Options for surgical trials in vulva cancer. Henry Kitchener, University of Manchester ANZGOG, March...
14
Options for surgical trials in vulva cancer. Henry Kitchener, University of Manchester ANZGOG, March 2013
-
Upload
emory-bennett -
Category
Documents
-
view
218 -
download
2
Transcript of Options for surgical trials in vulva cancer. Henry Kitchener, University of Manchester ANZGOG, March...

Options for surgical trials in vulva cancer.
Henry Kitchener, University of ManchesterANZGOG, March 2013

Role of surgery in early vulval cancer
To effect a cure by preventing recurrence.
Small tumours (straightforward)
Large tumours (more complex)
To preserve vulval function and avoid chronic lymphoedema.

Aims of surgery To excise the primary tumour and
minimise risk of local recurrence
To excise groin nodes (uni or bilateral)
To stage, in order to plan adjuvant treatment, assess margins
To avoid disfigurment
Conservation of function
Plastic procedures
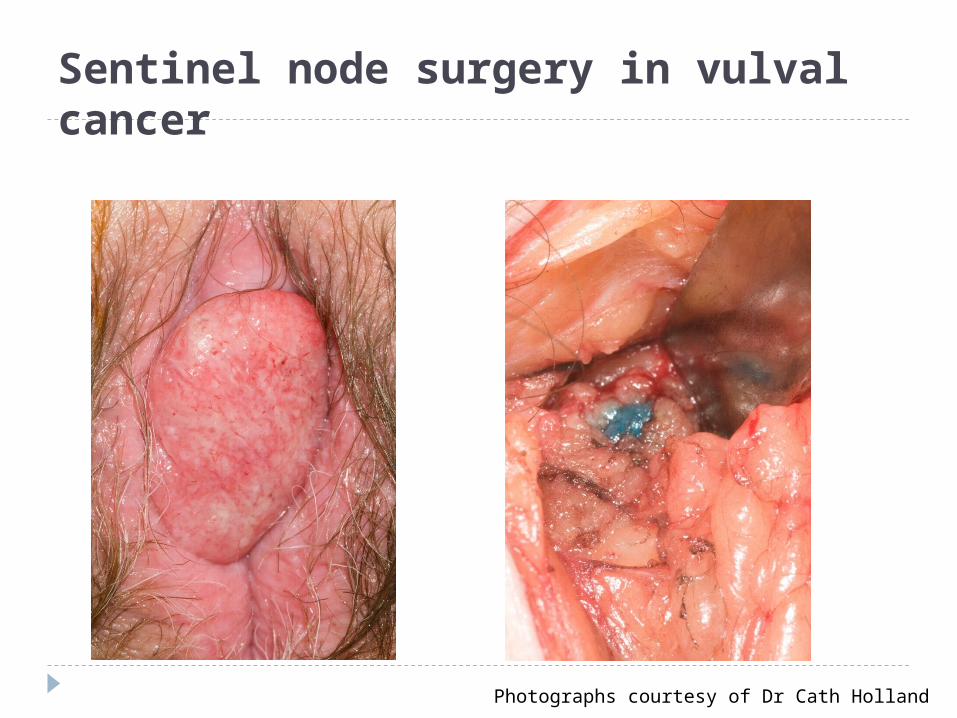
Sentinel node surgery in vulval cancer
Photographs courtesy of Dr Cath Holland

Evidence base from Cochrane Reviews of surgery for VIN and early cancer. VIN. (Pepas et al, 2011) One RCT of laser vs ultrasonic surgical aspiration. 30 patients; underpowered for primary outcome.
Early cancer (Ansink et al 1999) No adequate RCT’s. 3 observational studies. Radical local excision is safe (margin >8mm) Contralateral groin node dissection is unnecessary in
lateralised disease. Superficial groin node dissection is unsafe.
Note: Some studies rejected because early cancer could not be separated, and treatment not uniform.

Track record of surgical research in vulval cancer. Generally sparse Lack of RCT’sBut Surgery has been improved greatly by
incremental change Triple incision in the 1980’s Ipsilateral groin node dissection in the 1990’s Sentinel node dissection in the 2000’s
Approach has been “Innovate without increasing hazard”

Vulval cancer surgery
1960's 1980's 2000's
More radical
Enbloc radical vulvectomy (Way)

Challenges for surgical trials in vulval cancer.
Disease is rare
Survival is generally good
Many cases are easily managed
In problem cases, surgery may not be the solution

Vulval cancer: What do we know? It exists in two forms
HPV related (basiloid)
Lichen sclerosis related (differentiated)
Basiloid
Preceded by VIN3 whereas (differentiated) arises more spontaneously
May be more widespread and difficult to resect conservatively
Trend has been toward younger women (HPV, smoking)
HPV vaccination will protect

Vulval cancer: What else do we know?
Disease presents at an earlier age.
40-50% are HPV related.
Groin node dissection and RXT can result in considerable morbidity.
Sentinel node detection could avoid the need for most groin node dissections.
Chemoradiation can achieve dramatic responses but can have marked late effects
Role of surgery in VIN 3
To deal effectively with VIN 3 Unifocal (easy) Multifocal (difficult)
To preserve vulval function May not be feasible with widespread disease
and there is a risk of recurrence.
But, would anti-HPV strategies be more effective?

Antiviral Therapy
Imiquimod HPV Vaccines Photodynamic therapy
50 – 60% response rates Need to get rid of HPV 16

Trial in VIN3Problem: Widespread VIN3
Hypothesis: Eradication of widespread VIN3 may be facilitated by antiviral therapy followed by completion surgery
Intervention: Antiviral therapy followed by surgery
Control: Antiviral therapy
Outcome: Time to progression
Power: Based on superiority (based on 50% recurrence)

Conclusion
VIN3/vulval cancer surgical trials are challenging.
Need GCIG collaboration.
Role of completion surgery following antiviral therapy offers a potential trial setting