Pain killers y OMFD4 30 3 2… · Pregnancy and Lactation nOptimal management of dental pain during...
64
Pain killers
Transcript of Pain killers y OMFD4 30 3 2… · Pregnancy and Lactation nOptimal management of dental pain during...

Pain killers

Analgesics
Class of drugs which obtund pain without causing loss of
consciousness

Classification of analgesics
Two main classesn Non-narcoticn Narcotic

Local Anesthesia vs. Analgesics
n Local anesthesia causes loss of sensation in a localized area
n Analgesics work on whole body system and reduce pain without total loss of sensation

Non-Narcotics
For mild to moderate painAnalgesic, antipyretic, anti-inflammatoryInhibit prostaglandin productionSalicylates, NSAIDS, acetaminophen (no anti-inflammatory effect)

Acetaminophenn Indicated for the management of mild to moderate pain.n Acetaminophen is very safe if used in therapeutic doses.n Analgesic, antipyretic, not anti-inflammatoryn Often combined with narcoticsn 500-1000mg, p.o. q6hn Total dose not to exceed 4gm q 24hn Risk of hepatic necrosis at toxic doses (10-50 gm qd)n Patient with liver disease/hepatitis may have problems

Acetaminophenn It is devoid of the side effects that
accompany the nonsteroidal anti-inflammatory drugs (NSAIDs).
n For the management of severe pain acetaminophen is usually insufficient by itself, although it may be used in combination with an opioid such as codeine (Panadol Extra) or Abimol Extra

NSAIDs
n NSAIDs block the cyclooxygenase enzymes, which exist in 2 forms known as:-
1. cyclooxygenase-1 (COX-1)
2. cyclooxygenase-2 (COX-2)


NSAIDsn COX-1 is responsible for the synthesis of several
mediators,including:-1. The prostaglandins that protect the gastric mucosa
and that regulate renal blood flow2. The thromboxanes that initiate platelet aggregation.3. The Leukotrienes which promote inflammation and
can cause bronchospasm.

n Tissue damage such as pulpitis or periodontitis, or tissue damage resulting from surgery, will induce the production of COX-2, which leads to the synthesis of the prostaglandins that:-
1. Sensitize pain fibers
2. Promote inflammation

NSAIDsn Traditional NSAIDs block both
COX-1 and COX-2, but in recent
years, new NSAIDs have been
developed that are:-
n Much more selective for COX-2.
n These selective COX-2 inhibitors
were developed to be less damaging
to the gastric mucosa

NSAIDsn ASA is a well-known antipyretic and is
widely used for its antiplatelet action for
prophylaxis of:-
1. Myocardial infarction
2. In patients with a history of unstable
angina pectoris

NSAIDs

contraindicationsn Inhibition of prostaglandin synthesis will diminish the
protective effect of prostaglandins on the lining of
stomachgastric mucosa.
n Enteric-coated formulations may reduce the likelihood of
dyspepsia, but will not prevent gastric damage and
subsequent bleeding.

Selective Cox2 Inhibitor
n If acetaminophen is insufficient, one can
consider a selective COX-2 inhibitor, as
these inhibitors are much less likely to
induce gastric bleeding than traditional
NSAIDs. e.g. Celecoxib (Celebrex) and
rofecoxib (Vioxx)

platelet aggregationn NSAID-induced inhibition of thromboxane synthesis
results in a decrease in platelet aggregation. For most NSAIDs this effect is reversible within 24 hours.
n ASA is unique in that it irreversibly damages cyclooxygenase for the life of the platelet; if doses are high, one could consider withdrawing ASA for at least one week before surgery.

Allergy
n Bronchospasm and other allergy signs and symptoms can occur in susceptible patients as a result of redirecting the arachidonic acid breakdown into the leukotriene pathway
n ASA and NSAIDs are best avoided in patients with severe asthma.

NSAIDs & blood pressure
Intrarenal & extrarenal prostaglandins have a direct inhibition effect on the tubular reabsorption of sodium and chloride
n NSAIDs decrease intrarenal & extrarenal prostaglandins leading to:-
1. Vasoconstriction & decrease blood flow to kidneys2. Soduim and water retention.3. Increase blood pressure.

Use of Analgesics in Pregnancy and Lactation
n Optimal management of dental pain duringpregnancy is removal of the source of pain using
local anesthesia.n If, however, postoperative pain is present, an
analgesic may be necessary and should be made available.
n Acetaminophen is clearly the analgesic of choice in all stages of pregnancy.

n The use of NSAIDs, including ASA, is less favorable, particularly late in pregnancy.
n NSAIDs may predispose to ineffective contractions during labour, increased bleeding during delivery or premature closure of the ductus arteriosus of the heart.
nNSAIDs are therefore contraindicated in the third trimester.

Use of analgesics during lactation
nAs with pregnancy, acetaminophen is the analgesic of choice in lactation.
nASA and diflunisal may increase bleeding and should be avoided if possible.
n Opioids are considered safe in lactation.

Use of Analgesics for Elderly Patients
n Acetaminophen is the analgesic of choice in the elderly.n NSAIDs are a major concern due to the potential for
gastrointestinal bleeding, which becomes more likely with increasing age, if there is a history of gastric bleeding
n If they are necessary, one should greatly reduce doses and avoid concurrent use of 2 or more NSAIDs.

Overall Prescribing Recommendations

Narcotics

Opium - History• Friedrich Wilhelm Serturner
– A German Pharmacist– Isolated Morphine in 1803 and named it
after the Greek god of Dreams“MORPHEUS”

MORPHINE (Pharmacologicalactions) - CNS
• Analgesia:• Strong analgesic• Visceral pain is relieved better than somatic
pain• Degree of analgesia increases with dose• Nociceptive pain is better relieved than
Neuretic pain• Associated reactions to pain are also relieved
– apprehension, fear and autonomic effects• Tolerance to pain is better

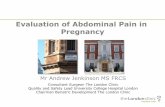
MORPHINE – Analgesiaaction
• Two components – spinal and supraspinal• Inhibits release of excitatory transmitters
from primary afferents – at Substantiagelatinosa of dorsal horn
• Exerted through Interneurones – gating ofpain
• At supraspinal level in cortex, meidbrain andmedulla - alter processing and interpretationand send inhibitory impulses throughdescending pthway

D
E

Morphine - The GateTheory

Pharmacological actions ofMorphine (CNS) – contd.
• Sedation:– Drowsiness and indifference to surroundings– Inability to concentrate and extravagant imagination –
colorful day dream– Apparent excitement– Larger doses produce sleep – EEG resembles normal
sleep• Mood effects:
– In Normal persons calming effect, mental clouding,feeling of detachment, lack of initiative etc. -unpleasant in absence of pain
– Sometimes DYSHORIA– But in persons with pain & addicts sense of wellbeing,
pleasurable floating feelings – kick– EUPHORIA

Pharmacological actions ofMorphine (CNS) – contd.
• Stimulation:• Depression:1. Respiratory centre
depression – Both rateand depth of respirationare diminished
1. CTZ – sensitize CTZto vestibular andother impulses
2. Edinger WestphalNucleus – miosis
3. Vagal centre –Bradycardia
4. Hippocampal cells –convulsions (inhibitionof GABA release)
• Dangerous in Headinjury and asthmatics
1. Cough Centre –Depressed
2. Temperature regulatingcentre – depressed
3. Vasomotor centre – highdoses cause fall in BP

Morphine - Effects

Pharmacological actionsof Morphine – contd.
• Neuro-endocrine:• GnRH and CRH are inhibited – FSH, LH and ACTH levels
are lowered – only short term – tolerance develops• Decrease in levels of Sex hormone and corticosteroids, but
no infertility• Increases ADH release – oliguria
• CVS: NO DIRECT EFFECT ON HEART• Vasodilatation – histamine release, depression of vasomotor
centre and directly on blood vessels decreasing the tone• Cardiac work reduction due to consistent vasodilatation

Pharmacological actionsof Morphine – contd.
• GIT: CONSTIPATION• Due to direct action on intestine reducing
propulsive movement, spasm of sphincters,decrease in all GIT secretions
• Smooth Muscles:• Billiary Tract: Billiary colic – closure of sph.
Of Oddi• Bladder: Urinary urgency but difficulty• Bronchi - Bronchospasm

Morphine -Pharmacokinetics
• Absorption and Distribution:• Variable orally (usually not given orally – 1 pass metabolism,st
given IM or IV)• Widely distributed – liver, spleen, kidney etc.• Enters Brain slowly• Readily crosses placental barrier – dependence in fetus
• Metaboloism:• In Liver by glucoronidation – water soluble metabolites• Morphine-6- Glucoronide – analgesic – in renal failure
prolong analgesia• Morphine-3-glucoronide – No analgesia – neuroexcitatory
• Excretion:• Via Urine, Plasma t1/2 = 2-3 Hrs• Action lasts for 4-6 Hrs• Completely eliminated in 24 Hrs
• Preparation: 10, 15, and 20 mg. (IV: 2 – 10 mg)

Morphine -Pharmacokinetics

Morphine – AdverseEffects
1. Respiratory Depression: Infant and Old2. Vomiting3. Sedation, Mental Clouding – sometimes dysphoria4. Hypotensive effect5. Rise in Intracranial Pressure6. Apnoea: Newborn7. Urinary retention8. Idiosyncrasy and allergy9. Acute Morphine Poisoning: occurs if >50 mg (Lethal dose –
250 mg), Gastric lavage with KMNO4, Specific antidote:Naloxone: 0.4 to 0.8 mg IV repeatedly in 2-3 minutes tillrespiration picks up
10. Tolerance and dependence

Morphine – Therapeuticuses
• Analgesic:1. Long Bone Fracture2. Myocardial Infarction3. Terminal stages of cancer4. Burn patients5. Postoperative patients6. Visceral pains – pulmonary embolism, pleurisy, acute
pericarditis7. Biliary colic and renal colic8. Obstetric analgesia9. Segmental analgesia

Morphine – OtherTherapeutic uses
• Preanaesthetic Medication• Balanced anaesthesia and surgical analgesia• Acute Left ventricular failure – Cardiac
asthma• Cough – not used but Codeine is used• Diarrhoea – colostomy - Loperamide,
Diphenoxylate

Morphine -Contraindications
1. Two Extremes of Age2. Bronchial asthma3. Respiratory insufficiency - empysema4. Head Injury5. Shock – Hypotension6. Undiagnosed acute abdomen7. BHP8. Renal Failure, Liver diseases and hypothyrodism9. Unstable personalities

Opioids - Classification1. Natural Opium Alkaloids: Morphine and Codeine2. Semi-synthetic: Diacetylmorphine (Heroin) and
Pholcodeine3. Synthetic Opioids:
• Phenylpiperidines:• Pethidine (Mepiridine) and its congeners – Diphenoxylate
and Loperamide• Fentanyl and its congeners – sufentanil, remifentanil and
alfentanil• Phenyl-heptylmines: Methadone and congeners like
Propoxyphene and Dextropropoxyphene••
Benzomorphans: PentazocineMorphinan compounds and congeners: Levorphanol andButorphanol

Pethidine• Morphine Vs Pethidine:
– 1/10th as potent as Morphine, but Efficacy is similar– Produces as much sedation, euphoria and respiratory
depression in equianalgesic dose and similar abusepotential
– Less spasmodic action in smooth muscles – less miosis,constipation and urinary retention
– Rapid but short duration of action (2-3 Hrs)– Vagolytic effect - Tachycardia– Devoid of antitussive action– Less histamine release – safer in asthmatics– Better oral absorption

Pethidine – contd.• Pharmacokinetics
– Well absorbed orally, bioavailability 50%– Effects appear in 10-15 min. after oral
absorption– On parenteral administration action lasts for
2-3 Hrs– Metabolized in liver – mepiridinic acid and
norpethidine– Norpethidine accumulates on chronic use– Excreted in urine

Pethidine – contd.• Adverse Effects:
• Similar to Morphine• Atropine like effects – dry mouth, blurred vision,
tachycardia• Overdose – tremors, mydriasis, delirium and convulsion due
to norpethidine accumulation• Uses:
• Analgesic as substitute of Morphine• Ptreanaesthetic medication• As analgesic during labour – less fetal respiratory
depression• Dose 50-100 mg IM/SC, oral – 50-100 mg tabs.

Methadone• Chemically dissimilar but similar in most of pharmacological
actions – analgesic, respiratory depression etc.• High action orally as well as parenterally• Single dose effect is – same with Morphine including
duration of action• Cumulation – on repeated administration (t1/2 24-36 Hrs)• Highly bound to plasma protein 80 to 90%• Metabolized in liver by – demethylation and cyclization• Excreted in urine• Slow action and less subjective effect – abuse potential is
low• Used as substitution therapy as opioid dependence: 1:4mg
and 1:20 mg of Morphine and Pethidine respectively• Codeine is used as substitution in Methadone addiction

Tramadol• Centrally acting analgesic• Very low action on opioid receptors (• Other mechanisms involved in analgesic action – 5-HT and
NA reuptake inhibition – spinal inhibition of pain• Effective both orally and IV (100mg = 10 mg Morphine)• Side effects are similar to Morphine but less prominent• Well tolerated and low abuse potential• Only Partially reversed by Naloxone• Used in chronic neuropathic pain and short diagnostic
procedures• Dose: 50-100 mg IM/IV/Oral
(Contramol)

Opioid Receptors• Mainly 3 (three) types of receptors – μ (mu), κ (kappa) and δ
(delta)• Subtypes: μ1, μ2, κ1, κ2, κ3, δ1 and δ2• Location: Peripheral Nerve endings, SG in spinal chord,
Periaqueductal gray (PAG) in midbrain and Brain stem(medulla, hypothalumus and also amygdala
• Opioids are – agonists, partial agonist or competitiveantagonists of these receptors
• Overall effect depends on nature of interaction and affinityto these
• Morphine is agonist of all but affinity is higher for mu

Effects of Different Opioid Receptor Stimulation:
μ receptor κ receptor δ receptorLocation
Effects
μ1 – supraspinal
μ2 - spinal
κ1 – spinal Spinal
κ3 -supraspinal supraspinal
Analgesia Spinal analgesia Spinal analgesia
Respiratorydepression
Dysphoria AffectivebehaviourSedation(Supraspinal)Sedation PsychomimeticRespiratorydepression
Euphoria PhysicalMiosis dependence
(nalorphinetype)
Reduced GImotility
Physical dependence
Loss of GI motilityAgonists Morphine, Codeine, PentazocineFentanyl andpentazocine weakly

Effects of OpioidReceptor Stimulation

Effects of Opioid ReceptorStimulation – contd.

Opioid Receptors –Intracellular mechanism
• All are G-protein coupled receptors• Located on prejunctional neurones• Inhibits release of transmitters – NA, DA, 5-HT,
GABA and Glutamate• Activation reduces intracellular cAMP formation -
Opening of K+ channel via μ and δ. and supressionof N type of Ca++ channels
• Ultimately Hyperpolarization and reducedintracellular Ca++release
Reduced Neurotransmitter

Endogenous OpioidPeptides
• Endorphins:• Derived from POMC• ß-endorphins: 2 Types - ß-endorphin1 and ß-endorphin-2• Primarilty μ agonist and also has δ action
• Enkephalins:• Derive from Proenkephalin• Met-ENK and leu-ENK• Met-ENK - Primarily μ and δ agonist and leu-ENK – δ
agonist• Dynorphins:
• Derive from Prodynorphin: DYN-A and DYN-B• Potent κ agonist and also have μ and δ action

Opioid Antagonists1. Pure antagonists: Naloxone, Naltrexone and
Nalmefene•••
Affinity for all receptors (μ, δ and κ)Can displace opioids bound to α-receptorsNo action on Normal person but reverses poisoning andwithdrawal symptoms in addicts
1. Mixed Agonist-antagonists: Nalorphine, Pentazocine,Butorphanol and Nalbuphine
2. Partial/weak μ agonist and κ antagonist:Buprenorphine

Nalorphine• Not used anymore• Previously used as Opioid antagonist• But, antagonism is restricted to μ-
receptor only and agonist of κ-receptor
• Drawbacks - dysphoria andpsychomimetic effects

Pentazocine• Weak α-receptor antagonist, but agonist of κ-receptor• One of the commonly used agents, given orally and IM• Low abuse liability• Pharmacokinetics:
– High 1 pass metabolism but effective orallyst
– Half life = 3-4 Hrs– Metabolized in liver by glucoronide conjugation– Dose: orally 50-100 mg and parenterally 30-60 mg IM
• Uses:Moderately severe pain in Injury, Burns, FractureTrauma, Cancer and Orthopaedic manuevers
(Fortwin, Fortagesic)

Pentazocine Vs Morphine• Spinal analgesia via kappa receptor• Dose is 30 mg Vs 10 mg and low ceiling effect• Sedation and Respiratory depression at lower doses• Tachycardia and rise in BP – dangerous in MI• Lesser smooth muscle spasms• Vomiting and other side effects are less• Subjective effects – lower ceiling (psycomimetic effects)• Tolerance develops on repeated use, but lesser than
Morphine• Withdrawal symptoms – both Morphine and Nalorphine like• Good analgesic in subjects not exposed to Morphine• Precipitate withdrawal – in Morphine addicts

Buprenorphine• Synthetic thebaine congener and highly lipid soluble• Given Sublingually or parenterally but not oral – high 1 pass st
metabolism• Selective μ-agonist analgesic• 20-30 times more potent than Morphine• Slow but longer duration of action upto 24 Hrs• Pharmacological effects are similar to Morphine• Has ceiling effect in analgesic and respiratory depression• Good analgesic for naive patients but addicts – precipitates
withdrawal syndrome• Lower tolerance and physical dependence than Morphine and abuse
liability• Withdrawal syndromes are similar to Morphine

Buprenorphine – contd.• Adverse Effects:
– Hypotension (Postural)– Respiratory depression (fatal in neonates) and cannot be
reversed by Naloxone• Uses:
– Long lasting painful conditions – cancer– Postoperative pain– Myocardial infarction
• Preparations: Norphine, Tidigesic• 0.3 mg/ml injections and 0.2 mg sublingual tablets

Naloxone• Competitive antagonist of all types of opioid
receptors• But, blocks μ-receptors at much lower dose• Always injected IV (0.4 t0 0.8 mg) - All symptoms
of Morphine action are antagonized – respiratorystimulation
• At higher doses 4-10 mg: antagonizes actions ofNalorphine and Pentazocine – dysmorphic andpsychomimetic effects are not suppressed (δ)
• Withdrawal symptoms: 0.4 mg doses – Morphineand 4-5 mg doses – Nalorphine and Pentazocine

Naloxone – contd.• Buprenorphine actions are prevented but not
reversed fully – tight bond with receptors• Also acts on endogenous opioids• Antagonizes respiratory depression of Diazepam
and N O2
• Uses:• Acute Morphine Poisoning (0.4 – 0.8 mg IV 2-3 min,maximum 10 mg.
• New Born – opioid poisoning• Reverse respiratory depression intr-aoperatively• Diagnosis of Morphine addiction• Alcohol intoxication



SAR - Opioids(Phenolic)
(Alcoholic) HeroinCodeineMorphine