
PARASITOLOGY DEPARTMENT University of Sumatera...
39
Ocular parasitiasis Nurfida Khairina Arrasyid PARASITOLOGY DEPARTMENT University of Sumatera Utara
Transcript of PARASITOLOGY DEPARTMENT University of Sumatera...

Ocular parasitiasis
Nurfida Khairina Arrasyid
PARASITOLOGY DEPARTMENT
University of Sumatera Utara

Ocular Helminthiasis
� Toxocara cani� Angiostrongylus cantonensis� Onchocerca volvulus� Onchocerca volvulus� Loa loa� Thelazia sp

Ocular toxocariasis cani
� Older children
� No history of pica
� Small dose of infection
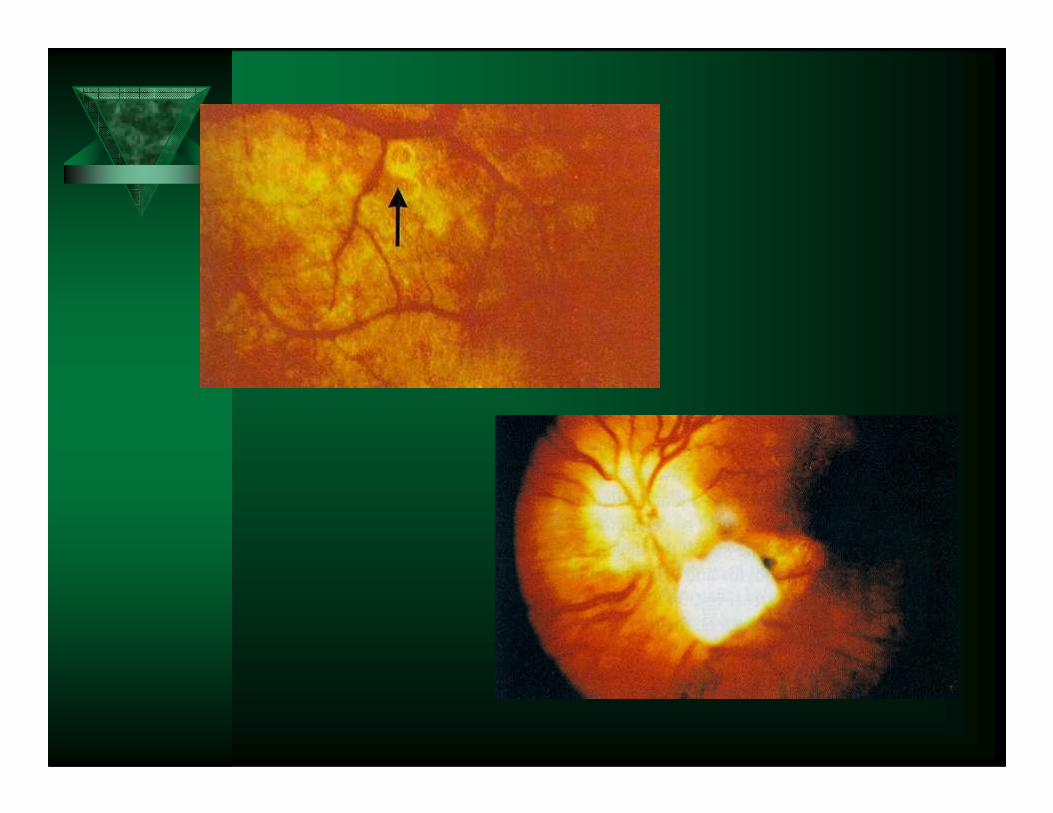
� Posterior painless lesion near optic disc
– granuloma
– asymptomatic
– visual defects
– unilateral loss of vision

PATHOGENESIS
� Larva in an eye cause chronic inflamation of the inner chamber or retina or provoke dangerous granulomas of the retina
This reactions can lead to blindness in the � This reactions can lead to blindness in the affected eye
� Ocular involvement has been reported in 245 patients with an average age of 7.5 years
Diagnosis Treatment
� Liver biopsy – granuloma
� Laser photocoagulation

Ocular angiostrongyliasis
� Defenitive host : rodent (Rattus norvegitusand Rattus rattus)
� Habitat : pulmonary artery of rodents
� Intermediate host : snail (Achatina, Pila)� Intermediate host : snail (Achatina, Pila)
� Distribution : Southeast Asia, India, Taiwan, China, Japan, Australia and Egypt

Mode of Human Infection
� Ingested 3rd stage larvae by
consuming intermediate host
(snail) or paratenic host (exp.
crabs, fresh water shrimp).
Ingested 3rd larvae from � Ingested 3rd larvae from
water which was
contaminated by dead
mollusc/snail, or vegetables
by secretions of mollusc
Patology & Symptoms
� Larvae in eye � Ocular angiostrongyliasis � blind
� Headache and stiff neck
� Vomiting
� Severe case : paresthesia and paralysis
Eosinophilic meningitis or eosinophilic meningoencephalitis
Diagnosis
� Anamnese � eating mollusc
� Clinical signs and symptoms
� Finding larvae (young adult worm) in
spinal fluid or other organs by surgery
� Serological test

Therapy
� Supportive
� Thiabendazole, Albendazole
Prevention
� Cooking all potential intermediate
and paratenic host before eat.

Ocular onchocerciasis
� Causative agent: Onchocerca volvulus
� Insect vector: Black flies, Simulium sp.Insect vector: Black flies, Simulium sp.
� Also known as “River blindness” –5% infected are blind (2 million)
� Distribution: Tropical Africa, Central America, spread to Arabian Peninsula.
Pathology/Pathogenesis
� Live microfilaria invade many parts of the eye, but here again they cause little reaction, their death leads to lessions
� Chronic inflamatory cells with eosinophils & neutrophils surround death Chronic inflamatory cells with eosinophils & neutrophils surround death worms, follow by fibroblast proliferation & chronic inflamatory infiltrates
� The most important cause of blindness is sclerosing keratitis a hardening inflamation of the cornea
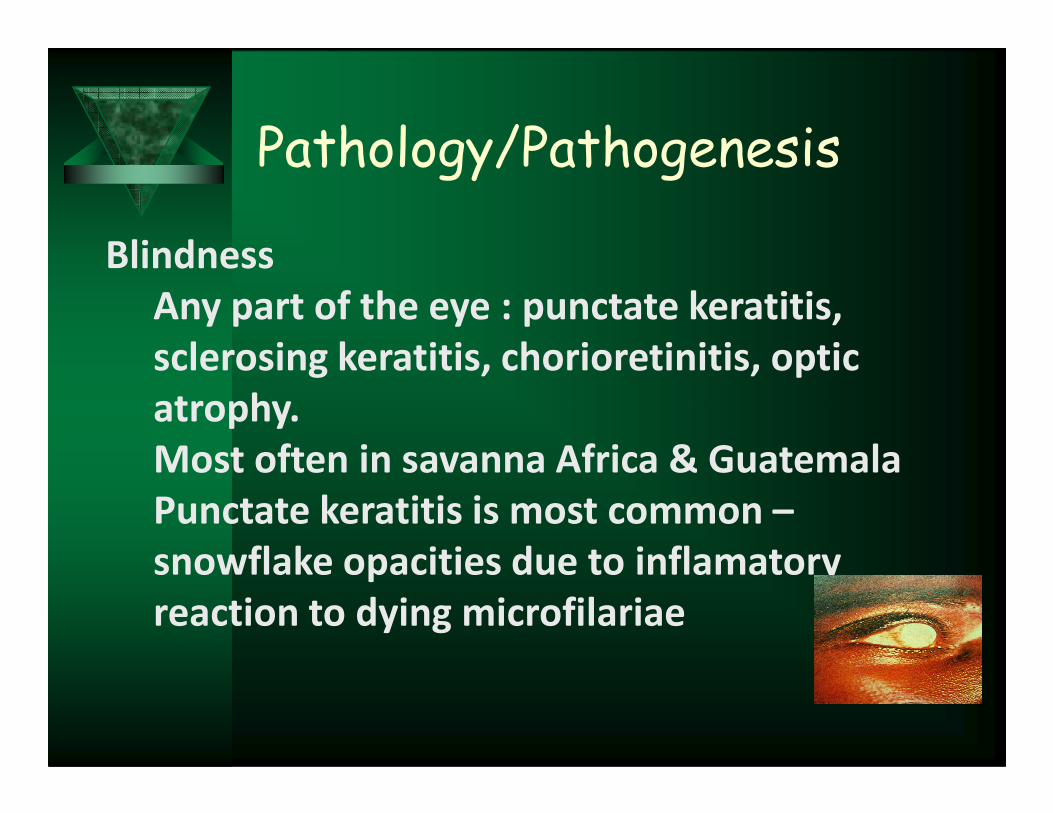
Pathology/Pathogenesis
Blindness
Any part of the eye : punctate keratitis,
sclerosing keratitis, chorioretinitis, optic
atrophy.atrophy.
Most often in savanna Africa & Guatemala
Punctate keratitis is most common –
snowflake opacities due to inflamatory
reaction to dying microfilariae

Diagnosis & Treatment
� Diagnosis– Slit-lamp examination– Serological method– Serological method– PCR has role in monitoring chemotherapy

Ocular loiasis
� Caused by the eye worm of Africa, Loa loa� Transmitted by mango flies, Chrysops sp.� Endemic only in rainforest areas of central and
west Africa – Nigeria, Cameroon, Zaire (Congo), west Africa – Nigeria, Cameroon, Zaire (Congo), Angola, Gabon, Chad & Sudan
� Mf in peripheral blood shows diurnal periodicity.� Mf has been shown in primate but has nocturnal
periodicity, probably a different species

� Occusianally adult worms migrate through the conjunctiva & cornea with swelling of the orbit
Pathology, Pathogenesis & Clinical manifestations

– Endemic patient
•Hypo-responsiveness
•90% positive for Mf
Pathology, Pathogenesis & Clinical manifestations
•90% positive for Mf
• Lower eosinophilia, parasite-specific IgG & lymphocyte proliferation
Nurfida Kh. Arrassyid

– Non-endemic population• Hyper-responsiveness
• Low positivity for Mf (10%)
• Higher level of eosinophilia (60-80%),
Pathology, Pathogenesis & Clinical manifestations
• Higher level of eosinophilia (60-80%), parasite-specific IgG & lymphocyte proliferation
• More severe & recurrent calabar swelling

Diagnosis & Treatment
� Diagnosis– Blood smear for Mf (mid-day sample)
– Biopsy– Biopsy
– Serological test (ELISA, IFA
� Treatment– DEC 8-10mg/kg in divided doses x 21 days
Ocular thelaziasis
Pathogenesis, Pathology & Symptomatology
� Thelazia produces damage to the tissues
associated with the eye.associated with the eye.
� Its presence in the conjunctival sac
provokes excess flow of lacrimal fluid.
� Its repeated migration across the corneal
conjunctiva irritates this layer & eventually
results in scarification & fibrous opacity of
the region

Pathogenesis, Pathology &
Symptomatology
� Paralysis of the muscles of the lower eyelid,
with ectropion, has been attributed to the
worms.
� The presence & movement of the parasites
in the conjunctival sac cause surprisingly
mild symptoms consisting of excessive
lacrimation, itching or pain.

Diagnosis & Treatment
Diagnosis :
� The presence of
creamy white
threaworm masses
Treatment :
Removal the worm with
forcepsthreaworm masses
coiled in the
conjunctival sac

OCULAR PROTOZOIASIS
Nurfida Khairina Arrasyid

Ocular protozoiosis
� Acanthamoeba sp
� Toxoplasma gondii
Ocular acanthamoebiasis
� Free living amoeba widely distributed in nature
� Facultative parasite of man and animal
� Causes infection :
1. CNS (Granulomatous Amebic
Encephalitis GAE)
2. Cornea (Keratitis)
3. Skin ulcers
Recent increase in the number of
cases of CNS infection as well as
cases of keratitiscases of keratitis
Problems with diagnosis and
effective treatment


Keratitis
• Inflammation of the cornea
• painful, vision threatening disease resulting
in blindness if untreatedin blindness if untreated
• painful eye, redness, photophobia
• infiltration of corneal epithelium leading to
ulceration, perineuritis, hypopyon
• very resistant to treatment resulting in tx
failure

•increasing no. of cases throughout the world
•related to contact lens wear (>80%)
•increasing usage of contact lenses but poor lens
hygienic care
•related to trauma (injury to the eyes by soil,
sand, contaminated water, mud splashing, foreign sand, contaminated water, mud splashing, foreign
bodies)
•progressive disease which resembles herpes
simplex

Risk factors
• Contact lens wear esp extended wear
• Trauma to the eye
• Use of home made saline• Use of home made saline
• Use of tap water to rinse lens
• Swimming while wearing CL
• Poor hygienic care of CL system

Diagnosis
• Hx of CL wear or injury to the eye
• Poor hygienic care of CL system
• Use of tap water or homemade saline
• Clinical presentation and finding of
perineuritisperineuritis
• Clinical spesimen is corneal scrapping or
biopsy which should be cultured onto NNA
overlay with E. coli
• Both trophozoite and cyst can be identified


• Other specimens include contact lens, CL
casing, CL saline and disinfectant, tap water
used to rinse lens
• The specimens should also be cultured for
Acanthamoeba using NNA overlay with E. Acanthamoeba using NNA overlay with E.
coli
• Examine under inverted microscope daily
until 14 days before a negative result is
confirmed

• Ocular toxoplasmosis is allegedly the
most common cause of posterior
uveitis in immunocompetent
Ocular toxoplasmosis
individuals.
• In most patients it is presumed to be
a reactivated congenital condition,
but instances of acquired infection
have also been reported.

�A white, sharp-edged but irregular neuroretinal
inflammatory focus is usually seen, frequently in
association with an old scar.
Pathogenesis, Pathology,
Symptoms
association with an old scar.
�In recurrent ocular toxoplasmosis, acute
inflammation may be restricted to a discrete
zone at the margin of an old scar.
Pathogenesis, Pathology,
Symptoms
� Chronic active or relapsing infections of
retinal cells by tachyzoites causes blinded
spot & extensive infection of the central spot & extensive infection of the central
macular area, which may lead to blindness
� Cysts & cyst rupture in the retina can also
lead to blindness
� Pathologic findings:
– necrotizing retinitis and uveitis

Signs , Symptoms,
Diagnosis & Treatment
� Acute retinochoroiditis include blurred
vission, scotoma,photophobia and pain
Pathology : coagulative necrosis of the � Pathology : coagulative necrosis of the
retina with inflamatory infiltrates & loose
granulomas in the choroid
� Funduscopic : vitritis


REFERENCE
Beaver, P.C., Jung, R.C. 1984. Clinical parasitology. 9th ed. Philadelphia, Lea & Febringer. p.292-294; 345
Gillespie, S., Pearson, R.D. 2001. Principle and practice of clinical parasitology.John Wiley & Son Ltd. p.124
Miyazaki, I. 1991. An Miyazaki, I. 1991. An illustrated book of helminthic zoonosis. Tokyo : International Medical Foundation of Japan, p. 347-353; 366; 428-434
Schimidt, G.D., Roberts, L.S. 2005. Foundation of parasitology. 7th ed. Mc Graw Hill. p. 118-119;136-137; 427-428; 458; 468-471












![sss.2. histologi 1 eye.ppt [Read-Only]ocw.usu.ac.id/course/download/1110000121-special-senses...Eye Eye Anatomy Anatomy External (Accesory) 1. Eyelids (palpebrae) 2. Conjunctiva 3.](https://static.fdocuments.in/doc/165x107/614ad43412c9616cbc69ab49/sss2-histologi-1-eyeppt-read-onlyocwusuacidcoursedownload1110000121-special-senses.jpg)



