or Return of Organization Exempt From Income...
23
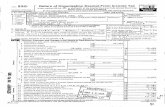
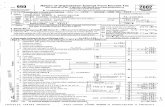
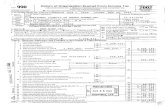
Return of Organization Exempt From Income Tax OMB No 1545-00, F or Under section 501(c), 527, or 4947(a)(1) of the Interna I Revenue Code (except black lung m benefit trust or private foundation) 2002, Department of the Treasury ~ The organization may have to use a copy of this return to satisfy state reporting requirements pps~~~ f ~ic Internal Reven ue Servi_e A For the 2002 calendar year, or tax year period beginning JUL 1 2002 and ending JUN 3 0 2003 B Check it C Name of organization applicable sIe~AS TERO COUNTY HOSPITAL ASSOCIATION p Address lab alor change BA GERALD CHAMPION REGIONAL MED . CENTER 85-0138775 pnn or Name Ochange s~ Number and street (or P 0 box rf mail is not delivered to street address) ,,,, Initial saEZ,fi-2669 N0 . SCENIC DR Fnal Instiuc- ~retum u~~5 City or town, state or country, and ZIP + 4 ,:,return p,MOGORDO NM 88311-0597 return Application " Section 501(c)(3) organizations and 4947(a)(1) nonexempt charitable trusts yea pending must attach a completed Schedule A (Farm 990 or 990-EZ) . k 4"9 0 I G Web site :lN /A a-: ' ~a J Organization type (Checkanlyone)1 O 501(C) ( 3 ),4 (insert no) E:1 4947(2)(1) pr Ej 52 ~, c, a K Check here " 0 if the organization's gross receipts are normally not more than $25,000 The organization need not file a return with the IRS, but if the organization received a Form 990 Package in the mail, it should file a return without financial data Some states require a complete return . H and I are not applicable to section 527 organizations. H(a) Is this a group return for affiliates? = Yes ~X No H(b) If 'Yes," enter number of affiliates 10, H(c) Are all affiliates included N/A = Yes = No (If "No," attach a list ) H(d) Is this a separate return filed by an or- ganization covered by a group rulings = Yes M No I Enter 4-di it GEN M Check " C] if the organization is not required to attach L Gross receipts Add lines 6b, Sb, 9b, and 10b to line 12 . 70 , 686 , 515 . Sch B (Form 990, 990-EZ, or 990-PF) . I 1 Revenue, Expenses, and Changes in Net Assets or Fund Balances 1 Contr'ihutions, gifts, grants, and similar amounts received a Direct public support _ 1 a b Indirect public support 1 e 76,910 . c Government contributions (grants) _ . 1c d Total (add lines to through tc) (cash $ 76, 910 . noncash $ ) ld 76,910 . 2 Program service revenue including government fees and contracts (from Part VII, line 93) 2 3 8,912,199 . 3 Membership dues and assessments 3 4 Interest on savings and temporary cash investments 4 5 Droiclends and interest from securities 5 6 a Gross rents SEE STATEMENT 1 6a 407,696 . b Less rental expenses 6b c Net "ental income or (loss) (subtract line 6b from line 6a) 6t 7 OthEr investment income (describe " 7 8 a Gro ::s amount from sale of assets other A Securities B Oilier than inventory 10,135,456 . Ba b Less cost or other basis and sales expenses 10 , 534 , 370 . 8b <398 914 . 8c c Gain or (loss) (attach schedule) __ d Net lain or (loss) (combine line 8c, columns (A) and (B)) STMT 2 8d 9 Special events and activities (attach schedule) a Gross revenue (not including $ of contributions reported on line 1a) 9a b Less . direct expenses other than fundraising expenses 9h c Net income or (loss) from special events (subtract line 9b from line 9a) 9c 10 a Gross saes of inventory, less 10a 20,509,485 . b Less cost of goods sold R ,1~ 10b 5 , 442 , 281 . c Gross profit or (loss) from sa es o a ~~ ~b ct line 10b from line 10a) STMT 3 10c 15 11 Other revenue (from Part VII, ipe 03~~y ~ A~ ~ 11 12 Tnt~il revenue add Imes 1d 5"BE'Y 86' 9~ iv a 1 ~ 12 54 nu 13 Program services (from line 4, c6am(H)~ _ , 13 34 14 Management and general Mfr m line ~A1 G~H 9 ~ / °~ ~ 14 16 15 Fundraising (from line 44, co -C~j ,. ~,~ ~ ~ 15 16 Payments to affiliates (attach schedule) 16 <398,914 .> 067,204 . 73,294 . 709,864 . 156,784 . 751,697 . 11280511 758898 861 2002 .09000 OTERO COUNTY HOSPITAL ASSOC 861 1 D Employer identification number Room/suite E Telephone number ( 505 ) 439-2104 F Accounting method. O Cash a) Accrual Other , D (s p ecify G1 7 C d N Q 0 CIQ 34,229 . 537,246 . 407,696 . I 17 Total exp enses add lines 16 and 44 column A 17 50, 908,481 . 18 Excess or (defied) for the year (subtract line 17 from line 12) 18 3, 801 , 383 . I d 19 Net assets or fund balances at beginning of year (from line 73, column (A)) 19 58, 018,423 . a ,l Q 20 Other changes m net assets or fund balances (attach explanaticri) SEE STATEMENT 4 20 726 , 162, 21 Net assets or fund balances at end of year (combine lines 18, 1 9, and 20) 21 62 , 5 45 , 968 . z2-~oa LHA For Paperwork Reduction Act Notice, see the separate instructions . Form 990 (2002)
Transcript of or Return of Organization Exempt From Income...

Return of Organization Exempt From Income Tax OMB No 1545-00,
F or Under section 501(c), 527, or 4947(a)(1) of the Interna I Revenue Code (except black lung m benefit trust or private foundation)
2002, Department of the Treasury ~ The organization may have to use a copy of this return to satisfy state reporting requirements pps~~~ f~ic Internal Revenue Servi_e
A For the 2002 calendar year, or tax year period beginning JUL 1 2002 and ending JUN 3 0 2003 B Check it C Name of organization
applicable sIe~AS TERO COUNTY HOSPITAL ASSOCIATION
p Address lab alor change BA GERALD CHAMPION REGIONAL MED . CENTER 85-0138775 pnn or Name Ochange s~ Number and street (or P 0 box rf mail is not delivered to street address) ,,,, Initial saEZ,fi-2669 N0 . SCENIC DR Fnal Instiuc-
~retum u~~5 City or town, state or country, and ZIP + 4 ,:,return
p,MOGORDO NM 88311-0597 return Application " Section 501(c)(3) organizations and 4947(a)(1) nonexempt charitable trusts yea pending
must attach a completed Schedule A (Farm 990 or 990-EZ) . k
4"9 0 I
G Web site:lN /A a-: ' ~a J Organization type (Checkanlyone)1 O 501(C) ( 3 ),4 (insert no) E:1 4947(2)(1) pr Ej 52
~, c, a K Check here " 0 if the organization's gross receipts are normally not more than $25,000 The organization need not file a return with the IRS, but if the organization received a Form 990 Package in the mail, it should file a return without financial data Some states require a complete return .
H and I are not applicable to section 527 organizations. H(a) Is this a group return for affiliates? = Yes ~X No H(b) If 'Yes," enter number of affiliates 10, H(c) Are all affiliates included N/A = Yes = No
(If "No," attach a list ) H(d) Is this a separate return filed by an or-
ganization covered by a group rulings = Yes M No I Enter 4-di it GEN M Check " C] if the organization is not required to attach
L Gross receipts Add lines 6b, Sb, 9b, and 10b to line 12 . 70 , 686 , 515 . Sch B (Form 990, 990-EZ, or 990-PF) .
I 1 Revenue, Expenses, and Changes in Net Assets or Fund Balances 1 Contr'ihutions, gifts, grants, and similar amounts received a Direct public support _ 1 a b Indirect public support 1 e 76,910 . c Government contributions (grants) _ . 1c d Total (add lines to through tc) (cash $ 76, 910 . noncash $ ) ld 76,910 .
2 Program service revenue including government fees and contracts (from Part VII, line 93) 2 3 8,912,199 . 3 Membership dues and assessments 3 4 Interest on savings and temporary cash investments 4 5 Droiclends and interest from securities 5 6 a Gross rents SEE STATEMENT 1 6a 407,696 .
b Less rental expenses 6b c Net "ental income or (loss) (subtract line 6b from line 6a) 6t
7 OthEr investment income (describe " 7 8 a Gro ::s amount from sale of assets other A Securities B Oilier
than inventory 10,135,456 . Ba b Less cost or other basis and sales expenses 10 , 534 , 370 . 8b
<398 914 . 8c c Gain or (loss) (attach schedule) __ d Net lain or (loss) (combine line 8c, columns (A) and (B)) STMT 2 8d
9 Special events and activities (attach schedule) a Gross revenue (not including $ of contributions
reported on line 1a) 9a b Less. direct expenses other than fundraising expenses 9h c Net income or (loss) from special events (subtract line 9b from line 9a) 9c
10 a Gross saes of inventory, less 10a 20,509,485 . b Less cost of goods sold
R ,1~ 10b 5 , 442 , 281 .
c Gross profit or (loss) from sa es o a ~~ ~b ct line 10b from line 10a) STMT 3 10c 15 11 Other revenue (from Part VII, ipe 03~~y ~ A~ ~ 11 12 Tnt~il revenue add Imes 1d 5"BE'Y 86' 9~ iv a 1 ~ 12 54 nu 13 Program services (from line 4, c6am(H)~�_ � , 13 34 14 Management and general Mfr m line ~A1 G~H 9 ~ / °~ ~ 14 16 15 Fundraising (from line 44, co -C~j ,. ~,~ ~ ~ 15 16 Payments to affiliates (attach schedule) 16
<398,914 .>
067,204 . 73,294 .
709,864 . 156,784 . 751,697 .
11280511 758898 861 2002 .09000 OTERO COUNTY HOSPITAL ASSOC 861 1
D Employer identification number
Room/suite E Telephone number ( 505 ) 439-2104
F Accounting method. O Cash a) Accrual Other ,
D (sp ecify
G1 7 C d
N Q
0
CIQ
34,229 . 537,246 .
407,696 .
I 17 Total ex penses add lines 16 and 44 column A 17 50, 908,481 . 18 Excess or (defied) for the year (subtract line 17 from line 12) 18 3, 801 , 383 . I
d 19 Net assets or fund balances at beginning of year (from line 73, column (A)) 19 58, 018,423 . a ,l Q 20 Other changes m net assets or fund balances (attach explanaticri) SEE STATEMENT 4 20 726 , 162,
21 Net assets or fund balances at end of year (combine lines 18, 1 9, and 20) 21 62 , 5 45 , 968 .
z2-~oa LHA For Paperwork Reduction Act Notice, see the separate instructions . Form 990 (2002)

' ~ OTERO COUNTY HOSPITAL ASSOCIATION ' DBA GERALD CHAMPION REGIONAL MED . CENTER 85-0138775 Statement of All organizations must complete column (A) Columns (B), (C), and (D) are required for section 501(c)(3) Page 2
"----' Functional Expenses and (4) organizations and section 4947(a)(1) nonexempt charitable trusts but optional for others Do not include amounts reported on line (B) Program (C) Management
ati nti oti anti ... ~a .,s o, .t i (A) TOt81 canncec anri naneral (D) Fundraising
22 Grants and allocations (attach schedule) cash $ 4 0 ; 5 5 0 . nonpsh $ 22
23 Specific assistance to individuals (attach schedule) 23 i
24 Benefits paid to or for members (attach schedule) 24 25 Compensation of officers, directors, etc 25 26 Other salaries and wages 26 27 Pension plan contributions 27 28 Other employee benefits 28 29 Payroll taxes 29 30 Professional fundraising fees 30 31 Accounting fees 31 32 Legal fees 32 33 Supplies 33 34 Telephone 34
35 Postage and shipping 35 36 Occupancy 36 37 Equipment rental and maintenance 37 38 Panting and publications 38 39 Travel i 39 40 Conferences, conventions, and meetings 40 41 Interest 1 41 42 Depreciation, depletion, etc (attach schedule) 42 43 Other expenses not covered above (itemize)
a 43 ; 43t
c 43c d 43t
SEE STATEMENT 5 431 8,040,663 . 2,141,342 . 6,899,321 . 0 .
Joint Costs Check " 0 if you are following SOP 9B-2 Are any point costs from a combined educational campaign and fundraising solicitation reported in (8) Program services ~ E::] Yes OX No If 'Yes," enter (i) the aggregate amount of these point costs $ , (ii) the amount allocated to Program services $ Hill the amount allocated to Management and general $ . and liv) the amount allocated to Fundraising $
What is the orgamzaUon's primary exempt purposes ~ PROVIDE ~HEALTHCARE SERVICES All organizations mist describe their exempt purpose achievements In a clear and concise manner State the number of clients served, publications issued, etc Discuss achievements that are not measurable (Section 501(c)(3) and (4) organizations and 4947(a)(1) nonexempt charitable trusts must also enter the amount of grants and allocations to others.)
a ALL PROGRAM SERVICE EXPENSES RELATE TO THE PROVISION OF MEDICAL CARE TO INDIVIDUALS IN OTERO COUNTY, NM, REGARDLESS OF ABILITY TO PAY .
(Grants and allocations $ b
I (Grants and allocations $ c
(Grants and allocations $ ) d
(Grants and allocation s $
34,156,784 .
e Other program services (attach schedule) (Grants and allocations $
f Total of Program Service Expenses (should equal line 44, column (B), Program services) " 34,156, 7 84 . 223011 01-22-03 Form 990 (2002)
2 2002 .09000 OTERO COUNTY HOSPITAL ASSOC 861 1 11280511 758898 861
40,550 .1 40,550 .1STATEMENT 5
329,793 . 0 . 329,793 . 19,067,932 . 16,487,775 . 2,580,157 .
694,689 . 604,379 . 90,310 . 4,530,349 . 3,974,931 . 555,418 . 1,381,998 . 1,202,338 . 179,660 .
74,782 . 74,782 . 105,369 . 105,369 .
8,417,089 . 8,050,519 . 366,570 . 138,339 . 136,978 . 1,361 . 171,882 . 99,271 . 72,611 .
1,306,420 . 1,070,966 . 235,454 . 1,665,277 . 1,185,198 . 480,079 .
37,768 . 15,995 . 21,773 .
222,462 . 146,542 . 75,920 . 469,708 . 469,708 .
4,213,411 . 4,213,411 .
44 orpanuabons compferonp columiis ft(o) wnymrse touts td lines 13-1 s ~ 44 1 5 L) , 9 L) 8 r 4 g 1 . 3 4 , 15 6 , 7 8 4 . 16 , 7 51, 6 9 7 .
0 .
Program Service Expenses
(Required for 501 (c)(3) and (4) orgs , and 4947(a)(1)
trusts, but optional for others

. i
' OTERO COUNTY HOSPITAL ASSOCIATION Form 990(2002) DBA GERALD CHAMPION REGIONAL MED . CENTER 85-0138775 Page 3
Park ~V Balance Sheets
Note . Where required, attached schedules and amounts within the description column (A) (B) should be for end-of-year amounts only. Beginning of year End of year
45 Cash '; non-interest-bearing 1,750 . 45 2,100 . 46 Savings and temporary cash investments 6 , 866,802 . 46 4,679,003 .
47 a Accounts receivable 47a 15,421,458 . b Hess allowance for doubtful accounts 47h 3,727,229 . 9,168,366 . 47c 11,694,229 .
48 a Pledges receivable 48a b Less allowance for doubtful accounts 48b 48c
49 Grants receivable 49 50 ReceNables from officers, directors, trustees,
and 4:ey employees 50 d 51 a Othe, notes and loans receivable 51a 1,839,898 .
b Less allowance for doubtful accounts 51b 1,203,591 . 51c 1,839,898 . 52 inventories for sage or use 813,073 . 52 829,511 . 53 Prepaid expenses and deferred charges 460,053 . 53 652 , 106 . 54 Investments - securities STMT 7 " E::] Cost M FMV 16,465,014 . 54 14, 302,693 . 55 a Investments - land, buildings, and
equipment basis 55a
b Less' accumulated depreciation 55b 55c 56 Investments - other 56 57 a Land, buildings, and equipment basis _ 57a 69,617,177 .
b Hess . accumulated depreciation 57e 19,338,099 . 41,235,868 . 57c 50,279,078 . 5s other assets (describe No- DEBT ISSUANCE COSTS ) 265 777 . 58 255 139 .
59 Total assets add lines 45 through 58 must e q ual line 74 76 , 480 , 294 . 59 8 4 , 5 33 , 757 . 60 Accounts payable and accrued expenses 3,439 , 406 . 60 5,163,152 . 61 Grants payable 61 62 Deferred revenue 650, 000 . 62
N d 63 Loans from officers, directors, trustees, and key employees 63 a 64 a lax-exempt bond liabilities _ STMT 8 13,995,000 . saa 13,015,000 .
b Mortgages and other notes payable _ STMT 9 16 , 61 . 64h 3,173,289 . 65 Other liabilities (describe " SEE STATEMENT 10 ~ 360 , 848 . 65 636 , 348 .
66 Totil liabilities add pines 60 throw h 65 18 , 461 , 871 . 66 21 , 987 , 789 . Organizations that follow SFAS 117, check here 00, 0 and complete lines 67 through
69 and lines 73 and 74 67 Unriistncted _ 58, 018, 423 . 67 62, 545, 968 . 68 Temlporanly restricted 68
m 69 Permanently restricted 69 Organizations that do not follow SFAS 117, check here " 0 and complete lines
ILL 70 through 74 ~°, 70 Capital stock, trust principal, or current funds _ 70
y 71 Paid-in or capital surplus, or land, building, and equipment fund 71 N a 72 Retained earnings, endowment, accumulated income, or other funds _ 72 °' z 73 Total net assets or fund balances (add lines 67 through 69 or lines 70 through 72,
column (A) must equal line 19, column (B) must equal line 21) 58 , 018 , 423 . 73 62 , 545 , 968 . 74 Tot if liabilities and net assets / fund balances (add lines 66 and 73)76,480,294.1 70 84,533,757 .
Form 990 is available for public inspection and, for some people, serves as the primary or sole source of information about a particular organization How the public perceives an organization in such cases may be determined by the information presented on its return Therefore, please make sure the return is complete and accurate and fully describes, m Part III, the organization's programs and accomplishments
3 2002 .09000 OTERO COUNTY HOSPITAL ASSOC 861 1 11280511 758898 861
223021 01-22-03

75 Did any officer ; director, trustee, or key employee receive aggregate compensation of more than $100,000 from your organization and all related organizations, of which more than $10,000 was provided by the rel ated orga ni zations If "Yes,' attach schedule 1 0 Yes [XJ No Form 990 (2002)
223031 01-22-0.3
11280511 758898 861 2002 .09000 OTERO COUNTY HOSPITAL ASSOC 861 1
~ OTERO COUNTY HOSPITAL ASSOCIATION Form890 2002 DBA GERALD CHAMPION REGIONAL MED . CENTER 85-0138775 Page a Part 1V-A (Reconciliation of Revenue per Audited Park N-B Reconciliation of Expenses per Audited
(Financial Statements with Revenue per Financial Statements with Expenses per Return Return
a Total revenue, gams, and other support a Total expenses and losses per per audited financial statements " a60,878,307 . audited financial statements " a 56,350,762 .
b Amounts included on line a but not on b Amounts included on line a but not on line 17, Form 990
line 12, Forrr'990 (1) Donated services (1) Net unrealized gams and use of facilities $
on investments $ 604, 437 . (2) Prior year adjustments (2) Donated services reported on line 20,
and use of facilities $ Form 990 $ (3) Recoveries of prior (3) Losses reported on
year grants ' $ line 20, Form 990 $ (4) Other (specify) (4) Other (specify) STMT 11, g 5,564,006 . STMT 12 g 5,442,281 .
Add amount :. on lines (1) through (4) _ " b 6,168,443 . Add amounts on lines (1) through (4) " b 5,442,281 . c dine a minus line b " c 5 4 , 7 0 9 , 8 6 4 . c dine a minus line b " c 50,908,481 . d Amounts inc'uded on line 12, Form d Amounts included on brie 17, Form
990 but not on line a : 990 but not on line a
(1) Investment expenses (1) Investment expenses not included on not included on brie 6b,Formi990 $ brie 6b, Form 990 $
(2) Other (specify) (2) Other (specify) . $ $
Add amount :r on lines (1) and (2) " d 0 " Add amounts on lines (1) and (2) _ " d D . e Total revenue per line 12, Form 990 e Total expenses per line 17, Form 990
(fine c plus line d) " e 5 4 709 , 864 . (line c plus line d) " e 5 0 9 0 8 4 81 . part Y List of Officers, Directors, Trustees, and Key Employees (List each one even it not compensated )
(B) Title and average hours (C) Compensation (D)Contnbutions to (E) Expense (A) Name and address per week devoted to (Ii not pai , enter P, ~S 8 def benefit account and i p osition -0- . coin ensation other allowances
----------------------------------
SEE STATEMENT 13 344 743 . 90 , 128 . 7 , 260 . ----------------------------------
- - - - - - - -- - - - - - - - - - - - - - - - - - - - - - - - - -
- - - - - - - -- - - - - - - - - - - - - - - - - - - - - - - - - -
- - - - - - - -- - - - - - - - - - - - - - - - - - - - - - - - - -
- - - - - - - -- - - - - - - - - - - - - - - - - - - - - - - - - -
- - - - - - - - - - - - - - - - - - - - - - - - -
- - - - - - - -- - - - - - - - - - - - - - - - - - - - - - - - - -
- - - - - - - -- - - - - - - - - - - - - - - - - - - - - - - - - -
- - - - - - - -- - - - - - - - - - - - - - - - - - - - - - - - - -
- - - - - - - - - - - - - - - - - - - - - - - - -
- - - - - - - -- - - - - - - - - - - - - - - - - - - - - - - - - -
i - - - - - - - - - - - - - - - - - - - - - -
------------------------- ----------------------------------

' OTERO COUNTY HOSPITAL ASSOCIATION Form 990(2002) DBA GERALD CHAMPION REGIONAL MED . CENTER 85-0138775 Pages
Par's YC Other Information Yes No 76 Did the organization engage m any activity not previously reported to the IRS If "Yes," attach a detailed description of each activity 76 X 77 Were any changes made m the organizing or governing documents but not reported to the IRS? 77 X
If 'Yes,' attach a conformed copy of the changes 78 a Did the organization have unrelated business gross income of $1,000 or more during the year covered by this returns 78a X
b It *Yes,* has It filed a tax return on Form 990-T for this years 78b X 79 Was there a (liquidation, dissolution, termination, or substantial contraction during the years 79 X
If 'Yes,' attach a statement 80 a Is the organization related (other than by association with a statewide or nationwide organization) through common membership,
governing bodies, trustees, officers, etc , to any other exempt or nonexempt organizations BOa X
b It°Yes ; enterthe name of the organization " WHITE SANDS HEALTH CARE SYSTEMS LLC and check whether it is [:1 exempt or ~X nonexempt
81 a Enter direct or indirect political expenditures See line 81 instructions 81a 0 .
b Did the organization file Form 1120-POL for this years 81b X 82 a Did the organization receive donated services or the use of materials, equipment, or facilities at no charge or at substantially less than
fair rental values 82a X b If "Yes," you may indicate the value of these items here Do not include this amount as revenue m Part I or as an
expense in fart II (See instructions m Part III ) 82b N/A
83 a Did the organization comply with the public inspection requirements for returns and exemption applications 83a X b Did the organization comply with the disclosure requirements relating to quid pro quo contributions'? _ _ 83b X
84 a Did the organization solicit any contributions or gifts that were not tax deductibles 84a X b If "Yes," did the organization include with every solicitation an express statement that such contributions or gifts were not
tax deductible? . N/A 84b 85 501(c)(4), (5), or (6) organizations. a Were substantially all dues nondeductible by members N/A_ 85a
b Did the organization make only in-house lobbying expenditures of $2,000 or less NBA 85b It 'Yes' was answered to either 85a or 85b, do not complete 85c through 85h below unless the organization received a waiver for proxy tax owed for tho prior year
c Dues, assessments, and similar amounts from members 85c N/A
d Section 162(e) lobbying and political expenditures 85d N/A
e Aggregate nondeductible amount of section 6033(e)(1)(A) dues notices 85e N/A f Taxable ami ;unt of lobbying and political expenditures (line 85d less 85e) 85f N/A g Does the organization elect to pay the section 6033(e) tax on the amount on line 85V N/A 85 h If section 6D33(e)(1)(A) dues notices were sent, does the organization agree to add the amount on line 85f to its reasonable estimate of dues
allocable to nondeductible lobbying and political expenditures for the following tax years N/A 85h 86 507(c)(7) organizations Enter a Initiation fees and capital contributions included on line 12 86a N/A
b Gross receipts, included on line 12, for public use of club facilities B6b N/A 87 501(c)(12) organizations Enter a Gross income from members or shareholders 87a N/A
b Gross income from other sources (Do not net amounts due or paid to other sources against amounts due or received from them ) 87b N/A
88 At any time during the year, did the organization own a 50% or greater interest in a taxable corporation or partnership, or an entity disregarded as separate from the organization under Regulations sections 301 7701-2 and 3017701-3? If 'Yes,* complete Part IX 88 X
89 a 501(c)(3) organizations Enter Amount of tax imposed on the organization during the year under section 4911 . 0 . , section 4 912 . 0 . , section 4955 . 0 .
b 501(c)(3) and 501(c)(4) organizations. Did the organization engage in any section 4958 excess benefit transaction during the year or did d become aware of an excess benefit transaction from a prior year If "Yes,' attach a statement explaining each transaction 89b X
c Enter Amount of tax imposed on the organization managers or disqualified persons during the year under sections 4912, 4955, and 4958 " 0 .
d Enter Amount of tax on line 89c, above, reimbursed by the organization _ " 0 . 90 a List the states with which a copy of this return is filed " NEW MEXICO
b Number of iimployees employed in the pay period that includes March 12, 2002 ~ 90b I 611 91 The books~uemcare of 110- JAMES R . CHILDERS 7elephoneno " 505-443-7848
Locatedat " 2669 N . SCENIC DRIVE, ALAMOGORDO, NM ZAP+4 . 88310
92 Section 49147(a)(1) nonexempt charitable trusts filing Form 990 in lieu of Form 1041- Check here and enter the amount of tax-exempt interest received or accrued during the tax year " 1 92 I N/A
223°°i 01-22-03 Form 990 (2002)
5 11280511 758898 861 2002 .09000 OTERO COUNTY HOSPITAL ASSOC 861 1

Part X I Information Regarding Transfers Associated v (a) Did the organization, during the year, receive any funds, directly or indirectly, U (b) Did the organization, during the year, pay premiums, directly or indirectly, on a Note' H "Yes" to b ,file Form 8870 and Form 4720 see instructions
Under penalties of penury, I declare that I have examined s return, including accoml Please correct, and compl Decla of prep r (o her fficer) is based on all infom Sign Here ' Signature of officer Date
Paid Preparer's'C ~� � _ V signature ~ r v ~ ~ ~ ~1~,
PfBp818r 'S Fum'sname (or ACCOUNTING &, C SULTING Use Only yours If self-employed), 'P .O . DRAWER JJ ) 223161 address, and
.~ ZIP .n CARLSBAD, NM 88221-752
11280511 758898 861 2002 .09000
i
IOTERO COUNTY HOSPITAL ASSOCIATION Form 990(2002) DBA GERALD CHAMPION REGIONAL MED . CENTER 85-0138775 Page 6
Analysis of Income-Producing Activities (See page 31 of the instructions ) Note Enter gross amounts unless otherwise Unrelated business income Fxuudea n section siz, 513, or sia
indicated , (A) (B) ~~~_ (D) Related or exempt Business Amount S,on Amount 93 Program service revenue code code function income
a NET PATIENT REVENUE & b RELATED INCOME 38,912,199 .
c d e f Medicare/Medicaid payments g Fees and contracts from government agencies .
94 Membership dues and assessments 95 Interest on savings and temporary cash investments 14 34,229 .
96 Dividends and interest from securities 14 537,246 .
97 Net rental income or (loss) from real estate a debt-financed property b not debt-financed property 3 0 4 0 7,696 .
98 Net rental income or (lass) from personal property 99 Other investment income 100 Gam or (loss) from sales of assets
other than inventory <398,914 .> 101 Net income or (loss) from special events 102 Gross profit or (loss) from sales of inventory . 15,06 7 ,204 .
103 Other revenue a CATERING 722320 35,413 .
b P T BILLING COMM 561499 31,004 . c DAY CARE 624410 6,877 .
d e
104 Subtotal (add columns (e), (v), and (E)) [ _73,294, 979,171 . 1 53,580,489 . 105 Total (add line 104, columns (B), (D), and (E)) __ " 54,632,954 . Note : Line 105 plus line 1d, Part 1, should equal the amount on line 12, Part l. part yr11Relationship of Activities to the Accomplishment of Exempt Purposes (See page 32 of the instructions)
Line No . Expl ;im how each activity for which income +s reported in column (E) of Part VII contributed importantly to the accomplishment of the organization's exem pt purposes (other than by providing funds for such purposes)
93 PATIENT AND OTHER REVENUES ARISE FROM THE PROVISION OF MEDICAL CARE D HEALTH EDUCATION TO THE ALAMOGORDO, NM COMMUNITY AND SURROUNDING
AREA . SERVICES INCLUDE INPATIENT, OUTPATIENT, AND ANCILLARY SERVICES IN ORDER TO PROVIDE DIAGNOSIS AND TREATMENT FOR PATIENTS .
paw IX Information Regarding Taxable Subsidiaries and Disregarded Entities (See page 32 of the instructions) A )
lB C ) E
Name, address . andEIN of corporation, Percentage of Nature ofactiwties Tota(0 ) inome End of~year
partnership, or disre arded enti ty ownership interest assets SEE S TATEMENT 14 l
o

ALAMOGOlZDO PHYSICAL THERAPY
QUORUM HEALTH RESOURCES INC .
PO BOX 305172, DEPT 7, NASHVILLE, TN 37230-5172
HDS SERVICES
DRAWER NO . 64758, DETROIT, MI 48264-0123
STAFF -SMART, - INC .
IETARY 1879,909 .
7 11280511 758898 861 2002 .09000 OTERO COUNTY HOSPITAL ASSOC 861 1
SCHEDULE A Organization Exempt Under Section 501(c)(3) OMB No ,sas-ooa7 (Form 990 or 990-EZ) (Except Private Foundation) and Section 501(e), 501(f), 501(k),
501(n), or Section 4947(a)(1) Nonexempt Charitable Trust
Department of the Treasury Supplementary Information-(See separate instructions .) 2002 In terna l Revenue Serv ice jo. MUST be completed by the above organizations and attached to their Form 990 or 990-EZ Name of the organization OTERO COUNTY HOSPITAL ASSOCIATION Employer identification number
DBA GERALD CHAMPION REGIONAL MED . CENTER 1 85 0138775 Pa1't 1 Compensation of the Five Highest Paid Employees Other Than Officers, Directors, and Trustees
(See page 1 of the instructions List each one If there are none, enter 'None ')
a Name and address of each emplo y ee aid (b) Title and average hours (d) contributions to (e) Expense per week devoted to (c) Compensation P ansO8 defertedt account and other
more than $50,000 p osition compensation allowances
MICHAELHICKEY ED DIR
3727 DRIFTWOOD, ALAMOGORDO, NM 88310 40 140,274 . 7,014 . 4,694 .
JANET BUCKMAN SST CFO
813 LARK SPUR AVE, ALAMOGORDO NM 8831040 104,028 . 5,201 . 4,669 .
LILLIE LEWIS ~MRKT DIR
404 SUNDIAL AVE ., ALAMOGORDO NM 8831040 99,049 . 4,952 . 4,607 .
HERBERT BOURNE UC MED DIR
318 YELLOWSTONE, ALAMOGORDO, NM 88310 5 2 101,095 . 0 . 2,649 .
DONNA J . WEST N ----------------------
2306 CHFRRY LANE, ALAMOGORDO NM 8831055 100,114 . 0 . 4,675 . Total number of other employees paid over $50,000
j Compensation of the Five Highest Paid Independent Contractors for Professional Services Part fl (Se e page 2 of the instructions List each one (whether individuals or firms) If there are none, enter'None °)
(a) Name and address of each independent contractor paid more than $50,000 (b) Type of service (c) Compensation
1401 E . ~lOTH ST ., ALAMOGORDO, NM 88310
COMPLETE RX LIMITED
PO BOX X828, HOUSTON, TX 77210-4829
HYSICAL THERAPY 13036035 .
HARMACY 1653,872 .
ANAGEMENT OMPNAY 11040790 .
PO BOX 910, DAPHINE, AL 36526 AGENCY PERSONNEL 798,673 . Total number of others receiving over $50,000 for professional services " ~ 7 3
zzaioi/oi-22-a3 LHA For Paperwork Reduction Act Notice, see the Instructions for Form 990 and Form 990-EZ . Schedule A (Form 990 or 990-EZ) 2002

13 0 An organization that is not controlled by any disqualified persons (other than foundation managers) and supports organizations described in (1) lines 5 through 12 above, or (2) section 501(c)(4), (5), or (6), if they meet the test of section 509(a)(2) (See section 509(a)(3)1
Provide the following information about the supported organizations (See page 5 of the instructions )
(a) Name(s) of supported organization(g) (b) Line number
from above
i 14 ED An organization organized and operated to test for public safety Section 509(a)(4) (See page 5 of the instructions )
Schedule A (Form 990 or 990-EZ) 2002
223711 01-22-03
8
11280511 758898 861 2002 .09000 OTERO COUNTY HOSPITAL ASSOC 861 1
~ OTERO COUNTY HOSPITAL ASSOCIATION Schedule A (Form~990 or 990-EZ) 2002 DBA GERALD CHAMPION REGIONAL MED . CENTER 85-0138775 Page 2
~ Statements About Activities (See page 2 of the instructions ) Yes No
1 During the year, has the organization attempted to influence national, state, or local legislation, including any attempt to influence public opinion on a legislative matter or referendums It 'Yes,* enter the total expenses paid or incurred m connection with the lobbying activities 1 $ $ (Must equal amounts on line 38, Part VI-A, or line i of Part VI-8 ) 1 X Organizations that made an election under section 501(h) by fling Form 5768 must complete Part VI-A Other organizations checking 'Yes,' must complete Part VI-B AND attach a statement giving a detailed description of the lobbying activities
2 During the yErar, has the organization, either directly or indirectly, engaged in any of the following acts with any substantial contributors, trustees, directors, officers, creators, key employees, or members of their families, or with any taxable organization with which any such person is affiliated as an officer, director, trustee, majority owner, or principal beneficiary? (if the answer to any question is "Yes, " attach a detailed statement explaining the transactions)
a Sale, exchange, or leasing of property 2a X
b Lending of money or other extension of credits _ 2b X
t Furnishing of goods, services, or facilities _ 2c X
d Payment of compensation (or payment or reimbursement of expenses if more than $1,000) 2d X
e Transfer of any part of its income or assets 2e X
3 Does the organization make grants for scholarships, fellowships, student loans, etc 9 (See Note below ) 3 X A Do you have~a section 403(b) annuity plan for your employees _ _ 4 X Note : Attach a statement to explain how the organization determines that Individuals or organizations receiving grants or loans from it in furtherance of its charitable programs "qualify" to receive payments .
I part IV Reason for Non-Private Foundation Status (See pages 3 through 5 of the instructions )
The organization is not a private foundation because it is (Please check only ONE applicable box ) 5 ~ A church, convention of churches, or association of churches Section 170(b)(1)(A)(i) 6 D A school Section 170(b)(1)(A)(u) (Also complete Part V ) 7 0 A hospital or a cooperative hospital service organization Section 170(b)(1)(A)(ui) 8 C] A Federal, state, or local government or governmental unit Section 170(b)(1)(A)(v) 9 0 ~1 medical research organization operated in conjunction with a hospital Section 170(b)(1)(A)(ui) Enter the hospital's name, city,
;roil state 10 D pan organization operated for the benefit of a college or university owned or operated by a governmental unit Section 170(b)(1)(A)(ro)
(Also complete the Support Schedule m Part IV-A ) 11a D An organization that normally receives a substantial part of its support from a governmental unit or from the general public
Section 170(b)(1)(A)(vQ (Also complete the Support Schedule in Part IV-A ) 11b C] A community trust Section 170(b)(1)(A)(w) (Also complete the Support Schedule in Part IV-A ) 12 E:1 .4n organization that normally receives (1) more than 331/3% of its support from contributions, membership fees, and gross
receipts from activities related to as charitable, etc , functions - subject to certain exceptions, and (2) no more than 33 1/3% of is support from gross investment income and unrelated business taxable income (less section 511 tax) from businesses acquired by the organization after June 30, 1975 See section 509(a)(2) (Also complete the Support Schedule in Part IV-A )

OTERO COUNTY HOSPITAL ASSOCIATION Schedule A (Form 990 or 990-EZ) 2002 DBA GERALD CHAMPION REGIONAL MED . CENTER 85-0138775 Page 3
Support Schedule (Complete only if you checked a box on line 10, 11, or 12 ) Use cash method of accounting. N/ A Note : You ma use the worksheet m the instructions for converting from the accrual to the cash method of accountin
Calendar year (or fiscal year beginning m) 1 (a) 2001 (b) 2000 (c) 1999 (d) 1998 (e) Total 15 Gifts, grant3, and contributions
received (Do not include unusual rants See line 28
16 Membership' fees received 17 Gross receipts from admissions,
merchandise sold or services performed, or furnishing of facilities in any activity that is related to the organization's charitable, etc , purpose
18 Gross income from interest, dividends, amounts received from payments on securities loans (sec- tion 512(a)(5)), rents, royalties, and unrelated business taxable income (less section 511 taxes) from businesses acquired by the organizatio n after June 30, 1975
19 Net incomElfrom unrelated business activities n ot included in line 18
pp Tax revenues levied for the organization's benefit and either paid to it o r expended on its behalf
21 The value of services or facilities furnished to the organization by a governmental unit without charge Do not include the value of services or facdities~ generally furnished to the public without charge
22 Other income Attach a schedule Do not include gain or (loss) from sale of capital assets
23 Total of lines 15 through 22 0 . 0 . 0 . 0 . 0 . 24 Line 23 minus line 17 25 Enter 1% of line 23
Organizations described on lines 1a or 11 : a Enter 2% of amount m column (e), line 24 0- 25a N/A Prepare a list for your records to show the name of and amount contributed by each person (other than a governmental unit or publicly supported organization) whose total gifts for 1998 through 2001 exceeded the amount shown m line 26a Do not file' this list with your return Enter the sum of all these excess amounts 1 26b N/A Total support for section 509(a)(1) test Enter line 24, column (e) 1 26e N/A Add Amounts from column (e) for lines 18 19
' 22 26b 1 266 N/A
Public sup poR (brie 26c minus line 26d total) _ 1 26e N/A Public su~porl percentage (line 26e (numerator) divided by line 26c (denominator)) 1 26f N/A % Organizations described on line 12 : a For amounts included m tines 15, 16, and 17 that were received from a 'disqualified person,' prepare a list for your records to i show the name of, and total amounts received in each year from, each 'disqualified person ' Do not file this list with your return . Enter the sum of such amounts for each year
(1998) (1999) (2001) (2000) For any amount included in line 17 that was received from each person (other than 'disqualified persons"), prepare a list for your records to show the name of, and amount received for each year, that was more than the larger of (1) the amount on line 25 for the year or (2) $5,000 (include in the list organizations described in tines 5 through 11, as well as individuals ) Do not file this list with your return . After computing the difference between the amount received and the larger amount described in (1) or (2), enter the sum of these differences (the excess amounts) for each year (2001) ' (2000) (1999) (1998) Add Amounts from column (e) for lines 15 16
17 20 21 1 27c N/A
26 b
c d
e f
27.
b
c
g Public support percentage (line 27e (numerator) divided by line 27f (denominator)) 1 27 N/A h investment income percentage line 18 column e numerator divided b line 27f denominator 1 27h N/A
28 Unusual Grants : For an organization described in line 10, 11, or 12 that received any unusual grants during 1998 through 2001, prepare a list for your records to show, fo' each year, the name of the contributor, the date and amount of the grant, and a brief description of the nature of the grant Do not file this list with your return . Do not include these grants m line 15
223121 01-22-0.3 i Schedule A (Form 990 or 990-E4 2002 g
11280511 758898 861 2002 .09000 OTERO COUNTY HOSPITAL ASSOC 861 1
d Add Line~27a total and line 27b total 00- 27d N/A e Public support (line 27c total minus fine 27d total) 1 27e N/A f Total support for section 509(a)(2) test Enter amount on line 23, column (e) 1 2711 N/A

223137 01-22-03
10
2002 .09000 OTERO COUNTY HOSPITAL ASSOC 861 1 11280511 753898 861
' ; OTERO COUNTY HOSPITAL ASSOCIATION Schedule A (Form 990 or 99o-EZ) 2002 DBA GERALD CHAMPION REGIONAL MED . CENTER 85-0138775 Page 4 Part V Private School Questionnaire (Seepage 7 of the instructions) N/A
(To be completed ONLY by schools that checked the box on line 6 in Part 11)
29 Does the organization have a racially nondiscriminatory policy toward students by statement in its charter, bylaws, other governing Yes NO
instrument, or m a resolution of its governing body 29 30 Does the organization include a statement of its racially nondiscriminatory policy toward students in all its brochures, catalogues,
and other written communications with the public dealing with student admissions, programs, and scholarships 30 31 Has the organization publicized its racially nondiscriminatory policy through newspaper or broadcast media during the period of
solicitation for students, or during the registration period if it has no solicitation program, in a way that makes the policy known to all parts of the general community it serves 31 It 'Yes,' please describe, if "No," please explain (If you need more space, attach a separate statement )
32 Does the organization maintain the following a Records indicating the racial composition of the student body, faculty, and administrative staff b Records documenting that scholarships and other financial assistance are awarded on a racially nondiscriminatory basis c Copies of alb catalogues, brochures, announcements, and other written communications to the public dealing with student
admissions, programs, and scholarships _ d Copies of all material used by the organization or on its behalf to solicit contributions?
If you answered 'No' to any of the above, please explain (If you need more space, attach a separate statement )
33 Does the organization discriminate by race in any way with respect to a Students' rights or privileges'? _ _ 33a b Admissions . policies? 33b c Employment of faculty or administrative staffs 33c d Scholarships or other financial assistance 33d e Educational policies? 33e t Use of facilities _ . 331 g Athletic programs9 33 h Other extrac" .urncularactivities? 33h
If you answered °Yes'to any of the above, please explain (If you need more space, attach a separate statement .)
34 a Does the organization receive any financial aid or assistance from a governmental agency _ 34a b Has the organization's right to such aid ever been revoked or suspended 34b
If you answ~ired 'Yes' to either 34a or b, please explain using an attached statement 35 Does the organization certify that it has complied with the applicable requirements of sections 4 01 through 4 05 of Rev Proc 75-50,
1975-2 C B 587, covering racial nondiscrimination? If "No," attach an explanation _ 35 Schedule A (Form 990 or 990-EZ) 2002

46 Lobbying ce ling amount (150% of lin e 45 ( e )) 0 .-
47 Total lobbyirig expenditure ;.
48 Grassroots nontaxable amount 1 0 .
49 Grassroots ceiling amount (150% of If e 48 ( e )) 0 .
50 Grassroots lobbying ex p enditures 0 .
Park VI-8 ' Lobbying Activity by Nonelecting Public Charities ' (For reporting only by organizations that did not complete Part VI-A) (See page 11 of the instructions ) N/A
During the year, did the organization attempt to influence national, state or local legislation, including any attempt to Yes No Amount influence public opinion on a legislative matter or referendum, through the use of a Volunteers b Paid staff or,management (Include compensation m expenses reported on lines c through h .) c Media advertisements _ d Mailings to members, legislators, orthe public e Publication :., or published or broadcast statements f Grants to other organizations for lobbying purposes g Direct contact with legislators, their staffs, government officials, or a legislative body h Rallies, demonstrations, seminars, conventions, speeches, lectures, or any other means i Total lobbying expenditures (Add lines C through h .) __ 0 .
If 'Yes'to any of the above, also attach a statement giving a detailed description of the lobbying activities 223141 01-22-03 Schedule A (Form 990 or 990-EZ) 2002
11 2002 .09000 OTERO COUNTY HOSPITAL ASSOC 861 1 11280511 758898 861
' OTERO COUNTY HOSPITAL ASSOCIATION SchedUle A (Form 990 or 990-EZ) 2002 DBA GERALD CHAMPION REGIONAL MED . CENTER 85-0138775 Page 5
Pan WA Lobbying Expenditures by Electing Public Charities (see page s of the instructions) N/A (To be completed ONLY by an eligible organization that filed Form 5768)
Check 10' a C~ if the or g anization belon g s to an affiliated g roup Check " b ~ if you checked "a" and "limited control" p rovisions a ppl y
Limits on Lobbying Expenditures (a) (b)
Affiliated group To be completed for ALL (The term expenditures" means amounts paid or incurred ) totals electing organizations
N/A
36 Total lobbying' expenditures to influence public opinion (grassroots lobbying) 36 37 Total lobbying expenditures to influence a legislative body (direct lobbying) 37 38 Total lobbying expenditures (add lines 36 and 37) 38 39 Other exempt purpose expenditures 39 40 Total exempt purpose expenditures (add lines 38 and 39) _ 40 41 Lobbying nortaxable amount Enter the amount from the following table
It the amounl'on line 40 is - The lobbying nontaxable amount Is - Not over $500,070 20% of we amount on line 40 Over $500,000 taut not over E1,000,000 $100,000 plus 15% of the excess over $500,000 Over $1,000,00() but not over $1,500,000 $175,000 plus 10% of the excess over $1,000,000 41 Over $1,500,00(1 but not over $17,000,000 _ $225,000 plus 5% of the excess over $1,500,000 Over $17,000,000 _ $1,000,000
42 Grassroots nontaxable amount (enter 25% of line 41) _ 42
43 Subtract line 42 from line 36 Enter -0- if line 42 is more than line 36 . 43 44 Subtract line 41 from line 38 Enter -0- if line 41 is more than line 38 44
Caution . If there is an amount on either line 43 or line 44, you must file Form 4720
4-Year Averaging Period Under Section 501(h) (Some organizations that made a section 501(h) election do not have to complete all of the five columns
i below See the instructions for lines 45 through 50 on page 11 of the instructions )
Lobbying Expenditures During 4-Year Averaging Period N/A Calendar year (or (a) (b) W (d) (e) fiscal year begin ning in) 10. 2002 2001 2000 1999 Total
45 Lobbying nontaxable amount

(i) Cash 51a(i) X (u) Otherassets a(ii) X Other transactions (i) Sales or exchanges of assets with a nonchantable exempt organization b(l) X (ii) Purchases of assets from a nonchantable exempt organization b(if) X (iii) Rental of facilities, equipment, or other assets b(iii) X (iv) Reimbursement arrangements b(iv) X (v) Loans or loan guarantees _ h (v) X
(vi) Performance of services or membership or fundraising solicitations b(vi) X Sharing of facilities, equipment, mailing lists, other assets, or paid employees c X If the answer to any of the above is 'Yes,' complete the following schedule Column (b) should always show the fair market value of the goods, other assets, or services given by the reporting organization If the organization received less than fair market value in any
52 a Is the organization directly or indirectly affiliated with, or related to, one or more tax-exempt organizations described in section 501 (c) of the Code (other than section 501(c)(3)) or in section 5279 . 01 El Yes No
223151 Schedule A (Form 990 or 990-EZ) 2002 01-22-03
11280511 758898 861 2002 .09000 OTERO COUNTY HOSPITAL ASSOC 861
' OTERO COUNTY HOSPITAL ASSOCIATION Schedule A (Form 990 or 990-EZ) 2002 DBA GERALD CHAMPION REGIONAL MED . CENTER 85-0138775 Page 6 ParF Vtf Information Regarding Transfers To and Transactions and Relationships With Noncharitable
Exempt Organizations (See page 12 of the instructions 51 Did the reporting organization directly or indirectly engage in any of the following with any other organization described m section
501(c) of the Code (other than section 501(c)(3) organizations) or in section 527, relating to political organizations a Transfers from the reporting organization to a noncharitable exempt organization of Yes No
12

ACTIVITY GROSS KIND AND LOCATION OF PROPERTY NUMBER RENTAL INCOME
DOCTOR OFFICES AT MEDICAL CENTER 1 406,576 . CONFERENCE ROOM RENTALS AT MEDICAL CENTER 2 1,120 .
TOTAL TO FORM 990, PART I, LINE 6A 407,696 .
FORM 990 ~ GAIN (LOSS) FROM PUBLICLY TRADED SECURITIES STATEMENT 2
GROSS COST OR EXPENSE NET GAIN SALES PRICE OTHER BASIS OF SALE OR (LOSS)
5,043,960 . 0 . <370,515 .>
2,822,989 . 0 . 2,151 . 2,667,421 . 0 . <30,550 .>
10,534,370 . 0 . <398,914 .>
4,673,445 .
2,825,140 . 2,636,871 .
10,135,456 .
16 STATEMENT(S) 1, 2 2002 .09000 OTERO COUNTY HOSPITAL ASSOC 861 1 16200511 758898 861
,OTERO COUNTY HOSPITAL ASSOCIATION DBA GE 85-0138775
?ORM 990 RENTAL INCOME STATEMENT 1
DESCRIPTION,I
WELLS FARGO INV . MGMT . ACCT . JP MORGAN BOND FUND ACCT . WELLS FARGO ACCT .
TO FORM 990, PART I, LINE 8

I
,OTERO COU~TY HOSPITAL ASSOCIATION DBA GE 85-0138775
FORM 990 I, INCOME AND COST OF GOODS SOLD STATEMENT 3 INCLUDED ON PART I, LINE 10
INCOME
1 . GROSS RECEIPTS . . . . . 2 . RETURNS'AND ALLOWANCES . . . . . . . . . . . 3 . LINE 1 LESS LINE 2 . . .
4 . COST OF~GOODS SOLD (LINE 13) . . . . . . . . 5 . GROSS PROFIT (LINE 3 LESS LINE 4) . . . . .
COST OF GOODS SOLD
6 . INVENTORY AT BEGINNING OF YEAR . . . . . . . 7 . MERCHANDISE PURCHASED . . . . . . . . . . . 8 . COST OF ~LABOR . . . . . 9 . MATERIALS AND SUPPLIES . . . . . . . . . . .
10 . OTHER COSTS . . . . . . 11 . ADD LINES 6 THROUGH 10 .
12 . INVENTORY AT END OF YEAR 13 . COST OF~GOODS SOLD (LINE 11 LESS LINE 12) . .
5,442,281
5,442,281
I 17 STATEMENT S) 3 11280511 7513898 861 2002 .09000 OTERO COUNTY HOSPITAL ASSOC 861 1
20,509,485
5,442,281
20,509,485
15,067,204
5,442,281

FORM 990 I OTHER EXPENSES STATEMENT 5
FUNDRAISING
<5,442,281 .> <5,442,281 .>
8,040,663 . 1,141,342 . 6,899,321 . TOTAL TO FM 990, LN 43
CHARITABLE OTHER GRANTS LESS ALAMOGORDO, NM NONE THAN $1,000 1,550 .
i
i 18 STATEMENT S) 4, 5, 6 11280511 758898 861 2002 .09000 OTERO COUNTY HOSPITAL ASSOC 861 1
.OTERO COUNTY HOSPITAL ASSOCIATION DBA GE 85-0138775
FORM 990 OTHER CHANGES IN NET ASSETS OR FUND BALANCES STATEMENT 4
DESCRIPTION AMOUNT
UNREALIZED GAINS - SECURITIES 604,437 . IMPAIRMENT OF ASSETS 121,725 .
TOTAL TO FORM 990, PART I, LINE 20 726,162 .
DESCRIPTION
PHYSICIAN FEES BAD DEBTS ADVERT I S IN(; QUALITY ASSURANCE SOFTWARE LICENSING INSURANCE TAXES & LICENSES PHYSICIAN RECRUITING PROFESSIONAL DUES CASUALTY CLAIMS OUTSIDE SERVICES MISCELLANEOUS LESS COST 4F GOODS SOLD OF INVENTORY
(A) (B) (C) PROGRAM MANAGEMENT
TOTAL SERVICES AND GENERAL
1,124,330 . 1,096,155 . 28,175 . 4,104,217 . 0 . 4,104,217 .
109,782 . 2,893 . 106,889 . 36,773 . 33,666 . 3,107 . 34,404 . 9,094 . 25,310 .
573,254 . 12,600 . 560,654 . 113,099 . 0 . 113,099 . 872,325 . 0 . 872,325 . 41,089 . 0 . 41,089 . 33,811 . 8,272 . 25,539 .
6,379,348 . 5,360,431 . 1,018,917 . 60,512 . 60,512 .
(D)
FORM 990 ; CASH GRANTS AND ALLOCATIONS STATEMENT 6
DONEE'S CLASSIFICATION DONEE'S NAME DONEE'S ADDRESS RELATIONSHIP AMOUNT
CHARITABLE UNITED WAY ALAMOGORDO, NM NONE 5,500 .
CHARITABLE I GCRMC FOUNDATION ALAMOGORDO, NM NONE 30,000 .
CHARITABLE FLICKENGER CENTER ALAMOGORDO, NM NONE 1,000 .

I
,OTERO COUNTY HOSPITAL ASSOCIATION DBA GE
CHARITABLE ~ AMERICAN CANCER ALAMOGORDO, NM SOCIETY
CHARITABLE i C .O .P .E . ALAMOGORDO, NM
CHARITABLE I MARCH OF DIMES ALAMOGORDO, NM
TOTAL INCLUDED ON FORM 990, PART II, LINE 22 40,550 .
FORM 990 GOVERNMENT SECURITIES STATEMENT 7
DESCRIPTION
US TREASURYi NOTES AND BONDS
TOTAL TO FORM 990, LINE 54, COL B
TOTAL GOV T SECURITIES
14,302,693 .
14,302,693 .
U .S . GOVERNMENT
14,302,693 .
14,302,693 .
STATE AND LOCAL GOV T
11280511 758898 861 19 STATEMENT S) 6, 7
2002 .09000 OTERO COUNTY HOSPITAL ASSOC 861 1
85-0138775
NONE 1,000 .
NONE 500 .
NONE 1,000 .

,OTERO COUNTY HOSPITAL ASSOCIATION DBA GE 85-0138775
FORM 990 TAX-EXEMPT BOND LIABILITIES OUTSTANDING STATEMENT 8
UNEXPENDED BOND TYPE OF
PROCEEDS FORM 8038 FILED
0 . FORM 8038
FORM 8038 DATE
THIRD PARTY INFORMATION
TOTAL INCLLJDED ON FORM 990, PART IV, LINE 64A 13,015,000 .
2 0 STATEMENT S) 8 2002 .09000 OTERO COUNTY HOSPITAL ASSOC 861 1 11280511 758898 861
PURPOSE OF ISSUE
SERIES 1997~HOSPITAL REVENUE BONDS
PROJECT ORIGINP;L ISSUE COMPLETION
AMOUNT DATE
17,950,000 . 12/ /00
ISSUE DATE
12/30/97
AMOUNT OF ISSUE
' OUTSTANDING
13,015,000 .

.OTERO BOUNTY HOSPITAL ASSOCIATION DBA GE 85-0138775
FORM 990 OTHER NOTES AND LOANS PAYABLE STATEMENT 9
LENDER'S NAME TERMS OF REPAYMENT
SECURITY PROVIDED BY BORROWER PURPOSE OF LOAN
COMPUTER EQUIPMENT
RELATIONSHIP OF LENDER
NONE
NONE
DESCRIPTION OF CONSIDERATION FMV OF
CONSIDERATION BALANCE DUE
0 . 3,172,052 .
TOTAL INCLUDED ON FORM 990, PART IV, LINE 64, COLUMN B 3,173,289 .
21 STATEMENT S) 9 11280511 758898 861 2002 .09000 OTERO COUNTY HOSPITAL ASSOC 861 1
LEASING 1 $1251 MONTHLY EQP LEASE ASSOCIATES/BARRINGTON
DATE OF MATURITY ORIGINAL INTEREST NOTE ,DATE LOAN AMOUNT RATE
10/10/00 10/10/03 39,648 . .00%
DESCRIPTION OF CONSIDERATION
LENDER'S NlME TERMS OF REPAYMENT
ALAMOGORDO FEDERAL $68,698 MONTHLY SAVINGS & I~OAN
I DATE OF MATURITY ORIGINAL INTEREST NOTE DATE LOAN AMOUNT RATE
11/01/02 l0/01/07 3,600,000 . 5 .40%
SECURITY PROVIDED BY BORROWER PURPOSE OF LOAN
REAL ESTATE
RELATIONSHIP OF LENDER
FMV OF CONSIDERATION BALANCE DUE
0 . 1,237 .

22 STATEMENT S) 10, 11, 12 11280511 758898 861 2002 .09000 OTERO COUNTY HOSPITAL ASSOC 861 1
,OTERO COUNTY HOSPITAL ASSOCIATION DBA GE 85-0138775
FORM 990 ; OTHER LIABILITIES STATEMENT 10
DESCRIPTION AMOUNT
ACCRUED INTEREST ON BONDS PAYABLE 336,348 . ESTIMATED THIRD-PARTY PAYOR LIABILITY 300,000 .
TOTAL TO FORM 990, PART IV, LINE 65, COLUMN B 636,348 .
FORM 990 OTHER REVENUE NOT INCLUDED ON FORM 990 STATEMENT 11
DESCRIPTIODI AMOUNT i
IMPAIRMENT OF ASSET, CHANGE IN ESTIMATE IDLE PROPERTY DEMOLITON 121,725 . COST OF INVENTORY SOLD 5,442,281 .
TOTAL TO FORM 490, PART IV-A 5,564,006 .
FORM 990 OTHER EXPENSES NOT INCLUDED ON FORM 990 STATEMENT 12
DESCRIPTIOtd AMOUNT
COST OF IN1IENTORY SOLD 5,442,281 .
TOTAL TO FARM 990, PART IV-B 5,442,281 .
i I

2 3 STATEMENT S) 13 11280511 7-58898 861 2002 .09000 OTERO COUNTY HOSPITAL ASSOC 861 1
i
.OTERO COUNTY HOSPITAL ASSOCIATION DBA GE 85-0138775
FORM 990 ! PART V - LIST OF OFFICERS, DIRECTORS, STATEMENT 13 TRUSTEES AND KEY EMPLOYEES
EMPLOYEE TITLE AND COMPEN- BEN PLAN EXPENSE
NAME AND ADDRESS AVRG HRS/WK SATION CONTRIB ACCOUNT
NORM ARNOLD CHAIRMAN OF THE BOARD 401 ROYCE AVE . 5 16,100 . 0 . 0 . ALAMOGORDO, . NM 88310
JIGGER OLSE;N SECRETARY 2493 DESERT HILLS DRIVE 3 0 . 0 . 0 . ALAMOGORDO,; NM 88310
JAIME ANDERSON BOARD MEMBER 710 MARYLAND 1 0 . 0 . 0 . ALAMOGORDO, NM 88310
ARTHUR AUSTIN, MD VICE CHAIRMAN 1101 9TH STREET 3 0 . 0 . 0 . ALAMOGORDO, NM 88310
FRED BAKER BOARD MEMBER 3000 HOPI TRAIL 2 0 . 0 . 0 . ALAMOGORDO,~ NM 88310
ROBERT HAMILTON BOARD MEMBER 1614 LA LUl PLACE 1 0 . 0 . 0 . ALAMOGORDO,~ NM 88310
JAMES HARRIS BOARD MEMBER P .O . BOX 3E0 1 0 . 0 . 0 . ALAMOGORDO,, NM 88311
BILL MERSHON BOARD MEMBER P .O . BOX 54 3 0 . 0 . 0 . MAYHILL, NM 88339
GREGORY RIC:HARDSON, MD BOARD MEMBER 1100 10TH STREET 1 0 . 0 . 0 . ALAMOGORDO, NM 88310
GARY JACKSON, DO BOARD MEMBER 211 SUDDER7'H DRVIE 1 0 . a . 0 . RUIDOSO, NM 88345
CECILIA ESTRADA ASHE BOARD MEMBER 500 E . 10TH ST 1 0 . 0 . 0 . ALAMOGORDO, . NM 88311

24 STATEMENT S) 13, 14 11280511 758898 861 2002 .09000 OTERO COUNTY HOSPITAL ASSOC 861 1
R I
,OTERO COUNTY HOSPITAL ASSOCIATION DBA GE 85-0138775
BILL MAYTON', BOARD MEMBER P 0 BOX 983, 1 0 . 0 . 0 . ALAMOGORDO,,NM 88310
CARL W . MAN,TEY CEO 1816 ARIZONA AVE . 40+ 193,000 . 50,245 . 7,260 . ALAMOGORDO,~NM 88310
JAMES A . KEELER CFO 644 EAGLE DR . 40+ 135,643 . 39,883 . 0 . ALAMOGORDO,~NM 88310
TOTALS INCLUDED ON FORM 990, PART V 344,743 . 90,128 . 7,260 .
i i
FORM 990 PART IX STATEMENT 14 INFORMATION REGARDING TAXABLE SUBSIDIARIES
NAME, ADDRESS & ID NUMBER PCT NATURE OF TOTAL END-OF-YEAR OF CORP OR PARTNERSHIP OWN BUSINESS INCOME ASSETS
WHITE SANDS~HEALTH CARE SYSTEMS, LLC . 50 .00% MANAGED CARE 234,205 . 395,712 . 1209 9TH STREET, ALAMOGORDO, NM 88310 85-0438529

Signature and Verification Under penalties of penury, I declare that I have examined this form, including accompanying schedules and statements, and to the best of my knowledge and belief, it is true, correct,,and complete, and that I am authorized to prepare this form
Date ature " l~ Notice to Applicant - To Be Completed by the IRS
We have approved this application . Please attach this form to the organization's return . D e have-not approved this application . However, we have granted a 10~day grace period from the later of the date shown below or the due
date of the organization's return (including any prior extensions) . This grace period is considered to be a valid extension of time for elections otherwise required to be made on a timely return . Please attach this form to the organization's return . L~s -(+~~ We have'not approved this application . After considering the reasons stated in item 7, we cannot grant your request for a e/xVt~fiblal{Afrtune to file . We are not granting the 10~day grace period . rt~~~OV~O
0 We cannot consider this application because it was filed after the due date of the return for which an extension was req c G_e&BJ . t~
Other - 1 C/Nn. ~~ 4 ?~n~ ~ZiBMIS EOpF S/(~yPR
ISKC ~~CD
Date "'u/h By
Director
Alternate Mailing Address - Enter the address if you want the copy of this application for an additional 3-month extension returned to an address different than the one entered above .
Name AC COUNTING & CONSULTING GROUP, L .L .P .
Type Number and street (include suite, room, or apt . no .) Or a P.O . box number or print 1P .O . DRAWER JJ
223832 City or town, province or state, and country (including postal or ZIP code)
oszz-oz C~~RLSBAD, NM 88221-7527 Form 8868 (12-2000)
10320213 758898 861 2002 .09000 OTERO COUNTY HOSPITAL ASSOC 861 1
. . r
Form 8868 (12-2000) Page 2 0 If you are filiig for an Additional (not automatic) 3-Month Extension, complete only Part II and check this box " X Note : Only complete Part II if you have already been granted an automatic 3-month extension on a previously filed Form 8868. 0 If you are fili ng for an Automatic 3-Month Extension, complete only Part I (on page 1) . Pad 11 Additional (not automatic) 3-Month Extension of Time - Must file Original and One Copy.
Name of Exempt Organization Employer identification number Type or TERO COUNTY HOSPITAL ASSOCIATION print. BA GERALD CHAMPION REGIONAL MED . CENTER 85-0138775 File by the excendea Number, street, and room or suite no . If a P .O . box, see instructions . For IRS use only due date for 2669 NO . SCENIC DR filing the return see City, town or post office, state, and ZIP code For a foreign address, see instructions . '"S"""'°"5 AMOGORDO, NM 88311-0597 Check type of return to be filed (File a separate application for each return) : D Form 990 F I Form 990-EZ ~ Form 990-T (sec 401(a) or 408(a) trust) ~ Form 1041-A ~ Form 5227 0 Form 8870 D Form 990-BL 0 Form 990-PF ~ Form 990~T (trust other than above) 0 Form 4720 ~ Form 6069
STOP: Do not complete Part II if you were not already granted an automatic 3-month extension on a previously filed Form 8868 .
" If the organization does not have an office or place of business in the United States, check this box a If this is for a Group Return, enter the organization's four digit Group Exemption Number (GEN) . If this is for the whole group, check this box " = . If it is for part of the group, check this box " 0 and attach a list with the names and EINs of all members the extension is for .
4 I request an additional 3-month extension of time until MAY 1 '] . 9n n a
. 5 For calendar year , or other tax year beginning L 1 r 2 0 2 and ending JUN 30 , 6 If this tar, year is for less than 12 months, check reason : D Initial return ~ Final return ~ Change in accounting period 7 State in detail why you need the extension
ADDI'PIONAL TIME IS NEEDED TO GATHER ALL THE NECESSARY INFORMATION TO PREPARE A COMPLETE AND ACCURATE TAX RETURN .
8a If this application is for Form 990-BL, 990~PF, 990-T, 4720, or 6069, enter the tentative tax, less any nonrefundable credits . See instructions $
b If this application is for Form 990-PF, 990~T, 4720, or 6069, enter any refundable credits and estimated tax payments made . Include any prior year overpayment allowed as a credit and any amount paid previously with Form 8868 $
c Balance Due. Subtract line 8b from line Sa Include your payment with this form, or, if required, deposit with FTD coupon or, if required, by using EFTPS (Electronic Federal Tax Payment System) . See instructions $ N/A

LHA For Pap erw9fic Reduction Act Notice, see instruction Form 888 (12-2000)
223831 OS-01-02
15011020 758898 891 2002 .06010 nTER0 C'niTNTY HOSPITAL ARROf R91 1
a
r
Form gggg Application for Extension of Time To File an (December 2000) Exempt Organization Return OMB No 15451709 Department of the Treasury Internal Revenue Ser vice 1 File a separate application for each return .
" If you are filing for an Automatic 3-Month Extension, complete only Part 1 and check this box . . . . . . . . . . " If you are filing for an Additional (not automatic) 3-Month Extension, complete only Part II (on page 2 of this form) . Note : Do not complete Part II unless you have already been granted an automatic 3-month extension on a previously filed Form 888.
Part 1 automatic 3-Month Extension of Time - Only submit original (no copies needed)
Note : Form 9901-T corporations requesting an automatic 6-month extension - check this box and complete Part I only C] All other corporations including Form 990-C filers) must use Form 7004 to request an extension of time to file income tax returns . Partnerships, REMICs and busts must use Form 8 736 to request an extension of time to file Form 1065, 1066, or 1041 .
Type or Name of Exempt Organization Employer identification number print OTERO COUNTY HOSPITAL ASSOCIATION
DBA GERALD CHAMPION REGIONAL MED . CENTER 85-0138775 File by the die date for Number, street, and room or suite no . If a P.O . box, see Instructions . filing your 26 69 NO . SCENIC DR return See instructions City; town or post office, state, and ZIP code . For a foreign address, see instructions .
AL.AMOGORDO, NM 88311-0597 Check type of return to be filed (file a separate application for each return) :
Form 990 ~ 0 Form 990-T (corporation) 0 Form 4720 [] Form 990-HL 0 Form 990-T (sec . 401(a) or 408(a) trust) 0 Form 5227 0 Form 990.11 ~ Form 990-T (trust other than above) ~ Form 6069 [~ Form 990-f'F ~ Form 1041-A 0 Form 8870
" If the organization does not have an office or place of business in the United States, check this box , . . . . . . . . � , �� . . . . . . �� , � " If this is for a Group Return, enter the organization's four digit Group Exemption Number (GEN) . If this is for the whole group, check this box 1 0 . If it is for part of the group, check this box 1 = and attach a list with the names and EINs of all members the extension will cover .
1 I request an automatic 3-month (6-month, for 990-T corporation) extension of time until FEBRUARY 17, 200 4 . to file the exempt organization return for the organization named above . The extension is for the organization's return for: 10 calandar year or " FX1 tax year beginning JUL 1, 2002 , and ending JUN 3 0 , 2 0 0 3
2 If this tax year is for less than 12 months, check reason : 0 Initial return ~ Final return 0 Change in accounting period
3a If this application is for Form 990-BL, 990-PF, 990~T, 4720, or 6069, enter the tentative tax, less any nonrefundable credits . See instructions , � . . _ . . . . . . . . . . . . . , . . , . $
b If this application is for Form 990-PF or 990-T, enter any refundable credits and estimated tax payments made . Include any prior year overpayment allowed as a credit . , � , � , , . . . . . . $
c Balance Die . Subtract line 3b from line 3a . Include your payment with this form, or, if required, deposit with FTD coupon or, if required, by using EFTPS (Electronic Federal Tax Payment System) . See instructions �� . , ., . $ N/A
Signature and Verification
Under penalties of perjury, I declare that I have examined this form, including accompanying schedules and statements, and to the best of my knowledge and belief, it is true, correct, and complete, and that I am authorized to prepare this form.