Opportunistic Infection Updates, 2018 -...
49
Opportunistic Infection Updates, 2018 Richard A. Murphy, MD, MPH Harbor-UCLA Medical Center Geffen School of Medicine at UCLA
Transcript of Opportunistic Infection Updates, 2018 -...

Opportunistic Infection Updates, 2018
Richard A. Murphy, MD, MPH
Harbor-UCLA Medical Center
Geffen School of Medicine at UCLA

Objectives
1. Describe context for persistence of OIs globally
2. Provide updates on the diagnosis & treatment of OIs

Deaths in HIV-infected persons with advanced HIV disease
Despite the number receiving ART >20 million globally, total deaths in those with advanced HIV have declined slowly Total number on ART
Number of deathsin advanced HIV
Nu
mb
er
of
de
ath
s, m
illio
ns
Calmy et al CID 2018:66 (Suppl 2)
Year

What proportion of patients begin ART with very advanced disease with CD4 cell count <100 in South Africa today?
1. 1 in 10 patients
2. 1 in 5 patients
3. 1 in 2 patients
4. None of the above

Patients are presenting to care with advanced HIV in South Africa
• Nationwide lab data from South Africa (NHLS)• % entering care with CD4
<100 estimated (red)
• From 2005-11, % entering care w/ CD4<100 declined
• From 2011 on, % starting ART w/ CD4<100 not • 2016: 17% CD4<100
• Men 2x as likely as women
Clin Infect Dis. 2018 Apr 1; 66(Suppl 2)

RFs for late presentation with advanced HIV in SA
• In 35 PHCs from 3 high burden districts in SA, >12,000 newly diagnosed patients during 2014-15
• 33% had CD4 < 200 at 1st visit
• Risk factors for presentation with CD4<200:• >50 years old, OR 3.4 (95% CI: 2.3-4.9)
• Male, OR 2.7 (95% CI: 1.5-4.9)
• Accessing care in urban inner city or urban township ~ OR 1.5
• Very late presentation in SA overly represented by older males, accessing care in urban inner cities and townships
Fomundam HN, et al. SAMJ 2018

Other reasons we still see patients with advanced HIV & OIs
- Not all with HIV receive continuous care- Reasons include migration, incarceration, mental illness
- Not all on ART achieve durable virologic suppression- Inadequate adherence in certain patient subgroups
- Failure from drug resistance with NNRTI-based regimens
https://www.cdc.gov/mmwr/volumes/67/wr/mm6701a6.htm?s_cid=mm6701a6_w#modalIdString_CDCTable_0

Advanced HIV disease in African hospitals:Most patients are ART-experienced
• Homa Bay, Kenya (N=338) prospective study of HIV-infected admitted:• 85% aware of HIV status at admission
• 65% ART-experienced
2/3 receiving ART failing with VL>1000
• Recent Edendale, SA prospective study of HIV-infected admitted: • 84% aware of status
• 79% were currently taking ART
Ousely et al CID 2018:66 (Suppl 2)
Homa Bay City, Kenya
Gupta-Wright et al Lancet 2018; 392: 292–301
• One contributors may be under-recognition in clinics of 1st line ART failure (VL > 1000)
• Multiple studies: Patients with 1st line failure not identified & switched promptly with switch delays of 4-6 months common• Why? Reporting delays, clinician switch
reluctance, poor patient follow-up
• Delayed 2nd line ART switch linked in 3 African countries with incr. risk of OI/ death
AIDS Res Hum Retroviruses. 2017 Dec;33(12):1181-1184.
ART-experienced patients with OIs in AfricaOne contributor? Late recognition of ART treatment failure
Cost ↓ for 2nd line regimens <$250/year
22nd IAC, Amsterdam
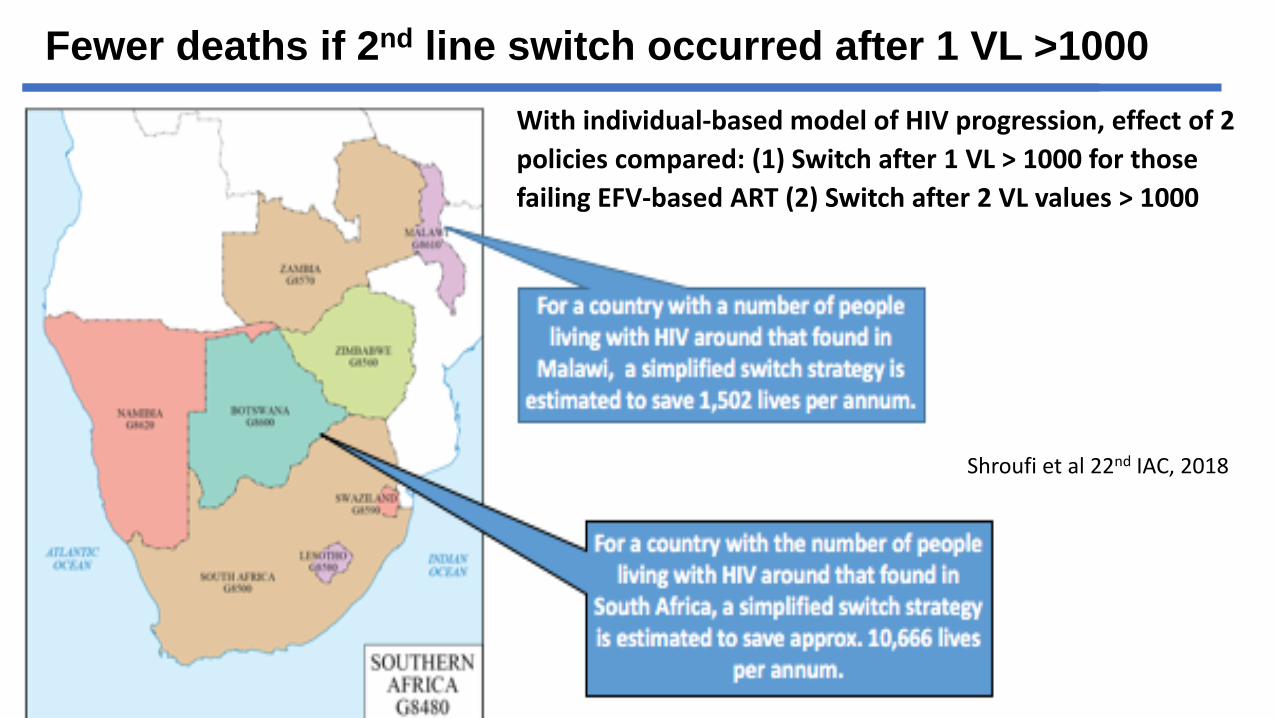
Fewer deaths if 2nd line switch occurred after 1 VL >1000
Shroufi et al 22nd IAC, 2018
With individual-based model of HIV progression, effect of 2
policies compared: (1) Switch after 1 VL > 1000 for those
failing EFV-based ART (2) Switch after 2 VL values > 1000
Case 1
• 26 yo HIV+ male with unknown CD4 count presents with 2 months of cough, fever and wt loss
• Previously on EFV-based first-line ART but no ART x 12 months and not taking cotrimoxazole.
• Over 24 hrs, acute on chronic shortness of breath
ID Images, 2006 Peter Lokken and Richard Murphy

Case 1
Exam
• HR 126, RR 26, Temp 37.5, BP 95/53, O2 96% RA
• + oral thrush, no rash, absent BS on L
Data
• WBC 14.5, Hb 11.6, PLT 298 and bicarb 14 mEq/L
• ABG: 7.47 / pCO2 26 mm Hg / pO2 161 mm Hg supplemental O2.
• EKG: Sinus tachycardia

Seriously ill HIV infected patientsadmitted in Cape Town with cough
• HIV-infected + cough any length hospitalized with >1 WHO danger sign
• N=484 (median CD4 89), 35% on ART at admission
• 12% died
• Linked with mortality: on ART at admission, unable to walk, low CD4• Among those on ART, 1/2 initiated within 6 months and 1/3
virologically failing
• Other WHO danger signs not linked w/mortality
Griesel et al. AIDS Res Ther (2018) 15:5
WHO Danger Signs:• Cannot stand• Temp >39C (102)• RR > 30• HR > 120
Medical officer discharge diagnosis:- TB (62%)- Pneumonia (52%)- PCP (10%)- Other (3%)

Making the diagnosis of PCP with few tools
• What available tests suggest PCP in adv. HIV admitted to hosp. (in absence of histological diagnosis or CT) ?
• PCP dx’ed by> 1000 copies/mL of DNA by PCR
• Probability of PCP:
Model Assuming Access to Pulse Oximetry:
4 pts (25%), 5 pts (42%), 6 pts (61%)
SAJHIVM. 2018;19(1), a851.
*Refer PCP to ICU? Cape Town: Mort. in PCP with resp. failure in ICU 60% with 98% intubated25% with TB coinfection. PCP mortality in ICU in SA similar to hi income (Chiliza N PLOS One, 2018)

Chest x-ray
What is the most likely diagnosis?
A. Pneumocystis pneumonia
B. Pulmonary tuberculosis
C. Pulmonary cryptococcosis
D. Pulmonary Kaposi’s sarcoma

Case 1
• Sputum samples revealed acid-fast bacilli
• What if the patient was not able to produce sputum?
• Any tests that could improve diagnostic yield if tuberculosis suspected in patient with CD4 < 100?

Added yield of urine LAM in HIV-infected inpatients
• RCT in S Africa + Malawi of consecutive inpatients with HIV
• N= 2600, 1/3 had CD4<100- Any CD4 cell count, no current TB Rx
- Standard arm: Sputum Xpert MTB/RIF
- Intervention: Sputum Xpert + urine LAM + urine Xpert
- 56-day mortality: No difference overall
- 40% confirmed TB, only LAM positive
- Among CD4<100 and in severe anemia, mortality was reduced 7%,with difference appearing after d/c
Ankur Gupta-Wright CROI 2018 Poster 1117
Low addedyield of urineXpert

Urine LAM Activism at IAC Amsterdam, 2018

Case 1
• A chest tube was placed.
• CD4 results: 78 cells/mm3

Case 1
• Four drug standard TB therapy was initiated with plan for initiation of ART within 2 weeks.
• What is the risk for immune reconstitution inflammatory syndrome (IRIS) in this patient and what can be done?

Paradoxical TB- IRIS
• Paradoxical TB-IRIS is a common complication when TB patients and low CD4 start on ART
• Meta-analysis:• Incidence ~18%
• Hospitalization in 25%
• TB IRIS-related mortality 2%
• Major RFs• Low CD4 cell count at ART start
• ART started rapidly after TB diagnosis, now standard of care with advanced HIV infection
Slide courtesy of Graeme Mentjes
Presents with new / recurrent inflammatory features typically in first 4 wks of ART
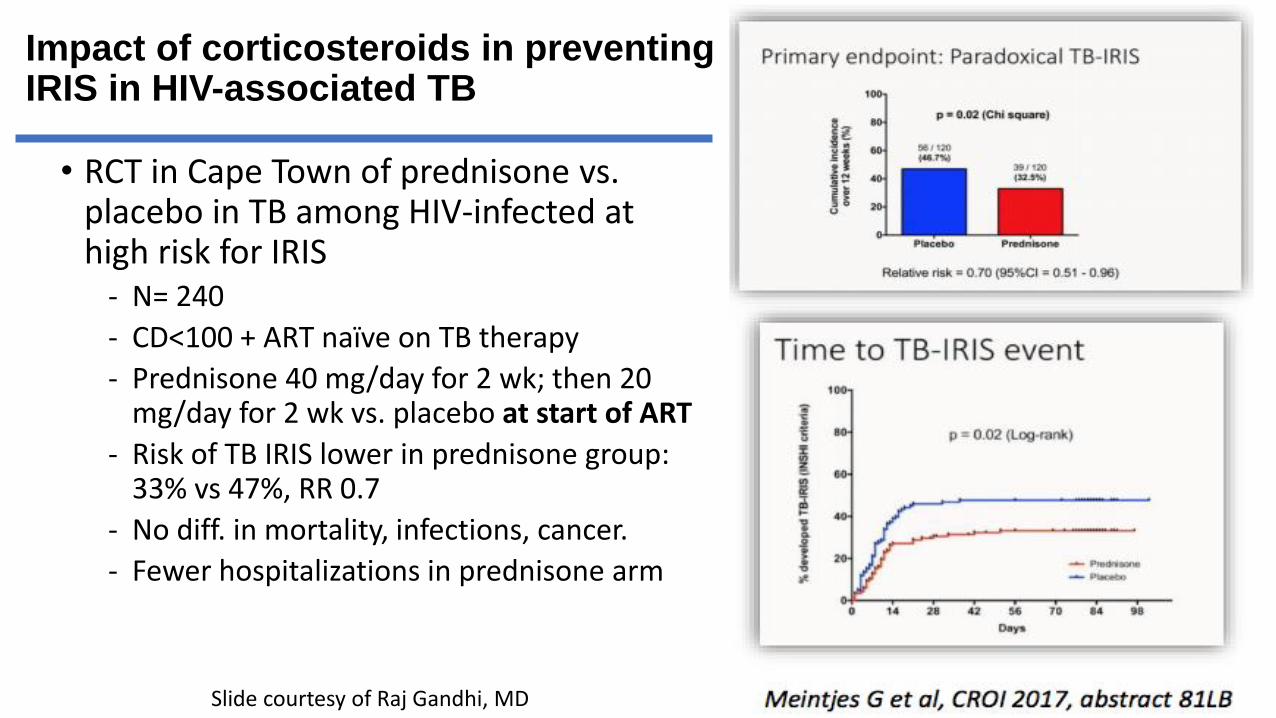
Impact of corticosteroids in preventing IRIS in HIV-associated TB
• RCT in Cape Town of prednisone vs. placebo in TB among HIV-infected at high risk for IRIS
- N= 240
- CD<100 + ART naïve on TB therapy
- Prednisone 40 mg/day for 2 wk; then 20 mg/day for 2 wk vs. placebo at start of ART
- Risk of TB IRIS lower in prednisone group: 33% vs 47%, RR 0.7
- No diff. in mortality, infections, cancer.
- Fewer hospitalizations in prednisone arm
Slide courtesy of Raj Gandhi, MD

Case 1
• With lung re-expansion, a parenchymal cavity was evident
• The patient was referred for outpatient ART
• ART was initiated 2 wks after initiation of TB therapy (without cortiosteroids)

Case 2
• 43 yo man comes to clinic with 2 weeks of HA, dizziness, and –according to family – rapid development of confusion
• 9 kg weight loss over 3 months
• No known PMH
• Rapid HIV test positive

Case 2
Exam:
• 37.2 HR 93 BP 118/70 RR 14 97% RA
• Tired but arousable and oriented
• No nuchal rigidity, non-focal neurological exam
Data:
• LP: 4 WBCs, 55 RBC. Glucose very depressed. Protein mildly elev.
• India ink stain positive
• Opening pressure 52 cm of H2O

Elevated intracranial pressure linked with poor outcomes in CCM but manometers not routinely available…

Using CSF flow rate during LP to measure ICP
• In Cape Town, 32 patients with CCM underwent 89 LPs with 22-G spinal needle.
• ICP was first measured with a manometer and then CSF flow rate in drops/min counted.
• Using 40 drops/minute cut-off, sensitivity was 91% for detecting raised ICP > 25 cm of H2O
• Only 5% of LPs misclassified with drop rate as “normal” when ICP actually elevated.
• When manometers not available, ICP can be accurately estimated with CSF drops/min with possible threshold of >40 drops/min.
J Acquir Immune Defic Syndr 2017;74:e64–e66

Case 2
• This patient (USA) received liposomal amphotericin B + 5-FC as initial induction therapy
• He received saline hydration (1 L NS) and K before IV dosing
• He developed acute renal failure by day 7 with GFR of 53 ml/min (reduced from 105 ml/min)

How common is acute kidney injury (GFR ↓ to <60 ml/min) in patients with CCM who receive amphotericin B deoxycholate and is there impact on subsequent mortality?
1. 20% develop AKI with no impact on mortality as AKI is reversible
2. 20% develop AKI with increased mortality
3. 40% develop AKI with no impact on mortality as AKI is reversible
4. 40% develop AKI with increased mortality

AKI common in CCM managed with AmB and↑mortality
• Substudy of large clinical trial of AmB + fluconazole in Uganda and SA. * AKI defined as CrCl of <60 ml/min
• AKI developed in ~40%; mean time to onset ~ 1 wk with RFs:
• Development of ↑ urine protein early on treatment
• Hi CD4Med. CD4: AKI (CD4 49) vs. No AKI (CD4 14)
• AKI was associated with mortality:
• AKI: 10 wk mort: 51% No AKI: 10 wk mort: 29% (P=0.01)
• All patients with severe AKI (GFR <30 ml/min) died
• In all those surviving, AKI fully resolved
Schutz C et al; OFID 2017
**SA recs: W/ onset of AKI (Cr 2x) - hold AmB + incr. saline hydration + monitorIf no improvement, cont. with (renal adjusted) fluconazole monotherapy
13 Govender et al SAJHIV Cryptococcal meningitis guidelines
Future rolefor 5-FC?

Induction treatment recommendations – S Africa
• 2 wks of AmB (1 mg/kg/day) plus fluconazole 800 mg/day
• Based in part on Viet. study in which this regimen had mortality similar to 4 wks of AmB monotherapy but had higher rates of CSF culture clearance
Day et al NEJM 368;14 April 4, 2013
The study also influenced WHO recs that recommended 2 wks of AmB + fluconazole
WHO now recommends 1 wkof AmB +5-FC for induction phase of treatment. Why?

ACTA CCM trial
• ACTA trial, N=721 with CCM randomized (median CD4 25) in Malawi, Zambia, Cameroon, Tanzania• Daily therapeutic LPs performed when OP elevated• Patients randomized to AmB received 1 L NS daily, K and Mg suppl.
• Pts randomized to oral regimen, 1 wk of AmB or 2 wks of AmB.
Next, AmB recipients randomized to flucon. or 5-FC.
- 1 Oral arm: - Fluconazole [1200 mg/day] + Flucytosine (5FC) [100 mg /kg/day] for 2 wks
- 4 IV arms :- 1 wk of amphotericin B (1 mg/kg/day) + oral drug- 2 wks of amphotericin B (1 mg/kg/day) + oral drug
Malloy SF et al NEJM 2018
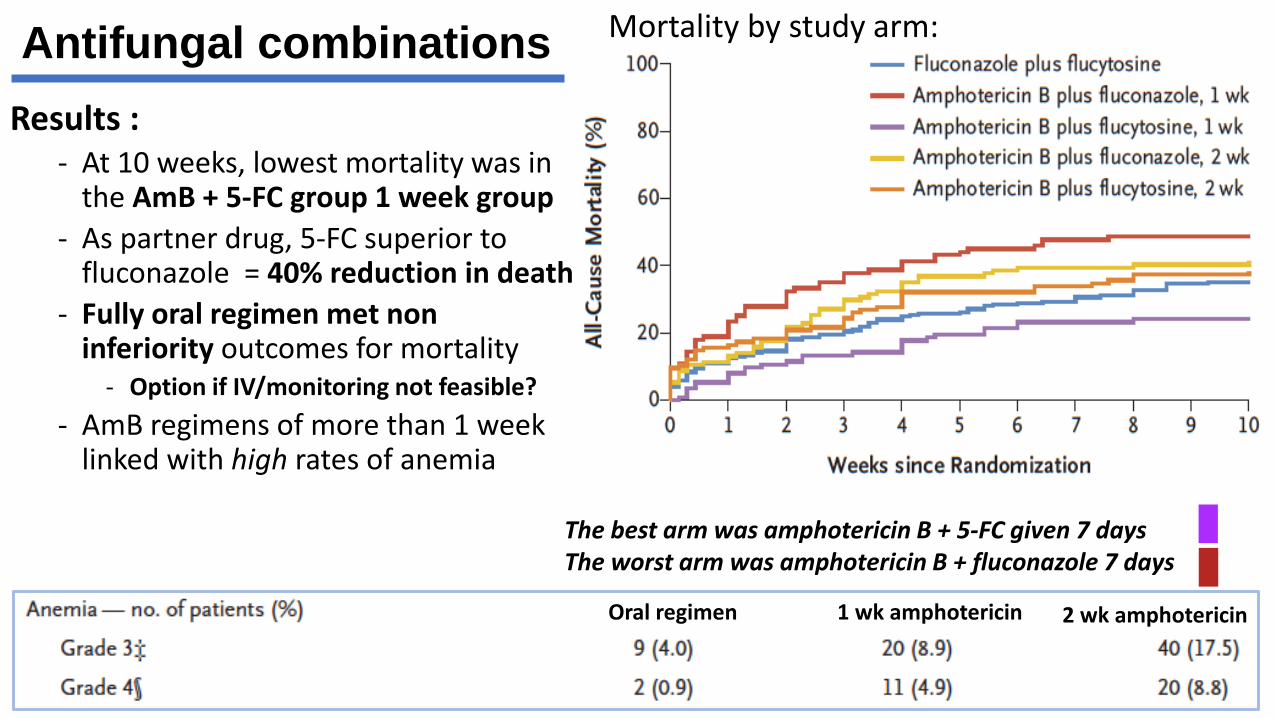
Antifungal combinations
Results :- At 10 weeks, lowest mortality was in
the AmB + 5-FC group 1 week group
- As partner drug, 5-FC superior to fluconazole = 40% reduction in death
- Fully oral regimen met non inferiority outcomes for mortality
- Option if IV/monitoring not feasible?
- AmB regimens of more than 1 week linked with high rates of anemia
Mortality by study arm:
The best arm was amphotericin B + 5-FC given 7 daysThe worst arm was amphotericin B + fluconazole 7 days
Oral regimen 1 wk amphotericin 2 wk amphotericin

Flucytosine (5-FC) access – where are we?
• 5-FC developed in 1957• Intracellular modification to 5-FU, joins fungal RNA, inhibits prot. synth.
• In lab, made during synthesis of FTC - off patent for decades !
• US cost $$$ = price manipulation by generic co’s - Valeant
• 5-FC access virtually non-existent in LMICs but may be changing• France: 5-FC sold by Meda Pharma $120 /14 days. Acquired by Mylan
• 2018: Mylan filed to register it with the WHO Prequalification Team (quality auditing for LMICs) opening door to broader access
• Mylan must register it in countries for 5-FC to become available
Next step is pushing for wider access to liposomal amphotericin B...

Case 2
• The patient has persistently elevated ICP of >30 cm of H2O
• After 2 weeks of induction therapy a VP shunt was placed
• The patient was demonstrated to be culture negative and was switched to fluconazole 400 mg/day as consolidation therapy.
• The plan was to initiate ART after 5-6 weeks

Question: After 2 wks of induction therapy with AmBand fluconazole, what proportion of patients still have positive CSF fungal culture with viable cryptococci?
A. 5%
B. 20%
C. 33-50%
D. None of the above

Fluconazole consolidation for CCM – 400 mg/day sufficient?
• After 2 wks of AmB-based induction, up to 50% have viable C. neoformans in CSF• CSF culture (+) after induction linked ↑ mort.
• As consolidation, fluc. 400 mg/day commonbut efficacy demonstrated after AmB + 5FC
• Impact of high-dose fluconazole consolidation tested in 2015 substudy• After induction, patients received fluconazole
800 mg/day until CSF sterile, median 40 days
Open Forum Infect Dis. 2015 Dec 28;2(4)
• With this strategy, relationship the mortality impact of (+) CSF culture at end of induction no longer observed and dosing was well tolerated• Mortality week 2-6, post induction CSF culture (+) 35% vs post induction CSF culture (-) 27%
Sterile CSF
Non-sterile CSF

A different consolidation paradigm until 5-FC is accessible?
Overall mortality through 48 weeks
AIDS Research and Hum Retro. Vol 34, No. 5, 2018
In the COAT study residually CSF (+) patients requireda median of 40 days of high dose fluconazole 800 mg/day

CrAg titer predicts CSF cryptococcal disease
• Ethiopian study, all serum CrAg positive patients were offered LP, not just symptomatic• CrAg <1:80 0% CSF CrAg positive
• CrAg 1:160 to 1:640 65% CSF CrAg positive
• CrAg >1:1280 100% CSF CrAg positive
• Significance of CNS symptoms in CrAg (+) patients?• 1/3 of CrAg (+) patients with CNS cryptococcal disease
had no symptoms; all had plasma CrAg >1:160CID 2018; 66 (S2) S152-9
Policy implications? May be worthwhile to calculate titers for plasma CrAg (+) and be more assertive with CSF eval. particularly for those with plasma CrAg of >1:160

Case 3
• 25 yo female HCW with a history of cough and fever initiated standard TB therapy based on CXR w/ LUL infiltrate + hilar LAN
• 4 wks into treatment, the patient had a seizure and was admitted.
• At admission the HIV status was not known. CT head was normal
• CSF: 4 PMLs/uL and 2 lymphs/uL, elevated protein, mildly depressed glucose, CrAg negative, no opening pressure
• TB meningitis was suspected

Absence of CSF pleocytosis in HIV-associated TB-M
• Background: Absence of pleocytosis common in CCM but can this be the case in TB meningitis?
• Cohort study, Uganda
• In 85 microbiologically-confirmed, HIV-associated TBM cases, 28 (33%) had <5 cells CSF and – in this group – mortality was 39%
• Combining cohorts in Uganda, Zimbabwe, Brazil and Vietnam absence of CSF pleocytosis in 12% of HIV-associated TB-M and was associated with poor prognosis
International Journal of Infectious Diseases 68 (2018) 77–78

Case 3
• The patient was found to be HIV-infected with a CD4 cell count of 42 cells/ul
• How can the diagnosis of TB-M be confirmed?

TB meningitis and Xpert MTB/RIF Ultra
• Prospective study of Xpert MTB/RIF Ultra, a re-engineered PCR-based assay
• N=129 HIV infected adults with suspected meningitis
• 22 of 129 diagnosed with TB-M by composite standard of any (+) micro test
• 21/22 cases captured by Xpert Ultra consistent with a 95% sensitivity.• Time to + result was 1 d vs med. 7 d for MGIT.
• Negative predictive value of Xpert Ultra was 99% (106 of 107 negative cases)• If the Xpert Ultra was negative, TB-M virtually
never present
Lancet Infect Dis 2018; 18: 68–75
22 patients with TB-M diagnosed by at least 1diagnostic test

Case 3
• The diagnosis of TB-M was suspected clinically.
• The patient initiated empirically on 4 drug anti-tuberculosis therapy + corticosteroids.

Other updates

Ready-to-use supplementary food in advanced HIV with TB
• Subjects: CD4<100 and underweight with TB coinfection
• Peanut-based RUSF 1000 kcal/day for 12 weeks vs. none.
• N=1805, median CD4 34 and with BMI <18.5 in 40%
• Despite greater weight gain, no effect on mortality at 24 or 48 wks• No benefit in those with lower BMI• It was not designed to look at impact on
retention and such an effect may existOverall mortality through 48 weeks
Mallewa J, et al The Lancet HIV , Volume 5 , 2018

Growth of AMR as a threat to patients with HIV-infection
• Lab-based study of blood cultures without patient-level information from 2 Ugandan hospitals; 2011 CLSI Standards followed
• 462 (14%) isolates grown from ~3,000 blood cultures
• Gram-positive isolates most commonly S. aureus• 1/3 of S. aureus were MRSA, only 4% sensitive to TMP/SMX
• Gram-negatives• Most common: E coli, 33% sensitive to ceftriaxone, 40%
sensitive to cipro
• Klebsiella, 15% sensitive to ceftriaxone, 23% sensitive to cipro
• Salmonella isolates, 50% MDR with resistance to 3 drug classes
Kajumbula et al EID 2018

Thanks for listening….
Special thanks for slides & advice to Yunus Moosa, Raj Gandhi, Graeme Meintjes
Resources:• SA HIV Clinicians Society
• Guideline for the prevention, diagnosis and management of cryptococcal meningitis among HIV-infected persons: (2013)
• DHHS • Guidelines for the Prevention and
Treatment of Opportunistic Infections in HIV-Infected Adults and Adolescents (2018)

Cryptococcal antigen (CrAg)screening
• WHO guidelines recommend CrAg screening in HIV with CD4<100• Ag detectable median 22 days before sxs
• Pre-emptive antifungal therapy for CrAg (+) HIV-infected patients prevents deaths
• Meta-analysis suggested that globally pooled prevalence of CrAg (+) is 6.5% in at CD4<100 and 2% in CD4 101-200• CrAg prevalence in inpatients higher (~10%)
versus outpatients (~6%)
• May be reasonable to revise CrAgscreening from CD4<100 to CD4<200 & perform routine inpatient CrAg screening
CID 2018; 66 (S2) S152-9
Dipstick lateral flow assay for serum or CSF: $2/test and takes 10 min with sensitivity ~99%