Paediatric respiratory tract infection surveillance: a...
18
14 March 2017 1 Paediatric respiratory tract infection surveillance: a community-based feasibility inception cohort study Emma C. Anderson 1, 2 , Suzanne M. Ingle 1, 2 , Peter Muir 1, 3 , Charles R. Beck 1, 2, 4 , John P. Leeming 5 , Christie Cabral 1, 2 , Joanna M. Kesten 1, 6 , and Alastair D. Hay 1, 2 bristol.ac.uk/eepris 1 NIHR Health Protection Research Unit in Evaluation of Interventions, University of Bristol 2 School of Social and Community Medicine, University of Bristol 3 Public Health England, Specialist Virology Centre, Bristol 4 Field Epidemiology Service, Public Health England, Bristol 5 North Bristol NHS Trust, Bristol Centre for Antimicrobial Research and Evaluation (BCARE) 6 NIHR Collaboration for Leadership in Applied Health Research and Care West (NIHR CLAHRC West) at University Hospitals Bristol NHS Foundation Trust, Bristol, UK
-
Upload
truongthuan -
Category
Documents
-
view
223 -
download
0
Transcript of Paediatric respiratory tract infection surveillance: a...

14 March 2017
1
Paediatric respiratory tract infection surveillance: a
community-based feasibility inception cohort study
Emma C. Anderson 1, 2, Suzanne M. Ingle 1, 2, Peter Muir 1, 3, Charles R. Beck 1, 2, 4,
John P. Leeming 5, Christie Cabral 1, 2, Joanna M. Kesten 1, 6, and Alastair D. Hay 1, 2
bristol.ac.uk/eepris
1 NIHR Health Protection Research Unit in Evaluation of Interventions, University of Bristol 2 School of Social and Community Medicine, University of Bristol 3 Public Health England, Specialist Virology Centre, Bristol 4 Field Epidemiology Service, Public Health England, Bristol 5 North Bristol NHS Trust, Bristol Centre for Antimicrobial Research and Evaluation (BCARE) 6 NIHR Collaboration for Leadership in Applied Health Research and Care West (NIHR CLAHRC West) at
University Hospitals Bristol NHS Foundation Trust, Bristol, UK

Background
• Burden of infectious diseases + children + RTIs
• Antimicrobial resistance
• Most research conducted at presentation
• Research needed to better understand: - who acquires infections (and why),
- natural history of infections among non-consulters,
- who consults (and why) and
- how to develop self care interventions
• Feasibility of recruitment & retention to community cohort study
2
bristol.ac.uk/eepris
14 March 2017

Aims
1. Establish feasibility of (predominately online) recruitment and retention to a
paediatric RTI community surveillance study
- with collection of syndromic and microbiological data
2. Estimate for community RTIs in children:
- symptom duration
- primary care consultation rates
3 3
14 March 2017
bristol.ac.uk/eepris
virus data

Methods
4
bristol.ac.uk/eepris
14 March 2017
Participants: Immunocompetent children ≥3 months to ≤14 years +parents/carers
Recruitment: (mainly) letters from GP surgeries in the Bristol area - Also: reminder letter, text, posters and cards in GP surgeries, UoB website, ‘snowball’ recruitment
Timeline: Enrolment end Feb–early June 2016 (staggered); no new RTIs after July
Enrolment: • Parent returns paper consent form in post to study team • Tel call (admin) to check eligibility and explain study process • Eligible parent emailed a link to complete baseline data online

14 March 2017
bristol.ac.uk/eepris
Data collection (1)
1. Parents provided baseline data online for eligible child/ren = Recruited - child characteristics, household demographics, health anxiety
2. Parents replied to weekly email (link). Yes = New study RTI
- confirm absence/presence of “new RTI” symptoms
5

14 March 2017
bristol.ac.uk/eepris
Data collection (2)
3. Once symptomatic:
- Parents - daily data online (symptoms severity)
- RN home visit - swabs (nasal & saliva) -> take to lab on ice (ideal)
- Parents took swabs (intended no help from RN) -> post to lab (pragmatic)
4. On recovery (parent-reported 2 days symptom free):
- Parents took (asymptomatic) swabs -> post to lab, final questions
5. Primary care medical notes review
- Medical history and consultation details for children with RTI
6

Results - recruitment
• 10 GP surgeries took part, 5 sent mailout
• Parent/carer of 10,310 children invited (94% no response)
- reminder letter sent from 4 surgeries to 8,401
- reminder text sent from 2 surgeries to 1543
• 485 children enrolled (4.7% of invited) from 331 families
7
bristol.ac.uk/eepris
14 March 2017

8
14 March 2017
bristol.ac.uk/eepris
Results - recruitment
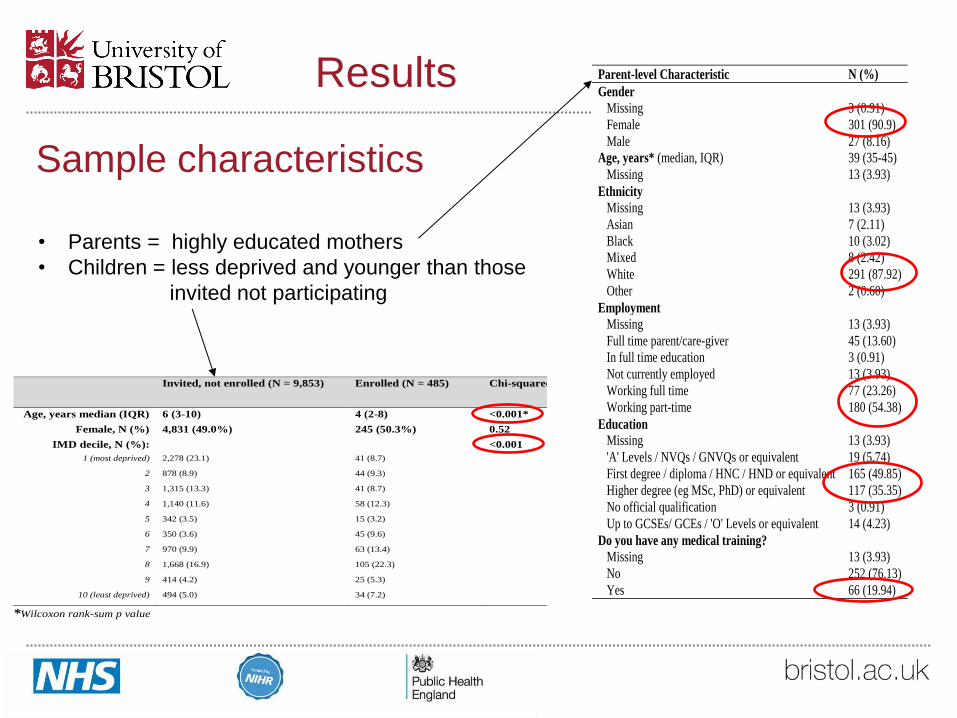
Sample characteristics
9
04 April 2017
Invited, not enrolled (N = 9,853) Enrolled (N = 485) Chi-squared p-value
Age, years median (IQR) 6 (3-10) 4 (2-8) <0.001*
Female, N (%) 4,831 (49.0%) 245 (50.3%) 0.52
IMD decile, N (%):
<0.001
1 (most deprived) 2,278 (23.1) 41 (8.7)
2 878 (8.9) 44 (9.3)
3 1,315 (13.3) 41 (8.7)
4 1,140 (11.6) 58 (12.3)
5 342 (3.5) 15 (3.2)
6 350 (3.6) 45 (9.6)
7 970 (9.9) 63 (13.4)
8 1,668 (16.9) 105 (22.3)
9 414 (4.2) 25 (5.3)
10 (least deprived) 494 (5.0) 34 (7.2)
*Wilcoxon rank-sum p value
Results Parent-level Characteristic N (%)
Gender
Missing 3 (0.91)
Female 301 (90.9)
Male 27 (8.16)
Age, years* (median, IQR) 39 (35-45)
Missing 13 (3.93)
Ethnicity
Missing 13 (3.93)
Asian 7 (2.11)
Black 10 (3.02)
Mixed 8 (2.42)
White 291 (87.92)
Other 2 (0.60)
Employment
Missing 13 (3.93)
Full time parent/care-giver 45 (13.60)
In full time education 3 (0.91)
Not currently employed 13 (3.93)
Working full time 77 (23.26)
Working part-time 180 (54.38)
Education
Missing 13 (3.93)
'A' Levels / NVQs / GNVQs or equivalent 19 (5.74)
First degree / diploma / HNC / HND or equivalent 165 (49.85)
Higher degree (eg MSc, PhD) or equivalent 117 (35.35)
No official qualification 3 (0.91)
Up to GCSEs/ GCEs / 'O' Levels or equivalent 14 (4.23)
Do you have any medical training?
Missing 13 (3.93)
No 252 (76.13)
Yes 66 (19.94)
• Parents = highly educated mothers
• Children = less deprived and younger than those
invited not participating
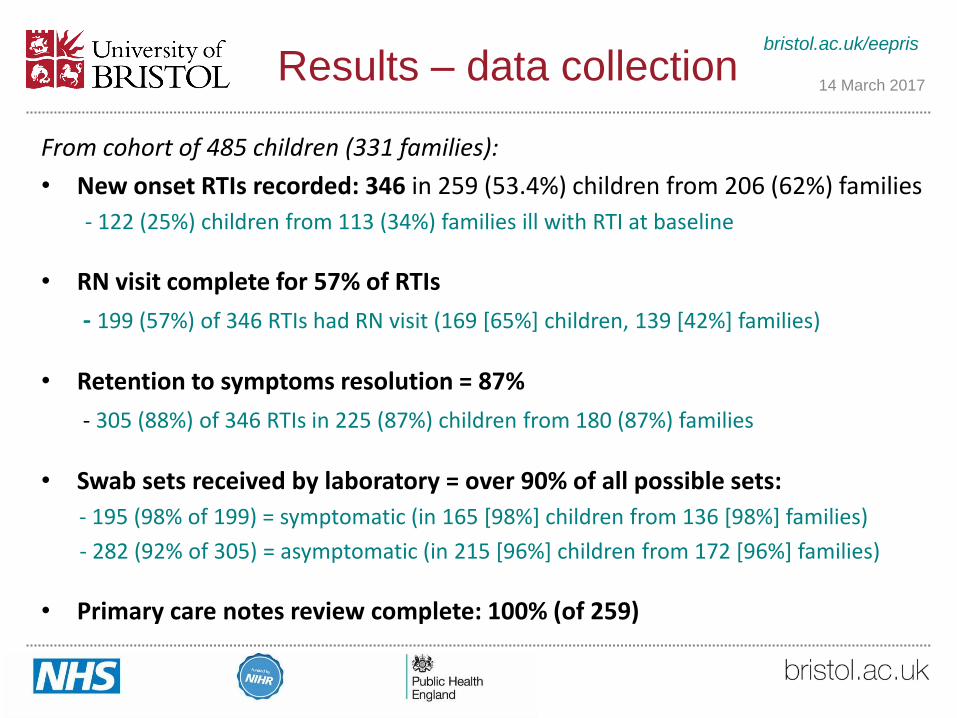
Results – data collection
From cohort of 485 children (331 families):
• New onset RTIs recorded: 346 in 259 (53.4%) children from 206 (62%) families
- 122 (25%) children from 113 (34%) families ill with RTI at baseline
• RN visit complete for 57% of RTIs
- 199 (57%) of 346 RTIs had RN visit (169 [65%] children, 139 [42%] families)
• Retention to symptoms resolution = 87%
- 305 (88%) of 346 RTIs in 225 (87%) children from 180 (87%) families
• Swab sets received by laboratory = over 90% of all possible sets:
- 195 (98% of 199) = symptomatic (in 165 [98%] children from 136 [98%] families)
- 282 (92% of 305) = asymptomatic (in 215 [96%] children from 172 [96%] families)
• Primary care notes review complete: 100% (of 259)
10
bristol.ac.uk/eepris
14 March 2017
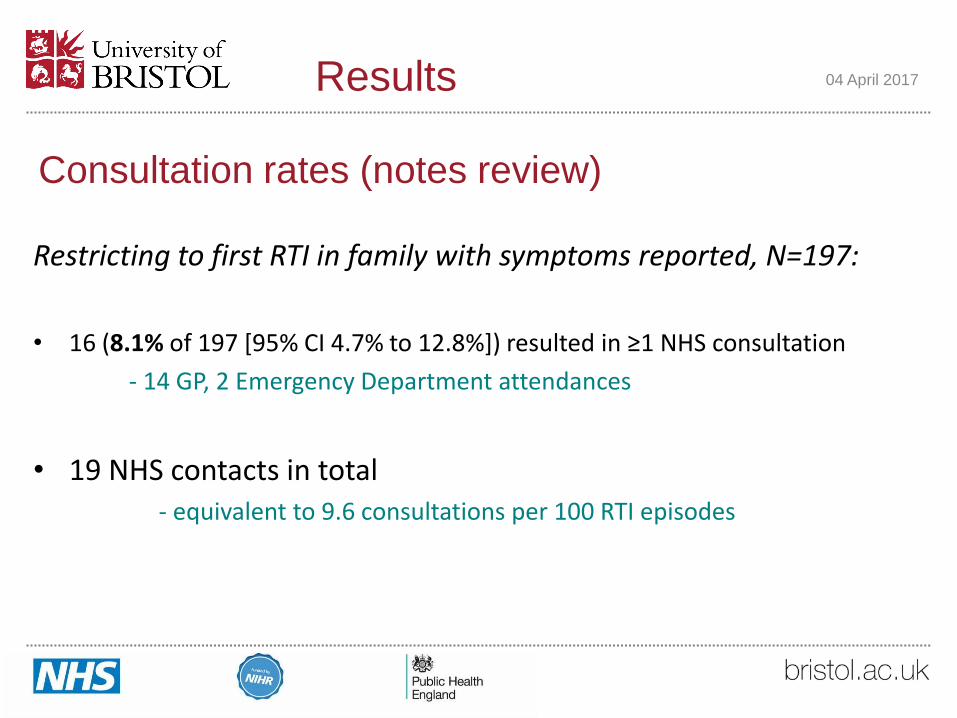
Consultation rates (notes review)
Restricting to first RTI in family with symptoms reported, N=197:
• 16 (8.1% of 197 [95% CI 4.7% to 12.8%]) resulted in ≥1 NHS consultation
- 14 GP, 2 Emergency Department attendances
• 19 NHS contacts in total - equivalent to 9.6 consultations per 100 RTI episodes
11
04 April 2017 Results

Symptoms duration (parent-reported)
RTI duration (days) by percentile
All 10th 25th 50th 75th 90th p-valuea
All (first RTIs per family) children 197 4 7 9 14 23 -
Consultingb and non-consultingb children
Consultingb 16 6 9 13 18 37 0.06
Non-consultingb 181 4 6 9 13 21
Upper and lower respiratory tract infection
Exclusively upperd RTI symptoms 86c 3 5 8 11 15 <0.001
Any lowerd RTI symptoms 104c 6 8 12 18 29.5
Constitutional symptom severity (mean maximum) scoree by upperd and lowerd RTI
Upperd RTI Lowerd RTI
Fever 0.55 1.07
Fatigue 0.83 1.71
Disruption to sleep 1.15 2.19
Disruption to other activities 0.67 1.43
12
04 April 2017
a Log-rank test for difference between consulting and non-consulting episodes b Any NHS (primary and secondary care) attendance according to medical notes
Restricting to first RTI in family with symptoms reported, N=197:
Results
• Median RTI duration = 9 days (IQR 7-14 days) • 23 days for resolution of symptoms in 90% children (95% CI 85%-94%)
• Weak evidence: consulting children longer duration than non-consulting
Conclusion
• Community infection surveillance is feasible
- Low response rates
- Less deprived families with younger children more likely to respond
- Excellent retention - Symptom data, Microbial data
• Novel evidence of consultation rate per community illness:
- Parents seek primary care support in around 1 in 12 RTI episodes
• Community RTI duration similar to duration gained from consulting populations (previous research)
• Parent-reported LRTI symptoms are prognostically significant
- longer duration, more severe symptoms
13
bristol.ac.uk/eepris
14 March 2017

Questions?
14
Acknowledgements
This research was partly funded by the NIHR Health Protection Research Unit
in Evaluation of Interventions at University of Bristol.
The views expressed are those of the author(s) and not necessarily those of the
NHS, the NIHR, the Department of Health or Public Health England.
bristol.ac.uk/eepris
bristol.ac.uk/eepris
14 March 2017

15
04 April 2017
URTI
LRTI
systemic
Results – LRTI vs URTI

16
04 April 2017
0.0
00
.25
0.5
00
.75
1.0
0
0 20 40 60 80analysis time
cluster = Exclusively URTI cluster = Mix
cluster = Exclusively LRTI cluster = Neither URTI or LRTI
Kaplan-Meier survival estimates
LRTI longer duration
median = 8 vs 12 days*
*P<0.001
Results – LRTI vs URTI

Severity of systemic symptoms
17
04 April 2017
Slide 17 of 17
bristol.ac.uk/eepris
Results – LRTI vs URTI
Upper and lower respiratory tract infection
Exclusively upperd RTI symptoms 86c 3 5 8 11 15 <0.001
Any lowerd RTI symptoms 104c 6 8 12 18 29.5
Constitutional symptom severity (mean maximum) scoree by upperd and lowerd RTI
Upperd RTI Lowerd RTI
Fever 0.55 1.07
Fatigue 0.83 1.71
Disruption to sleep 1.15 2.19
Disruption to other activities 0.67 1.43
Restricting to first RTI in family with symptoms reported, N=197
c 7 RTI episodes which did not report any URTI or LRTI-defining symptoms d Parent reported upper RTI symptoms: earache, sore throat, runny/blocked nose, ear discharge, dry cough or barking/croupy cough.
Parent reported lower RTI symptoms: wet/productive cough, breathing faster/shortness of breath, or wheeze/whistling chest e Maximum of daily scores in first 21 days, based on Likert scale zero (‘normal, no problem’) to six (‘as bad as it could be’)

The EEPRIS Study Team
18
31 October 2016
Professor Alastair Hay – Chief Investigator
Emma Anderson – Study Manager
and clinician interview lead
Anna Gilbertson – Research Nurse
Penny Seume – Administrator
Co-investigators Dr Suzanne Ingle – statistician, University of Bristol (UoB)
Dr Peter Muir – microbiology lead, Public Health England (PHE)
Dr Charles Beck – (PHE) – infection surveillance/ PHE advice
Dr John Leeming (UoB) – microbiology advice
Professor Adam Finn (UoB) – HPRU microbiology advice
Dr Jo Kesten (UoB) – qualitative lead for parent/child interviews
Collaborators Dr Christie Cabral (UoB) – qualitative advisor
Dr Isabel Lane (UoB) – clinician interviews, intervention development
Dr Katy Turner (UoB) – RTI modelling implications advice
Dr Jennifer Oliver (UoB) – HPRU microbiology advice
Professor William Hollingworth (UoB) – health economics advice
Dr Hannah Thornton (UoB) – microbiological methodology advice
Dr Isabel Oliver (PHE) – PHE perspective
Dr Richard Puleston (PHE) – epidemiology advice
Dr Paul Cleary (PHE) – epidemiology advice
Dr Tim Moss – Qualitative research/ health psychology advice,
Doctoral supervisor for Emma Anderson
Sue Milner – Research Nurse
Slide 18 of 17
bristol.ac.uk/eepris