Pathology of the Integumentary System Lecture 2people.upei.ca/hanna/skin2/skinL2-WebF17.pdf ·...
46
Pathology of the Integumentary System Lecture 2 Histopathologic Pattern Analysis (Web review) Paul Hanna Fall 2017
Transcript of Pathology of the Integumentary System Lecture 2people.upei.ca/hanna/skin2/skinL2-WebF17.pdf ·...

Pathology of the
Integumentary System
Lecture 2
Histopathologic Pattern Analysis
(Web review)
Paul Hanna Fall 2017
[For Information Only]
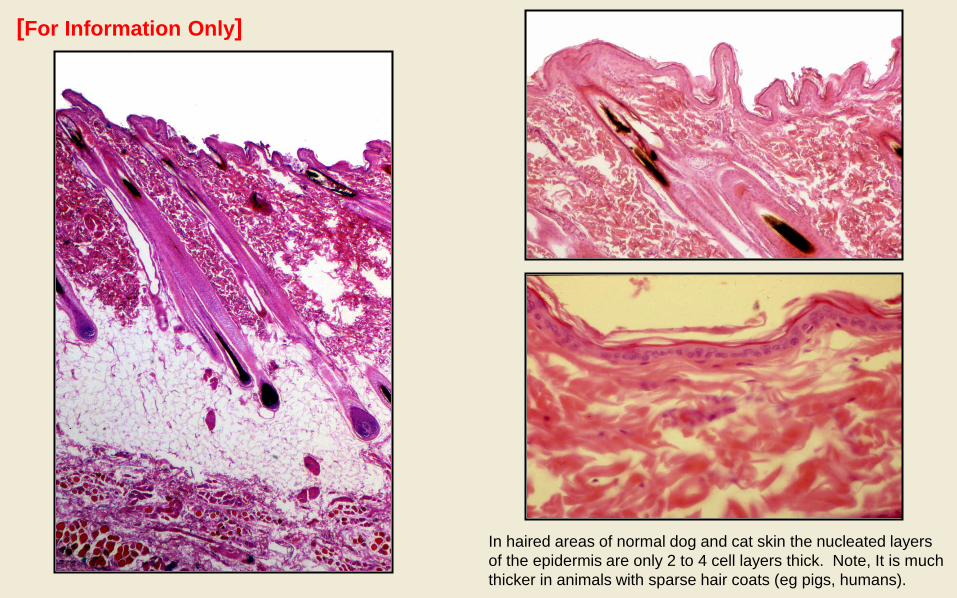
In haired areas of normal dog and cat skin the nucleated layers
of the epidermis are only 2 to 4 cell layers thick. Note, It is much
thicker in animals with sparse hair coats (eg pigs, humans).

Hyperkeratosis - increased thickness of stratum corneum;
ortho- (anuclear) or parakeratotic (nucleated)
Epidermal Changes
severe orthokeratotic hyperkeratosis in an alpaca with
congenital ichthyosis JAVMA 2013; 243:1701-3
parakeratotic hyperkeratosis in a dog with zinc-responsive
dermatosis.
[For Information Only]

Epidermal hyperplasia (acanthosis) - increased thickness of the noncornified epidermis.
a) Regular epidermal hyperplasia [For Information Only]

b) Irregular epidermal hyperplasia [For Information Only]

c) Papillated epidermal hyperplasia [For Information Only]

d) Pseudocarcinomatous epidermal hyperplasia [For Information Only]

Epidermal atrophy - decreased thickness of the noncornified epidermis
[For Information Only]

Intracellular edema
a) Hydropic (vacuolar) degeneration
[For Information Only]
hydropic degeneration of keratinocytes is characterized by a zone of cytoplasmic vacuolation immediately around nucleus

Intracellular edema
b) Ballooning degeneration
[For Information Only]
Ballooning degeneration of epidermal cells in Orf (parapox virus) infection

Intercellular edema (spongiosis) - accumulation of edema in the intercellular spaces
Spongiosis is characterized by the keratinocytes
being separated (pushed apart) by clear zones of
edema; note the intercellular bridges / “spines”
(desmosomes) of keratinocytes are prominent.
[For Information Only]
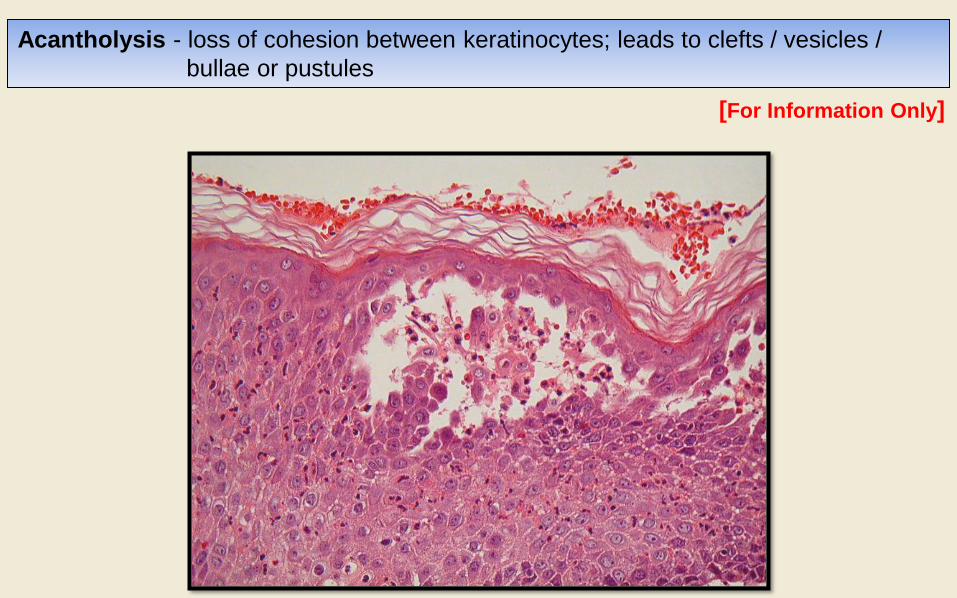
Acantholysis - loss of cohesion between keratinocytes; leads to clefts / vesicles /
bullae or pustules
[For Information Only]

Exocytosis - migration of inflammatory cells into the epidermis
[For Information Only]
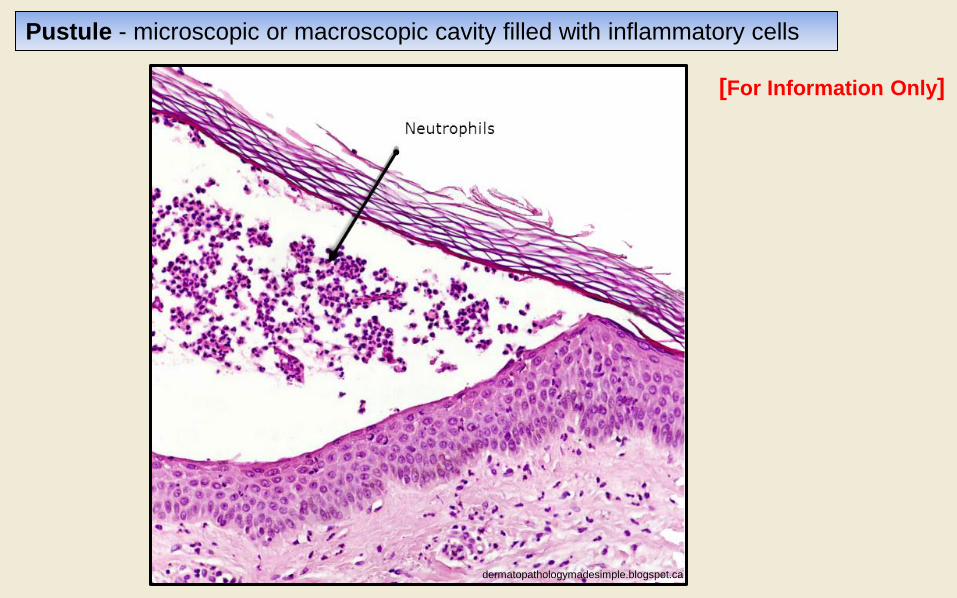
Pustule - microscopic or macroscopic cavity filled with inflammatory cells
dermatopathologymadesimple.blogspot.ca
[For Information Only]

Crust - surface accumulations of keratin, serum, inflammatory cells, debris, bacteria ...
[For Information Only]

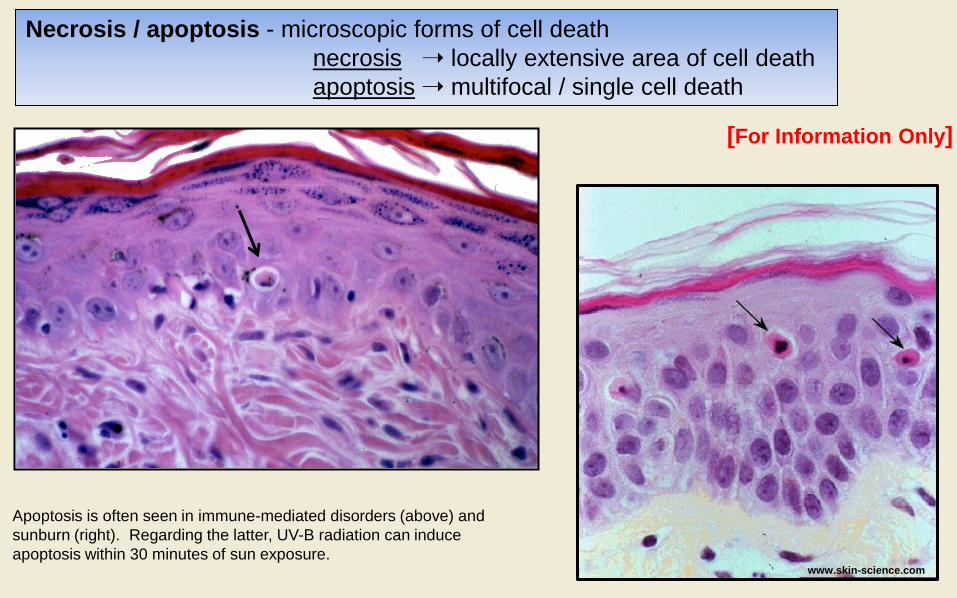
Necrosis / apoptosis - microscopic forms of cell death
necrosis locally extensive area of cell death
apoptosis multifocal / single cell death
[For Information Only]
Epidermal necrosis can be seen in
conditions such as burns (thermal or
chemical), ischemia / infarction and
some immune-mediated disorders
www.skin-science.com
[For Information Only]
Apoptosis is often seen in immune-mediated disorders (above) and
sunburn (right). Regarding the latter, UV-B radiation can induce
apoptosis within 30 minutes of sun exposure.
Necrosis / apoptosis - microscopic forms of cell death
necrosis locally extensive area of cell death
apoptosis multifocal / single cell death

Hyper - / hypopigmentation - increased or decreased amounts of melanin in the epidermis
[For Information Only]

Dermal edema - see widened spaces between dermal collagen &/or lymphatic dilation
Dermal Changes [For Information Only]

Collagen changes - including hyalinization, “degeneration”, mineralization, etc
[For Information Only]

[For Information Only]
Fibroplasia / fibrosis - formation and maturation of fibrous tissue, leading to
scarring (sclerosis).

[For Information Only]
Pigmentary incontinence - melanin granules free in the dermis or in dermal macrophages
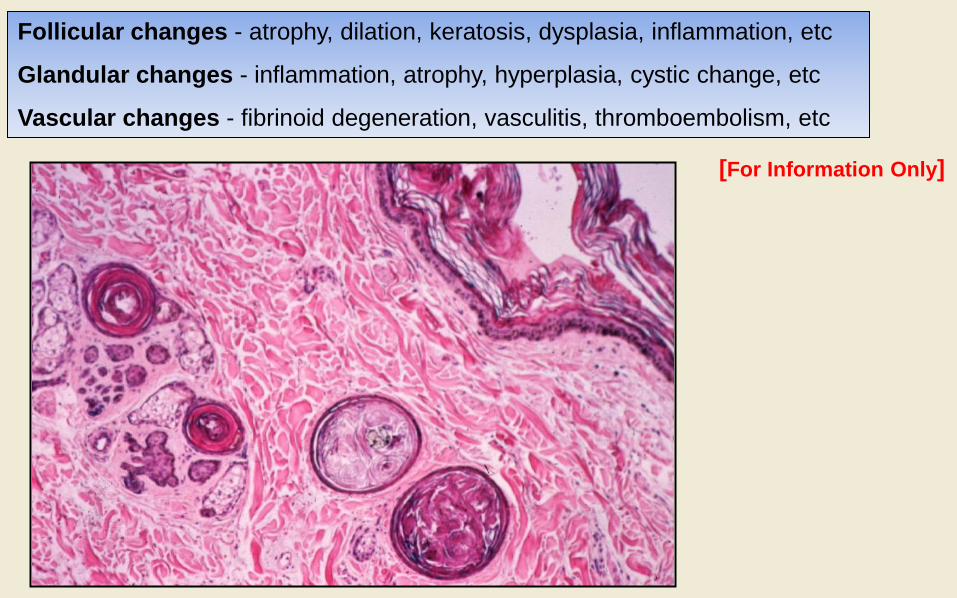
Follicular changes - atrophy, dilation, keratosis, dysplasia, inflammation, etc
Glandular changes - inflammation, atrophy, hyperplasia, cystic change, etc
Vascular changes - fibrinoid degeneration, vasculitis, thromboembolism, etc
[For Information Only]
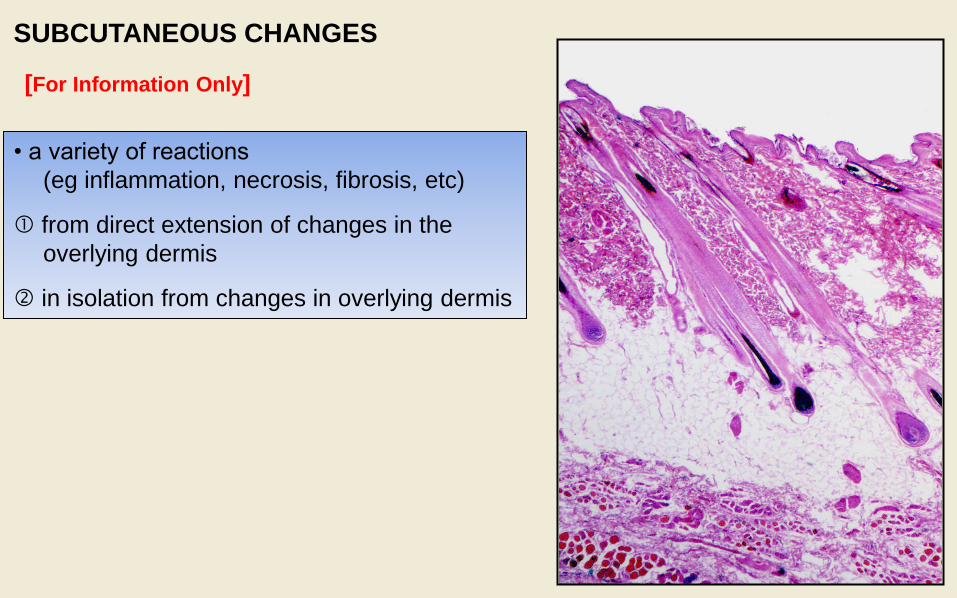
SUBCUTANEOUS CHANGES
• a variety of reactions
(eg inflammation, necrosis, fibrosis, etc)
from direct extension of changes in the
overlying dermis
in isolation from changes in overlying dermis
[For Information Only]


• dermatitis is not particularly useful term without qualification, since the skin
becomes inflamed in response to a myriad of causes
• pattern-analysis, at low magnification, relates inflammatory patterns to various
types of skin diseases
• details at higher magnification often allow for a specific diagnosis
HISTOPATHOLOGIC PATTERN-ANALYSIS

Normal
Normal skin – in the diagram the uniform lighter grey
appearance of the dermis is used to represent the uniformity
of the closely packed collagen fibers, while the darker grey
represents the uniformity of the epidermal layer.

1) PERIVASCULAR (INTERSTITIAL) DERMATITIS
• inflammatory reaction centred on the superficial and/or deep dermal vessels.
[note: the term interstitial dermatitis is often used when the inflammatory cells
are more widely dispersed than just surrounding the dermal blood vessels]
Perivascular (interstitial) dermatitis
Spongiotic perivascular (interstitial) dermatitis
Hyperplastic perivascular (interstitial) dermatitis

Perivascular (interstitial) dermatitis
• esp hypersensitivities.
note edema in the superficial dermis (ie “washed
out” appearance) and perivascular accumulation
of inflammatory cells.

Spongiotic perivascular (interstitial) dermatitis
• esp HS’s, contact dermatitis, ectoparasitism, viral, dermatophytosis, Malasseziasis, etc
Note: similar to perivascular / interstitial dermatitis with the
addition of epidermal spongiosis (ie intercellular edema).
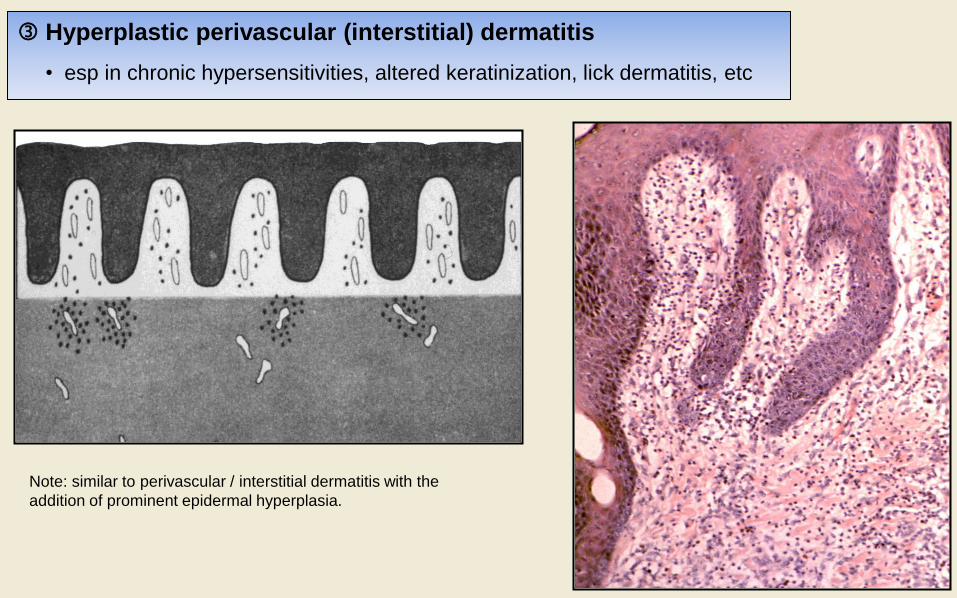
Hyperplastic perivascular (interstitial) dermatitis
• esp in chronic hypersensitivities, altered keratinization, lick dermatitis, etc
Note: similar to perivascular / interstitial dermatitis with the
addition of prominent epidermal hyperplasia.

2) INTERFACE DERMATITIS
• immune-mediated / autoimmune skin diseases, drug reactions, some viral infections, etc
Interface dermatitis – diagrams show obscuring of the dermoepidermal junction (ie interface) with hydropic
degeneration [left] and/or lichenoid infiltrate of inflammatory cells + hydropic degeneration [right]

3) VASCULITIS • seen with a variety of infections, immune mediated diseases, etc
Note, vasculitis denotes inflammation and damage of the
blood vessel wall; which is more obvious in the image above.

Nodular or multinodular dermatitis denotes discrete
cluster(s) of inflammatory cells within the dermis.
4) NODULAR AND DIFFUSE DERMATITIS
• esp traumatic implantation of foreign material / bacteria / fungi / protozoa
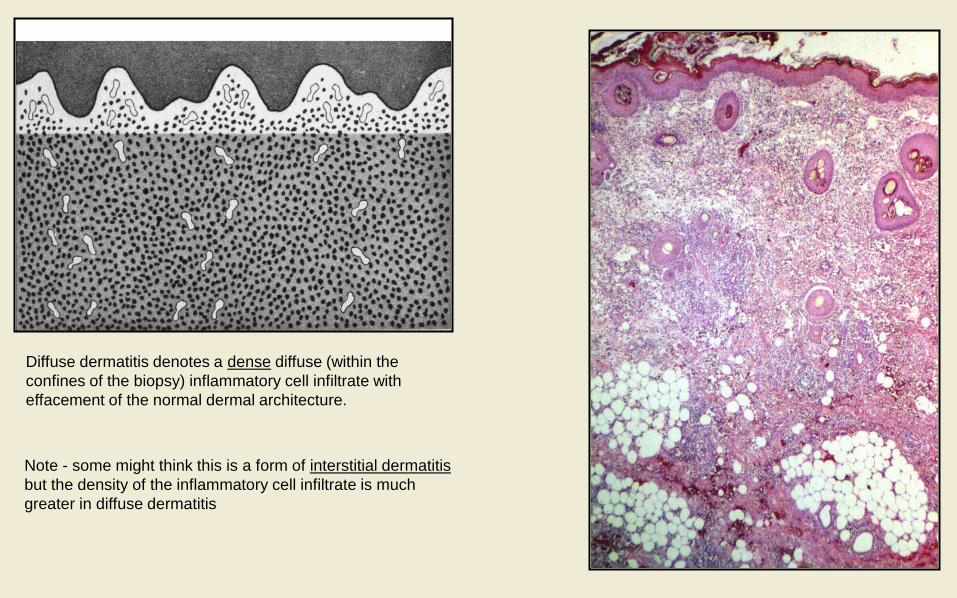
Diffuse dermatitis denotes a dense diffuse (within the
confines of the biopsy) inflammatory cell infiltrate with
effacement of the normal dermal architecture.
Note - some might think this is a form of interstitial dermatitis
but the density of the inflammatory cell infiltrate is much
greater in diffuse dermatitis
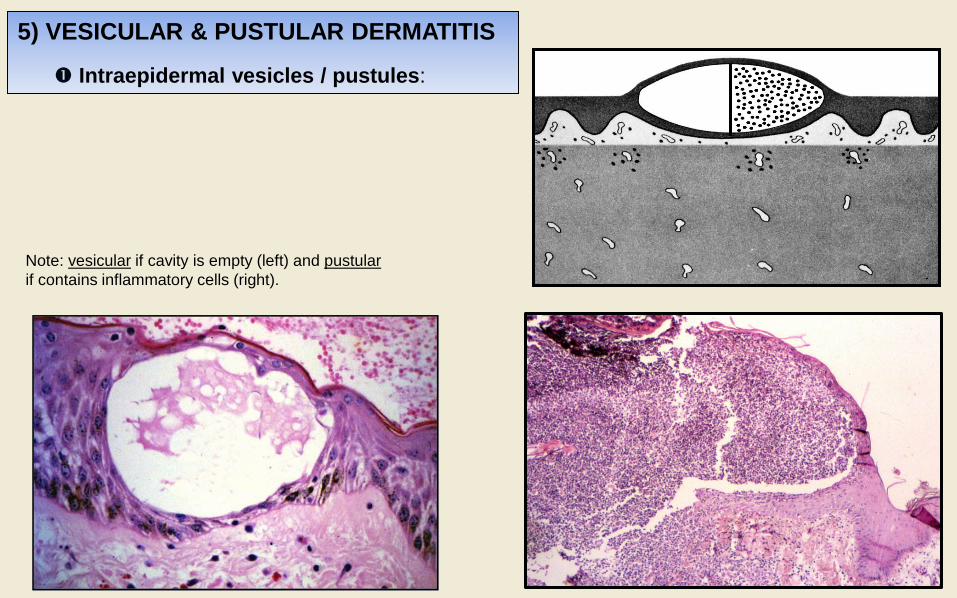
5) VESICULAR & PUSTULAR DERMATITIS
Intraepidermal vesicles / pustules:
Note: vesicular if cavity is empty (left) and pustular
if contains inflammatory cells (right).

a) acantholysis (eg neutrophilic enzymes, pemphigus Ab)
Normal Epidermis Leakage of neutrophil enzymes in
bacterial infections or Auto Ab’s (eg
pemphigus) damage desmosomal
adhesion molecules
Loss of cohesion between keratinocytes
results in intraepidermal vesicle /
pustule formation
Intraepidermal vesicles / pustules due to:

Normal Epidermis Ballooning degeneration of
keratinocytes due to viral
infection
Vesicle results from rupture &
coalescence of virally infected
(ballooning degenerate) cells
Intraepidermal vesicles / pustules due to:
b) coalescing ballooning degeneration in viral dermatitis
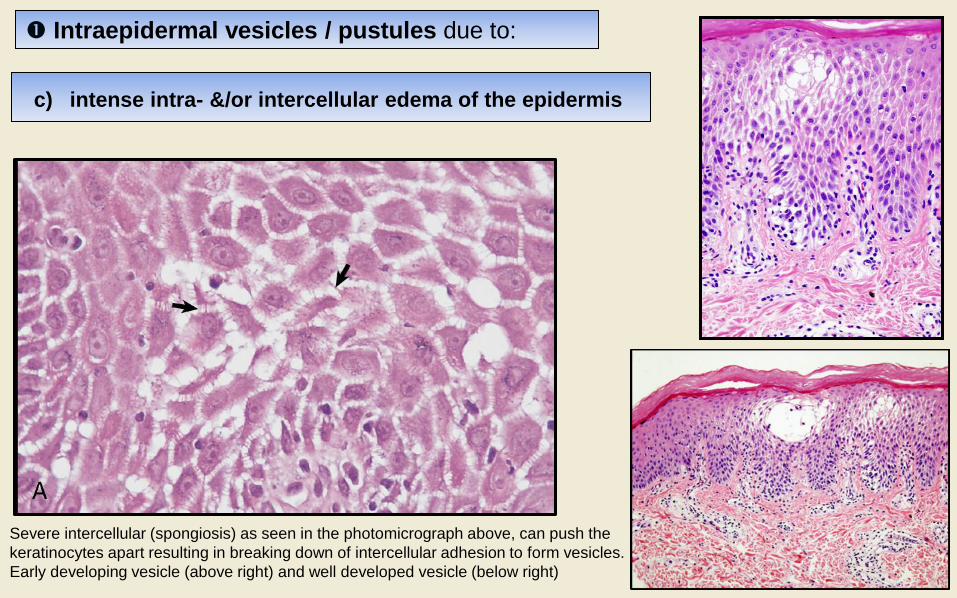
Intraepidermal vesicles / pustules due to:
c) intense intra- &/or intercellular edema of the epidermis
Severe intercellular (spongiosis) as seen in the photomicrograph above, can push the
keratinocytes apart resulting in breaking down of intercellular adhesion to form vesicles.
Early developing vesicle (above right) and well developed vesicle (below right)

5) VESICULAR & PUSTULAR DERMATITIS
Subepidermal vesicles / pustules
Note: vesicular if cavity is empty and pustular if
contains inflammatory cells.
Bullous pemphigoid showing subepidermal vesicle
a) genetic or autoimmune damage of hemidesmosome adhesion molecules
b) severe subepidermal edema and/or cellular infiltration damaging D/E junction
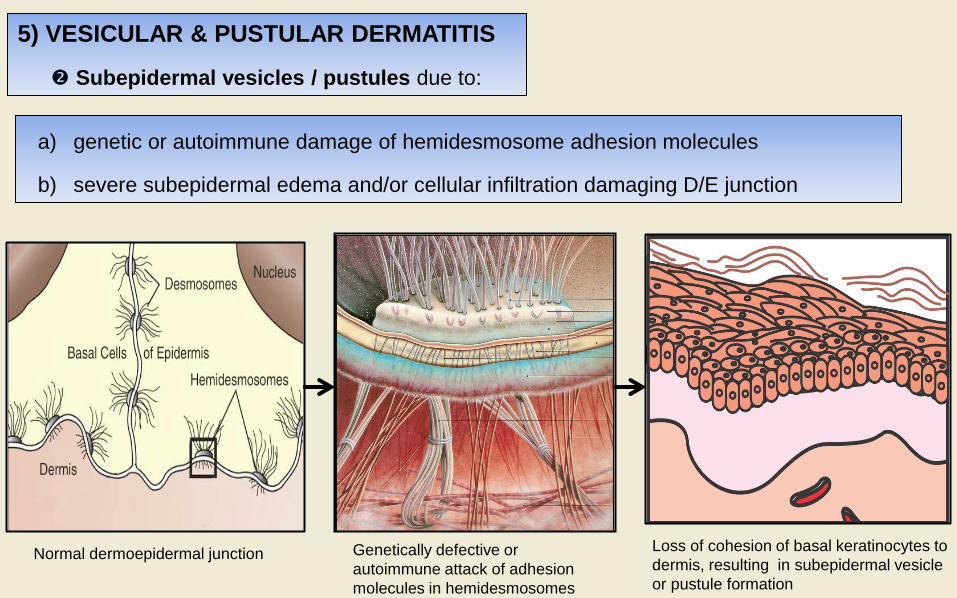
5) VESICULAR & PUSTULAR DERMATITIS
Subepidermal vesicles / pustules due to:
Normal dermoepidermal junction Genetically defective or
autoimmune attack of adhesion
molecules in hemidesmosomes
Loss of cohesion of basal keratinocytes to
dermis, resulting in subepidermal vesicle
or pustule formation

6) PERIFOLLICULITIS, FOLLICULITIS, FURUNCULOSIS
• especially due to bacteria (staph) or fungi (ringworm) or parasites (demodex)
Perifolliculitis – accumulation of
inflammatory cells surrounding hair
follicle.
Furunculosis – effacement / rupture of
the hair follicle due to intense
inflammation.
Folliculitis – accumulation of
inflammatory cells within the wall
&/or lumen of the hair follicle.

folliculitis furunculosis

7) PANNICULITIS
• often extension from nodular or diffuse dermatitis; nutritional, injection, idiopathic
Note: the inflammation in the subcutis can be lobular (in
fat) or septal (in connective tissue separating lobules),
but is mostly diffuse (ie involving both septa and lobules)
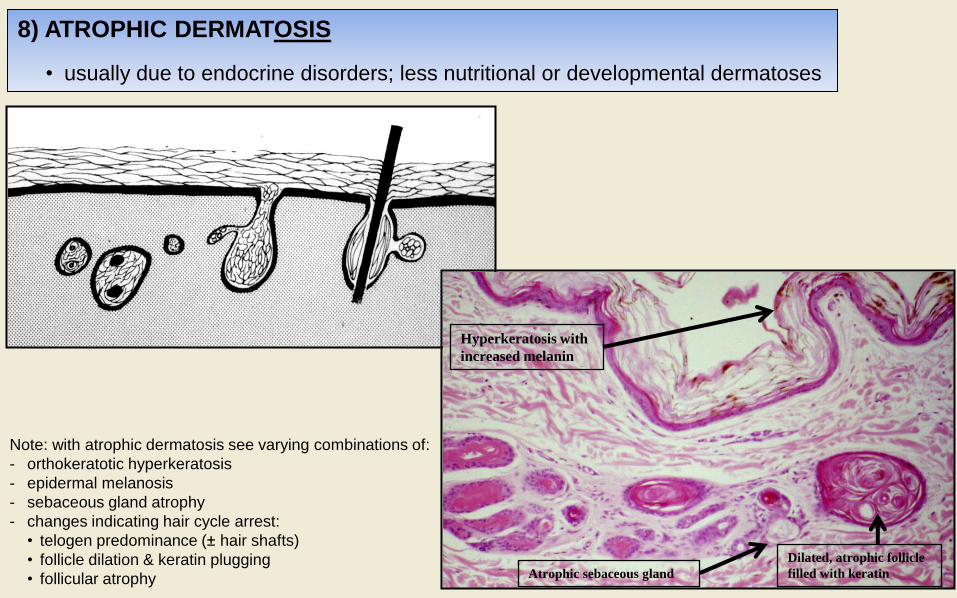
8) ATROPHIC DERMATOSIS
• usually due to endocrine disorders; less nutritional or developmental dermatoses
Note: with atrophic dermatosis see varying combinations of:
- orthokeratotic hyperkeratosis
- epidermal melanosis
- sebaceous gland atrophy
- changes indicating hair cycle arrest:
• telogen predominance (± hair shafts)
• follicle dilation & keratin plugging
• follicular atrophy
Hyperkeratosis with
increased melanin
Dilated, atrophic follicle
filled with keratin Atrophic sebaceous gland