Surgical Interventions for Dystonia

of 34
-
Upload
cheryl-benson -
Category
Documents
-
view
224 -
download
0
Transcript of Surgical Interventions for Dystonia
-
8/8/2019 Surgical Interventions for Dystonia
1/34
Sunc c.,qt x rn nvE Y ro rYSFoRDvsroynq
DystoniaMedicalResearch oundation
p
-
8/8/2019 Surgical Interventions for Dystonia
2/34
CONTRIBUTORSTheexpertise f the ollowing individuals ontributed igrrifrcantlyto thedevelopment f thispublication.Sincere hanks o:A. Leland Albright, MD Blair Ford' MD
Children'sHospitalof Pittsburgh ColumbiaPresbyterian edicalDepartrnent f Neurosurgery Center,NeurologicalnstitutePittsburgh,Pennsylvania NewYork,NewYorkJeffrey Arle, MD, PhD Mmiit Sangheta, PhDLaheyClinic Baylor Schoolof Medicine
Deparnnent f Neurosurgery Department fNeurologyBurlington,Massachusetts Houston,TexasJoel Blumin, MD Beniamin L. ll/alter, uIDPennsylvania ospital EmoryUniversitySchoolof Medicine
Department f Otolaryngology Departrnent f NeurologyPhiladelphia, ennsylvania Atlanta,GeorgiaGuy Bouvier,MDNotre DameHosPitalDeparEnent fSurgerySt. Larnbert,Quebec,Canada
This booklet was graciously reviewedby Scientific Director Mahlon R. Delong, MD,EmoryUniversity choolofMedicine
Department f NeurologYAtlanta.Georgia
Thisbookletwasunded n partby a grant from the
MedtronicFoundation.Writtenby Jessica eeley, ditor/Special rojectsCoordinatorADystonta Medical ResearchFoundation' Prinled 12/03 ' 500
-
8/8/2019 Surgical Interventions for Dystonia
3/34
Suncrcer-NrrnvENTloNson Dvsront.r
TlsI,n oF CoNTENTSI . I n t r o d u c t i o n . . . . . 2I I . P e r i p h e r a l u r g e r i e s . . . . . . . . 3
CervicalDystonia./SpasmodicTort icol l is .. . .3The BertrandProcedure: electivePeripheralDenervationRhizotomyM icrovascular ecompression
SpasmodicDysphonia/Larytgeal Dystonia. . . . . . . . .1Selective aryngealDenervation ndReinnervationThyroplastyB l e p h a r o sp a sm . . . . . . . . . . . . 1 0Myectomy Surgery
Genera l i zedDyston ia&Hemidyston ia . . . . . .12IntrathecalBaclofen
III. Brain Surgery: Lesioning Procedures &DeepBra inSt imu la t ion . . . . .15Lesioning Procedures: Pallidotomy & Thalamotomy
Deep Brain StimulationComparing Lesioning & DBSChildren & Brain Surgery
I V . Co n c l u s i o n . . . . . . . . . . 2 5V . A p p e n d i x . . . . . . . . . . . . 2 6
DystoniaThe Nervous SystemAnatomy
EyesNeckLarynx
V I . S o u r c e s . . . . . . . 3 1
-
8/8/2019 Surgical Interventions for Dystonia
4/34
SuncrcelhrrrrvrNttoNs ron DvsroNn
I.IxrnooucrloNAs research boutdystoniaprogresses,reatattention s beingpaid o therole of surgicalnterventionsor alleviatingsymptoms. urgical reatmentsfor dystoniamay bean option or caseshat do not respond o oralmedicationsr botulinum oxin njections. esearchersreactivelvrefiningcurrent echniques ndcollectingnformationaboutwhichpatientsmaybenefit he most rom surgical reatments.There s no singlesurgicalprocedurehat canbe applied o al l formsofdystonia.Surgicalproceduresor dystonia anbe divided nto two broadcategories: rain surgery andperipheral surgery.Peripheralsurgeryincludesprocedureshat targetpartsofthe bodyother han he brain.In both brainandperipheral rocedures,he goalof surgery s to intemrptthe faulty communication etween he brainandmuscleshat causesinvoluntarymusclemovements. urgery ntends o treatsymptoms ndimprove unctionbut doesnotcure heunderlying ondition.Because ystonia s a chronicdisorder,he management f symptoms sanongoing,ifelongprocess. ustasmedications ndbotulinum oxininjections reoftennotsingular olutions o an ndividual'sdystonia,surgery s one component f the total management f dystonia.Surgerydoesnot necessarily liminate he need or additional ormsof treatment.However, n manycases urgery mprovcsqualityof life andreducesheneed or medications r botulinum oxin.Like all surgical nterventions.operationso treatdystoniaare associated ith therisk of certaincompli-cations.
The patientselection rocessor determiningf an ndividual s a candi-date or surgerys deliberate ndprecise.Only a neurologist r neurosur-geonwho specializesn movement isorders an ecommend urgery ordystonia.The costof surgery ariesby procedure nd medicalcenter,andcoverages often on a case-by-caseasis or Medicareandprivateinsurance. he success fany surgicalprocedureies heavily n properdiagnosis,heexperience f the clinical eam,and he skill and artistryofthe surseon.
-
8/8/2019 Surgical Interventions for Dystonia
5/34
SuncrceLltrnvEr-ttors rrx Dysto NIe
II. Prnprnnar,SuRcnnvThe symptomsof dystoniaoccur when muscles f thebody receive aultyinformation ro m hebraincausinghem o contractnvoluntarily. hesefaulty nessagesriginatemostcommonly n apartof the braincalled hebasalganglia.Thesemessagesreconveyed ver brainpathwayso thespinal or dand, r om thespinal ord,extendnto he muscles ia nerves.Peripheral urgeries ccuroutside he brain andgenerally arget hespecificnervesand musclesaffectedby the incorrectmessagesrom thebrain.Peripheralurgeriesregenerally se d o treat ocaldystonia. nexceptions intrathecal aclofen,which targets he spinalcord and s usedto treatgeneralized r hemidystonia.However, or thepurposeof thispublication,adiscussion f intrathecal aclofen s ncludedunder hecategoryof peripheralsurgeries.
CERVICAL DYSTONIA/SPASMODIC TORTICOLLISThe Bertrand Procedure: Selective Peripheral Denervation
Selective eripheral denertation surgery or cervical dystonia scommonly referred o as the Bertrondprocedure.In the 1970s,Dr.ClaudeBertrand,with the collaboration f Dr. PedroMolina-Negro,developed his procedure sa peripheralapproacho treat cervicaldystonia.The termselective efers o the care aken o identify thenruscles f the neck affectedby dystonia,and the tenn denen'ationrefers o cutting he nerves hatsupply hosemuscles. hepurpose f theBertrandprocedures to reduceabnormalcontractionsn the affectedmuscles y severinghenerveso thesemuscles. he goalof theproce-dure s to leave ntact he supplyofnerves to unaffectedor less-affectedmuscles.Thisprocedures tailored o addressheuniqueneeds ndsymptoms feachpatient.The initial approach s often o denervatehe musclescausinghemostprominentdystonicmovement, nowing hatsome
-
8/8/2019 Surgical Interventions for Dystonia
6/34
Sunctc r lNlrnr, 'erroxs ronDvs oNtn
residualmovementsmay remain rom lesser-affec teduscles.f theresults o not sufficiently lleviate ymptoms. second rocedure aybeperformed.n manycases,he nitialsurgerysenough o significantlyimprove heabnormal osture.More aggressiveurgeries,n whichal lcervicalmusclesnvolved n thedystonia redenervatedn a singleoperation,may result n temporaryweaknessn the neck.An essential ar l of theprocedures thepre-operative valuationoproperly dentify hemusclesnvolvedand oassessf theprocedure illbenefit he ndividual.Patientswho may beeligible or thesurgeryareobserved linically by the physicianandwith EMG equipmento monitormuscleactivityandpinpoint he musclesaffectedby the dystonia.One basicelementof the Bertrandprocedures to cut rootletsof thespinalaccessory erve,whichsupplystemocleidomastoidmusclesn the neck,and ospare he nerves o thetrapeziusmuscle.The spinalaccessoryerve s oneof 12cranialnervesha toriginatein thebrainstem,which is thejunction of thebrain and hespinal ord.A secondelementof the Bertrandprocedures cutting heposterior ami (branch)ofone or more spinalnervesalong he cervicalvertebrae.(Thiselement f theproce-dure scalled osteriorramiseclonn'.) pinalnervesare arrangedn pairsalongthe engthof the spinalcordand supplymusclesandorgans.Some research
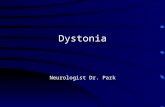
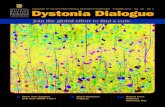
Rotatory orticol l is
Super ntecol l is
Figure ILaterocolis
sup; Retrocottis(,tb3rxInfer ior Antecol l is.)/ " -i /-/.,\!,..\/
-
8/8/2019 Surgical Interventions for Dystonia
7/34
Srnctc qr-lrcnr' r:rroNs on Dysrosl,r
suggestshat he amisectomyncreaseshe rnprovementn persons hohavebecome esistanto botulinum oxin lierapy.To dateover2.000ceruical ystonia atients av eundergonehisproce-dure.Some enters epofisignificantmprovementn as manyas887'o fcases. lthough heprocedurema ybenefit ndividualswith a range fsymptoms,hecategories f patientswho may have he best esults romtheBerlrand rocedure re ndividualsn which:. Symptomsmainlyaffect heneck. Symptoms av estabilizedor 3 years. Th ehead urns o oneside rotationalorticollis). Th ehead s tilted laterocolis). Th ehead urnsand spulledbackwardsrotationalorticolliswith
superioretrocollis). Th ehead umsand ilts orward rotationaiorticoliiswith superiorantecollis). The head spulledback superioretrocollis)
Dystonian which hehead urnsboth o the sideandeitherbackortbru'ardmayhave hebestoutcome.ndivrduals.r'lroespondo botuli-num oxin herapy swell asnon-respondersna ybe eligible.Theprocedure ayalsobe an option or a smallnumber f patients itligeneralizedystoniawho havevery defined ymptomsn th e neck.Sideeff-ects ay ncludenumbnessn thebackof the head, ightr resstthesurgery ite, orneernainingmovements.ifficultyswallolving, ndlackof beneflt.Patients reoftenable o so homeafler wo or threenights n thehospital.Studies avedemonstratedhat he Bertrand rocedurean significantlyimprole the posture f theneckw'itha better angeof nrotion.Physicaltherapybllowing he procedures very mportanto preserveange fmotion.
-
8/8/2019 Surgical Interventions for Dystonia
8/34
Suncrclr- NtenvrNrroNsoaDt'sroNre
RhizotomySince he ate 19thcentury,physicians aveattemptedo treatcervicaldystoniasurgicallyby cutting hespinalnerveshat supply hecontractingmuscles.While the ramisectomy lementof the Bertrandprocedureinvolves xcising pecitic ranches f theceruical pinalnerves ear hemuscle away rom thespinalcanaland spinalcord),pioneering urgeonsinitially attemptedo remove he nerveat the root (inside he spinalcanalnear he spinalcord).The procedure fcutting a nerveat the root iscalled a rhizotomy.Eachspinalnerve has wo roots:a dorsal posterior) ensory oot and aventral anterior)motorroot. The sensoly oot conveyssensorynforma-tion from hemuscles,ointsandskin o thespinal ord,and hemotorroot conveys ignals rom hespinal ord o themuscles. utting hesensory ootsdoesnot alterdystoniabut doeshelpspasticity.Cutting hemotor roots-which means utting 85-95%of the root innervatingadystonicmuscle-will effectively enervatehemuscle ut at hecostofinducing ignifi antweakness.Ventral hizotornyor dystoniawa susedwrdelybetweenhe 1930s ndthe 1970s ndwa softencombinedwith a denervation f the accessorynerve.By destroyinghe nerveat the root, heeffecton the muscle smoregeneralizednd may cause greater egree f weakness. heresults f these rocedureser eoverwheluringlyisappointing ndcaused hig h ncidence f complicationsn dystonia atients. heventralrhizotorny sa treatmentbr cervical ystoniawaseventuallyeplacednthe 1970s y the Berlrand rocedure.However, electmedical enters ontinueo incorporatehizotomiesntheirsurgical pproacheso cer-vicalystonia, nd esearchersontinue oexplore heeffects f severinghe nerves t different ocations long hecervical ertebraen order o provideadditionaI urgical pt ions ordystonia atients. elective orsal hizotomies recommonly one o treatspastic tiffness f the imbs diplegia).
-
8/8/2019 Surgical Interventions for Dystonia
9/34
Suncrclr lNrpnvsNrror.lson DvsroMA
Microv asc ular DecompressionMicrovascular decompression urgery for cervical dystonia is based onthe idea hatvariousblood vessels ompress nd rritatesomeof thecranialnerves particularly he spinalaccessory erve), esulting ndystonicsymptoms. hissurgical rocedurenvolves elocatinghebloodvesselswithout injuringthe vessels, erves, r muscles. he relocatedbloodvessels reheld n placewith small mplants.Sectioning f nervesmayor may not be ncluded n theprocedure. here s very little pub-lisheddataabout hisprocedure, nd t hasbeen argelyabandonedordystoniapatients.Adverseeffects nclude ackof benefit,cerebrospinalfluid leakage, nd stroke.There s evidence o suggesthat f a patientundergoes ecompressionurgery nd s not satisfiedwith the results, hepartial removalof the occipital bone and scarring hat results rommicrovascular ecompression ay make t difficult for a subsequentsurgeon o perform a safeand effective Bertrand procedure.
SPASMODTC DYSPHONIA/LARYNGEAL DYSTONIASelective Laryngeal Denervotion and Reinnemation
Selective laryngeal adduction denervation and reinnervation(SLAD/R) is a surgicalprocedureo treatadductorspasmodic ysphonia/laryngealdystoniaby cutting denervating) elected nd branches ftherecurrent aryngealnerye,which is a branchof the vaguscranialnerve.The first attemptso reduce he spasms f spasmodic ysphonia yseveringhe aryngeal erve ook place n the 1970s.Cutting he aryngealnerveparalyzedhe muscles ontrollingone sideof the larynx so hat helarynxcould not contractexcessively. arly resultswere good,butsymptoms eappearedn manypatients.Subsequentioneersn the fieldsought o improve he procedure y varying he methodby which thenerve was separatedrom the muscle.Recurrence f symptomsas wellas breathyvoicecontinuedo be a problem n many patients.
-
8/8/2019 Surgical Interventions for Dystonia
10/34
Sunocal hrBnvrxnoNs ponDvsroMA
Theelement hat distinguishes LAD/R from previous ncarnations f thesurgery s that, after he recurrent aryngealnerve s cut awayfrom thethyroarytenoid nd ateralcricoarytenoidmuscles, he nervestumpsarehookedup to anothernerve reinnervated), ne hat s not associated iththe dystonia.Supplying he musclewith anothernerveprevents heproblematic ranchof laryngealnerve rom growingbackandreconnect-ing to themuscle.Preventinghe aryngeal erve rom communicatingothe musclepreventshe spasms rom returningand helps o change heclosing orcesof the larynx. It is important o note hat he procedure sperformed ilaterally, nlikepreviousnerveoperations erformedoradductorSD. Becausehe disorderoriginates entrally n the brain, tlikely existsbilaterally n the arynx. t is therefore ogical o treatbothsides.Theprocedures accomplished y makingan ncision n the neckandthencreatinga smallwindow into the laryngeal artilageo exposeheunderlyingnervesand muscles.An operatingmicroscopes often used oaid in identificationand suturingofthe tiny nervebranches. heproce-dure akes hreeor four hours o complete.Greatcare s taken o pre-serve he backpartof the cartilage hat protects he nervebranchesothe breathingmuscles.SLAD/R isbestsuited or individualswith spasmodic ysphoniawithoutatremor. t may be an option for personswho are not satisfiedwithbotulinum oxin treatments.More than wo hundred ersonswith spas-modic dysphonia aveundergone LAD/R over he courseof about 0years.During he initial recoveryperiod,al l patients xperienceempo-raryvoice breathiness nd someexperience wallowingdifficulty.Theseissuesesolveovera few monthsand he patient s left with a near-normalvoice, ree of spasm.Studies ave ndicated hatasmanyas 85-90Yo f patients revery satisfiedwith the resultsof surgeryand heresults. o ar. havebeen ife lons.
-
8/8/2019 Surgical Interventions for Dystonia
11/34
Sunctcel INrsnwNloNsron DYsroNn
Thyroplasty'fiwroplas\,surgeriesncludea groupof surgical echniqueso modif-vthecarti lage urroundinghe arynx. fheseadjustable nd eversibleproceduresnvolvemanipulatinghecarti lage y implanting edees r:-;himso hold he issue n place. number f variations f thisprocedureare currentlyusedand are effective or restoration f the voiceafterparalysis r in changinghe pitchof thevoice.'lypeI thyroplasty asbeenused or theabductor arietyof spasmodicdysphonia. n thisprocedure,hevocalcordsarebrought loser ogetherin hopes f decreasinghe effectof the abductor pasms. esults remixed,with some atients etting ood eliefandothers avingminimaleffect.-lypelI thyroplasty s a procedureor adductorspasmodic ysphonia hatinvolves preadinghevocalcordsapartby inserting shim hatpreventsthem rom contactingeachotherduring he spasmshat occur with thisdisorder. lthoughsomepatients ave eported ood eliefof vocal strain,others eel the tradeoffto a breathvandweak voice is excessive.Researchersn the US andabroad ontinue o investigatehyroplastyprocedures. he advantage fthese proceduress that they are argelynon-destructivend do not alter he muscles r nervesupplyof thelarynx.They work throughadjustment f biomechanics loneand aretheoretically eversible, lthoughn practicehe reversibilitymaybelimited by scarring.
-
8/8/2019 Surgical Interventions for Dystonia
12/34
Sunctcal lttrnvENTtoNsFo RDvsro:l'te
BLEPHAROSPASMMyectomy
Surgicalem.val'f theeyelidandbrow-squeezinguscless ref'errecloasa mvecromv rocedure nd s used o treatblepharospasm.l,ectomvpreventshemuscles urroundingheeyes rom beingstimulated yremovinghemuscle.tseforeheavailability f'botulinumoxin,mvectomvwasessentiall;-heonly reatment ption orblepharospasm.[-heintroduction t'botulinunrtoxin njectionsn r989benefited anypersons ith brepharospasmtf ereby hanginghepopulation f individualsligible o. myeciorn,r-..candidatesbr mv'ectomv ecamehose or whombotulinumorin rsno tsufficient.Justas he patient election hanged,rreproceduretselfevorved.lnitially, heprocedurenvolvedemoving ll eyelid-squeezinguscresnbothupperan d ower idsaswell as he browareaat one ime.At thepresentime, heprocedures tailored o theneeds f the patients.t ismostcommon or thesurgeono remove he muscren th euppereyeridsand brow (full uppermvectomy) nd thenre_evaluatehe neld fo. alower myecromy t a laterdate.patientshear asterwhen the procedureis done n stages, ndsome ndividuars o not require he rowermyec-tomy.The full uppermyectomymaybe doneentirely hroughan eyebrowincision. he ncisionie s mmediately djacento thebrowhairandallowsaccesso the upper id orbicularismuscle, ndpartof th e ower idorbicularismuscleaswell as he procerus nd"o^rguto. muscresn thebrow area.Most of theorbicularismuscle s removedduring he eyelidsurgery. stripof densemuscle s left at themarginof the uppereyelidto helpmaintainsomevoluntaryclosureand o protect he eyelashoots.
l0
-
8/8/2019 Surgical Interventions for Dystonia
13/34
Sr ncrclr- NrenvrNrroNsonDvstotue
A limited upper myectomy s a partial uppermyectomy. t is available orthose ndividualswhoarebenefiting rom botulinum oxin but needsomething xtra o restore unction of the eyes. t may be helpful forthosepatientswho haveapraxia difficulty opening he eyes)or for thosewho n addition o blepharospasmav e tosis droopingids).Partialremovalof the orbicularismay subsequentlyecreasehe need orbotulinum oxin in these atients. limited myectomy sdone hroughanuppereyelidcreasencisionand nvolves emovalof theorbicularismusclewithin the upper id areaonly.Becausehere s less issue e-moval han he full uppermyectomy, atients ecover n less ime.Alimited myectomyalsogivesmorepredictable osmeticmprovementbecauseess issue s removed. t is not designed o replacea full uppermyectomy.Mostpatientswill still requirebotulinum oxin njectionsfollowing the limited myectomyprocedure.Personswho havestopped espondingo botulinum oxin aswell as hoserare ndividualswho fail to respond t all may be eligible or myectomy.Individual surgicalcenters ave reatedhundreds fblepharospasmpatientswith myectomy.Techniques sed or cosmeticsurgerysuchassculpting he fat beneath he brow andmanipulating he placementof thebrow,maybe mplementedo providea beneficialaesthetic swell asfunctional esult.Myectomysurgerycanbe doneunder ocal or generalanesthesia.hehealingprocessollowing a myectomymay take up to a year. n mostcases,he patients re able o keep heir eyesopen mmediately ollowingthe operation.However,considerablewelling,hematomasbloodaccu-mulation n lid), lymphedematissue luid), andbruisingmaybepresentearly n thepost-operativeeriodandprevent ompleteeyelidopening.Cool compressesn the first four to five days ollowedby warm com-presses revery helpfulat settling he id swellingand bruising.Thereare numerous otentialside effectsassociated ith myectomysurgery hatarepredictable nd, o somedegree, ccur n mostpatients.Numbness f the forehead egionoftenoccursand s usually emporary
l l
-
8/8/2019 Surgical Interventions for Dystonia
14/34
Sunctcel n-rrrveMnoNson DysroMA
but may lasta yearor more.Loss of tissuevolume n the eyelidareamayoccurwith themuscle emoval,but he mprovedbrow, id position,anddecreasedyelidwrinkling generallygivesan mprovedcosmetic ppear-ance.Decreased yelid closureoccursas a resultof eyelidmuscleremovaland may require he need or additionalartificial tearsandlubricating intment.As theeyelidswelling esolves,he eyelidclosureimproves nd he dry eyesymptoms enerallymprove.Chronic idswellingwhichmay lastsix monthsor longer n somepatients anbe achronicand roublesomeomplication.Chronic id swelling smuch esssevere ndpersistentn the modernmyectomypractices n which upperand ower id myectomies re performed eparately.nfection,hematoma,brow hair oss,andabnormalpositioningof the ower id canoccasionallyoccurbut areuncommon.Patientscontinue o improve in function aswell as n appearanceoraboutsix months to a year after myectomy surgery.Reportshave shownthatvisualdisability s mproved n approxim tely90Yo f patients. omepatientshavemore improvement han others.Touch-upproceduresarerequired n somecases, ndsome ndividualscontinue o requirebotuli-num oxin injections.
GENERALALED DYSTONIA & HEMIDYSTONIAIntrathecal Baclofen: The Baclofen Pump
Baclofen Lioresal@)s a medication ntroduced n the late 1960s satreatment or spasticity.'he medications alsocommonlyused o treatselect ases f dystonia.Baclofen n the spinal luid around hebrain andspinalcordsupplementshe body'ssupplyof a chemicalneurotransmittercalledGABA, which relaxesmusclemovement.The drug may be givenorally,but very high dosesmust often be used o ensurehat hedrugsafurateshe blood streamandreacheshe spinal luid. High doses fbaclofenmay cause ntolerable ide effectssuchas muscleweaknessand atigue.A surgically mplanted aclofenpumpdeliversbaclofendirectly o the spinal luid, andonly very smalldoses reneeded.Theterm intrathecal means n the spinal fluid.)
-
8/8/2019 Surgical Interventions for Dystonia
15/34
S I R ( , IC \ I I \ I F R \ N I I U \ \ I ' ( ) R \ S I O N I
Intrathecal aclofen herapysa non-destruc tive,dj stable,an d eversiblereatment.Several undred ystoniapatients av ebeen reatedu ith ntrathecalaclofen verthecourse fabout 0 years.It hasbeenused or childrenan dadultswith generalizeddystoniabothprimaryandsecondaryandhemidystoniau,ho espondo baclofen.Many personsreatedwithintrathecalaclofen aveacombination f dystonia ndcerebralpalsy. ntrathecalbaclofenmay be used o treatdystoniaaffecting heupperand ower imbs.In order o determinef anindividualseligible or ntrath-ecalbaclofen, e/she i l l undergoscreeningest o obseruehe body's
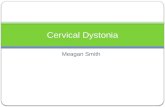
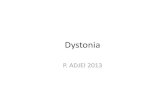
Figure2
f '
responseo baclofen. responseo the oral drugrnaynecessitatea screeningest o observehebody's esponseo a smalldose njecteddirectly nto hespinal luid.The nedications njected singa standardlumbarpuncture r spinal ap.The screeninges tprocedurenvolvesinjection f themedicationollowedby several or.rrsf observation.Relaxation f th emusclesndicatesha tan rnplantedaclofen urnpwilllikely be eff-ective. he effectsof the screening est are elnporaryandmay astseveral oursafter he njection. f a patient oesnot respond 1all to the screeningest,a secondestusing he same roceduremay betried the next day or at a laterdate.
;a
la*7, { rr t: t\{
l f i*s
I t t'q lt ec'q bcr ktf'erthutdvare in body.
I J
-
8/8/2019 Surgical Interventions for Dystonia
16/34
Suncrcer-NrenveunoNsor. DysroNn
Some hysicianssea continuousntrathecalnfusion f baclofen sascreening ethod, incemorepatientsespondo continuousnfusionha nto single njection creening oses.n the nfusion echnique, smallcatheters nsertednto hespinal luid and s connectedo anexternalpump hat nfuses aclofen n increasing oses ver wo to threeda_vs.Startig intrathecalacof'cnherapynvolves urgicaly' mplantingpro-{ramrnableump n thcbody.[-hedevice susuallyplaced ither othe ightor left of thebellv button, eneathhe skinand at of th eabdo-rnen.['hepurnp sconnectedo a thin tLrbehat s tunneled round heside f thebody o theback.A srnal lneedlentroduceshe ube o thespinalcanal. nce hesurgicalncisions re losed.hepump sadjustedby a remote omputerizedevice o deliver heamount f medicationappropriateor the ndividual.Theprocedureakesone o two hours.andthe hospitalstaymay range rom four to sevendays.Modest mprove-mentof symptoms aybe noticeable efore he ndividualsdischargedfrom hehospital, nd t may ak esix months r more o achievehe ullextentof benefit.Regularmaintenances a ke ycomponent f intrathecalaclofenherapy.Regular xams ndphysical herapymaybe a component f postopera-tive care.Pumpsmustbe refi l ledeveryone o four months n thephysician's fltce as a straightforward utpatient rocedure. he pump srefilledby nserting hin needlehroughheskin, nto hepump.Thefrequency f refi l l ing hepumpdepends n hedose equired.f neces-sary, he doctormayadjust he delivery ateof the pumpat the time ofthe refill by remotecontrol.The pump battery astsapproximately evenyears, epending n how muchmedicine sprogrammedo bedeliveredeachday.Before he battery uns out, thepumpwill need o be replacedwith a newpump hrougha surgicalprocedure. he catheter anusuallystay n placeand be reconnectedo the new pump.Baclofen n the spinal luid relaxesmuscleshroughout he body,andappears specially ffective or targeting ystonia n both he upperandlower half of the body. TB may be more effective or treatingsecondarydystoniahan or primarydystonia.
t4
-
8/8/2019 Surgical Interventions for Dystonia
17/34
Suncrcer- lrrnmmons nonDvsroNIA
Studieshaveshown hat intrathecalbaclofencan dramatically mprovesymptoms ndqualityof life. Somecenters ave eported ignificantirnprovementn as muchas 85Yo f patients.However, ike any surgerytheprocedures not without risks.Hardwarecomplicationsmay alsoarise ncluding infection andcatheterbreakageand disconnection. n asmallpercentage f cases, ymptomsmay resumeor worsenwithin thefirst year.The mostcommonside effectsare constipation, ecreasedmusclecontrol,anddrowsiness.
III. BncN Suncnny:LnsroxnvcPnocnouRns& DnBpBnenvSrnrur,l^noxThe goalsof brain surgery or personswith dystoniaare to decreasemusclespasms,ncreasemobility and unction,and mprovepain.There are currently two categoriesof brain surgery or dystonia:lesioningprocedures,which involve selectivedestructionof targeted,abnormal brain tissue, and deep brain stimulation (DBS), which mimicsthe effectsof lesioningby manipulating elective rain areaswith non-destructive lectricalpulses.Although risksexist,casestudies aveshown hat both esioningproce-duresand DBS canresult n marked mprovement f dystoniawithminimal complications.Somepatients reable o decrease r altogetherstopdrug herapy ollowing surgery.Dystoniamostoften originates n a partof the brain called he basalgangliawhich are nvolved n thecoordination ndcontrolof musclemovements. he basalgangliaare a groupof structureshat nclude heglobus pallidus (also called the pallidum), the thalamas, and the subtha-lamic nucleus. esioningproceduresor dystoniausually arget heglobuspallidusor the halamus; eepbrainstimulationusually argetsheglobuspallidusor subthalamic ucleus. heglobuspallidus sresponsiblefor theoutputof messagesrom thebasalganglia.The recipientof thisoutput s the halamus.The subthalamic ucleus s a tiny structureocateddirectlybeneathhe halamus nd s connectedo theglobuspallidus.
-
8/8/2019 Surgical Interventions for Dystonia
18/34
Suncrcel NrsnvsNTroNsonDysroNn
Differentpartsof the brain work together o help he body accomplishspecific ask,suchas apping he foot. 1-he artsof the braincommuni-cate ia pathways f individualbraincells hat ransmit hemicalmes-sagesrom one o the other. n an ndrvidualwith dystonia, hepathwaysthat acilitate he movementof the foot aredisrupted y abnormalactivity.Thegoalof brain surgery s to freeup the pathways o that hebrainandbody may accomplish he ntended unction-in thiscase,moving he oot.Brain surgerymay beperformedunilaterally on one sideof thebrain)orbilaterally on both sides).The effectsofsurgery occur on the sideofthebodyopposite o thesurgicalsite.To date,mostpersonswho haveundergone rain surgery or dystoniawere reatedor generalized ystonia.However, ndividualswho may beeligible or brain surgery ncludepersonswith focal,segmental, r gener-alizeddystoniawith significant, isabling ymptomshatdo notrespondsatisfactorilyo other herapies. dults aswell aschildrenwith primaryand secondary ystoniamaybe eligible.Basedon the imitedavailabledata,differentcategories f patientsmayresponddifferently to brain surgery.Although casesof both secondarydystoniasincluding ardivedystonia) nd ocaldystoniasmaybeeligible,it appears s houghpersonswith DYT-l generalized ystoniaare hebestcandidatesor brain surgery---ether esioningor DBS. Studies aveshownasmuch as 60-90%omprovementn DYT-l patients reatedwithlesioning r DBS.Patientswith secondary emidystoniamay b9eligiblefor brain surgery, hough they may not benefit asmuch as hosewithDYT-l dystonia.Researchersreexamining hepossibility hatpersonswith secondary ystonia may get greaterbenefit from lesioningor DBS tothe thalamus ather hanthe globuspallidus.There s limited data about he long-term effects of each approach.Brainsurgery or dystonia s an evolvingscience,and nvestigatorsarecontinu-ally collecting nformation.
l6
-
8/8/2019 Surgical Interventions for Dystonia
19/34
-
8/8/2019 Surgical Interventions for Dystonia
20/34
procedures performedunilaterally.Bilateralbrainsurgeriesncreaseheriskof complications, ndbilateral halamotomiesn particularareknownto oftencause peech mpairment.The primary factor that distinguishesmodern esioningproceduresromthoseof 50 yearsago s that surgeons re able o locate he lesioningtargetmoreaccurately. he following factorsmake t mucheasier or thesurgicaleam o locate he argetwithin thebrain,which is crucial oreducing he isk of complications. Stereotaclrcs-Surgeonsare able to target the precisearea of the
brainwith a computerized, -dimensional caleusingMRI andCAIscans.. Microelectrode recording and brain mapping-The surgical teamhas he ability to listen o the sounds f brain cells iring messageso
one another.Cells in different partsof the brain fire at very specificratesand in characteristicpatterns,and by listening o thesecells thesurgeon nows exactlywhere he electrode s within the brain.Several ecording ractsmay be necessaryo identiff the precisetarget.
Oncea physicianhas recommendedbrain surgery and pre-operativescreeningestsandpreparations re complete, he basicplanof operationfor pallidotomyand halamotomy re he same. he ndividual s fittedwith a head rameundergeneralor local anesthesia. hebrain s mappedwith imaging echnology o create blueprint or planningandmeasuringthe placement f the electrode.Under ocal anesthesia,he electrodesinserted hrougha smallhole n the skull nto thebrain.Thebrain tselfdoesnot feel pain,and he patient s awakeduringmostof the procedure.The surgical eam nteractswith the patient hroughout he procedure,andthepatientprovides eedback boutsymptoms ndhow he/she eels.Microelectrodeecording s used o confirm the arget.Themappingprocedurealonemay take up to severalhours.Once the target is defined,the surgeon nserts he thermalelectrodeand createsa lesion.Thethermal electrode s removedand he procedure s complete.A bilateral
l8
-
8/8/2019 Surgical Interventions for Dystonia
21/34
proceduremay be done n a singlesurgeryor in two separate urgeries.lf a second arget s to be lesioned, hemappingprocedures repeatedorthat specific arget.Most patientsare n thehospital or two or threedays. Vledications ay be temporarily esumed, ndaftera short ime thepatient eturns o the neurologistor a follow-upexam.'l 'hereis a smallbut eal iskof complicationsssociated ith lesioning.'l 'hemostseriousisk s a 1-2Yoncidence f stroke r hemorrhageuringthe mappingphaseof the surgery. lso, the argetof thepallidotomy, heinternal egment f theglobus allidus, s ocated ightaboveheoptictractwhich may be damagedf the electrodes not targeted recisely.-l 'herealsoexists he isk hat hepallidotomywill not mprove hesymp-toms.Howeveq heprocedure asbeenshown o dramaticallymprovedystonian some atients.
Deep Brain StimulationDeep rainstimulationDBS) nvolvesmplanting timulating lectrodesinto selectedargets n the brain n order o mimic theeffectsof lesioning.Surgeonsegan singDBS in placeof lesioningor Parkinson'siseasepatientsn th emid-1990s. BS alsohasapplicationso tremoran dpain.WhereasDBS hasbeenused o treat housands f personswithParkinson'sisease,heprocedureegan eingapplied o dystonia nly nthe late 1990s. he resultsof more han 200 dystoniapatientshavebeenpublished scase tudiesn medicalournals.BilateralpallidalDBSproduces ignificantbenefit n dystoniawithaverage mprovements f about50-60% n the Burke-Fahn-Marsdendystonia atingscale. omeprimarygeneralizedatients avebeenrepofted o haveup to 90% improvement.DBS hasalso beenperformedon personswith secondary ystonias, ervicaldystonia, egmentaldystonia, ndmyoclonicdystoniawith encouragingesults.
l9
-
8/8/2019 Surgical Interventions for Dystonia
22/34
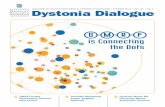
The completeDBS apparatusincludesheDBS electrode.a connectingwire, andapulsegenerator(a.k.a. brainpacemaker" rst imulator)thatcontainsa battery.Theinitialprocedureto implantDBSis denticalo thatof thepallidotomy nd halamotomy. nce hebrain arget s rnapped ndidentified,nstead f creating lesion, hesurgeon laceshe DBSelectrodento he arget. he wire andpulsegenerator aybe rlplantedat the same imeas heelectrode r at a laterdate.The generatorsimplanted nder hecollarbone r in theabdomen. heri re s thentunneled p tlie neck,behind heear.and o thesiteof theelectrodeth epatients undelgeneral nesthesiaol thispartof theprocedure).hewire is connectedo theelectrode.nd he ncisions reclosed.MostDBS proceduresnvolve he rnplantation f two generatorsnc'l redonein two surgeries.t ispossibleo mplant othgeneratorsn a singlesurgery, ut this sa verydernanding pproachor the patient.rnmedi-atelyaf ter heoperation,hepatientmay errporari lyesume redications.The patientmay be dischargedhe next day.Once hegenerators implanted,hepatientmustwait a weekor twobefore he batteries reactivated. hiswaitingperiod s necessaryoallow heswelling hatnormallyoccurswith th esurgery o diminish. heDBS electrode onveys lectrical ulsesnto hebrainusingpowerproduced y thebattery n thegenerator. series f visits o thehospitalare equired o adjust he voltage ettingso the needs f the ndividual. tmav take severalweeksor months o achieve he correctsettines.The
Figure3
Deep brain stimulation horchrore in body.
-
8/8/2019 Surgical Interventions for Dystonia
23/34
patientcan check he statusof the generator singa handhelddevice hatresembles TV remotecontrol. Using his device, he patientcandetermine f the generators on or off, and can urn it backon in theevent hat t shutsdown unexpectedly.Certainphenomenon uchasmagnetic ields caused y securitydevicesmay cause he battery otemporarily topworking.)The expected ife spanof a batteryat a typical voltage s about3-5 years.At a very high voltage, he batterymay need o be replacedaftera year,at a very low voltage,perhaps p to seven ears.Replacinga batterycanbe done undergeneralor local anesthesia san outpatientprocedure.Dystoniadoesnot respond o DBS in the samemanneras other move-mentdisorders o. For example, ersonsreated or tremorwill generallyimprovewithin seconds f turning hegenerator n. In patientswithdystonia, mprovementmay be delayed or days,and weeksor monthsmay passbefore he full extentof the benefit s reached.DBS doesnotnecessarilyliminate hepossibilityof subsequentrugor botulinum oxintreatments.Sideeffectsareminimal, but no procedures without risks.The main riskin DBS is a fatal hemorrhage. owever99-99.5%of patientsdo not havesigrificant bleeding.Despite igorousefforts o avoid t, infection sa riskin approximately2%o f patients. nfection can be seriousand warranttheremovalof the hardware. f this happens,t may be possible o re-implantthe hardwareonce the infection is treated.Hardware failure is also aconcern, hough his is rareandprecautions re n place n the eventofsituations uchas a battery ailing. lt is estimatedhat n 5% of DBSproceduresor dystoniasomecomplicationmay arise,mostof which canbe addressed ithout removing he hardware.Althoughno ongerconsideredinvestigational"or dystoniaby the Food& Drug Administration,DBS is in its infancyas a treatment or thisdisorder. hepreliminary esultsarequitepositive,and heproceduresexpectedo evolveover time asmorepatientsare treatedand moredatais collected.
-
8/8/2019 Surgical Interventions for Dystonia
24/34
Comparing Lesioning & DBSStudies aveshown hatboth esioningandDBS can dramaticallym-provedystonia.Both approaches re associated ith a small,but real,risk of complications.fhereha sno t beena clinicalstudy o compareheresults f lesioning roceduresndDBS.and he advantagesnddisad-vantages f each emainan open ssue.Lesioning roceduresndDBS havemanyelementsn commonncluding:. Patient election riteria. Area of brain targeted. Basicsurgicalprocedure. Potential or profoundbenefit o eligiblepatients. Riskofcomplications ncludinghemorrhageuringsurgeryhemiple-giaor hemiparesis,ensorympairments, peech/languagempairmentIn bothcases,he chanceof benefitmust be weighedagainst he risk ofcomplications. o two cases f dystoniaarealike, anddetermining hespecificapproach o treatment-in thiscase esioningor DBS-must bedecided fter carefuldiscussions mong he patient, amily members,neurologist and neurosurgeon.Of thedystoniapatientswho areeligible or brainsurgerymore ndividu-als arecurrentlybeing ecommendedor DBS thanpallidotomy.Thepallidotomy, oweveq s by no means nobsolete rocedure.Unlessapatient s against avinghardware nstalled n his/herbody, he endencyis to try DBS beforeproceedingo thepallidotomybecause BS isadjustable nd eversible.Financialandgeographicalssues annotbe overlooked.PersonswhohaveDBS must visit the doctor egularly or maintenanceheck-ups.Peoplewho live in remoteareas r areas ot in proximity to a majormovement isordercentermay be at a disadvantage. ravel o and romthecenter-and the expense f this travel-is a part of the ongoingmanagementequiredof DBS patients.
2.
-
8/8/2019 Surgical Interventions for Dystonia
25/34
Llecauseesioning reates permanenthangen the brain issue,here sa slightl;- igher iskof permanentomplicationsuring hesurgery uchasswallowing ifficult1,,peech ifflrcultv. ndcerebral emorrhage.Because llS involveshe mplantation f hardware, omplications':ssociated* i th heapparatusrepossible.ncludingnfection. rosionilrrr-rughheskin.hardware reakage.ndstimulatorailure.l-heriskofirardu'areomplications xists or as ongas hehardwares implanted.It rernainso be seenwhetherhepallidotomy r DBS is moreeffectivethan he other. -he experiencef the surgeon nd rnedical eamare heinost mportant etenninantsf successnd isk. l 'helowest ncidence fcorrrplicationsccursn majormedical entershatperform hese roce-Jrrres fierr. at ientshould hoose centerwitha long-standingxper-'i isein rnovenrentisorders nda clinical eamdevoted o surgery brdl'stonia ndmovement isorders. mov ement isorder eurolo gist ndasurgeon hould e speciallyrainedn functional urgeryan danelectro-physiologist hould eon staffforbrainmapping. n experiencedursingstaff salso mportant.Patients f bothcategoriesf brainsurgerymaybenefit rom physicaltherapy ndsupportiveherapyollowing he procedure.
B
LesioningControlleddestruction Non-destructive
Few post-op estrictions Common-senseestrictionsregardingactivity; must avoid
No cosmeticssues Hardwaremay be slightlyvisible beneathskin insomepeople
-
8/8/2019 Surgical Interventions for Dystonia
26/34
-
8/8/2019 Surgical Interventions for Dystonia
27/34
IV. Coxcr,usroNHavingsurgery s a very significantstep or an ndividual o take n thetreatrnent fdystonia. Ifyou are considering urgeryor ifsurgery hasbeen ecommendedo you by a movement isorderspecialist,he ollow-ingquestionsmayhelpyou nitiatediscussions ith yourdoctors:. What is the nameof the operationand what does he namemean?. Why is this specificsurgeryappropriateor my case?. What are the advantages f having surgery?. What benefitsmight I expect?. What are the risks?. What happens f I don't have he surgery?Are their alternative
treatments?. Wherecan I geta second pinion?. What is the experience f the medicalcenterand surgeonwith thisprocedure?
. Does he medical eampublish he resultsof surgicalcasestudies?. Wherewill the surgerybe done?. What kind of anesthetic ill be used generalor local)?. How long s the recoveryandwhat rehabilitation s necessary?. How muchwill thesurgerycostandwho will pay for it?Surgicalprocedures ay mprove unctionand better he ives of patientswho do not receiveadequateelief from medications nd/orbotulinumtoxin injections.A patientwho is considering urgerymustweigh heopportunity or benefitand heriskof complications. arefuldiscussionswith movement isorderspecialists ndbeingasknowledgeable spossibleaboutdystoniaandsurgerymay aide n the consideration ro-cess.The DystoniaMedicalResearch oundation an providenamesandcontact nformationof dystonia pecialists.Until a cure or dystonia s achieved, esearchersre workingdiligentlytowarddevelopingreatment ptions o improve he lives of affectedindividuals. urgerys an area f researchn whi ch vastprogresss beingmadeand n which the prospect f developingmore effective reatmentsis tremendouslyromising.
-
8/8/2019 Surgical Interventions for Dystonia
28/34
V.AppnuoxDystoniaDystonia s a neurologicalmovement isorder hatcausesmusclesn thebody o contractor spasmnvoluntarily.The nvoluntarymuscle ontrac-tionscause wisting,repetitive, ndpatternedmovements swell asabnormal ostures.Dystonia s not a singledisease ut a syndrome-a setof symptomshatcannotbe attributed o a singlecausebut share ommonelements. omeforms of dystoniamay affecta specific body area,suchas he neck,face, aw, eyes, imbs, or vocalcords.Whendystoniaaffectsa singlebody area, t is called/ocaldystonia.Focaldystonias ncludecervicaldystonia, lepharospasm,romandibular ystonia,writer'scramp,andlaryngealdystonia spasmodic ysphonia). egmental ystoniaaffectstwo or more adjacentbody areas. f two or more non-adjacent odyareasare affected, the dystonia is termed multifocal. Generalizeddystoniarefers o dystonia hat may affect the limbs, trunk, andothermajor bodyareas imultaneously.When dystoniaonly affectsmuscles none sideof the body, t is calledhemidystonia. lthough heoutwardappearances f the various forms of dystoniamay appearvery different,they all share he element f repetitive,patterned, ndoften wistinginvoluntary musclemovements.Dystoniaaffectsmen.women,and childrenof all agesandbackgrounds.Dystoniamaybe geneticor caused y factorssuchasphysical rauma,exposureo certainmedications, r otherneurological onditions.Dystonia s the hird mostcommonmovement isorderafterParkinson'sdisease nd remor,affectingan estimated 50,000personsn NorthAmerica.Nonetheless, ystonia s oftenmisunderstoody thepublicandmisdiagnosed y medicaldoctors.Dystonia sneitherapsychologicaldisorder, or does t affect ntellect.Dystonia snot fatal, but t is achronicdisorder hatcauses aryingdegrees f disabilityandpain, rommild to severe.
25
-
8/8/2019 Surgical Interventions for Dystonia
29/34
Tlrc Nervous System & BrainThe nervous ystem sdivided nto wo parts: hecentralnervoussystem(CNS)an d heperipheralnervous ystem PNS).The CNS consists f thebrain and he spinalcord.The PNSconsists f thenervesextending rom thespinal ord.These wo systems reresponsibleorall bodilyactivit ies,angingromheart ateandmusclernovemento emotions ndleaming.Thebrain s themostcomplex nd ntricateorgan n the humanbody.The .vrinkledraymassthatmakes p 80%of th ebrain scalled hecerebrqlcorler. Thispart s respon-sible or activities uclr sthinking, erceiving,nd
CentralNen'ous SystenlBrain and Spinal Cord
Figure 4
Cen'icalreg ionThoracicreg ion
Lumbarreq ionSacralreg ion
A na|om.t'of the rtet'vottr i s/er?producingand understandinganguage. he cerebral ortex s divided nt otrvo sidesor "hemispheres"-the right and the left. Although both henri-spheres ppear dentical, hey differ in purposeand firnction.Language.reasoning,nd ogiccapabi l i t ies r ig inaten the eft s ideof thebrainwhereasappreciation f shapes nd textures nd artistic alent soriginate nthe right side.The cerebral cortex is further divided into four sectionsor "lobes"-frontal,parietal, emporal,an d occipital.The frontal obe s involved n movement
PeripheralNenous
-
8/8/2019 Surgical Interventions for Dystonia
30/34
Figure 5
Basal gangliasncl related stnt(tttres ofilrc brain--pt'ofi I e vi ew.
BasalGangl iaGlobusPal l idusTh a la musSubstant ia igraCerebel lum
and decision-makin- skillsl the parietal obe nterpretsouch,pain.an dtemperatllre:he temporal ob e s involved n hearingand memory; and heoccipital ob e contains he vision center.Beneath he cerebral ortex ie structureshat help us move, sleep,wake,breathe, mell. hear,see, aste.and eat.Dystoniaaffectsan area n this deeppartof the brain Lrelievedo re_er"rlaterovement called he basalean_slia.nirnbalance t 'brainchemistr .yauseshe basal angl ia o serrdrrappropr iatemessageso th e muscles. ausing he m to contractand spasm uvoluntarily .
Figure 6ArtatomyE y e sTheorbiculariscul imuscleencirclesheopening f theeyesocketand acts o close heeyelids. he corrugator.nuscledraw's he eyebrolls ogether ndwrinkles hebrorv. he procerusmuscle s a facial nuscle etrveenthe eyebrows nd down he nose.
J. t&Ey'entttsclesn pro/ile
Orbicular iso c u l i
L o 1 1 1 1 u 1 . 1 1 > \ , 'Pr,,..-rur-;PY..i, j * : { '
28
-
8/8/2019 Surgical Interventions for Dystonia
31/34
N e c kThestemocleidomastoidndtrapeziusmuscles remajormusclesn the neck.The wostenrocleidomastoidusclesare hick muscles n eachsideofthe neck hatact o bend,rotate, lex, andextend hehead.The trapeziusmusclemoves heshoulder ladesupward n a shrug.
Th y roa ry ten o idmuscle
Sternoceidom s to id
Trapez ius
La te ra lcr icoarytenoimusc le
Inside larynr, viev'-fromabove
Figure 7
-ilt*r...--: ,,/
Anatomy of the neck.
LarynxThe larynx or "voice box" is an organ n theneck hatplaysa crucial rolein speaking ndbreathing.The frameworkof the arynx s madeup of thethyroid cartilage.The rontportionof the hyroid cartilage s visible nsomepeopleas he "Adam's apple."The vocal cordsare ocated n thecenterof the arynx.The thyroarytenoidmuscle s responsibleor closingthe vocalcords,and heposterior ricothyroidmuscle s responsibleoropening hevocalcords.Figure8 Pos te r i o rc i coarytenoi
D
-
8/8/2019 Surgical Interventions for Dystonia
32/34
Larynx (continued)Figure 9
Figure l0
Outer cartilage of larynx,angled view rom front
Cartilageof
larynx, ThvroidI .. cartilage\ -Cricoidcartilage
t"i-o:
StemocleidomastoidTrapezius
Supraclavicular. . fossa;;&,
Surface fthe neck.
-
8/8/2019 Surgical Interventions for Dystonia
33/34
VI. Souncps:' 'SurgeryPanel"presentations t 7d Worldwide DystoniaPatientSymposiurn& 2"dI-'amily ymposium. ovember -10.2002."tJpdateon SpasmodicDysphonia"& "SurgicalOptions or Dystonia"Presentations tM d-Atlantic RegionalSymposium,May 12, 2003.Activa@TherapyFact Sheet,Medtronic (2003)
-
8/8/2019 Surgical Interventions for Dystonia
34/34
SM Kitgore,H Bronte-Stewart, utcomeof palladialsurgery n primaryvs, secondarydystoni4Neurology,2002suppl ); 58,P05.l5l; ,4.395A Lang, Surgical reatment f Dystoni4 Dystonia3: Advances n Neurology,Vol 78,1998.
A Muenchau, Plamer,D DressleqN Quinn,A Lees,KP Bhati4 Selective eripheraldenrvationwith posteriorprimary ramisectomy s useful for botulinum toxin resistantpatientswith cervicaldystoni4 Neurology 1999;52(suppl.2):M94 (Abstract)MY Oh, AAbosch, SH kim, AE Lang,AM Lozano,Longterm hardware-related ompli-cations of deepbrain stimulation, Neurosurgery,2002;50 1268-1276 Abstract)T Taira,T Kobayashi, K Takahashi,T Hori, A new denervation or idiopathic cervicaldystoni4 J Neurosurg2002,Sep;97(2 uppl):201-6 Abstract)RH Walker,DM Sope, FO Danisi, IM German, RR Goodman, MF Brin, Intrathecalbaclofen herapy or dystoni4 Neurology 1999;52 (suppl.2);4521JL Vitek. M Evatt, IY Zhang,V Chockan, MR Delong, S Triche, RAE Bakay,Pallidotomyand deepbrainstimulationas a treatmentor dystoni4 Neurologl 1999;52(suppl.2):A294 Abstract)
ImagesFigure l-l'arsy, D., Vitek, J., Lozano, A., Surgical Treatmentof Parkinsonb DiseaseandOther MovementDisorders,Totow4 NJ: HumanaPress, 003.Figure 2-Image providedcourtesy f Medtronic.Figure 3-Imageprovidedcourtesy f Medtronic.Figure 4-DystoniaMedical Research oundation,8-18Guidebook,1994.Figure S-Henkel,J, "Parkinson'sDisease:New Treatments low Onslaught f Symp-toms," -FDl Corxumer: The vlagazineof the U.S. Food & Drug Administration,Yol.32,No. 4. July-August1988.Figure 6-Gray, H.,Anatomyof theHuman Body,Philadelphia: ea& Febiger, 9l8;Bartleby.com, 000. www.bartleby.com/07l. | | I 1212003.Figure 74ray,H., Anatomltof theHymanBod,, Philadelphia'.Lea&Febiger, 9l8;Bartleby.com, 000. wwwbartlebv.com/ 07/. | | I 1212003.Figure 8-Gray,H., Anatomyof theHuman Body,Philadelphia: ea& Febiger, 9l8;Bartleby. om,2000. www.bartteby.com/07/. | | I 1212003.Figure9-Gray.H.,AnatomltofheHumanBody,Philadelphia:ea&Febigeq 9l8;Bartlebv. om.2000. www.bartleby.om/ 07l. | | I 1212003Figure lO-Stark.F., Gray sAnatomy: A FacrFilled Coloring BooNPhiladelphia: unningPressBooks, 991
JZ