Outline of Patient Safety Huddle - hqinstitute.org · Outline of Patient Safety Huddle 1....
22
Outline of Patient Safety Huddle 1. Reflection 2. Safety Message/Slogan 3. Announcements 4. Boarding in ED. If yes, what support can we provide you to help resolve this? 5. Psychiatric holds in hospital o If yes, what support can we provide you to help resolve this? o What location? o Is there a sitter in place? 6. Patient Safety Issues/Concerns including: o Obstetrical o Perinatal o Medication Errors o Falls o Unexpected deaths o If yes on a-e, what actions need to occur today from our learning to avoid a re- occurrence of this issue? 7. Physician Safety Issues/Concerns What actions need to occur today from our learning to avoid a re-occurrence of this issue? 8. Caregiver Safety Issues/Concerns What actions need to occur today from our learning to avoid a re-occurrence of this issue? Does the issue need to be escalated to Employee Health? 9. How many patients have a length of Stay > 4 days (See documentation tool) 10. Delays of Service: What actions need to occur today from our learning to avoid a re-occurrence of this issue? 11. Code Blue/RRT Was the Code Blue/RRT well run? Are there any learning opportunities? 12. Did you experience any EMR related safety issues? 13. Plant Equipment Issues 14. Foleys (See documentation tool) 15. Central Lines (See documentation tool) 16. Skin Ulcers (See documentation tool) 17. Restraints (See documentation tool) 18. Recognition Add on themes on specific days: Tuesday: Review recruitment and open positions Wednesday: Close the loop on safety issues raised over the week Thursday: Review of Hand Hygiene, MDRO, CAUTI, CLABSI, SSI, HAPU, Falls Friday: HCAHPS and Patient Experience
Transcript of Outline of Patient Safety Huddle - hqinstitute.org · Outline of Patient Safety Huddle 1....

Outline of Patient Safety Huddle
1. Reflection
2. Safety Message/Slogan
3. Announcements
4. Boarding in ED. If yes, what support can we provide you to help resolve this?
5. Psychiatric holds in hospital
o If yes, what support can we provide you to help resolve this?
o What location?
o Is there a sitter in place?
6. Patient Safety Issues/Concerns including:
o Obstetrical
o Perinatal
o Medication Errors
o Falls
o Unexpected deaths
o If yes on a-e, what actions need to occur today from our learning to avoid a re-
occurrence of this issue?
7. Physician Safety Issues/Concerns What actions need to occur today from our learning to avoid a
re-occurrence of this issue?
8. Caregiver Safety Issues/Concerns
What actions need to occur today from our learning to avoid a re-occurrence of this issue?
Does the issue need to be escalated to Employee Health?
9. How many patients have a length of Stay > 4 days (See documentation tool)
10. Delays of Service: What actions need to occur today from our learning to avoid a re-occurrence
of this issue?
11. Code Blue/RRT Was the Code Blue/RRT well run? Are there any learning opportunities?
12. Did you experience any EMR related safety issues?
13. Plant Equipment Issues
14. Foleys (See documentation tool)
15. Central Lines (See documentation tool)
16. Skin Ulcers (See documentation tool)
17. Restraints (See documentation tool)
18. Recognition
Add on themes on specific days:
Tuesday: Review recruitment and open positions
Wednesday: Close the loop on safety issues raised over the week
Thursday: Review of Hand Hygiene, MDRO, CAUTI, CLABSI, SSI, HAPU, Falls
Friday: HCAHPS and Patient Experience
stevenbrass
Text Box
Attachment A

Foley Urinary Catheter Documentation Tool
Date
Unit
1. Please complete:
Please enter a number
2. How many patients do I have on the unit with a foley indwelling urinary catheter?
Please enter a number
3. How many patients were admitted with a foley indwelling urinary catheter with a questionable indication?
Patient A Patient B Patient C Patient D Patient E Patient F Patient G Patient H
Bladder outletobstruction
Critical Ins and OutMeasurements
Urological Surgery/PostOp
Open sacral wound orperineal wound
Comfort for end of life
4. Please indicate the clinical reason for the foley indwelling urinary catheter in each of your patients.
Patient A Patient B Patient C Patient D Patient E Patient F Patient G Patient H
Yes
No
Not applicable/ Patientis female
5. Was an external cathter (texas or condom catheter) attempted? If not why?
Patient A Patient B Patient C Patient D Patient E Patient F Patient G Patient H
Yes
No
6. Please indicate for each patient whether there is a nurse drive d/c protocol in place?
stevenbrass
Text Box
Attachment B


Central Line Documentation Tool
Date
Unit
1. Please complete:
Midline catheter
Peripherally InsertedCentral Catheter (PICC)
Subclavian
2. How many patients do I have on the unit with the following:
Patient A Patient B Patient C Patient D Patient E Patient F Patient G Patient H
Poor peripheral access
Hemodynamicmonitoring
Plamaphaeresis
VasopressorMedications
Nutrition
3. Please indicate the clinical reason for this venous access for each of your patients.
Patient A Patient B Patient C Patient D Patient E Patient F Patient G Patient H
4. How many days has the central line (PICC, midline, sublaclvian) been in place?
Patient A Patient B Patient C Patient D Patient E Patient F Patient G Patient H
Yes
No
5. Please indicate for each patient whether the dressing was checked today?
stevenbrass
Text Box
Attachment C

6. Please come to the Safety Huddle prepared to discuss the plan to remove the central line if there is noclear clinical indication.

Skin Ulcer Documentation Tool
1. How many patients do I have with:
Skin Ulcers
Patient A Patient B Patient C Patient D Patient E Patient F Patient G Patient H
Yes
No
2. Among the patients with ulcers on my unit were any present on admission? Were they documentedappropriately?
Patient A Patient B Patient C Patient D Patient E Patient F Patient G Patient H
Stage 1
Stage 2
Stage 3
Stage 4
3. What was the stage of the ulcer?
4. How many patients do I have AT RISK for skin ulcers?
Skin Ulcers
Patient A Patient B Patient C Patient D Patient E Patient F Patient G Patient H
Device
Disability/Immobility
Diarrhea/Incontinence
Diet/Poor nutrition
5. Among my patients AT RISK for skin ulcer what are the known risk factors?
stevenbrass
Text Box
Attachment D

Patient A Patient B Patient C Patient D Patient E Patient F Patient G Patient H
Conduct a pressureulcer admissionassessment for allpatients with ulcers or atrisk of ulcers
Ensuring that patientsare clean and dry
Consult the dieticianwhen nutritionalelements contribute torisk
Ensure a reliableprocess for redistributingpressure (e.g., use aturn clock as a reminderto staff, implement turnrounds, pressureredistributing beds andmattresses)
Reassess risk for allpatients daily
6. What intervention did I implement to reduce ulcers in this patient?

Restraint Documentation Tool
1. How many patients do I have on my unit with restraints?
Patient A Patient B Patient C Patient D Patient E Patient F Patient G Patient H
Yes
No
2. Is there a daily physician order for the restraints written?
Patient A Patient B Patient C Patient D Patient E Patient F Patient G Patient H
Yes
No
3. Have I tried alternatives like: moving a patient closer to nursing station or having family at the bedside?
4. Please come to huddle prepared to discuss why restraints have to be used for your patient rather than asitter.
stevenbrass
Text Box
Attachment E

30 Day Readmission Documentation Tool
1. Demographics: Name/MRN/ Diagnosis on 1st discharge/ Diagnosis on 2nd Admission
Yes No Comments
Mental health diagnsois
Substance abuse
Showing up in ED threetimes in two months
Polypharmacy >6medications
Leaving against medicaladvice
Patient lives alone
2. Readmission Risk Factors:
Yes No Comments
Did thepatient understandthe symptoms ofthe condition gettingworse?
Was thereadequate teaching topatient's family?
Were writtendischarge instructionsprovided to patient?
Did the patient havea follow up with thePCP arranged in 7 days?if no why?
Did the patient go tothe follow upappointment? If no why?
Did the patient filltheir prescriptions? If nowhy?
3. Were the following documented in EMR during the first admission?
stevenbrass
Text Box
Attachment F

4. What actions do we need to take to prevent another readmission? (i.e. education to patient and family)

Length of Stay > 4 days
1. Name of patient/ Medical Record Number/ Room Number
2. What is the diagnosis?
3. What is the cause for the prolonged length of stay?
Yes No Comments
Medical
Social
Administrative
4. What are the plans to transition the patient when the medical/social/administrative reasons are resolved?
Yes No Comments
Home
SNF
LTAC
Nursing Home
Rehab
Other
5. What support do you need either administratively or clinically to discharge the patient?
stevenbrass
Text Box
Attachment G

Safety Issue
DATE WHO AREA WHAT
Week of:_____________
stevenbrass
Text Box
Attachment H

Hospital Quality Institute Vanguard Award 2016
The Patient Safety Huddle:
One Step on Our Journey to Becoming a
High Reliability Organization
Providence Little Company of Mary Medical Center San Pedro
Address: 1300 West 7th Street, San Pedro, CA 90732
1
stevenbrass
Text Box
Attachment I
Table of Contents
1. Number of reported safety events by category per month for 2nd
quarter 2016
2. 2016 Regional metrics: CAUTI, CLABSI, SSI, C Diff, Falls
3. CLABSI
4. 30 Days Readmission Rate
5. Patient Experience Scores: Inpatient and Emergency
Department
6. Hand Hygiene Compliance 2015
7. Hand Hygiene Compliance 2016
2

Number of reported safety events by category per month for 2nd quarter 2016
April 2016
May 2016
June 2016
Legend
Open = Unresolved
Closed = Resolved
Total = Open + Closed

Regional Metrics:CAUTI, CLABSI, SSI, C Diff, Falls
4
Legend
SSI=surgical site infection
Hyst= hysterectomy
CLABSI=central line-associated blood stream infections
C diff= Clostridium difficile
CAUTI=-Catheter-Associated Urinary Tract Infection

Drill Down – CLABSI Rate / ICU CLABSI SIR 2015
CLABSI RATE / ICU CLABSI SIR
STATUS ACTION PLANS
Legend
CLABSI=central line-associated blood stream infections
SIR= standardized infection ratio
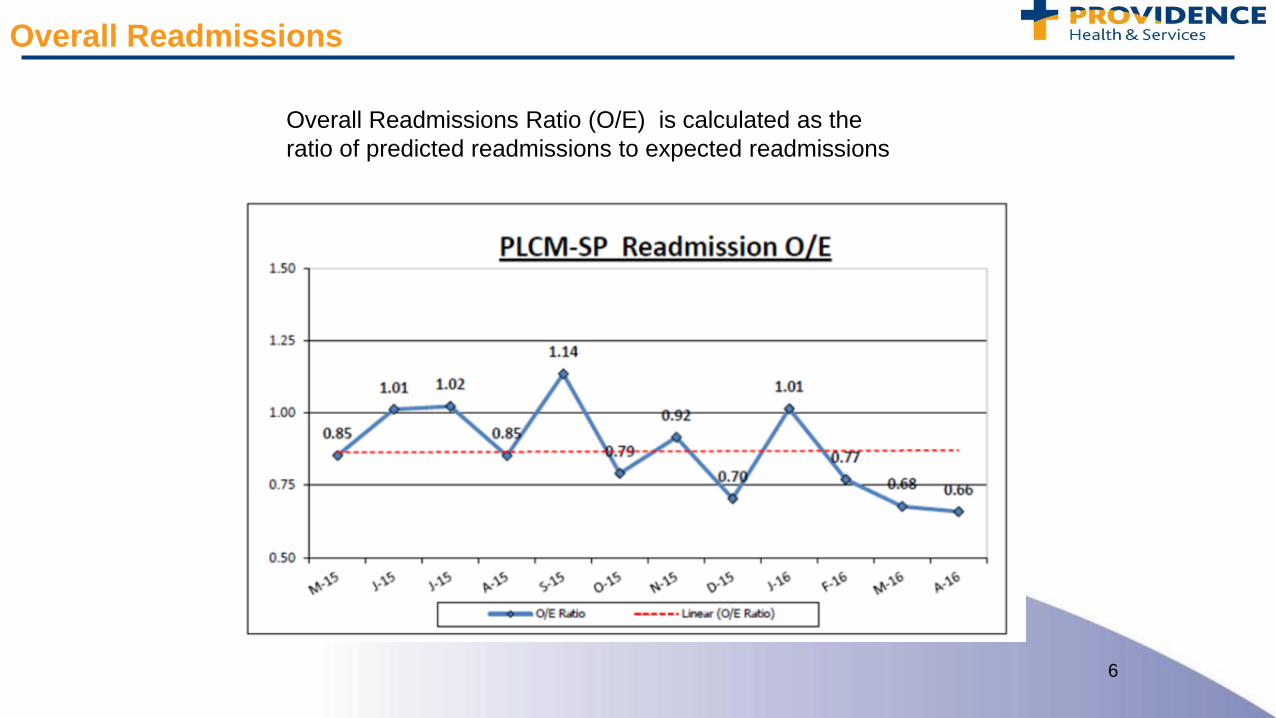
Overall Readmissions
6
Overall Readmissions Ratio (O/E) is calculated as the
ratio of predicted readmissions to expected readmissions

Patient Experience Scores
7
Inpatient Goal 72%
Emergency Goal 56%

Hand Hygiene Compliance 2015 HAND HYGIENE 2015

2016 Hand Hygiene Compliance by month and YTD
Behavioral Health Safety Huddle
Date: ___________________
In Attendance:
1. How many patients are currently on Bridges?
2. How many anticipated discharges today on Bridges?
3. How many male/female beds are available on Bridges?
4. How many anticipated transfers or requests do you have on Bridges from Providence or UCLA?
5. How many behavioral health patients are boarding in 2W/3W/3C/ICU?
a. On 5150
b. With Sitter
c. With medications for agitation ordered
6. How many behavioral health patients are boarding in the ED?
a. Are any anticipated to need admission?
1. Looking Back Past 24 hours
a. Do we have any patients in the hospital with a tendency towards violence?
b. Any patients at AWOL or attempt at AWOL?
c. Patient Safety Events: Code Greys, Injuries
d. Caregiver Safety Events: Assaults/Injuries
e. Administrative Updates: Important Updates, Announcements
f. Have we had to contact any regulatory bodies: APS, Police, CDPH, Social Worker
g. Have we confiscated any contraband items?
h. Has security and risk management been consulted?
i. Has environmental rounds been conducted by nursing and security every 4 hours?
2. Looking Ahead:
a. Any census or staffing issues impacting safety: sitters/nursing
b. High Risk Patients
c. Any safety issues that may impact other departments
d. Deficiencies in equipment, supplies that impact safety
e. Conditions inside or outside the hospital that could impact the delivery of safe, quality
care
3. Follow-up
a. Status reports on issues identified today or days before
stevenbrass
Text Box
Attachment J