
Delayed Cord Clamping - Prisma Health
12
2016 Midlands Perinatal Conference 1 KERRY M. SIMS, MD FACOG UNIVERSITY OF SOUTH CAROLINA Delayed Cord Clamping Objectives 1. Review history of cord clamping 2. Review current expert guidelines 3. Discuss benefits of delayed cord clamping in term and preterm neonates 4. Discuss risks of delayed cord clamping The Umbilical Cord Two Arteries One Vein Average length: 55 cm Blood flows from the placenta through the umbilical vein to the fetus Blood exits the fetus in the two umbilical arteries
Transcript of Delayed Cord Clamping - Prisma Health
2016 Midlands Perinatal Conference
1
K E R R Y M . S I M S , M D F A C O G
U N I V E R S I T Y O F S O U T H C A R O L I N A
Delayed Cord Clamping
Objectives
1. Review history of cord clamping
2. Review current expert guidelines
3. Discuss benefits of delayed cord clamping in term and preterm neonates
4. Discuss risks of delayed cord clamping
The Umbilical Cord
Two Arteries
One Vein
Average length: 55 cm
Blood flows from the placenta through the umbilical vein to the fetus
Blood exits the fetus in the two umbilical arteries
2016 Midlands Perinatal Conference
2
Aristotle 384-322 BC
“Frequently the child appears to be born dead, when it is feeble and when, before the tying of the cord, a flux of blood occurs into the cord and adjacent parts. Some nurses who have already acquired skill squeeze (the blood) back out of the cord (into the child's body) and at once the baby, who had previously been as if drained of blood, comes to life again.”
Timeline of Cord clamping & cutting
Described in 1688
Routine practice by the 19th century In 1801, Erasmus Darwin wrote, „Another thing very injurious
to the child, is the tying and cutting of the navel string too soon; which should always be left till the child has not only repeatedly breathed but till all pulsation in the cord ceases. As otherwise the child is much weaker than it ought to be.‟12
Budin in 1875 measured the amount of blood left in the placentas of the after early vs. late ligation & found 92 more cubic centimeters available to the infant
2016 Midlands Perinatal Conference
3
Immediate Cord Clamping
Common practice to clamp early, typically within 30s of birth.
Modern Day Cord clamping
Early Clamping within 1 minute of delivery
Late Clamping more than 5 minutes after delivery
Studies showing that 90% of blood volume was achieved within the first few breaths the infant took after birth
Most practionners clamped the cord within 15-20s of delivery
What is delayed cord clamping?
Delayed umbilical cord clamping is prolongation of the time between delivery of a neonate and clamping of the umbilical cord.
Immediate umbilical cord clamping is typically performed within 15 seconds of delivery, whereas delayed umbilical cord clamping is performed 25 seconds to 5 minutes after delivery.

2016 Midlands Perinatal Conference
4
Gorilla Birth
Gorilla Birth -- Urban Gorilla
2016 Midlands Perinatal Conference
5
Guidelines
ACOG Committee Opinion 2012
No good evidence to support or refute benefits of delayed cord clamping in term infants
Evidence does support delayed cord clamping in preterm infants
WHO
2012
Delayed umbilical cord clamping (not earlier than 1 min after birth) is recommended for improved maternal and infant health and nutrition outcomes
How much blood is given to the baby by delaying cord clamping?
Delayed cord clamping may increase the neonate‟s blood volume by as much as 8% to 24%. 80ml of blood at 1 minute
100ml of blood at 3 minutes
Transfusion of blood from placenta to baby through the cord
Simkin video
Blood demonstration
2016 Midlands Perinatal Conference
6
What are the benefits?
Increase blood volume
Decreased need for transfusion
Decreased intracranial hemorrhage in preterm infants
May prevent iron deficiency in the 1st year of life
Longer duration of placental transfusion after birth may be beneficial because this blood is enriched with immunoglobulins and stem cells, which provide the potential for improved organ repair and rebuilding after injury from disorders caused by preterm birth
What is the risk?
Timely resuscitation
Excessive placental transfusion Jaundice?
Excessive maternal hemorrhage
Technical difficulties
Warming of infant during cesarean section
Parents who desire cord blood banking
What does the data show?
Preterm infants and Term infants have different benefits and risks
2016 Midlands Perinatal Conference
7
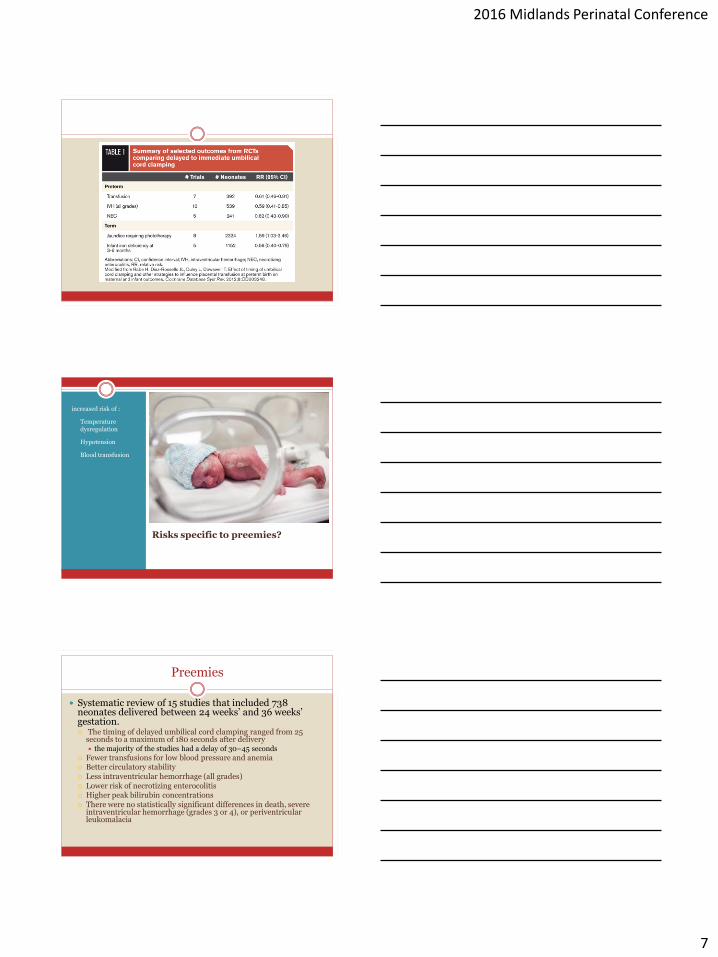
Risks specific to preemies?
increased risk of :
• Temperature dysregulation
• Hypotension
• Blood transfusion
Preemies
Systematic review of 15 studies that included 738 neonates delivered between 24 weeks‟ and 36 weeks‟ gestation. The timing of delayed umbilical cord clamping ranged from 25
seconds to a maximum of 180 seconds after delivery the majority of the studies had a delay of 30–45 seconds
Fewer transfusions for low blood pressure and anemia Better circulatory stability Less intraventricular hemorrhage (all grades) Lower risk of necrotizing enterocolitis Higher peak bilirubin concentrations There were no statistically significant differences in death, severe
intraventricular hemorrhage (grades 3 or 4), or periventricular leukomalacia
2016 Midlands Perinatal Conference
8
Long term???
One small study showed no difference in infant development at 7 months
Current trial going on in Australia for infants delivered at <30 weeks gestation -- Australian Placental Transfusion Study [APTS]
Term infants
Cochrane Review -- 15 randomized trials of delayed cord clamping in term neonates, including 3911 women
Higher neonatal hemoglobin concentration at 24 to 48 hours of life
Lower likelihood of iron deficiency at 3–6 months
Increased risk of jaundice requiring phototherapy
Jaundice
The risk of jaundice must be weighed against the risk of iron deficiency.
“In developed nations where phototherapy is widely available, delayed umbilical cord clamping to increase iron stores has low potential for morbidity.” -- SMFM
2016 Midlands Perinatal Conference
9
Delivery position of baby?
No difference in volume of placental transfusion
placed on mom‟s chest
or held at the level of the vagina
How about risks to the mother?
Theoretical risks include delaying delivery of the placenta delays uterine contraction and increases blood loss
In cesarean deliveries, maternal blood loss also occurs through the hysterotomy incision, and delaying closure may lead to increased risk of hemorrhage
Maternal risks
Very few studies
Cochrane Review 2008 2989 mothers
No difference in rates of postpartum hemorrhage
no differences were seen in mean blood loss, need for transfusion, postpartum hemoglobin concentration, or need for manual removal of the placenta
2016 Midlands Perinatal Conference
10
“Milking” the cord
Squeezing the blood down the cord to the baby Typically, the delivering provider will “strip” a segment of the
umbilical cord toward the fetal umbilicus 3–4 times before clamping the umbilical cord
Rapid bolus of blood to the infant
“Milking”
One small trial involving infants born between 24 and 28 weeks looked at milking vs. immediate clamping
Higher initial Hb concentration
Higher mean systemic blood pressure
Reduced need for blood transfusion
Higher urine output during the first 72 hours
Shorter duration of mechanical ventilation and supplemental oxygen
Contraindications
Infants Congenital anomalies
Reversed or absent end diastolic flow
Severe depression
Maternal Placental abnormalities with increased risk of hemorrhage
Accreta, previa, abruption
Severe anemia
2016 Midlands Perinatal Conference
11
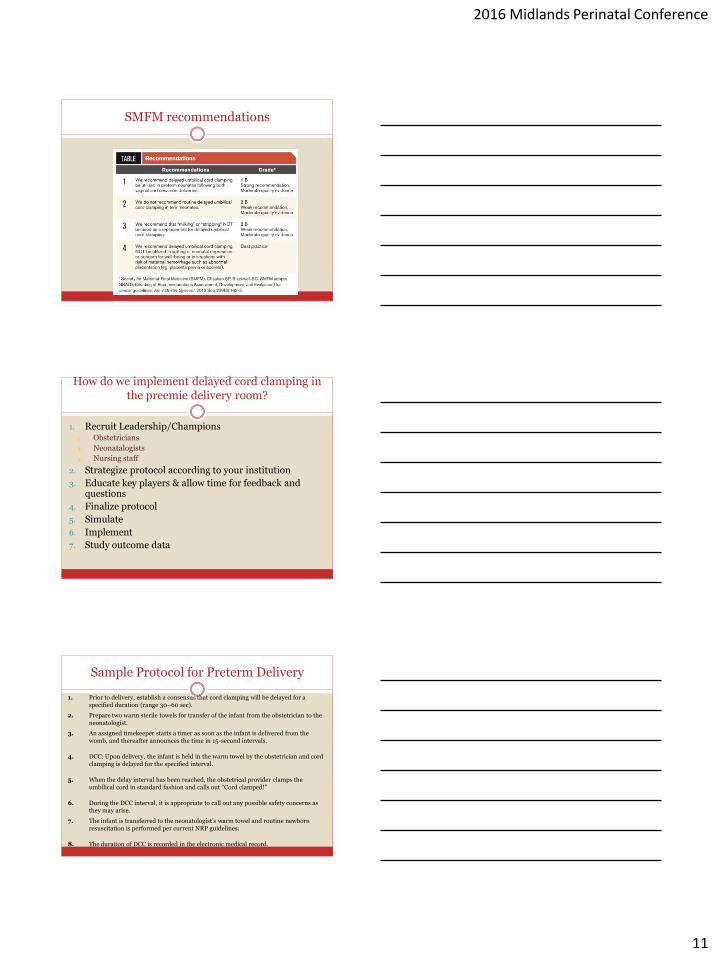
SMFM recommendations
How do we implement delayed cord clamping in the preemie delivery room?
1. Recruit Leadership/Champions 1. Obstetricians
2. Neonatalogists
3. Nursing staff
2. Strategize protocol according to your institution
3. Educate key players & allow time for feedback and questions
4. Finalize protocol
5. Simulate
6. Implement
7. Study outcome data
Sample Protocol for Preterm Delivery
1. Prior to delivery, establish a consensus that cord clamping will be delayed for a specified duration (range 30–60 sec).
2. Prepare two warm sterile towels for transfer of the infant from the obstetrician to the neonatologist.
3. An assigned timekeeper starts a timer as soon as the infant is delivered from the womb, and thereafter announces the time in 15-second intervals.
4. DCC: Upon delivery, the infant is held in the warm towel by the obstetrician and cord clamping is delayed for the specified interval.
5. When the delay interval has been reached, the obstetrical provider clamps the umbilical cord in standard fashion and calls out “Cord clamped!”
6. During the DCC interval, it is appropriate to call out any possible safety concerns as they may arise.
7. The infant is transferred to the neonatologist‟s warm towel and routine newborn resuscitation is performed per current NRP guidelines.
8. The duration of DCC is recorded in the electronic medical record.
2016 Midlands Perinatal Conference
12
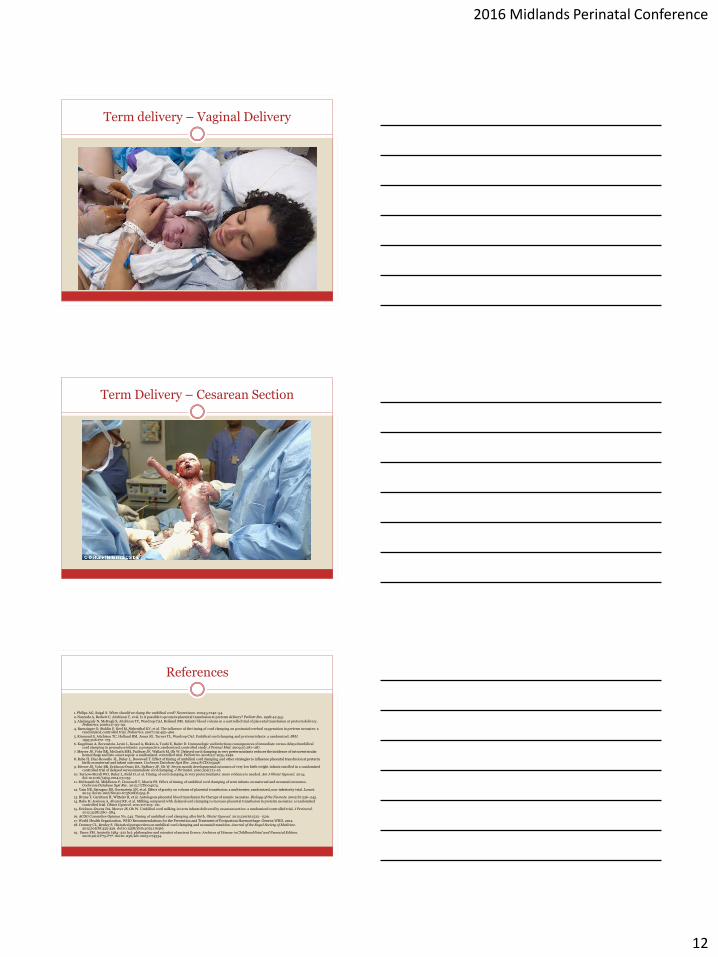
Term delivery – Vaginal Delivery
Term Delivery – Cesarean Section
References
1. Philips AG, Saigal S. When should we clamp the umbilical cord? Neoreviews. 2004;5:e142–54. 2. Narenda A, Beckett C, Aitchison T, et al. Is it possible to promote placental transfusion at preterm delivery? Pediatr Res. 1998;44:453.
3. Aladangady N, McHugh S, Aitchison TC, Wardrop CAJ, Holland BM. Infants‟ blood volume in a controlled trial of placental transfusion at preterm delivery. Pediatrics. 2006;117:93–99.
4. Baenzinger O, Stoklin F, Keel M, Siebenthal KV, et al. The influence of the timing of cord clamping on postnatal cerebral oxygenation in preterm neonates: a randomized, controlled trial. Pediatrics. 2007;119:455–460.
5. Kinmond S, Aitchison TC, Holland BM, Jones JG, Turner TL, Wardrop CAJ. Umbilical cord clamping and preterm infants: a randomized. BMJ. 1993;306:172–175.
6. Kugelman A, Borenstein-Levin L, Kessel A, Riskin A, Toubi E, Bader D. Immunologic and infectious consequences of immediate versus delayed umbilical cord clamping in premature infants: a prospective, randomized, controlled study. J Perinat Med. 2009;37:281–287.
7. Mercer JS, Vohr BR, McGrath MM, Padbury JF, Wallach M, Oh W. Delayed cord clamping in very preterm infants reduces the incidence of intraventricular hemorrhage and late-onset sepsis: a randomized, controlled trial. Pediatrics. 2006;117:1235–1242.
8. Rabe H, Diaz-Rossello JL, Duley L, Dowswell T. Effect of timing of umbilical cord clamping and other strategies to influence placental transfusion at preterm birth on maternal and infant outcomes. Cochrane Database Syst Rev. 2012;8:CD003248.
9. Mercer JS, Vohr BR, Erickson-Owns DA, Padbury JF, Oh W. Seven month developmental outcomes of very low birth weight infants enrolled in a randomized controlled trial of delayed versus immediate cord clamping. J Perinatol. 2010;30(1):11–16.
10. Tarnow-Mordi WO, Duley L, Field D, et al. Timing of cord clamping in very preterm infants: more evidence is needed. Am J Obstet Gynecol. 2014; doi:10.1016/j.ajog.2014.03.055.
11. McDonald SJ, Middleton P, Dowswell T, Morris PS. Effect of timing of umbilical cord clamping of term infants on maternal and neonatal outcomes. Cochrane Database Syst Rev. 2013;7:CD004074.
12. Vain NE, Satragno DS, Gorenstein AN, et al. Effect of gravity on volume of placental transfusion: a multicenter, randomized, non-inferiority trial. Lancet. 2014; doi:10.1016/S0140-6736(08)61345-8.
13. Brune T, Garritsen H, Witteler R, et al. Autologous placental blood transfusion for therapy of anemic neonates. Biology of the Neonate. 2002;81:236–243. 14. Rabe H, Jewison A, Alvarez RF, et al. Milking compared with delayed cord clamping to increase placental transfusion in preterm neonates: a randomized
controlled trial. Obstet Gynecol. 2011;117:205–211. 15. Erickson-Owens DA, Mercer JS, Oh W. Umbilical cord milking in term infants delivered by cesarean section: a randomized controlled trial. J Perinatol.
2012;32(8):580–584. 16. ACOG Committee Opinion No. 543. Timing of umbilical cord clamping after birth. Obstet Gynecol. 2012;120(6):1522–1526.
17. World Health Organization. WHO Recommendations for the Prevention and Treatment of Postpartum Haemorrhage. Geneva:WHO, 2012. 18. Downey CL, Bewley S. Historical perspectives on umbilical cord clamping and neonatal transition. Journal of the Royal Society of Medicine.
2012;105(8):325-329. doi:10.1258/jrsm.2012.110316.
19. Dunn PM. Aristotle (384–322 bc): philosopher and scientist of ancient Greece. Archives of Disease in Childhood Fetal and Neonatal Edition. 2006;91(1):F75-F77. doi:10.1136/adc.2005.074534.


















