Page 1 Page 274 Pelvis and Sacrum: Where It All Comes...
14
Page 274 Pelvis and Sacrum: Where It All Comes Together 2010 AAO Convocation Presentation to American Academy Osteopathy Convocation 2010 Charles J Smutny III, DO FAAO and Bryan Larsen PhD Des Moines University M M i R ia E n t e r p r i s e Medical Research and Informatics Informatics Management Disclosure: I have received funding from the AAO to I have received funding from the AAO to support the creation and testing of the electronic SOAP note (eSOAP). Page 1
Transcript of Page 1 Page 274 Pelvis and Sacrum: Where It All Comes...

Page 274 Pelvis and Sacrum: Where It All Comes Together 2010 AAO Convocation
Presentation to American Academy Osteopathy Convocation 2010Charles J Smutny III, DO FAAO andBryan Larsen PhDDes Moines University
MMiRiaE n t e r p r i s e
Medical Research andInformatics Informatics Management
Disclosure:
I have received funding from the AAO toI have received funding from the AAO tosupport the creation and testing of the
electronic SOAP note (eSOAP).
Page 1

2010 AAO Convocation Pelvis and Sacrum: Where It All Comes Together Page 275
Why this guy Smutny?:
I suspect that the Goddess Dionysus had something to do with this.
I am a self proclaimed Physician/Philosopher with experience in Osteopathic Medicine as a Professor, Practitioner , Teaching clinician and Neuromusculoskeletal Medicine Residency Director. My life experience includes teaching and studying Secondary education Sciences, medical education Basic Sciences and Clinical Sciences, Information Technology
d h i l i iand mechanical engineering.
I am indebted to the osteopathic profession for the many opportunities it has provided for me to grow as a professional and as a human being.
I am a volunteer on behalf and for the professionI am a scientific observer of and for the profession
I’ve been working on THIS project for more than 10 years
Observations:
The osteopathic profession deserves more respect than it has gottenThe osteopathic profession needs EBM validation of its methods
As does all of medicine A lack of common parlance has limited aggregation of findings
Physician investigators have been few in the osteopathic professionPractitioners have limited time for validating their methodsPractitioners have limited time for validating their methods
The LBORC created a paper SOAP note to consistently record OMTRecognized that SOAP could lead to validation of OMT methods
Realized this in many studies where the paper SOAP was used for data collection
Recognized SOAP could have an electronic incarnation (1998)
Whoa Nellie! Fight the Seduction of Financial Incentives for EHRs Modern Medicine 10/2009
No, Don’t but an EMR now! Yes, Buy an EMR now!? Medscape 8/2009 From Journal of HITEMR now!? Medscape 8/2009 From Journal of HIT
EHRs fix everything myths and 9 other myths. FPM 14(3) 2007, AAFP
New guidelines address safe Electronic record use. AHRQ via Medscape 9/2009
Electronic Personal Health Records, should Doctors worry? Medscape 10/2008 abstracted from Modern Medicine
Page 2

Page 276 Pelvis and Sacrum: Where It All Comes Together 2010 AAO Convocation
Choosing and implementing an electronic health record. This subject is in most medical journals totaling “n?” times a year.1.2 billion in grants approved 9/2009. Grants include $598 million to set up some 70 health information technology centers to help healthcare institutions acquire electronic health record systems and $564 million to develop a nationwide system of health information networks, Vice President Joe Biden's office said in a White House statement.
Some thoughts:Whose, where, how much, what kind of networks, who has access,
how do you get access, who owns the data, how can the data be used, what is the penalty for mis-use?
American Recovery and Reinvestment Act dubbed the Health Information Technology for Economic and Clinical Health (HITECH) Act.April 9 2009 NEJM questions the terms “meaningful use” (Clinical or cost effectiveness and which first?)
Stimulus package has Billions for Healthcare 3/2009 (where? Do the math!)
Personal data safety?Where should the controls lie or with whom?What data is necessary for national decision making an why?g yWhat protects the patient from data assaults?Language of network interchange? (UMLS)
What is making clinical a decision based on?How do we the people, indisputably support Tort Reform, fight insurance inflation and protect our rights as patients?
Page 3

2010 AAO Convocation Pelvis and Sacrum: Where It All Comes Together Page 277
Evidence Based Medicine (EBM)The Cost of the current standard Randomly Controlled Trials (RCT)
Also begs the question, what is a valid controlOutcomes studies and numbersPooled data collectionMultivariate analysis - statistics in extremely large cross sectional studies with 1000’s of variables (truly a Phase IV or real world study)
Randomized controlled clinical trials are and will continue to be the foundation for evidence-based medicineThe rigor demanded by such studies is arduous and time g yconsuming and may not be doable in the context of busy practicesThe number of patients in an RCT is usually in the dozens; hundreds for multi-center trialsYet, we urge clinicians to participate in clinical research projects – but there are relatively few clinicians who consistently produce primary research, especially in OMT
Requires the aggregation of multiple RCTsRigorous inclusion of RCTs for aggregation
i d f i trequired for consistencyConsistency requires common parlance and common methods applied uniformly
But these don’t readily fit the osteopathic paradigm, philosophy or practical reality
Page 4

Page 278 Pelvis and Sacrum: Where It All Comes Together 2010 AAO Convocation
It is a tall order for OMT office based practitioners (or any other private clinician) to conduct RCTs and also productively practice medicineIt i ll th t ibilit f OMTIt is all the more remote a possibility for many OMT practitioners (and clinicians in general) to band together for multi-center clinical trials related to (OMT) practice in support of true EBM
We can lament -- or find other approaches (sit or get off the *?@#$^*&)
some clinical questions could be answered from already existing data?the pre-existing data involved an impressive number (thousands) of records?number (thousands) of records?many clinicians could contribute to the creation of useful clinical data without disrupting their clinical practice?such data addressed clinical questions specific to the osteopathic profession as well as traditional medicine?
Wouldn’t that be great?
But what form should data take?But what form should data take?
Page 5

2010 AAO Convocation Pelvis and Sacrum: Where It All Comes Together Page 279
Retrospective Medical Record Review
Prospective Clinical Study Focusing on Specific Data Elements
Study Types
Disease RegistryWith Limited Fields
Extensive Database of Clinical Data Without Reference to a Particular Condition
The Osteopathic eSOAP(it’s where data comes from)
• By DO’s – For DO’s• A tool and an EHR with a difference• Embedded osteopathic language and UMLS
languagelanguage– OMT mainly in the structural exam– New neuromuscular module being added
• Consistent with holistic approach– 4000 data fields allow recording “virtually anything”
• Sensitive to constraints of clinical practice– Clinicians can use as much or as little of the record
as they need
Navigation Pane
Physician and Practice Information
(NPI)
Patient Information
Subjective
Objective
Assessment
Billing ReportsAnd
Standardized Communications
Documents
PQRI, CAP Extraction
Add-on Modules
Patient Information
Quick SummariesAllergies, Vitals
Problem ListTicklers
Plan
Documents
Page 6

Page 280 Pelvis and Sacrum: Where It All Comes Together 2010 AAO Convocation
The Navigation Pane
Page 7

2010 AAO Convocation Pelvis and Sacrum: Where It All Comes Together Page 281
Page 8
Page 282 Pelvis and Sacrum: Where It All Comes Together 2010 AAO Convocation
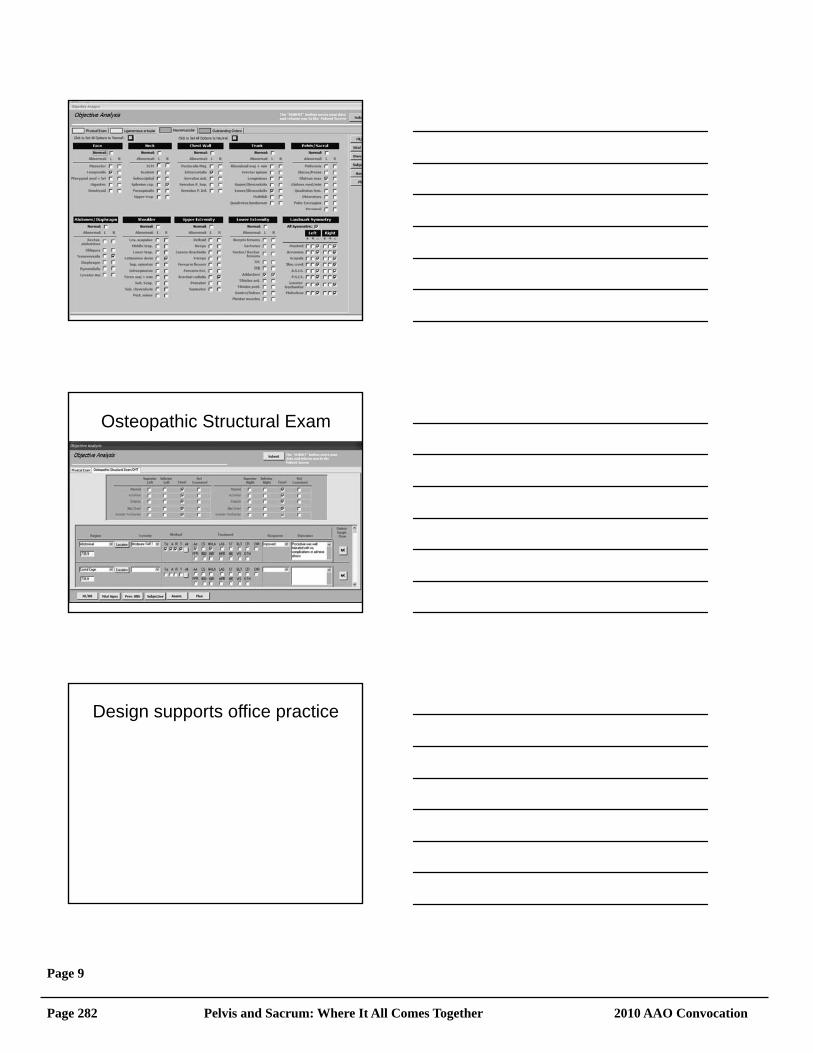
Osteopathic Structural Exam
Design supports office practice
Page 9

2010 AAO Convocation Pelvis and Sacrum: Where It All Comes Together Page 283
Other Value-added Tools
Fully customizable “problem list”Problem list means different things to different people
Other value-added tools
Record EditingAnd Locking
Special PurposeModules
Details of the eSOAP tabs• Subjective
– CC/HPI memo specifics– ROS– PMH/FSH
• Including preventive health summaries
• Assessment – Contains autofilling of ICD9
codes for osteopathic diagnoses and link to look up table for other diagnoseshealth summaries
• Objective– Physical Exam
• Each element with 2o
screens– Osteopathic structural
exam with OMM record– Neuromuscular exam– Cranial exam
• Plan– General Plan– Scoring– Coding
Page 10

Page 284 Pelvis and Sacrum: Where It All Comes Together 2010 AAO Convocation
Report Engine• 4 kinds of reports currently available
– Assessment Report is the summary of all positive findings that will go on the patient’s record (a review before closing the record)
Billi R t t i 1997 E&M id li– Billing Report contains 1997 E&M guidelinecalculations for diagnostic coding suggestions for the business office and insurance records
– Pharmacy Report– a prescription pad generating faxable RX’s
– A Narrative Report- A systematic defensablebasis for a complete narrative report
On screen real-time scrolling assessment reportElectronic transfer of Rx to pharmacy
Practicing PhysicianAuthorized
Researchers
eSOAP(Access)
Upload Module(Data Stays in
Physician/Patient Control)
Middle WareInterface (.net)
NODSQL Server
Plain EnglishQuery Engine
AdministratorExpert Researcher
Page 11

2010 AAO Convocation Pelvis and Sacrum: Where It All Comes Together Page 285
Evidence PyramidMeta-Analysis
Systematic Review Secondary Analysis OfData SetsNational Osteopathic
Database
Randomized Controlled Trial
Cohort studies
Case Control studies
Case Series/Case Reports
Animal research
What Secondary Data Analysis Promises
• The eSOAP is used as a data collection tool for physicians engaged in research
• The eSOAP is used for recording patient encounters in regular clinical practiceg p
• The eSOAP becomes familiar to osteopathic medical students and residents
• Clinicians upload de-identified records to the NOD• Researchers mine the NOD data• Analysis of mined data demonstrates quality of care,
efficacy of outcomes, and helps define areas of research needs
Page 12

Page 286 Pelvis and Sacrum: Where It All Comes Together 2010 AAO Convocation
Q1 how many records? 65000Q2 how many are male? 35000Q h 8 ?Q3 how many are >85 yrs? 3500Q4 how many had hip replacement? 400Q5 how many have decreased ADL? 210Q5 how many receive congregate meals? 104Q6 how many do not drive 96Q7 how many receive have dx CHF <20
Messages to Go
Uniform consistent and common terminology is critical for databases and registries that are useful
Paper and electronic soapnotes enforce common usage. Limiting non specificity
The National Osteopathic Database can accept deidentified records with most fields
When sufficient data is banked, data mining to establish efficacy is possible
Questions
• Is the eSOAP an EMR? • Is it for the solo practitioner?• Is it a tool for the individual researcher?• Is it mainly for the profession, to create a
national data base? Not anymore!• Might it be a teaching tool for OMS?• How much re-engineering is needed for each of
the above?• How will costs be covered?
Page 13

2010 AAO Convocation Pelvis and Sacrum: Where It All Comes Together Page 287
E-SOAP …. can we afford not to do this?What costs would you personally be able to support?
Cost of ownershipCost of renewals an updates
Would you be willing to suggest design considerations bi-annually for a discount on costs?Please take an index card and submit your answers!
Page 14