Oromandibular dystonia after dental treatments: a report ... · Oromandibular dystonia after dental...
5
379 Oromandibular dystonia after dental treatments: a report of two cases Soo-Mi Jang 1 , Yeong-Cheol Cho 1 , Iel-Yong Sung 1 , Sun-Young Kim 2 , Jang-Ho Son 1 Departments of 1 Oral and Maxillofacial Surgery, 2 Neurology, Ulsan University Hospital, College of Medicine, Ulsan University, Ulsan, Korea Abstract (J Korean Assoc Oral Maxillofac Surg 2012;38:379-83) Oromandibular dystonia (OMD) is a rare focal form of dystonia caused by prolonged muscles spasms in the mouth, face, and jaw. OMD can develop after dental treatment, as poorly aligned dentures or multiple tooth extraction may cause an impairment of proprioception in the oral cavity, leading to the subsequent development of dystonia. These repetitive involuntary jaw movements may interfere with chewing, swallowing, and speaking. We report here two cases of OMD after dental procedures. Key words: Tooth extraction, Dystonic disorders, Jaw, Tongue, Focal [paper submitted 2012. 10. 31 / revised 2012. 11. 27 / accepted 2012. 11. 27] symptoms of the disorder 1,2 . The mechanism of OMD is not well-understood. Some cases of OMD after dental treatment have been reported, although the causal relationship between these procedures and dystonia is still unclear 4,5 . This paper describes 2 cases of peripherally induced OMD. Since the onset of dystonia occurred after a dental procedure, we sought to discuss some aspects of clinical manifestations, diagnostic criteria, mechanisms, and treatment options for OMD. II. Cases Report 1. Case 1 A 59-year-old female with a 12-month history of abnormal jaw protrusive movement and opening was referred by a local practitioner. According to her, her problem started during the dental extraction of her lower right molar teeth and immediate implantation (Fig. 1), and the symptoms worsened over time. Although the local practitioner tried to adjust the occlusion, the symptom was not relieved. She was healthy, with no significant medical history or family history of neurological disorder. The intra-oral examination revealed severe dental attrition of her residual teeth and unstable occlusion.(Fig. 2) The extraoral examination confirmed the involuntary protrusive I. Introduction Dystonia is a neurological movement disorder wherein sustained muscle contractions cause twisting and repetitive movements or abnormal postures. The disorder may be hereditary or may be caused by other factors such as birth- related or other physical trauma, infection, poisoning (e.g., lead poisoning), or reaction to pharmaceutical drugs parti- cularly neuroleptics 1 . Oromandibular dystonia (OMD) is focal dystonia involving the masticatory muscles, muscles of facial expression, and those of the tongue and pharynx. Involuntary, inappropriate, repetitive, or sustained muscle contractions cause varying degrees of jaw opening, closing, deviation, protrusion, or retrusion as well as facial grimacing, abnormal tongue or pharyngeal movement, or any combination of these 2,3 . OMD is a rare, often misdiagnosed disease that is difficult to manage. Its treatment has been limited to minimizing the Jang-Ho Son Department of Oral and Maxillofacial Surgery, Ulsan University Hospital, College of Medicine, Ulsan University, 877, Bangeojinsunhwan-doro, Dong-gu, Ulsan 682-714, Korea TEL: +82-52-250-8823 FAX: +82-52-250-7236 E-mail: [email protected] This is an open-access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0/), which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited. CC CASE REPORT http://dx.doi.org/10.5125/jkaoms.2012.38.6.379 pISSN 2234-7550 · eISSN 2234-5930
-
Upload
nguyenngoc -
Category
Documents
-
view
221 -
download
1
Transcript of Oromandibular dystonia after dental treatments: a report ... · Oromandibular dystonia after dental...

379
Oromandibular dystonia after dental treatments: a report of two cases
Soo-Mi Jang1, Yeong-Cheol Cho1, Iel-Yong Sung1, Sun-Young Kim2, Jang-Ho Son1
Departments of 1Oral and Maxillofacial Surgery, 2Neurology, Ulsan University Hospital, College of Medicine, Ulsan University, Ulsan, Korea
Abstract (J Korean Assoc Oral Maxillofac Surg 2012;38:379-83)
Oromandibular dystonia (OMD) is a rare focal form of dystonia caused by prolonged muscles spasms in the mouth, face, and jaw. OMD can develop after dental treatment, as poorly aligned dentures or multiple tooth extraction may cause an impairment of proprioception in the oral cavity, leading to the subsequent development of dystonia. These repetitive involuntary jaw movements may interfere with chewing, swallowing, and speaking. We report here two cases of OMD after dental procedures.
Key words: Tooth extraction, Dystonic disorders, Jaw, Tongue, Focal[paper submitted 2012. 10. 31 / revised 2012. 11. 27 / accepted 2012. 11. 27]
symptomsofthedisorder1,2.ThemechanismofOMDisnot
well-understood.SomecasesofOMDafterdentaltreatment
havebeenreported,althoughthecausalrelationshipbetween
theseproceduresanddystoniaisstillunclear4,5.
Thispaperdescribes2casesofperipherallyinducedOMD.
Sincetheonsetofdystoniaoccurredafteradentalprocedure,
wesoughttodiscusssomeaspectsofclinicalmanifestations,
diagnosticcriteria,mechanisms,andtreatmentoptionsfor
OMD.
II. Cases Report
1. Case 1
A59-year-oldfemalewitha12-monthhistoryofabnormal
jawprotrusivemovementandopeningwasreferredbya
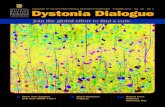
localpractitioner.According toher,herproblemstarted
duringthedentalextractionofherlowerrightmolarteeth
and immediate implantation (Fig.1),and thesymptoms
worsenedovertime.Althoughthelocalpractitionertriedto
adjusttheocclusion,thesymptomwasnotrelieved.Shewas
healthy,withnosignificantmedicalhistoryorfamilyhistory
ofneurologicaldisorder.
Theintra-oralexaminationrevealedseveredentalattrition
ofher residual teethandunstableocclusion.(Fig.2)The
extraoralexaminationconfirmedtheinvoluntaryprotrusive
I. Introduction
Dystonia isaneurologicalmovementdisorderwherein
sustainedmusclecontractionscausetwistingandrepetitive
movementsorabnormalpostures.Thedisordermaybe
hereditaryormaybecausedbyotherfactorssuchasbirth-
relatedorotherphysicaltrauma,infection,poisoning(e.g.,
leadpoisoning),orreactiontopharmaceuticaldrugsparti-
cularlyneuroleptics1.
Oromandibulardystonia(OMD)isfocaldystoniainvolving
themasticatorymuscles,musclesoffacialexpression,and
thoseofthetongueandpharynx.Involuntary,inappropriate,
repetitive,orsustainedmusclecontractionscausevarying
degreesof jawopening,closing,deviation,protrusion,or
retrusionaswellasfacialgrimacing,abnormal tongueor
pharyngealmovement,oranycombinationofthese2,3.
OMDisarare,oftenmisdiagnoseddiseasethatisdifficult
tomanage.Itstreatmenthasbeenlimitedtominimizingthe
Jang-Ho SonDepartment of Oral and Maxillofacial Surgery, Ulsan University Hospital, College of Medicine, Ulsan University, 877, Bangeojinsunhwan-doro, Dong-gu, Ulsan 682-714, KoreaTEL: +82-52-250-8823 FAX: +82-52-250-7236E-mail: [email protected]
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0/), which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
CC
CASE REPORThttp://dx.doi.org/10.5125/jkaoms.2012.38.6.379
pISSN 2234-7550·eISSN 2234-5930
J Korean Assoc Oral Maxillofac Surg 2012;38:379-83
380
Fig. 1. Radiological examination at the initial visit.Soo-Mi Jang et al: Oromandibular dystonia after dental treatments: a report of two cases. J Korean Assoc Oral Maxillofac Surg 2012
Fig. 2. Clinical photo revealing unstable occlusion.Soo-Mi Jang et al: Oromandibular dystonia after dental treatments: a report of two cases. J Korean Assoc Oral Maxillofac Surg 2012
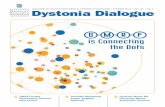
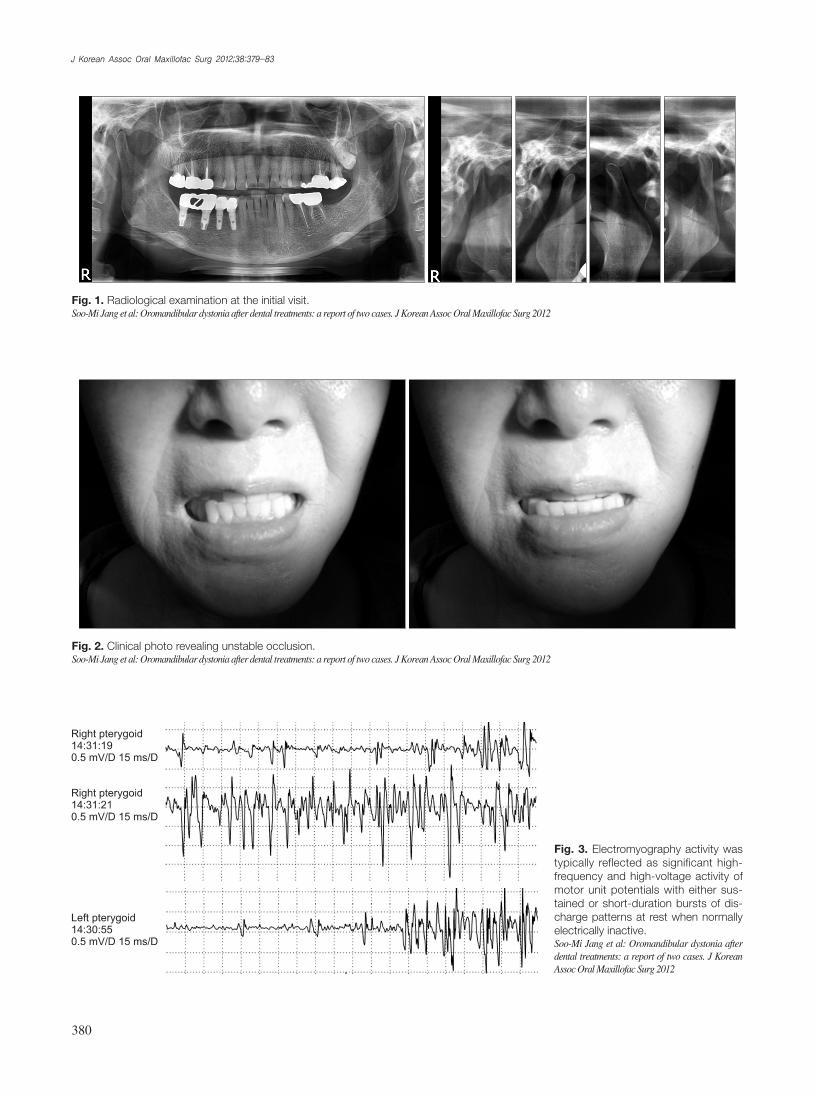
Fig. 3. Electromyography activity was typically reflected as significant high-frequency and high-voltage activity of motor unit potentials with either sus-tained or short-duration bursts of dis-charge patterns at rest when nor mally electrically inactive.Soo-Mi Jang et al: Oromandibular dystonia after dental treatments: a report of two cases. J Korean Assoc Oral Maxillofac Surg 2012
Oromandibular dystonia after dental treatments: a report of two cases
381
OMDwasmade.
2. Case 2
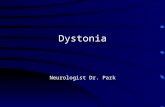
A57-year-oldfemalewithnoprevioushistoryofmove-
mentdisordersandwhowastakingnorelevantmedication
experiencedsuddenonsetofinvoluntaryjawtremor, limi-
tationofmouthopening,andprotrusivetonguemovements
following theextractionofboth lowermolar teethand
immediatepartialdenture6monthsago.(Fig.5)Thesym-
ptomsworsenedovertimeandinterferedwithherspeaking
andeating.
The clinical examination revealed thedenture to be
generallyunstable.Shehadspontaneoustonguemovements
evenwhenshewasnotspeaking.Themovementsworsened
whenherdentureswereremoved.
Shehadnoother relevantmedicaland familyhistory.
Shewas referred to theneurologist for aneurological
exam.Thecranialmagneticresonanceimagingrevealedno
abnormalities,andtheresultoftheneurologicalexamination
wasnormalsaveforthepresenceofabnormalmovement.A
diagnosisoflingualprotrusiveOMDwasmade.
Shewasprescribedbaclofen,analgesics,andocclusal
stabilization appliance.Afteroralmedication andoral
appliancetherapyfor1month,thesymptomimproved,and
shewasreferredtoaprosthodontistfortherepairofherold,
ill-fittingdenture.
Atthefollow-up1monthlater,mildtonguetremorwith
protrusionandjawtremorwereobserved.BTXinjectioninto
thegenioglossusmusclewasrecommended,butthepatient
refusedbecauseoffinancialproblemsandthesymptomsdid
notcauseanydisability.Onlytheoralmedicationofbaclofen
wascontinued.
andopeningmovementwithslightdeviationtowardtheright
side.
Shewasprescribedbaclofen(Baclan;YooyoungPharma-
ceuticalCo.,Ltd.,Seoul,Korea)10mgthreetimesadayand
analgesicsfor thereliefofchronicmusclespasm.Despite
the treatmentwithamusclerelaxantfor threeweeks, the
symptomspersisted.
Shewasreferredtoaneurologistforelectromyography
(EMG).(Fig.3)TheEMGrecordingsrevealedthatherproblem
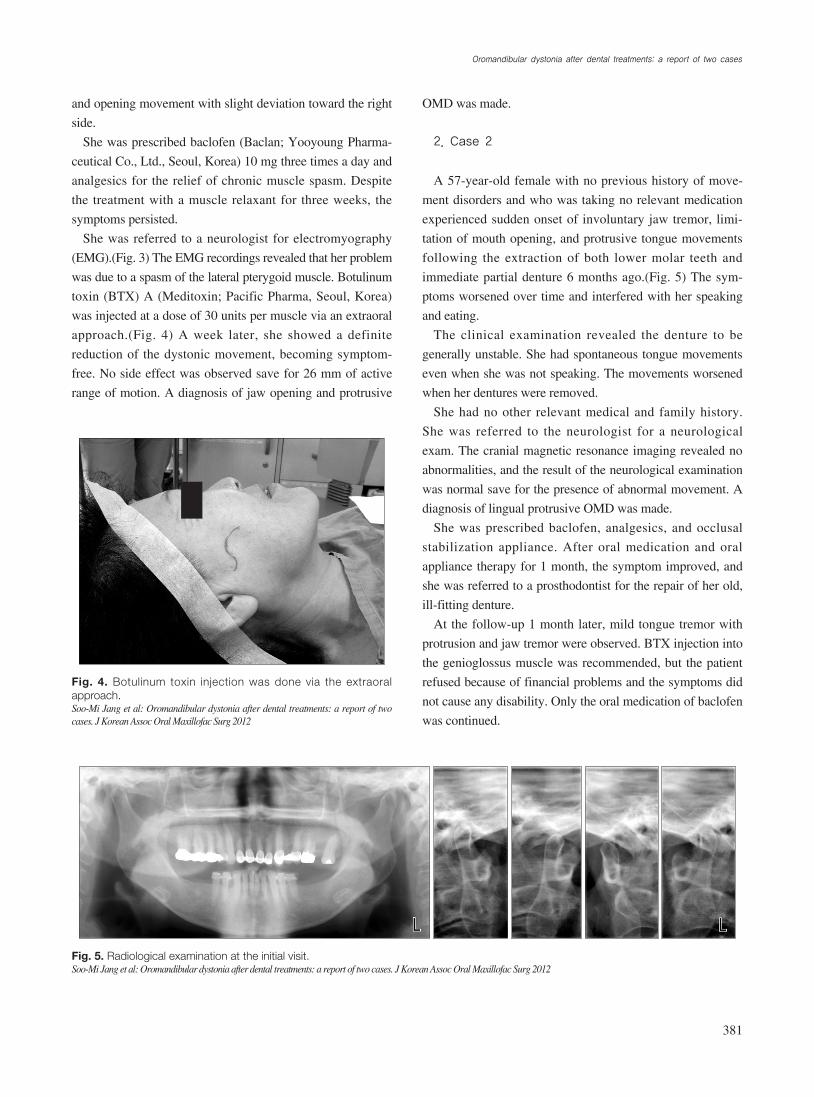
wasduetoaspasmofthelateralpterygoidmuscle.Botulinum
toxin(BTX)A(Meditoxin;PacificPharma,Seoul,Korea)
wasinjectedatadoseof30unitspermuscleviaanextraoral
approach.(Fig. 4)Aweek later, she showedadefinite
reductionof thedystonicmovement,becomingsymptom-
free.Nosideeffectwasobservedsavefor26mmofactive
rangeofmotion.Adiagnosisofjawopeningandprotrusive
Fig. 5. Radiological examination at the initial visit.Soo-Mi Jang et al: Oromandibular dystonia after dental treatments: a report of two cases. J Korean Assoc Oral Maxillofac Surg 2012
Fig. 4. Botulinum toxin injection was done via the extraoral approach.Soo-Mi Jang et al: Oromandibular dystonia after dental treatments: a report of two cases. J Korean Assoc Oral Maxillofac Surg 2012

J Korean Assoc Oral Maxillofac Surg 2012;38:379-83
382
Thepathophysiologyofdystoniaisunclearbutisthought
tooriginate in the centrallymediateddysregulationof
movementduetodefectinthebasalgangliaparticularlyin
thesensorymotorregionsoftheputamen.Themechanism
ofperipherallyinduceddystonia-asillustratedbyOMD-is
alsobasedonthetheoryofsensorypathwaydisruptionatthe
levelofthebasalganglia15-17.
Dentalinterventioncanberegardedasperipheraliatrogenic
injury.TherehavebeenseveralreportsofOMDfollowing
dentalprocedures3,7,18.Thompsonetal.reportedonewoman
whodevelopedOMDfollowingdentalextraction8.Traumatic
situations in themouth-suchaspoorlyaligneddentures
ormultipleextractions-maycausean impairmentof the
proprioceptionoftheoralcavity,leadingtothesubsequent
developmentofdystonia8,19.Themuscleconditionworsened
over theyear.Note,however, that thecausalrelationship
betweentheseproceduresanddystoniaisstillunclear4.
OMDisdifficult tomanage,andits treatmenthasbeen
limitedtominimizingthesymptomsofthedisorder.Note,
however, that thereareseveral treatmentoptions thatcan
relievesomeof thesymptomsofdystonia,sophysicians
canselectatherapeuticapproachbasedoneachindividual’
s symptoms12,13.Treatment approachesused tomanage
OMDincludemedication,BTX, localanestheticblocks,
dentalappliances,behavioralmodificationandpsychological
support, andsurgicalprocedures12,13.Oralmedication is
theusualfirstlineoftreatment,butthereisnomedication
topreventdystoniaorslowitsprogression.Tetrabenazine,
clonazepam,orotheroraldrugshavebeenassessed in
a systematicway in large studies.The results of oral
medicationforOMDhavebeenlargelydisappointing.Some
authorsfindtheoralmedicationofbaclofentobeusefulfor
OMD10,13,18.
BTXinjectioninto theaffectedmusclewithorwithout
EMGguidanceisasecond-linetherapy7,13.Botoxhasbeen
proventobesuperior tomedical treatmentparticularly in
focaldystonias20.Injectionsofsmallamountsofthischemical
intotheaffectedmusclespreventmusclecontractions,and
they canprovide temporary improvement in abnormal
postures andmovements characterizingdystonia7.The
toxindecreasesmusclespasmsbyblockingthereleaseof
theneurotransmitteracetylcholine,whichnormallycauses
musclestocontract.Theeffectistypicallyseenafewdays
aftertheinjections,anditcanlastforseveralmonthsbefore
theinjectionsneedtoberepeated2,7.
Physical therapy,useofsplints,stressmanagement,and
biofeedbackmayalsohelpindividualswithcertainformsof
III. Discussion
Dystoniaisapersistentposturefromtheco-contraction
ofagonistsandantagonistsand isgenerallyconsidered
partofthespectrumofdyskinesia2,6.Dyskinesiaconsistsof
adverseeffectsincludingdiminishedvoluntarymovements
andpresenceof involuntarymovements,similar toticsor
chorea1.Dystoniaisaneurologicalmovementdisorderrarely
seenbyoralandmaxillofacialsurgeons7whereinsustained
musclecontractionscausetwisting,repetitivemovements,or
abnormalpostures1,2,5.Themovementsmaybepainful,and
someindividualswithdystoniamayhavetremororother
neurologicalfeatures.Severaldifferentformsofdystonia
mayaffectonlyonemuscle,groupsofmuscles,ormuscles
throughoutthebody1,8,9.Thecauseofmajorityofthecases
isnotknown.Hereditaryorother factors suchasbirth-
related,otherphysicaltrauma,infection,poisoning(e.g.,lead
poisoning),andreactiontopharmaceuticaldrugsparticularly
neurolepticsarepresumedtobethepossiblecauses8-10.
Therearedifferentwaysofdystoniaclassification-itcan
beclassifiedbyetiologyintoprimary(alsoreferredtoas
idiopathic,inherited,orfamilial)andsecondaryforms(also
referredtoasacquired).Primarydystoniareferstodystonia
thatdoesnothaveaclearcause.Manyinstancesofdystonia
are idiopathic.Thesecondaryformofdystoniadevelops
duetoenvironmentalfactors, long-termneurolepticdrugs
(tardivedystonia),neurologicaldisease,braininjury,Wilson’
sdisease,andperipheraltrauma.Themostcommonformis
tardivedystonia,whichdevelopsasasideeffectoflong-term
treatmentwithantipsychoticdrugs11.
Dystoniacanalsobeclassifiedbyageofonset,anatomically
byregionofdistributionsuchasfocal,segmental,multifocal,
andgeneralized,andfurtherintotheaffectedbodyparts2,12,13.
OMDisfocaldystoniainvolvingthemasticatorymuscles,
musclesoffacialexpression,andthoseof thetongueand
pharynx.Involuntary,inappropriate,repetitive,orsustained
musclecontractionscausevaryingdegreesofjawopening,
closing,deviation,protrusion,orretrusionaswellasfacial
grimacing,abnormaltongue,orpharyngealmovementorany
combinationofthese,withthemuscleconditionworsening
over theyear2,3.OMDisclassifiedas jawopening, jaw
closing,jawdeviating,lingualdystonia,orcombinationsof
these2,4,8.
FocalOMDisextremelyrare.TheprevalenceofOMD
varies,reportedlyashighas6.9casesper100,000.Women
seemtobeaffectedmorefrequentlythanmen,withtheonset
typicallybetweentheageof45and70years14.

Oromandibular dystonia after dental treatments: a report of two cases
383
treatment:casereportsanddiscussion.NZDentJ2009;105:18-21.4. Maestre-ferrínL,BurgueraJA,Peñarrocha-diagoM,Peñarrocha-
diagoM.Oromandibulardystonia:adentalapproach.MedOralPatolOralCirBucal2010;15:e25-7.
5. MarsdenCD.Blepharospasm-oromandibulardystoniasyndrome(Brueghel’ssyndrome).Avariantofadult-onsettorsiondystonia?JNeurolNeurosurgPsychiatry1976;39:1204-9.
6. KumarPJ,ClarkML.Clinicalmedicine.6thed.Edinburgh:Saunders;2005:1227.
7. HeiseGJ,MullenMP.Oromandibulardystonia treatedwithbotulinumtoxin:reportofcase.JOralMaxillofacSurg1995;53:332-5.
8. BlanchetPJ,RompréPH,LavigneGJ,LamarcheC.Oraldyskinesia:aclinicaloverview.IntJProsthodont2005;18:10-9.
9. JankovicJ.Etiologyanddifferentialdiagnosisofblepharospasmandoromandibulardystonia.AdvNeurol1988;49:103-16.
10. ClarkGT.Medicalmanagementoforalmotordisorders:dystonia,dyskinesiaanddrug-induceddystonicextrapyramidalreactions.JCalifDentAssoc2006;34:657-67.
11. KarthaN.Therapeutic challenges in dystonia.NeurolClin2010;28:927-40.
12. JankovicJ.Treatmentofdystonia.LancetNeurol2006;5:864-72.13. BatlaA,StamelouM,BhatiaKP.Treatmentoffocaldystonia.Curr
TreatOptionsNeurol2012;14:213-29.14. NuttJG,MuenterMD,AronsonA,KurlandLT,MeltonLJ3rd.
Epidemiologyof focalandgeneralizeddystonia inRochester,Minnesota.MovDisord1988;3:188-94.
15. NeychevVK,GrossRE,LehéricyS,HessEJ,JinnahHA.Thefunctionalneuroanatomyofdystonia.NeurobiolDis2011;42:185-201.
16. HallettM.Neurophysiologyofdystonia: theroleof inhibition.NeurobiolDis2011;42:177-84.
17. ColosimoC,SuppaA,FabbriniG,BolognaM,BerardelliA.Craniocervicaldystonia:clinicalandpathophysiologicalfeatures.EurJNeurol2010;17(Suppl1):15-21.
18. ChidiacJJ.Oromandibulardystoniatreatmentfollowingalossofverticaldimension.DentUpdate2011;38:120-2.
19. SingerC,PapapetropoulosS.Acomparisonofjaw-closingandjaw-opening idiopathicoromandibulardystonia.ParkinsonismRelatDisord2006;12:115-8.
20. TanEK, Jankovic J.Tardive and idiopathicoromandibulardystonia:aclinicalcomparison.JNeurolNeurosurgPsychiatry2000;68:186-90.
dystonia12,13.Surgicaltherapiesincludeperipheralandcentral
surgery.Peripheraldenervationormyectomy is seldom
neededsinceOMDusuallyrespondswelltoBTXandmust
bedelayedwhileothertreatmentoptionsareeffective12,13.
These2peripherallyinducedOMDcasesfolloweddental
procedure,withnofamilyhistoryofmovementdisorders,
organicbrainlesion,orexposuretoneurolepticdrugs.The
onlypredisposingfactorwastherecentdentalextractionand
prosthetic treatment.These2patientsexperiencedashort
latencyperiodbetweentheextractionandonsetofdystonia,
andthesymptomsworsenedovertime.Thecloseassociation
oftime,locationoftheprocedure,andonsetofsymptoms
suggeststhattheonsetofdystoniamayhavebeencausedby
thedentalintervention.
Becauseof its rareoccurrence,patientswithOMDare
probablyoftenmisdiagnosed,or theirdiagnosismaybe
delayed.Consequently, thesepatientsmayalso receive
incorrectdental treatment,andthesymptomsmayworsen
overtheyears.
OMDmaybe caused or aggravated by someof the
otherdentalandprostheticproblems.Thus, inplanning
thedental treatmentandprocedure, thesubtypeofOMD
andthepossibledystonicmovementsandforcesshouldbe
considered.
References
1. ScottBL.Evaluationandtreatmentofdystonia.SouthMedJ2000;93:746-51.
2. LeeKH.Oromandibulardystonia.OralSurgOralMedOralPatholOralRadiolEndod2007;104:491-6.
3. ThorburnDN,LeeKH.Oromandibulardystoniafollowingdental