand outcome of polytraumatized patients with pelvic inju-ries. A six-year experience. Eur J Trauma 2000;26:278—86.
50. Ertel W, Friedl HP, Trentz O. Multiple organ dysfunctionsyndrome (MODS) following multiple trauma: rationaleand concept of therapeutic approach. Eur J Pediatric Surg1994;4:243—8.
51. Ertel W, Keel M, Buergi U, et al. Granulocyte colony-stimu-lating factor inhibits neutrophil apoptosis at the local siteafter severe head and thoracic injury. J Trauma1999;46:784—92.
52. Ertel W, Keel M, Bonaccio M, et al. Release of anti-inflam-matory mediators after mechanical trauma correlateswith severity of injury and clinical outcome. J Trauma1995;39:879—85.

Pathophysiology of polytrauma 705
53. Ertel W, Keel M, Eid K, et al. Control of severe haemorrhageusing C-clamp and pelvic packing in multiply injuredpatients with pelvic ring disruption. J Orthop Trauma2001;15:468—74.
54. Ertel W, Keel M, Infanger M, et al. Circulating mediators inserum of injured patients with septic complications inhibitneutrophil apoptosis through up-regulation of protein-tyr-osine phosphorylation. J Trauma 1998;44:767—75.
55. Ertel W, Keel M, Marty D, et al. Significance of systemicinflammation in 1278 trauma patients. Unfallchirurg1998;101:520—6.
56. Ertel W, Keel M, Neidhardt R, et al. Inhibition of the defencesystem stimulating interleukin-12 interferon-gamma path-way during critical illness. Blood 1997;89:1612—20.
57. Ertel W, Keel M, Steckholzer U, et al. Interleukin-10 attenu-ates the release of pro-inflammatory cytokines butdepresses splenocyte functions in murine endotoxemia.Arch Surg 1996;131:51—6.
58. Ertel W, Keel M, Stocker R, et al. Detectable concentrationsof Fas ligand in cerebrospinal fluid after severe head injury.J Neuroimmunol 1997;80:93—6.
59. Ertel W, Oberholzer A, Platz A, et al. Incidence and clinicalpattern of the abdominal compartment syndrome after‘‘damage-control’’ laparotomy in 311 patients with severeabdominal and/or pelvic trauma. Crit Care Med 2000;28:1747—53.
60. Ertel W, Trentz O. Causes of shock in the severely trauma-tized patient: emergency treatment. In: Goris RJA, TrentzO, editors. The integrated approach to trauma care. Berlin,Heidelberg, New York: Springer-Verlag; 1995. p. 78—87.
61. Fan J, Kapus A, Li YH, et al. Priming for enhanced alveolarfibrin deposition after haemorrhagic shock: role of tumornecrosis factor. Am J Respir Cell Mol Biol 2000;22:412—21.
62. Feldman Z, Contant CF, Pahwa R, et al. The relationshipbetween hormonal mediators and systemic hypermetabo-lism after severe head injury. J Trauma 1993;34:806—16.
63. Ferreira FL, Bota DP, Bross A, et al. Serial evaluation of theSOFA score to predict outcome in critically ill patients. JAMA2001;286:1754—8.
64. Finney SJ, Evans TW. Emerging therapies in severe sepsis.Thorax 2002;57(Suppl. II):ii8—14.
65. Fisher CJ, Agosti JM, Opal SM, et al., Soluble TNF RecetporStudy Group. Treatment of septic shock with the tumornecrosis factor receptor Fc fusion protein. N Eng J Med1996;334:1697—702.
66. Fosse E, Pillgram-Larsen J, Svennevig JL, et al. Complementactivation in injured patients occurs immediately and isdependent on the severity of the trauma. Injury 1998;29:509—14.
67. Fujishima S, Aikawa N. Neutrophil-mediated tissue injuryand its modulation. Intensive Care Med 1995;21:277—85.
68. Gando S, Kameue T, Matsuda N, et al. Combined activationof coagulation and inflammation has an important role inmultiple organ dysfunction and poor outcome after severetrauma. Thromb Haemost 2002;88:943—9.
69. Geng Y, Gulbins E, Altman A, Lotz M. Monocyte deactivationby interleukin-10 via inhibition of tyrosine kinase activityand the Ras signaling pathway. Proc Natl Acad Sci U S A1994;91:8602—6.
70. Gennarelli TA, Champion HR, Copes WS, Sacco WJ. Compar-ison of mortality, morbidity, and severity of 59,713 headinjured patients with 114,447 patients with extracranialinjuries. J Trauma 1994;37:962—8.
71. Giannoudis PV, Hildebrand F, Pape HC. Inflammatory serummarkers in patients with multiple trauma. J Bone Joint Surg(Br) 2004;86-B:313—23.
72. Gilgun-Sherki Y, Rosenbaum Z, Melamed E, Offen D. Anti-oxidant therapy in acute central nervous system injury:current state. Pharmacol Rev 2002;54:271—84.
73. Goris RJ, te Boekhorst TP, Neytinck JK, Gimbreve JS. Multi-ple organ failure–—generalized autodestructive inflamma-tion? Arch Surg 1985;120:1109—15.
74. Gosling P, Dickson GR. Serum C-reactive protein in patientswith serious trauma. Injury 1992;23:483—6.
75. Green D, Kroemer G. The central executioners of apoptosis:caspases or mitochondria? Trends Cell Biol 1998;8:267—71.
76. Greenspan L, McLellan BA, Greig H. Abbreviated injury scaleand injury severity score: a scoring chart. J Trauma1985;25:60—4.
77. Grote K, Flach I, Luchtefeld M, et al. Mechanicalstretch enhances mRNA expression and proenzyme releaseof matrix metalloproteinase-2 (MMP-2) via NAD(P)H oxi-dase-derived reactive oxygen species. Circ Res 2003;92:e80—6.
78. Harter L, Keel M, Hentze H, et al. Spontaneous neutrophilapoptosis in patients with sepsis is independent of caspaseactivity. J Trauma 2001;50:982—8.
79. Harter L, Keel M, Hentze H, et al. Caspase-3 activity ispresent in cerebrospinal fluid from patients with traumaticbrain injury. J Neuroimmunol 2001;121:76—8.
80. Harter L, Mica L, Stocker R, et al. Increased expression oftoll-like receptor-2 and -4 on leukocytes from patients withsepsis. Shock 2004;22:403—9.
81. Haga Y, Beppu T, Doi K, et al. Systemic inflammatoryresponse syndrome and organ dysfunction following gastro-intestinal surgery. Crit Care Med 1997;25:1994—2000.
82. Haslett C, Savill JS,WhyteMKB, et al. Granulocyte apoptosisand the control of inflammation. Philos Trans R Soc Lond BBiol Sci 1994;345:327—33.
83. Heagy W, Hansen C, Nieman K, West MA. Evidence for aCD14- and serum-independent pathway in the induction ofendotoxin-tolerance in human monocytes and THP-1 mono-cytic cells. Shock 2003;19:321—7.
84. Heagy W, Hansen C, Nieman K, et al. Impaired mitogen-activated protein kinase activation and altered cytokinesecretion in endotoxin-tolerant human monocytes. JTrauma 2000;49:806—14.
85. Heagy W, Nieman K, Hansen C, et al. Lower levels of wholeblood LPS-stimulated cytokine release are associated withpoorer clinical outcomes in surgical ICU patients. Surg Infect2003;4:171—80.
86. Hecke F, Schmidt U, Kola A, et al. Circulating complementproteins in multiple trauma patients-correlation with injuryseverity, development of sepsis, and outcome. Crit CareMed 1997;25:2015—24.
87. Helling TS, Evans LL, Fowler DL, et al. Infectious complica-tions in patients with severe head injury. J Trauma1988;28:1575—7.
88. Hensler T, Sauerland S, Bouillon B, et al. Associationbetween injury pattern of patients with multiple injuriesand circulating levels of soluble tumor necrosis factorreceptors, interleukin-6, and interleukin-10 and poly-morphonuclear neutrophil elastase. J Trauma 2002;52:962—70.
89. Hildebrand F, Giannoudis P, Kretteck C, Pape HC. Damagecontrol: extremities. Injury 2004;35:678—89.
90. Hill AG, Hill GL. Metabolic response to severe injury. Br JSurg 1998;85:884—90.
91. Hotchkiss RS, Karl IE. The pathophysiology and treatment ofsepsis. N Engl J Med 2003;348:138—50.
92. Hotchkiss RS, Swanson PE, Freeman BD, et al. Apoptotic celldeath in patients with sepsis, shock, and multiple organdysfunction. Crit Care Med 1999;27:1230—51.
706 M. Keel, O. Trentz
93. Holmes CL, Russell JA, Walley KR. Genetic polymorphisms insepsis and septic shock: role in prognosis and potential fortherapy. Chest 2003;124:1103—15.
94. Idell S. Coagulation, fibrinolysis, and fibrin depositionin acute lung injury. Crit Care Med 2003;31(Suppl. 4):213—220.
95. Jarrar D, Chaudry IH, Wang P. Organ dysfunction followinghaemorrhage and sepsis: mechanisms and therapeuticapproaches. Int J Mol Med 1999;4:575—83 [review].
96. Jeschke MG, Klein D, Herndon DN. Insulin treatmentimproves the systemic inflammatory reaction to severetrauma. Ann Surg 2004;239(4):553—60.
97. Jimenez MF, Watson RWG, Parodo J, et al. Dysregulatedexpression of neutrophil apoptosis in the systemicinflammatory response syndrome. Arch Surg 1997;132:1263—1270.
98. Kazzaz JA, Xu J, Palaia TA, et al. Cellular oxygen toxicity.Oxidant injury without apoptosis. J Biol Chem 1996;271:15182—6.
99. Keel M, Bonaccio M, Steckholzer U, et al. Increased plasmalevel of Type I (p55) and Type II (p75) TNF-receptors follow-ing trauma. Swiss Surg 1995;5:241—4.
100. Keel M, Ecknauer E, Stocker R, et al. Different pattern oflocal and systemic release of pro-inflammatory and anti-inflammatory mediators in severely injured patients withchest trauma. J Trauma 1996;40:907—12.
101. Keel M, Schregenberger N, Steckholzer U, et al. Endotoxintolerance after severe injury and its regulatory mechan-isms. J Trauma 1996;41:430—8.
102. Keel M, Ungethuem U, Steckholzer U, et al. Interleukin-10counterregulates pro-inflammatory cytokine induced inhi-bition of neutrophil apoptosis during severe sepsis. Blood1997;90:3356—63.
103. Kong SE, Blennerhassett LR, Heel KA, et al. Ischaemia—reperfusion injury to the intestine. Aust N Z J Surg1998;68:554—61.
104. Kossmann T, Stahel PF, Lenzlinger PM, et al. Interleukin-8released into the cerebrospinal fluid after brain injury isassociated with blood—brain barrier dysfunction and nervegrowth factor production. J Cereb Blood Flow Metab1997;17:280—9.
105. Kretzschmar M, Pfeiffer L, Schmidt C, Schirrmeister W.Plasma levels of glutathione, alpha-tocopherol and lipidperoxides in polytraumatized patients; evidence for a sti-mulating effect of TNF alpha on glutathione synthesis. ExpToxicol Pathol 1998;50:477—83.
106. Laird AM, Miller PR, Kilgo PD, et al. Relationship of earlyhyperglycemia to mortality in trauma patients. J Trauma2004;56:1058—62.
107. Laroux FS, Pavlick KP, Hines IN, et al. Role of nitric oxide ininflammation. Acta Physiol Scand 2001;173:113—8.
108. Law MM, Cryer HG, Abraham E. Elevated levels of solubleICAM-1 correlate with the development of multiple organfailure in severely injured trauma patients. J Trauma1994;37:100—9.
109. Lee A, Whyte MKB, Haslett C. Inhibition of apoptosis andprolongation of neutrophil functional longevity by inflam-matory mediators. J Leukoc Biol 1993;54:283—8.
110. Lee YJ, Park CH, Yun JW, Lee YS. Predictive comparisons ofprocalcitonin (PCT) level, arterial ketone body ratio (AKBR),APACHE III score and multiple organ dysfunction score(MODS) in systemic inflammatory response syndrome (SIRS).Yonsei Med J 2004;29(45):29—37.
111. Lenardo MJ. Fas and the art of lymphocyte maintenance. JExp Med 1996;183:721—4.
112. Leone M, Boutiere B, Camoin-Jau L, et al. Systemicendothelial activation is greater in septic than in trau-
matic-haemorrhagic shock but does not correlate withendothelial activation in skin biopsies. Crit Care Med2002;30:808—14.
113. Levi M, de Jonge E, van der Poll T. New treatment strategiesfor disseminated intravascular coagulation based on currentunderstanding of the pathophysiology. Ann Med 2004;36:41—9.
114. Lewen A, Matz P, Chan PH. Free radical pathways in CNSinjury. J Neurotrauma 2000;17:871—90.
115. Lo EH, Wang X, Cuzner ML. Extracellular proteolysis in braininjury and inflammation: role for plasminogen activatorsand matrix metalloproteinases. J Neurosci Res 2002;69:1—9.
116. Lyons A, Kelly JL, Rodrick ML, et al. Major injury inducesincreased production of interleukin-10 by cells of theimmune system with a negative impact on resistance toinfection. Ann Surg 1997;226:450—8.
117. Mahidhara R, Billiar TR. Apoptosis in sepsis. Crit Care Med2000;28:N105—13.
118. Malone DL, Kuhls D, Napolitano LM, et al. Back to basics:validation of the admission systemic inflammatory responsesyndrome score in predicting outcome in trauma. J Trauma2001;51:458—63.
119. Marshall JC, Cook DJ, Christou NV, et al. Multiple organdysfunction score: a reliable descriptor of a complex clinicaloutcome. Crit Care Med 1995;23:1638—52.
120. Martin TR, Cytokines. the acute respiratory distresssyndrome (ARDS): a question of balance. Nat Med 1997;3:272—3.
121. Martin C, Boisson C, Haccoun M, et al. Patterns of cytokineevolution (tumor necrosis-a and interleukin-6) after septicshock, hemorrhagic shock, and severe trauma. Crit CareMed 1997;25:1813—9.
122. Martin GS, Mannino DM, Eaton S, Moss M. The epidemiologyof sepsis in the United State from 1979 through 2000. N EnglJ Med 2003;348:1546—54.
123. Martins PS, Kallas EG, Neto MC, et al. Upregulation ofreactive oxygen species generation and phagocytosis, andincreased apoptosis in human neutrophils during severesepsis and septic shock. Shock 2003;20:208—12.
124. Matute-Bello G, Liles WC, Radella F, et al. Neutrophil apop-tosis in the acute respiratory distress syndrome. Am J RespirCrit Care Med 1997;156:1969—77.
125. Maxwell RA, Fabian TC, Croce MA, Davis KA. Secondaryabdominal compartment syndrome: an underappreciatedmanifestation of severe hemorrhagic shock. J Trauma1999;47:995—9.
126. Menger MD, Richter S, Yamauchi JI, Vollmar B. Intravitalmicroscopy for the study of the microcirculation invarious disease states. Ann Acad Med Singapore 1999;28:542—56.
127. Mimoz O, Benoist JF, Edouard AR, et al. Procalcitonin andC-reactive protein during the eraly post-traumatic systemicinflammatory response syndrome. Intensive Care Med1996;24:185—8.
128. Mock CN, Jurkovich GJ, nii-Amon-Kotei D, et al. Traumamortality patterns in three nations at different economiclevels: implications for global trauma system development.J Trauma 1998;44:804—14.
129. Mollnes TE, Fosse E. The complement system in trauma-related and ischemic tissue damage: a brief review. Shock1994;2:301—10.
130. Moore FA. The role of the gastrointestinal tract in pos-tinjury multiple organ failure. Am J Surg 1999;178:449—53.
131. Moore FA, McKinley BA, Moore EE. The next generation inshock resuscitation. Lancet 2004;363(9425):1988—96.

Pathophysiology of polytrauma 707
132. Morganti-Kossmann MC, Lenzlinger PM, Hans V, et al. Pro-duction of cytokines following brain injury. Mol Psychiatry1997;2:133—6.
133. Nagase H, Woessner Jr JF. Matrix metalloproteinases. J BiolChem 1999;274:21491—4.
134. Nagata S. Apoptosis by death factor. Cell 1997;88:355—65.
135. Napolitano LM, Ferrer T, McCarter R, Scalea T. Systemicinflammatory response syndrome (SIRS) score on admissionindependently predicts mortality and length of stay intrauma patients. J Trauma 2000;49:647—52.
136. Nathens AB, Neff MJ, Jurkovich GJ, et al. Randomized,prospective trial of antioxidant supplementation incritically ill surgical patients. Ann Surg 2002;236(6):814—22.
137. Neff MJ. The epidemiology and definition of the acuterespiratory distress syndrome. Respir Care Clin N Am2003;9:273—82.
138. Neidhardt R, Keel M, Steckholzer U, et al. Relationship ofinterleukin-10 plasma levels to severity of injury and clinicaloutcome in injured patients. J Trauma 1997;42:863—71.
139. Nemeth I, Boda D. Xanthine oxidase activity and bloodglutathione redox ratio in infants and children with septicshock syndrome. Intensive Care Med 2001;27:216—21.
140. Neumann B, Zantl N, Veihelmann A, et al. Mechanismsof acute inflammatory lung injury induced by abdominalsepsis. Int Immunol 1999;11:217—27.
141. Nowotarski PJ, Turen CH, Brumback RJ, Scarboro JM. Con-version of external fixation to intramedullary nailing forfractures of the shaft of the femur in multiply injuredpatients. J Bone Joint Surg Am 2000;82:781—8.
142. Nussler AK, Wittel UA, Nussler NC, Beger HG. Leukocytes,the Janus cells in inflammatory disease. Langenbecks ArchSurg 1999;384:222—32.
143. Oberholzer A, Keel M, Zellweger R, et al. Incidence of septiccomplications in multiple injured patients is gender speci-fic. J Trauma 2000;48:932—7.
144. Ogura H, Tanaka H, Koh T, et al. Enhanced production ofendothelial microparticles with increased binding to leuko-cytes in patients with severe systemic inflammatoryresponse syndrome. J Trauma 2004;56:823—30.
145. Oka M, Hirazawa K, Yamamoto K, et al. Induction of Fas-mediated apoptosis on circulating lymphocytes by surgicalstress. Ann Surg 1996;4:434—40.
146. O’Sullivan ST, Lederer JA, Horgan AF, et al. Major injuryleads to predominance of the T helper-2 lymphocyte phe-notype and diminished interleukin-12 production associatedwith decreased resistance to infection. Ann Surg 1995;222:482—92.
147. Pape H-CC., Giannoudis P, Krettek C. The timing of fracturetreatment in polytrauma patients: relevance of damagecontrol orthopedic surgery. Am J Surg 2002;183:622—9.
148. Parisi DM, Koval K, Egol K. Fat embolism syndrome. Am JOrthop 2002;31:507—12.
149. Peng R, Chang C, Gilmore D, Bongard F. Epidemiology ofimmediate and early trauma deaths at an urban level Itrauma center. Am Surg 1998;64:950—4.
150. Plank LD, Hill GL. Sequential metabolic changes followinginduction of systemic inflammatory response in patientswith severe sepsis or major blunt trauma. World J Surg2000;24:630—8.
151. Poldermann KH, Girbes AR. Drug intervention trials in sep-sis: divergent results. Lancet 2004;363:1721—3.
152. Powell WC, Fingleton B, Wilson CL, et al. The metallopro-teinase matrilysin proteolytically generates active solubleFas ligand and potentiates epithelial cell apoptosis. CurrBiol 1999;9:1441—7.
153. Power C, Fanning N, Redmond HP. Cellular apoptosisand organ injury in sepsis: a review. Shock 2002;18:197—211.
154. Pryor JP, Reilly PM. Initial care of the patient with bluntpolytrauma. Clin Orthop 2004;422:30—6.
155. Rangel-Frausto MS, Pittet D, Costigan M, et al. The naturalhistory of the systemic inflammatory response syndrome(SIRS). A prospecitve study. JAMA 1995;273:117—23.
156. Rathmell JC, Thompson CB. The central effectors of celldeath in the immune system. Annu Rev Immunol 1999;17:781—828.
157. Regel G, Grotz M, Weltner T, et al. Pattern of organ failurefollowing severe trauma. Word J Surg 1996;20:422—9.
158. Regel G, Lobenhoffer P, Grotz M, et al. Treatment results ofpatients with multiple trauma: an analysis of 3, 406 casestreated between 1972 and 1991 at a German level I traumacenter. J Trauma 1995;38:70—8.
159. Rensing H, Bauer M. Multiple organ failure. Mechanisms,clinical manifestation and therapeutical strategies. Anaes-thesist 2001;50:819—41.
160. Rigby AC, Grant MA. Protein S: a conduit between antic-oagulation and inflammation. Crit Care Med 2004;32(Suppl.5):336—41.
161. Rivers E, Nguyen B, Havstad S, et al., Early Goal-DirectedTherapy Collaborative Group. Early goal-directed therapy inthe treatment of severe sepsis and septic shock. N Engl JMed 2001;345:1368—77.
162. Rolando N, Wade J, Davalos M, et al. The systemic inflam-matory response syndrome in acute liver failure. Hepatol-ogy 2000;32:734—9.
163. Rose S, Marzi I. Pathophysiology of polytrauma. ZentralblChir 1996;121:896—913.
164. Rotstein OD. Modeling the two-hit hypothesis for evaluatingstrategies to prevent organ injury after shock/resuscita-tion. J Trauma 2003;54(Suppl. 5):203—6.
165. Roumen RM, Redl H, Schlag G, et al. Inflammatory mediatorsin relation to the development of multiple organ failure inpatients after severe blunt trauma. Crit Care Med1995;23:474—80.
166. Roumen RMH, Hendriks T, van der Ven-Jongekrijg J. Cyto-kine patterns in patients after major vascular surgery,hemorrhagic shock, and severe blunt trauma: relation withsubsequent adult respiratory distress syndrome and multi-ple organ failure. Ann Surg 1993;6:769—76.
167. Saul TG, Ducker TB. Effect of intracranial pressure monitor-ing and aggressive treatment on mortality in severe headinjury. J Neurosurg 1982;56:498—503.
168. Sauaia A, Moore FA, Moore EE, et al. Epidemiology of traumadeaths: a reassessment. J Trauma 1995;38:185—93.
169. Schmidt OI, Infanger M, Heyde CE, et al. The role ofneuroinflammation in traumatic brain injury. Eur J Trauma2004;30:135—49.
170. Schoffel U, Bonnaire F, van Specht BU, Kuner EH. Monitoringthe response to injury. Injury 1991;22:377—82.
171. Schroder O, Laun RA, Held B, et al. Association of inter-leukin-10 promoter polymorphism with the incidenceof multiple organ dysfunction following major trauma:results of a prospective pilot study. Shock 2004;21(4):306—10.
172. Seekamp A, Jochum M, Ziegler M, et al. Cytokinesand adhesion molecules in elective and accidentaltrauma-related ischemia/reperfusion. J Trauma 1998;44:874—82.
173. Shackford SR, Mackersie RC, Davis JW, et al. Epidemiologyand pathology of traumatic deaths occurring at a level Itrauma center in a regionalized system: the importance ofsecondary brain injury. J Trauma 1989;29:1392—7.

708 M. Keel, O. Trentz
174. Shafi S, Kauder DR. Fluid resuscitation and blood replace-ment in patients with polytrauma. Clin Orthop2004;422:37—42.
175. Shohami E, Beit-Yannai E, Horowitz M, Kohen R. Oxidativestress in closed-head injury: brain antioxidant capacity asan indicator of functional outcome. J Cereb Blood FlowMetab 1997;17:1007—19.
176. Siegel JH, Gens DR, Mamantov T, et al. Effect of associatedinjuries and blood volume replacement on death, rehabili-tation needs, and disability in blunt traumatic brain injury.Crit Care Med 1991;19:1252—65.
177. Singer M, De Santis V, Vitale D, Jeffcoate W. Multiorganfailure is an adaptive, endocrine-mediate, metabolicresponse to overwhelming systemic inflammation. Lancet2004;364:545—8.
178. Skidgel RA, Gao XP, Brovkovych V, et al. Nitric oxide stimu-lates macrophage inflammatory protein-2 expression insepsis. J Immunol 2002;169:2093—101.
179. Smail N, Messiah A, Edouard A, et al. Role of systemicinflammatory response syndrome and infection in the occur-rence of early multiple organ dysfunction syndromefollowing severe trauma. Intensive Care Med 1995;21:813—816.
180. Smith JA. Neutrophils, host defense, and inflammation: adouble-edged sword. J Leuk Biol 1994;56:672—86.
181. Sosin DM, Sacks JJ, Smith SM. Head injury–—associateddeaths in the United States from 1979 to1986. JAMA1989;262:2251—5.
182. Stahel PF, Morganti-Kossmann MC, Kossmann T. The role ofthe complement system in traumatic brain injury. Brain ResRev 1998;27:243—56.
183. Stocker R, Bernays T, Kossmann T, Imhof HG. Monitoring andtreatment of acute head injury. In: Goris RJA, Trentz O,editors. The integrated approach to trauma care. Berlin,Heidelberg, New York: Springer-Verlag; 1995 . p. 196—200.
184. Stocker R, Burgi U. Controversies in nutrition of the criti-cally ill patients. In: Vincent JL, editor. Yearbook of inten-sive care and emergency medicine. Berlin, Heidelberg, NewYork: Springer-Verlag; 1999. p. 98—104.
185. Sugimoto K, Hirata M, Majima M, et al. Evidence for a role ofkallikrein—kinin system in patients with shock after blunttrauma. Am J Physiol 1998;274:1556—60.
186. Suliburk JW, Ware DN, Balogh Z, et al. Vacuum-assistedwound closure achieves early fascial closure of openabdomens after severe trauma. J Trauma 2003;55:1155—60.
187. Suter PM, Suter S, Girardin E, et al. High bronchoalveolarlevels of tumor necrosis factor and its inhibitors, interleu-kin-1, interferon, and elastase, in patients with adultrespiratory distress syndrome after trauma, shock, or sep-sis. Am Rev Respir Dis 1992;145:1016—22.
188. Talmor M, Hydo L, Barie PS. Relationship of systemic inflam-matory response syndrome to organ dysfunction, length ofstay, and mortality in critical surgical illness. Arch Surg1999;134:81—7.
189. Tanaka H, Ishikawa K, Nishino M, et al. Changes in granu-locyte colony-stimulating factor concentration in patientswith trauma and sepsis. J Trauma 1996;40:718—26.
190. Texereau J, Pene F, Chiche JD, et al. Importance ofhemostatic gene polymorphisms for susceptibility to andoutcome of severe sepsis. Crit Care Med 2004;32(Suppl. 5):313—319.
191. The Veterans Administration Systemic Sepsis CooperativeStudy Group. Effect of high-dose glucocorticoid therapy onmortality in patients with clinical signs of systemic sepsis. NEngl J Med 1987;317:659—65.
192. Till GO, Friedl HP, Ward PA. Lung injury and complementactivation: role of neutrophils and xanthine oxidase. FreeRadic Biol Med 1991;10:379—86.
193. Trentz O. Polytrauma: pathophysiology, priorities, andmanagement. In: Ruedi TP, Murphy WM, editors. AO prin-ciples of fracture management. Stuttgarg, New York:Thieme-Verlag; 2000. p. 661—73.
194. Van der Sluis CK, ten Duis HJ, Geertzen JH. Multiple injuries:an overview of the outcome. J Trauma 1995;38:681—6.
195. Van Griensen M, Krettek C, Pape HC. Immune reactions aftertrauma. Eur J Trauma 2003;29:181—92.
196. Velmahos GC, Jindal A, Chan L, et al. Prophylactic anti-biotics after severe trauma: more is not better. Int Surg2001;86:176—83.
197. Wahlstrom K, Bellingham J, Rodriguez JL, West MA. Inhibi-tory kappaBalpha control of nuclear factor-kappaB is dys-regulated in endotoxin tolerant macrophages. Shock1999;11:242—7.
198. Wang P, Wu P, Siegel MI, et al. Interleukin (IL)-10 inhibitsnuclear factor kB (NFkB) activation in human monocytes:IL-10 and IL-4 suppress cytokine synthesis by differentmechanisms. J Biol Chem 1995;270:9558—63.
199. Wang X, Mori T, Jung JC, et al. Secretion of matrix metallo-proteinase-2 and -9 after mechanical trauma injury in ratcortical cultures and involvement of MAP kinase. J Neuro-trauma 2002;19:615—25.
200. Wang JH, Redmond HP, Watson RW, Bouchier-Hayes D. Roleof lipopolysaccharide and tumor necrosis factor-alpha ininduction of hepatocyte necrosis. Am J Physiol 1995;269:G297—304.
201. Wanner GA, Keel M, Steckholzer U, et al. Relationshipbetween procalcitonin plasma levels and severity of injury,sepsis, organ failure, and mortality in injured patients. CritCare Med 2000;28:950—7.
202. Waydhas C, Nast-Kolb D, Trupka A, et al. Posttraumaticinflammatory response, secondary operations, and latemultiple organ failure. J Trauma 1996;40:624—30.
203. West MA, Heagy W. Endotoxin tolerance: a review. Crit CareMed 2002;30(Suppl. 1):S64—73.
204. Whicher JT, Evans SW. Acute phase proteins. Hosp Update1990;899—905.
205. Wichmann MW, Ayala A, Chaudry IH. Severe depression ofhost immune functions following closed-bone fracture, soft-tissue trauma, and haemorrhagic shock. Crit Care Med1998;26:1372—8.
206. Winterbourn CC, Buss IH, Chan TP, et al. Proteincarbonyl measurements show evidence of early oxidativestress in critically ill patients. Crit Care Med 2000;28:143—9.
207. Woiciechowsky C, Asadullah K, Nestler D, et al. Sympatheticactivation triggers systemic interleukin-10 release in immu-nodepression induced by brain injury. Nat Med 1998;4:808—13.
208. Woiciechowsky C, Schoning B, Lanksch WR, et al. Mecha-nisms of brain-mediated systemic anti-inflammatory syn-drome causing immunodepression. J Mol Med 1999;77:769—80.
209. Woolf PD. Hormonal responses to trauma. Cirt Care Med1992;20:216—26.
210. Yada-Langui MM, Coimbra R, Lancellotti C, et al. Hypertonicsaline and pentoxifylline prevent lung injury and bacterialtranslocation after hemorrhagic shock. Shock 2000;14:594—8.
211. Zilow G, Joka T, Obertacke U, et al. Generation of anaphy-latoxin C3a in plasma and bronchoalveolar lavage fluid intrauma patients at risk for the adult respiratory distresssyndrome. Crit Care Med 1992;20:468—73.

Pathophysiology of polytrauma 709
212. Zimmerman GA, McIntyre TM, Prescott SM, Stafforini DM.The platelet-activating factor signaling system and its reg-ulators in syndromes of inflammation and thrombosis. CritCare Med 2002;30(Suppl. 5):294—301.
213. Zweigner J, GrammHJ, Singer OC, et al. High concentrationsof lipopolysaccharide-binding protein in serum of patientswith severe sepsis or septic shock inhibit the lipopolysacchar-ide response in human monocytes. Blood 2001;98:3800—8.