
Paraquat Poisoning Case Report · 2014. 2. 26. · 10/8: paraquat (B) 2.32 PPM, Cr 0.72, Na 143, K...
37
Paraquat (巴拉刈) Poisoning Case Report Chi-Ling Lin, 18 FEB, 2014 Department of pharmacy, Chang Gung Memorial Hospital at Chiayi 1
Transcript of Paraquat Poisoning Case Report · 2014. 2. 26. · 10/8: paraquat (B) 2.32 PPM, Cr 0.72, Na 143, K...

Paraquat (巴拉刈) Poisoning Case Report
Chi-Ling Lin, 18 FEB, 2014
Department of pharmacy, Chang Gung Memorial Hospital at Chiayi
1

Outline
1. Case presentation
2. Paraquat poisoning
1) Toxicology
2) Laboratory monitoring
3) Management
3. Clinical trials
4. Discussion
5. Conclusion
2

Case Presentation
• Chief complaint:
Suicide with paraquat this afternoon
• Present Illness:
This 45 year-old male patient had history of alcohol consumption and psychiatry disorders. This time, he drank about over 10ml of paraquat which mixed with alcohol (about 300ml) in this afternoon. He was found persistent vomiting by his family, and was sent to ER then. There was no dyspnea, no fever, with clear conscious status. At ER, NG irrigation and charcoal was given. Urine paraquat test was done and revealed over 50ppm. He was then admitted to our MICU for further management. 3

Past History • 1.Unknown psyciatry disorder
• 2.Right ring finger and little finger crushing injury with traumatic amputation status post Microsurgical replantation on 20100413
• 3.Right replanted ring finger gangran change status post amputation on 20100423
• 4.Right middle finger laceration post wound repair on 20100413
• 5.Alcohol withdraw syndrome
• 6.L-spine HIVD s/p several years ago at 台南奇美醫院
• 7. Allergy (-), smoking +, alcohol + 4
Physical Examination
• T:37.6/℃ P:114/min R:17/min BR:133/91/mmHg
• 身高:173 體重:68
• GENERAL APPEARANCE: ill- looking
• CONSCIOUSNESS: Clear, E 4 V 5 M 6
• HEENT: Oral cavity : Intact oral mucosa
• CHEST: Breath pattern: smooth, No USE OF accessory muscles
Breathing sound:bilateral clear, No wheezing,No crackles
• SKIN: Skin intact , No wound
5

Laboratory Findings 血液 10/4
PM 5:24 生化 PM
5:24
WBC 7.1 Sugar 89
RBC 4.71 Creatinine 0.73
Hb 14.8 ALT/GPT 35
HCT 45.1 Na 149
PLT 172 K 3.8
Seg. 57.8 Alcohol 257.3
Lymphocyte 36.0 Cholinesterase 8432
檢體:U Paraquat (U) PPM >50(10/04)
Impression: Paraquat intoxication, alcoholism
6
Paraquat Poisoning
• Introduction
• Toxicology
• Clinical features
• PE & Lab.
• Management
• Initial resuscitation
• Gastrointestinal decontamination
• Hemoperfusion
• Anti-inflammatory & immunosuppressive therapy
• Anti-oxidant therapy 7

巴拉刈簡介
8

巴拉刈簡介
• 巴拉刈(Paraquat, 百草枯) 1 ‘-dimethyl-4,4’bipyriIium dichloride)是一種藍綠色、無特殊氣味或略帶阿摩尼亞味的除草劑。
• 產品包括克蕪蹤、速草淨、可樂松、全草滅、青草滅等。
• 巴拉刈有很高的致死率,口服極少量未稀釋的巴拉刈溶液(約10 ml)即可對人體造成非常嚴重的傷害。
9

Severity in Paraquat Poisoning
Severity in Paraquat Poisoning (SIPP) = Paraquat concentration (mg/L) X time since poisoning (hour) Score <10 -- Survival
10

Toxicology
11

12

臨床表現 • 服入少於7.5 ml的20%濃縮液(20 mg/kg)只會產生輕
微中毒,包括嘔吐、腹瀉以及短暫肺腎功能障礙。
• 7.5~15 ml (20~40 mg/kg)會造成中至重度的中毒,通常會在2~6日內導致全身性的器官毒性,其中以腎臟和肺臟為主。腎毒性主要傷害近曲小管,腎衰竭發展相當迅速,幾個小時到幾天內就可能發生。
• 肺部病變可以分兩個階段: 1 ~3天的急性肺泡炎以及接下來的肺部纖維化。病人一開始通常會有3~7天的呼吸障礙,之後會因逐步纖維化與嚴重缺氧,最多在5週後進展至死亡。
• 15ml 以上的20% 濃縮液(40mg/kg)則是致命的劑量,會導致猛暴性器官衰竭,包括肺水腫、心臟、腎和肝衰竭以及腦水腫、昏迷等。這些患者通常呈現缺氧、休克和代謝性酸中毒。絕大部份都在數小時到幾天內就會死亡。
13

診斷與實驗室檢查
• 藉由病史詢問以及理學檢查,包括服入藍綠色液體、隨同帶來醫院的殘餘農藥瓶、洗胃出現藍綠色液體、口腔出現不明原因之潰瘍等。
• 確定診斷需進行定性與定量之檢測。尿液定性檢測是把10 mL待測尿液加入2 mL試劑(1 0 mL 1N NaOH+0.1 mg sodium dithionite需檢測前才
泡製) ,濃度1 mg/mL (1ppm)以上,於白色背景下觀察會呈現藍色反應。
• 定量的檢測方式包括氣相色層分析法和高壓液相色層分析法(Gas chromatography and
• high pressure liquid chromatography)與放射免疫分析法(Radioimmunoassay) 。這些檢驗也是良好預後的指標。
14

Chest X-ray
British Journal of Clinical Pharmacology Volume 72, Issue 5, pages 745-757, 11 OCT 2011 DOI: 10.1111/j.1365-2125.2011.04026.x http://onlinelibrary.wiley.com/doi/10.1111/j.1365-2125.2011.04026.x/full#f3
15
Chest radiograph demonstrating diffuse alveolar shadowing of a patient 7days after ingestion of paraquat

High resolution CT scan of chest demonstrating bilateral pulmonary fibrosis 11 days after paraquat poisoning


巴拉刈中毒處置
18

Treatment Recommendation
19

Supportive Care Summary
20

Summary of Clinical Studies
21

HP-CVVH vs HP
CP + MP + DEX
Thiol antioxidant
Vitamin C
Vitamin E
22

Glucocorticoid with cyclophosphamide for paraquat-induced lung fibrosis
23

Glucocorticoid with cyclophosphamide for paraquat-induced lung fibrosis
24

Objective: A novel anti-inflammatory method to treat severe paraquat-poisoned patients
Design: Randomized controlled trial
Patient: Twenty-three paraquat-poisoned patients with >50% and <90% predictive mortality assessed by plasma paraquat levels were assigned to control and study groups at a proportion of 1:2.
Measurements and Main Results: We measured patient mortality during the study period. The mortality rate (85.7%, six of seven) of the control group was higher than that of the study group (31.3%, five of 16; p .0272).
initial pulse therapy methylprednisolone (1 g/day for 3days) and cyclophosphamide (15 mg/kg/day for 2 days), followed by dexamethasone 20 mg/day until PaO2 was >11.5 kPa (80 mm Hg) and repeated pulse if PaO2 < 60 mmHg

10/4 SOAP S
• 10/14自述喝巴拉松與酒半罐 just now
• Persist greenish vomitus
O
• Consciousness : E4V5M6, CXR: mild pulmonary congestion
• Paraquat (U) >50 PPM, alcohol 257.3 mg/dL
A
• Paraquat poisoning
• Alcoholism
P
• NG tube, charcoal decontamination, follow plasma paraquat
• Hemoperfusion, IVF (D5S 1000cc+ Vit B 4cc run 80cc/hr), Pulse oximeter, EKG MONITOR, Cyclophosphamide and methylprednisolone
26

Hemoperfusion .Hemoperfusion Order .Dialyzer: Active Charcoal .Duration: 8 Hrs .Vascular access: femoral catheter puncture .Blood flow: 250 ~ 300ml .Ultrafiltration: 0 kg .ACT: 250~300 sec, check F/S Q2H .Recheck urine paraquet level about 4 Hrs later after hemoperfusion
27

[Medication for paraquet intoxication] A. Cyclophosphamide 1 gm + D5W 100ml IVF QD x 2 days B. Methylprednisolone 1 gm + D5W 100ml IVF QD x 3 days C. Then Dexamethasone (5mg/ml/amp) 1 amp IVF q8h x 11 days (4th to 14th day)
1st day PaO2 70.8 mmHg 4th day PaO2 80.9 mmHg 10/19: dexamethasone PO, reduced dose gradually to 0.25mg qd (10/28)
28

10/12: T-bilirubin 3.2, AST 86, ALT 51, Cr 2.93, Na 149, K 5.4
Jaundice, r/o sepsis related
Abd. Echo: parenchymal liver disease, normal biliary tree
10/22: T-bil 1.9, D-bil 0.4
Neither renal or liver is the usual mode of death.
No long-term effects have been reported.
Disease Progression Acute renal injury
10/8 Urine retention, on Foley
T35.8℃P106R18, BP 175/107
10/8: paraquat (B) 2.32 PPM, Cr 0.72, Na 143, K 3.7
10/11: BUN 104.0, Cr 3.23, Na 149, K 3.9 10/28 Cr 1.09
AKI, RIFLE-F, suspected paraquat intoxication related
4-days after paraquat inestion
Acute tubular necrosis or volume depletion
Abnormal liver function
29
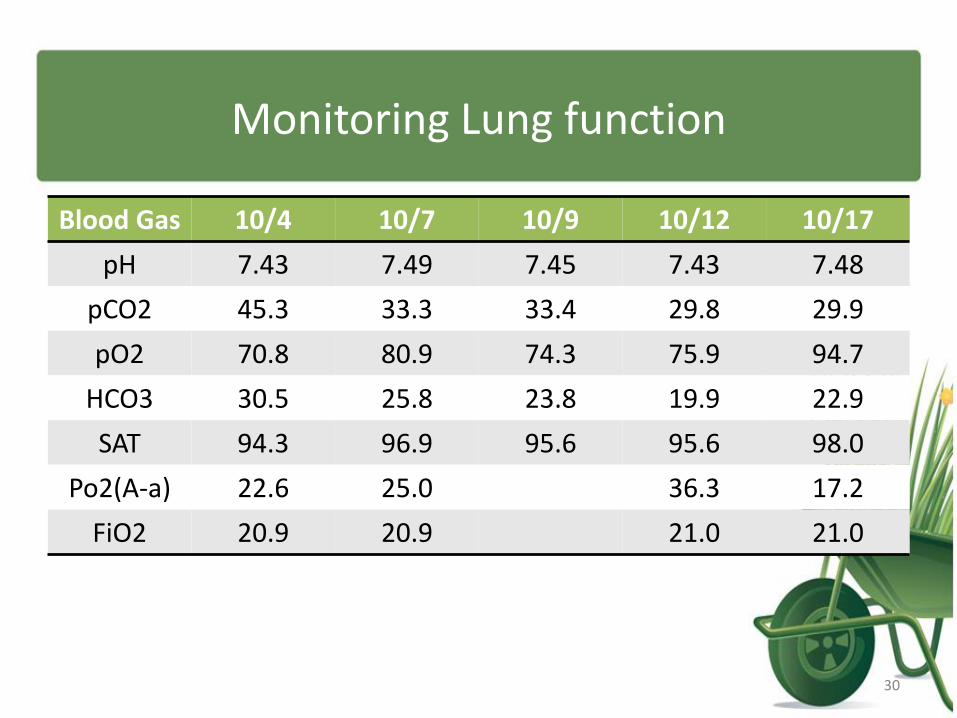
Monitoring Lung function
Blood Gas 10/4 10/7 10/9 10/12 10/17
pH 7.43 7.49 7.45 7.43 7.48
pCO2 45.3 33.3 33.4 29.8 29.9
pO2 70.8 80.9 74.3 75.9 94.7
HCO3 30.5 25.8 23.8 19.9 22.9
SAT 94.3 96.9 95.6 95.6 98.0
Po2(A-a) 22.6 25.0 36.3 17.2
FiO2 20.9 20.9 21.0 21.0
30

Medication Record
31

Problem: Febrile Neutropenia
10/11 Fever
Smooth breath pattern
Intermittent irritability
Tachycardia & tachypnea
T 38.3℃ P 122 R20 BP 178/90
10/11 WBC 2600, ANC 2288
10/14 WBC 1800, ANC 1350,
Hb 10.6, PLT 174
B/C: Enterob. Cloacae
CXR: mild infiltration
1. Ceftazidime was changed to piperacillin/tazobactam~10/21
2. Adjusting dose due to AKI
3. Complete 10~14 day course
Febrile neutropenia ?
(ANC<500?)
Sepsis, one week after Endoxan therapy
SOAP
32

Problem: Steroid-induced myopathy
10/15 Smooth breath pattern
Irritability, limbs twitching, general tremor
Can’t rise up hand and leg
Can’t sitting up with rigidness
T 35.1℃P 107 R24 BP146/106
E4V5M6
Babinski sign: negative
Brain MRI,EEG: negative
CPK: 54, in normal range
1. Hold quetiapine
2. IV form steroid was shifted to oral and tapered gradually
3. Aggressive rehab program
1. Quetiapine induced EPS, dyskinesia
2. Glucocorticoid related myopathy
SOAP
33

Steroids related myopathy
•
•

Summary • A paraquat-poisoned case report, he was survived.
• Pulse therapy with methylprednisolone and cyclophosphamide: efficacy & toxicity.
• The patient had renal and liver toxicity. Fortunately, lung toxicity was not observed during hospital period.
• Neutropenia with sepsis caused by cyclophosphamide. Myopathy caused by steroids.
• Paraquat (B) 2.32 → < 0.01 ppm
• Paraquat (U) > 50 ppm → < 5 ppm
35
參考資料
• JL L et al. Repeated pulse of methylprednisolone and cyclophosphamide with continuous dexamethasone therapy for patients with severe paraquat poisoning. Crit Care Med 2006;34:368-73.
• JL L et al. Improved survival in severe paraquat poisoning with repeated pulse therapy of cyclophosphamide and steroids. Intensive Care Med 2011;37:1006-13.
• Indika B. Gawarammana & Nicholas A. Buckley. Medical management of paraquat ingestion. Br J Clin Pharmacol 2011;72:745-57.
• 蔣文芳, 詹正雄, 陳金順 巴拉測中毒及治療 腎臟與透析:民國102年25卷3期
• 蔡文仁, 洪培豪, 潘吉豐, 吳志仁, 陳逸洲 , 陳漢湘 巴拉刈中毒的治療新進展 內科學誌 2013;24:48-63.
36
謝謝聆聽!
37


















