.p ,-r - fac.ksu.edu.sa · cholesteatoma, or impaded cerumen of keratosis obturans. Bellinger8 has...
3
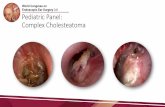
103 Temporomandibular joint ankylosis caused by mastoiditis: Presentation of a rare case and literature review Abdulaziz AI Weteidt, BDS,MSc Asma El Ekrish*, BDS Khalid AI Mutairi*, BDS Sultan AI Foghm*, BDS ~L>.rl} y-hJ1 ~I <b......ly /J...dl ~I ~I;S )- J-\5' }";;",,"..I;-'-"Y' .j-J...dl~I ~I JWI, ~ ~ ~"" <.,;c y..<..JS' ~ JW'JI _.s:..:.~IJ')' ~I....., JA-JI..:.LJI~ ,-'-'-,I)')' ~1J'.r'l.jJ;, JA-JI..:.LJI..?~,-",,",)Ir-":4:--. ~I JWIC)r-"\......i.:,JI)"-'WIj'..I;..w1 J!~.:,JI), ,,-,WJJ.Ij'..I;..wIC)~~ ~ r-/J...dI~I~IJWICJ\>.)~L,..-i. ~ ,~)~ ..,..,...,)i,~4:l~, ..?r-U~....a:,.)i . ,\...:.J-I) ~ )1 .):,')lJ ~j::\1 ~4:l'J1 ...".., J\5' .kklS.u .j-J...dl~I ~I JW'J ;~'c <Jl>- L>..?~ .~4:l'JI)..?)1 c/' JW~ <,....,!)i yL.- 'Ji -:...;\5' C')'-JI cJl:; . ~~ <,'-J...dl u..:...J1 .p J>-I..I.:lI) ~ r-.1.e ..:r,:L.oL.J.1 .:,,:......illl <..;,L.:....,I) ...,...;LJ,.I ..;G ~I ~I J~I j' --.J\; c'Y-J1) . <.,>-I.f-I ;,L.-I..ul j' ~.w r-' ,-r )..w.~1 C:'-' <.,;\5:...!) <>...".c) <J~ Ankylosis is a Greek word meaning a stiff joint. Temporomandibular joint ankylosis is the development of complete or incomplete limitation of movement of the temporomandibular joint by bone or fibrous tissue. There are many predisposing factors that contribute to ankylosis, including age of the patient, trauma to the mandible, damage to the articular disc and duration of immobilization foilowing fracture of the mandible. The articular disc can be damaged by trauma, infection or neoplasm. The etiology and treatment of temporomandibular joint ankylosis have been well documented in the literature, with trauma and infection being the leading causes. A rare case of temporomandibular joint ankylosis in a young girl is presented. It was an infection sequela following otitis media and mastoiditis. Treatment consisted of resecting the ankylosed joint, bilateral coronoidectomy and replacement of the resected condyle with a costochondral graft and an interpositional temporalis muscle graft. Treatment outcome was satisfactorily successful with a mouth opening of 3.2 cm two years following the surgery. Case Report A seven-year old Saudi girl was admitted to the Riyadh Dental (enter because of limitation of mouth opening which started when she was two years old. Her father said that she had an abrupt onset of fever at the age of 18 months and a concomitant swelling of the left post-auricular region after contrading measles. She then developed progressive restriction of mouth opening. At first presentation, the maximum inter- incisal distance was 10 mm with deviation of the mandible to the left side with opening of about 3-4 mm (Fig. 1). There was no history of trauma and no scar was visible in the mental or submental region. A post-auricular scar indicated that she was treated for acute mastoiditis (Fig. 2). Radiographic exami- nation (ortho-pantomograph, eT scan-axial and coronal) showed a deformed, mushroomed left condyle with both coronoid processes elongated (Fig.3). The patient was taken to the operating room Received 25 Sept. 1999; Revised 04 Dec. 1999; Accepted 27 Feb. 2000 tChairman and Senior Registrar; 'Resident, Dept. of Oral and Maxillofacial Surgery, Riyadh Dental Center Riyadh Medical Complex Saudi Dentai Journal, Vol. 12, No. 2, May - August 2000 FIQ. 1. At initial presentation, the maximum inter incisal distance was 10 mm with a significant deviation of the mandible to the left side on opening. where a left condyledomy and coronoidedomy were performed through an Alkayat & Bramly approach including stripping of the muscles attached to the left ramus and angle of the mandible. The contralateral coronoid process was Address reprint requests to: Dr. Abdulaziz AI Weteid PO Box 22455 Riyadh 11495, KSA
Transcript of .p ,-r - fac.ksu.edu.sa · cholesteatoma, or impaded cerumen of keratosis obturans. Bellinger8 has...

103
Temporomandibular joint ankylosis caused by mastoiditis:Presentation of a rare case and literature review
Abdulaziz AI Weteidt, BDS,MScAsma El Ekrish*, BDS
Khalid AI Mutairi*, BDSSultan AI Foghm*, BDS
~L>.rl} y-hJ1 ~I <b......ly/J...dl ~I ~I;S )- J-\5' }";;",,"..I;-'-"Y' .j-J...dl~I ~I JWI, ~ ~ ~"" <.,;cy..<..JS'~ JW'JI_.s:..:.~IJ')' ~I....., JA-JI..:.LJI~ ,-'-'-,I)')' ~1J'.r'l.jJ;, JA-JI..:.LJI..?~,,-",,",)Ir-":4:--. ~I JWIC)r-"\......i.:,JI)"-'WIj'..I;..w1
J!~.:,JI), ,,-,WJJ.Ij'..I;..wIC)~~ ~ r-/J...dI~I~IJWICJ\>.)~L,..-i. ~ ,~)~ ..,..,...,)i,~4:l~, ..?r-U~....a:,.)i. ,\...:.J-I)~ )1 .):,')lJ ~j::\1 ~4:l'J1 ..."..,J\5'.kklS.u .j-J...dl~I ~I JW'J ;~'c <Jl>-L>..?~ .~4:l'JI)..?)1 c/' JW~ <,....,!)iyL.- 'Ji
-:...;\5'C')'-JIcJl:; . ~~ <,'-J...dlu..:...J1.p J>-I..I.:lI)~ r-.1.e ..:r,:L.oL.J.1.:,,:......illl<..;,L.:....,I)...,...;LJ,.I..;G ~I ~I J~I j' --.J\; c'Y-J1). <.,>-I.f-I;,L.-I..ul j' ~.w r-' ,-r )..w.~1 C:'-' <.,;\5:...!)<>...".c)<J~
Ankylosis is a Greek word meaning a stiff joint. Temporomandibular joint ankylosis is the development of complete or incompletelimitation of movement of the temporomandibular joint by bone or fibrous tissue. There are many predisposing factors thatcontribute to ankylosis, including age of the patient, trauma to the mandible, damage to the articular disc and duration ofimmobilization foilowing fracture of the mandible. The articular disc can be damaged by trauma, infection or neoplasm. The etiologyand treatment of temporomandibular joint ankylosis have been well documented in the literature, with trauma and infection beingthe leading causes. A rare case of temporomandibular joint ankylosis in a young girl is presented. It was an infection sequelafollowing otitis media and mastoiditis.
Treatment consisted of resecting the ankylosed joint, bilateral coronoidectomy and replacement of the resected condyle with acostochondral graft and an interpositional temporalis muscle graft.
Treatment outcome was satisfactorily successful with a mouth opening of 3.2 cm two years following the surgery.
Case Report
A seven-year old Saudi girl was admitted to theRiyadh Dental (enter because of limitation ofmouth opening which started when she was twoyears old. Her father said that she had an abruptonset of fever at the age of 18 months and aconcomitant swelling of the left post-auricularregion after contrading measles. She thendeveloped progressive restriction of mouthopening. At first presentation, the maximum interincisal distance was 10 mm with deviation of themandible to the left side with opening of about 3-4mm (Fig. 1).There was no history of trauma and noscarwas visible in the mental or submental region.A post-auricular scar indicated that she was treatedfor acute mastoiditis (Fig. 2). Radiographic examination (ortho-pantomograph, eT scan-axial andcoronal) showed a deformed, mushroomed leftcondyle with both coronoid processes elongated(Fig.3).
The patient was taken to the operating room
Received 25 Sept. 1999; Revised 04 Dec. 1999;Accepted 27 Feb. 2000
tChairman and Senior Registrar; 'Resident, Dept. of Oral andMaxillofacial Surgery, Riyadh Dental CenterRiyadh Medical Complex
Saudi Dentai Journal, Vol. 12, No. 2, May - August 2000
FIQ. 1. At initial presentation, the maximum inter incisaldistance was 10 mm with a significant deviation of the
mandible to the left side on opening.
where a left condyledomy and coronoidedomywere performed through an Alkayat & Bramlyapproach including stripping of the musclesattached to the left ramus and angle of themandible. The contralateral coronoid process was
Address reprint requests to:Dr. Abdulaziz AI WeteidPO Box 22455Riyadh 11495, KSA

104
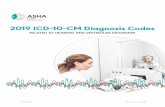
FI!;!. 2. Post auricular scar Indicating previous treatment foracute mastoiditis.
FI!;!. 3. Coronal cut of a scan showing a deformed,mushroom shaped left condyle.
Fig. 4. Intra-operative view showing maximum inter incisalopening (46 mm) after resedion of the left condyle
and both coronoid processes.
TEMPOROMANDIBULARJOINT ANKYLOSIS
Fig. 5. Passive mouth opening of 32 mm eighteen monthspost surgery.
reseded throu\;!h an intraoral approach. Anintraoperative interincisal distance of 46 mm wasachieved (Fi\;!. 4). A costo-chondral rib \;!raft wasfixed with wires to replace the reseded leftcondyle. An interpositional temporalis muscle\;!raft was used to aid in preventin\;! re-ankylosis.
The post-operative period was uneventful andthe patient was dischar\;!ed from the hospital onthe sixth post-operative day with a passive mouthinterincisal openin\;! of 35 mm. Ei\;!hteen monthslater, her mouth openin\;! was 32 mm with sli\;!htdeviation (less than 2 mm) of the mandible to theleft side while openin\;! (Fi\;!.5).
Discussion
Temporomandibular joint ankylosis is arelatively rare condition in the Western world,however hi\;!her incidences have been reported indeveloping countries. It is a serious condition thataffeds speech, dental health, masticatory fundionand can cause si\;!nificant secondary growthdeformities if untreated.1-J
A classification of ankylosis was proposed byKazanjian4 in 1938 that divided the disorder intotrue and false ankylosis. True ankylosis can becaused by a variety of conditions, with trauma andinfedion being the most common. Infedionswhich may lead to temporomandibular jointankylosis include osteomyelitis, adinomycosis,rheumatoid arthritis, diphtheria, typhoid,tonsillitis, mastoiditis, suppurative arthritis,measles, scarlet fever and otitis media.s
Straith6 has classified joint inflammation into
Saudi Dental Journal. Vol. 12, No. 2, May - Au~ust 2000
•

AL WETEID ET AL
those secondary to blood stream infection, thosesecondary to local inflammatory processes and toprimary inflammation of the joint. Otitis media is acommon complication of measles in children andit is a secondary infection by hemolyticstreptococci. It is reportedly more likely to affedthe temporomandibular joint if there is anobstrudion to the exit of pus, such as aural polyps,cholesteatoma, or impaded cerumen of keratosisobturans. Bellinger8 has pointed out thatsuppurative arthritis arising in the joint, frequentlycreates an exit into the external auditory meatuswhere it may be misdiagnosed as otitis media.Since only a thin plate of bone separates themiddle ear from the glenoid fossa, it seemsreasonable that otitis media can involve the joint ifthere isa barrier to the pus exiting the middle ear.
Mastoiditis and osteomyelitis of the temporalbone or mandible also are contributing fadors tothe development of temporomandibular jointankylosis. Infedions can spread from mastoiditisin three different ways: direct extension,thrombophlebitis and hematogenousdissem ination. The bony walls of the pneumatizedspace of the mastoid are important barriers to thespread of infedion. In the child, dense barriers ofbone may not be developed enough to preventthe spread of infedionJ However, theseinfections are in a state of decline as a result of thedevelopment of more effedive antibiotics. Kieth9and Wright and Moffet'O have emphasized thatgrowth and maturation chan~es are notcompleted in the temporomandibular joint untilthe second uecade of life. Between six monthsand two and one half years, the articular tubercleand glenoid fossa take on a mature appearancebut the articular eminence does not complete itsmature S-shape morphology until six to sevenyears of age.9 They also found that thetympanosquamosal fissure remains open mediallyand is divided into petrosquamosal andpetrotympanic fissures by the presence of thetegmen tympani. This could explain how thespread of infedion from the middle ear andmastoid reaches the temporomandibular joint. Inaddition, Moffet" stated that the tympanic platedoes not complete its ossification untilapproximately five years of age, thus providing apathway for the dired extension of infedion fromthe middle ear.
In a series of 44 cases of temporomandibularjoint ankylosis, Topazians reported that 19 caseswere associated with inflammation and four of
Saudi Dental Journal, Vo!. 12.No. 2.May - August 2000
105
them with otitis media. He pointed out that theincidence of trauma as an etiologic fador rangedfrom 26% to 75%, whereas the incidence ofinfedion ranged from 44% to 68%. Straith6 in 1948reported 16 cases of ankylosis in which six caseswere associated with otitis media and mastoiditis.
Heggie3 in a review of 24 cases of ankylosis statedthat seven cases were caused by infedion.Sleewaegen'2 reported that two of his five caseswere caused by inflammation, one of them beingosteomyelitis and the other otitis media. One caseof neonatal septicemia causing ankylosis has beenreported by Kennet.13 Finally, Haidar'4 reportedeight cases of ankylosis, all of which were causedby trauma to the temporomandibular joint.
References
1. Miller GA, PaQe HI and Griffith CR.Temporomandibular joint ankylosis: Review of theliterature and report of two cases of bilateralinvolvement.J Oral SurQ1975;33:792.
2. WilliamsJL, Rowe and Williams. Maxillofacial Injuries(2nd ed.). Churchill LivinQstone Vo!. 1,1994,440.
3. HeQQie AA. Concepts in the manaQement oftemporomandibular ankylosis. Ann RAustralas ColiDentSurQ 1996;13:132-5.
4. Kazanjian VH. Ankylosis of the temporomandibularjoint. AmJ Orthod 1938;24:1181.
5. Topazian RG. EtioloQY of ankylosis of thetemporomandibular joint: Analysis of 44 cases.JOralSurQ1964;22:227.
6. Straith CL and Lewis JR. Ankylosis of thetemporomandibular joint. Plast Reconstr SurQ1948;3:464.
7. Faer b er T H, En n i s RL and All e n GA .Temporomandibular joint ankylosis followinQmastoiditis: Report of a case. J Oral Maxillofac SurQ1990;48(8)866-70.
8. BellinQer DH. Temporomandibular ankylosis and itssurQical corrections. J Am Dent Assoc 1940; 27:1563.
9. Kieth DA. Development of the temporomandibularjoint. BrJOral SurQ1982;20:217.
10. WriQht DM and Moffet BC.The post-natal Qrowth ofthe human temporomandibular joint. Am J Anat1974;141:235.
11. Moffet B.The morphoQenesis of the temporomandibular joint. AmJ Orthod 1986; 52: 401.
12. SleewaeQen N et a!. Five cases of temporomandibular joint ankylosis in children. ActaStomatol BelQ1971;68: 95.
13. Kennet S.Temporomandibular joint ankylosis: Therationale for QraftinQ in the younQ patient. J OralSurQ 1973; 31: 744.
14. Haidar Z. Ankylosis of the temporomandibularjoint: Causes and manaQement. J Oral Med 1986;41: 246.
•