Orthopedics 5th year, 1st lecture (Dr. Hamid)
54
Anatomy of the Cervical Spine
-
Upload
college-of-medicine-sulaymaniyah -
Category
Health & Medicine
-
view
1.437 -
download
0
description
The lecture has been given on May 4th, 2011 by Dr. Hamid.
Transcript of Orthopedics 5th year, 1st lecture (Dr. Hamid)

Anatomy of the Cervical Spine
Cervical Spine Anatomy
bullPrimary functionndashMobility support and
protection of spinal canal and neural structures
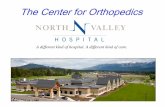
Cervical Spine Anatomy
bullVertebrae (7)
bullIntervertebral discs (6)
bullPairs of exiting nerve roots (8)
bullCervical lordosis Occ-C7 averages 40deg
ndashMost of the lordosis occurs at the C1-C2 segment
11
22
33
44
5566
77
Cervical Spine AnatomybullApproximately 50 of flexion-
extension motion occurs at occiput-C1
bullApproximately 50 of rotation occurs at C1-C2
bullLesser amounts of flexion-extension rotation and lateral
bending occur segmentally between C2-C7
Cervical Spine Anatomy
Cervical Spine Anatomy
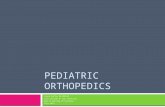
bullAtypical vertebral
bullstructure C1 (atlas)
bullVertebral canalforamen
bullAnterior arch
bullAnterior tubercle
bullTransverse process
bullPosterior arch
bullTransverse foramen
bullLateral massOccipital condyles
Foramen magnum
Superior
Inferior
Cervical Spine Anatomy
bullAtypical cervical
bullvertebra C2 (axis)
bullOdontoid process or dens
bullVertebral canalforamen
bullFacet joints
bullTransverse process
bullTransverse foramen
bullBifid spinous process
bullLamina
anterior view
posterior view
Cervical Spine Anatomy
bullThe odontoid process of the axis (C2) extends
cranially to form the axis of rotation with atlas (C1)
Cervical Spine Anatomy
bullLigamentsndashThe cervical spine also
features a complex arrangement of ligaments to supplement its structure and
mobility
Cervical Spine Anatomy
bullLigamentsndashAnterior longitudinal
ligament
ndashPosterior longitudinal ligament
ndashLigamentum flavum
ndashIntertransverse ligaments
ndashInterspinous ligaments
ndashLigamentum nuchae
Cervical Spine Anatomy
bullLigamentsndashAnterior longitudinal
ligament
ndashPosterior longitudinal ligament
ndashLigamentum flavum
ndashIntertransverse ligaments
ndashInterspinous ligaments
ndashLigamentum nuchae
Cervical Spine Anatomy
bullLigamentsndashAnterior longitudinal
ligament
ndashPosterior longitudinal ligament
ndashLigamentum flavum
ndashIntertransverse ligaments
ndashInterspinous ligaments
ndashLigamentum nuchae
Cervical Spine Anatomy
bullLigamentsndashAnterior longitudinal
ligament
ndashPosterior longitudinal ligament
ndashLigamentum flavum
ndashIntertransverse ligaments
ndashInterspinous ligaments
ndashLigamentum nuchae
Cervical Spine Anatomy
bullLigamentsndashAnterior longitudinal
ligament
ndashPosterior longitudinal ligament
ndashLigamentum flavum
ndashIntertransverse ligaments
ndashInterspinous ligaments
ndashLigamentum nuchae
Cervical Spine Anatomy
bullLigamentsndashAnterior longitudinal
ligament
ndashPosterior longitudinal ligament
ndashLigamentum flavum
ndashIntertransverse ligaments
ndashInterspinous ligaments
ndashLigamentum nuchae
Cervical Spine Anatomy
bull Neural elementsndash8 pair of cervical nervesndashExit the spinal canal
superior to the vertebrae for which they are
numberedbullC1 nerves exit the canal
between Occ amp C1bullC2 nerves exit the canal
between C1 amp C2bullC8 nerves exit the canal
between C7 amp T1
Cervical Spine Anatomy
bull ArteriesndashCarotid arteries
bullLocated anterior and bilateral to the spine
ndashVertebral arteriesbullEnter the transverse
foramen at C6 and continue through C1
Cervical Spine Anatomy
bull VeinsndashJugular veins
bullLocated bilateral and anterior to the spine
ndashVertebral veinsbullLocated within the
transverse foramen of C1-C7
Cervical Spine Anatomy
Neural and Circulatory Elements
Torticollis
bullInfantile ndashcongenital ndash
bullCause and discription
bullClinical feature
DDXX-ray
Treatment
bullSecondary torticollis
bull
Prolapsed Intervertebral Discs
Introduction
bull Male predominance
bull 30 ndash 50 yrs
bull Smokers
bull Sudden flexionamp Twisting
bullFUNCTION OF SPINE
bullndashCombination of stability and
bullmobility due to 2 types of joints
bull1048708Facet Joints
bull1048708Intervertebral disc
bullTYPES OF JOINTSbullA- Facet joint- Typical (Diathrodial)
bull1048708 Lined with synovial membrane
bull1048708 Minimal resistance to movemetns
bullB- IVD
bulllining
bull1048708 Disc- Bears load associated with erect
bullpostur
bull1048708 Allows movements between hellip Bodies
bullANATOMY OF
bullINTERVERTEBRAL DISC
bull1 -Annulus- concentric laminae of collagen
bullfibrils
bull ndashOutermost ndash Sharpey fibers attached to bone
bullTough - type I collagen
bull ndashInner ndash less tough ndash type II collagen
bull2 -Nucleus pulposus
bullonly type II collagen
Nerve root
bull Medial amp inferior to the pedicle at
each level
bull More susceptiple for mechanical
deformation
--lack an epineurium
--reduced collagen content
--more parallel orientation of nfibres
fig
Pathology
bull Normal aging
bull -disc degeneration-displacement of facet joint
bull -acute disc herneation-pain
bull -2ndary effect-aquired SS
---Effects of pressure on the nerve root
Pathophysiology bull Effects of pressure on the nerve root
-Compressive
bull -Deformation-stramp funchanges
Classification
bull A-Site5-66-7
bull B-Direction posterolat
bull C-Amount
---Bulge
--Herniation
1-Protrusion
2-extrusion
3- sequestration
Effects of prolapse
Clinical picture
bullPressure on Dura
bullPressure on root
bullPressure on cord
bullMixed
Imagingbull X-raybull MRIbull CT scans with or without myelography -intolerant to MRI -Unsuitable for MRIbull gadolinium-enhanced MRI This will help to delineate which part of the
previous operation site is disc and which is epidural fibrosis (the latter enhancing)
DDX
bullAcute muscularampST strain
bullNeuralgic amyatrophy
bull Infection
Tumor
bullRotator cuff syndrome
Treatmentbull usually have a good prognosis
bull In up to four-fifths of patients symptoms
will resolve spontaneously within a 12-week
period
bull However if pain persists beyond this time
there is a slow resolution of pain in the
majority of patients
bull By approximately 4 years there is no difference in the incidence of pain in
patients treated non-operatively or surgically
bull Surgical results will deteriorate after
symptoms have been present for 1
year
Non-operative treatment
bull ANALGESICSampANTIINFLAMATORY
bull REST-collar
bull Reduce-traction
bull
Indications for diskectomybull Strong indications for surgical intervention
-Acute mylopathy or myloradiculopathy
-Progressive Neurological deficit
bull Relative indications
bull Failure of conservative treatment-refractory
bull Significant motor deficit
bull Severe incapacitating pain - does not respond to any form of treatment
surgical treatment--ANTERIOR OPEN APPROACH
--POSTERIOR OPEN APPROACH
--Microdisectomy
--Chemonucleolysis
--percutanious
Complications
1--Approach relatedbull 2--mechanical intraopbull 3-early postop wound infectionsDiscitis bull Haematoma-Airway obsbull 4-late postop-Non-union-Instability-deformity

Cervical Spine Anatomy
bullPrimary functionndashMobility support and
protection of spinal canal and neural structures
Cervical Spine Anatomy
bullVertebrae (7)
bullIntervertebral discs (6)
bullPairs of exiting nerve roots (8)
bullCervical lordosis Occ-C7 averages 40deg
ndashMost of the lordosis occurs at the C1-C2 segment
11
22
33
44
5566
77
Cervical Spine AnatomybullApproximately 50 of flexion-
extension motion occurs at occiput-C1
bullApproximately 50 of rotation occurs at C1-C2
bullLesser amounts of flexion-extension rotation and lateral
bending occur segmentally between C2-C7
Cervical Spine Anatomy
Cervical Spine Anatomy
bullAtypical vertebral
bullstructure C1 (atlas)
bullVertebral canalforamen
bullAnterior arch
bullAnterior tubercle
bullTransverse process
bullPosterior arch
bullTransverse foramen
bullLateral massOccipital condyles
Foramen magnum
Superior
Inferior
Cervical Spine Anatomy
bullAtypical cervical
bullvertebra C2 (axis)
bullOdontoid process or dens
bullVertebral canalforamen
bullFacet joints
bullTransverse process
bullTransverse foramen
bullBifid spinous process
bullLamina
anterior view
posterior view
Cervical Spine Anatomy
bullThe odontoid process of the axis (C2) extends
cranially to form the axis of rotation with atlas (C1)
Cervical Spine Anatomy
bullLigamentsndashThe cervical spine also
features a complex arrangement of ligaments to supplement its structure and
mobility
Cervical Spine Anatomy
bullLigamentsndashAnterior longitudinal
ligament
ndashPosterior longitudinal ligament
ndashLigamentum flavum
ndashIntertransverse ligaments
ndashInterspinous ligaments
ndashLigamentum nuchae
Cervical Spine Anatomy
bullLigamentsndashAnterior longitudinal
ligament
ndashPosterior longitudinal ligament
ndashLigamentum flavum
ndashIntertransverse ligaments
ndashInterspinous ligaments
ndashLigamentum nuchae
Cervical Spine Anatomy
bullLigamentsndashAnterior longitudinal
ligament
ndashPosterior longitudinal ligament
ndashLigamentum flavum
ndashIntertransverse ligaments
ndashInterspinous ligaments
ndashLigamentum nuchae
Cervical Spine Anatomy
bullLigamentsndashAnterior longitudinal
ligament
ndashPosterior longitudinal ligament
ndashLigamentum flavum
ndashIntertransverse ligaments
ndashInterspinous ligaments
ndashLigamentum nuchae
Cervical Spine Anatomy
bullLigamentsndashAnterior longitudinal
ligament
ndashPosterior longitudinal ligament
ndashLigamentum flavum
ndashIntertransverse ligaments
ndashInterspinous ligaments
ndashLigamentum nuchae
Cervical Spine Anatomy
bullLigamentsndashAnterior longitudinal
ligament
ndashPosterior longitudinal ligament
ndashLigamentum flavum
ndashIntertransverse ligaments
ndashInterspinous ligaments
ndashLigamentum nuchae
Cervical Spine Anatomy
bull Neural elementsndash8 pair of cervical nervesndashExit the spinal canal
superior to the vertebrae for which they are
numberedbullC1 nerves exit the canal
between Occ amp C1bullC2 nerves exit the canal
between C1 amp C2bullC8 nerves exit the canal
between C7 amp T1
Cervical Spine Anatomy
bull ArteriesndashCarotid arteries
bullLocated anterior and bilateral to the spine
ndashVertebral arteriesbullEnter the transverse
foramen at C6 and continue through C1
Cervical Spine Anatomy
bull VeinsndashJugular veins
bullLocated bilateral and anterior to the spine
ndashVertebral veinsbullLocated within the
transverse foramen of C1-C7
Cervical Spine Anatomy
Neural and Circulatory Elements
Torticollis
bullInfantile ndashcongenital ndash
bullCause and discription
bullClinical feature
DDXX-ray
Treatment
bullSecondary torticollis
bull
Prolapsed Intervertebral Discs
Introduction
bull Male predominance
bull 30 ndash 50 yrs
bull Smokers
bull Sudden flexionamp Twisting
bullFUNCTION OF SPINE
bullndashCombination of stability and
bullmobility due to 2 types of joints
bull1048708Facet Joints
bull1048708Intervertebral disc
bullTYPES OF JOINTSbullA- Facet joint- Typical (Diathrodial)
bull1048708 Lined with synovial membrane
bull1048708 Minimal resistance to movemetns
bullB- IVD
bulllining
bull1048708 Disc- Bears load associated with erect
bullpostur
bull1048708 Allows movements between hellip Bodies
bullANATOMY OF
bullINTERVERTEBRAL DISC
bull1 -Annulus- concentric laminae of collagen
bullfibrils
bull ndashOutermost ndash Sharpey fibers attached to bone
bullTough - type I collagen
bull ndashInner ndash less tough ndash type II collagen
bull2 -Nucleus pulposus
bullonly type II collagen
Nerve root
bull Medial amp inferior to the pedicle at
each level
bull More susceptiple for mechanical
deformation
--lack an epineurium
--reduced collagen content
--more parallel orientation of nfibres
fig
Pathology
bull Normal aging
bull -disc degeneration-displacement of facet joint
bull -acute disc herneation-pain
bull -2ndary effect-aquired SS
---Effects of pressure on the nerve root
Pathophysiology bull Effects of pressure on the nerve root
-Compressive
bull -Deformation-stramp funchanges
Classification
bull A-Site5-66-7
bull B-Direction posterolat
bull C-Amount
---Bulge
--Herniation
1-Protrusion
2-extrusion
3- sequestration
Effects of prolapse
Clinical picture
bullPressure on Dura
bullPressure on root
bullPressure on cord
bullMixed
Imagingbull X-raybull MRIbull CT scans with or without myelography -intolerant to MRI -Unsuitable for MRIbull gadolinium-enhanced MRI This will help to delineate which part of the
previous operation site is disc and which is epidural fibrosis (the latter enhancing)
DDX
bullAcute muscularampST strain
bullNeuralgic amyatrophy
bull Infection
Tumor
bullRotator cuff syndrome
Treatmentbull usually have a good prognosis
bull In up to four-fifths of patients symptoms
will resolve spontaneously within a 12-week
period
bull However if pain persists beyond this time
there is a slow resolution of pain in the
majority of patients
bull By approximately 4 years there is no difference in the incidence of pain in
patients treated non-operatively or surgically
bull Surgical results will deteriorate after
symptoms have been present for 1
year
Non-operative treatment
bull ANALGESICSampANTIINFLAMATORY
bull REST-collar
bull Reduce-traction
bull
Indications for diskectomybull Strong indications for surgical intervention
-Acute mylopathy or myloradiculopathy
-Progressive Neurological deficit
bull Relative indications
bull Failure of conservative treatment-refractory
bull Significant motor deficit
bull Severe incapacitating pain - does not respond to any form of treatment
surgical treatment--ANTERIOR OPEN APPROACH
--POSTERIOR OPEN APPROACH
--Microdisectomy
--Chemonucleolysis
--percutanious
Complications
1--Approach relatedbull 2--mechanical intraopbull 3-early postop wound infectionsDiscitis bull Haematoma-Airway obsbull 4-late postop-Non-union-Instability-deformity

Cervical Spine Anatomy
bullVertebrae (7)
bullIntervertebral discs (6)
bullPairs of exiting nerve roots (8)
bullCervical lordosis Occ-C7 averages 40deg
ndashMost of the lordosis occurs at the C1-C2 segment
11
22
33
44
5566
77
Cervical Spine AnatomybullApproximately 50 of flexion-
extension motion occurs at occiput-C1
bullApproximately 50 of rotation occurs at C1-C2
bullLesser amounts of flexion-extension rotation and lateral
bending occur segmentally between C2-C7
Cervical Spine Anatomy
Cervical Spine Anatomy
bullAtypical vertebral
bullstructure C1 (atlas)
bullVertebral canalforamen
bullAnterior arch
bullAnterior tubercle
bullTransverse process
bullPosterior arch
bullTransverse foramen
bullLateral massOccipital condyles
Foramen magnum
Superior
Inferior
Cervical Spine Anatomy
bullAtypical cervical
bullvertebra C2 (axis)
bullOdontoid process or dens
bullVertebral canalforamen
bullFacet joints
bullTransverse process
bullTransverse foramen
bullBifid spinous process
bullLamina
anterior view
posterior view
Cervical Spine Anatomy
bullThe odontoid process of the axis (C2) extends
cranially to form the axis of rotation with atlas (C1)
Cervical Spine Anatomy
bullLigamentsndashThe cervical spine also
features a complex arrangement of ligaments to supplement its structure and
mobility
Cervical Spine Anatomy
bullLigamentsndashAnterior longitudinal
ligament
ndashPosterior longitudinal ligament
ndashLigamentum flavum
ndashIntertransverse ligaments
ndashInterspinous ligaments
ndashLigamentum nuchae
Cervical Spine Anatomy
bullLigamentsndashAnterior longitudinal
ligament
ndashPosterior longitudinal ligament
ndashLigamentum flavum
ndashIntertransverse ligaments
ndashInterspinous ligaments
ndashLigamentum nuchae
Cervical Spine Anatomy
bullLigamentsndashAnterior longitudinal
ligament
ndashPosterior longitudinal ligament
ndashLigamentum flavum
ndashIntertransverse ligaments
ndashInterspinous ligaments
ndashLigamentum nuchae
Cervical Spine Anatomy
bullLigamentsndashAnterior longitudinal
ligament
ndashPosterior longitudinal ligament
ndashLigamentum flavum
ndashIntertransverse ligaments
ndashInterspinous ligaments
ndashLigamentum nuchae
Cervical Spine Anatomy
bullLigamentsndashAnterior longitudinal
ligament
ndashPosterior longitudinal ligament
ndashLigamentum flavum
ndashIntertransverse ligaments
ndashInterspinous ligaments
ndashLigamentum nuchae
Cervical Spine Anatomy
bullLigamentsndashAnterior longitudinal
ligament
ndashPosterior longitudinal ligament
ndashLigamentum flavum
ndashIntertransverse ligaments
ndashInterspinous ligaments
ndashLigamentum nuchae
Cervical Spine Anatomy
bull Neural elementsndash8 pair of cervical nervesndashExit the spinal canal
superior to the vertebrae for which they are
numberedbullC1 nerves exit the canal
between Occ amp C1bullC2 nerves exit the canal
between C1 amp C2bullC8 nerves exit the canal
between C7 amp T1
Cervical Spine Anatomy
bull ArteriesndashCarotid arteries
bullLocated anterior and bilateral to the spine
ndashVertebral arteriesbullEnter the transverse
foramen at C6 and continue through C1
Cervical Spine Anatomy
bull VeinsndashJugular veins
bullLocated bilateral and anterior to the spine
ndashVertebral veinsbullLocated within the
transverse foramen of C1-C7
Cervical Spine Anatomy
Neural and Circulatory Elements
Torticollis
bullInfantile ndashcongenital ndash
bullCause and discription
bullClinical feature
DDXX-ray
Treatment
bullSecondary torticollis
bull
Prolapsed Intervertebral Discs
Introduction
bull Male predominance
bull 30 ndash 50 yrs
bull Smokers
bull Sudden flexionamp Twisting
bullFUNCTION OF SPINE
bullndashCombination of stability and
bullmobility due to 2 types of joints
bull1048708Facet Joints
bull1048708Intervertebral disc
bullTYPES OF JOINTSbullA- Facet joint- Typical (Diathrodial)
bull1048708 Lined with synovial membrane
bull1048708 Minimal resistance to movemetns
bullB- IVD
bulllining
bull1048708 Disc- Bears load associated with erect
bullpostur
bull1048708 Allows movements between hellip Bodies
bullANATOMY OF
bullINTERVERTEBRAL DISC
bull1 -Annulus- concentric laminae of collagen
bullfibrils
bull ndashOutermost ndash Sharpey fibers attached to bone
bullTough - type I collagen
bull ndashInner ndash less tough ndash type II collagen
bull2 -Nucleus pulposus
bullonly type II collagen
Nerve root
bull Medial amp inferior to the pedicle at
each level
bull More susceptiple for mechanical
deformation
--lack an epineurium
--reduced collagen content
--more parallel orientation of nfibres
fig
Pathology
bull Normal aging
bull -disc degeneration-displacement of facet joint
bull -acute disc herneation-pain
bull -2ndary effect-aquired SS
---Effects of pressure on the nerve root
Pathophysiology bull Effects of pressure on the nerve root
-Compressive
bull -Deformation-stramp funchanges
Classification
bull A-Site5-66-7
bull B-Direction posterolat
bull C-Amount
---Bulge
--Herniation
1-Protrusion
2-extrusion
3- sequestration
Effects of prolapse
Clinical picture
bullPressure on Dura
bullPressure on root
bullPressure on cord
bullMixed
Imagingbull X-raybull MRIbull CT scans with or without myelography -intolerant to MRI -Unsuitable for MRIbull gadolinium-enhanced MRI This will help to delineate which part of the
previous operation site is disc and which is epidural fibrosis (the latter enhancing)
DDX
bullAcute muscularampST strain
bullNeuralgic amyatrophy
bull Infection
Tumor
bullRotator cuff syndrome
Treatmentbull usually have a good prognosis
bull In up to four-fifths of patients symptoms
will resolve spontaneously within a 12-week
period
bull However if pain persists beyond this time
there is a slow resolution of pain in the
majority of patients
bull By approximately 4 years there is no difference in the incidence of pain in
patients treated non-operatively or surgically
bull Surgical results will deteriorate after
symptoms have been present for 1
year
Non-operative treatment
bull ANALGESICSampANTIINFLAMATORY
bull REST-collar
bull Reduce-traction
bull
Indications for diskectomybull Strong indications for surgical intervention
-Acute mylopathy or myloradiculopathy
-Progressive Neurological deficit
bull Relative indications
bull Failure of conservative treatment-refractory
bull Significant motor deficit
bull Severe incapacitating pain - does not respond to any form of treatment
surgical treatment--ANTERIOR OPEN APPROACH
--POSTERIOR OPEN APPROACH
--Microdisectomy
--Chemonucleolysis
--percutanious
Complications
1--Approach relatedbull 2--mechanical intraopbull 3-early postop wound infectionsDiscitis bull Haematoma-Airway obsbull 4-late postop-Non-union-Instability-deformity

Cervical Spine AnatomybullApproximately 50 of flexion-
extension motion occurs at occiput-C1
bullApproximately 50 of rotation occurs at C1-C2
bullLesser amounts of flexion-extension rotation and lateral
bending occur segmentally between C2-C7
Cervical Spine Anatomy
Cervical Spine Anatomy
bullAtypical vertebral
bullstructure C1 (atlas)
bullVertebral canalforamen
bullAnterior arch
bullAnterior tubercle
bullTransverse process
bullPosterior arch
bullTransverse foramen
bullLateral massOccipital condyles
Foramen magnum
Superior
Inferior
Cervical Spine Anatomy
bullAtypical cervical
bullvertebra C2 (axis)
bullOdontoid process or dens
bullVertebral canalforamen
bullFacet joints
bullTransverse process
bullTransverse foramen
bullBifid spinous process
bullLamina
anterior view
posterior view
Cervical Spine Anatomy
bullThe odontoid process of the axis (C2) extends
cranially to form the axis of rotation with atlas (C1)
Cervical Spine Anatomy
bullLigamentsndashThe cervical spine also
features a complex arrangement of ligaments to supplement its structure and
mobility
Cervical Spine Anatomy
bullLigamentsndashAnterior longitudinal
ligament
ndashPosterior longitudinal ligament
ndashLigamentum flavum
ndashIntertransverse ligaments
ndashInterspinous ligaments
ndashLigamentum nuchae
Cervical Spine Anatomy
bullLigamentsndashAnterior longitudinal
ligament
ndashPosterior longitudinal ligament
ndashLigamentum flavum
ndashIntertransverse ligaments
ndashInterspinous ligaments
ndashLigamentum nuchae
Cervical Spine Anatomy
bullLigamentsndashAnterior longitudinal
ligament
ndashPosterior longitudinal ligament
ndashLigamentum flavum
ndashIntertransverse ligaments
ndashInterspinous ligaments
ndashLigamentum nuchae
Cervical Spine Anatomy
bullLigamentsndashAnterior longitudinal
ligament
ndashPosterior longitudinal ligament
ndashLigamentum flavum
ndashIntertransverse ligaments
ndashInterspinous ligaments
ndashLigamentum nuchae
Cervical Spine Anatomy
bullLigamentsndashAnterior longitudinal
ligament
ndashPosterior longitudinal ligament
ndashLigamentum flavum
ndashIntertransverse ligaments
ndashInterspinous ligaments
ndashLigamentum nuchae
Cervical Spine Anatomy
bullLigamentsndashAnterior longitudinal
ligament
ndashPosterior longitudinal ligament
ndashLigamentum flavum
ndashIntertransverse ligaments
ndashInterspinous ligaments
ndashLigamentum nuchae
Cervical Spine Anatomy
bull Neural elementsndash8 pair of cervical nervesndashExit the spinal canal
superior to the vertebrae for which they are
numberedbullC1 nerves exit the canal
between Occ amp C1bullC2 nerves exit the canal
between C1 amp C2bullC8 nerves exit the canal
between C7 amp T1
Cervical Spine Anatomy
bull ArteriesndashCarotid arteries
bullLocated anterior and bilateral to the spine
ndashVertebral arteriesbullEnter the transverse
foramen at C6 and continue through C1
Cervical Spine Anatomy
bull VeinsndashJugular veins
bullLocated bilateral and anterior to the spine
ndashVertebral veinsbullLocated within the
transverse foramen of C1-C7
Cervical Spine Anatomy
Neural and Circulatory Elements
Torticollis
bullInfantile ndashcongenital ndash
bullCause and discription
bullClinical feature
DDXX-ray
Treatment
bullSecondary torticollis
bull
Prolapsed Intervertebral Discs
Introduction
bull Male predominance
bull 30 ndash 50 yrs
bull Smokers
bull Sudden flexionamp Twisting
bullFUNCTION OF SPINE
bullndashCombination of stability and
bullmobility due to 2 types of joints
bull1048708Facet Joints
bull1048708Intervertebral disc
bullTYPES OF JOINTSbullA- Facet joint- Typical (Diathrodial)
bull1048708 Lined with synovial membrane
bull1048708 Minimal resistance to movemetns
bullB- IVD
bulllining
bull1048708 Disc- Bears load associated with erect
bullpostur
bull1048708 Allows movements between hellip Bodies
bullANATOMY OF
bullINTERVERTEBRAL DISC
bull1 -Annulus- concentric laminae of collagen
bullfibrils
bull ndashOutermost ndash Sharpey fibers attached to bone
bullTough - type I collagen
bull ndashInner ndash less tough ndash type II collagen
bull2 -Nucleus pulposus
bullonly type II collagen
Nerve root
bull Medial amp inferior to the pedicle at
each level
bull More susceptiple for mechanical
deformation
--lack an epineurium
--reduced collagen content
--more parallel orientation of nfibres
fig
Pathology
bull Normal aging
bull -disc degeneration-displacement of facet joint
bull -acute disc herneation-pain
bull -2ndary effect-aquired SS
---Effects of pressure on the nerve root
Pathophysiology bull Effects of pressure on the nerve root
-Compressive
bull -Deformation-stramp funchanges
Classification
bull A-Site5-66-7
bull B-Direction posterolat
bull C-Amount
---Bulge
--Herniation
1-Protrusion
2-extrusion
3- sequestration
Effects of prolapse
Clinical picture
bullPressure on Dura
bullPressure on root
bullPressure on cord
bullMixed
Imagingbull X-raybull MRIbull CT scans with or without myelography -intolerant to MRI -Unsuitable for MRIbull gadolinium-enhanced MRI This will help to delineate which part of the
previous operation site is disc and which is epidural fibrosis (the latter enhancing)
DDX
bullAcute muscularampST strain
bullNeuralgic amyatrophy
bull Infection
Tumor
bullRotator cuff syndrome
Treatmentbull usually have a good prognosis
bull In up to four-fifths of patients symptoms
will resolve spontaneously within a 12-week
period
bull However if pain persists beyond this time
there is a slow resolution of pain in the
majority of patients
bull By approximately 4 years there is no difference in the incidence of pain in
patients treated non-operatively or surgically
bull Surgical results will deteriorate after
symptoms have been present for 1
year
Non-operative treatment
bull ANALGESICSampANTIINFLAMATORY
bull REST-collar
bull Reduce-traction
bull
Indications for diskectomybull Strong indications for surgical intervention
-Acute mylopathy or myloradiculopathy
-Progressive Neurological deficit
bull Relative indications
bull Failure of conservative treatment-refractory
bull Significant motor deficit
bull Severe incapacitating pain - does not respond to any form of treatment
surgical treatment--ANTERIOR OPEN APPROACH
--POSTERIOR OPEN APPROACH
--Microdisectomy
--Chemonucleolysis
--percutanious
Complications
1--Approach relatedbull 2--mechanical intraopbull 3-early postop wound infectionsDiscitis bull Haematoma-Airway obsbull 4-late postop-Non-union-Instability-deformity

Cervical Spine Anatomy
Cervical Spine Anatomy
bullAtypical vertebral
bullstructure C1 (atlas)
bullVertebral canalforamen
bullAnterior arch
bullAnterior tubercle
bullTransverse process
bullPosterior arch
bullTransverse foramen
bullLateral massOccipital condyles
Foramen magnum
Superior
Inferior
Cervical Spine Anatomy
bullAtypical cervical
bullvertebra C2 (axis)
bullOdontoid process or dens
bullVertebral canalforamen
bullFacet joints
bullTransverse process
bullTransverse foramen
bullBifid spinous process
bullLamina
anterior view
posterior view
Cervical Spine Anatomy
bullThe odontoid process of the axis (C2) extends
cranially to form the axis of rotation with atlas (C1)
Cervical Spine Anatomy
bullLigamentsndashThe cervical spine also
features a complex arrangement of ligaments to supplement its structure and
mobility
Cervical Spine Anatomy
bullLigamentsndashAnterior longitudinal
ligament
ndashPosterior longitudinal ligament
ndashLigamentum flavum
ndashIntertransverse ligaments
ndashInterspinous ligaments
ndashLigamentum nuchae
Cervical Spine Anatomy
bullLigamentsndashAnterior longitudinal
ligament
ndashPosterior longitudinal ligament
ndashLigamentum flavum
ndashIntertransverse ligaments
ndashInterspinous ligaments
ndashLigamentum nuchae
Cervical Spine Anatomy
bullLigamentsndashAnterior longitudinal
ligament
ndashPosterior longitudinal ligament
ndashLigamentum flavum
ndashIntertransverse ligaments
ndashInterspinous ligaments
ndashLigamentum nuchae
Cervical Spine Anatomy
bullLigamentsndashAnterior longitudinal
ligament
ndashPosterior longitudinal ligament
ndashLigamentum flavum
ndashIntertransverse ligaments
ndashInterspinous ligaments
ndashLigamentum nuchae
Cervical Spine Anatomy
bullLigamentsndashAnterior longitudinal
ligament
ndashPosterior longitudinal ligament
ndashLigamentum flavum
ndashIntertransverse ligaments
ndashInterspinous ligaments
ndashLigamentum nuchae
Cervical Spine Anatomy
bullLigamentsndashAnterior longitudinal
ligament
ndashPosterior longitudinal ligament
ndashLigamentum flavum
ndashIntertransverse ligaments
ndashInterspinous ligaments
ndashLigamentum nuchae
Cervical Spine Anatomy
bull Neural elementsndash8 pair of cervical nervesndashExit the spinal canal
superior to the vertebrae for which they are
numberedbullC1 nerves exit the canal
between Occ amp C1bullC2 nerves exit the canal
between C1 amp C2bullC8 nerves exit the canal
between C7 amp T1
Cervical Spine Anatomy
bull ArteriesndashCarotid arteries
bullLocated anterior and bilateral to the spine
ndashVertebral arteriesbullEnter the transverse
foramen at C6 and continue through C1
Cervical Spine Anatomy
bull VeinsndashJugular veins
bullLocated bilateral and anterior to the spine
ndashVertebral veinsbullLocated within the
transverse foramen of C1-C7
Cervical Spine Anatomy
Neural and Circulatory Elements
Torticollis
bullInfantile ndashcongenital ndash
bullCause and discription
bullClinical feature
DDXX-ray
Treatment
bullSecondary torticollis
bull
Prolapsed Intervertebral Discs
Introduction
bull Male predominance
bull 30 ndash 50 yrs
bull Smokers
bull Sudden flexionamp Twisting
bullFUNCTION OF SPINE
bullndashCombination of stability and
bullmobility due to 2 types of joints
bull1048708Facet Joints
bull1048708Intervertebral disc
bullTYPES OF JOINTSbullA- Facet joint- Typical (Diathrodial)
bull1048708 Lined with synovial membrane
bull1048708 Minimal resistance to movemetns
bullB- IVD
bulllining
bull1048708 Disc- Bears load associated with erect
bullpostur
bull1048708 Allows movements between hellip Bodies
bullANATOMY OF
bullINTERVERTEBRAL DISC
bull1 -Annulus- concentric laminae of collagen
bullfibrils
bull ndashOutermost ndash Sharpey fibers attached to bone
bullTough - type I collagen
bull ndashInner ndash less tough ndash type II collagen
bull2 -Nucleus pulposus
bullonly type II collagen
Nerve root
bull Medial amp inferior to the pedicle at
each level
bull More susceptiple for mechanical
deformation
--lack an epineurium
--reduced collagen content
--more parallel orientation of nfibres
fig
Pathology
bull Normal aging
bull -disc degeneration-displacement of facet joint
bull -acute disc herneation-pain
bull -2ndary effect-aquired SS
---Effects of pressure on the nerve root
Pathophysiology bull Effects of pressure on the nerve root
-Compressive
bull -Deformation-stramp funchanges
Classification
bull A-Site5-66-7
bull B-Direction posterolat
bull C-Amount
---Bulge
--Herniation
1-Protrusion
2-extrusion
3- sequestration
Effects of prolapse
Clinical picture
bullPressure on Dura
bullPressure on root
bullPressure on cord
bullMixed
Imagingbull X-raybull MRIbull CT scans with or without myelography -intolerant to MRI -Unsuitable for MRIbull gadolinium-enhanced MRI This will help to delineate which part of the
previous operation site is disc and which is epidural fibrosis (the latter enhancing)
DDX
bullAcute muscularampST strain
bullNeuralgic amyatrophy
bull Infection
Tumor
bullRotator cuff syndrome
Treatmentbull usually have a good prognosis
bull In up to four-fifths of patients symptoms
will resolve spontaneously within a 12-week
period
bull However if pain persists beyond this time
there is a slow resolution of pain in the
majority of patients
bull By approximately 4 years there is no difference in the incidence of pain in
patients treated non-operatively or surgically
bull Surgical results will deteriorate after
symptoms have been present for 1
year
Non-operative treatment
bull ANALGESICSampANTIINFLAMATORY
bull REST-collar
bull Reduce-traction
bull
Indications for diskectomybull Strong indications for surgical intervention
-Acute mylopathy or myloradiculopathy
-Progressive Neurological deficit
bull Relative indications
bull Failure of conservative treatment-refractory
bull Significant motor deficit
bull Severe incapacitating pain - does not respond to any form of treatment
surgical treatment--ANTERIOR OPEN APPROACH
--POSTERIOR OPEN APPROACH
--Microdisectomy
--Chemonucleolysis
--percutanious
Complications
1--Approach relatedbull 2--mechanical intraopbull 3-early postop wound infectionsDiscitis bull Haematoma-Airway obsbull 4-late postop-Non-union-Instability-deformity

Cervical Spine Anatomy
bullAtypical vertebral
bullstructure C1 (atlas)
bullVertebral canalforamen
bullAnterior arch
bullAnterior tubercle
bullTransverse process
bullPosterior arch
bullTransverse foramen
bullLateral massOccipital condyles
Foramen magnum
Superior
Inferior
Cervical Spine Anatomy
bullAtypical cervical
bullvertebra C2 (axis)
bullOdontoid process or dens
bullVertebral canalforamen
bullFacet joints
bullTransverse process
bullTransverse foramen
bullBifid spinous process
bullLamina
anterior view
posterior view
Cervical Spine Anatomy
bullThe odontoid process of the axis (C2) extends
cranially to form the axis of rotation with atlas (C1)
Cervical Spine Anatomy
bullLigamentsndashThe cervical spine also
features a complex arrangement of ligaments to supplement its structure and
mobility
Cervical Spine Anatomy
bullLigamentsndashAnterior longitudinal
ligament
ndashPosterior longitudinal ligament
ndashLigamentum flavum
ndashIntertransverse ligaments
ndashInterspinous ligaments
ndashLigamentum nuchae
Cervical Spine Anatomy
bullLigamentsndashAnterior longitudinal
ligament
ndashPosterior longitudinal ligament
ndashLigamentum flavum
ndashIntertransverse ligaments
ndashInterspinous ligaments
ndashLigamentum nuchae
Cervical Spine Anatomy
bullLigamentsndashAnterior longitudinal
ligament
ndashPosterior longitudinal ligament
ndashLigamentum flavum
ndashIntertransverse ligaments
ndashInterspinous ligaments
ndashLigamentum nuchae
Cervical Spine Anatomy
bullLigamentsndashAnterior longitudinal
ligament
ndashPosterior longitudinal ligament
ndashLigamentum flavum
ndashIntertransverse ligaments
ndashInterspinous ligaments
ndashLigamentum nuchae
Cervical Spine Anatomy
bullLigamentsndashAnterior longitudinal
ligament
ndashPosterior longitudinal ligament
ndashLigamentum flavum
ndashIntertransverse ligaments
ndashInterspinous ligaments
ndashLigamentum nuchae
Cervical Spine Anatomy
bullLigamentsndashAnterior longitudinal
ligament
ndashPosterior longitudinal ligament
ndashLigamentum flavum
ndashIntertransverse ligaments
ndashInterspinous ligaments
ndashLigamentum nuchae
Cervical Spine Anatomy
bull Neural elementsndash8 pair of cervical nervesndashExit the spinal canal
superior to the vertebrae for which they are
numberedbullC1 nerves exit the canal
between Occ amp C1bullC2 nerves exit the canal
between C1 amp C2bullC8 nerves exit the canal
between C7 amp T1
Cervical Spine Anatomy
bull ArteriesndashCarotid arteries
bullLocated anterior and bilateral to the spine
ndashVertebral arteriesbullEnter the transverse
foramen at C6 and continue through C1
Cervical Spine Anatomy
bull VeinsndashJugular veins
bullLocated bilateral and anterior to the spine
ndashVertebral veinsbullLocated within the
transverse foramen of C1-C7
Cervical Spine Anatomy
Neural and Circulatory Elements
Torticollis
bullInfantile ndashcongenital ndash
bullCause and discription
bullClinical feature
DDXX-ray
Treatment
bullSecondary torticollis
bull
Prolapsed Intervertebral Discs
Introduction
bull Male predominance
bull 30 ndash 50 yrs
bull Smokers
bull Sudden flexionamp Twisting
bullFUNCTION OF SPINE
bullndashCombination of stability and
bullmobility due to 2 types of joints
bull1048708Facet Joints
bull1048708Intervertebral disc
bullTYPES OF JOINTSbullA- Facet joint- Typical (Diathrodial)
bull1048708 Lined with synovial membrane
bull1048708 Minimal resistance to movemetns
bullB- IVD
bulllining
bull1048708 Disc- Bears load associated with erect
bullpostur
bull1048708 Allows movements between hellip Bodies
bullANATOMY OF
bullINTERVERTEBRAL DISC
bull1 -Annulus- concentric laminae of collagen
bullfibrils
bull ndashOutermost ndash Sharpey fibers attached to bone
bullTough - type I collagen
bull ndashInner ndash less tough ndash type II collagen
bull2 -Nucleus pulposus
bullonly type II collagen
Nerve root
bull Medial amp inferior to the pedicle at
each level
bull More susceptiple for mechanical
deformation
--lack an epineurium
--reduced collagen content
--more parallel orientation of nfibres
fig
Pathology
bull Normal aging
bull -disc degeneration-displacement of facet joint
bull -acute disc herneation-pain
bull -2ndary effect-aquired SS
---Effects of pressure on the nerve root
Pathophysiology bull Effects of pressure on the nerve root
-Compressive
bull -Deformation-stramp funchanges
Classification
bull A-Site5-66-7
bull B-Direction posterolat
bull C-Amount
---Bulge
--Herniation
1-Protrusion
2-extrusion
3- sequestration
Effects of prolapse
Clinical picture
bullPressure on Dura
bullPressure on root
bullPressure on cord
bullMixed
Imagingbull X-raybull MRIbull CT scans with or without myelography -intolerant to MRI -Unsuitable for MRIbull gadolinium-enhanced MRI This will help to delineate which part of the
previous operation site is disc and which is epidural fibrosis (the latter enhancing)
DDX
bullAcute muscularampST strain
bullNeuralgic amyatrophy
bull Infection
Tumor
bullRotator cuff syndrome
Treatmentbull usually have a good prognosis
bull In up to four-fifths of patients symptoms
will resolve spontaneously within a 12-week
period
bull However if pain persists beyond this time
there is a slow resolution of pain in the
majority of patients
bull By approximately 4 years there is no difference in the incidence of pain in
patients treated non-operatively or surgically
bull Surgical results will deteriorate after
symptoms have been present for 1
year
Non-operative treatment
bull ANALGESICSampANTIINFLAMATORY
bull REST-collar
bull Reduce-traction
bull
Indications for diskectomybull Strong indications for surgical intervention
-Acute mylopathy or myloradiculopathy
-Progressive Neurological deficit
bull Relative indications
bull Failure of conservative treatment-refractory
bull Significant motor deficit
bull Severe incapacitating pain - does not respond to any form of treatment
surgical treatment--ANTERIOR OPEN APPROACH
--POSTERIOR OPEN APPROACH
--Microdisectomy
--Chemonucleolysis
--percutanious
Complications
1--Approach relatedbull 2--mechanical intraopbull 3-early postop wound infectionsDiscitis bull Haematoma-Airway obsbull 4-late postop-Non-union-Instability-deformity

Cervical Spine Anatomy
bullAtypical cervical
bullvertebra C2 (axis)
bullOdontoid process or dens
bullVertebral canalforamen
bullFacet joints
bullTransverse process
bullTransverse foramen
bullBifid spinous process
bullLamina
anterior view
posterior view
Cervical Spine Anatomy
bullThe odontoid process of the axis (C2) extends
cranially to form the axis of rotation with atlas (C1)
Cervical Spine Anatomy
bullLigamentsndashThe cervical spine also
features a complex arrangement of ligaments to supplement its structure and
mobility
Cervical Spine Anatomy
bullLigamentsndashAnterior longitudinal
ligament
ndashPosterior longitudinal ligament
ndashLigamentum flavum
ndashIntertransverse ligaments
ndashInterspinous ligaments
ndashLigamentum nuchae
Cervical Spine Anatomy
bullLigamentsndashAnterior longitudinal
ligament
ndashPosterior longitudinal ligament
ndashLigamentum flavum
ndashIntertransverse ligaments
ndashInterspinous ligaments
ndashLigamentum nuchae
Cervical Spine Anatomy
bullLigamentsndashAnterior longitudinal
ligament
ndashPosterior longitudinal ligament
ndashLigamentum flavum
ndashIntertransverse ligaments
ndashInterspinous ligaments
ndashLigamentum nuchae
Cervical Spine Anatomy
bullLigamentsndashAnterior longitudinal
ligament
ndashPosterior longitudinal ligament
ndashLigamentum flavum
ndashIntertransverse ligaments
ndashInterspinous ligaments
ndashLigamentum nuchae
Cervical Spine Anatomy
bullLigamentsndashAnterior longitudinal
ligament
ndashPosterior longitudinal ligament
ndashLigamentum flavum
ndashIntertransverse ligaments
ndashInterspinous ligaments
ndashLigamentum nuchae
Cervical Spine Anatomy
bullLigamentsndashAnterior longitudinal
ligament
ndashPosterior longitudinal ligament
ndashLigamentum flavum
ndashIntertransverse ligaments
ndashInterspinous ligaments
ndashLigamentum nuchae
Cervical Spine Anatomy
bull Neural elementsndash8 pair of cervical nervesndashExit the spinal canal
superior to the vertebrae for which they are
numberedbullC1 nerves exit the canal
between Occ amp C1bullC2 nerves exit the canal
between C1 amp C2bullC8 nerves exit the canal
between C7 amp T1
Cervical Spine Anatomy
bull ArteriesndashCarotid arteries
bullLocated anterior and bilateral to the spine
ndashVertebral arteriesbullEnter the transverse
foramen at C6 and continue through C1
Cervical Spine Anatomy
bull VeinsndashJugular veins
bullLocated bilateral and anterior to the spine
ndashVertebral veinsbullLocated within the
transverse foramen of C1-C7
Cervical Spine Anatomy
Neural and Circulatory Elements
Torticollis
bullInfantile ndashcongenital ndash
bullCause and discription
bullClinical feature
DDXX-ray
Treatment
bullSecondary torticollis
bull
Prolapsed Intervertebral Discs
Introduction
bull Male predominance
bull 30 ndash 50 yrs
bull Smokers
bull Sudden flexionamp Twisting
bullFUNCTION OF SPINE
bullndashCombination of stability and
bullmobility due to 2 types of joints
bull1048708Facet Joints
bull1048708Intervertebral disc
bullTYPES OF JOINTSbullA- Facet joint- Typical (Diathrodial)
bull1048708 Lined with synovial membrane
bull1048708 Minimal resistance to movemetns
bullB- IVD
bulllining
bull1048708 Disc- Bears load associated with erect
bullpostur
bull1048708 Allows movements between hellip Bodies
bullANATOMY OF
bullINTERVERTEBRAL DISC
bull1 -Annulus- concentric laminae of collagen
bullfibrils
bull ndashOutermost ndash Sharpey fibers attached to bone
bullTough - type I collagen
bull ndashInner ndash less tough ndash type II collagen
bull2 -Nucleus pulposus
bullonly type II collagen
Nerve root
bull Medial amp inferior to the pedicle at
each level
bull More susceptiple for mechanical
deformation
--lack an epineurium
--reduced collagen content
--more parallel orientation of nfibres
fig
Pathology
bull Normal aging
bull -disc degeneration-displacement of facet joint
bull -acute disc herneation-pain
bull -2ndary effect-aquired SS
---Effects of pressure on the nerve root
Pathophysiology bull Effects of pressure on the nerve root
-Compressive
bull -Deformation-stramp funchanges
Classification
bull A-Site5-66-7
bull B-Direction posterolat
bull C-Amount
---Bulge
--Herniation
1-Protrusion
2-extrusion
3- sequestration
Effects of prolapse
Clinical picture
bullPressure on Dura
bullPressure on root
bullPressure on cord
bullMixed
Imagingbull X-raybull MRIbull CT scans with or without myelography -intolerant to MRI -Unsuitable for MRIbull gadolinium-enhanced MRI This will help to delineate which part of the
previous operation site is disc and which is epidural fibrosis (the latter enhancing)
DDX
bullAcute muscularampST strain
bullNeuralgic amyatrophy
bull Infection
Tumor
bullRotator cuff syndrome
Treatmentbull usually have a good prognosis
bull In up to four-fifths of patients symptoms
will resolve spontaneously within a 12-week
period
bull However if pain persists beyond this time
there is a slow resolution of pain in the
majority of patients
bull By approximately 4 years there is no difference in the incidence of pain in
patients treated non-operatively or surgically
bull Surgical results will deteriorate after
symptoms have been present for 1
year
Non-operative treatment
bull ANALGESICSampANTIINFLAMATORY
bull REST-collar
bull Reduce-traction
bull
Indications for diskectomybull Strong indications for surgical intervention
-Acute mylopathy or myloradiculopathy
-Progressive Neurological deficit
bull Relative indications
bull Failure of conservative treatment-refractory
bull Significant motor deficit
bull Severe incapacitating pain - does not respond to any form of treatment
surgical treatment--ANTERIOR OPEN APPROACH
--POSTERIOR OPEN APPROACH
--Microdisectomy
--Chemonucleolysis
--percutanious
Complications
1--Approach relatedbull 2--mechanical intraopbull 3-early postop wound infectionsDiscitis bull Haematoma-Airway obsbull 4-late postop-Non-union-Instability-deformity

Cervical Spine Anatomy
bullThe odontoid process of the axis (C2) extends
cranially to form the axis of rotation with atlas (C1)
Cervical Spine Anatomy
bullLigamentsndashThe cervical spine also
features a complex arrangement of ligaments to supplement its structure and
mobility
Cervical Spine Anatomy
bullLigamentsndashAnterior longitudinal
ligament
ndashPosterior longitudinal ligament
ndashLigamentum flavum
ndashIntertransverse ligaments
ndashInterspinous ligaments
ndashLigamentum nuchae
Cervical Spine Anatomy
bullLigamentsndashAnterior longitudinal
ligament
ndashPosterior longitudinal ligament
ndashLigamentum flavum
ndashIntertransverse ligaments
ndashInterspinous ligaments
ndashLigamentum nuchae
Cervical Spine Anatomy
bullLigamentsndashAnterior longitudinal
ligament
ndashPosterior longitudinal ligament
ndashLigamentum flavum
ndashIntertransverse ligaments
ndashInterspinous ligaments
ndashLigamentum nuchae
Cervical Spine Anatomy
bullLigamentsndashAnterior longitudinal
ligament
ndashPosterior longitudinal ligament
ndashLigamentum flavum
ndashIntertransverse ligaments
ndashInterspinous ligaments
ndashLigamentum nuchae
Cervical Spine Anatomy
bullLigamentsndashAnterior longitudinal
ligament
ndashPosterior longitudinal ligament
ndashLigamentum flavum
ndashIntertransverse ligaments
ndashInterspinous ligaments
ndashLigamentum nuchae
Cervical Spine Anatomy
bullLigamentsndashAnterior longitudinal
ligament
ndashPosterior longitudinal ligament
ndashLigamentum flavum
ndashIntertransverse ligaments
ndashInterspinous ligaments
ndashLigamentum nuchae
Cervical Spine Anatomy
bull Neural elementsndash8 pair of cervical nervesndashExit the spinal canal
superior to the vertebrae for which they are
numberedbullC1 nerves exit the canal
between Occ amp C1bullC2 nerves exit the canal
between C1 amp C2bullC8 nerves exit the canal
between C7 amp T1
Cervical Spine Anatomy
bull ArteriesndashCarotid arteries
bullLocated anterior and bilateral to the spine
ndashVertebral arteriesbullEnter the transverse
foramen at C6 and continue through C1
Cervical Spine Anatomy
bull VeinsndashJugular veins
bullLocated bilateral and anterior to the spine
ndashVertebral veinsbullLocated within the
transverse foramen of C1-C7
Cervical Spine Anatomy
Neural and Circulatory Elements
Torticollis
bullInfantile ndashcongenital ndash
bullCause and discription
bullClinical feature
DDXX-ray
Treatment
bullSecondary torticollis
bull
Prolapsed Intervertebral Discs
Introduction
bull Male predominance
bull 30 ndash 50 yrs
bull Smokers
bull Sudden flexionamp Twisting
bullFUNCTION OF SPINE
bullndashCombination of stability and
bullmobility due to 2 types of joints
bull1048708Facet Joints
bull1048708Intervertebral disc
bullTYPES OF JOINTSbullA- Facet joint- Typical (Diathrodial)
bull1048708 Lined with synovial membrane
bull1048708 Minimal resistance to movemetns
bullB- IVD
bulllining
bull1048708 Disc- Bears load associated with erect
bullpostur
bull1048708 Allows movements between hellip Bodies
bullANATOMY OF
bullINTERVERTEBRAL DISC
bull1 -Annulus- concentric laminae of collagen
bullfibrils
bull ndashOutermost ndash Sharpey fibers attached to bone
bullTough - type I collagen
bull ndashInner ndash less tough ndash type II collagen
bull2 -Nucleus pulposus
bullonly type II collagen
Nerve root
bull Medial amp inferior to the pedicle at
each level
bull More susceptiple for mechanical
deformation
--lack an epineurium
--reduced collagen content
--more parallel orientation of nfibres
fig
Pathology
bull Normal aging
bull -disc degeneration-displacement of facet joint
bull -acute disc herneation-pain
bull -2ndary effect-aquired SS
---Effects of pressure on the nerve root
Pathophysiology bull Effects of pressure on the nerve root
-Compressive
bull -Deformation-stramp funchanges
Classification
bull A-Site5-66-7
bull B-Direction posterolat
bull C-Amount
---Bulge
--Herniation
1-Protrusion
2-extrusion
3- sequestration
Effects of prolapse
Clinical picture
bullPressure on Dura
bullPressure on root
bullPressure on cord
bullMixed
Imagingbull X-raybull MRIbull CT scans with or without myelography -intolerant to MRI -Unsuitable for MRIbull gadolinium-enhanced MRI This will help to delineate which part of the
previous operation site is disc and which is epidural fibrosis (the latter enhancing)
DDX
bullAcute muscularampST strain
bullNeuralgic amyatrophy
bull Infection
Tumor
bullRotator cuff syndrome
Treatmentbull usually have a good prognosis
bull In up to four-fifths of patients symptoms
will resolve spontaneously within a 12-week
period
bull However if pain persists beyond this time
there is a slow resolution of pain in the
majority of patients
bull By approximately 4 years there is no difference in the incidence of pain in
patients treated non-operatively or surgically
bull Surgical results will deteriorate after
symptoms have been present for 1
year
Non-operative treatment
bull ANALGESICSampANTIINFLAMATORY
bull REST-collar
bull Reduce-traction
bull
Indications for diskectomybull Strong indications for surgical intervention
-Acute mylopathy or myloradiculopathy
-Progressive Neurological deficit
bull Relative indications
bull Failure of conservative treatment-refractory
bull Significant motor deficit
bull Severe incapacitating pain - does not respond to any form of treatment
surgical treatment--ANTERIOR OPEN APPROACH
--POSTERIOR OPEN APPROACH
--Microdisectomy
--Chemonucleolysis
--percutanious
Complications
1--Approach relatedbull 2--mechanical intraopbull 3-early postop wound infectionsDiscitis bull Haematoma-Airway obsbull 4-late postop-Non-union-Instability-deformity

Cervical Spine Anatomy
bullLigamentsndashThe cervical spine also
features a complex arrangement of ligaments to supplement its structure and
mobility
Cervical Spine Anatomy
bullLigamentsndashAnterior longitudinal
ligament
ndashPosterior longitudinal ligament
ndashLigamentum flavum
ndashIntertransverse ligaments
ndashInterspinous ligaments
ndashLigamentum nuchae
Cervical Spine Anatomy
bullLigamentsndashAnterior longitudinal
ligament
ndashPosterior longitudinal ligament
ndashLigamentum flavum
ndashIntertransverse ligaments
ndashInterspinous ligaments
ndashLigamentum nuchae
Cervical Spine Anatomy
bullLigamentsndashAnterior longitudinal
ligament
ndashPosterior longitudinal ligament
ndashLigamentum flavum
ndashIntertransverse ligaments
ndashInterspinous ligaments
ndashLigamentum nuchae
Cervical Spine Anatomy
bullLigamentsndashAnterior longitudinal
ligament
ndashPosterior longitudinal ligament
ndashLigamentum flavum
ndashIntertransverse ligaments
ndashInterspinous ligaments
ndashLigamentum nuchae
Cervical Spine Anatomy
bullLigamentsndashAnterior longitudinal
ligament
ndashPosterior longitudinal ligament
ndashLigamentum flavum
ndashIntertransverse ligaments
ndashInterspinous ligaments
ndashLigamentum nuchae
Cervical Spine Anatomy
bullLigamentsndashAnterior longitudinal
ligament
ndashPosterior longitudinal ligament
ndashLigamentum flavum
ndashIntertransverse ligaments
ndashInterspinous ligaments
ndashLigamentum nuchae
Cervical Spine Anatomy
bull Neural elementsndash8 pair of cervical nervesndashExit the spinal canal
superior to the vertebrae for which they are
numberedbullC1 nerves exit the canal
between Occ amp C1bullC2 nerves exit the canal
between C1 amp C2bullC8 nerves exit the canal
between C7 amp T1
Cervical Spine Anatomy
bull ArteriesndashCarotid arteries
bullLocated anterior and bilateral to the spine
ndashVertebral arteriesbullEnter the transverse
foramen at C6 and continue through C1
Cervical Spine Anatomy
bull VeinsndashJugular veins
bullLocated bilateral and anterior to the spine
ndashVertebral veinsbullLocated within the
transverse foramen of C1-C7
Cervical Spine Anatomy
Neural and Circulatory Elements
Torticollis
bullInfantile ndashcongenital ndash
bullCause and discription
bullClinical feature
DDXX-ray
Treatment
bullSecondary torticollis
bull
Prolapsed Intervertebral Discs
Introduction
bull Male predominance
bull 30 ndash 50 yrs
bull Smokers
bull Sudden flexionamp Twisting
bullFUNCTION OF SPINE
bullndashCombination of stability and
bullmobility due to 2 types of joints
bull1048708Facet Joints
bull1048708Intervertebral disc
bullTYPES OF JOINTSbullA- Facet joint- Typical (Diathrodial)
bull1048708 Lined with synovial membrane
bull1048708 Minimal resistance to movemetns
bullB- IVD
bulllining
bull1048708 Disc- Bears load associated with erect
bullpostur
bull1048708 Allows movements between hellip Bodies
bullANATOMY OF
bullINTERVERTEBRAL DISC
bull1 -Annulus- concentric laminae of collagen
bullfibrils
bull ndashOutermost ndash Sharpey fibers attached to bone
bullTough - type I collagen
bull ndashInner ndash less tough ndash type II collagen
bull2 -Nucleus pulposus
bullonly type II collagen
Nerve root
bull Medial amp inferior to the pedicle at
each level
bull More susceptiple for mechanical
deformation
--lack an epineurium
--reduced collagen content
--more parallel orientation of nfibres
fig
Pathology
bull Normal aging
bull -disc degeneration-displacement of facet joint
bull -acute disc herneation-pain
bull -2ndary effect-aquired SS
---Effects of pressure on the nerve root
Pathophysiology bull Effects of pressure on the nerve root
-Compressive
bull -Deformation-stramp funchanges
Classification
bull A-Site5-66-7
bull B-Direction posterolat
bull C-Amount
---Bulge
--Herniation
1-Protrusion
2-extrusion
3- sequestration
Effects of prolapse
Clinical picture
bullPressure on Dura
bullPressure on root
bullPressure on cord
bullMixed
Imagingbull X-raybull MRIbull CT scans with or without myelography -intolerant to MRI -Unsuitable for MRIbull gadolinium-enhanced MRI This will help to delineate which part of the
previous operation site is disc and which is epidural fibrosis (the latter enhancing)
DDX
bullAcute muscularampST strain
bullNeuralgic amyatrophy
bull Infection
Tumor
bullRotator cuff syndrome
Treatmentbull usually have a good prognosis
bull In up to four-fifths of patients symptoms
will resolve spontaneously within a 12-week
period
bull However if pain persists beyond this time
there is a slow resolution of pain in the
majority of patients
bull By approximately 4 years there is no difference in the incidence of pain in
patients treated non-operatively or surgically
bull Surgical results will deteriorate after
symptoms have been present for 1
year
Non-operative treatment
bull ANALGESICSampANTIINFLAMATORY
bull REST-collar
bull Reduce-traction
bull
Indications for diskectomybull Strong indications for surgical intervention
-Acute mylopathy or myloradiculopathy
-Progressive Neurological deficit
bull Relative indications
bull Failure of conservative treatment-refractory
bull Significant motor deficit
bull Severe incapacitating pain - does not respond to any form of treatment
surgical treatment--ANTERIOR OPEN APPROACH
--POSTERIOR OPEN APPROACH
--Microdisectomy
--Chemonucleolysis
--percutanious
Complications
1--Approach relatedbull 2--mechanical intraopbull 3-early postop wound infectionsDiscitis bull Haematoma-Airway obsbull 4-late postop-Non-union-Instability-deformity

Cervical Spine Anatomy
bullLigamentsndashAnterior longitudinal
ligament
ndashPosterior longitudinal ligament
ndashLigamentum flavum
ndashIntertransverse ligaments
ndashInterspinous ligaments
ndashLigamentum nuchae
Cervical Spine Anatomy
bullLigamentsndashAnterior longitudinal
ligament
ndashPosterior longitudinal ligament
ndashLigamentum flavum
ndashIntertransverse ligaments
ndashInterspinous ligaments
ndashLigamentum nuchae
Cervical Spine Anatomy
bullLigamentsndashAnterior longitudinal
ligament
ndashPosterior longitudinal ligament
ndashLigamentum flavum
ndashIntertransverse ligaments
ndashInterspinous ligaments
ndashLigamentum nuchae
Cervical Spine Anatomy
bullLigamentsndashAnterior longitudinal
ligament
ndashPosterior longitudinal ligament
ndashLigamentum flavum
ndashIntertransverse ligaments
ndashInterspinous ligaments
ndashLigamentum nuchae
Cervical Spine Anatomy
bullLigamentsndashAnterior longitudinal
ligament
ndashPosterior longitudinal ligament
ndashLigamentum flavum
ndashIntertransverse ligaments
ndashInterspinous ligaments
ndashLigamentum nuchae
Cervical Spine Anatomy
bullLigamentsndashAnterior longitudinal
ligament
ndashPosterior longitudinal ligament
ndashLigamentum flavum
ndashIntertransverse ligaments
ndashInterspinous ligaments
ndashLigamentum nuchae
Cervical Spine Anatomy
bull Neural elementsndash8 pair of cervical nervesndashExit the spinal canal
superior to the vertebrae for which they are
numberedbullC1 nerves exit the canal
between Occ amp C1bullC2 nerves exit the canal
between C1 amp C2bullC8 nerves exit the canal
between C7 amp T1
Cervical Spine Anatomy
bull ArteriesndashCarotid arteries
bullLocated anterior and bilateral to the spine
ndashVertebral arteriesbullEnter the transverse
foramen at C6 and continue through C1
Cervical Spine Anatomy
bull VeinsndashJugular veins
bullLocated bilateral and anterior to the spine
ndashVertebral veinsbullLocated within the
transverse foramen of C1-C7
Cervical Spine Anatomy
Neural and Circulatory Elements
Torticollis
bullInfantile ndashcongenital ndash
bullCause and discription
bullClinical feature
DDXX-ray
Treatment
bullSecondary torticollis
bull
Prolapsed Intervertebral Discs
Introduction
bull Male predominance
bull 30 ndash 50 yrs
bull Smokers
bull Sudden flexionamp Twisting
bullFUNCTION OF SPINE
bullndashCombination of stability and
bullmobility due to 2 types of joints
bull1048708Facet Joints
bull1048708Intervertebral disc
bullTYPES OF JOINTSbullA- Facet joint- Typical (Diathrodial)
bull1048708 Lined with synovial membrane
bull1048708 Minimal resistance to movemetns
bullB- IVD
bulllining
bull1048708 Disc- Bears load associated with erect
bullpostur
bull1048708 Allows movements between hellip Bodies
bullANATOMY OF
bullINTERVERTEBRAL DISC
bull1 -Annulus- concentric laminae of collagen
bullfibrils
bull ndashOutermost ndash Sharpey fibers attached to bone
bullTough - type I collagen
bull ndashInner ndash less tough ndash type II collagen
bull2 -Nucleus pulposus
bullonly type II collagen
Nerve root
bull Medial amp inferior to the pedicle at
each level
bull More susceptiple for mechanical
deformation
--lack an epineurium
--reduced collagen content
--more parallel orientation of nfibres
fig
Pathology
bull Normal aging
bull -disc degeneration-displacement of facet joint
bull -acute disc herneation-pain
bull -2ndary effect-aquired SS
---Effects of pressure on the nerve root
Pathophysiology bull Effects of pressure on the nerve root
-Compressive
bull -Deformation-stramp funchanges
Classification
bull A-Site5-66-7
bull B-Direction posterolat
bull C-Amount
---Bulge
--Herniation
1-Protrusion
2-extrusion
3- sequestration
Effects of prolapse
Clinical picture
bullPressure on Dura
bullPressure on root
bullPressure on cord
bullMixed
Imagingbull X-raybull MRIbull CT scans with or without myelography -intolerant to MRI -Unsuitable for MRIbull gadolinium-enhanced MRI This will help to delineate which part of the
previous operation site is disc and which is epidural fibrosis (the latter enhancing)
DDX
bullAcute muscularampST strain
bullNeuralgic amyatrophy
bull Infection
Tumor
bullRotator cuff syndrome
Treatmentbull usually have a good prognosis
bull In up to four-fifths of patients symptoms
will resolve spontaneously within a 12-week
period
bull However if pain persists beyond this time
there is a slow resolution of pain in the
majority of patients
bull By approximately 4 years there is no difference in the incidence of pain in
patients treated non-operatively or surgically
bull Surgical results will deteriorate after
symptoms have been present for 1
year
Non-operative treatment
bull ANALGESICSampANTIINFLAMATORY
bull REST-collar
bull Reduce-traction
bull
Indications for diskectomybull Strong indications for surgical intervention
-Acute mylopathy or myloradiculopathy
-Progressive Neurological deficit
bull Relative indications
bull Failure of conservative treatment-refractory
bull Significant motor deficit
bull Severe incapacitating pain - does not respond to any form of treatment
surgical treatment--ANTERIOR OPEN APPROACH
--POSTERIOR OPEN APPROACH
--Microdisectomy
--Chemonucleolysis
--percutanious
Complications
1--Approach relatedbull 2--mechanical intraopbull 3-early postop wound infectionsDiscitis bull Haematoma-Airway obsbull 4-late postop-Non-union-Instability-deformity

Cervical Spine Anatomy
bullLigamentsndashAnterior longitudinal
ligament
ndashPosterior longitudinal ligament
ndashLigamentum flavum
ndashIntertransverse ligaments
ndashInterspinous ligaments
ndashLigamentum nuchae
Cervical Spine Anatomy
bullLigamentsndashAnterior longitudinal
ligament
ndashPosterior longitudinal ligament
ndashLigamentum flavum
ndashIntertransverse ligaments
ndashInterspinous ligaments
ndashLigamentum nuchae
Cervical Spine Anatomy
bullLigamentsndashAnterior longitudinal
ligament
ndashPosterior longitudinal ligament
ndashLigamentum flavum
ndashIntertransverse ligaments
ndashInterspinous ligaments
ndashLigamentum nuchae
Cervical Spine Anatomy
bullLigamentsndashAnterior longitudinal
ligament
ndashPosterior longitudinal ligament
ndashLigamentum flavum
ndashIntertransverse ligaments
ndashInterspinous ligaments
ndashLigamentum nuchae
Cervical Spine Anatomy
bullLigamentsndashAnterior longitudinal
ligament
ndashPosterior longitudinal ligament
ndashLigamentum flavum
ndashIntertransverse ligaments
ndashInterspinous ligaments
ndashLigamentum nuchae
Cervical Spine Anatomy
bull Neural elementsndash8 pair of cervical nervesndashExit the spinal canal
superior to the vertebrae for which they are
numberedbullC1 nerves exit the canal
between Occ amp C1bullC2 nerves exit the canal
between C1 amp C2bullC8 nerves exit the canal
between C7 amp T1
Cervical Spine Anatomy
bull ArteriesndashCarotid arteries
bullLocated anterior and bilateral to the spine
ndashVertebral arteriesbullEnter the transverse
foramen at C6 and continue through C1
Cervical Spine Anatomy
bull VeinsndashJugular veins
bullLocated bilateral and anterior to the spine
ndashVertebral veinsbullLocated within the
transverse foramen of C1-C7
Cervical Spine Anatomy
Neural and Circulatory Elements
Torticollis
bullInfantile ndashcongenital ndash
bullCause and discription
bullClinical feature
DDXX-ray
Treatment
bullSecondary torticollis
bull
Prolapsed Intervertebral Discs
Introduction
bull Male predominance
bull 30 ndash 50 yrs
bull Smokers
bull Sudden flexionamp Twisting
bullFUNCTION OF SPINE
bullndashCombination of stability and
bullmobility due to 2 types of joints
bull1048708Facet Joints
bull1048708Intervertebral disc
bullTYPES OF JOINTSbullA- Facet joint- Typical (Diathrodial)
bull1048708 Lined with synovial membrane
bull1048708 Minimal resistance to movemetns
bullB- IVD
bulllining
bull1048708 Disc- Bears load associated with erect
bullpostur
bull1048708 Allows movements between hellip Bodies
bullANATOMY OF
bullINTERVERTEBRAL DISC
bull1 -Annulus- concentric laminae of collagen
bullfibrils
bull ndashOutermost ndash Sharpey fibers attached to bone
bullTough - type I collagen
bull ndashInner ndash less tough ndash type II collagen
bull2 -Nucleus pulposus
bullonly type II collagen
Nerve root
bull Medial amp inferior to the pedicle at
each level
bull More susceptiple for mechanical
deformation
--lack an epineurium
--reduced collagen content
--more parallel orientation of nfibres
fig
Pathology
bull Normal aging
bull -disc degeneration-displacement of facet joint
bull -acute disc herneation-pain
bull -2ndary effect-aquired SS
---Effects of pressure on the nerve root
Pathophysiology bull Effects of pressure on the nerve root
-Compressive
bull -Deformation-stramp funchanges
Classification
bull A-Site5-66-7
bull B-Direction posterolat
bull C-Amount
---Bulge
--Herniation
1-Protrusion
2-extrusion
3- sequestration
Effects of prolapse
Clinical picture
bullPressure on Dura
bullPressure on root
bullPressure on cord
bullMixed
Imagingbull X-raybull MRIbull CT scans with or without myelography -intolerant to MRI -Unsuitable for MRIbull gadolinium-enhanced MRI This will help to delineate which part of the
previous operation site is disc and which is epidural fibrosis (the latter enhancing)
DDX
bullAcute muscularampST strain
bullNeuralgic amyatrophy
bull Infection
Tumor
bullRotator cuff syndrome
Treatmentbull usually have a good prognosis
bull In up to four-fifths of patients symptoms
will resolve spontaneously within a 12-week
period
bull However if pain persists beyond this time
there is a slow resolution of pain in the
majority of patients
bull By approximately 4 years there is no difference in the incidence of pain in
patients treated non-operatively or surgically
bull Surgical results will deteriorate after
symptoms have been present for 1
year
Non-operative treatment
bull ANALGESICSampANTIINFLAMATORY
bull REST-collar
bull Reduce-traction
bull
Indications for diskectomybull Strong indications for surgical intervention
-Acute mylopathy or myloradiculopathy
-Progressive Neurological deficit
bull Relative indications
bull Failure of conservative treatment-refractory
bull Significant motor deficit
bull Severe incapacitating pain - does not respond to any form of treatment
surgical treatment--ANTERIOR OPEN APPROACH
--POSTERIOR OPEN APPROACH
--Microdisectomy
--Chemonucleolysis
--percutanious
Complications
1--Approach relatedbull 2--mechanical intraopbull 3-early postop wound infectionsDiscitis bull Haematoma-Airway obsbull 4-late postop-Non-union-Instability-deformity

Cervical Spine Anatomy
bullLigamentsndashAnterior longitudinal
ligament
ndashPosterior longitudinal ligament
ndashLigamentum flavum
ndashIntertransverse ligaments
ndashInterspinous ligaments
ndashLigamentum nuchae
Cervical Spine Anatomy
bullLigamentsndashAnterior longitudinal
ligament
ndashPosterior longitudinal ligament
ndashLigamentum flavum
ndashIntertransverse ligaments
ndashInterspinous ligaments
ndashLigamentum nuchae
Cervical Spine Anatomy
bullLigamentsndashAnterior longitudinal
ligament
ndashPosterior longitudinal ligament
ndashLigamentum flavum
ndashIntertransverse ligaments
ndashInterspinous ligaments
ndashLigamentum nuchae
Cervical Spine Anatomy
bullLigamentsndashAnterior longitudinal
ligament
ndashPosterior longitudinal ligament
ndashLigamentum flavum
ndashIntertransverse ligaments
ndashInterspinous ligaments
ndashLigamentum nuchae
Cervical Spine Anatomy
bull Neural elementsndash8 pair of cervical nervesndashExit the spinal canal
superior to the vertebrae for which they are
numberedbullC1 nerves exit the canal
between Occ amp C1bullC2 nerves exit the canal
between C1 amp C2bullC8 nerves exit the canal
between C7 amp T1
Cervical Spine Anatomy
bull ArteriesndashCarotid arteries
bullLocated anterior and bilateral to the spine
ndashVertebral arteriesbullEnter the transverse
foramen at C6 and continue through C1
Cervical Spine Anatomy
bull VeinsndashJugular veins
bullLocated bilateral and anterior to the spine
ndashVertebral veinsbullLocated within the
transverse foramen of C1-C7
Cervical Spine Anatomy
Neural and Circulatory Elements
Torticollis
bullInfantile ndashcongenital ndash
bullCause and discription
bullClinical feature
DDXX-ray
Treatment
bullSecondary torticollis
bull
Prolapsed Intervertebral Discs
Introduction
bull Male predominance
bull 30 ndash 50 yrs
bull Smokers
bull Sudden flexionamp Twisting
bullFUNCTION OF SPINE
bullndashCombination of stability and
bullmobility due to 2 types of joints
bull1048708Facet Joints
bull1048708Intervertebral disc
bullTYPES OF JOINTSbullA- Facet joint- Typical (Diathrodial)
bull1048708 Lined with synovial membrane
bull1048708 Minimal resistance to movemetns
bullB- IVD
bulllining
bull1048708 Disc- Bears load associated with erect
bullpostur
bull1048708 Allows movements between hellip Bodies
bullANATOMY OF
bullINTERVERTEBRAL DISC
bull1 -Annulus- concentric laminae of collagen
bullfibrils
bull ndashOutermost ndash Sharpey fibers attached to bone
bullTough - type I collagen
bull ndashInner ndash less tough ndash type II collagen
bull2 -Nucleus pulposus
bullonly type II collagen
Nerve root
bull Medial amp inferior to the pedicle at
each level
bull More susceptiple for mechanical
deformation
--lack an epineurium
--reduced collagen content
--more parallel orientation of nfibres
fig
Pathology
bull Normal aging
bull -disc degeneration-displacement of facet joint
bull -acute disc herneation-pain
bull -2ndary effect-aquired SS
---Effects of pressure on the nerve root
Pathophysiology bull Effects of pressure on the nerve root
-Compressive
bull -Deformation-stramp funchanges
Classification
bull A-Site5-66-7
bull B-Direction posterolat
bull C-Amount
---Bulge
--Herniation
1-Protrusion
2-extrusion
3- sequestration
Effects of prolapse
Clinical picture
bullPressure on Dura
bullPressure on root
bullPressure on cord
bullMixed
Imagingbull X-raybull MRIbull CT scans with or without myelography -intolerant to MRI -Unsuitable for MRIbull gadolinium-enhanced MRI This will help to delineate which part of the
previous operation site is disc and which is epidural fibrosis (the latter enhancing)
DDX
bullAcute muscularampST strain
bullNeuralgic amyatrophy
bull Infection
Tumor
bullRotator cuff syndrome
Treatmentbull usually have a good prognosis
bull In up to four-fifths of patients symptoms
will resolve spontaneously within a 12-week
period
bull However if pain persists beyond this time
there is a slow resolution of pain in the
majority of patients
bull By approximately 4 years there is no difference in the incidence of pain in
patients treated non-operatively or surgically
bull Surgical results will deteriorate after
symptoms have been present for 1
year
Non-operative treatment
bull ANALGESICSampANTIINFLAMATORY
bull REST-collar
bull Reduce-traction
bull
Indications for diskectomybull Strong indications for surgical intervention
-Acute mylopathy or myloradiculopathy
-Progressive Neurological deficit
bull Relative indications
bull Failure of conservative treatment-refractory
bull Significant motor deficit
bull Severe incapacitating pain - does not respond to any form of treatment
surgical treatment--ANTERIOR OPEN APPROACH
--POSTERIOR OPEN APPROACH
--Microdisectomy
--Chemonucleolysis
--percutanious
Complications
1--Approach relatedbull 2--mechanical intraopbull 3-early postop wound infectionsDiscitis bull Haematoma-Airway obsbull 4-late postop-Non-union-Instability-deformity

Cervical Spine Anatomy
bullLigamentsndashAnterior longitudinal
ligament
ndashPosterior longitudinal ligament
ndashLigamentum flavum
ndashIntertransverse ligaments
ndashInterspinous ligaments
ndashLigamentum nuchae
Cervical Spine Anatomy
bullLigamentsndashAnterior longitudinal
ligament
ndashPosterior longitudinal ligament
ndashLigamentum flavum
ndashIntertransverse ligaments
ndashInterspinous ligaments
ndashLigamentum nuchae
Cervical Spine Anatomy
bullLigamentsndashAnterior longitudinal
ligament
ndashPosterior longitudinal ligament
ndashLigamentum flavum
ndashIntertransverse ligaments
ndashInterspinous ligaments
ndashLigamentum nuchae
Cervical Spine Anatomy
bull Neural elementsndash8 pair of cervical nervesndashExit the spinal canal
superior to the vertebrae for which they are
numberedbullC1 nerves exit the canal
between Occ amp C1bullC2 nerves exit the canal
between C1 amp C2bullC8 nerves exit the canal
between C7 amp T1
Cervical Spine Anatomy
bull ArteriesndashCarotid arteries
bullLocated anterior and bilateral to the spine
ndashVertebral arteriesbullEnter the transverse
foramen at C6 and continue through C1
Cervical Spine Anatomy
bull VeinsndashJugular veins
bullLocated bilateral and anterior to the spine
ndashVertebral veinsbullLocated within the
transverse foramen of C1-C7
Cervical Spine Anatomy
Neural and Circulatory Elements
Torticollis
bullInfantile ndashcongenital ndash
bullCause and discription
bullClinical feature
DDXX-ray
Treatment
bullSecondary torticollis
bull
Prolapsed Intervertebral Discs
Introduction
bull Male predominance
bull 30 ndash 50 yrs
bull Smokers
bull Sudden flexionamp Twisting
bullFUNCTION OF SPINE
bullndashCombination of stability and
bullmobility due to 2 types of joints
bull1048708Facet Joints
bull1048708Intervertebral disc
bullTYPES OF JOINTSbullA- Facet joint- Typical (Diathrodial)
bull1048708 Lined with synovial membrane
bull1048708 Minimal resistance to movemetns
bullB- IVD
bulllining
bull1048708 Disc- Bears load associated with erect
bullpostur
bull1048708 Allows movements between hellip Bodies
bullANATOMY OF
bullINTERVERTEBRAL DISC
bull1 -Annulus- concentric laminae of collagen
bullfibrils
bull ndashOutermost ndash Sharpey fibers attached to bone
bullTough - type I collagen
bull ndashInner ndash less tough ndash type II collagen
bull2 -Nucleus pulposus
bullonly type II collagen
Nerve root
bull Medial amp inferior to the pedicle at
each level
bull More susceptiple for mechanical
deformation
--lack an epineurium
--reduced collagen content
--more parallel orientation of nfibres
fig
Pathology
bull Normal aging
bull -disc degeneration-displacement of facet joint
bull -acute disc herneation-pain
bull -2ndary effect-aquired SS
---Effects of pressure on the nerve root
Pathophysiology bull Effects of pressure on the nerve root
-Compressive
bull -Deformation-stramp funchanges
Classification
bull A-Site5-66-7
bull B-Direction posterolat
bull C-Amount
---Bulge
--Herniation
1-Protrusion
2-extrusion
3- sequestration
Effects of prolapse
Clinical picture
bullPressure on Dura
bullPressure on root
bullPressure on cord
bullMixed
Imagingbull X-raybull MRIbull CT scans with or without myelography -intolerant to MRI -Unsuitable for MRIbull gadolinium-enhanced MRI This will help to delineate which part of the
previous operation site is disc and which is epidural fibrosis (the latter enhancing)
DDX
bullAcute muscularampST strain
bullNeuralgic amyatrophy
bull Infection
Tumor
bullRotator cuff syndrome
Treatmentbull usually have a good prognosis
bull In up to four-fifths of patients symptoms
will resolve spontaneously within a 12-week
period
bull However if pain persists beyond this time
there is a slow resolution of pain in the
majority of patients
bull By approximately 4 years there is no difference in the incidence of pain in
patients treated non-operatively or surgically
bull Surgical results will deteriorate after
symptoms have been present for 1
year
Non-operative treatment
bull ANALGESICSampANTIINFLAMATORY
bull REST-collar
bull Reduce-traction
bull
Indications for diskectomybull Strong indications for surgical intervention
-Acute mylopathy or myloradiculopathy
-Progressive Neurological deficit
bull Relative indications
bull Failure of conservative treatment-refractory
bull Significant motor deficit
bull Severe incapacitating pain - does not respond to any form of treatment
surgical treatment--ANTERIOR OPEN APPROACH
--POSTERIOR OPEN APPROACH
--Microdisectomy
--Chemonucleolysis
--percutanious
Complications
1--Approach relatedbull 2--mechanical intraopbull 3-early postop wound infectionsDiscitis bull Haematoma-Airway obsbull 4-late postop-Non-union-Instability-deformity

Cervical Spine Anatomy
bullLigamentsndashAnterior longitudinal
ligament
ndashPosterior longitudinal ligament
ndashLigamentum flavum
ndashIntertransverse ligaments
ndashInterspinous ligaments
ndashLigamentum nuchae
Cervical Spine Anatomy
bullLigamentsndashAnterior longitudinal
ligament
ndashPosterior longitudinal ligament
ndashLigamentum flavum
ndashIntertransverse ligaments
ndashInterspinous ligaments
ndashLigamentum nuchae
Cervical Spine Anatomy
bull Neural elementsndash8 pair of cervical nervesndashExit the spinal canal
superior to the vertebrae for which they are
numberedbullC1 nerves exit the canal
between Occ amp C1bullC2 nerves exit the canal
between C1 amp C2bullC8 nerves exit the canal
between C7 amp T1
Cervical Spine Anatomy
bull ArteriesndashCarotid arteries
bullLocated anterior and bilateral to the spine
ndashVertebral arteriesbullEnter the transverse
foramen at C6 and continue through C1
Cervical Spine Anatomy
bull VeinsndashJugular veins
bullLocated bilateral and anterior to the spine
ndashVertebral veinsbullLocated within the
transverse foramen of C1-C7
Cervical Spine Anatomy
Neural and Circulatory Elements
Torticollis
bullInfantile ndashcongenital ndash
bullCause and discription
bullClinical feature
DDXX-ray
Treatment
bullSecondary torticollis
bull
Prolapsed Intervertebral Discs
Introduction
bull Male predominance
bull 30 ndash 50 yrs
bull Smokers
bull Sudden flexionamp Twisting
bullFUNCTION OF SPINE
bullndashCombination of stability and
bullmobility due to 2 types of joints
bull1048708Facet Joints
bull1048708Intervertebral disc
bullTYPES OF JOINTSbullA- Facet joint- Typical (Diathrodial)
bull1048708 Lined with synovial membrane
bull1048708 Minimal resistance to movemetns
bullB- IVD
bulllining
bull1048708 Disc- Bears load associated with erect
bullpostur
bull1048708 Allows movements between hellip Bodies
bullANATOMY OF
bullINTERVERTEBRAL DISC
bull1 -Annulus- concentric laminae of collagen
bullfibrils
bull ndashOutermost ndash Sharpey fibers attached to bone
bullTough - type I collagen
bull ndashInner ndash less tough ndash type II collagen
bull2 -Nucleus pulposus
bullonly type II collagen
Nerve root
bull Medial amp inferior to the pedicle at
each level
bull More susceptiple for mechanical
deformation
--lack an epineurium
--reduced collagen content
--more parallel orientation of nfibres
fig
Pathology
bull Normal aging
bull -disc degeneration-displacement of facet joint
bull -acute disc herneation-pain
bull -2ndary effect-aquired SS
---Effects of pressure on the nerve root
Pathophysiology bull Effects of pressure on the nerve root
-Compressive
bull -Deformation-stramp funchanges
Classification
bull A-Site5-66-7
bull B-Direction posterolat
bull C-Amount
---Bulge
--Herniation
1-Protrusion
2-extrusion
3- sequestration
Effects of prolapse
Clinical picture
bullPressure on Dura
bullPressure on root
bullPressure on cord
bullMixed
Imagingbull X-raybull MRIbull CT scans with or without myelography -intolerant to MRI -Unsuitable for MRIbull gadolinium-enhanced MRI This will help to delineate which part of the
previous operation site is disc and which is epidural fibrosis (the latter enhancing)
DDX
bullAcute muscularampST strain
bullNeuralgic amyatrophy
bull Infection
Tumor
bullRotator cuff syndrome
Treatmentbull usually have a good prognosis
bull In up to four-fifths of patients symptoms
will resolve spontaneously within a 12-week
period
bull However if pain persists beyond this time
there is a slow resolution of pain in the
majority of patients
bull By approximately 4 years there is no difference in the incidence of pain in
patients treated non-operatively or surgically
bull Surgical results will deteriorate after
symptoms have been present for 1
year
Non-operative treatment
bull ANALGESICSampANTIINFLAMATORY
bull REST-collar
bull Reduce-traction
bull
Indications for diskectomybull Strong indications for surgical intervention
-Acute mylopathy or myloradiculopathy
-Progressive Neurological deficit
bull Relative indications
bull Failure of conservative treatment-refractory
bull Significant motor deficit
bull Severe incapacitating pain - does not respond to any form of treatment
surgical treatment--ANTERIOR OPEN APPROACH
--POSTERIOR OPEN APPROACH
--Microdisectomy
--Chemonucleolysis
--percutanious
Complications
1--Approach relatedbull 2--mechanical intraopbull 3-early postop wound infectionsDiscitis bull Haematoma-Airway obsbull 4-late postop-Non-union-Instability-deformity

Cervical Spine Anatomy
bullLigamentsndashAnterior longitudinal
ligament
ndashPosterior longitudinal ligament
ndashLigamentum flavum
ndashIntertransverse ligaments
ndashInterspinous ligaments
ndashLigamentum nuchae
Cervical Spine Anatomy
bull Neural elementsndash8 pair of cervical nervesndashExit the spinal canal
superior to the vertebrae for which they are
numberedbullC1 nerves exit the canal
between Occ amp C1bullC2 nerves exit the canal
between C1 amp C2bullC8 nerves exit the canal
between C7 amp T1
Cervical Spine Anatomy
bull ArteriesndashCarotid arteries
bullLocated anterior and bilateral to the spine
ndashVertebral arteriesbullEnter the transverse
foramen at C6 and continue through C1
Cervical Spine Anatomy
bull VeinsndashJugular veins
bullLocated bilateral and anterior to the spine
ndashVertebral veinsbullLocated within the
transverse foramen of C1-C7
Cervical Spine Anatomy
Neural and Circulatory Elements
Torticollis
bullInfantile ndashcongenital ndash
bullCause and discription
bullClinical feature
DDXX-ray
Treatment
bullSecondary torticollis
bull
Prolapsed Intervertebral Discs
Introduction
bull Male predominance
bull 30 ndash 50 yrs
bull Smokers
bull Sudden flexionamp Twisting
bullFUNCTION OF SPINE
bullndashCombination of stability and
bullmobility due to 2 types of joints
bull1048708Facet Joints
bull1048708Intervertebral disc
bullTYPES OF JOINTSbullA- Facet joint- Typical (Diathrodial)
bull1048708 Lined with synovial membrane
bull1048708 Minimal resistance to movemetns
bullB- IVD
bulllining
bull1048708 Disc- Bears load associated with erect
bullpostur
bull1048708 Allows movements between hellip Bodies
bullANATOMY OF
bullINTERVERTEBRAL DISC
bull1 -Annulus- concentric laminae of collagen
bullfibrils
bull ndashOutermost ndash Sharpey fibers attached to bone
bullTough - type I collagen
bull ndashInner ndash less tough ndash type II collagen
bull2 -Nucleus pulposus
bullonly type II collagen
Nerve root
bull Medial amp inferior to the pedicle at
each level
bull More susceptiple for mechanical
deformation
--lack an epineurium
--reduced collagen content
--more parallel orientation of nfibres
fig
Pathology
bull Normal aging
bull -disc degeneration-displacement of facet joint
bull -acute disc herneation-pain
bull -2ndary effect-aquired SS
---Effects of pressure on the nerve root
Pathophysiology bull Effects of pressure on the nerve root
-Compressive
bull -Deformation-stramp funchanges
Classification
bull A-Site5-66-7
bull B-Direction posterolat
bull C-Amount
---Bulge
--Herniation
1-Protrusion
2-extrusion
3- sequestration
Effects of prolapse
Clinical picture
bullPressure on Dura
bullPressure on root
bullPressure on cord
bullMixed
Imagingbull X-raybull MRIbull CT scans with or without myelography -intolerant to MRI -Unsuitable for MRIbull gadolinium-enhanced MRI This will help to delineate which part of the
previous operation site is disc and which is epidural fibrosis (the latter enhancing)
DDX
bullAcute muscularampST strain
bullNeuralgic amyatrophy
bull Infection
Tumor
bullRotator cuff syndrome
Treatmentbull usually have a good prognosis
bull In up to four-fifths of patients symptoms
will resolve spontaneously within a 12-week
period
bull However if pain persists beyond this time
there is a slow resolution of pain in the
majority of patients
bull By approximately 4 years there is no difference in the incidence of pain in
patients treated non-operatively or surgically
bull Surgical results will deteriorate after
symptoms have been present for 1
year
Non-operative treatment
bull ANALGESICSampANTIINFLAMATORY
bull REST-collar
bull Reduce-traction
bull
Indications for diskectomybull Strong indications for surgical intervention
-Acute mylopathy or myloradiculopathy
-Progressive Neurological deficit
bull Relative indications
bull Failure of conservative treatment-refractory
bull Significant motor deficit
bull Severe incapacitating pain - does not respond to any form of treatment
surgical treatment--ANTERIOR OPEN APPROACH
--POSTERIOR OPEN APPROACH
--Microdisectomy
--Chemonucleolysis
--percutanious
Complications
1--Approach relatedbull 2--mechanical intraopbull 3-early postop wound infectionsDiscitis bull Haematoma-Airway obsbull 4-late postop-Non-union-Instability-deformity

Cervical Spine Anatomy
bull Neural elementsndash8 pair of cervical nervesndashExit the spinal canal
superior to the vertebrae for which they are
numberedbullC1 nerves exit the canal
between Occ amp C1bullC2 nerves exit the canal
between C1 amp C2bullC8 nerves exit the canal
between C7 amp T1
Cervical Spine Anatomy
bull ArteriesndashCarotid arteries
bullLocated anterior and bilateral to the spine
ndashVertebral arteriesbullEnter the transverse
foramen at C6 and continue through C1
Cervical Spine Anatomy
bull VeinsndashJugular veins
bullLocated bilateral and anterior to the spine
ndashVertebral veinsbullLocated within the
transverse foramen of C1-C7
Cervical Spine Anatomy
Neural and Circulatory Elements
Torticollis
bullInfantile ndashcongenital ndash
bullCause and discription
bullClinical feature
DDXX-ray
Treatment
bullSecondary torticollis
bull
Prolapsed Intervertebral Discs
Introduction
bull Male predominance
bull 30 ndash 50 yrs
bull Smokers
bull Sudden flexionamp Twisting
bullFUNCTION OF SPINE
bullndashCombination of stability and
bullmobility due to 2 types of joints
bull1048708Facet Joints
bull1048708Intervertebral disc
bullTYPES OF JOINTSbullA- Facet joint- Typical (Diathrodial)
bull1048708 Lined with synovial membrane
bull1048708 Minimal resistance to movemetns
bullB- IVD
bulllining
bull1048708 Disc- Bears load associated with erect
bullpostur
bull1048708 Allows movements between hellip Bodies
bullANATOMY OF
bullINTERVERTEBRAL DISC
bull1 -Annulus- concentric laminae of collagen
bullfibrils
bull ndashOutermost ndash Sharpey fibers attached to bone
bullTough - type I collagen
bull ndashInner ndash less tough ndash type II collagen
bull2 -Nucleus pulposus
bullonly type II collagen
Nerve root
bull Medial amp inferior to the pedicle at
each level
bull More susceptiple for mechanical
deformation
--lack an epineurium
--reduced collagen content
--more parallel orientation of nfibres
fig
Pathology
bull Normal aging
bull -disc degeneration-displacement of facet joint
bull -acute disc herneation-pain
bull -2ndary effect-aquired SS
---Effects of pressure on the nerve root
Pathophysiology bull Effects of pressure on the nerve root
-Compressive
bull -Deformation-stramp funchanges
Classification
bull A-Site5-66-7
bull B-Direction posterolat
bull C-Amount
---Bulge
--Herniation
1-Protrusion
2-extrusion
3- sequestration
Effects of prolapse
Clinical picture
bullPressure on Dura
bullPressure on root
bullPressure on cord
bullMixed
Imagingbull X-raybull MRIbull CT scans with or without myelography -intolerant to MRI -Unsuitable for MRIbull gadolinium-enhanced MRI This will help to delineate which part of the
previous operation site is disc and which is epidural fibrosis (the latter enhancing)
DDX
bullAcute muscularampST strain
bullNeuralgic amyatrophy
bull Infection
Tumor
bullRotator cuff syndrome
Treatmentbull usually have a good prognosis
bull In up to four-fifths of patients symptoms
will resolve spontaneously within a 12-week
period
bull However if pain persists beyond this time
there is a slow resolution of pain in the
majority of patients
bull By approximately 4 years there is no difference in the incidence of pain in
patients treated non-operatively or surgically
bull Surgical results will deteriorate after
symptoms have been present for 1
year
Non-operative treatment
bull ANALGESICSampANTIINFLAMATORY
bull REST-collar
bull Reduce-traction
bull
Indications for diskectomybull Strong indications for surgical intervention
-Acute mylopathy or myloradiculopathy
-Progressive Neurological deficit
bull Relative indications
bull Failure of conservative treatment-refractory
bull Significant motor deficit
bull Severe incapacitating pain - does not respond to any form of treatment
surgical treatment--ANTERIOR OPEN APPROACH
--POSTERIOR OPEN APPROACH
--Microdisectomy
--Chemonucleolysis
--percutanious
Complications
1--Approach relatedbull 2--mechanical intraopbull 3-early postop wound infectionsDiscitis bull Haematoma-Airway obsbull 4-late postop-Non-union-Instability-deformity

Cervical Spine Anatomy
bull ArteriesndashCarotid arteries
bullLocated anterior and bilateral to the spine
ndashVertebral arteriesbullEnter the transverse
foramen at C6 and continue through C1
Cervical Spine Anatomy
bull VeinsndashJugular veins
bullLocated bilateral and anterior to the spine
ndashVertebral veinsbullLocated within the
transverse foramen of C1-C7
Cervical Spine Anatomy
Neural and Circulatory Elements
Torticollis
bullInfantile ndashcongenital ndash
bullCause and discription
bullClinical feature
DDXX-ray
Treatment
bullSecondary torticollis
bull
Prolapsed Intervertebral Discs
Introduction
bull Male predominance
bull 30 ndash 50 yrs
bull Smokers
bull Sudden flexionamp Twisting
bullFUNCTION OF SPINE
bullndashCombination of stability and
bullmobility due to 2 types of joints
bull1048708Facet Joints
bull1048708Intervertebral disc
bullTYPES OF JOINTSbullA- Facet joint- Typical (Diathrodial)
bull1048708 Lined with synovial membrane
bull1048708 Minimal resistance to movemetns
bullB- IVD
bulllining
bull1048708 Disc- Bears load associated with erect
bullpostur
bull1048708 Allows movements between hellip Bodies
bullANATOMY OF
bullINTERVERTEBRAL DISC
bull1 -Annulus- concentric laminae of collagen
bullfibrils
bull ndashOutermost ndash Sharpey fibers attached to bone
bullTough - type I collagen
bull ndashInner ndash less tough ndash type II collagen
bull2 -Nucleus pulposus
bullonly type II collagen
Nerve root
bull Medial amp inferior to the pedicle at
each level
bull More susceptiple for mechanical
deformation
--lack an epineurium
--reduced collagen content
--more parallel orientation of nfibres
fig
Pathology
bull Normal aging
bull -disc degeneration-displacement of facet joint
bull -acute disc herneation-pain
bull -2ndary effect-aquired SS
---Effects of pressure on the nerve root
Pathophysiology bull Effects of pressure on the nerve root
-Compressive
bull -Deformation-stramp funchanges
Classification
bull A-Site5-66-7
bull B-Direction posterolat
bull C-Amount
---Bulge
--Herniation
1-Protrusion
2-extrusion
3- sequestration
Effects of prolapse
Clinical picture
bullPressure on Dura
bullPressure on root
bullPressure on cord
bullMixed
Imagingbull X-raybull MRIbull CT scans with or without myelography -intolerant to MRI -Unsuitable for MRIbull gadolinium-enhanced MRI This will help to delineate which part of the
previous operation site is disc and which is epidural fibrosis (the latter enhancing)
DDX
bullAcute muscularampST strain
bullNeuralgic amyatrophy
bull Infection
Tumor
bullRotator cuff syndrome
Treatmentbull usually have a good prognosis
bull In up to four-fifths of patients symptoms
will resolve spontaneously within a 12-week
period
bull However if pain persists beyond this time
there is a slow resolution of pain in the
majority of patients
bull By approximately 4 years there is no difference in the incidence of pain in
patients treated non-operatively or surgically
bull Surgical results will deteriorate after
symptoms have been present for 1
year
Non-operative treatment
bull ANALGESICSampANTIINFLAMATORY
bull REST-collar
bull Reduce-traction
bull
Indications for diskectomybull Strong indications for surgical intervention
-Acute mylopathy or myloradiculopathy
-Progressive Neurological deficit
bull Relative indications
bull Failure of conservative treatment-refractory
bull Significant motor deficit
bull Severe incapacitating pain - does not respond to any form of treatment
surgical treatment--ANTERIOR OPEN APPROACH
--POSTERIOR OPEN APPROACH
--Microdisectomy
--Chemonucleolysis
--percutanious
Complications
1--Approach relatedbull 2--mechanical intraopbull 3-early postop wound infectionsDiscitis bull Haematoma-Airway obsbull 4-late postop-Non-union-Instability-deformity

Cervical Spine Anatomy
bull VeinsndashJugular veins
bullLocated bilateral and anterior to the spine
ndashVertebral veinsbullLocated within the
transverse foramen of C1-C7
Cervical Spine Anatomy
Neural and Circulatory Elements
Torticollis
bullInfantile ndashcongenital ndash
bullCause and discription
bullClinical feature
DDXX-ray
Treatment
bullSecondary torticollis
bull
Prolapsed Intervertebral Discs
Introduction
bull Male predominance
bull 30 ndash 50 yrs
bull Smokers
bull Sudden flexionamp Twisting
bullFUNCTION OF SPINE
bullndashCombination of stability and
bullmobility due to 2 types of joints
bull1048708Facet Joints
bull1048708Intervertebral disc
bullTYPES OF JOINTSbullA- Facet joint- Typical (Diathrodial)
bull1048708 Lined with synovial membrane
bull1048708 Minimal resistance to movemetns
bullB- IVD
bulllining
bull1048708 Disc- Bears load associated with erect
bullpostur
bull1048708 Allows movements between hellip Bodies
bullANATOMY OF
bullINTERVERTEBRAL DISC
bull1 -Annulus- concentric laminae of collagen
bullfibrils
bull ndashOutermost ndash Sharpey fibers attached to bone
bullTough - type I collagen
bull ndashInner ndash less tough ndash type II collagen
bull2 -Nucleus pulposus
bullonly type II collagen
Nerve root
bull Medial amp inferior to the pedicle at
each level
bull More susceptiple for mechanical
deformation
--lack an epineurium
--reduced collagen content
--more parallel orientation of nfibres
fig
Pathology
bull Normal aging
bull -disc degeneration-displacement of facet joint
bull -acute disc herneation-pain
bull -2ndary effect-aquired SS
---Effects of pressure on the nerve root
Pathophysiology bull Effects of pressure on the nerve root
-Compressive
bull -Deformation-stramp funchanges
Classification
bull A-Site5-66-7
bull B-Direction posterolat
bull C-Amount
---Bulge
--Herniation
1-Protrusion
2-extrusion
3- sequestration
Effects of prolapse
Clinical picture
bullPressure on Dura
bullPressure on root
bullPressure on cord
bullMixed
Imagingbull X-raybull MRIbull CT scans with or without myelography -intolerant to MRI -Unsuitable for MRIbull gadolinium-enhanced MRI This will help to delineate which part of the
previous operation site is disc and which is epidural fibrosis (the latter enhancing)
DDX
bullAcute muscularampST strain
bullNeuralgic amyatrophy
bull Infection
Tumor
bullRotator cuff syndrome
Treatmentbull usually have a good prognosis
bull In up to four-fifths of patients symptoms
will resolve spontaneously within a 12-week
period
bull However if pain persists beyond this time
there is a slow resolution of pain in the
majority of patients
bull By approximately 4 years there is no difference in the incidence of pain in
patients treated non-operatively or surgically
bull Surgical results will deteriorate after
symptoms have been present for 1
year
Non-operative treatment
bull ANALGESICSampANTIINFLAMATORY
bull REST-collar
bull Reduce-traction
bull
Indications for diskectomybull Strong indications for surgical intervention
-Acute mylopathy or myloradiculopathy
-Progressive Neurological deficit
bull Relative indications
bull Failure of conservative treatment-refractory
bull Significant motor deficit
bull Severe incapacitating pain - does not respond to any form of treatment
surgical treatment--ANTERIOR OPEN APPROACH
--POSTERIOR OPEN APPROACH
--Microdisectomy
--Chemonucleolysis
--percutanious
Complications
1--Approach relatedbull 2--mechanical intraopbull 3-early postop wound infectionsDiscitis bull Haematoma-Airway obsbull 4-late postop-Non-union-Instability-deformity

Cervical Spine Anatomy
Neural and Circulatory Elements
Torticollis
bullInfantile ndashcongenital ndash
bullCause and discription
bullClinical feature
DDXX-ray
Treatment
bullSecondary torticollis
bull
Prolapsed Intervertebral Discs
Introduction
bull Male predominance
bull 30 ndash 50 yrs
bull Smokers
bull Sudden flexionamp Twisting
bullFUNCTION OF SPINE
bullndashCombination of stability and
bullmobility due to 2 types of joints
bull1048708Facet Joints
bull1048708Intervertebral disc
bullTYPES OF JOINTSbullA- Facet joint- Typical (Diathrodial)
bull1048708 Lined with synovial membrane
bull1048708 Minimal resistance to movemetns
bullB- IVD
bulllining
bull1048708 Disc- Bears load associated with erect
bullpostur
bull1048708 Allows movements between hellip Bodies
bullANATOMY OF
bullINTERVERTEBRAL DISC
bull1 -Annulus- concentric laminae of collagen
bullfibrils
bull ndashOutermost ndash Sharpey fibers attached to bone
bullTough - type I collagen
bull ndashInner ndash less tough ndash type II collagen
bull2 -Nucleus pulposus
bullonly type II collagen
Nerve root
bull Medial amp inferior to the pedicle at
each level
bull More susceptiple for mechanical
deformation
--lack an epineurium
--reduced collagen content
--more parallel orientation of nfibres
fig
Pathology
bull Normal aging
bull -disc degeneration-displacement of facet joint
bull -acute disc herneation-pain
bull -2ndary effect-aquired SS
---Effects of pressure on the nerve root
Pathophysiology bull Effects of pressure on the nerve root
-Compressive
bull -Deformation-stramp funchanges
Classification
bull A-Site5-66-7
bull B-Direction posterolat
bull C-Amount
---Bulge
--Herniation
1-Protrusion
2-extrusion
3- sequestration
Effects of prolapse
Clinical picture
bullPressure on Dura
bullPressure on root
bullPressure on cord
bullMixed
Imagingbull X-raybull MRIbull CT scans with or without myelography -intolerant to MRI -Unsuitable for MRIbull gadolinium-enhanced MRI This will help to delineate which part of the
previous operation site is disc and which is epidural fibrosis (the latter enhancing)
DDX
bullAcute muscularampST strain
bullNeuralgic amyatrophy
bull Infection
Tumor
bullRotator cuff syndrome
Treatmentbull usually have a good prognosis
bull In up to four-fifths of patients symptoms
will resolve spontaneously within a 12-week
period
bull However if pain persists beyond this time
there is a slow resolution of pain in the
majority of patients
bull By approximately 4 years there is no difference in the incidence of pain in
patients treated non-operatively or surgically
bull Surgical results will deteriorate after
symptoms have been present for 1
year
Non-operative treatment
bull ANALGESICSampANTIINFLAMATORY
bull REST-collar
bull Reduce-traction
bull
Indications for diskectomybull Strong indications for surgical intervention
-Acute mylopathy or myloradiculopathy
-Progressive Neurological deficit
bull Relative indications
bull Failure of conservative treatment-refractory
bull Significant motor deficit
bull Severe incapacitating pain - does not respond to any form of treatment
surgical treatment--ANTERIOR OPEN APPROACH
--POSTERIOR OPEN APPROACH
--Microdisectomy
--Chemonucleolysis
--percutanious
Complications
1--Approach relatedbull 2--mechanical intraopbull 3-early postop wound infectionsDiscitis bull Haematoma-Airway obsbull 4-late postop-Non-union-Instability-deformity

Torticollis
bullInfantile ndashcongenital ndash
bullCause and discription
bullClinical feature
DDXX-ray
Treatment
bullSecondary torticollis
bull
Prolapsed Intervertebral Discs
Introduction
bull Male predominance
bull 30 ndash 50 yrs
bull Smokers
bull Sudden flexionamp Twisting
bullFUNCTION OF SPINE
bullndashCombination of stability and
bullmobility due to 2 types of joints
bull1048708Facet Joints
bull1048708Intervertebral disc
bullTYPES OF JOINTSbullA- Facet joint- Typical (Diathrodial)
bull1048708 Lined with synovial membrane
bull1048708 Minimal resistance to movemetns
bullB- IVD
bulllining
bull1048708 Disc- Bears load associated with erect
bullpostur
bull1048708 Allows movements between hellip Bodies
bullANATOMY OF
bullINTERVERTEBRAL DISC
bull1 -Annulus- concentric laminae of collagen
bullfibrils
bull ndashOutermost ndash Sharpey fibers attached to bone
bullTough - type I collagen
bull ndashInner ndash less tough ndash type II collagen
bull2 -Nucleus pulposus
bullonly type II collagen
Nerve root
bull Medial amp inferior to the pedicle at
each level
bull More susceptiple for mechanical
deformation
--lack an epineurium
--reduced collagen content
--more parallel orientation of nfibres
fig
Pathology
bull Normal aging
bull -disc degeneration-displacement of facet joint
bull -acute disc herneation-pain
bull -2ndary effect-aquired SS
---Effects of pressure on the nerve root
Pathophysiology bull Effects of pressure on the nerve root
-Compressive
bull -Deformation-stramp funchanges
Classification
bull A-Site5-66-7
bull B-Direction posterolat
bull C-Amount
---Bulge
--Herniation
1-Protrusion
2-extrusion
3- sequestration
Effects of prolapse
Clinical picture
bullPressure on Dura
bullPressure on root
bullPressure on cord
bullMixed
Imagingbull X-raybull MRIbull CT scans with or without myelography -intolerant to MRI -Unsuitable for MRIbull gadolinium-enhanced MRI This will help to delineate which part of the
previous operation site is disc and which is epidural fibrosis (the latter enhancing)
DDX
bullAcute muscularampST strain
bullNeuralgic amyatrophy
bull Infection
Tumor
bullRotator cuff syndrome
Treatmentbull usually have a good prognosis
bull In up to four-fifths of patients symptoms
will resolve spontaneously within a 12-week
period
bull However if pain persists beyond this time
there is a slow resolution of pain in the
majority of patients
bull By approximately 4 years there is no difference in the incidence of pain in
patients treated non-operatively or surgically
bull Surgical results will deteriorate after
symptoms have been present for 1
year
Non-operative treatment
bull ANALGESICSampANTIINFLAMATORY
bull REST-collar
bull Reduce-traction
bull
Indications for diskectomybull Strong indications for surgical intervention
-Acute mylopathy or myloradiculopathy
-Progressive Neurological deficit
bull Relative indications
bull Failure of conservative treatment-refractory
bull Significant motor deficit
bull Severe incapacitating pain - does not respond to any form of treatment
surgical treatment--ANTERIOR OPEN APPROACH
--POSTERIOR OPEN APPROACH
--Microdisectomy
--Chemonucleolysis
--percutanious
Complications
1--Approach relatedbull 2--mechanical intraopbull 3-early postop wound infectionsDiscitis bull Haematoma-Airway obsbull 4-late postop-Non-union-Instability-deformity

bullInfantile ndashcongenital ndash
bullCause and discription
bullClinical feature
DDXX-ray
Treatment
bullSecondary torticollis
bull
Prolapsed Intervertebral Discs
Introduction
bull Male predominance
bull 30 ndash 50 yrs
bull Smokers
bull Sudden flexionamp Twisting
bullFUNCTION OF SPINE
bullndashCombination of stability and
bullmobility due to 2 types of joints
bull1048708Facet Joints
bull1048708Intervertebral disc
bullTYPES OF JOINTSbullA- Facet joint- Typical (Diathrodial)
bull1048708 Lined with synovial membrane
bull1048708 Minimal resistance to movemetns
bullB- IVD
bulllining
bull1048708 Disc- Bears load associated with erect
bullpostur
bull1048708 Allows movements between hellip Bodies
bullANATOMY OF
bullINTERVERTEBRAL DISC
bull1 -Annulus- concentric laminae of collagen
bullfibrils
bull ndashOutermost ndash Sharpey fibers attached to bone
bullTough - type I collagen
bull ndashInner ndash less tough ndash type II collagen
bull2 -Nucleus pulposus
bullonly type II collagen
Nerve root
bull Medial amp inferior to the pedicle at
each level
bull More susceptiple for mechanical
deformation
--lack an epineurium
--reduced collagen content
--more parallel orientation of nfibres
fig
Pathology
bull Normal aging
bull -disc degeneration-displacement of facet joint
bull -acute disc herneation-pain
bull -2ndary effect-aquired SS
---Effects of pressure on the nerve root
Pathophysiology bull Effects of pressure on the nerve root
-Compressive
bull -Deformation-stramp funchanges
Classification
bull A-Site5-66-7
bull B-Direction posterolat
bull C-Amount
---Bulge
--Herniation
1-Protrusion
2-extrusion
3- sequestration
Effects of prolapse
Clinical picture
bullPressure on Dura
bullPressure on root
bullPressure on cord
bullMixed
Imagingbull X-raybull MRIbull CT scans with or without myelography -intolerant to MRI -Unsuitable for MRIbull gadolinium-enhanced MRI This will help to delineate which part of the
previous operation site is disc and which is epidural fibrosis (the latter enhancing)
DDX
bullAcute muscularampST strain
bullNeuralgic amyatrophy
bull Infection
Tumor
bullRotator cuff syndrome
Treatmentbull usually have a good prognosis
bull In up to four-fifths of patients symptoms
will resolve spontaneously within a 12-week
period
bull However if pain persists beyond this time
there is a slow resolution of pain in the
majority of patients
bull By approximately 4 years there is no difference in the incidence of pain in
patients treated non-operatively or surgically
bull Surgical results will deteriorate after
symptoms have been present for 1
year
Non-operative treatment
bull ANALGESICSampANTIINFLAMATORY
bull REST-collar
bull Reduce-traction
bull
Indications for diskectomybull Strong indications for surgical intervention
-Acute mylopathy or myloradiculopathy
-Progressive Neurological deficit
bull Relative indications
bull Failure of conservative treatment-refractory
bull Significant motor deficit
bull Severe incapacitating pain - does not respond to any form of treatment
surgical treatment--ANTERIOR OPEN APPROACH
--POSTERIOR OPEN APPROACH
--Microdisectomy
--Chemonucleolysis
--percutanious
Complications
1--Approach relatedbull 2--mechanical intraopbull 3-early postop wound infectionsDiscitis bull Haematoma-Airway obsbull 4-late postop-Non-union-Instability-deformity

DDXX-ray
Treatment
bullSecondary torticollis
bull
Prolapsed Intervertebral Discs
Introduction
bull Male predominance
bull 30 ndash 50 yrs
bull Smokers
bull Sudden flexionamp Twisting
bullFUNCTION OF SPINE
bullndashCombination of stability and
bullmobility due to 2 types of joints
bull1048708Facet Joints
bull1048708Intervertebral disc
bullTYPES OF JOINTSbullA- Facet joint- Typical (Diathrodial)
bull1048708 Lined with synovial membrane
bull1048708 Minimal resistance to movemetns
bullB- IVD
bulllining
bull1048708 Disc- Bears load associated with erect
bullpostur
bull1048708 Allows movements between hellip Bodies
bullANATOMY OF
bullINTERVERTEBRAL DISC
bull1 -Annulus- concentric laminae of collagen
bullfibrils
bull ndashOutermost ndash Sharpey fibers attached to bone
bullTough - type I collagen
bull ndashInner ndash less tough ndash type II collagen
bull2 -Nucleus pulposus
bullonly type II collagen
Nerve root
bull Medial amp inferior to the pedicle at
each level
bull More susceptiple for mechanical
deformation
--lack an epineurium
--reduced collagen content
--more parallel orientation of nfibres
fig
Pathology
bull Normal aging
bull -disc degeneration-displacement of facet joint
bull -acute disc herneation-pain
bull -2ndary effect-aquired SS
---Effects of pressure on the nerve root
Pathophysiology bull Effects of pressure on the nerve root
-Compressive
bull -Deformation-stramp funchanges
Classification
bull A-Site5-66-7
bull B-Direction posterolat
bull C-Amount
---Bulge
--Herniation
1-Protrusion
2-extrusion
3- sequestration
Effects of prolapse
Clinical picture
bullPressure on Dura
bullPressure on root
bullPressure on cord
bullMixed
Imagingbull X-raybull MRIbull CT scans with or without myelography -intolerant to MRI -Unsuitable for MRIbull gadolinium-enhanced MRI This will help to delineate which part of the
previous operation site is disc and which is epidural fibrosis (the latter enhancing)
DDX
bullAcute muscularampST strain
bullNeuralgic amyatrophy
bull Infection
Tumor
bullRotator cuff syndrome
Treatmentbull usually have a good prognosis
bull In up to four-fifths of patients symptoms
will resolve spontaneously within a 12-week
period
bull However if pain persists beyond this time
there is a slow resolution of pain in the
majority of patients
bull By approximately 4 years there is no difference in the incidence of pain in
patients treated non-operatively or surgically
bull Surgical results will deteriorate after
symptoms have been present for 1
year
Non-operative treatment
bull ANALGESICSampANTIINFLAMATORY
bull REST-collar
bull Reduce-traction
bull
Indications for diskectomybull Strong indications for surgical intervention
-Acute mylopathy or myloradiculopathy
-Progressive Neurological deficit
bull Relative indications
bull Failure of conservative treatment-refractory
bull Significant motor deficit
bull Severe incapacitating pain - does not respond to any form of treatment
surgical treatment--ANTERIOR OPEN APPROACH
--POSTERIOR OPEN APPROACH
--Microdisectomy
--Chemonucleolysis
--percutanious
Complications
1--Approach relatedbull 2--mechanical intraopbull 3-early postop wound infectionsDiscitis bull Haematoma-Airway obsbull 4-late postop-Non-union-Instability-deformity

Prolapsed Intervertebral Discs
Introduction
bull Male predominance
bull 30 ndash 50 yrs
bull Smokers
bull Sudden flexionamp Twisting
bullFUNCTION OF SPINE
bullndashCombination of stability and
bullmobility due to 2 types of joints
bull1048708Facet Joints
bull1048708Intervertebral disc
bullTYPES OF JOINTSbullA- Facet joint- Typical (Diathrodial)
bull1048708 Lined with synovial membrane
bull1048708 Minimal resistance to movemetns
bullB- IVD
bulllining
bull1048708 Disc- Bears load associated with erect
bullpostur
bull1048708 Allows movements between hellip Bodies
bullANATOMY OF
bullINTERVERTEBRAL DISC
bull1 -Annulus- concentric laminae of collagen
bullfibrils
bull ndashOutermost ndash Sharpey fibers attached to bone
bullTough - type I collagen
bull ndashInner ndash less tough ndash type II collagen
bull2 -Nucleus pulposus
bullonly type II collagen
Nerve root
bull Medial amp inferior to the pedicle at
each level
bull More susceptiple for mechanical
deformation
--lack an epineurium
--reduced collagen content
--more parallel orientation of nfibres
fig
Pathology
bull Normal aging
bull -disc degeneration-displacement of facet joint
bull -acute disc herneation-pain
bull -2ndary effect-aquired SS
---Effects of pressure on the nerve root
Pathophysiology bull Effects of pressure on the nerve root
-Compressive
bull -Deformation-stramp funchanges
Classification
bull A-Site5-66-7
bull B-Direction posterolat
bull C-Amount
---Bulge
--Herniation
1-Protrusion
2-extrusion
3- sequestration
Effects of prolapse
Clinical picture
bullPressure on Dura
bullPressure on root
bullPressure on cord
bullMixed
Imagingbull X-raybull MRIbull CT scans with or without myelography -intolerant to MRI -Unsuitable for MRIbull gadolinium-enhanced MRI This will help to delineate which part of the
previous operation site is disc and which is epidural fibrosis (the latter enhancing)
DDX
bullAcute muscularampST strain
bullNeuralgic amyatrophy
bull Infection
Tumor
bullRotator cuff syndrome
Treatmentbull usually have a good prognosis
bull In up to four-fifths of patients symptoms
will resolve spontaneously within a 12-week
period
bull However if pain persists beyond this time
there is a slow resolution of pain in the
majority of patients
bull By approximately 4 years there is no difference in the incidence of pain in
patients treated non-operatively or surgically
bull Surgical results will deteriorate after
symptoms have been present for 1
year
Non-operative treatment
bull ANALGESICSampANTIINFLAMATORY
bull REST-collar
bull Reduce-traction
bull
Indications for diskectomybull Strong indications for surgical intervention
-Acute mylopathy or myloradiculopathy
-Progressive Neurological deficit
bull Relative indications
bull Failure of conservative treatment-refractory
bull Significant motor deficit
bull Severe incapacitating pain - does not respond to any form of treatment
surgical treatment--ANTERIOR OPEN APPROACH
--POSTERIOR OPEN APPROACH
--Microdisectomy
--Chemonucleolysis
--percutanious
Complications
1--Approach relatedbull 2--mechanical intraopbull 3-early postop wound infectionsDiscitis bull Haematoma-Airway obsbull 4-late postop-Non-union-Instability-deformity

Introduction
bull Male predominance
bull 30 ndash 50 yrs
bull Smokers
bull Sudden flexionamp Twisting
bullFUNCTION OF SPINE
bullndashCombination of stability and
bullmobility due to 2 types of joints
bull1048708Facet Joints
bull1048708Intervertebral disc
bullTYPES OF JOINTSbullA- Facet joint- Typical (Diathrodial)
bull1048708 Lined with synovial membrane
bull1048708 Minimal resistance to movemetns
bullB- IVD
bulllining
bull1048708 Disc- Bears load associated with erect
bullpostur
bull1048708 Allows movements between hellip Bodies
bullANATOMY OF
bullINTERVERTEBRAL DISC
bull1 -Annulus- concentric laminae of collagen
bullfibrils
bull ndashOutermost ndash Sharpey fibers attached to bone
bullTough - type I collagen
bull ndashInner ndash less tough ndash type II collagen
bull2 -Nucleus pulposus
bullonly type II collagen
Nerve root
bull Medial amp inferior to the pedicle at
each level
bull More susceptiple for mechanical
deformation
--lack an epineurium
--reduced collagen content
--more parallel orientation of nfibres
fig
Pathology
bull Normal aging
bull -disc degeneration-displacement of facet joint
bull -acute disc herneation-pain
bull -2ndary effect-aquired SS
---Effects of pressure on the nerve root
Pathophysiology bull Effects of pressure on the nerve root
-Compressive
bull -Deformation-stramp funchanges
Classification
bull A-Site5-66-7
bull B-Direction posterolat
bull C-Amount
---Bulge
--Herniation
1-Protrusion
2-extrusion
3- sequestration
Effects of prolapse
Clinical picture
bullPressure on Dura
bullPressure on root
bullPressure on cord
bullMixed
Imagingbull X-raybull MRIbull CT scans with or without myelography -intolerant to MRI -Unsuitable for MRIbull gadolinium-enhanced MRI This will help to delineate which part of the
previous operation site is disc and which is epidural fibrosis (the latter enhancing)
DDX
bullAcute muscularampST strain
bullNeuralgic amyatrophy
bull Infection
Tumor
bullRotator cuff syndrome
Treatmentbull usually have a good prognosis
bull In up to four-fifths of patients symptoms
will resolve spontaneously within a 12-week
period
bull However if pain persists beyond this time
there is a slow resolution of pain in the
majority of patients
bull By approximately 4 years there is no difference in the incidence of pain in
patients treated non-operatively or surgically
bull Surgical results will deteriorate after
symptoms have been present for 1
year
Non-operative treatment
bull ANALGESICSampANTIINFLAMATORY
bull REST-collar
bull Reduce-traction
bull
Indications for diskectomybull Strong indications for surgical intervention
-Acute mylopathy or myloradiculopathy
-Progressive Neurological deficit
bull Relative indications
bull Failure of conservative treatment-refractory
bull Significant motor deficit
bull Severe incapacitating pain - does not respond to any form of treatment
surgical treatment--ANTERIOR OPEN APPROACH
--POSTERIOR OPEN APPROACH
--Microdisectomy
--Chemonucleolysis
--percutanious
Complications
1--Approach relatedbull 2--mechanical intraopbull 3-early postop wound infectionsDiscitis bull Haematoma-Airway obsbull 4-late postop-Non-union-Instability-deformity

bullFUNCTION OF SPINE
bullndashCombination of stability and
bullmobility due to 2 types of joints
bull1048708Facet Joints
bull1048708Intervertebral disc
bullTYPES OF JOINTSbullA- Facet joint- Typical (Diathrodial)
bull1048708 Lined with synovial membrane
bull1048708 Minimal resistance to movemetns
bullB- IVD
bulllining
bull1048708 Disc- Bears load associated with erect
bullpostur
bull1048708 Allows movements between hellip Bodies
bullANATOMY OF
bullINTERVERTEBRAL DISC
bull1 -Annulus- concentric laminae of collagen
bullfibrils
bull ndashOutermost ndash Sharpey fibers attached to bone
bullTough - type I collagen
bull ndashInner ndash less tough ndash type II collagen
bull2 -Nucleus pulposus
bullonly type II collagen
Nerve root
bull Medial amp inferior to the pedicle at
each level
bull More susceptiple for mechanical
deformation
--lack an epineurium
--reduced collagen content
--more parallel orientation of nfibres
fig
Pathology
bull Normal aging
bull -disc degeneration-displacement of facet joint
bull -acute disc herneation-pain
bull -2ndary effect-aquired SS
---Effects of pressure on the nerve root
Pathophysiology bull Effects of pressure on the nerve root
-Compressive
bull -Deformation-stramp funchanges
Classification
bull A-Site5-66-7
bull B-Direction posterolat
bull C-Amount
---Bulge
--Herniation
1-Protrusion
2-extrusion
3- sequestration
Effects of prolapse
Clinical picture
bullPressure on Dura
bullPressure on root
bullPressure on cord
bullMixed
Imagingbull X-raybull MRIbull CT scans with or without myelography -intolerant to MRI -Unsuitable for MRIbull gadolinium-enhanced MRI This will help to delineate which part of the
previous operation site is disc and which is epidural fibrosis (the latter enhancing)
DDX
bullAcute muscularampST strain
bullNeuralgic amyatrophy
bull Infection
Tumor
bullRotator cuff syndrome
Treatmentbull usually have a good prognosis
bull In up to four-fifths of patients symptoms
will resolve spontaneously within a 12-week
period
bull However if pain persists beyond this time
there is a slow resolution of pain in the
majority of patients
bull By approximately 4 years there is no difference in the incidence of pain in
patients treated non-operatively or surgically
bull Surgical results will deteriorate after
symptoms have been present for 1
year
Non-operative treatment
bull ANALGESICSampANTIINFLAMATORY
bull REST-collar
bull Reduce-traction
bull
Indications for diskectomybull Strong indications for surgical intervention
-Acute mylopathy or myloradiculopathy
-Progressive Neurological deficit
bull Relative indications
bull Failure of conservative treatment-refractory
bull Significant motor deficit
bull Severe incapacitating pain - does not respond to any form of treatment
surgical treatment--ANTERIOR OPEN APPROACH
--POSTERIOR OPEN APPROACH
--Microdisectomy
--Chemonucleolysis
--percutanious
Complications
1--Approach relatedbull 2--mechanical intraopbull 3-early postop wound infectionsDiscitis bull Haematoma-Airway obsbull 4-late postop-Non-union-Instability-deformity

bullTYPES OF JOINTSbullA- Facet joint- Typical (Diathrodial)
bull1048708 Lined with synovial membrane
bull1048708 Minimal resistance to movemetns
bullB- IVD
bulllining
bull1048708 Disc- Bears load associated with erect
bullpostur
bull1048708 Allows movements between hellip Bodies
bullANATOMY OF
bullINTERVERTEBRAL DISC
bull1 -Annulus- concentric laminae of collagen
bullfibrils
bull ndashOutermost ndash Sharpey fibers attached to bone
bullTough - type I collagen
bull ndashInner ndash less tough ndash type II collagen
bull2 -Nucleus pulposus
bullonly type II collagen
Nerve root
bull Medial amp inferior to the pedicle at
each level
bull More susceptiple for mechanical
deformation
--lack an epineurium
--reduced collagen content
--more parallel orientation of nfibres
fig
Pathology
bull Normal aging
bull -disc degeneration-displacement of facet joint
bull -acute disc herneation-pain
bull -2ndary effect-aquired SS
---Effects of pressure on the nerve root
Pathophysiology bull Effects of pressure on the nerve root
-Compressive
bull -Deformation-stramp funchanges
Classification
bull A-Site5-66-7
bull B-Direction posterolat
bull C-Amount
---Bulge
--Herniation
1-Protrusion
2-extrusion
3- sequestration
Effects of prolapse
Clinical picture
bullPressure on Dura
bullPressure on root
bullPressure on cord
bullMixed
Imagingbull X-raybull MRIbull CT scans with or without myelography -intolerant to MRI -Unsuitable for MRIbull gadolinium-enhanced MRI This will help to delineate which part of the
previous operation site is disc and which is epidural fibrosis (the latter enhancing)
DDX
bullAcute muscularampST strain
bullNeuralgic amyatrophy
bull Infection
Tumor
bullRotator cuff syndrome
Treatmentbull usually have a good prognosis
bull In up to four-fifths of patients symptoms
will resolve spontaneously within a 12-week
period
bull However if pain persists beyond this time
there is a slow resolution of pain in the
majority of patients
bull By approximately 4 years there is no difference in the incidence of pain in
patients treated non-operatively or surgically
bull Surgical results will deteriorate after
symptoms have been present for 1
year
Non-operative treatment
bull ANALGESICSampANTIINFLAMATORY
bull REST-collar
bull Reduce-traction
bull
Indications for diskectomybull Strong indications for surgical intervention
-Acute mylopathy or myloradiculopathy
-Progressive Neurological deficit
bull Relative indications
bull Failure of conservative treatment-refractory
bull Significant motor deficit
bull Severe incapacitating pain - does not respond to any form of treatment
surgical treatment--ANTERIOR OPEN APPROACH
--POSTERIOR OPEN APPROACH
--Microdisectomy
--Chemonucleolysis
--percutanious
Complications
1--Approach relatedbull 2--mechanical intraopbull 3-early postop wound infectionsDiscitis bull Haematoma-Airway obsbull 4-late postop-Non-union-Instability-deformity

bullANATOMY OF
bullINTERVERTEBRAL DISC
bull1 -Annulus- concentric laminae of collagen
bullfibrils
bull ndashOutermost ndash Sharpey fibers attached to bone
bullTough - type I collagen
bull ndashInner ndash less tough ndash type II collagen
bull2 -Nucleus pulposus
bullonly type II collagen
Nerve root
bull Medial amp inferior to the pedicle at
each level
bull More susceptiple for mechanical
deformation
--lack an epineurium
--reduced collagen content
--more parallel orientation of nfibres
fig
Pathology
bull Normal aging
bull -disc degeneration-displacement of facet joint
bull -acute disc herneation-pain
bull -2ndary effect-aquired SS
---Effects of pressure on the nerve root
Pathophysiology bull Effects of pressure on the nerve root
-Compressive
bull -Deformation-stramp funchanges
Classification
bull A-Site5-66-7
bull B-Direction posterolat
bull C-Amount
---Bulge
--Herniation
1-Protrusion
2-extrusion
3- sequestration
Effects of prolapse
Clinical picture
bullPressure on Dura
bullPressure on root
bullPressure on cord
bullMixed
Imagingbull X-raybull MRIbull CT scans with or without myelography -intolerant to MRI -Unsuitable for MRIbull gadolinium-enhanced MRI This will help to delineate which part of the
previous operation site is disc and which is epidural fibrosis (the latter enhancing)
DDX
bullAcute muscularampST strain
bullNeuralgic amyatrophy
bull Infection
Tumor
bullRotator cuff syndrome
Treatmentbull usually have a good prognosis
bull In up to four-fifths of patients symptoms
will resolve spontaneously within a 12-week
period
bull However if pain persists beyond this time
there is a slow resolution of pain in the
majority of patients
bull By approximately 4 years there is no difference in the incidence of pain in
patients treated non-operatively or surgically
bull Surgical results will deteriorate after
symptoms have been present for 1
year
Non-operative treatment
bull ANALGESICSampANTIINFLAMATORY
bull REST-collar
bull Reduce-traction
bull
Indications for diskectomybull Strong indications for surgical intervention
-Acute mylopathy or myloradiculopathy
-Progressive Neurological deficit
bull Relative indications
bull Failure of conservative treatment-refractory
bull Significant motor deficit
bull Severe incapacitating pain - does not respond to any form of treatment
surgical treatment--ANTERIOR OPEN APPROACH
--POSTERIOR OPEN APPROACH
--Microdisectomy
--Chemonucleolysis
--percutanious
Complications
1--Approach relatedbull 2--mechanical intraopbull 3-early postop wound infectionsDiscitis bull Haematoma-Airway obsbull 4-late postop-Non-union-Instability-deformity

Nerve root
bull Medial amp inferior to the pedicle at
each level
bull More susceptiple for mechanical
deformation
--lack an epineurium
--reduced collagen content
--more parallel orientation of nfibres
fig
Pathology
bull Normal aging
bull -disc degeneration-displacement of facet joint
bull -acute disc herneation-pain
bull -2ndary effect-aquired SS
---Effects of pressure on the nerve root
Pathophysiology bull Effects of pressure on the nerve root
-Compressive
bull -Deformation-stramp funchanges
Classification
bull A-Site5-66-7
bull B-Direction posterolat
bull C-Amount
---Bulge
--Herniation
1-Protrusion
2-extrusion
3- sequestration
Effects of prolapse
Clinical picture
bullPressure on Dura
bullPressure on root
bullPressure on cord
bullMixed
Imagingbull X-raybull MRIbull CT scans with or without myelography -intolerant to MRI -Unsuitable for MRIbull gadolinium-enhanced MRI This will help to delineate which part of the
previous operation site is disc and which is epidural fibrosis (the latter enhancing)
DDX
bullAcute muscularampST strain
bullNeuralgic amyatrophy
bull Infection
Tumor
bullRotator cuff syndrome
Treatmentbull usually have a good prognosis
bull In up to four-fifths of patients symptoms
will resolve spontaneously within a 12-week
period
bull However if pain persists beyond this time
there is a slow resolution of pain in the
majority of patients
bull By approximately 4 years there is no difference in the incidence of pain in
patients treated non-operatively or surgically
bull Surgical results will deteriorate after
symptoms have been present for 1
year
Non-operative treatment
bull ANALGESICSampANTIINFLAMATORY
bull REST-collar
bull Reduce-traction
bull
Indications for diskectomybull Strong indications for surgical intervention
-Acute mylopathy or myloradiculopathy
-Progressive Neurological deficit
bull Relative indications
bull Failure of conservative treatment-refractory
bull Significant motor deficit
bull Severe incapacitating pain - does not respond to any form of treatment
surgical treatment--ANTERIOR OPEN APPROACH
--POSTERIOR OPEN APPROACH
--Microdisectomy
--Chemonucleolysis
--percutanious
Complications
1--Approach relatedbull 2--mechanical intraopbull 3-early postop wound infectionsDiscitis bull Haematoma-Airway obsbull 4-late postop-Non-union-Instability-deformity

fig
Pathology
bull Normal aging
bull -disc degeneration-displacement of facet joint
bull -acute disc herneation-pain
bull -2ndary effect-aquired SS
---Effects of pressure on the nerve root
Pathophysiology bull Effects of pressure on the nerve root
-Compressive
bull -Deformation-stramp funchanges
Classification
bull A-Site5-66-7
bull B-Direction posterolat
bull C-Amount
---Bulge
--Herniation
1-Protrusion
2-extrusion
3- sequestration
Effects of prolapse
Clinical picture
bullPressure on Dura
bullPressure on root
bullPressure on cord
bullMixed
Imagingbull X-raybull MRIbull CT scans with or without myelography -intolerant to MRI -Unsuitable for MRIbull gadolinium-enhanced MRI This will help to delineate which part of the
previous operation site is disc and which is epidural fibrosis (the latter enhancing)
DDX
bullAcute muscularampST strain
bullNeuralgic amyatrophy
bull Infection
Tumor
bullRotator cuff syndrome
Treatmentbull usually have a good prognosis
bull In up to four-fifths of patients symptoms
will resolve spontaneously within a 12-week
period
bull However if pain persists beyond this time
there is a slow resolution of pain in the
majority of patients
bull By approximately 4 years there is no difference in the incidence of pain in
patients treated non-operatively or surgically
bull Surgical results will deteriorate after
symptoms have been present for 1
year
Non-operative treatment
bull ANALGESICSampANTIINFLAMATORY
bull REST-collar
bull Reduce-traction
bull
Indications for diskectomybull Strong indications for surgical intervention
-Acute mylopathy or myloradiculopathy
-Progressive Neurological deficit
bull Relative indications
bull Failure of conservative treatment-refractory
bull Significant motor deficit
bull Severe incapacitating pain - does not respond to any form of treatment
surgical treatment--ANTERIOR OPEN APPROACH
--POSTERIOR OPEN APPROACH
--Microdisectomy
--Chemonucleolysis
--percutanious
Complications
1--Approach relatedbull 2--mechanical intraopbull 3-early postop wound infectionsDiscitis bull Haematoma-Airway obsbull 4-late postop-Non-union-Instability-deformity

Pathology
bull Normal aging
bull -disc degeneration-displacement of facet joint
bull -acute disc herneation-pain
bull -2ndary effect-aquired SS
---Effects of pressure on the nerve root
Pathophysiology bull Effects of pressure on the nerve root
-Compressive
bull -Deformation-stramp funchanges
Classification
bull A-Site5-66-7
bull B-Direction posterolat
bull C-Amount
---Bulge
--Herniation
1-Protrusion
2-extrusion
3- sequestration
Effects of prolapse
Clinical picture
bullPressure on Dura
bullPressure on root
bullPressure on cord
bullMixed
Imagingbull X-raybull MRIbull CT scans with or without myelography -intolerant to MRI -Unsuitable for MRIbull gadolinium-enhanced MRI This will help to delineate which part of the
previous operation site is disc and which is epidural fibrosis (the latter enhancing)
DDX
bullAcute muscularampST strain
bullNeuralgic amyatrophy
bull Infection
Tumor
bullRotator cuff syndrome
Treatmentbull usually have a good prognosis
bull In up to four-fifths of patients symptoms
will resolve spontaneously within a 12-week
period
bull However if pain persists beyond this time
there is a slow resolution of pain in the
majority of patients
bull By approximately 4 years there is no difference in the incidence of pain in
patients treated non-operatively or surgically
bull Surgical results will deteriorate after
symptoms have been present for 1
year
Non-operative treatment
bull ANALGESICSampANTIINFLAMATORY
bull REST-collar
bull Reduce-traction
bull
Indications for diskectomybull Strong indications for surgical intervention
-Acute mylopathy or myloradiculopathy
-Progressive Neurological deficit
bull Relative indications
bull Failure of conservative treatment-refractory
bull Significant motor deficit
bull Severe incapacitating pain - does not respond to any form of treatment
surgical treatment--ANTERIOR OPEN APPROACH
--POSTERIOR OPEN APPROACH
--Microdisectomy
--Chemonucleolysis
--percutanious
Complications
1--Approach relatedbull 2--mechanical intraopbull 3-early postop wound infectionsDiscitis bull Haematoma-Airway obsbull 4-late postop-Non-union-Instability-deformity

Pathophysiology bull Effects of pressure on the nerve root
-Compressive
bull -Deformation-stramp funchanges
Classification
bull A-Site5-66-7
bull B-Direction posterolat
bull C-Amount
---Bulge
--Herniation
1-Protrusion
2-extrusion
3- sequestration
Effects of prolapse
Clinical picture
bullPressure on Dura
bullPressure on root
bullPressure on cord
bullMixed
Imagingbull X-raybull MRIbull CT scans with or without myelography -intolerant to MRI -Unsuitable for MRIbull gadolinium-enhanced MRI This will help to delineate which part of the
previous operation site is disc and which is epidural fibrosis (the latter enhancing)
DDX
bullAcute muscularampST strain
bullNeuralgic amyatrophy
bull Infection
Tumor
bullRotator cuff syndrome
Treatmentbull usually have a good prognosis
bull In up to four-fifths of patients symptoms
will resolve spontaneously within a 12-week
period
bull However if pain persists beyond this time
there is a slow resolution of pain in the
majority of patients
bull By approximately 4 years there is no difference in the incidence of pain in
patients treated non-operatively or surgically
bull Surgical results will deteriorate after
symptoms have been present for 1
year
Non-operative treatment
bull ANALGESICSampANTIINFLAMATORY
bull REST-collar
bull Reduce-traction
bull
Indications for diskectomybull Strong indications for surgical intervention
-Acute mylopathy or myloradiculopathy
-Progressive Neurological deficit
bull Relative indications
bull Failure of conservative treatment-refractory
bull Significant motor deficit
bull Severe incapacitating pain - does not respond to any form of treatment
surgical treatment--ANTERIOR OPEN APPROACH
--POSTERIOR OPEN APPROACH
--Microdisectomy
--Chemonucleolysis
--percutanious
Complications
1--Approach relatedbull 2--mechanical intraopbull 3-early postop wound infectionsDiscitis bull Haematoma-Airway obsbull 4-late postop-Non-union-Instability-deformity

Classification
bull A-Site5-66-7
bull B-Direction posterolat
bull C-Amount
---Bulge
--Herniation
1-Protrusion
2-extrusion
3- sequestration
Effects of prolapse
Clinical picture
bullPressure on Dura
bullPressure on root
bullPressure on cord
bullMixed
Imagingbull X-raybull MRIbull CT scans with or without myelography -intolerant to MRI -Unsuitable for MRIbull gadolinium-enhanced MRI This will help to delineate which part of the
previous operation site is disc and which is epidural fibrosis (the latter enhancing)
DDX
bullAcute muscularampST strain
bullNeuralgic amyatrophy
bull Infection
Tumor
bullRotator cuff syndrome
Treatmentbull usually have a good prognosis
bull In up to four-fifths of patients symptoms
will resolve spontaneously within a 12-week
period
bull However if pain persists beyond this time
there is a slow resolution of pain in the
majority of patients
bull By approximately 4 years there is no difference in the incidence of pain in
patients treated non-operatively or surgically
bull Surgical results will deteriorate after
symptoms have been present for 1
year
Non-operative treatment
bull ANALGESICSampANTIINFLAMATORY
bull REST-collar
bull Reduce-traction
bull
Indications for diskectomybull Strong indications for surgical intervention
-Acute mylopathy or myloradiculopathy
-Progressive Neurological deficit
bull Relative indications
bull Failure of conservative treatment-refractory
bull Significant motor deficit
bull Severe incapacitating pain - does not respond to any form of treatment
surgical treatment--ANTERIOR OPEN APPROACH
--POSTERIOR OPEN APPROACH
--Microdisectomy
--Chemonucleolysis
--percutanious
Complications
1--Approach relatedbull 2--mechanical intraopbull 3-early postop wound infectionsDiscitis bull Haematoma-Airway obsbull 4-late postop-Non-union-Instability-deformity

Clinical picture
bullPressure on Dura
bullPressure on root
bullPressure on cord
bullMixed
Imagingbull X-raybull MRIbull CT scans with or without myelography -intolerant to MRI -Unsuitable for MRIbull gadolinium-enhanced MRI This will help to delineate which part of the
previous operation site is disc and which is epidural fibrosis (the latter enhancing)
DDX
bullAcute muscularampST strain
bullNeuralgic amyatrophy
bull Infection
Tumor
bullRotator cuff syndrome
Treatmentbull usually have a good prognosis
bull In up to four-fifths of patients symptoms
will resolve spontaneously within a 12-week
period
bull However if pain persists beyond this time
there is a slow resolution of pain in the
majority of patients
bull By approximately 4 years there is no difference in the incidence of pain in
patients treated non-operatively or surgically
bull Surgical results will deteriorate after
symptoms have been present for 1
year
Non-operative treatment
bull ANALGESICSampANTIINFLAMATORY
bull REST-collar
bull Reduce-traction
bull
Indications for diskectomybull Strong indications for surgical intervention
-Acute mylopathy or myloradiculopathy
-Progressive Neurological deficit
bull Relative indications
bull Failure of conservative treatment-refractory
bull Significant motor deficit
bull Severe incapacitating pain - does not respond to any form of treatment
surgical treatment--ANTERIOR OPEN APPROACH
--POSTERIOR OPEN APPROACH
--Microdisectomy
--Chemonucleolysis
--percutanious
Complications
1--Approach relatedbull 2--mechanical intraopbull 3-early postop wound infectionsDiscitis bull Haematoma-Airway obsbull 4-late postop-Non-union-Instability-deformity

bullPressure on Dura
bullPressure on root
bullPressure on cord
bullMixed
Imagingbull X-raybull MRIbull CT scans with or without myelography -intolerant to MRI -Unsuitable for MRIbull gadolinium-enhanced MRI This will help to delineate which part of the
previous operation site is disc and which is epidural fibrosis (the latter enhancing)
DDX
bullAcute muscularampST strain
bullNeuralgic amyatrophy
bull Infection
Tumor
bullRotator cuff syndrome
Treatmentbull usually have a good prognosis
bull In up to four-fifths of patients symptoms
will resolve spontaneously within a 12-week
period
bull However if pain persists beyond this time
there is a slow resolution of pain in the
majority of patients
bull By approximately 4 years there is no difference in the incidence of pain in
patients treated non-operatively or surgically
bull Surgical results will deteriorate after
symptoms have been present for 1
year
Non-operative treatment
bull ANALGESICSampANTIINFLAMATORY
bull REST-collar
bull Reduce-traction
bull
Indications for diskectomybull Strong indications for surgical intervention
-Acute mylopathy or myloradiculopathy
-Progressive Neurological deficit
bull Relative indications
bull Failure of conservative treatment-refractory
bull Significant motor deficit
bull Severe incapacitating pain - does not respond to any form of treatment
surgical treatment--ANTERIOR OPEN APPROACH
--POSTERIOR OPEN APPROACH
--Microdisectomy
--Chemonucleolysis
--percutanious
Complications
1--Approach relatedbull 2--mechanical intraopbull 3-early postop wound infectionsDiscitis bull Haematoma-Airway obsbull 4-late postop-Non-union-Instability-deformity

Imagingbull X-raybull MRIbull CT scans with or without myelography -intolerant to MRI -Unsuitable for MRIbull gadolinium-enhanced MRI This will help to delineate which part of the
previous operation site is disc and which is epidural fibrosis (the latter enhancing)
DDX
bullAcute muscularampST strain
bullNeuralgic amyatrophy
bull Infection
Tumor
bullRotator cuff syndrome
Treatmentbull usually have a good prognosis
bull In up to four-fifths of patients symptoms
will resolve spontaneously within a 12-week
period
bull However if pain persists beyond this time
there is a slow resolution of pain in the
majority of patients
bull By approximately 4 years there is no difference in the incidence of pain in
patients treated non-operatively or surgically
bull Surgical results will deteriorate after
symptoms have been present for 1
year
Non-operative treatment
bull ANALGESICSampANTIINFLAMATORY
bull REST-collar
bull Reduce-traction
bull
Indications for diskectomybull Strong indications for surgical intervention
-Acute mylopathy or myloradiculopathy
-Progressive Neurological deficit
bull Relative indications
bull Failure of conservative treatment-refractory
bull Significant motor deficit
bull Severe incapacitating pain - does not respond to any form of treatment
surgical treatment--ANTERIOR OPEN APPROACH
--POSTERIOR OPEN APPROACH
--Microdisectomy
--Chemonucleolysis
--percutanious
Complications
1--Approach relatedbull 2--mechanical intraopbull 3-early postop wound infectionsDiscitis bull Haematoma-Airway obsbull 4-late postop-Non-union-Instability-deformity

DDX
bullAcute muscularampST strain
bullNeuralgic amyatrophy
bull Infection
Tumor
bullRotator cuff syndrome
Treatmentbull usually have a good prognosis
bull In up to four-fifths of patients symptoms
will resolve spontaneously within a 12-week
period
bull However if pain persists beyond this time
there is a slow resolution of pain in the
majority of patients
bull By approximately 4 years there is no difference in the incidence of pain in
patients treated non-operatively or surgically
bull Surgical results will deteriorate after
symptoms have been present for 1
year
Non-operative treatment
bull ANALGESICSampANTIINFLAMATORY
bull REST-collar
bull Reduce-traction
bull
Indications for diskectomybull Strong indications for surgical intervention
-Acute mylopathy or myloradiculopathy
-Progressive Neurological deficit
bull Relative indications
bull Failure of conservative treatment-refractory
bull Significant motor deficit
bull Severe incapacitating pain - does not respond to any form of treatment
surgical treatment--ANTERIOR OPEN APPROACH
--POSTERIOR OPEN APPROACH
--Microdisectomy
--Chemonucleolysis
--percutanious
Complications
1--Approach relatedbull 2--mechanical intraopbull 3-early postop wound infectionsDiscitis bull Haematoma-Airway obsbull 4-late postop-Non-union-Instability-deformity

Treatmentbull usually have a good prognosis
bull In up to four-fifths of patients symptoms
will resolve spontaneously within a 12-week
period
bull However if pain persists beyond this time
there is a slow resolution of pain in the
majority of patients
bull By approximately 4 years there is no difference in the incidence of pain in
patients treated non-operatively or surgically
bull Surgical results will deteriorate after
symptoms have been present for 1
year
Non-operative treatment
bull ANALGESICSampANTIINFLAMATORY
bull REST-collar
bull Reduce-traction
bull
Indications for diskectomybull Strong indications for surgical intervention
-Acute mylopathy or myloradiculopathy
-Progressive Neurological deficit
bull Relative indications
bull Failure of conservative treatment-refractory
bull Significant motor deficit
bull Severe incapacitating pain - does not respond to any form of treatment
surgical treatment--ANTERIOR OPEN APPROACH
--POSTERIOR OPEN APPROACH
--Microdisectomy
--Chemonucleolysis
--percutanious
Complications
1--Approach relatedbull 2--mechanical intraopbull 3-early postop wound infectionsDiscitis bull Haematoma-Airway obsbull 4-late postop-Non-union-Instability-deformity

bull By approximately 4 years there is no difference in the incidence of pain in
patients treated non-operatively or surgically
bull Surgical results will deteriorate after
symptoms have been present for 1
year
Non-operative treatment
bull ANALGESICSampANTIINFLAMATORY
bull REST-collar
bull Reduce-traction
bull
Indications for diskectomybull Strong indications for surgical intervention
-Acute mylopathy or myloradiculopathy
-Progressive Neurological deficit
bull Relative indications
bull Failure of conservative treatment-refractory
bull Significant motor deficit
bull Severe incapacitating pain - does not respond to any form of treatment
surgical treatment--ANTERIOR OPEN APPROACH
--POSTERIOR OPEN APPROACH
--Microdisectomy
--Chemonucleolysis
--percutanious
Complications
1--Approach relatedbull 2--mechanical intraopbull 3-early postop wound infectionsDiscitis bull Haematoma-Airway obsbull 4-late postop-Non-union-Instability-deformity

Non-operative treatment
bull ANALGESICSampANTIINFLAMATORY
bull REST-collar
bull Reduce-traction
bull
Indications for diskectomybull Strong indications for surgical intervention
-Acute mylopathy or myloradiculopathy
-Progressive Neurological deficit
bull Relative indications
bull Failure of conservative treatment-refractory
bull Significant motor deficit
bull Severe incapacitating pain - does not respond to any form of treatment
surgical treatment--ANTERIOR OPEN APPROACH
--POSTERIOR OPEN APPROACH
--Microdisectomy
--Chemonucleolysis
--percutanious
Complications
1--Approach relatedbull 2--mechanical intraopbull 3-early postop wound infectionsDiscitis bull Haematoma-Airway obsbull 4-late postop-Non-union-Instability-deformity

Indications for diskectomybull Strong indications for surgical intervention
-Acute mylopathy or myloradiculopathy
-Progressive Neurological deficit
bull Relative indications
bull Failure of conservative treatment-refractory
bull Significant motor deficit
bull Severe incapacitating pain - does not respond to any form of treatment
surgical treatment--ANTERIOR OPEN APPROACH
--POSTERIOR OPEN APPROACH
--Microdisectomy
--Chemonucleolysis
--percutanious
Complications
1--Approach relatedbull 2--mechanical intraopbull 3-early postop wound infectionsDiscitis bull Haematoma-Airway obsbull 4-late postop-Non-union-Instability-deformity

surgical treatment--ANTERIOR OPEN APPROACH
--POSTERIOR OPEN APPROACH
--Microdisectomy
--Chemonucleolysis
--percutanious
Complications
1--Approach relatedbull 2--mechanical intraopbull 3-early postop wound infectionsDiscitis bull Haematoma-Airway obsbull 4-late postop-Non-union-Instability-deformity

Complications
1--Approach relatedbull 2--mechanical intraopbull 3-early postop wound infectionsDiscitis bull Haematoma-Airway obsbull 4-late postop-Non-union-Instability-deformity