Tumors of nose and paranasal sinus dr.sithanandhakumar -13.06.16

E
C
Pp
A
a
Fb
I
Rtipot
1d
uropean Annals of Otorhinolaryngology, Head and Neck diseases (2013) 130, 26—29
Available online at
www.sciencedirect.com
ASE REPORT
aranasal sinus rhabdomyosarcoma: A rare tumor ofoor prognosis
. El Sanharawia, B. Coulibalyb, J.-P. Bessedea, K. Aubrya,∗
Service d’oto-rhinolaryngologie et chirurgie cervico-faciale, CHU de Limoges, 2, avenue Martin-Luther-King, 87000 Limoges,ranceService d’anatomo-pathologie, CHU de Limoges, 2, avenue Martin-Luther-King, 87000 Limoges, France
KEYWORDSParanasal sinuses;Rhabdomyosarcoma;Epistaxis;Exophthalmia;Ophthalmoplegia
SummaryIntroduction: Rhabdomyosarcoma (RMS) is a rare sarcoma, in which paranasal sinus locationsare exceptional in adults.Case report: We report a case of ethmoid metastatic RMS in a 48-year-old patient, discoveredin connection with recurrent epistaxis associated with exophthalmia and ophthalmoplegia. Thetumor was inoperable and chemotherapy based on adriamycin was initiated. The course was,however, marked by rapid worsening of symptoms and the patient’s death.
Discussion: Paranasal sinus RMS shows no specific clinical signs, and diagnosis is mainly basedon immunohistochemical analysis. The association of surgery and chemo-radiotherapy is theoptimal attitude, but surgical resection is often impossible due to local extension. Prognosis inadults is poor.© 2012 Elsevier Masson SAS. All rights reserved.C
Atfieoti
ntroduction
habdomyosarcoma (RMS) is a tumor of the conjunctiveissue, found more frequently and with better prognosisn children than adults. ENT forms are not unusual, butaranasal sinus locations are exceptional. We report a casef adult evolved ethmoid RMS, and discuss the characteris-ics, diagnosis and treatment of such tumors.
∗ Corresponding author.E-mail address: [email protected] (K. Aubry).
usewaaht
879-7296/$ – see front matter © 2012 Elsevier Masson SAS. All rights reoi:10.1016/j.anorl.2012.07.002
ase report
48-year-old man was referred to ENT for recurrent epis-axis. Brain and facial sinus CT found 30 × 25 mm tissularlling of the left anterior and medial ethmoid cells, withthmoid and papyraceous lamina bone lysis without intra-rbital extension. Biological assessment found anemia andhrombopenia. A myelogram was therefore taken, whichndicated massive metastatic medullary invasion. Biopsies,nder general anesthesia, proved highly hemorrhagic. Sub-equent recurrent epistaxis required platelet transfusionvery two days; very rapid onset of left exophthalmiaas associated with ptosis, superior palpebral edema
nd ophthalmoplegia. Contrast-enhanced cervico-thoraco-bdomino-pelvic CT showed no secondary pulmonary orepatic locations. MRI found tumoral extension towardhe frontal sinus, frontal cortex and left intra-orbitalserved.

Paranasal sinus rhabdomyosarcoma: A rare tumor of poor prognosis 27
ced sscle
tipcmi
D
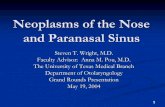
Figure 1 Brain MRI (horizontal T1-weighted gadolinium-enhanextension, exerting a mass effect on the right medial rectus mu
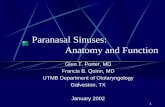
region (Fig. 1). 18-fluoro-desoxy-glucose positron emis-sion tomography (18FDG-PET) found hypermetabolic cervicallymph-node sites and diffuse osteo-medullary infiltration(Fig. 2). Definitive anatomopathologic examination diag-nosed grade-3 alveolar RMS on the Fédération Nationale desCentres de Lutte Contre le Cancer (FNCLCC) classification.Immunohistochemistry was positive for anti-desmin, anti-NCAM (neural cell adhesion molecule) and anti-myogeninantibodies, and negative for anti-caldesmon antibodies
(Fig. 3). Fluorescence in situ hybridization (FISH) analy-sis found FKHR gene rearrangement. A multidisciplinaryteam meeting decided, given the tumoral extension, on ini-tial adriamycin-based chemotherapy associated to regularRtw
Figure 2 18FDG-PET. A. Horizontal, sagittal and frontal slices in Clesion with bone lysis areas. B. Scintigraphic images, showing diffuseright: non-corrected attenuation MIP.
lices). A. Left ethmoid tumoral syndrome with left intra-orbital. B. Left frontal lobe tumoral invasion.
ransfusion and neutrophil growth factor injection. Afternitial improvement in general health status and disap-earance of the epistaxis, there was rapid deterioration ofonsciousness, due to onset of left frontal intraparenchy-atous cerebral hematoma; the patient died 5 weeks after
nitiation of chemotherapy.
iscussion
MS is a rare malignant tumor, originating in the conjunc-ive and derivative tissue. It is especially rare in adults,hereas it is the most frequent form of soft-tissue tumor
T paired to scintigraphy, showing infiltration via the skull-base osteo-medullary infiltration. Left: corrected attenuation MIP;
28 A. El Sanharawi et al.
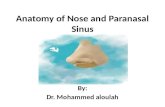
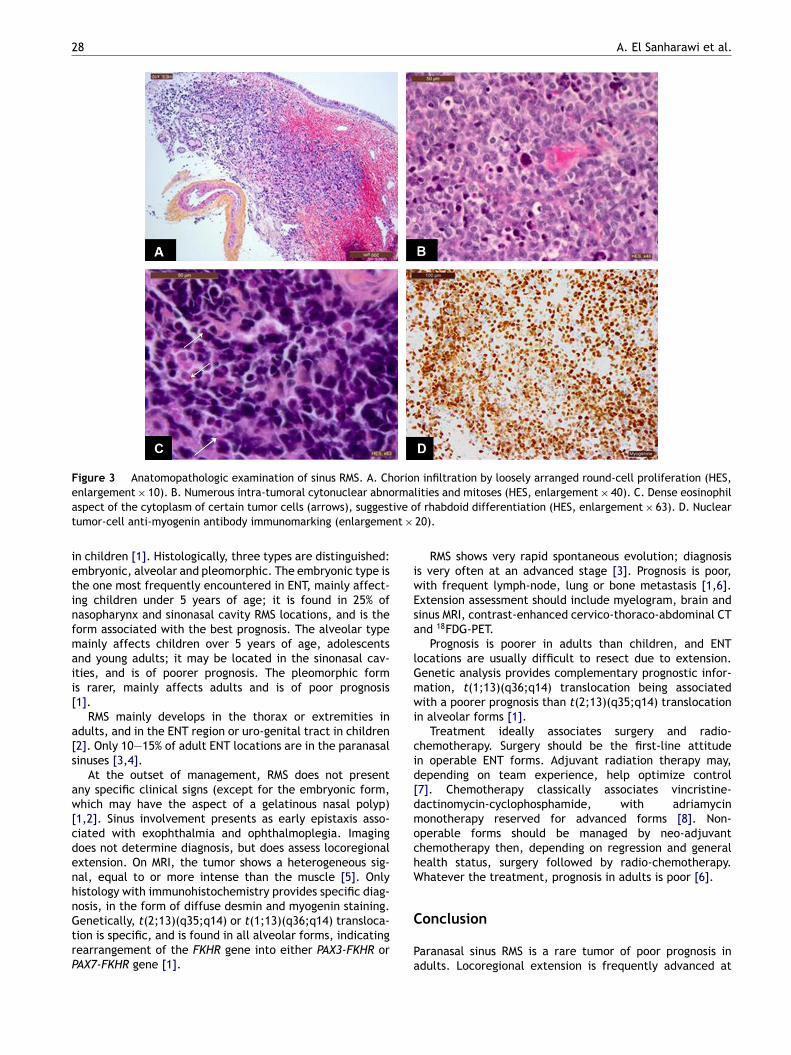
Figure 3 Anatomopathologic examination of sinus RMS. A. Chorion infiltration by loosely arranged round-cell proliferation (HES,enlargement × 10). B. Numerous intra-tumoral cytonuclear abnormalities and mitoses (HES, enlargement × 40). C. Dense eosinophila ive ot nt ×
ietinfmaii[
a[s
aw[cdenhnGtrP
iwEsa
lGmwi
cid[dmochW
spect of the cytoplasm of certain tumor cells (arrows), suggestumor-cell anti-myogenin antibody immunomarking (enlargeme
n children [1]. Histologically, three types are distinguished:mbryonic, alveolar and pleomorphic. The embryonic type ishe one most frequently encountered in ENT, mainly affect-ng children under 5 years of age; it is found in 25% ofasopharynx and sinonasal cavity RMS locations, and is theorm associated with the best prognosis. The alveolar typeainly affects children over 5 years of age, adolescents
nd young adults; it may be located in the sinonasal cav-ties, and is of poorer prognosis. The pleomorphic forms rarer, mainly affects adults and is of poor prognosis1].
RMS mainly develops in the thorax or extremities indults, and in the ENT region or uro-genital tract in children2]. Only 10—15% of adult ENT locations are in the paranasalinuses [3,4].
At the outset of management, RMS does not presentny specific clinical signs (except for the embryonic form,hich may have the aspect of a gelatinous nasal polyp)
1,2]. Sinus involvement presents as early epistaxis asso-iated with exophthalmia and ophthalmoplegia. Imagingoes not determine diagnosis, but does assess locoregionalxtension. On MRI, the tumor shows a heterogeneous sig-al, equal to or more intense than the muscle [5]. Onlyistology with immunohistochemistry provides specific diag-osis, in the form of diffuse desmin and myogenin staining.
enetically, t(2;13)(q35;q14) or t(1;13)(q36;q14) transloca-ion is specific, and is found in all alveolar forms, indicatingearrangement of the FKHR gene into either PAX3-FKHR orAX7-FKHR gene [1].C
Pa
f rhabdoid differentiation (HES, enlargement × 63). D. Nuclear20).
RMS shows very rapid spontaneous evolution; diagnosiss very often at an advanced stage [3]. Prognosis is poor,ith frequent lymph-node, lung or bone metastasis [1,6].xtension assessment should include myelogram, brain andinus MRI, contrast-enhanced cervico-thoraco-abdominal CTnd 18FDG-PET.
Prognosis is poorer in adults than children, and ENTocations are usually difficult to resect due to extension.enetic analysis provides complementary prognostic infor-ation, t(1;13)(q36;q14) translocation being associatedith a poorer prognosis than t(2;13)(q35;q14) translocation
n alveolar forms [1].Treatment ideally associates surgery and radio-
hemotherapy. Surgery should be the first-line attituden operable ENT forms. Adjuvant radiation therapy may,epending on team experience, help optimize control7]. Chemotherapy classically associates vincristine-actinomycin-cyclophosphamide, with adriamycinonotherapy reserved for advanced forms [8]. Non-
perable forms should be managed by neo-adjuvanthemotherapy then, depending on regression and generalealth status, surgery followed by radio-chemotherapy.hatever the treatment, prognosis in adults is poor [6].
onclusion
aranasal sinus RMS is a rare tumor of poor prognosis indults. Locoregional extension is frequently advanced at

ogno
[
[
[
[
[
Paranasal sinus rhabdomyosarcoma: A rare tumor of poor pr
diagnosis, limiting treatment options and worsening progno-sis. Surgery followed by radio-chemotherapy is the attitudeof choice in locally advanced and metastatic forms.
Disclosure of interest
The authors declare that they have no conflicts of interestconcerning this article
References
[1] Casiraghi O, Lefevre M. Undifferentiated malignant round celltumors of the sinonasal tract and nasopharynx. Ann Pathol2009;29:296—312.
[2] Agamanolis DP, Dasu S, Krill Jr CE. Tumors of skeletal muscle.Hum Pathol 1986;17:778—95.
[3] Chen SC, Bee YS, Lin MC, et al. Extensive alveolar-typeparanasal sinus and orbit rhabdomyosarcoma with intracranial
sis 29
invasion treated successfully. J Chin Med Assoc 2011;74:140—3.
4] Callender TA, Weber RS, Janjan N, et al. Rhabdomyosarcomaof the nose and paranasal sinuses in adults and children.Otolaryngol Head Neck Surg 1995;112:252—7.
5] Legendre BW, Nelson BL. Alveolar rhabdomyosarcomaof the paranasal sinuses. Head Neck Pathol 2008;2:302—4.
6] Moon HS, Kwon SW, Lee JH. A case of alveolar rhabdomyosar-coma of the ethmoid sinus invading the orbit in an adult. KoreanJ Ophthalmol 2006;20:70—5.
7] Donaldson SS, Anderson JR. Rhabdomyosarcoma: many sim-ilarities, a few philosophical differences. J Clin Oncol2005;23:2586—7.
8] Burke M, Anderson JR, Kao SC, et al. Assessment of responseto induction therapy and its influence on 5-year failure-free
survival in group III rhabdomyosarcoma: the Intergroup Rhab-domyosarcoma Study-IV experience — a report from the SoftTissue Sarcoma Committee of the Children’s Oncology Group.J Clin Oncol 2007;25:4909—13.