
Orbital hypertelorism- Dr Narendra Uttamrao Markad, DNB Plastic Surgery
33
Orbital Hypertelorism January 22 nd ,2015
-
Upload
narendra-markad -
Category
Health & Medicine
-
view
98 -
download
6
Transcript of Orbital hypertelorism- Dr Narendra Uttamrao Markad, DNB Plastic Surgery

Orbital Hypertelorism
January 22nd,2015

Introduction• Abnormal increase in the
interorbital distance (between the bony orbits at fronto-lacrimal junction)
• Avg ICD 25mm in women 28mm in men
• Symmetrical or asymmetrical
• Unilateral or bilateral
• Asso. with various conditions like craniofacial dysplasia, encephaloceles, dermoid cysts, glial tumors and craniosynostosis syndromes like Apert syndrome
Mulliken – defines ORH as ICD & OCD > 2 SD from age- and gender- matched means


Embryology & Pathology• ORH is not a disease in itself but the manifestation of a craniofacial
deformity that may be present in a variety of craniofacial conditions
• Probably gets established at about 28 mm embryo stage - defective development of the nasal capsule leads to freezing of the
future frontonaso-orbito-ethmoid complex
frontonasal prominence remains in its embryonic position, the optic placodes cannot move towards the midline resulting in ORH
• Early ossification of the lesser wings of sphemoids leads to arrest of orbits in the foetal position (Mann)
Deficient latero-medial movement of the orbit
Skeletal pathology –• Increased ICD with broad nose• Overexpanded ethmoid sinuses• Maxillary anomalies,mainly insufficient anterior growth in the
upper maxilla resulting in maxillary retrusion & malocclusionsIn severe cases – • Inferior displacement of cribriform plate• Temporal displacement of orbits• Decreased A-P dimension of lateral orbital wall In unilateral cases – • Inferior and lateral displacement of orbits• Orbital dystopia
Optic foramina are usually spared - allows orbital movement without damaging to optic nerve


Tessier Classification – 1st degree 30 – 34 mm ICD(For adults) 2nd degree 35 – 40 mm ICD 3rd degree > 40 mm ICD
For children, • Farkas et al: Mean ICD @ 1st yr of age 25-27 mm by 5 yrs of age 27-30 mm > 20 yrs of age 31-33 mm
• Munro : CT scan based grading Type I - parallel medial orbital walls more commom Type II - wedge shaped posteriorly Type III - oval widest dimension Type IV - wedge shaped anteriorly post to globe ; difficuct to correct

Munro : CT scan based grading

Preoperative evaluation & planning
• Ophthalmologic evaluation - document visual status, presence or absence of amblyopia and extraocular dysfunction
• 3D CT face
• P-A cephalogram
• Planning team should involve neurosurgeon and orthodontist

Aims of surgery :- Bring to orbits closer together- Correct orbital dystopia, if present- Narrow the nasal dorsum and create normal nose with adequate projection
Timing of surgery :- If asso. with faciocraniosynostosis - craniosynostosis has to be corrected
independently before 1 year of age
- If asso. with encephalocele – should be operated as early as possible
- If no neurosurgical emergency or craniosynostosis – surgery after age 4 and preferably before age 8 (at completion of cerebral growth and before frontal sinus growth)
- Secondary procedures like revision rhinoplasty and orthognathic surgery at skeletal maturity

Approaches
Box Osteotomy • Tessier et al.(1967) – Combined craniofacial route for an en bloc
mobilization of the orbits medially after resection of midline structures including cribriform plate (negative impact on olfactation)
In Tessier’s protocol, especially in adults, a supraorbital bar is kept in place in order to ensure stability of the mobilized orbits
• Converse et al – Combined cranifacial route with preservation of cribriform plate & removal of paramedian segments, thus preserving nasofrontal junction as base for bone grafting in nasal reconstrucion
Bipartition technique• van der Meulen – mobilization of the two hemifaces Instead of infraorbital rim osteotomy, the osteotomies pass through
the zygomatic arch, the pterygomaxillary junction with midline palatal split

Patient selection Orbital shift or bipartition?
• The maxillary arch: If the maxillary arch is narrow and inverted with the incisors being higher than the molars – Facial bipartition If the maxillary arch and occlusion are normal – Box osteotomy
• The axis of the orbits: If the axis is normal - a horizontal mobilization by box osteotomy If the orbits are laterally and downwardly oblique - facial bipartition
• The nasal fossae: If narrow - Bipartition, improves the airways by enlarging the lower part of face
• Extent of the hypertelorism: If severe cases – Bipartition Mild to moderate cases – box osteotomy

Surgical TechniquesBox osteotomy- Permits a translational movement towards midline along the horizontal or
vertical axes as per needs of ORH
- Orbits are sectioned in a 360° fashion,with osteotomies made posterior to the equator of the globes (“functional orbital volume”)
- The orbits and contained globes are mobilized towards midline as individual cubes (“box osteotomies”)
- When the interorbital distance is greater than 40 mm, the neurosurgical approach is critical because it allows access to the orbital roof and the central ethmoidosphenoidal area
- Extracranial approach alone is only possible if the cribriform plate is very high and the deformity is minimal

Box-shift mobilization of orbits Before mobilization of the orbits After mobilization of the orbits
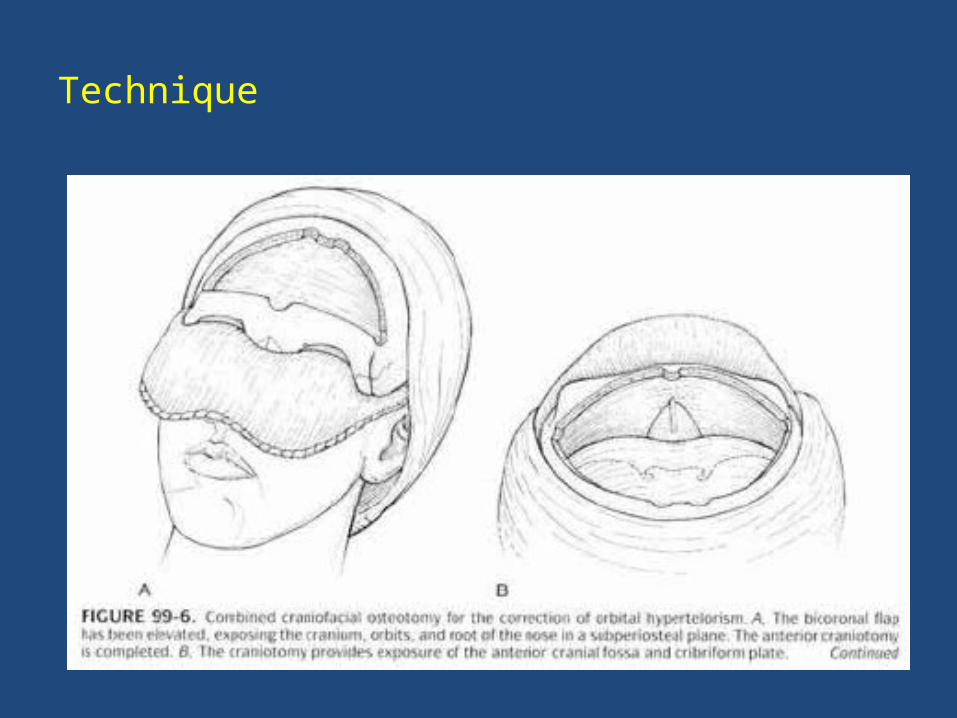
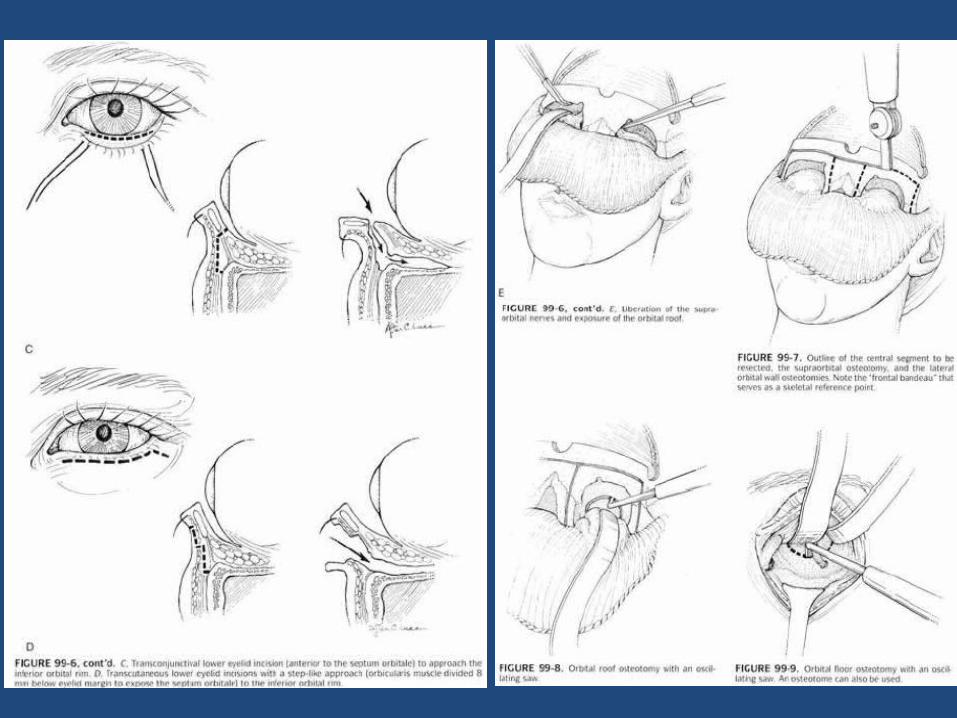
Technique



Facial bipartition- Technique shares many surgical steps in common with box osteotomy Differences are :• V-shape resection of bone at the nose • Absence of osteotomy in the infraorbital rim, instead the osteotomies pass through the zygomatic arch, the pterygomaxillary junction• Palatal bone is split in midline • Medialization, of orbitomaxillary segment instead of orbits, creates an
opening at the palatal level, corrects narrow palatal arch and also widens nasal fossae,thus improving breathing
• Results in change of orbital axis• Occlusal splint is used to ensure maxillary occlusion postoperatively

Medialization of the two hemifaces after bipartition Before medialization After medialization


Subcranial or U-shaped osteotomy
• Hypertelorisms < 35 mm ICD - single medial wall mobilization
• In selected cases presenting with mild symmetrical hypertelorism (35–40 mm) with large frontal sinuses and a high pituitary sella -
supraorbital rim and roof of the orbits are left in place with mobilization of the other three walls as U- shaped orbital segments
• Osteotomy is made at level of frontozygomatic suture and carried through full thickness lateral orbital wall f/b floor and medial wall osteotomy
• Comined intra- and extra-cranial approach OR only extracranial approach can be used foe exposure


Associated Procedures
• Medial canthopexy : canthal ligaments are fixed with transnasal SS wires
• Nasal reconstruction : cantilever split calvarial bone graft for dorsal augmentation
• Fronto-galeal flap : described by Jackson et al to interpose b/w nasal cavity and dura after resection of ethmoid sinuses and nasal septum
• Excess skin : may be treated initially by sagittal resection OR can be postponed as this tissue may contract over time
Delay in midline skin resection is beneficial as it provides some degree of skin excess required during secondary rhinoplasty for dorsal nasal bone grafting

Postoperative care
• Close monitoring is best achieved in a specialized pediatric intensive care unit for at least the first 24 hours
• Prophylactic antibiotic therapy
• Degree of postoperative airway edema may dictate a prolonged intubation extending up to 3 or 4 days
• The prophylactic preoperative tarsorrhaphy is left in place until after successful extubation

Outcomes, prognosis, and complications
• Excessive bleeding
• Cerebrospinal fluid leakage through the nose, may require lumbar drainage if persistent after 3 days
• Infection linked to an insufficient cranialization of the frontal sinus - best prevented by operating early after the age of 4 years, when the frontal sinus has usually not yet developed
• Ophthalmological complications such as keratitis or chemosis are best prevented by the initial tarsorrhaphy
Blindness represents an exceptionally rare but dramatic complication
• Postoperative strabismus is common, and care should be taken to sufficiently medialize the medial orbital walls posterior to the osteotomies so as to avoid a step-off that may impinge on the medial rectus muscles
• insufficient correction - most likely to occur not by relapse, but by soft-tissue relaxation, especially at the medial canthi
• Temporal hollowing
Secondary procedures
• Soft-tissue problems are more complex to treat than bony irregularities
• Temporal hollowness can be addressed by fat grafting • Secondary rhinoplsaty• Orthognathic and orthodontic procedures

Recurrences of hypertelorism
• Recurrences are not frequent if the repair has been performed after 4 years of age, at the completion of skull growth
• Higher recurrence rate if the hypertelorism corrected earlier age as brain growth might counteract medialization of the orbits
• Relapse rate are higher for maxillary retrusion if ORH is asso. with craniosynostosis,because of inherent lack of growth in craniosynostosis




…THANK YOU…


















