Outcomes of planned celiac artery coverage during TEVAR
6
From the Society for Vascular Surgery Outcomes of planned celiac artery coverage during TEVAR Manish Mehta, MD, MPH, R. Clement Darling III, MD, John B. Taggert, MD, Sean P. Roddy, MD, Yaron Sternbach, MD, Kathleen J. Ozsvath, MD, Paul B. Kreienberg, MD, and Philip S. K. Paty, MD, Albany, NY Objective: Successful thoracic endovascular aneurysm repair (TEVAR) requires adequate proximal and distal fixation and seal. We report our experience of planned celiac artery coverage during endovascular repair of complex thoracic aortic aneurysms (TAA). Methods: Since 2004, 228 patients underwent TEVAR under elective (n 162, 71%) and emergent circumstances (66, 29%). Patients with inadequate distal stent grafts landing zones during TEVAR underwent detailed evaluation of the gastroduodenal arcade with communicating collaterals between the celiac and superior mesenteric artery (SMA) by computed tomography angiography and intraoperative arteriogram. If needed, in presence of a patent SMA and demonstration of collaterals to the celiac artery, the stent grafts were extended to the SMA with celiac artery coverage. Furthermore, instances when further lengthening of distal thoracic stent graft landing zone was needed to obtain an adequate seal, the SMA was partially covered with the endograft, and a balloon expandable stent was routinely deployed in proximal SMA to maintain patency. Outcome data were prospectively collected and analyzed retrospectively. Results: Thirty-one of 228 (14%) patients with TEVAR required celiac artery interruption; 24 (77%) had demonstrable collaterals to the SMA. Twelve (39%) of 31 patients underwent additional partial SMA coverage by stent graft, and proximal SMA stent. The majority of patients were females (n 20, 65%), the mean age was 74 years (range 55-87 years), and the mean TAA size was 6.5 cm. Postoperative complications included visceral ischemia in 2 (6%) patients, paraplegia in 2 (6%) patients, and death in 2 (6%) patients. All type 1b endoleaks (n 2, 6%) and type 2 endoleaks vial retrograde flow from the celiac artery (n 3, 10%) were successfully treated by transfemoral coil embolization. Over a mean follow-up of 15 months, there have been no other complications of mesenteric ischemia, spinal cord ischemia, SMA in-stent stenosis, or conversion to open surgical repair. Conclusions: Our findings suggest that celiac artery coverage to facilitate adequate distal sealing during TEVAR with complex TAA is relatively safe in the presence of SMA-celiac collaterals. Pre-existing SMA stenosis can be successfully treated by balloon expandable stents during TEVAR, and endoleaks arising from distal stent grafts attachment site or via retrograde flow from the celiac artery can be successfully managed by transfemoral coil embolization. Although early results are encouraging, long-term efficacy of these procedures remains to be determined and vigilant follow-up is needed. ( J Vasc Surg 2010;52:1153-8.) It has been over a decade since the introduction of thoracic endovascular aneurysm repair (TEVAR), and to- day there is ample evidence suggesting early and midterm advantages of this endovascular procedure over the tradi- tional open thoracic aortic reconstruction in anatomically suitable patients. 1-3 Anatomically suitability during TEVAR implies that patients with descending thoracic aortic aneu- rysms (TAA) have adequate proximal and distal thoracic stent graft landing zones, which according to “instructions for use” of thoracic stent grafts, would include a 2 cm aneurysm free normal thoracic aorta distal to the left com- mon carotid artery, and similarly a 2 cm aneurysm free normal thoracic aorta proximal to the celiac artery. Al- though extensions of the proximal thoracic stent graft landing zones that include coverage of the left subclavian artery with or without extra-anatomic left carotid-subcla- vian bypass, or even the left carotid artery coverage with extra-anatomic right to left carotid-carotid and left carotid- subclavian bypass have been considered relatively safe, other extra-anatomic visceral reconstructions that include celiac/superior mesenteric bypass or “debranching” to ex- tend the distal landing zones have been associated with significant morbidity and mortality. 4 The importance of collateralization through the vis- ceral arterial tree has been well understood, and it is rare for symptoms of visceral/intestinal ischemia to develop with stenosis or even occlusion of one of the mesenteric arteries. 5 There are several important collateral pathways between the celiac and the superior mesenteric artery that supply blood flow to the abdominal viscera, and when either of these two arteries is narrowed or occluded the collateral pathways across the pancreaticoduodenal arteries From The Institute for Vascular Health and Disease, Albany Medical Col- lege, The Vascular Group, and The Center for Vascular Awareness, Inc. Competition of interest: Dr Mehta is on the advisory board of Cordis Corporation and Trivascular, Inc. Dr Mehta is a speaker/consultant for W.L. Gore and Associates, Inc, Medtronic, Inc, Trivascular, Inc, Cordis Corporation, and ev3 Endovascular, Inc. Presented at the 2008 Vascular Annual Meeting, March 5, 2008, Las Vegas, Nev. Reprint requests: Manish Mehta, MD, MPH, The Vascular Group, 43 New Scotland Ave, MC 157, Albany, NY 12208 (e-mail: mehtam@ albanyvascular.com). The editors and reviewers of this article have no relevant financial relationships to disclose per the JVS policy that requires reviewers to decline review of any manuscript for which they may have a competition of interest. 0741-5214/$36.00 Copyright © 2010 by the Society for Vascular Surgery. doi:10.1016/j.jvs.2010.06.105 1153
-
Upload
manish-mehta -
Category
Documents
-
view
215 -
download
1
Transcript of Outcomes of planned celiac artery coverage during TEVAR

From the Society for Vascular Surgery
Outcomes of planned celiac artery coverageduring TEVARManish Mehta, MD, MPH, R. Clement Darling III, MD, John B. Taggert, MD, Sean P. Roddy, MD,Yaron Sternbach, MD, Kathleen J. Ozsvath, MD, Paul B. Kreienberg, MD, andPhilip S. K. Paty, MD, Albany, NY
Objective: Successful thoracic endovascular aneurysm repair (TEVAR) requires adequate proximal and distal fixation andseal. We report our experience of planned celiac artery coverage during endovascular repair of complex thoracic aorticaneurysms (TAA).Methods: Since 2004, 228 patients underwent TEVAR under elective (n � 162, 71%) and emergent circumstances (66,29%). Patients with inadequate distal stent grafts landing zones during TEVAR underwent detailed evaluation of thegastroduodenal arcade with communicating collaterals between the celiac and superior mesenteric artery (SMA) bycomputed tomography angiography and intraoperative arteriogram. If needed, in presence of a patent SMA anddemonstration of collaterals to the celiac artery, the stent grafts were extended to the SMA with celiac artery coverage.Furthermore, instances when further lengthening of distal thoracic stent graft landing zone was needed to obtain anadequate seal, the SMA was partially covered with the endograft, and a balloon expandable stent was routinely deployedin proximal SMA to maintain patency. Outcome data were prospectively collected and analyzed retrospectively.Results: Thirty-one of 228 (14%) patients with TEVAR required celiac artery interruption; 24 (77%) had demonstrablecollaterals to the SMA. Twelve (39%) of 31 patients underwent additional partial SMA coverage by stent graft, andproximal SMA stent. The majority of patients were females (n � 20, 65%), the mean age was 74 years (range 55-87 years),and the mean TAA size was 6.5 cm. Postoperative complications included visceral ischemia in 2 (6%) patients, paraplegiain 2 (6%) patients, and death in 2 (6%) patients. All type 1b endoleaks (n � 2, 6%) and type 2 endoleaks vial retrogradeflow from the celiac artery (n � 3, 10%) were successfully treated by transfemoral coil embolization. Over a meanfollow-up of 15 months, there have been no other complications of mesenteric ischemia, spinal cord ischemia, SMAin-stent stenosis, or conversion to open surgical repair.Conclusions: Our findings suggest that celiac artery coverage to facilitate adequate distal sealing during TEVAR withcomplex TAA is relatively safe in the presence of SMA-celiac collaterals. Pre-existing SMA stenosis can be successfullytreated by balloon expandable stents during TEVAR, and endoleaks arising from distal stent grafts attachment site or viaretrograde flow from the celiac artery can be successfully managed by transfemoral coil embolization. Although earlyresults are encouraging, long-term efficacy of these procedures remains to be determined and vigilant follow-up is needed.
(J Vasc Surg 2010;52:1153-8.)It has been over a decade since the introduction ofthoracic endovascular aneurysm repair (TEVAR), and to-day there is ample evidence suggesting early and midtermadvantages of this endovascular procedure over the tradi-tional open thoracic aortic reconstruction in anatomicallysuitable patients.1-3 Anatomically suitability during TEVARimplies that patients with descending thoracic aortic aneu-rysms (TAA) have adequate proximal and distal thoracicstent graft landing zones, which according to “instructions
From The Institute for Vascular Health and Disease, Albany Medical Col-lege, The Vascular Group, and The Center for Vascular Awareness, Inc.
Competition of interest: Dr Mehta is on the advisory board of CordisCorporation and Trivascular, Inc. Dr Mehta is a speaker/consultant forW.L. Gore and Associates, Inc, Medtronic, Inc, Trivascular, Inc, CordisCorporation, and ev3 Endovascular, Inc.
Presented at the 2008 Vascular Annual Meeting, March 5, 2008, Las Vegas,Nev.
Reprint requests: Manish Mehta, MD, MPH, The Vascular Group, 43New Scotland Ave, MC 157, Albany, NY 12208 (e-mail: [email protected]).
The editors and reviewers of this article have no relevant financial relationshipsto disclose per the JVS policy that requires reviewers to decline review of anymanuscript for which they may have a competition of interest.
0741-5214/$36.00Copyright © 2010 by the Society for Vascular Surgery.
doi:10.1016/j.jvs.2010.06.105for use” of thoracic stent grafts, would include a 2 cmaneurysm free normal thoracic aorta distal to the left com-mon carotid artery, and similarly a 2 cm aneurysm freenormal thoracic aorta proximal to the celiac artery. Al-though extensions of the proximal thoracic stent graftlanding zones that include coverage of the left subclavianartery with or without extra-anatomic left carotid-subcla-vian bypass, or even the left carotid artery coverage withextra-anatomic right to left carotid-carotid and left carotid-subclavian bypass have been considered relatively safe,other extra-anatomic visceral reconstructions that includeceliac/superior mesenteric bypass or “debranching” to ex-tend the distal landing zones have been associated withsignificant morbidity and mortality.4
The importance of collateralization through the vis-ceral arterial tree has been well understood, and it is rarefor symptoms of visceral/intestinal ischemia to developwith stenosis or even occlusion of one of the mesentericarteries.5 There are several important collateral pathwaysbetween the celiac and the superior mesenteric artery thatsupply blood flow to the abdominal viscera, and wheneither of these two arteries is narrowed or occluded the
collateral pathways across the pancreaticoduodenal arteries1153

JOURNAL OF VASCULAR SURGERYNovember 20101154 Mehta et al
become vital. With critical stenosis or occlusion of the celiacartery, blood flow to the liver, spleen, stomach, and duo-denum precedes from the superior mesenteric artery(SMA) to the pancreaticoduodenal collaterals to the he-patic artery. Furthermore, the incidence of a replaced righthepatic artery that originates from the SMA is 15% to 20%,which helps provide collateral blood flow between the twovisceral arteries.6
When dealing with TAA, in the “real world” clinicalscenarios, patients sometimes present with extensive aneu-rysmal involvement that extends up to the distal thoracicaorta, precluding an adequate distal stent graft landingzone, and coverage of the celiac artery to facilitate adequatestent graft fixation and seal is necessary. Visceral arteryrevascularizations during TEVAR are complex proceduresand their associated morbidity and mortality. In light of thecomplexity of visceral revascularization in TAA patients,and the fact that the celiac and the SMA have a richcollateral network has set the stage for us to evaluate thefeasibility and efficacy of celiac artery coverage withoutrevascularization during TEVAR. We report our experienceof planned celiac artery coverage during endovascular re-pair of complex TAA.
METHODS
Our initial TEVAR experience began in 2004, andsince, 228 patients underwent TEVAR for treatment oflesions in the thoracic aorta. Early in our experience,TEVAR was performed for patients with distal stent graftlanding zone of at least 2 cm, in accordance with the“indications for use” of the FDA approved and commer-cially available thoracic stent grafts. As our experienceevolved and we were faced with patients with complex TAAthat extended up to the celiac artery, we were forced toevaluate the outcomes of celiac artery coverage duringTEVAR in treating these high-risk patients.
Patients with large fusiform TAA �6 cm, or saccularTAA irrespective of size, with inadequate distal stentgraft landing zones above the celiac artery underwent adetailed evaluation of the gastroduodenal collateral cir-culation between the SMA and the celiac artery by compu-ted tomography angiography (CTA). When CTA wasnon-demonstratable for gastroduodenal collaterals or failedto indicate aberrant replaced right hepatic artery originat-ing from the SMA, preoperative and/or intraoperativeselective arteriogram was performed to further delineatethe existence of these collaterals. The arteriogram wasobtained in the anterior-posterior as well as lateral projec-tions, and when selective catheterization failed to indicategastroduodenal-pancreaticoduodenal collaterals, tempo-rary celiac artery occlusion with a 5 to 6 mm balloon wasobtained prior to superior mesenteric arteriogram.
Patients considered high risk for open surgical thoraco-abdominal aortic reconstructions were considered forTEVAR with coverage of celiac artery to achieve a seal atthe distal stent graft landing zone. TEVAR procedureswere performed using general or spinal anesthesia using
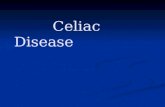
TAG thoracic stent graft (WL Gore & Associates, Flagstaff,Ariz), or Talent thoracic stent graft (Medtronic Ave, SantaRosa, Calif). Cerebral spinal fluid (CSF) drainage was usedselectively, and in general reserved for patients with priorabdominal aortic reconstructions via open surgical or en-dovascular means, or in patients that required extensivecoverage of the thoracic aorta during TEVAR. The se-quence of placement of the thoracic stent grafts be itproximal to distal or vice versa was up to the discretion ofthe vascular surgeon. Patients with celiac artery stent graftcoverage that presented with critical SMA stenosis or whenfurther lengthening of the distal thoracic stent graft landingzone was needed to obtain an adequate seal and the SMAwas partly covered with the stent graft, access into the SMAwas obtained via a 6F guide sheath or a 4 to 5 mm ballooncatheter prior to stent graft deployment, and subsequently,a balloon expandable stent was routinely deployed in theproximal SMA to maintain patency. (Fig 1, A, B, and C)
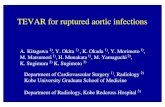
At the completion of TEVAR, patient assessment in-cluded an arteriogram to identify distal stent graft seal, withcareful evaluation for the presence of distal type Ib en-doleak, or type II endoleak via retrograde flow into theTAA from the celiac artery, and for patency of the SMA.During the postoperative period, clinical parameters sug-gesting presence of visceral ischemia or malperfusion wereevaluated, including the development of lactic acidosis,leukocytosis, fever, and abdominal pain. Postoperativefollow-up included routine clinical evaluation at 1 monthand every 6 months thereafter, and initial CTA at 1 month,6 months, 12 months, and yearly thereafter (Fig 2). Duringfollow-up, any endoleaks noted at the distal thoracic aorticstent graft attachment site were treated by coil emboliza-tion procedures. By means of a transfemoral approach, aguide catheter was traversed across the distal stent graftattachment site in between the stent graft and the thoracicaortic wall. The catheter was advanced into the distal tho-racic aortic aneurysm and coils were placed in proximity tothe celiac artery, or the site of the endoleak channel. (Fig 3,A, B, and C) All data were prospectively collected in avascular registry and Institutional Review Board approvalwas obtained for evaluation of all patient outcomes data.
RESULTS
Over a 5-year period, 31 (14%) of 228 patients withTEVAR required celiac artery stent graft coverage, and 12(39%) of these 31 patients required additional partial cov-erage of the SMA. All 12 patients with complete celiacartery coverage and partial SMA coverage underwent bal-loon expandable stent placement in the SMA. None of thepatients had both complete celiac artery and SMA cover-age.
The demographics and operative findings are listed inTable I; the majority of patients were females (65%), themean age was 74 years (range 55-87 years), the mean TAAsize was 6.5 cm (range 5.4 cm-8.2 cm) and comparableamong both genders, and the mean estimated blood losswas 379 cc. During the postoperative period, on postoper-ative day 1 complications of visceral ischemia developed in
two patients (6%); one patient developed shock liver and
the SM
JOURNAL OF VASCULAR SURGERYVolume 52, Number 5 Mehta et al 1155
required emergent right renal to hepatic artery revascular-ization, and died. A preoperative CTA indicated gastrodu-odenal collateral pathways between the celiac artery and theSMA. The TEVAR procedure required stent graft coveragefrom distal to the subclavian artery to just above the SMA,
Fig 1. A, Celiac artery stent graft coverage (thick armesenteric artery (SMA) stent (arrow) during thoracic engraft coverage. C, Following SMA stent, marked enhancnetwork (arrows) supplying the celiac artery catheter in
Fig 2. Origin of celiac artery coverage with thoracic stent graft,patent superior mesenteric artery (SMA) with collaterals to theceliac artery.
the operative blood loss was 250 cc, the procedure time was
50 minutes, and was considered uneventful. A secondpatient developed acalculus cholecystitis and underwent asuccessful open surgical cholecystectomy. One other pa-tient developed ischemic colitis affecting the sigmoid co-lon; at the time of sigmoid resection, the stomach, smallbowel, and the proximal colon were not ischemic. Intraop-erative findings also indicated antegrade pulsatile flow inthe SMA, retrograde pulsatile flow in the celiac via well-developed collaterals, and the ischemic sigmoid colitis wasconsidered to be embolic and not related to celiac arterycoverage. Two (6%) patients developed paraplegia; one hada prior infrarenal abdominal aortic aneurysm repair 3 yearsprior to TEVAR, and underwent CSF drainage. On post-operative day 1, the CSF drain malfunctioned, and thepatient developed symptoms of spinal cord ischemia thatwere irreversible. The second patient had TEVAR for acomplex TAA with coverage of the left subclavian arteryand a carotid-subclavian polytetrafluoroethylene (PTFE)bypass. The procedure time was approximately 230 min-utes, the operative blood loss of 1250 cc, and the patienthad iliac artery rupture during TEVAR requiring emergentiliofemoral bypass. The 30-day operative mortality was 6%;one patient died with complications of visceral ischemia,and second patient suffered complications of myocardialinfarction (Table II).
During the postoperative follow-up, endoleaks werenoted on CTA evaluations in 9 (29%) patients; 4 (13%)patients had type II endoleaks from intercostal arteries, 3(10%) patients had a type II endoleak via retrograde flowfrom the celiac artery, and 2 (6%) patients had a type Ibendoleak from distal stent graft attachment site. All five(16%) patients with endoleaks from retrograde flow via the
and critical SMA stenosis (thin arrow). B, Superiorscular aneurysm repair (TEVAR) with celiac artery stentt of gastroduodenal and pancreatiocduodenal collateralA.
row)dovaemen
celiac artery or from the distal stent graft attachment site

of T
JOURNAL OF VASCULAR SURGERYNovember 20101156 Mehta et al
were treated successfully by coil embolization. At a meanfollow-up of 15 months, two (6%) patients with stent graftmigration from distal attachment site required additionalstent graft extensions. Over a mean follow-up of 15months, there have been no other complications of mesen-teric ischemia, spinal cord ischemia, SMA in-stent stenosis,or conversion to open surgical repair.
DISCUSSION
TEVAR has evolved to become a viable option fortreatment for aortic lesions that affect the descending tho-racic aorta. When thoracic aneurysms are extensive andexpand beyond the limitations of currently available tho-racic endoprosthesis, surgeons and interventionalists areoften forced to make improvements that are technically andtechnologically driven to facilitate repair of these complexand extensive aneurysms that if untreated or treated bysurgical reconstruction are associated with a significantmorbidity and mortality.7,8 In evaluating our single center
Table I. Patient demographics
TEVAR with celiac arterycoverage 31
Male/female 11 (35%), 20 (65%)Mean age 74.2 yearsMean TAA size 6.5 cm (range 5.4 cm-8.2 cm)Coronary artery disease 18 (58%)Hypertension 28 (90%)Chronic obstructive pulmonary
disease 12 (39%)Pre-existing renal failure
(dialysis) 4 (12%)Mean estimated blood loss 379 cc
TAA, Thoracic aortic aneurysms; TEVAR, thoracic endovascular aneurysmrepair.
Fig 3. A, Type Ib endoleak (arrow) from stent graft ditype Ib endoleak channel. C, Coil embolization (arrow)
experience of 31 TEVAR patients with intentional celiac
artery coverage, the findings suggest that the incidence ofcomplications of visceral ischemia in these patients is 6%,and the incidence of death with associated visceral ischemiais 3%. With celiac artery coverage during TEVAR, theoverall potential for any possible complications of visceralischemia can occur in 16% (5/31) of the patients. Inconsidering the alternative of treating patients that wouldotherwise require surgical thoracoabdominal aortic recon-structions or hybrid endovascular procedures with surgicalvisceral artery debranching, the morbidity and mortality ofintentional celiac artery coverage during TEVAR in pa-tients that on CTA and/or arteriography have demon-strated the presence of visceral collateral pathways betweenthe celiac and the SMA would seem acceptable.
Although our experience of intentional celiac arterycoverage to facilitate distal stent graft seal zone duringTEVAR is the largest to-date, several other centers havepublished data with comparable results.9-11 Their findingsalso suggest the feasibility and short-term efficacy of celiac
Table II. Complications in TEVAR patients with celiaccoverage
TEVAR with celiac arterycoverage 31 Outcome
Visceral ischemia 2 (6%)- Shock liver 1 (3%) Death- Acalculus cholecystitis 1 (3%) Cholecystectomy
Paraplegia 2 (6%) 1 death30-day mortality 2 (6%)Type 1b endoleak @ distal
attachment site 2 (6%) Coil embolizationType II endoleak: celiac artery
retrograde flow 3 (10%) Coil embolization
TEVAR, Thoracic endovascular aneurysm repair.
nding zone. B, Transfemoral guide catheter access intoype Ib endoleak via transfemoral guide catheter.
stal la
artery stent graft coverage to facilitate TEVAR with a caveat

JOURNAL OF VASCULAR SURGERYVolume 52, Number 5 Mehta et al 1157
that selective celiac and SMA arteriography alone might notreadily predict the complications of visceral ischemia. Whenplanning celiac artery coverage during TEVAR for complexthoracic aortic aneurysms that with limited distal suprace-liac stent graft landing zone, several assertions can be madebased on the currently available data, these include: (1) athorough evaluation of the celiac and SMA collaterals viaCTA and/or arteriography, (2) treatment of coexistingcritical SMA occlusive disease, (3) objective evaluation ofsubtle signs and symptoms of mesenteric ischemia duringthe perioperative period, and (4) consideration for cerebralspinal fluid drainage.
A thorough evaluation of the celiac and SMA collateralsvia CTA and/or arteriography should be considered essen-tial prior to planning TEVAR and celiac artery coverage.Studies evaluating CTA and standard arteriography haveindicated that the accuracy of CTA for depicting visceralarterial anatomy and identifying branches of the gastrodu-odenal and pancreaticodudenal arteries that are the collat-eral communications between the celiac and the SMA is�90%.12 Of course, CTA and even arteriography onlyindicate the mere presence of collaterals and do not allowfor assessment of the direction of blood flow. When CTAfails to demonstrate visceral collaterals between the celiacand the SMA, selective arteriogram is necessary and oftenrequires temporary occlusion of the celiac artery with a 5 to6 mm balloon catheter prior to selective superior mesen-teric arteriography to assess the visceral collaterals.
Coexisting occlusive disease in the SMA should beevaluated via angiography prior to stent graft deployment.Instances when celiac artery coverage with stent graft isneeded and the presence of severe SMA occlusive disease isidentified, even when asymptomatic, placement of a bal-loon expandable stent in the SMA should be considered.Theoretically, this could help prevent mesenteric/visceralischemia that might otherwise develop in patients as theirabdominal organs rely on the SMA with critical stenosis asthe sole blood supply. In our experience, 39% of the pa-tients with celiac artery coverage had either coexistingsevere SMA occlusive disease or partial stent graft coverageof the SMA, and underwent balloon expandable stentplacement to maintain patency of the SMA. We have nocomparative data to evaluate what might the outcomeshave been if the SMA did not undergo stent placement;however, since none of these patients have developedsymptoms of visceral ischemia, we have continued to em-ploy this strategy when managing these complex TAAs.
Preoperative evaluation of patient for the presence ofsymptoms of chronic mesenteric ischemia, as subtle as theymight be, should be thoroughly evaluated prior to embark-ing on these procedures. Although we did not experiencethis in our patients, we would recommend routine gastro-intestinal workup by a gastroenterologist including endos-copy, CTA, and preoperative angiography in select patientsas needed. Furthermore, during the postoperative period,signs and symptoms of mesenteric ischemia should becarefully evaluated by subjective clinical examinations, as
well as objective data such as assessment of leukocytosis,lactic acidosis, elevation of amylase/lipase, and liver func-tion tests. Finally, patients that develop signs and/or symp-toms of visceral ischemia should undergo prompt visceralrevascularization.
Placement of cerebral spinal fluid (CSF) drainage cath-eters should be considered in these patients since theseprocedures require significant coverage of the thoracicaorta, and the distal extent of the stent grafts usuallyextends to the T12-L1 level, which could potentially alsocover the artery of Adamkiewicz.13,14 Although the etiol-ogy for developing complications of spinal cord ischemia(SCI) during TEVAR are multifactorial and not necessarilyjust related to coverage of the artery of Adamkiewicz,significant coverage of the thoracic aorta during TEVARdoes increase the risk for developing SCI and should beevaluated during these procedures.
Finally, CTA alone might be inadequate in differenti-ating between a type Ib endoleak (inadequate distal stentgraft seal) and a type II endoleak (persistent retrogradeceliac artery flow into the TAA), and selective transfemoralangiography if often needed to differentiate between theendoleak types. In such instances, when postoperative CTAsuggests an endoleak in proximity to the distal stent graftattachment site, selective SMA catheterization and arterio-gram with anterior-posterior and lateral imaging can beused to identify type II endoleak via retrograde flow fromthe celiac artery. For treatment of these endoleaks, anembolization procedure can be performed via a transfemo-ral approach. An angled/directional catheter is directedbetween the stent graft and the aortic wall and used toaccess the aneurysm sac. The catheter is placed in proximityto the celiac artery and/or the endoleak channel and ap-propriately sized coils are selectively deployed. If a persis-tent type II endoleak from celiac artery is suspected prior toTEVAR, selective coil embolization of the celiac artery canbe performed prior to or during TEVAR.
CONCLUSION
In conclusion, TEVAR has become an acceptablemeans for managing patients with TAA and is generallyconsidered to be associated with less morbidity and mor-tality compared with open surgical repair of complex tho-racic aortic aneurysms. Our initial experience of 31 patientswith celiac artery coverage during TEVAR suggests anacceptably low incidence of visceral ischemic complicationsin select patients with demonstrable pancreaticoduodenaland gastroduodenal arterial collaterals between the celiacand SMA. We believe preoperative CTA and selective vis-ceral angiography are complementary in identifying visceralcollateral circulation and should be thoroughly evaluateduntil we fully recognize the strengths and limitations ofthese procedures in predicting visceral ischemia. Patientswith planned celiac artery stent graft coverage that havepreexisting severe SMA stenosis should be considered forSMA stent placement at the time of TEVAR to optimizevisceral collateral circulation. Although these results arepromising, currently available data only suggests that celiac
artery coverage to facilitate lengthening the distal stent
JOURNAL OF VASCULAR SURGERYNovember 20101158 Mehta et al
graft seal zone is feasible with limited morbidity and mor-tality in select patients, and its long-term efficacy remains tobe evaluated. Finally, it is obvious that the ideal thoracicstent graft for treating these complex thoracic aortic aneu-rysms is not yet available, and although future modifica-tions in stent graft design that are inclusive of fenestrationsand branch graft technology appear promising, for the timebeing these devices are not readily available. Currently,available data on SMA stenting in patients with visceralischemia suggest 20% to 40% in-stent stenosis at meanfollow-up of 3 to 5 years, and there is the possibility ofpatients developing delayed mesenteric ischemia at long-term follow-up.15-17 Therefore, it is vital that patients thatundergo these complex procedures undergo vigilant long-term follow-up to assess not only for the stent graft integ-rity, but also for the SMA stents in select patients.
AUTHOR CONTRIBUTIONS
Conception and design: MM, YSAnalysis and interpretation: MM, RDData collection: MM, PPWriting the article: MM, JTCritical revision of the article: PK, MMFinal approval of the article: MMStatistical analysis: MM, SRObtained funding: MM, KOOverall responsibility: MM
REFERENCES
1. Dake MD, Miller DC, Semba CP, Mitchell RS, Walker PJ, Liddell RP.Transluminal placement of endovascular stent-grafts for the treatmentof descending thoracic aortic aneurysms. N Engl J Med 1994;331:1729-34.
2. Leurs LJ, Bell R, Degrieck Y, Thomas S, Hobo R, Lundbom J. Endo-vascular treatment of thoracic aortic diseases: combined experiencefrom the EUROSTAR and United Kingdom Thoracic Endograft reg-istries. J Vasc Surg 2004;40:670-9; discussion 679-80.
3. Makaroun MS, Dillavou ED, Wheatley GH, Cambria, RP. Five-yearresults of endovascular treatment with Gore TAG device compared with
open repair of thoracic aortic aneurysms. J Vas Surg 2008;47:912-8.4. Murphy ED, Beck AW, Clagget GP, DiMaio JM, Jessen ME, Arki FR.Combined aortic debranching and thoracic endovascular aneurysmrepair (TEVAR) effective but at a cost. Arch Surg 2009;144:222-7.
5. Valentine RJ, Martin JD, Myers SI, Rossi MB, Clagett GP. Asymptom-atic celiac and superior mesenteric artery stenosis are more prevalentamong patients with unsuspected renal stenosis. J Vasc Surg 1991;14:195.
6. Olofsson PA, Connelly DP, Stoney RJ. Surgery of the celiac andmesenteric arteries. In: Haimovici H, editor. Vascular surgery: princi-ples and techniques. Norwalk, CT: Appleton Lange; 1989. p. 750.
7. Bakaeen FG, Chu D, Huh J, LeMaire SA, Soltero ER, Petersen NJ, et al.Contemporary outcomes of open thoracic aortic surgery in a veteranpopulation: do risk models exaggerate mortality. Am J Surg 2009;198:889-94.
8. Patel R, Cairad MF, Paruchuri V, Kwolek CJ, Chung TK, Cambria RP.Thoracoabdominal aneurysm repair: hybrid versus open repair. J VascSurg 2009;50:15-22.
9. Leon LR, Mills JL, Jordan W, Morasch MM, Kovacs M, Becker GJ, etal. The risks of celiac artery coverage during endoluminal repair ofthoracic and thoracoabdominal aortic aneurysms. Vasc Endovasc Surg2009;43:51-60.
10. Belenky A, Haddad M, Idov I, Knizhnik M, Litvin S, Bachar GN, et al.Celiac trunk embolization as a means of elongating short distal descend-ing thoracic aortic aneurysm necks, prior to endovascular aortic repair.Cardiovasc Intervent Radiol 2009;32:923-7.
11. Vaddineni SK, Taylor SM, Patterson MA, Jordan WD. Outcome afterceliac artery coverage during endovascular thoracic aortic aneurysmrepair: preliminary results. J Vasc Surg 2007;45:467-71.
12. Savastano S, Teso S, Corra S, Fantozzi O, Miotto D. Multislice CTangiography of the celiac and superior mesenteric arteries: comparisonwith arteriographic findings. Radiol Med 2002;103:456-63.
13. Lazorthes G. Arterial vascularization of the spinal cord. J Neurosurg1971; 35:253-62.
14. Feezor RJ, Martin TD, Hess PJ Jr, Daniels MJ, Beaver TM, Klodell CT,et al. Extent of aortic coverage and incidence of spinal cord ischemiaafter thoracic endovascular aneurysm repair. Ann Thorac Surg 2008;86:1809-14.
15. Gibbons CP, Roberts DE. Endovascular treatment of chronic arterialmesenteric ischemia: a changing perspective? Semin Vasc Surg 2010;23:47-53.
16. Dias NV, Acosta S, Resch T, Sonesson B, Alhadad A, Malina M, et al.Mid-term outcome of endovascular revascularization for chronic mes-enteric ischaemia. Br J Surg 2010;97:195-201.
17. Fioole B, van de Rest HJ, Meijer JR, van Leersum M, van Koeverden S,Moll FL, et al. Percutaneous transluminal angioplasty and stenting asfirst-choice treatment in patients with chronic mesenteric ischemia. JVasc Surg 2010;51:386-91.
Submitted Mar 22, 2010; accepted June 17, 2010.














![Gallbladder · Latin vesica fellea; vesica biliaris Gray's subject #250 1197 [1] System Digestive system (GI Tract) Artery Cystic artery Vein Cystic vein Nerve Celiac ganglia, vagus[2]](https://static.fdocuments.in/doc/165x107/5c8da86009d3f219388ce415/gallbladder-latin-vesica-fellea-vesica-biliaris-grays-subject-250-1197-1.jpg)
