
OUTCOME OF DELAYED CORD CLAMPING IN TERM NEONATES …
68
i OUTCOME OF DELAYED CORD CLAMPING IN TERM NEONATES AT THE FEDERAL MEDICAL CENTRE, ABEOKUTA: A RANDOMIZED CONTROLLED STUDY A DISSERTATION SUBMITTED BY: DR. AWOLAJA, BABATUNDE STEPHEN M.B;B.S (Ibadan) DEPARTMENT OF OBSTETRICS AND GYNAECOLOGY FEDERAL MEDICAL CENTRE, ABEOKUTA. TO: THE NATIONAL POSTGRADUATE MEDICAL COLLEGE OF NIGERIA. FOR THE PART TWO FELLOWSHIP EXAMINATION IN THE FACULTY OF OBSTETRICS AND GYNAECOLOGY NOVEMBER 2016
Transcript of OUTCOME OF DELAYED CORD CLAMPING IN TERM NEONATES …

i
OUTCOME OF DELAYED CORD CLAMPING IN TERM NEONATES
AT THE FEDERAL MEDICAL CENTRE, ABEOKUTA: A RANDOMIZED
CONTROLLED STUDY
A DISSERTATION SUBMITTED BY:
DR. AWOLAJA, BABATUNDE STEPHEN M.B;B.S (Ibadan)
DEPARTMENT OF OBSTETRICS AND GYNAECOLOGY
FEDERAL MEDICAL CENTRE, ABEOKUTA.
TO:
THE NATIONAL POSTGRADUATE MEDICAL COLLEGE
OF NIGERIA.
FOR THE PART TWO FELLOWSHIP EXAMINATION IN
THE FACULTY OF OBSTETRICS AND GYNAECOLOGY
NOVEMBER 2016

ii
DEDICATION
Gabriel Koleade and Deborah Olufunmilayo Awolaja, my late parents.

iii
SUPERVISOR’S ENDORSEMENT
I hereby declare that this dissertation: Outcome of delayed cord clamping in term neonates at
the Federal Medical Centre, Abeokuta was conceptualized and developed after a problem
identification and discussion with me by Dr Awolaja Babatunde Stephen.
I also supervised the conduct of the study, analysis of the data and write-up of this final report.
I am certain that the candidate undertook the study conscientiously.
.........................................................................................
DR. D.O. AWONUGA
M.B.B.S., FMCOG, FWACS, MSc (Rep. Biology)
Consultant Obstetrician/Gynaecologist
Department of Obstetrics & Gynaecology
Federal Medical Centre, Abeokuta

iv
SUPERVISOR’S ENDORSEMENT
I hereby declare that this dissertation: Outcome of delayed cord clamping in term neonates at
the Federal Medical Centre, Abeokuta was conceptualized and developed after a problem
identification and discussion with me by Dr Awolaja Babatunde Stephen.
I also supervised the conduct of the study, analysis of the data and write-up of this final report.
I am certain that the candidate undertook the study conscientiously.
........................................................................................
DR. A.S. ADEBAYO
M.B.B.S., FWACS
Consultant Obstetrician/Gynaecologist
Department of Obstetrics & Gynaecology
Federal Medical Centre, Abeokuta.

v
SUPERVISOR’S ENDORSEMENT
I hereby declare that this dissertation: Outcome of delayed cord clamping in term neonates at
the Federal Medical Centre, Abeokuta was conceptualized and developed after a problem
identification and discussion with me by Dr Awolaja Babatunde Stephen.
I also supervised the conduct of the study, analysis of the data and write-up of this final report.
I am certain that the candidate undertook the study conscientiously.
........................................................................................
DR. I.O.F. DEDEKE
M.B.chB., FWACPaed
Consultant Neonatologist
Department of Paediatrics
Federal Medical Centre, Abeokuta.

vi
DECLARATION
I hereby declare that this work, outcome of delayed cord clamping in term neonates at the
Federal Medical Centre, Abeokuta is genuine unless otherwise acknowledged.
..................................................................................
Dr. Awolaja Babatunde Stephen (MBBS, Ibadan)

vii
ACKNOWLEDGEMENT
My profound gratitude goes to God Almighty for his sustenance, my preceptor Dr A.S
Adebayo for looking through the initial draft and all the other consultants, Dr A.O Oladimeji,
Dr M.O Alao, Dr K.I Hunyinbo and Dr T.A Ogunfunmilayo for their contribution and
guidance.
My profound gratitude also goes to my Head of Department Dr D.O Awonuga for his review
and comments, to Dr I.O.F Dedeke Head of Paediatrics Department for her review,
comments, contribution to the statistical analysis and for constantly urging me on and for
practically keeping me on my toes during the final write up.
I would like to thank all my colleagues for their advice and constructive criticism, my junior
colleagues, midwives and all the members of the nursing department who helped out during
the study and to the paediatric residents who helped with sample collection and clinical
assessment of the babies.
Special thanks go to Dr Olawale and Miss Damilola who helped with the laboratory analysis
of the blood samples.
To my wife, Adenike and children Oluwasemiloore and Oluwafikemi, I am deeply grateful.
Lastly, I would like to thank, and very specially, the women and children who participated in
the study. For without them, the study would not have been possible.

viii
TABLE OF CONTENT
TITLE i
DEDICATION ii
ENDORSEMENT iii
DECLARATION vi
ACKNOWLEDGEMENT vii
CONTENT viii
ABBREVIATIONS x
LIST OF TABLES xi
ABSTRACT xii
CHAPTER ONE
INTRODUCTION 1
CHAPTER TWO
LITERATURE REVIEW 3
JUSTIFICATION 14
CHAPTER THREE
OBJECTIVE 15
CHAPTER FOUR
METHODOLOGY 16
ETHICAL CONSIDERATION 21
CHAPTER FIVE
RESULTS 23
TABLES 26
HYPOTHESIS TESTING 30

ix
CHAPTER SIX
DISCUSSION 31
LIMITATIONS OF THE STUDY 35
CONCLUSION 36
RECOMMENDATIONS 37
AREAS OF FURTHER RESEARCH 37
REFERENCES 38
APPENDICES 43
x
ABBREVIATIONS
eds editors
e.g. for example
et al and others
g gram
s second
μg microgram
BSc Bachelor of Science
CI confidence interval
DCC delayed cord clamping
dL decilitre
ECC early cord clamping
EDTA ethylenediamine tetraacetate
EMCS emergency caesarean section
FMC Federal Medical Centre
Fl femtolitre
FMCOG Fellow of the Medical College of Obstetrics
and Gynaecology
FWACS Fellow of the West African College of Surgeons
HND Higher National Diploma
HREC Health Research Ethics Committee
IDA iron deficiency anaemia
Kg kilogram
LMP last menstrual period
MBBS Bachelor of Medicine;Bachelor of Surgery
mg milligram
NCE National Certificate of Education
ND National Diploma
NTD neural tube defect
PCV packed cell volume
PPH postpartum haemorrhage
SD standard deviation
SPSS statistical package for social sciences
USS ultrasound scan
WHO world health organization

xi
LIST OF TABLES PAGE
Table I. Maternal characteristics 26
Table II. Newborn characteristics 26
Table III. Neonatal haematological outcome at 24 hours of life 27
Table IV. Neonatal secondary outcome 28
Table V. Haematocrit at 6 weeks of life 29

xii
ABSTRACT
Background: Early cord clamping has been postulated as a major cause of anaemia in
infancy and there is no sound evidence to support this approach which might deprive the
newborn of some benefits such as an increase in iron storage. Iron deficiency anaemia is a
serious health problem that affects the physical and cognitive development of children.
Therefore, it is important to develop cost-effective interventions aimed at improving the
haematologic status of the millions of children affected by this condition worldwide. Delayed
clamping of the umbilical cord increases newborn iron endowment and is not associated with
adverse effects.
Objective: To determine the haematological and clinical effects of delayed umbilical cord
clamping in term neonates.
Methodology: This was a prospective randomized controlled study which was carried out at
the labour ward of the department of Obstetrics and Gynaecology, Federal Medical Centre,
Abeokuta. A total of 110 mother-infant pairs who met the inclusion criteria were assessed
and randomized into two groups; early cord clamping group (within 10s) and delayed cord
clamping group (at 2 minutes) and followed up until 6 weeks postpartum.
Results: Ninety-nine mother-infant pairs completed the study. At 24 hours of life, the mean
venous haematocrit was significantly higher in babies that had delayed cord clamping (t =
10.51, df = 97, p = 0.0001), an effect that persisted until 6 weeks postpartum. The delayed
cord clamping group also had a significantly lower prevalence of anaemia at 24 hours. (p =
0.0001).
Although the mean serum bilirubin was significantly higher in the delayed cord clamping
group, there were no significant differences in respiratory symptoms, admission into NICU,
need for phototherapy and newborn length of hospital stay between the two groups.
Conclusion: Delayed cord clamping compared with early cord clamping resulted in
improved neonatal haematocrit value and reduced prevalence of anaemia at 24 hours of life,
without increasing the risk of neonatal morbidity.
Recommendation: The practice is safe and should be incorporated into delivery protocols in
our environment to reduce the incidence of neonatal anaemia.

1
CHAPTER ONE
1.0 INTRODUCTION
The optimal timing of umbilical cord clamping has been and still remains a highly
controversial issue.1-4 Clamping and cutting of the umbilical cord at birth is by far the oldest
and most prevalent interventions in humans. In spite of this, the ideal timing for cord
clamping has yet to be established and there are no clear-cut guidelines on the clamping of
umbilical cord after child birth.
Before the mid 1950s, the term “early clamping” was defined as umbilical cord
clamping within 1 minute of birth, and “late clamping” was usually reserved for clamping
done more than 5 minutes after birth. Investigators in Sweden, the United States and Canada,
in a series of studies of blood volume changes after birth reported that in healthy term babies,
more than 90% of blood volume was achieved within the first few breaths the baby took after
birth.5 Due to the results of these findings and the lack of specific recommendation regarding
the optimal timing, the interval between birth and umbilical cord clamping began to be
shortened.
Also, management of the third stage of labour has typically focused on women and
prevention of postpartum haemorrhage. A systematic review published in 2000 found that
active management of third stage of labour which involved the use of oxytocics, early cord
clamping, and controlled cord traction was superior to expectant management in terms of
maternal blood loss.6 For this reason, early clamping was accepted into obstetric practice
without much consideration.
However, there is growing evidence that our haste to clamp the umbilical cord and
pass the baby off is ill advised. It has been argued that early cord clamping puts the newborn
at increased risk of hypovolaemic damage and iron loss, as well as several blood disorders
and type 2 diabetes, as a consequence of loss of haemopoietic stem cells.7,8
Furthermore, early cord clamping has been postulated as a major cause of anaemia in
infancy, and this has led some investigators to recommend late clamping as a low-cost
intervention to reduce anaemia during the first 6 months of life.
One of the most critical factors contributing to neonatal and infant mortality in
developing countries is anaemia,9 which has been repeatedly shown to be an intractable
problem even with antimalarial and iron interventions.
In developing countries, up to 50% of children become anaemic by 12 months of
age.10 Iron deficiency anaemia (IDA) during infancy and childhood is of particular concern

2
because of potentially detrimental effects on development, some of which might be
irreversible even after iron treatment.11 Iron stores at birth are a major factor influencing
growth and the occurrence of IDA during infancy12 and available evidence suggests that it is
important to prevent iron deficiency in infants in order to achieve optimal brain development.
However, the types of interventions that can be implemented during this time are
either not cost effective or difficult to implement, especially in developing countries.
A first step towards reducing anaemia in infancy can be taken during birth. Delayed
cord clamping could be a cost-effective intervention to improve the iron status of babies at
birth.
Studies have shown that delayed cord clamping could contribute to preventing iron
deficiency anaemia in the first year of life.13,14 A recent systematic review confirms the
benefit of delayed cord clamping.15
The reason for this effect is based on the fact that after birth, the newborn is delivered
with a placental transfusion of approximately 80 ml of blood at 1 minute after birth and 100
ml at 3 minutes after birth.7,16 This volume will supply 40-50 mg/kg of extra iron to the
approximately 75 mg/kg of body iron that term newborn babies have, reaching a total of 115-
120 mg/kg which might prevent iron deficiency in the first year of life.4,14
Conversely, some observational studies suggest that delayed umbilical cord clamping
put newborns at higher risk of suffering from polycythaemia, respiratory symptoms,
hyperbilirubinaemia, and other neonatal disorders.17-19 However, there have been no
randomized controlled trials showing the risk of these harmful effects on the newborn.
Many tertiary institutions in Nigeria still practice early cord clamping, despite weight
of current evidence demonstrating the benefits of delayed cord clamping after birth, and there
is no published local data on the subject matter.
The aim of this study was to evaluate the haematological and clinical effects of
delayed cord clamping in term neonates at the Federal Medical Centre, Abeokuta.

3
CHAPTER TWO
2.0 LITERATURE REVIEW
The optimal timing of cord clamping has been a controversial issue for decades, and
there is little agreement among doctors and midwives about the optimal time to clamp the
umbilical cord after birth.20
The most important point of difference relate to maternal and infant safety. Many
healthcare workers worldwide tend to clamp the cord and pass the baby off as quickly as
possible. Infants in resource poor settings are the main victims of immediate clamping, as this
prevents a cost-free means of boosting their small iron stores.20
Delayed clamping of the umbilical cord is a physiological and inexpensive means of
enhancing haematologic status, preventing anaemia, enriching iron stores and ferritin levels
of infants and it is of particular importance for developing countries in which anaemia during
infancy and childhood is highly prevalent.10
2.1 THE FETAL-PLACENTAL CIRCULATION
During pregnancy, the fetal-placental circulation transports oxygen and nutritional
elements from the placenta to the fetus, and metabolic residues from the fetus to the placenta.
The total fetal blood volume is approximately 115 ml/kg. The proportion of fetal blood that at
any moment circulates in the placenta diminishes during pregnancy, and is estimated to be
around 50% at 30 weeks of gestation and 35% at term.21
For a normal term pregnancy, with a fetus weighing 3.5kg, this distribution
corresponds to approximately 140ml of blood in the placenta and 260 ml in the fetus.
After delivery, blood circulates in the umbilical arteries from the newborn baby
mainly during the first 25 seconds and after 45 seconds, the circulation becomes negligible
indicating a closure of the fetal-placental circulation. In contrast, the blood flow from the
placental side to the baby through the umbilical vein is maintained during the first 3 minutes
of birth, largely influenced by uterine contractions.22 Consequently, a net transfusion of blood
from the placenta to the baby is accomplished.
The total placental transfusion to the baby is about 30 ml/kg, leaving 15 ml/kg in the
placenta. The placental transfusion occurs mainly within 1 minute, and is usually complete
after 3 minutes.23 Also, the level of the baby in relation to the placenta affects the placental
transfusion.

4
If the baby is held 20 cm below the placenta, the complete transfusion will be
performed within 1 minute, but if the baby is held 20 cm above the level of the placenta, the
transfusion will be about 20 ml/kg, and at 40 cm above the placenta, no transfusion occurs.
The rate of transfusion is also dependent on uterine contractions.24
2.2 UMBILICAL CORD CLAMPING AFTER BIRTH
In 1801, Erasmus Darwin wrote “Another thing very injurious to the child is the tying
and cutting of the navel string too soon, which should always be left till the child has not only
repeatedly breathed but till all pulsation in the cord ceases. As otherwise the child is much
weaker than it ought to be, a part of the blood being left in the placenta which ought to have
been in the child.”25
Most mammals in the animal kingdom wait until the expulsion of the placenta to
sever the umbilical cord from their newborn after delivery. In humans, the attendant aiding
the delivery clamps and severs the umbilical cord much before the placenta is delivered; often
within a few seconds of the baby’s birth.
The practice of early cord clamping started in the 20th century with increasing number
of women opting for hospital births and increasing number of obstetricians conducting such
deliveries.26
Early clamping and cutting of the umbilical cord is widely practised as part of the
management of labour but recent studies suggest that it may be harmful to the baby.27
Early clamping of the cord was one of the first routine medical interventions in
labour. Its place in modern births was guaranteed by its incorporation into the triad of
interventions that make up the active management of the third stage of labour. The earliest
references are clear about the other two components of active management – oxytocin to
contract the uterus and prevent postpartum haemorrhage, and controlled cord traction to
prevent retention of the placenta.28
But early cord clamping had no specific rationale, and it probably entered the protocol
by default because it was already part of standard practice. When this package was shown to
reduce postpartum haemorrhage in the 1980s, early cord clamping became enshrined in the
modern management of labour.27

5
2.3 ACTIVE MANAGEMENT OF THE THIRD STAGE OF LABOUR
The third stage of labour is that period of time from birth of the baby until delivery of
the placenta.6
There are two contrasting approaches to managing the third stage of labour: active
management and expectant or physiological management.
Expectant management is a non-interventionist approach which involves waiting for
signs of placental separation and allowing the placenta to deliver spontaneously or aided by
gravity, maternal effort or nipple stimulation. Active management usually involves the
clinician intervening in the process through three interrelated processes; the administration of
a prophylactic uterotonic drug; early cord clamping and cutting; and controlled traction of the
umbilical cord.29
A major reason for practising active management is its association with reduced risk
of postpartum haemorrhage (PPH), the major complication of the third stage of labour.6
PPH is the most common fatal complication of pregnancy and childbirth in the world30,31 and
is a major contributor to the conservatively estimated 500,000 maternal deaths occurring
throughout the world annually.30,32 Whilst the majority of maternal deaths (99%) occur in
low-income countries33, the risk of PPH should not be underestimated for any birth.34
Although active management leads to reduced risk of PPH, it is important to establish which
component of the strategy lead to this reduced risk.
Trials show that early cord clamping has no effect on the risk of retained placenta or
postpartum haemorrhage.35,36
Evidence from a Cochrane review supports this result – prophylactic oxytocin reduces
the risk of postpartum haemorrhage whether the rest of the active management package is
adopted or not.37 Another systematic review published in 2008 studied the effects of different
cord clamping times on maternal blood loss and found that delayed clamping poses no
additional threats to women.29
2.3.1 DEFINITION OF EARLY AND DELAYED CORD CLAMPING
Different definitions of early cord clamping (ECC) have been used, with the time
varying from immediately to within one minute after delivery of the baby. In modern trials,
ECC has usually been defined as clamping within 10 – 30 seconds after birth.
Delayed cord clamping is usually defined as cord clamping within 2 – 3 minutes after
delivery or after cessation of cord pulsations.29,38

6
2.3.2 EFFECTS OF EARLY AND DELAYED CORD CLAMPING IN TERM
NEONATES
Advocates for early cord clamping argue that delayed cord clamping can be
physiologically distressing on the baby’s circulation and that the risk of polycythaemia and
jaundice is increased. Other rationales for ECC are the recommendation to practice ‘active
management of the third stage of labour,’ in which ECC has been a part, and the routine
assessment of the acid-base status of umbilical cord blood at birth. More recently, the new
possibility of harvesting haematopoietic stem cells from the placental-fetal blood has been
associated with a need for ECC. Since an increased volume of blood can be collected from
the placental circulation after early cord clamping, a higher count of stem cells can be
harvested.
In the past, paediatricians recommended early cord clamping because of fears that
over-transfusion caused polycythaemia, hyperviscosity syndrome or hyperbilirubinaemia.
However, a recent high quality meta-analysis of randomized controlled trials from the past 15
years convincingly showed that delayed cord clamping in full term neonates for a minimum
of two minutes is beneficial to the newborn, and that this benefit extends into infancy.39
The benefits include, improved haematological status measured as haematocrit value,
ferritin concentration, and stored iron, and a clinically important reduction in the risk of
anaemia. An increase was seen in polycythaemia, but it seemed to be benign. No significant
differences were seen between delayed and early cord clamping in the risk of neonatal
jaundice.
Although paediatricians think that early cord clamping is needed in babies who
require immediate neonatal resuscitation, these cases are exceptions. Most newborn babies do
not require resuscitation, immediate drying and keeping them warm is all that is needed. Less
than 10% of newborns need help to start breathing at birth (stimulation, positioning, clearing
the airway), and about 1% need extensive resuscitation.40 When respiratory efforts are absent
or inadequate despite initial stabilization, inflation breaths by mask ventilation are the
priority.40 The earliest time to assess whether these inflation breaths are successful is about
60 seconds after delivery. All these steps can be done while the umbilical cord is intact.41
Immediate clamping to enable resuscitation away from the mother could deprive the
baby of the much needed extra blood volume, and the resulting hypovolemia might adversely
affect tissue perfusion. Furthermore, as long as the uterus is not contracting and the placenta
has not been detached, the baby may still receive oxygen via the intact placental-fetal
circulation.

7
2.3.3 IRON DEFICIENCY ANAEMIA
Iron deficiency is the most common cause of anaemia in every country of the world.
Iron is one of the most common elements in the Earth’s crust, yet iron deficiency is the most
common cause of anaemia, affecting about 500 million people worldwide.42 This is because
the body has a limited ability to absorb iron and excess loss of iron as a result of haemorrhage
is frequent. Also, in many developing countries, dietary intake is inadequate from childhood.
Iron deficiency and iron deficiency anaemia are major public health problems in
young children worldwide, and are associated with poor neurodevelopment.
Young children are at particular risk of iron deficiency because of high iron
requirements during rapid growth in combination with low iron intake. Globally, about a
quarter of preschool children have iron deficiency anaemia, the most severe form of iron
deficiency.43
Its prevalence is highest among under five children in developing countries where
approximately 50% are affected.10
Iron is essential for several aspects of brain development, including myelination,
dendritogenesis, neurotransmitter function, and neuronal and glial energy metabolism.43,44
Iron deficiency anaemia in young children is associated with long lasting cognitive and
behavioural deficits.45 Iron deficiency without established anaemia has also been associated
with altered affective responding, impaired motor development, and cognitive delays.11,46-48
Two recent meta-analysis have concluded that iron supplementation improves psychomotor
and mental development in infants and children.49,50
Consequently, since delayed cord clamping (DCC) is associated with improved iron
status in infants, it could also have an impact on iron deficiency related adverse effects.
2.4 COMPARATIVE STUDIES ON EARLY VS DELAYED CORD CLAMPING
Physiological and health effects of cord clamping in relation to time after delivery
have been studied since 1875.51 Yet the controversies surrounding the optimal timing of cord
clamping remain unresolved.
Grajeda13 et al., 1997 conducted a randomized clinical trial in a low-income
Guatemalan population in which the effect of delayed clamping of the umbilical cord on
infant iron status was examined.
They randomly assigned 69 Guatemalan newborns into one of three groups at the time
of delivery: 1, cord clamping immediately after delivery (n = 21): 2, clamping when the cord

8
stopped pulsating, with the baby placed at the level of the placenta (n = 26): or 3, clamping
when the cord stopped pulsating, with the newborn placed below the level of the placenta
(n = 22). Maternal and infant haematologic assessments were performed at the time of
delivery and 2 months postpartum. At baseline, the newborns had similar haematocrit status
and the clinical assessment (including jaundice) revealed no significant difference in newborn
health status across groups. However, polycythaemia (percentage with a haematocrit value >
0.65) was more likely to occur in the group with delayed clamping and placement of the
newborn below the placenta (2 of 22) than in the other two groups (0 of 22). Both subjects
with polycythaemia were asymptomatic and their haematocrit values were just above the cut-
off value (0.656 and 0.660).Two months after delivery, infants in the two groups with
delayed cord clamping had significantly higher haematocrit values and haemoglobin
concentrations than did those in the early clamping group. The percentage with haematocrit
values < 0.33 was 88% in the control group compared with 42% in group 2 and 55% in group
3 (p = 0.01). Maternal haematologic indexes were similar among groups both at baseline and
2 months after delivery. Their result suggested that waiting until the umbilical cord stopped
pulsating (~ 1 minute after delivery) is a feasible low-cost intervention that can reduce
anaemia in infants in developing countries.
A limitation of this study was that all the deliveries were attended by the first author
who also performed all anthropometric measurements on the infants hence the possibility of
selection and ascertainment biases cannot be excluded.
Gupta and Ramji52, 2002 in a randomized controlled trial to study the effects of cord
clamping on iron stores of infants born to anaemic mothers at 3 months of age, randomized
102 neonates into early (n = 43) or delayed cord clamping (n = 59). The women assigned to
the early cord-clamping group had their cords clamped immediately after the birth of the
baby while those assigned to delayed cord-clamping group had their cords clamped after the
placenta had descended into the vagina. The mean infant ferritin and haemoglobin at 3
months were significantly higher in the delayed clamping group (118.4 μg/L and 99 g/L) than
in the early clamping group (73 μg/L and 88 g/L). The mean decrease in haemoglobin (g/L)
at 3 months adjusted for co-variates was significantly less in the delayed clamping group
compared to the early clamping group (-1.09, 95% CI -1.58 to -0.62, p <0.001). The odds for
anaemia (<100 g/L) at 3 months was 7.7 (95% CI 1.84 – 34.9) times higher in the early
compared to the delayed clamping group. They therefore concluded that iron stores and
haemoglobin in infancy can be improved in neonates born to anaemic mothers by delaying
cord clamping at birth.

9
Van Rheenen53 et al., 2007 conducted a randomized controlled trial to assess whether
delaying umbilical cord clamping was effective in improving the haematological status of
term infants living in a malaria-endemic area, and whether this was associated with
complications in infants and mothers.
They randomly assigned 105 women delivering at term in Mpongwe Mission Hospital
Zambia, to delayed cord clamping (DCC, n = 55) or immediate cord clamping (controls, n =
50) groups. Nine cases in the DCC group and four cases in the control group were excluded
from the analyses. Ninety-one mother-infant pairs were actively followed- up on a bi-
monthly basis until the infants reached the age of 6 months. The haemoglobin (Hb) change
from cord values and the proportion of anaemic infants was compared, and secondary
outcomes related to infant and maternal safety.
Throughout the observation period infant Hb levels in both groups declined, but more
rapidly in controls than in the DCC group [difference in Hb change from baseline at 4 months
1.1 g/dl, 95% CI 0.2;2.1]. By 6 months, this difference had disappeared (0.0 g/dl, 95% CI -
0.9;0.8). The odds ratio for iron deficiency anaemia in the DCC group at 4 months was 0.3
(95% CI 0.1;1.0), but no differences were found between the groups at 6 months. No adverse
events were seen in infants and mothers.
Their findings indicated that DCC could help improve the haematological status of
term infants living in a malaria-endemic region at 4 months of age. However, the beneficial
haematological effect disappeared by 6 months.
The strengths of this study are its randomized design, the low drop-out rate for a rural
area, and the control for confounding factors which could influence infant haematological
status. A limitation is that mothers who were already assigned to a treatment group could
later become ineligible which could not be avoided in view of the timing and nature of the
intervention. Also, the investigators, assessors and mothers were not blinded to the assigned
intervention. This could have biased the clinical evaluation for hyperviscosity syndrome and
hyperbilirubinaemia.
Chaparro54 et al., 2006 in another randomized controlled trial to assess whether a 2-
minute delay in the clamping of the umbilical cord of normal-weight, full-term infants
improved iron and haematological status up to 6 months of age. In their study,476 mother-
infant pairs were recruited at a large Obstetrics hospital in Mexico City, randomly assigned to
delayed clamping (2 minutes after delivery of the baby’s shoulders) or early clamping
(around 10 seconds after delivery), and followed up until 6 months postpartum.

10
Three hundred and fifty eight (75%) mother-infant pairs completed the trial. At 6 months of
age, infants who had delayed clamping had significantly higher mean corpuscular volume
(81.0 fL vs 79.5 fL 95% CI -2.5 to -0.6, p = 0.001), ferritin (50.7 μg/L vs 34.4 μg/L 95% CI -
30.7 to -1.9, p = 0.0002), and total body iron. The effect of delayed cord clamping was
significantly greater for infants born to mothers with low ferritin at delivery, breastfed infants
not receiving iron-fortified milk or formula, and infants born with birth weight between
2500g and 3000g. A cord clamping delay of 2 minutes increased 6-month iron stores by
about 27-47 mg. They recorded no significant increase in the risk of neonatal polycythaemia
and jaundice.
They concluded that a delay in cord clamping of 2 minutes could help prevent iron
deficiency from developing before 6 months of age, when iron-fortified complementary foods
could be introduced.
The findings by Chaparro et al agrees with the findings of Grajeda et al and findings
by Gupta and Ramji which showed improved haematological and iron status at 2-3 months.
However, in contrast with the study by van Rheenen, this effect lasted beyond 3 months.
Andersson O55 et al., 2011 in a bid to investigate the effects of delayed umbilical cord
clamping on neonatal outcomes and iron status at 4 months of age in a European setting
conducted a randomized controlled trial in a Swedish county hospital in which 400 full term
babies born after a low risk pregnancy were randomized to delayed umbilical cord clamping
(≥180seconds after delivery) or early clamping (≤10 seconds after delivery). The main
outcome measures were haemoglobin and iron status at 4 months of age with the power
estimate based on serum ferritin levels. Secondary outcomes included neonatal anaemia,
early respiratory symptoms, polycythaemia, and need for phototherapy. In total, 382 infants
constituted the study population, and their data was analysed according to intention to treat.
From their study, they found out that at 4 months of age, infants showed no significant
differences in haemoglobin concentration between the groups, but infants subjected to
delayed cord clamping had 45% (95% confidence interval 23% to 71%) higher mean ferritin
concentration (117 μg/L v 81 μg/L, p < 0.001) and a lower prevalence of iron deficiency (1
(0.6%) v 10 (5.7%), p = 0.01, relative risk reduction 0.90; number needed to treat=20 (17 to
67)). As for secondary outcomes, the delayed cord clamping group had lower prevalence of
neonatal anaemia at 2 days of age (2(1.2%) v 10 (6.3%), p = 0.02, relative risk reduction
0.80, number needed to treat 20 (15 to 111)). There were no significant differences between
groups in postnatal respiratory symptoms, polycythaemia, or hyperbilirubinaemia requiring
phototherapy. They therefore concluded that delayed cord clamping, compared with early

11
clamping, resulted in improved iron status and reduced prevalence of iron deficiency at 4
months of age, and reduced prevalence of neonatal anaemia, without demonstrable adverse
effects.
The strength of this study laid in the fact that it is one of the largest randomized
controlled studies comparing delayed and early cord clamping in full term infants, and the
first to assess effects on iron status beyond the neonatal period in a high income country.
One limitation of the study was that it was not possible to measure the amount of
blood actually transfused from the placenta into the newborn child. Another limitation was
that the study included only full term, low risk deliveries by healthy mothers from a well
nourished population. The findings may not be generalisable to term infants with various
perinatal risk factors such as maternal diabetes or intrauterine growth restriction.
The findings from this study are supported by results from the studies by Grajeda et
al, Gupta and Ramji, and Chaparro et al. Although these were studies carried out in low and
middle income populations, this study also showed that delayed cord clamping could be
beneficial in high income countries.
Emhamed56 et al., 2004 in a randomized controlled trial to evaluate the early effects
of delayed cord clamping in term neonates born to Libyan mothers. One hundred and four
mother-baby pairs were randomly assigned into early (n=46) cord clamping (within 10
seconds after delivery) or delayed (n=58) cord clamping (after the cord stopped pulsating). At
baseline, the groups had similar demographic and biomedical characteristics, except for a
difference in maternal haemoglobin, which was significantly higher in the early clamping
group (11.7 g/dL (SD 1.3) versus 10.9 g/dL, (SD 1.6); P = 0.0035). Twenty-four hours after
delivery the mean infant haemoglobin level was significantly higher in the delayed clamping
group (18.5 g/dL versus 17.1 g/dL; p = 0.0005). No significant differences were found in
clinical jaundice or plethora. Surprisingly, blood analysis showed that two babies in the early
clamping group had total serum bilirubin levels (>15 mg/dL) that necessitated phototherapy.
There were no babies in the delayed clamping group who required phototherapy. Three
babies in the delayed clamping group had polycythaemia without symptoms, for which no
partial exchange transfusion was necessary.
They therefore concluded that delaying cord clamping until pulsations stop increases
the red cell mass in term neonates. It is a safe, simple and low cost delivery procedure that
should be incorporated in integrated programmes aimed at reducing iron deficiency anaemia
in infants in developing countries.

12
Ceriani Cernadas36 et al., 2006 conducted a study to evaluate the effect of timing of
cord clamping on neonatal venous haematocrit values and clinical outcome at term. It was a
randomized controlled trial performed in 2 Obstetrical units in Argentina on neonates born at
term without complications to mothers with uneventful pregnancies. They randomly assigned
newborns into cord clamping within the first 15 seconds (group 1), at 1 minute (group 2), or
at 3 minutes (group 3) after birth. The baby’s venous haematocrit value was measured 6
hours after birth.
Two hundred and seventy-six newborns were recruited, and mean venous haematocrit
values at 6 hours of life were 53.5% (group 1), 57.0% (group 2), and 59.4% (group 3).
Statistical analyses were performed, and results were equivalent among groups because the
haematocrit increase in neonates with late clamping was within the prespecified physiologic
range. The prevalence of haematocrit at <45% (anaemia) was significantly lower in groups 2
and 3 than in group 1. The prevalence of haematocrit at >65% was similar in groups 1 and 2
(4.4% and 5.9%, respectively) but significantly higher in group 3 (14.1%) versus group 1
(4.4%). There were no significant differences in other neonatal outcomes and in maternal
postpartum haemorrhage.
They concluded that in term newborns, cord clamping at 1 or 3 minutes after birth
resulted in an increase of venous haematocrit levels measured at 6 hours, within physiologic
ranges, and a decreased prevalence of neonatal anaemia without any harmful effect in
newborns or mothers. This practice has been shown to be safe and should be implemented to
increase neonatal iron storage at birth.
The findings from this study was in agreement with the findings from the study by
Emhamed et al., Though both studies were looking at the early effects of delayed cord
clamping on neonatal outcomes at term as their primary outcomes, there were variations in
what constituted delayed cord clamping in both studies. The study by Emhamed et al was a
two arm study with cord clamping done after the cord stopped pulsating while the study by
Ceriani Cernadas et al was a three arm study with delayed cord clamping done at 1 and 3
minutes.
A limitation of the study is that, given the characteristic of the intervention, the
physician in charge of the intervention (umbilical cord clamping) could not be blinded.
However, the health professionals who made the neonatal evaluations after birth and the
personnel in charge of the biochemical tests were blinded to the group assignment.
Jaleel R57 et al., 2009 in a study to determine the effect of delayed umbilical cord
clamping on haemoglobin (Hb) and bilirubin levels of neonates, and to identify newborn

13
babies with anaemia and refer them for treatment, randomly allocated patients admitted into
the labour ward into 2 groups. Group A included women in whom the umbilical cord was
clamped immediately after birth. In Group B, clamping was delayed until cessation of
pulsations in the cord. After cutting the cord, blood sample was obtained from the cut end of
the cord of the newborn for Hb and bilirubin. After 6 hours of birth, another blood sample
was obtained from the antecubital vein for serum bilirubin.
They recruited 200 women, 100 in each group. The mean maternal Hb was 9.75g/dl in
group A and 9.95 g/dl in group B. The average neonatal Hb was 14.1 g/dl in group A and
15.2 g/dl in group B (p = 0.008). In all, 49% of neonates in group A and 37% in group B had
Hb <14 g/dl. Serum bilirubin values at birth and at 6 hours of birth were 1.8 mg/dl and 2.5
mg/dl for group A and 1.9 mg/dl and 2.7 mg/dl for group B respectively. The difference in
bilirubin after 6 hours in the 2 groups was insignificant (p = 0.186)
They concluded that delayed cord clamping in term newborn babies, results in an
increase in haemoglobin, without causing unacceptable side effects, and it can be used as a
simple and cost free intervention for reducing the prevalence of anaemia in infants in
developing countries.
The finding from this study was consistent with findings by Ceriani Cernadas et al,
and Emhamed et al.
Based on the literature reviewed, there is considerable evidence demonstrating the
benefits of delaying cord clamping in term neonates. Delayed cord clamping seems to drive
up mean haematocrit values and serum concentrations of bilirubin, without increasing the
number of babies needing treatment for jaundice or polycythaemia.39
Early cord clamping does not benefit mothers or babies and may even be harmful.
In Nigeria, most tertiary institutions still practice early cord clamping despite weight of
current evidence demonstrating the benefits of delayed cord clamping especially in term
neonates in developing countries. As yet, there is no published local data demonstrating the
effect of timing of umbilical cord clamping in term neonates.
This study hopes to generate a local data, and also to find out whether the result obtained
would be in agreement with the mounting evidence that delayed cord clamping benefits term
neonates.

14
2.5 JUSTIFICATION
Numerous studies have confirmed that delayed umbilical cord clamping at birth
enhances red cell mass and improves iron status during infancy.4,13,57,58
Since many children living in less developed countries such as ours belong to anaemia risk
group, an effective intervention is therefore needed to improve child survival.
Delayed cord clamping is a simple, cost-free and safe delivery procedure that might
offer a sustainable strategy to reduce the risk of early infant anaemia when other interventions
are not yet feasible.
This study might help in the review of the timing of umbilical cord clamping in our
environment.

15
CHAPTER THREE
3.0 GENERAL OBJECTIVE
To determine the haematological and clinical effects of delayed umbilical cord
clamping in term neonates 24 hours after birth at the Federal Medical Centre, Abeokuta
3.1 SPECIFIC OBJECTIVES
1. To evaluate the effect of delayed cord clamping on haematocrit level at 24 hours of life.
2. To determine the effect of delayed cord clamping on bilirubin level at 24 hours of life.
3. To assess the effect of delayed cord clamping on neonatal morbidity (including
polycythaemia, need for phototherapy, and respiratory symptoms)
4. To evaluate the effect of delayed cord clamping on the infant’s haematocrit level at 6
weeks of life
3.2 HYPOTHESIS
10 Delayed cord clamping will not enhance neonatal haematocrit level
1i Delayed cord clamping will enhance neonatal haematocrit level
20 Delayed cord clamping does not increase the risk of neonatal morbidity
2i Delayed cord clamping increases the risk of neonatal morbidity

16
CHAPTER FOUR
4.0 METHODOLOGY
4.1 STUDY DESIGN
A prospective randomized controlled study.
4.2 STUDY AREA
The study was carried out in the labour ward of the Department of Obstetrics and
Gynaecology as well as the neonatal unit of the Department of Paediatrics at the Federal
Medical Centre, Abeokuta.
Abeokuta is the capital city of Ogun state and is located in South-Western Nigeria. It is
situated 74 km north of Lagos along Ogun River and has a population of about 600 000
people with most of its inhabitants being “Egbas”, a sub-group of the Yoruba people.
Abeokuta is made up of two local government areas: Abeokuta North and Abeokuta South.
Federal Medical Centre, Abeokuta is a tertiary health care centre located in Idi-Aba
within Abeokuta South local government area on the outskirts of the city. It has an annual
average delivery rate of 1200 live births per annum.
The department of Obstetrics and Gynaecology consists of seven units: Antenatal, labour and
postnatal wards, gynaecological emergency unit, gynaecological ward, Outpatient clinics and
the Family Planning unit, while the Paediatrics department consists of the neonatal ward,
children’s ward, children’s emergency room, the paediatrics outpatient department, and the
consultant specialist clinics.
4.3 STUDY POPULATION
All pregnant women presenting for vaginal delivery at the Federal Medical Centre,
Abeokuta during the study period, who met the inclusion criteria. The hospital offers
obstetric services to the Abeokuta community and its environs. The patients are mainly civil
servants, teachers, traders and a minority being farmers. They belong to two main religions,
Christianity and Islam though a few are traditionalists.

17
4.3.1 INCLUSION CRITERIA
Women with uncomplicated, singleton, term pregnancy (gestational age 37+0 to 41+6)
determined by LMP or early USS who were admitted into the labour ward for vaginal
delivery during the study period, and who gave consent for the study.
4.3.2 EXCLUSION CRITERIA
1. Rhesus negative blood group
2. HBsAg positive women
3. HIV positive women
4. Multiple pregnancy
5. Severe antepartum haemorrhage
6. Gestational diabetes mellitus
7. Preeclampsia
8. Intrauterine growth restriction
9. Instrumental delivery
10. Need for early cord clamping (tight nuchal cord, resuscitation)
11. Major congenital abnormality (NTDs)
12. Infants weighing <2.5kg
Criteria 1 to 8 were applied before randomization while criteria 9 to 11 were applied after
randomization.
4.4 SAMPLE SIZE DETERMINATION
The sample size for the study was calculated using the formula for comparison of two
means.59
n = (u + v) 2 (σ1 2 + σ0
2 )
(μ1 – μ 0) 2
Where,
n = minimal sample size per group
u = standard normal deviate corresponding to the probability of making type II
error (β) of 20%. Power at 80% = 0.84
v = standard normal deviate corresponding to the probability of type I error (α) at 5% =
1.96

18
σ0 = standard deviation of heamatocrit level after 24 hours in control group in a previous
study by Emhamed et al56 = 5.7
σ1 = standard deviation of haematocrit level after 24 hours in the intervention
group in a previous study by Emhamed et al56 = 6.3
μ1 – μ 0 = difference between the means in haematocrit level between the two groups
= 3.6
n= (0.84 + 1.96)2 (6.32 + 5.72)
(52.9 – 49.3)2
n = (7.84) (39.69 + 32.49)
(3.6)2
n = 43.6 ≈ 44
Therefore, the minimum sample size in each group was 44
For the two groups, total sample size = 44 + 44 = 88
For an attrition rate of 20%, adjustment factor =
100____ = 1.25
100 – 20
Therefore, desired sample size was
1.25 x 88 = 110
Hence, a minimum of 110 participants was required for statistical inference.

19
4.5 STUDY PROCEDURE
Pregnant women were given information about the study at the antenatal clinic by the
investigator. Those who fulfilled the inclusion criteria who presented for vaginal delivery at
the labour ward following spontaneous onset of labour, or those planned for induction of
labour, were again informed about the study by the investigator or the resident doctor
assigned to do so and informed consent was obtained.
Eligible participants were randomly assigned into either of the two groups; delayed
cord clamping (intervention) group and the early cord clamping (control) group.
Randomization was achieved by a computer generated random number list between 1
and 110. All 55 numbers generated by the computer were assigned to the delayed cord
clamping (intervention) group, while the remaining 55 numbers were assigned to the early
cord clamping (control) group. The numbers from 1 to 110 were written on pieces of paper
and placed in a large brown opaque envelope from where each woman drew from until
completion of the study. The numbers generated by the computer which belonged to the
intervention group were written boldly on cardboard paper and placed in the labour ward for
easy identification by the attending doctor or midwife.
Before delivery, a semi structured pretested questionnaire was used to obtain socio-
economic and demographic details from the mother as well as information on reproductive
health.
The delivery was supervised or conducted by the investigator, the designated
registrar, or midwife who had been fully briefed on the methodology of delayed cord
clamping.
Following delivery, the babies were placed on a draped adjustable trolley, distal to the
mother’s perineum, and adjusted to be at par with the level of the uterus. The babies were
dried and wrapped in warm linen to prevent hypothermia, and remained in this position until
the cord was clamped.
For the patients randomized into the DCC group, the umbilical cord was double
clamped and cut between clamps at two minutes. The exact time was recorded by the use of a
stopwatch, by the research assistant and it was measured as the time from complete expulsion
of the fetus to the first clamp on the umbilical cord.
Those randomized into the ECC group, had clamping done within 10 seconds after
delivery, which is the routine standard of care at the centre. Ten international units of
oxytocin was administered to the mother intramuscularly or intravenously if she had an

20
intravenous canula in-situ after cord clamping. Labour and delivery were conducted
following the standard practice of care.
At 24 hours of life, blood was obtained from the dorsum of the hand of the baby after
cleaning with methylated spirit, for the estimation of venous haematocrit and serum bilirubin.
Blood was collected in 2 heparinised capillary tubes which was sealed at one end with
modelling clay and centrifuged for 5 minutes using HaematoSpin 1400 (Hawksley, England).
Haematocrit estimation was done using the Micro-Haematocrit reader (Hawksley, England)
at the side laboratory by the designated registrar in the labour ward. The side laboratory is
fully operational on a 24 hour basis, and at all times, the designated registrar in the labour
ward was informed about the time of sample collection which was boldly written on a white
sticker attached to the patient’s case note.
The estimation of serum bilirubin was done by obtaining 4 ml of blood in Lithium
Heparin vacuum tube and analysed using the RANDOX BILIRUBIN kit which employs the
colorimetric method based on that described by Jendrassik and Grof (1938). The samples for
bilirubin estimation were centrifuged immediately after collection at 4000g for 15 minutes,
and the supernatant was carefully collected using a disposable plastic pipette and placed in
plain sample bottles. The sample bottles were placed in a small brown envelope (to protect
them from light) and stored in the refrigerator at 4-80C and analysed within 24 hours of
separation. The analysis was carried out in the hospital laboratory by the designated
laboratory scientist.
All the babies were examined by the paediatric resident at birth, and 24 hours post
delivery for clinical signs of hyperviscosity syndrome, hyperbilirubinaemia and
polycythaemia.
All the baby’s anthropometric measurements (weight and length) were obtained using
the Salter 15kg-50g model 180 baby weighing scale and an infantometer respectively.
Before discharge, an assessment of gestational age was completed by the Ballard-external
method.60 This was done by the paediatric resident.
All neonatal diagnoses as well as the outcome variables were recorded in the data sheet.
Neonatal anaemia was defined as a venous haematocrit level of <45%, polycythaemia as
venous haemantocrit of >65%, hyperbilirubinaemia as bilirubin >10 mg/dL at 24 hours of
life, clinical jaundice as yellowness of the sclera and/or skin and neonatal tachypnoea as
respiratory rate > 60/ minute.

21
Given the characteristics of the intervention, the accoucheur was not blinded. However, the
paediatrician performing neonatal examinations as well as the registrar and laboratory staff
performing analysis of blood samples were blinded to each baby’s allocation group.
The babies were scheduled for a follow-up visit at the postnatal clinic after 6 weeks,
where venous blood sample for haematocrit, weight and length measurements were obtained
and recorded on the data sheet.
4.5.1 DATA COLLECTION INSTRUMENT
A semi structured pretested questionnaire was used to obtain information from eligible
participants. The questionnaire was divided into the following sections:
Section A: Socio-demographic information
Section B: Antenatal care information
Section C: Reproductive Health
4.5.2 ANALYSIS OF DATA
Data obtained at the end of the study was processed using SPSS version 19.
Quantitative variables were presented using means and standard deviations, categorical
variables were presented using proportions. Associations was tested using chi squared test
and Student’s t test for categorical and continuous variables respectively. Significance level
was set at 5%.
Data analysis was done by the researcher with the assistance of a medical statistician
and findings were compared with those of previous studies.
4.6 ETHICAL CONSIDERATION
Ethical permission to carry out the study was sought from the hospital’s Health
Research Ethics Committee (HREC) before the commencement of the study.
4.6.1 INFORMED CONSENT
Detailed information, explanation and nature of the study was offered to every
woman found to be eligible for the study and an informed consent was obtained. Each
participant was given the opportunity to ask questions about the study and appropriate
answers were provided.
The informed consent was translated into the local language and read to every
prospective participant in the language she understood.

22
4.6.2 CONFIDENTIALITY OF DATA
The participants were assured of the confidentiality of the data and access to study
data was made available only to study personnel.
4.6.3 BENEFICIENCE TO PARTICIPANTS
The study is hoped to be beneficial to patients in the long run as it seeks to prevent or
slow the onset of iron deficiency by increasing the infant’s iron endowment at birth.
4.6.4 NON-MALFICENCE TO PARTICIPANTS
The study was not in any way harmful to the participants
4.6.5 RIGHT TO DECLINE/WITHDRAWAL FROM THE STUDY
Participants were assured of their right to decline or withdraw from the study at
anytime and following their withdrawal, they were not denied any benefit or care.
4.6.7 FUNDING FOR THE STUDY
The funding for the study was provided solely by the researcher
4.6.8 QUALITY ASSURANCE
The objectives and methodology of the study was clearly explained and discussed at a
stakeholders meeting involving the researcher, doctors and nurses working in the labour
ward, post-natal ward as well as the neonatal unit, and the laboratory scientist.
The data sheet was introduced to the doctors who were involved in filling them.
4.7 DISSEMINATION OF FINDINGS
The findings of the study will be disseminated by submission of the dissertation to the
National Postgraduate Medical College of Nigeria for the part II Fellowship Examination in
the Faculty of Obstetrics and Gynaecology and within the Department of Obstetrics and
Gynaecology, Federal Medical Centre, Abeokuta.
It will also be published in a peer reviewed journal in conjunction with the
supervising consultants.

23
CHAPTER FIVE
5.0 RESULTS
During the study period, a total of 110 mother-infant pairs who met the eligibility
criteria for the study were counselled and consented for the study. Fifty-five mother-infant
pairs were randomized into the early cord clamping (ECC) group and another 55 into the
delayed cord clamping (DCC) group.
A total of 11 (10%) mother-infant pairs (7 from the ECC group and 4 from the DCC
group) did not turn up for the follow up visit at the post-natal clinic and were thus excluded
from the analysis.
As a result, 48 (43.6%) mother-infant pairs remained in the ECC group and 51 (46.4%) in the
DCC group.
Table I shows the maternal characteristics. The mean (SD) age of mothers in the ECC group
was 31.3 (4.5) years while that of mothers in the DCC group was 31.0 (4.2) years (t = 0.34, df
= 97, p = 0.732). There was no statistically significant age difference between the two groups.
Most of the women in both groups were < 35 years, accounting for thirty-eight (79.2%) and
39 (76.5%) in the ECC and DCC groups respectively. None of the mothers was a teenager.
Many of the women were multiparous 65 (65.7%), while 34 (34.3%) were primipara.
Of the multiparous women, only one (1.0%) woman was grand-multipara and she belonged
to the DCC group. Majority of the mothers 86 (86.9%) had tertiary level of education; 41
(85.4%) for the ECC group and 45 (88.2%) for the DCC group. Only 3 (3.0%) participants
had none or primary level of education.
The mean (SD) prepartal haematocrit was significantly higher in the ECC group
39.9% (3.3) than in the DCC group 36.8% (4.1); (t = 4.13, df = 97, p = 0.0001)
The mean (SD) number of ANC visits was found to be similar for both groups; 6.3
(2.4) for the ECC group and 6.4 (2.7) in the DCC group.
The mean (SD) EBL was 187.5ml (74.7) and 201.6ml (72.7) for the ECC and DCC
groups respectively. Although the mean EBL in the DCC group was higher than that in the
ECC group, this was not statistically significant. (t = 0.95, df = 97, p = 0.344). None of the
participants had primary post-partum haemorrhage.
Table II shows the baseline characteristics of the babies. The mean (SD) gestational
age of babies in the ECC group was 39.7 weeks (1.1) while that of babies in the DCC group
was 39.2 weeks (1.2); (t = 2.16, df = 97, p = 0.033)
The sex distribution of the babies showed that there were more males in the ECC
group compared with the DCC group which had more females.
24
The mean (SD) apgar score at the first minute of life revealed that babies in the DCC
group had higher apgar scores compared with babies in the ECC group; 8.4 (0.7) vs 7.8 (1.1).
This difference was statistically significant; (t = 3.26, df = 97, p = 0.002)
The mean (SD) birth weight of babies in the ECC group was 3050g (329), and that of
babies in the DCC group was 3150g (426). This did not differ significantly; (t = 1.30, df = 97,
p = 0.196). Likewise, the birth length of babies in both groups did not differ significantly.
The mean (SD) birth length of babies in the ECC group was 48.7 cm (1.8) and 49.2 cm (2.6)
for babies in the DCC group; (t= 1.11, df = 97, p = 0.271).
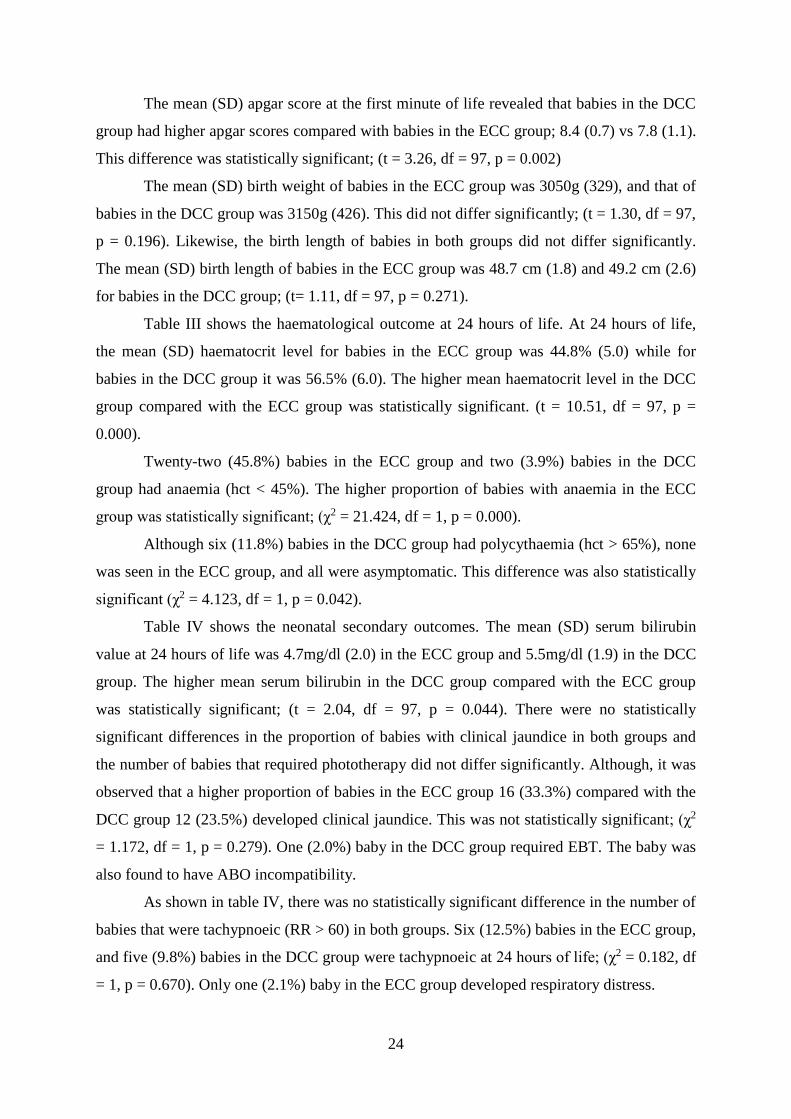
Table III shows the haematological outcome at 24 hours of life. At 24 hours of life,
the mean (SD) haematocrit level for babies in the ECC group was 44.8% (5.0) while for
babies in the DCC group it was 56.5% (6.0). The higher mean haematocrit level in the DCC
group compared with the ECC group was statistically significant. (t = 10.51, df = 97, p =
0.000).
Twenty-two (45.8%) babies in the ECC group and two (3.9%) babies in the DCC
group had anaemia (hct < 45%). The higher proportion of babies with anaemia in the ECC
group was statistically significant; (χ2 = 21.424, df = 1, p = 0.000).
Although six (11.8%) babies in the DCC group had polycythaemia (hct > 65%), none
was seen in the ECC group, and all were asymptomatic. This difference was also statistically
significant (χ2 = 4.123, df = 1, p = 0.042).
Table IV shows the neonatal secondary outcomes. The mean (SD) serum bilirubin
value at 24 hours of life was 4.7mg/dl (2.0) in the ECC group and 5.5mg/dl (1.9) in the DCC
group. The higher mean serum bilirubin in the DCC group compared with the ECC group
was statistically significant; (t = 2.04, df = 97, p = 0.044). There were no statistically
significant differences in the proportion of babies with clinical jaundice in both groups and
the number of babies that required phototherapy did not differ significantly. Although, it was
observed that a higher proportion of babies in the ECC group 16 (33.3%) compared with the
DCC group 12 (23.5%) developed clinical jaundice. This was not statistically significant; (χ2
= 1.172, df = 1, p = 0.279). One (2.0%) baby in the DCC group required EBT. The baby was
also found to have ABO incompatibility.
As shown in table IV, there was no statistically significant difference in the number of
babies that were tachypnoeic (RR > 60) in both groups. Six (12.5%) babies in the ECC group,
and five (9.8%) babies in the DCC group were tachypnoeic at 24 hours of life; (χ2 = 0.182, df
= 1, p = 0.670). Only one (2.1%) baby in the ECC group developed respiratory distress.

25
A total of six (6.1%) babies, three (5.9%) from the DCC group and three (6.3%) from the
ECC group were admitted to NICU. The mean (SD) length of hospital stay was 2.7 days (2.0)
in the ECC group and 2.4 days (1.2) in the DCC group. No statistically significant difference
was observed in the mean length hospital stay in either group; (t = 0.91, df = 97, p = 0.364)
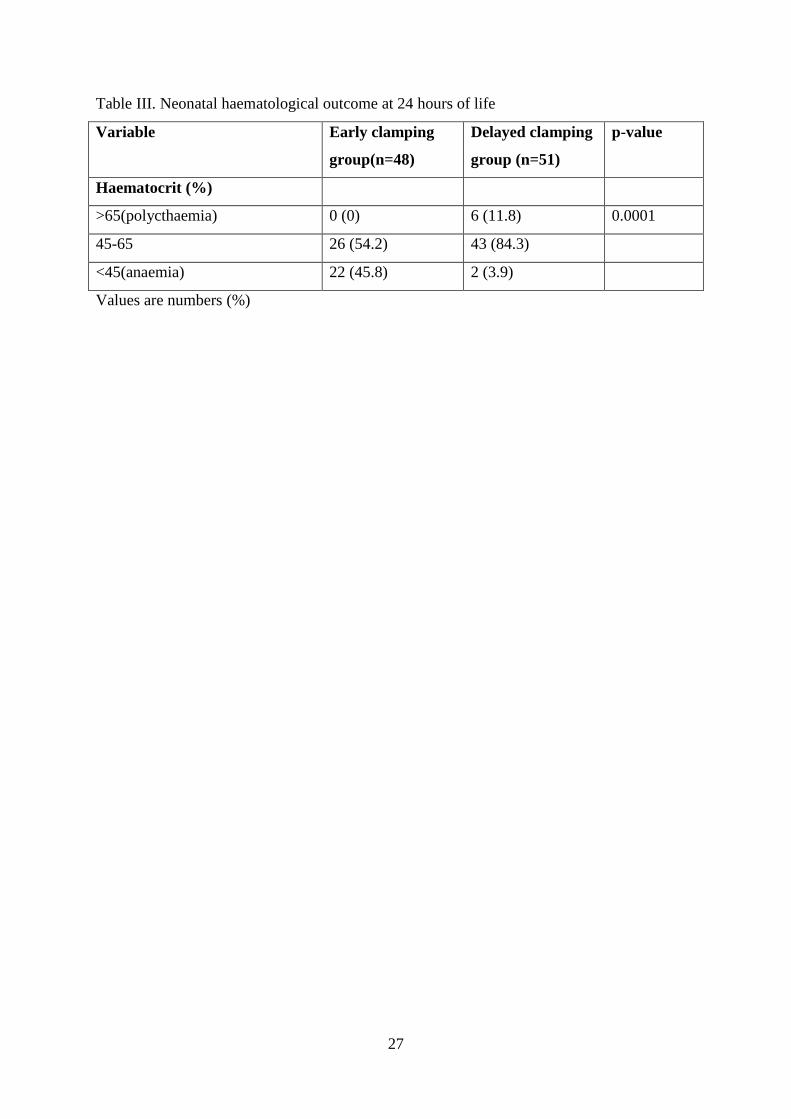
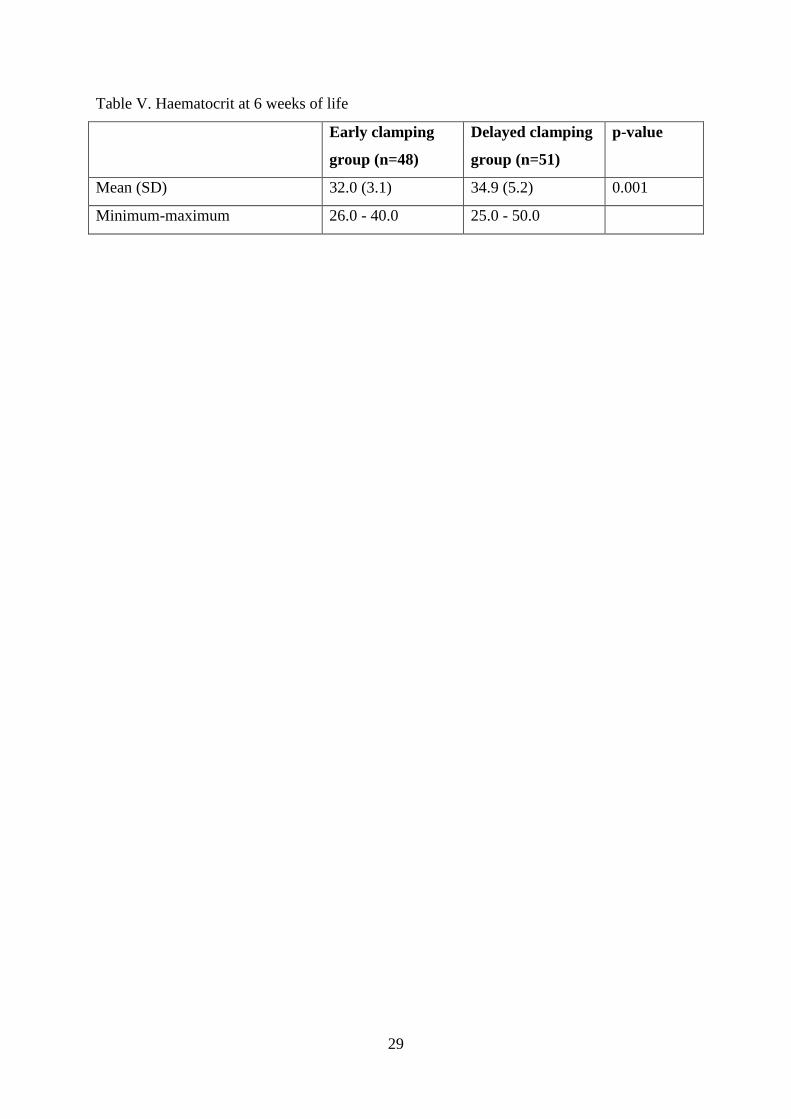
At 6 weeks of life, as shown in table V, the mean (SD) haematocrit level was 32.0%
(3.1) in the ECC group and 34.9% (5.2) in the DCC group. The higher mean haematocrit
level in the DCC group compared with the ECC group was statistically significant. (t = 3.34,
df = 97, p = 0.001).
Although more babies in the ECC group 9 (18.8%) compared with 4 (7.8%) in the DCC
group had a haematocrit < 30% at 6 weeks of life, this difference was not statistically
significant; (χ2 = 1.711, df = 1, p = 0.191).
There was no significant difference in the mean (SD) weights of the babies at 6 weeks in both
groups; 4.9 kg (0.8) in the DCC group vs 4.7 kg (0.7) in the ECC group; (t = 1.32, df = 97, p
= 0.190).

26
Table I. Maternal characteristics
Variable Early clamping
group (n=48)
Delayed clamping
group (n=51)
p-value
Age (years)
<35 38 (79.2) 39 (76.5) 0.747
≥35 10 (20.8) 12 (23.5)
Parity (including study child)
Primipara 15 (31.2) 19 (37.3) 0.486
Multipara 33 (68.8) 31 (60.8)
Grand multipara 0 (0) 1 (1.9)
Educational level
None or primary 1 (2.1) 2 (3.9) 0.661
Secondary 6 (12.5) 4 (7.8)
Tertiary 41 (85.4) 45 (88.3)
Prepartal haematocrit (%)
<30 2 (4.2) 1 (2.0) 0.957*
≥30 46 (95.8) 50 (98.0)
Number of antenatal visits
<4 6 (12.5) 7 (13.7) 0.857
≥4 42 (87.5) 44 (86.3)
Values are numbers (%) * Yates’s correction
Table II. Newborn characteristics
Variable Early clamping
group(n=48)
Delayed clamping
group(n=51)
p-value
Sex
Male 26 (54.2) 20 (39.2) 0.136
Female 22 (45.8) 31 (60.8)
Apgar score at 1 min
≥7 45 (93.8) 51 (100) 0.220*
<7 3 (6.2) 0 (0)
Values are numbers (%), * Yates’s correction
27
Table III. Neonatal haematological outcome at 24 hours of life
Variable Early clamping
group(n=48)
Delayed clamping
group (n=51)
p-value
Haematocrit (%)
>65(polycthaemia) 0 (0) 6 (11.8) 0.0001
45-65 26 (54.2) 43 (84.3)
<45(anaemia) 22 (45.8) 2 (3.9)
Values are numbers (%)

28
Table IV. Neonatal secondary outcomes
Variable Early clamping
group (n=48)
Delayed clamping
group (n=51)
p-value
Serum bilirubin at 24 hrs
(mg/dl)
≥10 1 (2.1) 1 (2.0) 1.000*
<10 47 (97.9) 50 (98.0)
Clinical jaundice
yes 16 (33.3) 12 (23.5) 0.279
no 32 (66.7) 39 (76.5)
Phototherapy
yes 2 (4.2) 3 (5.9) 1.000*
no 46 (95.8) 48 (94.1)
EBT
yes 0 (0) 1 (2.0) 1.000*
no 48 (100) 50 (98.0)
Respiratory rate at 24 hrs
>60 6 (12.5) 5 (9.8) 0.670
≤60 42 (87.5) 46 (90.2)
Respiratory distress
yes 1 (2.1) 0 (0) 0.976*
no 47 (97.9) 51 (100)
NICU admission
yes 3 (6.3) 3 (5.9) 1.000*
no 45 (93.7) 48 (94.1)
Mean length of hospital stay
in days (SD)
2.7 (2.0) 2.4 (1.2) 0.364
Values are numbers (%) unless otherwise stated, * Yates’s correction
29
Table V. Haematocrit at 6 weeks of life
Early clamping
group (n=48)
Delayed clamping
group (n=51)
p-value
Mean (SD) 32.0 (3.1) 34.9 (5.2) 0.001
Minimum-maximum 26.0 - 40.0 25.0 - 50.0

30
5.1 HYPOTHESIS TESTING
Hypothesis 1
The alternate hypothesis that delayed cord clamping will enhance neonatal haematocrit level
was hereby accepted based on a p-value of 0.0001 which was found to be statistically
significant.
Hypothesis 2
The null hypothesis that delayed cord clamping does not increase the risk of neonatal
morbidity was hereby accepted because there was no statistically significant difference in the
risk of neonatal morbidity.
31
CHAPTER SIX
6.0 DISCUSSION
This prospective randomised controlled study was done to determine the effect of a
two minute delay in umbilical cord clamping of term neonates on haematocrit level, and the
risk of morbidity 24 hours after birth at the Federal Medical Centre, Abeokuta. The study also
went further to evaluate the effect of delayed cord clamping on the infant’s haematocrit level
at 6 weeks postpartum.
Most of the mothers in the study were less than 35 years, mostly multiparous and
majority had a tertiary level of education reflecting the young dynamic nature of the
population and the emphasis placed on education in South West Nigeria.
Although the mean prepartal haematocrit was significantly higher in the ECC group
compared with the DCC group, there were no significant differences in the other
demographic and biomedical variables of women between the two groups. This is similar to
the finding in the study by Emhamed56 et al in Libya.
However, in their study, they found a significantly higher number of women with
anaemia in the DCC group compared with the ECC group on admission to labour room. In
the present study, only 3 women had anaemia upon admission into labour ward (2 women in
the ECC group and 1 woman in the DCC group). This reflects the emphasis placed on routine
PCV checks during the ANC clinic and correction of anaemia prior to delivery. It may also
be a reflection on the level of adherence to routine haematinics during ANC.
The study found a significant increase in the mean neonatal haematocrit value at 24
hours of life of babies in the DCC group compared with babies in the ECC group. This
finding was consistent with that of Emhamed56 et al, Ceriani Cernadas36 et al in Argentina,
van Rheenen53 et al in Zambia, Andersson O55 et al in Sweden, Chaparro54 et al in Mexico
and Jaleel R57 et al in Pakistan but different from findings in the study conducted by
Grajeda13 et al in Guatemala, Gupta and Ramji52 in India and Jahazi61 et al in Iran.
In the studies by Emhamed et al and Van Rheenen et al, they found a significantly
higher haematocrit in the DCC group compared with the ECC group after 24 hours. In both
studies, delayed cord clamping was done after caessation of cord pulsation at an average of
3.5 and 5 minutes respectively. In this study, delayed clamping was done at 2 minutes. Both
studies looked at the early haematological effects of delayed cord clamping as was done in
the present study.
In the Libyan study, the babies were placed on the mother’s abdomen (above the level of the
placenta), while in the Zambian study, the babies were placed 10 cm below the vaginal
introitus (below the level of the placenta). In the present study, babies were placed at the

32
same level as the placenta. This shows that the level of the newborn after delivery does not
significantly influence haematocrit value in the first 24 hours.
Andersson O et al, in their study which was conducted in a high income country, also found a
significantly higher haematocrit level in the DCC group at a median age of 2.4 days. Ceriani
Cernadas et al as part of their secondary outcome measures looked at heamtocrit value at 24
to 48 hours and also found a significantly higher haematocrit in the DCC group at 1 and 3
minutes. Theirs was a 3-arm study with delayed clamping done at 1 and 3 minutes. Both
studies included eligible mothers that had vaginal delivery as well as caesarean section. The
present study was limited to vaginal deliveries only.
Chaparro et al and Jaleel et al also found a significantly higher haematocrit/haemoglobin
value in the DCC group at 4-8 hours after birth.
The study by Gupta and Ramji did not find a significant difference in the haemoglobin value
of newborn at birth, while Grajeda et al did not find a significant difference in haematocrit
value at 24 hours between the two groups.
In the Indian study, though delayed cord clamping was done after decent of the
placenta into the vagina, with the newborn held below the level of the placenta, haemoglobin
estimation at birth was done using cord blood sample which may be responsible for the lack
of significant difference. Studies have shown that cord blood haematocrit is not affected by
placental transfusion.62 In the present study, sample for haematocrit estimation was obtained
after 24 hours from the dorsum of the hand of the baby.
In the Guatemalan study, the lack of a significant difference in haematocrit value at
24 hours may be attributed to the method of randomization. The study population consisted
of 3 groups, and randomization was done by day of the week, that is, a different delivery
method was used per day so that each treatment was repeated every third working day. Also,
venous sample for haematocrit estimation was obtained from a subset of babies (the last 41
recruited into the study). This may not have given every baby an equal chance of being
selected compared to the present study in which randomization was achieved by a computer
generated random number list, thus every baby had an equal chance of being selected.
Jahazi et al in Iran also did not find a significant difference in haematocrit value at 2
and 18 hours of life. In their study, early cord clamping was done at 30s compared with < 10s
in the present study. This timing might have enhanced placental transfusion as placental
transfusion is said to occur when cord clamping is delayed for at least 5s7.
The proportion of babies with anaemia at 24 hours was significantly higher in the
ECC group compared with the DCC group. This finding was consistent with studies done by
Andersson O et al and Ceriani Cernadas et al. This might be related to the high prevalence of

33
maternal iron deficiency in our environment which has also been reported in high income
countries.63 The study by Jaleel et al in Pakistan did not show a significant difference in the
proportion of babies with anaemia in either group. The observed lack of difference might be
due to the use of cord blood which was obtained at birth for the estimation of haemoglobin.
However, in the present study, venous blood sample obtained from the dorsum of the hand of
the baby after 24 hours was used for the estimation of haematocrit.
In the present study, the mean serum bilirubin at 24 hours was significantly higher in
the DCC group compared with the ECC group. This finding was different from that
documented by Andersson O et al, Ceriani Cernadas et al, Emhamed et al, and Jaleel et al; all
of which found no significant difference in total bilirubin value in either group, which might
be due to the different techniques employed in the assessment of serum bilirubin.
However, no significant differences were observed in the number of babies with
hyperbilirubinaemia and clinical jaundice which were consistent with the studies done by
Chaparro et al, Andersson O et al, Ceriani Cernadas et al, Emhamed et al, and Jaleel et al and
also in agreement with a recent meta-analysis.39
As observed in the present study, six babies had polycythaemia, and none was seen in
the ECC group. None of the babies however were symptomatic. This was consistent with the
Libyan and Mexican studies, but the difference did not reach a significant level for both
studies. Although consistent with the study carried out in Guatemala, this was a 3-arm study,
and the proportion of neonates with polycythaemia was significantly higher in those that had
delayed clamping done with the baby placed below the level of the placenta than in those that
had the baby placed at the same level as the placenta. Babies were placed at the same level as
the placenta in the present study.
No significant differences were observed in the groups with regard to the proportion
of neonates with polycythaemia in the Zambian study which set the cut-off for polycythaemia
as PCV > 70 percent compared with > 65 percent in the present study.
In the present study, no significant differences were observed in the number of babies
that required phototherapy or in the number of babies with respiratory symptoms in either
group which was consistent with the studies done by Ceriani Cernadas et al, and Andersson
O et al.
One baby required EBT in the DCC group, who was discovered to have ABO
incompatibility. No other study documented the need for EBT among babies with delayed
cord clamping. This corroborates the fact that associated morbidities could result in the need
for EBT apart from a high haematocrit level.

34
No significant difference was observed in admission rate to NICU in the present study
as observed in the study done by Ceriani Cernadas et al, the only recent study that reported
this outcome variable.39
Though the length of hospital stay in the present study was longer in the ECC group
compared with the DCC group, it was not statiscally significant. This was consistent with the
Argentinean study.
At the 6th week of life, the haematocrit value of the babies was assessed and it was
observed that babies in the DCC group had a significantly higher haematocrit value compared
to babies in the ECC group. This observed effect was similar to that found at 2 months by
Grajeda et al and at 3 months by Gupta and Ramji.
The findings were inconsistent with the studies conducted by Andersson O et al and
Chaparro et al which found no significant difference in haematocrit value at 4 and at 6
months respectively. However, the Mexican study went ahead to analyse the iron status
(mean corpuscular volume, ferritin, body iron, and stored iron) of the babies at 6 months and
it was found to be significantly higher in the DCC group. The mean ferritin concentration was
also significantly higher at 4 months in the DCC group in the Swedish study. The present
study was only limited to 6 weeks postpartum and the indicators of iron status were not
analysed.
In the present study and as reported in a Cochrane review, there was no significant
difference in the mean postpartum blood loss between the early and delayed cord clamping
groups.29 None of the participants in the present study had primary PPH. Postpartum blood
loss was quantified by visual estimation.
No significant differences were observed in neonatal adverse event rates between the two
groups and no maternal or neonatal mortality was observed in the study population.
Delayed cord clamping in this randomized controlled study improved neonatal
haematocrit value in the first 24 hours of life and at 6 weeks postpartum and it did not
increase the risk of neonatal morbidity.

35
6.1 LIMITATIONS OF THE STUDY
Given the characteristics of the intervention, the mother as well as the resident doctor
or midwife conducting the delivery could not be blinded to the assigned intervention.
Serum ferritin which is the most sensitive indicator of iron status was not assayed for
as was done in other studies because it is not routinely done in the hospital laboratory.
A follow up study for a longer period could not be done in view of the nature of the
timing of the residency training programme.

36
6.2 CONCLUSION
In the present study, it was concluded that
Delaying clamping of the umbilical cord in term neonates for two minutes after
delivery resulted in a higher mean haematocrit value of the newborn in the first 24
hours of life.
Delayed cord clamping resulted in persistence of a high haematocrit value up to 6
weeks postpartum.
Delayed cord clamping resulted in a significant reduction in the proportion of
anaemic neonates and it did not increase the risk of neonatal morbidity.

37
6.3 RECOMMENDATION
Delayed cord clamping is beneficial to babies by enhancing their haematocrit value without
increasing adverse neonatal outcomes.
This practice is safe and should therefore be incorporated into delivery protocols in our
environment to reduce the incidence of neonatal anaemia.
6.4 AREAS OF FURTHER RESEARCH
1. Impact of delayed cord clamping on ABO incompatibility.
2. Delayed cord clamping at caesarean section in view of the rising caesarean section
rate in our environment.
3. Effect of delayed cord clamping on serum ferritin level.

38
REFERENCES
1. AGSP. 100 years on, and still no answer [commentary]. Paediatrics. 1975;55:813
2. World Health Organization. Maternal and Newborn Health/Safe Motherhood, Care of the
Umbilical cord: A Review of the Evidence. Geneva Switzerland: Department of Reproductive
Health and Research, World Health Organization;1998. Document WHO/RHT/MSM/98.4
3. Peltonen T. Placental transfusion: Advantage and disadvantage. Eur J Pediatr. 1981;137:141-
6
4. Pisacane A. Neonatal prevention of iron deficiency – Placental transfusion is a cheap and
physiological solution. BMJ. 1996;312:136-7
5. Philip AG, Saigal S. When should we clamp the umbilical cord? Neoreviews 2004;5:42-54
6. Prendiville WJ, Elbourne D, McDonald S. Active versus expectant management in the third
stage of labour. Cochrane Database Syst Rev 2000;2:CD000007
7. Mercer JS. Current best evidence: A review of the literature on umbilical cord clamping. J
Midwifery Womens Health. 2001;46:402-14
8. Mercer JS, Skovgaard RL. Neonatal transitional physiology. J Perinat Neonatal Nurs.
2002;15:56-75
9. Brabin BJ, Prinsen-Geerligs P, Verhoeff F, Kazembe P. Anaemia prevention for reduction of
mortality in mothers and children. Transactions of the Royal Society of Tropical Medicine
and Hygiene. 2003b;97:36-38
10. ACC/SCN. Preventing and treating anaemia. In: Allen LH, Gillespie SR, eds. What works? A
review of the efficacy and effectiveness of nutrition interventions. Geneva: ACC/SCN in
collaboration with the Asian Development Bank, Manila, 2001:43-54
11. Grantham-McGregor S, Ani C. A review of the studies of iron deficiency on cognitive
development in children. J Nutr. 2001;131:649S-68S
12. Blood. In: Haneef SM, Maqbool S, Arif MA, eds. Textbook of Paediatrics. Lahore :
International Book Bank; 2004.545-85
13. Grajeda R, Perez-Escamilla R, Dewey KG. Delayed clamping of the umbilical cord improves
haematologic status of Guatemalan infants at 2 months of age. Am J Clin Nutr. 1997;65:425-
31
14. Michaelsen KF, Milman N, Samuelson G. A longitudinal study of iron status in healthy
Danish infants: Effects of early iron status, growth velocity and dietary factors. Acta
Paediatr. 1995;84:1035-44
39
15. Van Rheenen P, Brabin BJ. Late umbilical cord clamping as an intervention for reducing iron
deficiency anaemia in term infants in developing and industrialised countries: A systematic
review. Ann Trop Paediatr. 2004;24:3-16
16. ACOG Committee Opinion No.543. Timing of umbilical cord clamping after birth.
Committee Opinion, American College of Obstetricians and Gynaecologists. Obstet
Gynaecol 2012;120:1522-6
17. Rosenkrantz TS. Polycythaemia and Hyperviscosity in the newborn. Semin Thromb.
Haemost. 2003;29:515-27
18. Rabe H, Reynolds G, Diaz-Rossello J. Early versus delayed umbilical cord clamping in
preterm infants (review). Cochrane Database Syst Rev. 2004;4: CD003248
19. Eichenbaum-Pikser G, Zasloff JS. Delayed clamping of the umbilical cord: A review with
implications for practice. J Midwifery Womens Health. 2009; 5(4):321-6
20. Van Rheenen PF, Brabin BJ. A practical approach to timing cord clamping in resource poor
settings. BMJ. 2006;333:954-8
21. Coggins M, Mercer J. Delayed cord clamping: Advantages for infants. Nurs Womens Health.
2009;13:132
22. Farrar D, Airey R, Law G, Tufnell D, Cattle B, Duley L. Measuring placental transfusion for
term births: Weighing babies with cord intact. BJOG 2011;118:70-75
23. Gutierrez A, Velasquez R, Iriarte M. Analysis of clinical course in term patients with early
and delayed umbilical cord clamping after birth. The Internet Journal of Paediatrics and
Neonatology. 2009; 11(2)
24. Yao AC, Lind J. Effect of gravity on placental transfusion. Lancet. 1969;2(7619): 505-8
25. Dunn PM. Dr. Erasmus Darwin (1731-1802) of Lichfield and placental respiration. Arch Dis
Child Foetal Neonata Ed. 2003;88:F346-F348
26. Raju TNK, Singal N. Optimal timing for clamping the umbilical cord after birth. Clin
Perinatol. 2012;39(4): 889-900
27. Weeks A. Umbilical cord clamping after birth. BMJ. 2007;335:312-3
28. Spencer PM. Controlled cord traction in management of the third stage of labour. BMJ.
1962;1:1728-32
29. McDonald SJ, Middleton P. Effect of timing of umbilical cord clamping of term infants on
maternal and neonatal outcomes. Cochrane Database Syst Rev. 2008;2:CD004074
30. UNICEF. Maternal mortality. http://www.childiinfo.org/eddb/mat_mortal/index.htm
(accessed 24 October 2002)
31. WHO. Department of making pregnancy safer. WHO recommendations for the prevention of
postpartum haemorrhage. Geneva: WHO, 2007

40
32. WHO. The World Health Report 2005: Making every mother and child count. Geneva:
WHO, 2005
33. World Health Organization. Making pregnancy safer (MPR).
http://www.who.int/reproductive-health/mps/index.htm (accessed 24 October 2002)
34. McDonald S. Physiology and management of the third stage of labour. In: Fraser D, Cooper
M eds. Myles textbook for midwives. 14th edition. Edinburg. Churchill Livingstone, 2003:
507-30
35. Oxford Midwives Research Group. A study of the relationship between the delivery to cord
clamping interval and the time of cord separation. Midwifery. 1991;7:167-176
36. Ceriani Cernadas JM, Carroli G, Pellegrini L, Otano L, Ferreira M, Ricci, C et al. The effect
of timing of cord clamping on neonatal venous haematocrit values and clinical outcome at
term: A randomized, controlled trial. Paediatrics. 2006;117:e779-86
37. Cotter A, Ness A, Tolosa J. Prophylactic oxytocin for the third stage of labour. Cochrane
Database Syst Rev. 2001;(4):CD001808
38. Begley CM, Gyte GM, Murphy DJ, Devane D, McDonald SJ, McGuire W. Active versus
expectant management for women in the third stage of labour. Cochrane Database Syst Rev.
2010;7(7):CD007412
39. Hutton EK, Hassan ES. Late vs early clamping of the umbilical cord in full-term neonates:
Systematic review and meta-analysis of controlled trials. JAMA. 2007;297:1241-52
40. Richmond S, Wyllie J. European Resuscitation Council Guidelines for resuscitation 2010
section 7. Resuscitation of babies at birth. Resuscitation. 2010;81:1389-99
41. Mercer JS, Skovgaard RL. Neonatal transitional physiology: A new paradigm. J Perinat
Neonat Nurs. 2002;15(4):56-75
42. Hoffbrand AV, Moss PAH. Hypochromic anaemias. In: Hoffbrand AV, Moss PAH eds.
Essential Haematology. 6th edition. West Sussex. Wiley-Blackwell, 2011:33-49
43. Beard J. Recent evidence from human and animal studies regarding iron status and infant
development. J Nutr. 2007;137:524S-30S
44. Carlson ES, Tkac I, Magid R, O’Connor MB, Andrews NC, Schallert T et al. Iron is essential
for neuron development and memory function in mouse hippocampus. J Nutr. 2009;139:672-
9
45. McCann JC, Ames BN. An overview of evidence for a causal relation between iron
deficiency during development and deficits in cognitive or behavioural function. Am J Clin
Nutr. 2007;85:931-45

41
46. Gunnarsson BS, Thorsdottir I, Palsson G, Gretarsson SJ. Iron status at 1 and 6 years versus
developmental scores at 6 years in a well-nourished affluent population. Acta Paediatr.
2007;96:391-5
47. Thomas DG, Grant SL, Aubuchon-Endsley NL. The role of iron in neurocognitive
development. Dev Neuropsychol. 2009;34:196-222
48. Lozoff B, Beard J, Connor J, Barbara F, Georgieff M, Schallert T. Long-lasting neural and
behavioural effects of iron deficiency in infancy. Nutr Rev. 2006;64:S34-43
49. Szajewska H, Ruszczynski M, Chmielewska A. Effect of iron supplementation in
nonanaemic pregnant women, infants, and young children on the mental performance and
psychomotor development of children: A systematic review of randomized controlled trials.
Am J Clin Nutr. 2010;91:1684-90
50. Sachdev H, Gera T, Nestel P. Effect of iron supplementation on mental and motor
development in children: Systematic review of randomized controlled trials. Public Health
Nutr. 2005;8:117-132
51. Budin P. At what point should we practice the ligation of the umbilical cord? Progr Med
(Paris). 1875;3:765
52. Gupta R, Ramji S. Effect of delayed cord clamping on iron stores in infants born to anaemic
mothers: A randomized controlled trial. Indian paediatr. 2002;39:130-5
53. Van Rheenen P, de Moor L, Eschbach S, de Grooth H, Brabin B. Delayed cord clamping and
haemoglobin levels in infancy: a randomized controlled trial in term babies. Trop Med Int
Health. 2007;12:603-16
54. Chaparro CM, Neufeld LM, Tena AG, Eguia-Liz CR, Dewey KG. Effect of timing of
umbilical cord clamping on iron status in Mexican infants: A randomized controlled trial.
Lancet. 2006;367:1997-2004
55. Andersson O, Hellstrom-Westas L, Andersson D, Domellof M. Effect of delayed versus early
umbilical cord clamping on neonatal outcomes and iron status at 4 months: A randomized
controlled trial. BMJ. 2011;343:d7157
56. Emhamed MO, van Rheenen P, Brabin BJ. The early effects of delayed cord clamping in
term infants born to Libyan mothers. Trop Doct. 2004;34:218-22
57. Jaleel R, Deeba F, Khan A. Timing of umbilical cord clamping and neonatal haematological
status. J Pak Med Assoc. 2009;59:468-70
58. Rabe H, Reynolds GJ, Diaz-Rossello JL. A systematic review and meta-analysis of a brief
delay in clamping the umbilical cord of preterm infants. Neonatology. 2008;93:138-44

42
59. Kirkwood BR, Sterne JAC. Calculation of required sample size. In: Kirkwood BR, Sterne
JAC eds. Essential Medical Statistics. 2nd edition. Malden Massachusetts. Blackwell Science
Ltd, 2003: 413-28
60. Ballard JL, Khoury JC, Wedig K, et al: New Ballard Score, expanded to include extremely
premature infants. J Paediatrics. 1991; 119:417-23
61. Jahazi A, Kordi M, Mirbehbahani NB, Mazloom SR. The effect of early and late umbilical
cord clamping on neonatal haematocrit. J Perinatology. 2008; 28: 523-25.
62. Linderkamp O, Nelle M, KrausM, Zilow EP. The effect of early and late cord clamping on
blood viscosity and other hemorheological parameters in full-term neonates. Acta paediatrica
1992; 81: 745-50
63. Male C, Persson LA, Freeman V, Guerra A, van’t Hof MA, Haschke F. Prevalence of iron
deficiency in 12-months old infants from 11 European areas and influence of dietary factors
on iron status (Euro-Growth study). Acta Paediatr 2001; 90: 492-8

43
APPENDIX I
OUTCOME OF DELAYED CORD CLAMPING IN TERM NEONATES
AT THE FEDERAL MEDICAL CENTRE, ABEOKUTA.
CONSENT FORM (ENGLISH)
Dear Ma,
My name is Dr Awolaja Babatunde Stephen. I am a senior registrar in the Department
of Obstetrics and Gynaecology. The main purpose of this study is to find out if tying the
umbilical cord of babies born at term after waiting for 2 minutes has any effect on their blood
level and other blood characteristics at the Federal Medical Centre, Abeokuta.
There is no fixed rule regarding the most favourable timing for tying the cord.
Various studies have shown that waiting for sometime before tying the cord can be of benefit
to the infant by improving iron status especially in a developing country like ours where
shortage of blood due to iron deficiency is prevalent.
If you wish to take part in this study, you will be asked some questions and some
other information concerning you will be obtained and recorded in my data sheets.
After meeting the criteria to participate in the study, you will be placed in either of
two groups; the delayed cord clamping (intervention) group or the early cord clamping
(control) group. If you fall into the intervention group, after delivery of your baby, a delay of
2 minutes would be observed before tying the umbilical cord. While if you fall into the
control group, the umbilical cord would be tied within 10 seconds of delivery as it is
routinely practised in the hospital.
All of your information will be kept confidential to the extent required by the law and
your personal identity will not be revealed in any publication or release of results.
Your decision to join in this study is voluntary and you may wish to quit at any time, and if
you quit, you will not be denied any benefit or care.
For more information, you may call the researcher Dr. Awolaja Babatunde Stephen on this
line 0803 291 1203.

44
Investigator's Statement
I have provided an explanation of the above research program. The participant was given an
opportunity to discuss the study. A copy of the consent form has been given to the participant
for attestation.
_______________________________ __________
Signature of Investigator or Interviewer Date
Participant’s Statement
I,.............................................................................. certify that I have read, had read or it had
been translated to me the components of the study and I understand the description of this
study. I have asked and received answers to all my questions about the study. I voluntarily
consent to join the study. I understand that I may quit the study at any time. I understand that
I may ask further questions at any time. I have had an opportunity to carefully review the
consent form and asked questions about it.
___________________________________ __________
Signature/ Left Thumb Print of Participant Date
___________________________________ __________
Signature of Translator Date
(Where the patient does not speak English, to be done by someone that speaks the same
language as the patient)
___________________________________ __________
Signature of Witness Date

45
APPENDIX I
ABAJADE ESI LORI ITESEDURO IDAWOO OMO TITUN NI ILE IWOSAN
FEDERAL MEDICAL CENTRE, ABEOKUTA.
CONSENT FORM (YORUBA)
Mama mi tooto,
Oruko mi ni Onisegun Oyinbo Awolaja Babatunde Stephen. Moje olugbaniwole agba ni eka
eto iloyun ati ibimo. Koko ise iwadii yi ni lati mo boya siso iwo omo fun bi iseju meji, ni ipa
Kankan ko lori ipo eje omo ati irisi miiran lori eje ni ile iwosan Federal Medical Center,
Abeokuta.
Kosi ilana kan pato nipa ona ti o dara ju lori wiwo agogo fun didawoo. Opolopo lwadii ti fi
han pe diduro fun igba die ki a to so iwo le je anfaani fun omo owo lati le se daradara lori
ilera won paapaa julo ni awon ilu ti idagbasoke ti ba bii tiwa ti o ni isoro aito eje.
Ti e ba nifee lati kopa ninu ise iwadii yii, a o beere awon ibeere ati awon ohun to ye lati mo
nipa re ni a o gba a,ti a o si ko o sile sinu iwe iwadi mi.
Leyin ti o ba ti yege atikopa ninu ise iwadii naa, a o fi o si okan ninu awon owo meji,
iteseduro idawo (idasi), owo kin-in-ni tabi owo keji itete dawoo(akoso). Ti a ba bo si owo
idasi, lehin ibimo re iteseduro iseju meji yoo waye ki a to ta iwo ni koko. Ti o ba si je owo
akoso ni o bo si, a o ta koko iwo naa laarin iseju winiwini mewaa ti o ba bimo tan gege bi
won ti n se nile iwosan.
Gbogbo asiri iwadi re ni yoo wa ni pipamo gege bi ofin se laa kale ati pe aami idanimo re ko
ni han sita ninu abajade tabi se afihan re ninu abajade esi.
Ipinu re lati kopa ninu ise iwadii yii kokon dandan, ati pe o le kuro ni igba-kugba.
Fun mimo si nipa ise yii, o le pe aago Oluwadii Onisegun Oyinbo Awolaja Babatunde
Stephen sori ero ibanisoro yi 08032911203

46
Oro Oluwadi
Mo ti se alaye lori eto iwadii oke yii. Awon akopa si ni anfaani lati soro lori ise naa.
Iwe ifohunsokan si ti lo si odo akopa gege bi eri
_______________________________ _______________________
Ibowoluwe oluwadi/Aforowanilenuwo Ojo
Oro Olukopa
Emi,---------------------------------------------------- jejee pe mo ti kaa/won si ti se ogbufo
ohun ti ise naa dale fun mi, mo si gbo agboye re. Mo ti beere gbogbo ibeere, mo si ti gbo
idahun re lori ise iwadi naa. Ifinufedo mi ni mo fi darapo mo ise iwadii naa. Mo si mo pe mo
le yeba (Kuro) nigbakugba ti o ba wun mi. Mo si mo pe mo le beere ibeere siwaju sii ni
igbakungba. Mo mo pe mo ni igbalaaye lati se atunse lori iwe ifohunsokan ati lati beere
ibeere lori re.
____________________________ ________________________
Ibowoluwe/Iteka Owo Osi Akopa Ojo
____________________________ _________________________
Ibowoluwe Ogbufo Ojo
(Ti alaisan ko ba le so ede Geesi ki eni ti o gbo ede alaisan se e)
_____________________________ _______________________
Ibowoluwe Olujerii Ojo

47
APPENDIX I
OUTCOME OF DELAYED CORD CLAMPING IN TERM NEONATES AT THE
FEDERAL MEDICAL CENTRE, ABEOKUTA.
CONSENT FORM (IGBO)
Ezigbo Nne,
Aham bu Dokita Awolaja Babatunde Stephen. Abum, Registra ukwu na Departmenti
nke Obstetrics na Gynaecology (ebe nafu maka umunwanyi, ma obu ihe gbasara
umunwanyi). Isi okwu nke ihe omumu a bu ichoputa maka nkechi eriri otubo umuaka amuru
ohuru (nozuru onwa itolu na afo ), ma onware mmetuta na odidi obara ha n’ime Federal
Medical Centre, Abeokuta.
Eweghi iwu jigidere oge kacha mma iji kechie eriri otubo. Otutu ihe omumu egosi la
na ichere nwamgbe oge tupu ekechie eriri otubo ga enyere nwata ahu aka n’ibuli onodu iron
ya kachakwa n’ime obodo n’emepeghi emepe di ka nke anyi ebe obara diala n’ihi okiko iron
zuru onu.
Oburu na ichoro isoro na ihe omumua, aga aju gi ufodi ajuju tinyere na aga eweputa
ufodu ihe gbasara gi idetu ya na ime data sheet mu.
Oburu na igafee iwu kwagidere isonye na ihe omumua, a ga etinye gi n’ otu ime
grupu abua. “Ogbugbu oge na njide eriri otubo” (mgbochi) grupu, ma obu “Nkechi n’oge nke
eriri otubo” (Nlereanya) grupu. Oburu na idabara n’ime mgbochi grupu, mgbe imuputara
nwa, ogbugbu oge nkeji abua ka aga egbu tupu, ekechie eriri otubo ya. Ma oburu na idaba na
“Nlereanya” grupu, aga ekechi eriri otubo nwagi osiso amuputara ya tupu sekondu iri agaefee
bu ka esi eme bu ya na ulo ogwu anyi a.
Ihe nile gbasara gi ga ano na nzuzo otu iwu si we kwuo, aha eji mara gi ga bu kwa ihe
ezoro ezo n’ime ihe odide mgbasa ozi.
Nkwenye gi na ihe omumua ga esi n’obi gi puta, tinyere na iga apu mgbe obula ichoro
ipu. Ma odaputa na ipuru, ogaghi egbochi anyi inyegi uru nile na nlekota nile kwesiri gi.
Oburu na icho nkowa ihe ndi ozo, kpoo onye isi omumu a Dokita Awolaja Babatunde
Stephen na akara igwe 08032911203.
Imee la.
48
Investigator’s Statement
I have provided an explanation of the above research program. The participant was
given an opportunity to discuss the study. A copy of the consent form has been given to the
participant for attestation.
_______________________ ___________________
Signature of Investigation Date
Participant’s Statement
Mu……………………………………………………….. kwenyere na mu aguola ma
gughari-kwaa ihe no na ihe omumua, ma ghota kwa otu ihe omumumu a di. Ajuolam ajuju
ma natakwa oziza n’ile banyere ihe omumua. Eweputalam onwem site na ime obim isoro na
ihe omumua. Aghotaram na mu ga akwusi ihe omumua oge obula omasirimu. Aghotaram na
mu nwere ike iju ajuju ndi ozo oge obula. Enwere mu oghere mkpachapu anya itule formu
nkwekolita ma juokwa ajuju banyere ya.
_____________________ ___________________
Signature/Left Thumb Date
Print of participant
_____________________ ____________________
Signature of Translator Date
(Where the patient does not speak English, to be done by someone that speaks the same
language as the patient)
____________________ __________________
Signature of Witness Date

49
APPENDIX II
RECRUITMENT DATA SHEET
OUTCOME OF DELAYED CORD CLAMPING IN TERM NEONATES AT THE
FEDERAL MEDICAL CENTRE, ABEOKUTA.
DATA SHEET I
SERIAL NUMBER................... HOSPITAL NUMBER...............
RANDOMIZATION NUMBER........... PHONE NUMBER................
NAME..................................................................................
AGE...........................................................................................
ADDRESS....................................................................................
LEVEL OF EDUCATION: [1] None [2] Primary [3] Secondary [4] NCE [5] ND [6] HND
[7] BSc [8] Postgraduate
OCCUPATION....................................................................
HUSBAND’S OCCUPATION............................................
RELIGION: 1. Christianity 2. Islam 3. Others, specify..................
PARITY.............................. NO OF LIVING CHILDREN.......................
LMP...................... EDD.............................
ESTIMATED GESTATIONAL AGE...............................(WKS)
BOOKING STATUS..............................................................
IF BOOKED, NO OF ANC VISITS..........................
DATE OF LAST ANC VISIT.......................
IS THE PATIENT ON IRON SUPPLEMENT: 1. YES 2. NO
DID SHE RECEIVE ANY ANTIMALARIAL DRUG? 1. YES 2. NO
BLOOD GROUP............................ GENOTYPE......................
DATE OF RECRUITMENT................................
TIME OF RECRUITMENT..................................
WEIGHT AT BOOKING....................................(Kg)
HEIGHT AT BOOKING....................................(m)

50
APPENDIX III
RECRUITMENT DATA SHEET
OUTCOME OF DELAYED CORD CLAMPING IN TERM NEONATES AT THE
FEDERAL MEDICAL CENTRE, ABEOKUTA.
DATA SHEET II
SERIAL NUMBER................... HOSPITAL NUMBER...............
RANDOMIZATION NUMBER........... PHONE NUMBER................
INFORMATION ON LABOUR
DATE AND TIME OF ONSET OF LABOUR.....................................
TYPE OF LABOUR: 1. SPONTANEOUS, 2.AUGMENTED, 3. INDUCED
DATE AND TIME OF DELIVERY.......................................
WAS EPISIOTOMY GIVEN? 1. YES 2. NO
ANY COMPLICATION OF THIRD STAGE ? 1. YES 2.NO
IF YES, WHICH ONE? 1. ATONY,
2. RETAINED PLACENTA
3.CERVICAL/PERINEAL LACERATION,
4. OTHERS SPECIFY............
EBL............................... (mL)
WAS OXYTOCICS GIVEN? 1. YES 2. NO
IF YES, 1. OXYTOCIN 2.MISOPROSTOL 3. ERGOMETRINE 4.OTHERS,
SPECIFY.............
WAS THERE POST RANDOMIZATION EXCLUSION? 1. YES 2.NO
IF YES, WHY? 1.Birth asphyxia 2. Instrumental delivery 3. Needed immediate
resuscitation 4. EMCS 5.Others, specify........................
PREPARTUM HAEMATOCRIT....................%
POSTPARTUM HAEMATOCRIT..................%

51
APPENDIX IV
RECRUITMENT DATA SHEET
OUTCOME OF DELAYED CORD CLAMPING IN TERM NEONATES AT THE
FEDERAL MEDICAL CENTRE, ABEOKUTA.
DATA SHEET III
SERIAL NUMBER................... HOSPITAL NUMBER...............
RANDOMIZATION NUMBER........... PHONE NUMBER................
INFORMATION ABOUT THE BABY
ESTIMATED GESTATIONAL AGE......................... (WKS)
DATE OF BIRTH.................................. TIME OF BIRTH...........................
SEX: 1.= MALE 2 = FEMALE
WEIGHT........................ (kgs) LENGTH............... (cm)
DID THE BABY CRY IMMEDIATELY AFTER BIRTH? 1.YES 2.NO
DID THE BABY REQUIRE RESUSCITATION? 1. YES 2.NO
APGAR SCORES AT 1 MINUTE.................., AT 5 MINUTES..............
DID THE BABY HAVE ANY CONGENITAL MALFORMATION? 1. YES 2.NO
WAS THE BABY BREASTFED AFTER DELIVERY? 1.YES 2. NO
HAEMATOCRIT AT 24 HOURS..................%
SERUM BILIRUBIN LEVEL AT 24 HOURS.......................mg/dL
RESPIRATORY RATE AT 24 HOURS.................../minute
DID THE BABY DEVELOP JAUNDICE BEFORE DISCHARGE 1. YES 2.NO
IF YES, WAS SERUM BILIRUBIN LEVEL DONE? 1. YES 2.NO
IF YES, SERUM BILIRUBIN LEVEL.........................mg/dL
DID THE BABY REQUIRE NICU ADMISSION FOR JAUNDICE/OTHER REASONS?
1. YES 2. NO
DID THE BABY REQUIRE PHOTOTHERAPY? 1. YES 2. NO
IF YES, HOW MANY TIMES...................
DID THE BABY REQUIRE EXCHANGE TRANSFUSION? 1. YES 2.NO
DATE OF DISCHARGE.......................................

52
APPENDIX V
RECRUITMENT DATA SHEET
OUTCOME OF DELAYED CORD CLAMPING IN TERM NEONATES AT THE
FEDERAL MEDICAL CENTRE, ABEOKUTA.
DATA SHEET IV
SERIAL NUMBER................... HOSPITAL NUMBER...............
RANDOMIZATION NUMBER........... PHONE NUMBER................
INFORMATION ABOUT THE BABY AT 6 WEEKS
WEIGHT..................(kg)
LENGTH..................(cm)
HAS THE BABY BEEN EXCLUSIVELY BREAST FED? 1.YES 2. NO
DID THE BABY RECEIVE IRON SUPPLEMENT? 1.YES 2. NO
ANY ILLNESS IN THE LAST 6 WEEKS? 1.YES 2. NO
IF YES, SPECIFY.........................
HAEMATOCRIT....................%
WAS THERE POST- RANDOMIZATION EXCLUSION? 1.YES 2. NO
IF YES, WHY?................

53
APPENDIX VI
WORK PLAN
Activity MAR
2014
APRIL
2014
MAY
2014
DEC
2014
JAN
2015
APRIL
2015
MAY
2015
JUNE
2015
JULY
2015
AUG
2015
Proposal writing XX XX
Ethical clearance XX
Submission of
proposal to college
XX XX
Pilot study XX
Data collection XX XX XX XX XX
Data
analysis
NOV
2015
Review of draft by
supervisor
DEC
2015
Final write up DEC
2015
Submission of
work to college
JAN
2016
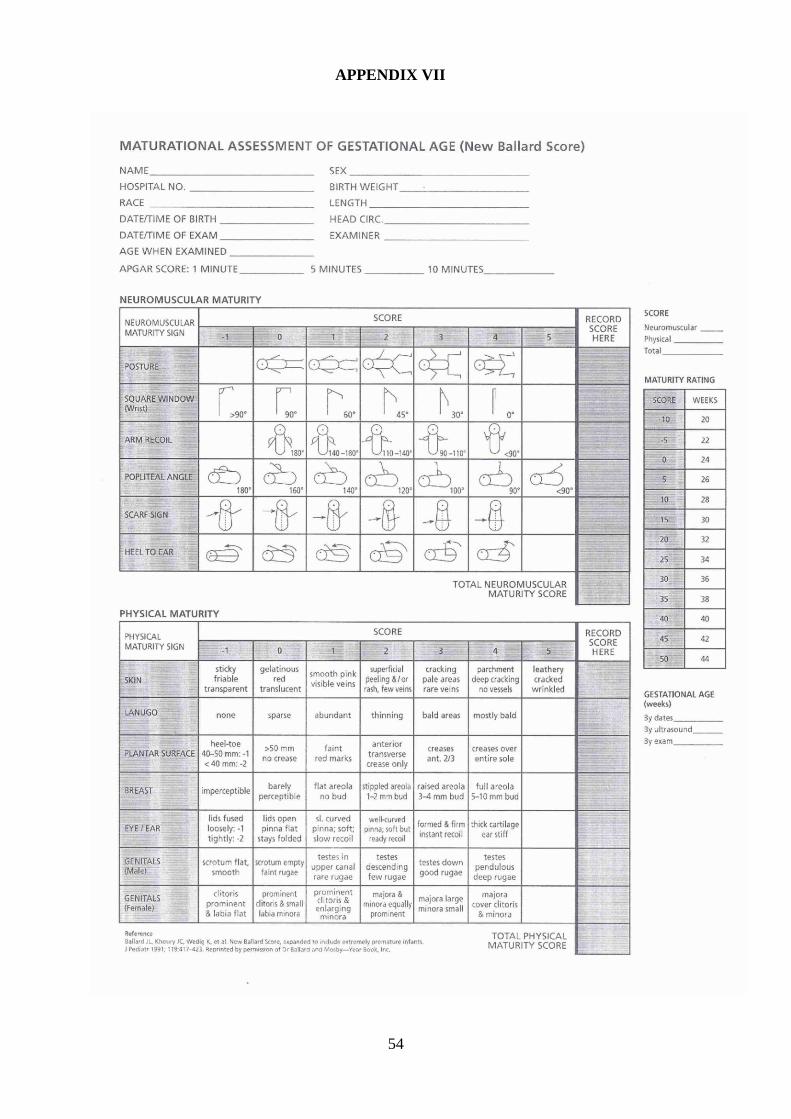
54
APPENDIX VII

55
APPENDIX VIII

56
APPENDIX IX















![SyMRI detects delayed myelination in preterm neonates · pathologiesofpretermneonates[12–14].However,convention-al MRI is a highly time-consuming procedure and currently lacks diagnostic](https://static.fdocuments.in/doc/165x107/60e6d1440f207a78304f5a8d/symri-detects-delayed-myelination-in-preterm-neonates-pathologiesofpretermneonates12a14howeverconvention-al.jpg)


