Panoramic Radiographic Detection of Systemic Disease · Maxillofacial Radiology, Professor of...
9
Volume 4, Issue 3 US $6.00 Editor: Allan G. Farman, BDS, PhD (odont.), DSc (odont.), Diplomate of the American Board of Oral and Maxillofacial Radiology, Professor of Radiology and Imaging Sciences, Department of Surgical and Hospital Dentistry, The University of Louisville School of Dentistry, Louisville, KY. Contributor: Dr. C.J. Nortjé, BChD, PhD, DSc, Professor of Oral and Maxillofacial Radiology, The University of the Western Cape, South Africa, President of the International Association of DentoMaxilloFacial Radiology. Featured Article: Panoramic Radiographic Detection of Systemic Disease In The Recent Literature: Osteoporosis Radiation-associated Meningioma Learning Objectives: Learn through examples how to review panoramic radiographs to screen for early detection of systemic diseases. Learn how to observe and detect features of systemic diseases when they produce changes in panoramic radiographs. Understand the limitations of panoramic radiography in detecting systemic diseases. For the purposes of this report, “systemic disease” will be interpreted as conditions that are spread out within the body rather than localized strictly to the tissues of the oral cavity. Since it would take many volumes to review all such conditions, the intent of this issue of Panoramic Imaging News is to review a few examples of conditions where initial panoramic radiographic findings Panoramic Radiographic Detection of Systemic Disease By Dr. Allan G. Farman in collaboration with Dr. C. J. Nortjé granular appearance of bone in the skull [2]. Osteoporosis can lead to pain, especially in the lower back. It can also result in pathologic fracture, loss of physical stature, and severe kyphosis. Radiologic features of osteoporo- sis in the jaws (Fig. 1) include relative radiolucency of both jaws and reduced definition of the cortices. The accuracy with which panoramic radiographs can be used to assess the likelihood of a person having osteoporosis is still in debate, with evidence being divided, rather than polarized for or against. Fig. 1: Osteoporosis – Cropped panoramic image shows a relative radiolucency of both jaws with reduced definition of the cortices. 1.1. Evidence supporting panoramic radiographs to screen for osteoporo- sis: In 1991, Benson et al. defined a radiomorphometric index of mandibular cortical bone mass, the panoramic mandibular index (PMI) [4]. Differences in the index in a population of 353 adult subjects, equally divided by sex, age (30 through 79), and racial group (Black, Hispanic, White), were evalu- ated with respect to side, racial group, suggested widespread disease of significance enough to affect the quality of life and longevity of the patient. The possibility of detecting carotid calcifications, indicative of cardiovascular disease – the leading cause of death in the US population – was previously addressed in Volume 1, Issue 2 (2001); hence, that topic is not repeated here. 1. Osteoporosis Osteoporosis results in excessive bone porosity and fragility. It is the most common metabolic disease and presents a major public health problem among the elderly, especially amongst postmenopausal Caucasian and Asian women [1]. It is also found in sedentary or immobilized individuals, and in patients on long-term steroid therapy [2]. The asymptomatic progres- sion of osteoporosis, in conjunction with the possibility of catastrophic disability, makes this disorder a major public health priority [3]. Cardinal radiographic features of osteoporosis in the skeleton as a whole include generalized osteopenia that is often most prominent in the spine, thinning and accentuation of the bone cortices, and accentuation of primary and loss of secondary trabeculation. Ancillary radiologic features include spontaneous, atraumatic fracture, especially of the spine, wrist, hip or ribs, basilar invagination in the skull and
-
Upload
nguyenphuc -
Category
Documents
-
view
221 -
download
1
Transcript of Panoramic Radiographic Detection of Systemic Disease · Maxillofacial Radiology, Professor of...
Volume 4, Issue 3 US $6.00
Editor:Allan G. Farman, BDS, PhD (odont.),DSc (odont.), Diplomate of theAmerican Board of Oral andMaxillofacial Radiology, Professor ofRadiology and Imaging Sciences,Department of Surgical and HospitalDentistry, The University ofLouisville School of Dentistry,Louisville, KY.
Contributor:Dr. C.J. Nortjé, BChD, PhD, DSc,Professor of Oral and MaxillofacialRadiology, The University of theWestern Cape, South Africa, Presidentof the International Association ofDentoMaxilloFacial Radiology.
Featured Article:Panoramic Radiographic Detectionof Systemic Disease
In The Recent Literature:Osteoporosis
Radiation-associated Meningioma
Learning Objectives:Learn through examples how toreview panoramic radiographs toscreen for early detection of systemicdiseases.
Learn how to observe and detectfeatures of systemic diseases whenthey produce changes in panoramicradiographs.
Understand the limitations ofpanoramic radiography in detectingsystemic diseases.
For the purposes of this report,“systemic disease” will be interpreted asconditions that are spread out within thebody rather than localized strictly to thetissues of the oral cavity. Since it wouldtake many volumes to review all suchconditions, the intent of this issue ofPanoramic Imaging News is to review afew examples of conditions where initialpanoramic radiographic findings
Panoramic RadiographicDetection of Systemic DiseaseBy Dr. Allan G. Farman incollaboration with Dr. C. J. Nortjé
granular appearance of bone in theskull [2]. Osteoporosis can lead to pain,especially in the lower back. It can alsoresult in pathologic fracture, loss ofphysical stature, and severe kyphosis.
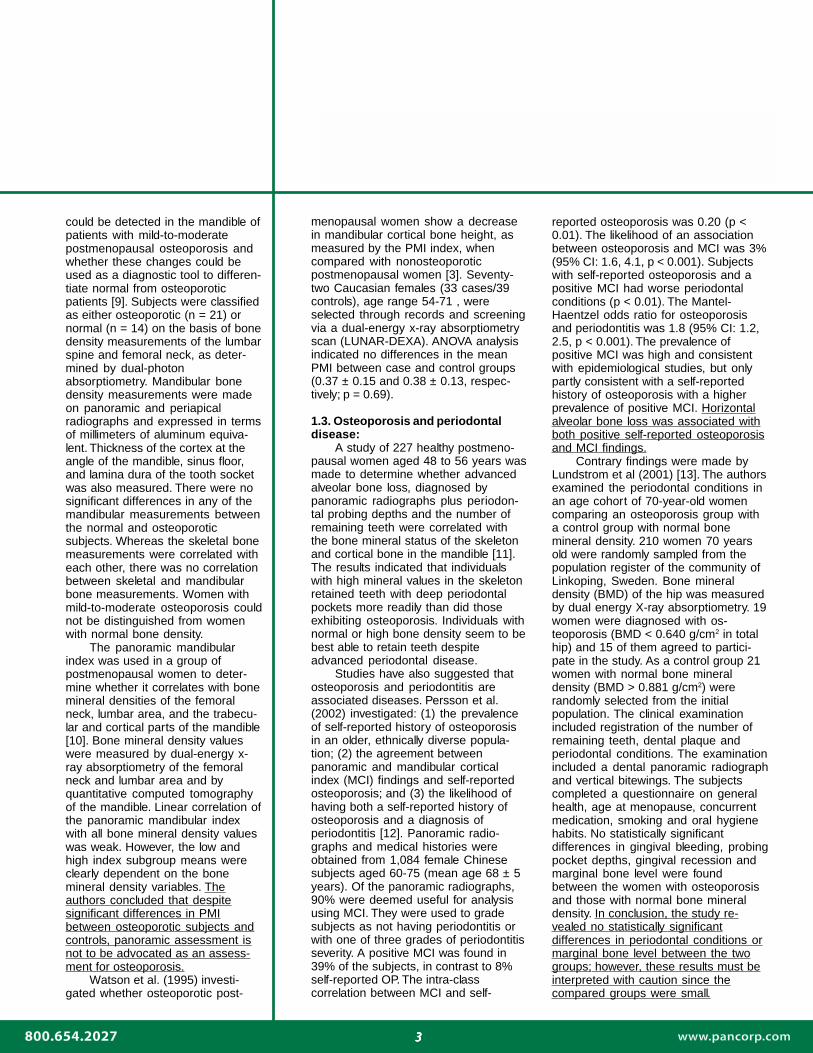
Radiologic features of osteoporo-sis in the jaws (Fig. 1) include relativeradiolucency of both jaws and reduceddefinition of the cortices. The accuracywith which panoramic radiographs canbe used to assess the likelihood of aperson having osteoporosis is still indebate, with evidence being divided,rather than polarized for or against.
Fig. 1: Osteoporosis – Cropped panoramicimage shows a relative radiolucency of bothjaws with reduced definition of the cortices.
1.1. Evidence supporting panoramicradiographs to screen for osteoporo-sis:
In 1991, Benson et al. defined aradiomorphometric index of mandibularcortical bone mass, the panoramicmandibular index (PMI) [4]. Differencesin the index in a population of 353 adultsubjects, equally divided by sex, age(30 through 79), and racial group(Black, Hispanic, White), were evalu-ated with respect to side, racial group,
suggested widespread disease ofsignificance enough to affect thequality of life and longevity of thepatient. The possibility of detectingcarotid calcifications, indicative ofcardiovascular disease – theleading cause of death in the USpopulation – was previouslyaddressed in Volume 1, Issue 2(2001); hence, that topic is notrepeated here.
1. OsteoporosisOsteoporosis results in
excessive bone porosity andfragility. It is the most commonmetabolic disease and presents amajor public health problemamong the elderly, especiallyamongst postmenopausalCaucasian and Asian women [1]. Itis also found in sedentary orimmobilized individuals, and inpatients on long-term steroidtherapy [2]. The asymptomatic progres-sion of osteoporosis, in conjunction withthe possibility of catastrophic disability,makes this disorder a major publichealth priority [3].
Cardinal radiographic features ofosteoporosis in the skeleton as a wholeinclude generalized osteopenia that isoften most prominent in the spine,thinning and accentuation of the bonecortices, and accentuation of primaryand loss of secondary trabeculation.Ancillary radiologic features includespontaneous, atraumatic fracture,especially of the spine, wrist, hip or ribs,basilar invagination in the skull and

22222
“ The researchers concluded that panoramic radiography can be used to assessthe likelihood of osteoporosis.”
sex, age, and combinations of thesevariables. Blacks were found to have agreater mean PMI than Hispanics orWhites, who were demographicallysimilar. Age-related changes comparingyounger and older age groups withineach sex and racial group indicated asignificant decrease in mean PMI withincreasing age in Black and Hispanicwomen. The mean PMI in white menincreased with advancing age.
A retrospective investigation wascarried out to determine the strength ofassociation of spinal bone density andthe density of selected mandibular sitesas determined from panoramic radio-graphs [1]. Panoramic films of knownlow bone density and high bone densityin women between the ages of 50 and75 were evaluated. These radiographswere randomized and then converted todigital images for density analysis.Significant differences were foundbetween the groups at the 95thpercentile level. Hence, according to thisstudy, blinded observers should be ableto differentiate between persons of highand low bone density using panoramicradiographs.
The relationship between oralsigns and osteoporosis was investi-gated to assess the possibility of usingthis as an indicator of osteoporosis.Taguchi et al. (1995) studied 64postmenopausal women aged 50 to 70.Osteoporotic signs consisted of thoracicspine fracture as demonstrated onlateral chest radiographs. Oral signswere the number of teeth present,mandibular cortical width, alveolar boneresorption, and the morphologicclassification of the inferior cortex onpanoramic radiographs. The number ofteeth present (N) was highly signifi-cantly related to the probability ofthoracic spine fracture and was used toderive the probability equation for thepresence of thoracic spine fracture:probability value = 1/(1 + e-z), Z =18.68-0.29 age -0.27N. A probabilityvalue > 0.5 suggested the possibility ofthoracic spine fracture. It was concludedthat this equation combined withpanoramic radiographic findings couldserve as a simple and useful tool fordentists to assess the possibility oflatent osteoporosis [5].
The usefulness of width andmorphology of the inferior cortex of the
mandible on panoramic radiographswas evaluated in the diagnosis ofpostmenopausal osteoporosis [6]. Thewidth and morphology of the mandibu-lar inferior cortex on panoramicradiographs were compared withtrabecular bone mineral density (TBMD)of the 3rd lumbar vertebrae (L3)measured by dual energy quantitativecomputed tomography in 29 premeno-pausal and 95 postmenopausalwomen. There was a significantnegative correlation between the width(Kendall’s tau = -0.36, p < 0.001) andmorphology (Kendall’s tau = -0.49, p <0.001) of the mandibular inferior cortexand the L3 TBMD. Regression analysisshowed that significant linear relation-ships were observed between the L3TBMD and age (p < 0.001), corticalwidth (p < 0.05), morphology (p < 0.05),controlling body mass index, number ofteeth present, and menopausal status(R2 = 0.42). The researchers concludedthat panoramic radiography can beused to assess the likelihood ofosteoporosis.
The value of clinical and radio-graphic indices in the diagnosis ofpatients with low skeletal bone masswas investigated among 135 healthyperimenopausal women, aged 45-55attending for regular dental treatment[7]. Bone mineral density was measuredfor the spine and femoral neck, usingdual energy X-ray absorptiometry. Eachpatient’s osteoporosis status wascalculated according to the WHO criteriafor Caucasian women. Each patientreceived a dental panoramic radio-graph, and the width of the inferiormandibular cortex (mental index, (MI))was measured. The body mass index(BMI) and simple calculated osteoporo-sis risk estimation (SCORE) indiceswere calculated. The SCORE index wasa significant factor in predicting lowbone mass, with the weight of thepatient being the only significantconstituent factor. MI, BMI and SCOREindices were significantly correlatedwith skeletal bone density. When thelogistic regression model included MI,BMI, and SCORE indices, all threevariables were significant predictors oflow skeletal bone mass. A thinning ofthe mandibular cortices (MI < 3 mm) in anormal perimenopausal female wasassociated with low skeletal bone mass.
If, in addition, the patient isunderweight (BMI is below 20kg/m2) or has a high SCORE index (=6) then this assessed increase inrisk was found to be reliable inscreening for osteoporosis.
Nakamoto et al. (2003) lookedinto whether untrained generaldental practitioners are capable ofdetermining from panoramicradiographs whether women havelow bone mineral density (BMD)[8]. The investigators studiedobserver agreement and diagnos-tic efficacy in detecting women withlow BMD. This was accomplishedwhen 27 GDPs assessed theappearance (normal or eroded) ofthe mandibular inferior cortex ondental panoramic radiographs of100 postmenopausal women whohad completed BMD assessmentsof the lumbar spine and of thefemoral neck. Intra-and inter-observer agreements wereanalyzed with kappa statistics. Thediagnostic efficacy (sensitivity,specificity, and predictive values)was analyzed by comparing twogroups classified by the mandibu-lar inferior cortex (women withnormal and women with erodedmandibular inferior cortex) withthose classified by BMD (womenwith normal BMD and women withosteopenia or osteoporosis). Themean sensitivity and specificitywere 77% and 40%, respectively,when BMD of the lumbar spinewas used as the standard, and75% and 39%, respectively, whenBMD of the femoral neck com-prised the standard. Nineteen ofthe 21 untrained general dentalpractitioners presented a moderateto almost perfect intra-observeragreement. It was concluded thatdental panoramic radiographsmight be used in clinical dentalpractice to identify postmeno-pausal women who have undetec-ted low BMD.
1.2. Evidence against usingpanoramic radiographs to screenfor osteoporosis:
Mohajery and Brooks (1992)conducted a trial to determinewhether radiographic changes
33333
could be detected in the mandible ofpatients with mild-to-moderatepostmenopausal osteoporosis andwhether these changes could beused as a diagnostic tool to differen-tiate normal from osteoporoticpatients [9]. Subjects were classifiedas either osteoporotic (n = 21) ornormal (n = 14) on the basis of bonedensity measurements of the lumbarspine and femoral neck, as deter-mined by dual-photonabsorptiometry. Mandibular bonedensity measurements were madeon panoramic and periapicalradiographs and expressed in termsof millimeters of aluminum equiva-lent. Thickness of the cortex at theangle of the mandible, sinus floor,and lamina dura of the tooth socketwas also measured. There were nosignificant differences in any of themandibular measurements betweenthe normal and osteoporoticsubjects. Whereas the skeletal bonemeasurements were correlated witheach other, there was no correlationbetween skeletal and mandibularbone measurements. Women withmild-to-moderate osteoporosis couldnot be distinguished from womenwith normal bone density.
The panoramic mandibularindex was used in a group ofpostmenopausal women to deter-mine whether it correlates with bonemineral densities of the femoralneck, lumbar area, and the trabecu-lar and cortical parts of the mandible[10]. Bone mineral density valueswere measured by dual-energy x-ray absorptiometry of the femoralneck and lumbar area and byquantitative computed tomographyof the mandible. Linear correlation ofthe panoramic mandibular indexwith all bone mineral density valueswas weak. However, the low andhigh index subgroup means wereclearly dependent on the bonemineral density variables. Theauthors concluded that despitesignificant differences in PMIbetween osteoporotic subjects andcontrols, panoramic assessment isnot to be advocated as an assess-ment for osteoporosis.
Watson et al. (1995) investi-gated whether osteoporotic post-
menopausal women show a decreasein mandibular cortical bone height, asmeasured by the PMI index, whencompared with nonosteoporoticpostmenopausal women [3]. Seventy-two Caucasian females (33 cases/39controls), age range 54-71 , wereselected through records and screeningvia a dual-energy x-ray absorptiometryscan (LUNAR-DEXA). ANOVA analysisindicated no differences in the meanPMI between case and control groups(0.37 ± 0.15 and 0.38 ± 0.13, respec-tively; p = 0.69).
1.3. Osteoporosis and periodontaldisease:
A study of 227 healthy postmeno-pausal women aged 48 to 56 years wasmade to determine whether advancedalveolar bone loss, diagnosed bypanoramic radiographs plus periodon-tal probing depths and the number ofremaining teeth were correlated withthe bone mineral status of the skeletonand cortical bone in the mandible [11].The results indicated that individualswith high mineral values in the skeletonretained teeth with deep periodontalpockets more readily than did thoseexhibiting osteoporosis. Individuals withnormal or high bone density seem to bebest able to retain teeth despiteadvanced periodontal disease.
Studies have also suggested thatosteoporosis and periodontitis areassociated diseases. Persson et al.(2002) investigated: (1) the prevalenceof self-reported history of osteoporosisin an older, ethnically diverse popula-tion; (2) the agreement betweenpanoramic and mandibular corticalindex (MCI) findings and self-reportedosteoporosis; and (3) the likelihood ofhaving both a self-reported history ofosteoporosis and a diagnosis ofperiodontitis [12]. Panoramic radio-graphs and medical histories wereobtained from 1,084 female Chinesesubjects aged 60-75 (mean age 68 ± 5years). Of the panoramic radiographs,90% were deemed useful for analysisusing MCI. They were used to gradesubjects as not having periodontitis orwith one of three grades of periodontitisseverity. A positive MCI was found in39% of the subjects, in contrast to 8%self-reported OP. The intra-classcorrelation between MCI and self-
reported osteoporosis was 0.20 (p <0.01). The likelihood of an associationbetween osteoporosis and MCI was 3%(95% CI: 1.6, 4.1, p < 0.001). Subjectswith self-reported osteoporosis and apositive MCI had worse periodontalconditions (p < 0.01). The Mantel-Haentzel odds ratio for osteoporosisand periodontitis was 1.8 (95% CI: 1.2,2.5, p < 0.001). The prevalence ofpositive MCI was high and consistentwith epidemiological studies, but onlypartly consistent with a self-reportedhistory of osteoporosis with a higherprevalence of positive MCI. Horizontalalveolar bone loss was associated withboth positive self-reported osteoporosisand MCI findings.
Contrary findings were made byLundstrom et al (2001) [13]. The authorsexamined the periodontal conditions inan age cohort of 70-year-old womencomparing an osteoporosis group witha control group with normal bonemineral density. 210 women 70 yearsold were randomly sampled from thepopulation register of the community ofLinkoping, Sweden. Bone mineraldensity (BMD) of the hip was measuredby dual energy X-ray absorptiometry. 19women were diagnosed with os-teoporosis (BMD < 0.640 g/cm2 in totalhip) and 15 of them agreed to partici-pate in the study. As a control group 21women with normal bone mineraldensity (BMD > 0.881 g/cm2) wererandomly selected from the initialpopulation. The clinical examinationincluded registration of the number ofremaining teeth, dental plaque andperiodontal conditions. The examinationincluded a dental panoramic radiographand vertical bitewings. The subjectscompleted a questionnaire on generalhealth, age at menopause, concurrentmedication, smoking and oral hygienehabits. No statistically significantdifferences in gingival bleeding, probingpocket depths, gingival recession andmarginal bone level were foundbetween the women with osteoporosisand those with normal bone mineraldensity. In conclusion, the study re-vealed no statistically significantdifferences in periodontal conditions ormarginal bone level between the twogroups; however, these results must beinterpreted with caution since thecompared groups were small.

44444
2. Diabetes MellitusDiabetes mellitus is a common
disorder of carbohydrate metabolismthrough either decreased production ofinsulin or tissue resistance to the effectsof insulin [14]. The former (Type-1diabetes) is insulin-dependent; the latter(Type-2 diabetes) is non-insulin-depen-dent and primarily treated by dietarymodification.
Taylor et al. (1998) tested thehypothesis that the risk for alveolar boneloss is greater, and bone loss progres-sion more severe, for subjects withpoorly-controlled Type-2 diabetes mellituscompared to individuals without Type-2diabetes or with better-controlled disease[15]. The poorly-controlled group hadglycosylated hemoglobin (HbA1) > 9%;the better-controlled group had HbA1 <9%. The study was conducted amongresidents of the Gila River IndianCommunity. Of 359 subjects aged 15 to57 with less than 25% radiographic boneloss at baseline, 338 did not havediabetes, 14 were better-controlleddiabetics, and 7 were poorly-controlleddiabetics. Panoramic radiographs wereused to assess interproximal bone level.Bone scores (scale 0-4) corresponding tobone loss of 0%, 1% to 24%, 25% to49%, 50% to 74%, or > 75% were usedto identify the worst bone score in thedentition. Change in worst bone score atfollow-up was specified on a 4-categoryordinal scale as no change, or a 1-, 2-, 3-, or 4-category increase over baseline.Poorly-controlled diabetes, age, calculus,time to follow-up examination, and initialworst bone score were statisticallysignificant explanatory variables inordinal logistic regression models. Poorly-controlled Type-2 diabetes mellitus waspositively associated with greater risk fora change in bone score (compared tosubjects without diabetes). The cumula-tive odds ratio (COR) at each threshold ofthe ordered response was 11 (95% CI =2.5, 53.3). When contrasted with subjectswith better-controlled diabetes, the CORfor those in the poorly-controlled groupwas 5 (95% CI = 0.8, 53.3). The COR forsubjects with better-controlled diabeteswas 2 (95% CI = 0.7, 6.5), when con-trasted to those without diabetes. Theseresults suggest that poorer glycemiccontrol leads to both an increased risk foralveolar bone loss and more severeprogression over those without Type-2
diabetes mellitus. There may also be agradient, with the risk for bone lossprogression for those with better-controlled Type-2 diabetes, intermediatebetween those for poorly-controlleddiabetes and non-diabetics.
Using panoramic radiographs, acase-control study performed on 664Japanese men aged 46-57 yearsassessed periodontal disease. Thisinvestigation also demonstrated acorrelation between the degree of failureof control of Type-2 diabetes and theamount of alveolar bone loss [16].Comparing diabetics to control subjects,a research report from Finland failed todemonstrate an increase in the microf-
renal disease, or renal osteodystro-phy. The radiologic features of bothforms of hyperparathyroidism aresimilar. These include generalizedosteoporosis, unilocular or multilocu-lar cystic radiolucencies in bone(Brown tumor), attenuation or loss oflamina dura surrounding the teeth,and calcifications in muscles andsubcutaneous tissues (Fig. 2, 3).
It is often considered thathistopathologic study of a biopsyspecimen is the basis for diagnosis of“cystic” lesions of the jaws. Unfortu-nately, the Brown tumor provides nodefinitive histologic answer. Nuclearmedicine or serologic confirmation is
Fig. 2: Primary Hyperparathyroidism – A.Panoramic radiograph demonstratingunilocular cystic lesion distal to the leftmandibular second premolar. B. Periapicalradiograph showing loss of lamina duradistal to the left mandibular secondpremolar tooth. C. Histopathologic studyof the Brown tumor showing numerousmultinucleated giant cells. D. The lesionhealed and the lamina dura reconsti-tuted following removal of the parathy-roid tumor.
lora that couldcontribute to theincreased rate ofperiodontitis [17].
The degree ofmarginal alveolarbone loss has alsobeen assessed in agroup of youngsubjects with Type-1 diabetes mellitus[18]. A clear trendtowards increasedmarginal bone losswas seen in thesubjects with thepoorest controlleddiabetes. Thesubjects with goodmetabolic controland no complications were no moresusceptible to marginal bone loss thannon-diabetic controls of the same age.
3. HyperparathyroidismPrimary hyperparathyroidism is
relatively rare and results from anexcess secretion of parathyroidhormones due to a hormone-producingbenign or malignant neoplasm [19,20].Most persons with primary hyperpar-athyroidism are over age 60. Womenare more commonly affected than men[14]. Secondary hyperparathyroidismresults in excess secretion of parathy-roid hormone due to parathyroidhyperplasia compensating for ametabolic disorder that has resulted inretention of phosphate or depletion ofthe serum calcium level [3]. Secondaryhyperparathyroidism is most commonlyfound as a complication of end-stage
usually needed. The Brown tumorlesion is composed of fibrousconnective tissue containing areas ofhemorrhage and foreign-body typemultinucleated giant cells. This can beeasily confused with other conditionssuch as the giant cell tumor, foreignbody granuloma, aneurismal bonecyst, or osteoclastoma.
55555
“ It was concluded that panoramic radiography is useful in monitoring renalosteodystrophy, especially to assess the response to therapy such asparathyroidectomy or renal transplantation.”
In Italy, 45 patients afflicted withchronic renal failure (29 men and16 women; mean age: 48 years)and on hemodialysis for 4 to 245months (mean: 67 months) wereexamined using panoramic imagesplus radiographs of the skull,hands, shoulders and clavicles,pelvis and spine [21]. The controlgroup (45 subjects with no renaldiseases) was examined only bypanoramic radiography. Dental andskeletal radiographs were rated ona 0-6 score and compared toassess possible relationshipsbetween skeletal and dentalradiographic changes. Twenty-sixdialysis patients (58% of all dialysispatients studied) had the followingradiographic abnormalities in thejaws: osteoporosis (100%), laminadura reduction or loss (27%),calcifications of soft tissues orsalivary glands (15%), focalosteosclerosis adjacent to toothroots (12%), and Brown tumors(8%). Radiographic abnormalitiesin the hand, shoulder and pelviswere found in 51% of dialysispatients. In the control group, only16% had jaw lesions includingosteopenia, cortex reduction at themandibular angles and cyst-likelesions. Caries and periodontaldisease experience did not differbetween the dialysis group and the
controls. It was concluded that pan-oramic radiography is useful in monitor-ing renal osteodystrophy, especially toassess the response to therapy such asparathyroidectomy or renal transplanta-tion.
A Bosnian study of panoramic andperiapical radiographs of 42 patientson hemodialysis and having renalosteodystrophy, demonstrated aprogressive increase in periodontaldisease, loss of lamina dura, deviationin the trabecular pattern, Brown tumor“pseudocyst” formation and pulpcalcifications [22].
4. Specific InfectionsNot all systemic conditions that can
produce jaw lesions are as common asthe ones discussed above, but theirdetection is equally important for thecorrect treatment to be commenced. Inthe developed world there had been adecline in advanced lesions fromspecific infections; however, with agrowing population of immune-compro-mised individuals as a result of the morewidespread use of immunosuppressiveregimens subsequent to organ trans-plantation, and through the AIDSepidemic, a resurgence of previously“vanquished” organisms is possible.
4.1. Tuberculosis:Tuberculosis is a specific infection
caused by the acid-fast bacillus Myco-bacterium tuberculosis. Almost allcases arise from pulmonary disease.Involvement of the oral tissues is rare,occurring in less than one in 50 withtuberculosis [2]. Oral tissues areinvolved through direct inoculation,extension from other infection sites, orhematogenous seeding. Patients withjawbone lesions complain of repeatedattacks of “toothache-like” pain andthere is usually swelling of the affectedarea. Sinus tracts develop as theswellings rupture and may drainintraorally or extraorally. Trismus may bepresent, especially if the temporoman-dibular joint is involved.
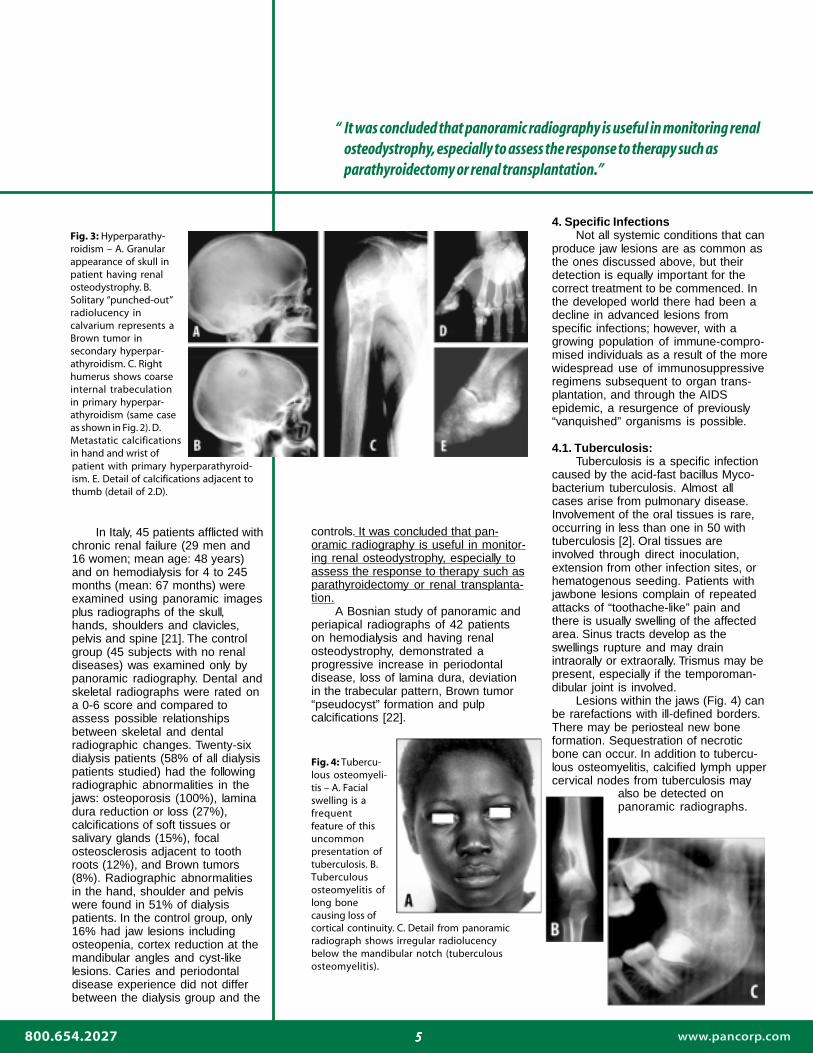
Lesions within the jaws (Fig. 4) canbe rarefactions with ill-defined borders.There may be periosteal new boneformation. Sequestration of necroticbone can occur. In addition to tubercu-lous osteomyelitis, calcified lymph uppercervical nodes from tuberculosis may
Fig. 3: Hyperparathy-roidism – A. Granularappearance of skull inpatient having renalosteodystrophy. B.Solitary “punched-out”radiolucency incalvarium represents aBrown tumor insecondary hyperpar-athyroidism. C. Righthumerus shows coarseinternal trabeculationin primary hyperpar-athyroidism (same caseas shown in Fig. 2). D.Metastatic calcificationsin hand and wrist of
Fig. 4: Tubercu-lous osteomyeli-tis – A. Facialswelling is afrequentfeature of thisuncommonpresentation oftuberculosis. B.Tuberculousosteomyelitis oflong bonecausing loss ofcortical continuity. C. Detail from panoramicradiograph shows irregular radiolucencybelow the mandibular notch (tuberculousosteomyelitis).
also be detected onpanoramic radiographs.
patient with primary hyperparathyroid-ism. E. Detail of calcifications adjacent tothumb (detail of 2.D).

66666
“ The cardinal radiographic signs of metastases to the jaw include a wellcircumscribed but uncorticated lytic lesion, especially in the posterior mandible,with highly irregular outline, or multiple small areas of bone destruction thatgradually coalesce to form large ill-defined areas of bone destruction.”
4.2. Syphilis:Syphilis is caused by infection with
the spirochete Treponema pallidum. Itmay be congenital or acquired after birth.The acquired form can be subclassifiedinto three distinctive stages: primary,secondary and tertiary. Bone may beaffected in congenital syphilis and in boththe secondary and tertiary stages ofacquired syphilis (Fig. 5). The jaws arerarely affected by syphilis. When they arethe palate is more frequently involvedthan the mandible. Radiographic featuresof bone involvement by syphilis include:deposition of subperiosteal new bonealong the inferior border of the mandible(syphilitic periostitis); gummatous destruc-tion of bone, especially the palate,resulting in a large radiolucent area; well-demarcated destruction along a corticalmargin; or multiple radiolucencies withpoorly-defined margins and sequestration(syphilitic osteomyelitis).
5. Metastatic MalignanciesMetastatic tumors to the jaws are
rarely reported; however, metastases maywell constitute the most common malig-nant tumors affecting the skeleton [2].Nevertheless, most metastases to boneare found in the spine, pelvis, skull, ribs,or the humerus. It is reported that approxi-mately 1% of malignant neoplasmsmetastasize to the jaws, and metastasescomprise about 1% of all oral malignan-cies. To qualify as a metastasis, the lesionmust be localized to bone as distin-guished from direct invasion – and itshould be histopathologically verifiable asa metastasis. Most metastases occur inmature individuals over age 50. Theprocess of metastasis occurs by one ofthree routes: seeding of an adjacent bodycavity, lymphatic spread or hematog-enous dissemination. The most commonprimary sites for tumors metastasizing tothe jaws in adults are from organs belowthe clavicle, namely: breast, kidney, lung,colon, rectum, prostate, stomach, skin,testes, bladder, ovary, and cervix. Abovethe clavicle, the most frequent primary sitefor metastases to the jaw is the thyroidgland. In children metastatic disease isextremely rare. When this does occur inchildhood, the primary cause is usually aneuroblastoma, retinoblastoma, or Wilmstumor.
The clinical presentation of meta-static disease to the jaws is nonspecific,
Fig. 5: A-D. Congenital syphilis. (Notedeficient bridge of nose.) Lytic lesionsin the center of the palate are outsidethe panoramic focal trough. E-F.Tertiary syphilis. (Note gummatousdestruction in nasal cavity.)
including local pain, swelling, numbness,paresthesia of the lip and chin, andloosening or extrusion of the teeth.Pathologic fractures may also occur butare considered rare (Fig. 6).
The cardinal radiographic signs ofmetastases to the jaw include a well-circumscribed but uncorticated lyticlesion, especially in the posteriormandible, with highly irregular outline, ormultiple small areas of bone destructionthat gradually coalesce to form large ill-defined areas of bone destruction (Fig. 6& 7). Ancillary signs include periapical orperiradicular radiolucency or radiopacitywithout evidence of pulpal pathology,failure of an extraction socket to heal,generalized loss of the lamina dura, or“floating” teeth.
In a 12-month period, cancermetastatic to the mandible was diag-nosed in eight patients at the Oral andMaxillofacial Surgery Clinic of theUniversity of Vienna (1997) [23]. Six ofthem were presented with pain mimick-ing toothache, temporomandibular jointdisorders, or trigeminal neuralgia, andtwo showed osteopenic bone lesions on
panoramic radiography combinedwith perimandibular swelling.Anesthesia of the lower lip was theone common clinical feature in alleight cases. Histology revealedbreast, lung, renal cancer, and amalignancy of inconclusive origin.
Thirty metastases of malignanttumors in jaws were retrospectivelystudied in the Pathology Depart-ment of the Hospital de la Pitie,Paris, France (1991) [24]. Theyoccurred more often in women thanin men (17 F:13 M). In 21 cases, theprimary cancer was known and hadbeen treated 1 to 4 years earlier. Inthe other 9 cases, discovery of thebone metastasis led to the discoveryof a latent tumor. Clinical signs andsymptoms included swelling, pain,loosening of teeth, and labio-mentalanaesthesia, but rarely pathologicfracture. All but two patients had aradiolucent lesion. The metastasesalmost always involved the mandible(95 %), most often in the molar areaor angle. Histologically, the majorityof lesions were adenocarcinomas
77777
References1. Mohammad AR, Alder M, McNally MA. A pilot study of
panoramic film density at selected sites in the mandible topredict osteoporosis. Int J Prosthodont 1996;9:290-294.
2. Farman AG, Nortjé CJ, Wood RE. Oral and maxillofacialdiagnostic imaging. St Louis: Mosby-Year Book 1993.
3. Watson EL, Katz RV, Adelezzi R, Gift HC, Dunn SM. Themeasurement of mandibular cortical bone height inosteoporotic vs. non-osteoporotic postmenopausal women.Spec Care Dentist 1995;15:124-128.
4. Benson BW, Prihoda TJ, Glass BJ. Variations in adultcortical bone mass as measured by a panoramicmandibular index. Oral Surg Oral Med Oral Pathol1991;71:349-356.
5. Taguchi A, Tanimoto K, Suei Y, Otani K, Wada T. Oral signsas indicators of possible osteoporosis in elderly women.Oral Surg Oral Med Oral Pathol Oral Radiol Endod1995;80:612-616.
6. Taguchi A, Suei Y, Ohtsuka M, Otani K, Tanimoto K, OhtakiM. Usefulness of panoramic radiography in the diagnosis ofpostmenopausal osteoporosis in women. Width andmorphology of inferior cortex of the mandible.Dentomaxillofac Radiol 1996;25:263-267.
7. Horner K, Devlin H, Harvey L. Detecting patients with lowskeletal bone mass. J Dent. 2002;30:171-175.
8. Nakamoto T, Taguchi A, Ohtsuka M, Suei Y, Fujita M,Tanimoto K, Tsuda M, Sanada M, Ohama K, Takahashi J,Rohlin M. Dental panoramic radiograph as a tool to detectpostmenopausal women with low bone mineral density:untrained general dental practitioners’ diagnosticperformance. Osteoporos Int 2003;14:659-664.
9. Mohajery M, Brooks SL. Oral radiographs in the detection ofearly signs of osteoporosis. Oral Surg Oral Med Oral Pathol1992;73:112-117. [From the University of Michigan School ofDentistry, Ann Arbor.
10. Klemetti E, Kolmakov S, Heiskanen P, Vainio P, Lassila V.Panoramic mandibular index and bone mineral densities inpostmenopausal women. Oral Surg Oral Med Oral Pathol1993;75:774-779.
11. Klemetti E, Collin HL, Forss H, Markkanen H, Lassila V.Mineral status of skeleton and advanced periodontal disease.J Clin Periodont 1994;21:184-188.
12. Persson RE, Hollender LG, Powell LV, MacEntee MI, WyattCC, Kiyak HA, Persson GR. Assessment of periodontalconditions and systemic disease in older subjects. I. Focuson osteoporosis. J Clin Periodontol 2002;29:796-802.
13. Lundstrom A, Jendle J, Stenstrom B, Toss G, Ravald N.Periodontal conditions in 70-year-old women withosteoporosis. Swed Dent J 2001;25:89-96.
14. Neville BW, Damm DD, Allen CM, Bouquot JE. Oral andmaxillofacial pathology. Philadelphia: EB SaundersCompany 1995.
15. Taylor GW, Burt BA, Becker MP, Genco RJ, Shlossman M.Glycemic control and alveolar bone loss progression in type2 diabetes. Ann Periodontol 1998;3:30-39.
16. Marugame T, Hayasaki H, Lee K, Eguchi H, Matsumoto S.Alveolar bone loss associated with glucose tolerance inJapanese men. Diabet Med 2003;20:746-751.
17. Collin HL, Uusitupa M, Niskanen L, Kontturi-Narhi V,Markkanen H, Koivisto AM, Meurman JH. Periodontalfindings in elderly patients with non-insulin dependentdiabetes mellitus. J Periodontol 1998;69:962-966.
18. Tervonen T, Karjalainen K, Knuuttila M, Huumonen S.Alveolar bone loss in type 1 diabetic subjects. J ClinPeriodontol 2000;27:567-571.
19. Morano S, Cipriani R, Gabriele A, Medici F, Pantellini F.Recurrent Brown tumors as initial manifestation of primaryhyperparathyroidism. An unusual presentation. Minerva Med2000;91:117-122.
20. Migita H, Ohno A. Oral bony lesion in a patient with medicalhistory of hyperparathyroidism. Int J Oral Surg 1979;8:67-70.
21. Scutellari PN, Orzincolo C, Bedani PL, Romano C.Radiographic manifestations in teeth and jaws in chronickidney insufficiency. Radiol Med (Torino) 1996;92:415-420.
22. Ganibegovic M. Dental radiographic changes in chronicrenal diseases.Med Arh 2000;54:115-118.
23. Glaser C, Lang S, Pruckmayer M, Millesi W, Rasse M,Marosi C, Leitha T. Clinical manifestations and diagnosticapproach to metastatic cancer of the mandible. Int J OralMaxillofac Surg 1997;26:365-368.
24. Auriol M, Chomette G, Wann A, Guilbert F. Metastases ofmalignant tumor in the jaw. Analysis of 30 case reports. RevStomatol Chir Maxillofac 1991;92:155-159.
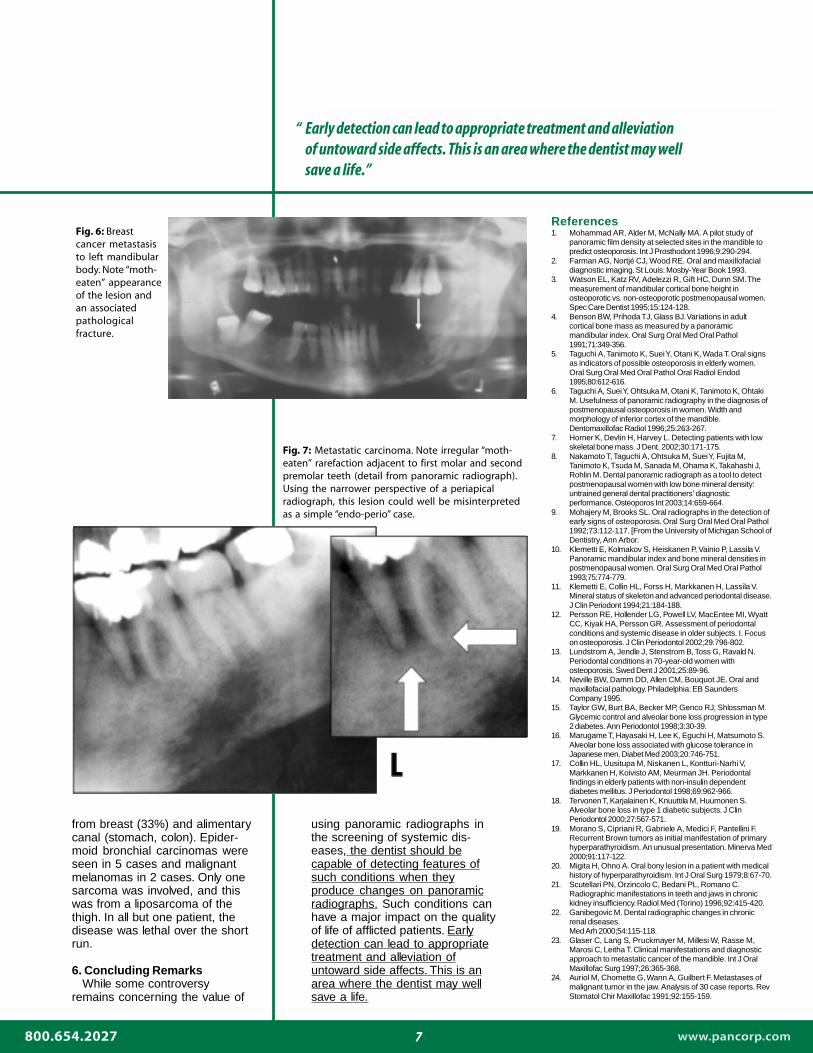
from breast (33%) and alimentarycanal (stomach, colon). Epider-moid bronchial carcinomas wereseen in 5 cases and malignantmelanomas in 2 cases. Only onesarcoma was involved, and thiswas from a liposarcoma of thethigh. In all but one patient, thedisease was lethal over the shortrun.
6. Concluding Remarks While some controversyremains concerning the value of
using panoramic radiographs inthe screening of systemic dis-eases, the dentist should becapable of detecting features ofsuch conditions when theyproduce changes on panoramicradiographs. Such conditions canhave a major impact on the qualityof life of afflicted patients. Earlydetection can lead to appropriatetreatment and alleviation ofuntoward side affects. This is anarea where the dentist may wellsave a life.
Fig. 6: Breastcancer metastasisto left mandibularbody. Note “moth-eaten” appearanceof the lesion andan associatedpathologicalfracture.
Fig. 7: Metastatic carcinoma. Note irregular “moth-eaten” rarefaction adjacent to first molar and secondpremolar teeth (detail from panoramic radiograph).Using the narrower perspective of a periapicalradiograph, this lesion could well be misinterpretedas a simple “endo-perio” case.
“ Early detection can lead to appropriate treatment and alleviationof untoward side affects. This is an area where the dentist may wellsave a life.”

88888
©2004 Panoramic Corporation (7-04)
88888
The Richmond Institute for Continuing DentalEducation is an ADA CERP Recognized Provider.
Osteoporosis: Mandibular corticalshape was significantly associatedwith biochemical mark so dentistsmay be able to identify postmeno-pausal women with low BMD byusing dental panoramic radio-graphs.Taguchi A, Sanada M, Krall E,Nakamoto T, Ohtsuka M, Suei Y,Tanimoto K, Kodama I, Tsuda M,Ohama K. Relationship betweendental panoramic radiographicfindings and biochemical markersof bone turnover. J Bone Miner Res2003;18:1689-1694. [From theDepartment of Oral and Maxillofa-cial Radiology, Hiroshima UniversityDental Hospital, Japan.]
Recent studies suggest that man-dibular inferior cortical shape andwidth on dental panoramic radio-graphs may be useful screening toolsfor low skeletal bone mineral density(BMD) or increased risk of os-teoporotic fracture. Of 609 womenwho visited the authors’ clinic for BMDassessment between 1996 and 2002,82 Japanese postmenopausalwomen (age range 46-68 years ofage; mean age 54 +/- 5 years), wererecruited for a study to furtherexamine this relationship. Biochemi-cal markers of bone turnover andlumbar spine BMD measurementswere compared with panoramicradiographic findings. Mandibularinferior cortical shape (normal, mild/moderate erosion, severe erosion)and width were evaluated on dentalpanoramic radiographs. BMD at thelumbar spine (L2-L4) was measuredby DXA and categorized as normal(T-score > -1.0), osteopenia (T-score, -1.0 to -2.5), or osteoporosis (T-score <
In The Recent Literature:-2.5). Bone turnover was estimatedby serum total alkaline phosphatase(ALP) and urinary N-telopeptidecross-links of type I collagen (NTx),corrected for creatinine. The odds oflow spine BMD in subjects withmandibular cortical erosion were 3.8(95% CI, 1.2-12.5). Mandibularcortical erosion was significantlyassociated with increased NTx (p <0.001) and ALP (p < 0.05) levels.Mandibular cortical width wassignificantly associated with spineBMD but not with NTx and ALP levels.In conclusion, the results suggest thatmandibular inferior cortical shape ondental panoramic radiographs maybe an indicator of bone turnover andspine BMD in postmenopausalwomen. Dentists may be able toidentify postmenopausal women withincreased risk of osteopenia andosteoporosis on dental panoramicradiographs.
Radiation-associated meningioma:Full-mouth series performed 15-40years ago, when radiation exposurefrom full-mouth series was greaterthan it is now, were associated withan increased risk of meningioma.No increased risk to meningiomawas observed with panoramicradiographs, cephalograms orbitewings.Longstreth WT Jr, Phillips LE,Drangsholt M, Koepsell TD, CusterBS, Gehrels JA, van Belle G. DentalX-rays and the risk of intracranialmeningioma: a population-basedcase-control study. Cancer 20041;100:1026-1034. [From the Depart-ment of Neurology, University ofWashington, Seattle, USA.]
Ionizing radiation is a likely causeof intracranial meningioma. Theauthors investigated whether therisk of intracranial meningioma wasassociated with past dentalradiographic procedures; specifi-cally, posterior bitewings, full-mouthseries, and lateral cephalometricand panoramic radiographs. Apopulation-based case-controlstudy was made among residentsof various counties in westernWashington State. Case patients (n= 200) each had an incident ofintracranial meningioma that wasconfirmed histologically. Random-digit dialing and Medicare eligibilitylists were used to identify twocontrol subjects to be age- andgender-matched to each casepatient. Exposures were deter-mined during an in-person inter-view. The authors compared self-report and dental records in asubset of study participants. Of the4 dental radiographic proceduresevaluated, only the full-mouth series(specifically, = 6 over a lifetime) wasassociated with a significantlyincreased risk of meningioma(odds ratio, 2.06; 95% confidencelimits, 1.03-4.17). However, evi-dence for a dose-response relationwas lacking (p for trend = 0.33). Therisk was elevated with the aggre-gate number of full-mouth series in10-year periods from approximately15-40 years before diagnosis, withsignificant elevations in the 10-yearperiods beginning 22-30 yearsbefore diagnosis. The risks in theseanalyses were even greater whenonly women were considered.
(847) 458-0063
(847) 458-0063
2260 Wendt St., Algonquin, IL 60102