Our Aging Population: Mental Health in the Advancing Years Sara J. Czaja Department of Psychiatry...
29
Our Aging Population: Mental Health in the Advancing Years Sara J. Czaja Department of Psychiatry and Behavioral Sciences Center on Aging University of Miami Miller School of Medicine This research discussed is supported in part by grants from the NIH/NIA, NINR, Langeloth Foundation, AOA, J&J, and AT&T
-
Upload
ashley-dorsey -
Category
Documents
-
view
214 -
download
0
Transcript of Our Aging Population: Mental Health in the Advancing Years Sara J. Czaja Department of Psychiatry...

Our Aging Population: Mental Health in the
Advancing Years
Sara J. CzajaDepartment of Psychiatry and Behavioral
SciencesCenter on Aging
University of Miami Miller School of Medicine
This research discussed is supported in part by grants from the NIH/NIA, NINR, Langeloth Foundation, AOA, J&J, and AT&T

Overview of Presentation
• Provide a brief overview of the current demographic trends.
• Summarize findings regarding mental health of older adults.
• Summarize findings regarding family caregiving and mental health.
• Present examples of on-going caregiver intervention research at UM.
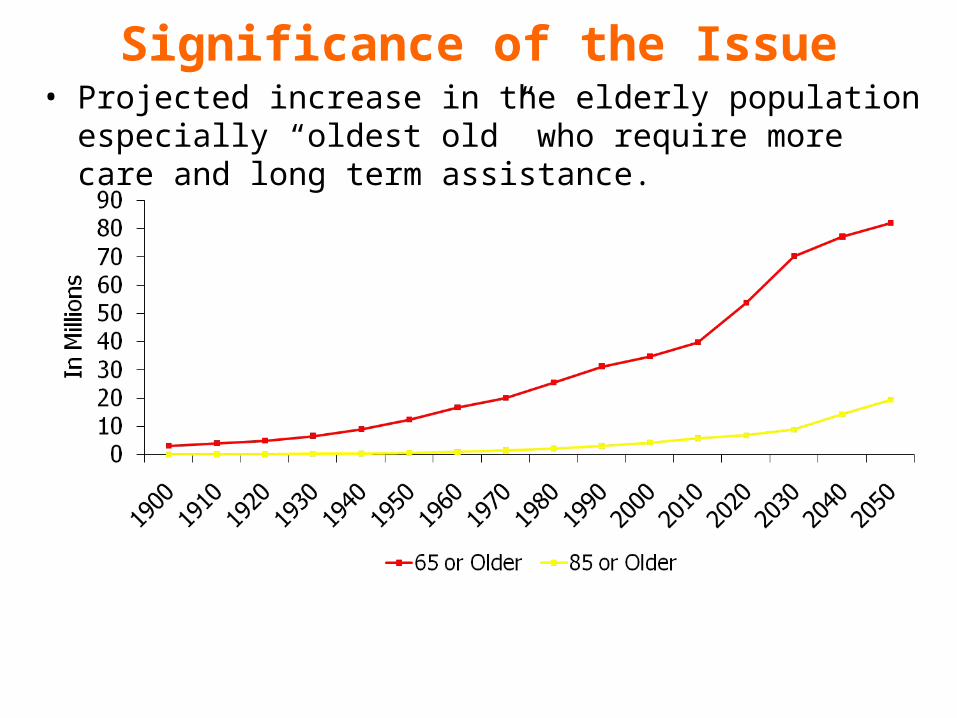
Significance of the Issue• Projected increase in the elderly population especially “oldest ol
d” who require more care and long term assistance.


Older Adults and Depression • Diagnosed rates of depression:
– Community Dwelling Older Adults• Major depression ~ 2%• Minor depression ~ 10%• Depressive symptoms ~ 14%
– Primary Care Settings ~7 - 36%– Hospitalized patient ~ 25%– Long term care residents ~ 20 – 47%
• Primary health care providers often fail to diagnosis depression in older patients.
• Ethnic and racial minorities are less likely than Caucasian elderly to seek specialty mental health care.
Older Adults and Depression • Prevalence of depression (major and minor) in
persons with dementia: 30-50%.• Depression is associated with cognitive
impairment.• History of depression has been shown to be
linked to increased risk to develop Alzheimer’s disease (AD) and vascular dementia later in life.

Reasons for Non-Recognition of Geriatric Depression
• Symptoms attributed to chronic medical conditions due to somatic presentations.
• Often do not complain of depressed mood or other symptoms such as crying spells, or irritability.
• Social isolation and withdrawal. • Symptoms not prominent every day.• Depression seen as “normal” part of aging. • Psychosocial and physical losses divert attention from
consideration of depression diagnosis. • Stigma.

Consequences of Untreated Depression• Worldwide, depression is a leading cause of
disability adjusted life years (DALY).• Increased health services utilization.• Greater morbidity and mortality due to co-
occurring cardiovascular disease. • Increased risk for suicide.• Withdrawal/social isolation.• Fatigue/lack of energy.

Depression and family Caregivers
Significance of the Issue Changes in healthcare dynamics – moving towards a
partnership model of care. Trend from in-patient to out-patient care and increased
reliance on family members to provide needed care and support.
Family caregivers represent the largest source of long-term care for older adults. 29% of the U.S. adult population is providing care for
someone who is disabled, seriously ill or aged and 59% expects to be a caregiver in the future.
66% of caregivers are providing caregiver for an adult aged 50+ and 15 million adults are providing care for someone with Alzheimer’s disease or other dementia.
Health and needs of family caregivers are often overlooked.

Alzheimer’s Association, 2015

Definition of Family Caregiving
Schulz & Quittner (1998). Health Psychology
“Extraordinary care involving significant expenditure of time and energy often for months or years, requiring the performance of tasks that may be physically demanding and unpleasant.”
extraordinary care -- tasks that exceed the bounds of what is normative or usual for a parental, sibling, or spousal relationship.
assistance is provided for no compensation, either voluntarily or because there are no other alternatives.
caregivers typically do not receive formal training for the caregiving role.
Caregiving Tasks• Care Coordination
– Primary Care MD– Specialist MD– Physical Therapist/Occupational
Therapist– Insurance company
• Personal Care Tasks– Bathing – Dressing/Grooming– Eating – Toileting/Transferring
• Household Tasks– Shopping– Managing finances– Transportation
• Medical or Nursing Tasks– Managing medications, including
IVs– Operating medical equipment– Using monitors or assistive devices– Wound care
• Emotional, Cognitive and Behavioral Support– Helping with depression/social
isolation– Managing wandering– Managing behavioral agitation– Helping with memory (names,
locations)
Mental Health Consequences of Caregiving 40 % to 70% of caregivers have clinically significant
symptoms of depression Depression tends to be higher among: Female and spousal caregivers Caregivers of dementia patients and those with mental
illness.
Depression is associated with behavior problems, cognitive impairments and care burden
Caregivers use prescription drugs for depression, anxiety, and insomnia 2-3 time more thanthe rest of the population.

Transition group
Burton, Zdaniuk, & Schulz et al. (2003). The Gerontologist

Caregiver Intervention Studies: Summary of Findings
There have been numerous studies aimed at developing interventions for caregivers
On average, successful in: Alleviating burden Depression Increasing general subjective well-being Increasing ability/knowledge Delaying placement
Many caregivers do not have access to or take advantage of existing programs and resources

Community REACH
• Translation of REACH II Multi-componet Psychosocial Intervention Program to a Community Agency: United HomeCare Services– Largest Community Care for the
Elderly Agency in the State of Florida• Partners: UM Center on Aging,
Alzheimer’s Association, Alliance on Aging, United HomeCare Services

Program Design• Target sample: 150 dyads recruited over three-years. • The intervention duration was 6-months.• The intervention consisted of 12 individual sessions
(6 home sessions and 6 telephone sessions) and 5 telephone support-group sessions:– Education about caregiving and dementia– Caregiving skills– Management of behavioral problems– Stress management– Self-care and health– Social support
• The intervention was delivered by United Home Care who were trained and supervised by the UM team.
• Pre-Post Study Design.

Sample Characteristics (N = 146 dyads)• Caregiver:
– Gender: Female: 77%; Male: 23%– Age: mean = 65.7 yrs; SD = 12.8– Providing care from 6 months to up to 32 years– Hispanic: 83%– CESD 16 or > : 47%
• CR:– Gender: Female 61%; Male 39%– Age: mean = 82.4 yrs; SD = 6.1– MMSE: mean = 11.1; SD = 7.80– ADLs: mean = 4.5; SD = 1.8– IADLS: mean = 7.21; SD =1.03
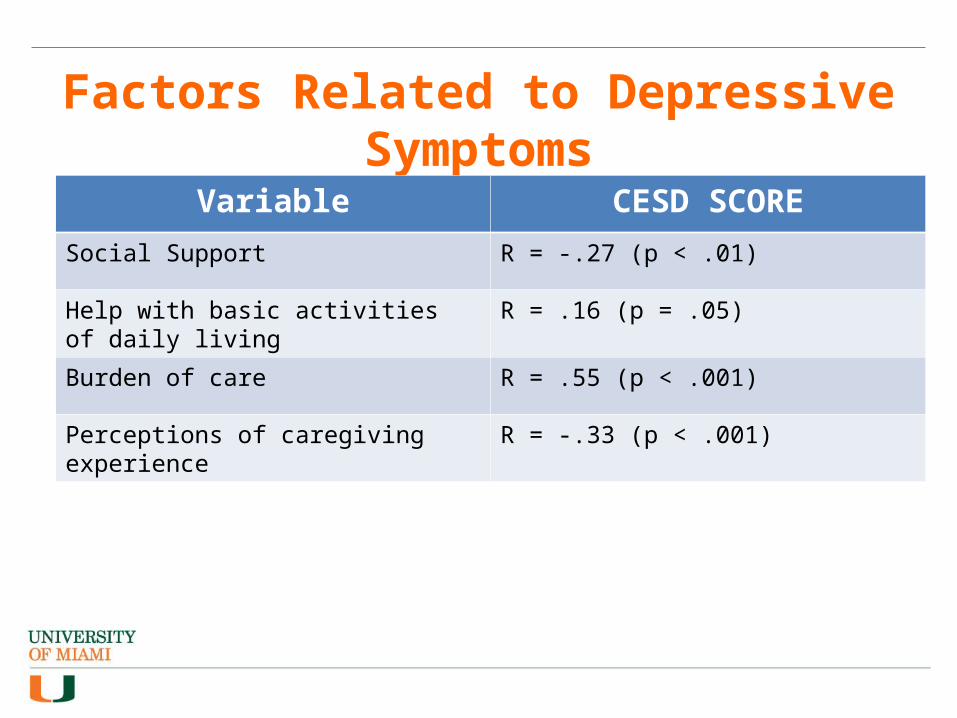
Factors Related to Depressive Symptoms
Variable CESD SCORE
Social Support R = -.27 (p < .01)
Help with basic activities of daily living R = .16 (p = .05)
Burden of care R = .55 (p < .001)
Perceptions of caregiving experience R = -.33 (p < .001)

Results: 6th month follow-up (n = 109)• Decrease in CG depressive symptoms (p <.01).• Decrease in overall burden (p <.01).• Significantly less bothered by care recipients behavior (p <.001).• Increased use of formal care and services for CG and CR (p <.01).• Increase in perceived social support (p <.01).• Increase in positive feelings about being in the caregiver role (p
<.05).• Increase in quality of sleep (p <.01).

Results: 12th month follow-up (n = 101)
• The impact of the intervention on caregiver outcomes was maintained at 12 months.
• No changes (from 6 mths) in CG depression, burden, being bothered by CR behavior, or positive feelings about being a CG.
• Decrease in perceived social support and use of formal care and services for the CR.
Program Evaluation• Caregivers indicated that they benefited a great deal from
participating in the intervention (89%).
• The majority felt that the intervention did a great deal to make caregivers life easier (61%).
• All of the caregivers (100%) indicated that they would recommend the intervention to a friend.
• Most (85%) indicated that the support groups were valuable.• Caregiving benefits:
– Better understanding of memory loss– Better able to provide care for their loved ones– Helped to keep the CR living at home– Enhanced the CGs’ life
Sample Caregiver Reaction “My name is L.D., 80 y/o; caregiver of my 81 y/o husband J.D. diagnosed with Alzheimer. I don't know how would I have survived physically and emotionally without the help received from United Home Care. Through the REACH program where sharing with other people takes away the feeling of loneliness; then my counselors have been everything to me. They have given me the strength and support that have kept me from a total breakdown; now I have the tools they taught me to care for myself. The help of having a respite provided me to have time for myself. Your program provides the help, strength and support so much needed by families of caregivers. In my case I could not have continued without REACH. THANK YOU, L.D.”

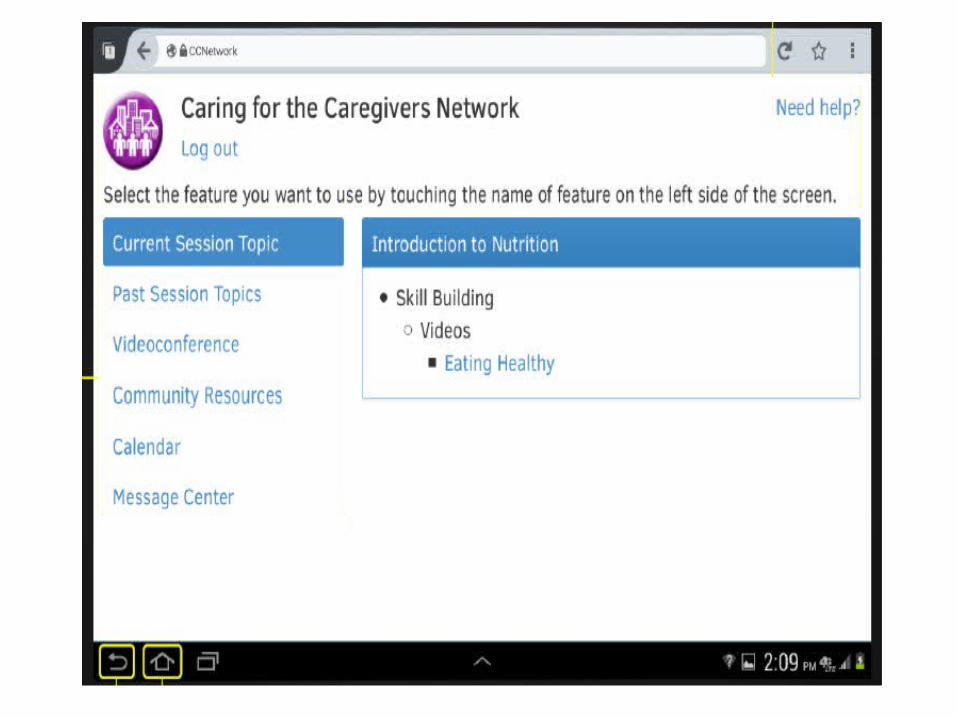
A Tailored Technology Intervention for Diverse Family Caregivers of AD
Patients

Study Aims and GoalsAims:•Evaluate the acceptability of a culturally tailored technology-based psychosocial intervention for family caregivers of AD patients.•Evaluate the impact of the intervention on caregiver outcomes (emotional distress, burden, caregiving skills).•Gather data on ethnic differences in response to the intervention.Overall Goals: Develop an effective intervention program that:•Improves the quality of life of caregivers of AD patients•Enhance skills of and access to formal and informal support for caregivers

Study Design

Depression is often undiagnosed in older adults and family caregivers.
Consequences of depression in late life are significant.
Need better strategies for assessment of depression in older patients and family caregivers.
Need better information on the link between cognitive impairment and depression.
Non-pharmacological intervention approaches are successful in improving caregiver outcomes.
More information is needed on the biological markers of depression
Summary and Conclusions