
Opioid Therapy for Cancer-Related Pain - Donau-Universit¤t Krems
139
Opioid Therapy for Cancer-Related Pain A Systematic Review of the Comparative Efficacy, Effectiveness and Risk of Harms of Extended-Release Opioids October 2012 Department for Evidence-based Medicine and Clinical Epidemiology
Transcript of Opioid Therapy for Cancer-Related Pain - Donau-Universit¤t Krems

Opioid Therapy for Cancer-Related Pain A Systematic Review of the Comparative Efficacy, Effectiveness and
Risk of Harms of Extended-Release Opioids
October 2012
Department for Evidence-based Medicine and Clinical Epidemiology

Authors
Ursula Griebler, PhD, MPH
Anna Glechner, MD
Christina Kien, MSc
Michaela Strobelberger, MA
Bita Mesgarpour PharmD, MPH
Megan G. Van Noord, MSIS
Andrea Michalek-Sauberer, MD
External Reviewers
Engelbert Deusch, MD
Gerald Gartlehner, MD, MPH
Kylie Thaler, MD, MPH
Ekkehard Schweitzer,MD, DEAA
Funding Source
This review was funded by Grünenthal GmBH
Imprint
Danube University Krems
Department for Evidence-based Medicine and Clinical Epidemiology
Dr.-Karl-Dorrek-Straße 30
3500 Krems an der Donau, Austria
Table of Contents 1 Executive Summary ........................................................................................................................................ 1
1.1 Background ............................................................................................................................................ 1
1.2 Methods ................................................................................................................................................ 2
1.3 Results ................................................................................................................................................... 4
1.4 Discussion .............................................................................................................................................. 5
2 Introduction.................................................................................................................................................... 6
2.1 Background ............................................................................................................................................ 6
2.1.1 Cancer Pain ........................................................................................................................................ 6
2.1.2 Treatment Strategies (Opioids) ......................................................................................................... 8
2.1.3 Pharmacology of Analgesic Opioids ................................................................................................ 10
2.2 Scope and Key Questions .................................................................................................................... 17
3 Methods ....................................................................................................................................................... 19
3.1 Topic Refinement and Review Protocol .............................................................................................. 19
3.2 Search Strategy .................................................................................................................................... 19
3.3 Eligibility Criteria .................................................................................................................................. 20
3.3.1 Population ....................................................................................................................................... 20
3.3.2 Intervention..................................................................................................................................... 20
3.3.3 Control ............................................................................................................................................. 21
3.3.4 Outcomes ........................................................................................................................................ 21
3.3.5 Timing .............................................................................................................................................. 22
3.3.6 Setting ............................................................................................................................................. 22
3.4 Study Selection .................................................................................................................................... 22
3.5 Data Extraction .................................................................................................................................... 23
3.6 Risk of Bias Assessment of Individual Studies ..................................................................................... 23
3.7 Data Synthesis ..................................................................................................................................... 24
3.8 Strength of Body of Evidence .............................................................................................................. 24
4 Results .......................................................................................................................................................... 26
4.1 Introduction ......................................................................................................................................... 26
4.2 Results of Literature Searches ............................................................................................................. 26
4.3 Description of Included Studies ........................................................................................................... 27
4.4 Key Question 1: Comparative Efficacy and Effectiveness of Extended-Release Opioids ..................... 28
4.4.1 Description of Included Studies ...................................................................................................... 28
4.4.2 Key Points ........................................................................................................................................ 30
4.4.3 Detailed Synthesis ........................................................................................................................... 30
4.5 Key Question 2: Comparative Risk of Harms of Extended-Release Opioids ........................................ 42
4.5.1 Description of Included Studies ...................................................................................................... 42
4.5.2 Key Points ........................................................................................................................................ 45
4.5.3 Detailed Synthesis ........................................................................................................................... 46
4.5.3.1.2 Comparative Risk of Serious Adverse Events .......................................................................... 50

4.6 Key Question 3: Efficacy, Effectiveness, or Risk for Harms in Subpopulations .................................... 83
5 Discussion ..................................................................................................................................................... 84
5.1 Key Findings and Strength of Evidence ................................................................................................ 84
5.2 Gaps in the Evidence ........................................................................................................................... 85
6 Conclusions................................................................................................................................................... 86
7 References .................................................................................................................................................... 87
8 Appendices ................................................................................................................................................... 90
List of Tables Table 1: Extended-Release Opioid Analgesic Products. ........................................................................................ 11 Table 2: Extended-Release Opioids Approved for Treatment of Moderate to Severe Pain in Austria
1,
Switzerland2, Germany
3, UK
4, and US
5. ................................................................................................................. 12
Table 3: Included Drugs and Combination of Drugs.............................................................................................. 21 Table 4: Outcomes and Eligibility Criteria. ............................................................................................................ 22 Table 5: Definitions of the Grades of the Overall Quality of Evidence. ................................................................ 25 Table 6: Outcomes Viewed as Critical or Important for Decision-Making. ........................................................... 25 Table 7: Characteristics of the Available Evidence for KQ1. ................................................................................. 29 Table 8: Risk of Bias Summary for RCTs Included for KQ1. ................................................................................... 29 Table 9: Study Characteristics for all Studies Included for KQ1, the Investigated Outcomes and Risk of Bias Ratings. .................................................................................................................................................................. 31 Table 10: Study Characteristics and Summary of Findings on Pain Intensity. ...................................................... 35 Table 11: Study Characteristics and Summary of Findings on Quality Of Life. ..................................................... 38 Table 12: Study Characteristics and Summary of Findings on Functional Capacity. ............................................. 39 Table 13: Study Characteristics and Summary of Findings on Patient Perceived Effectiveness. .......................... 40 Table 14: Study Characteristics and Summary of Findings on Cognitive Performance......................................... 41 Table 15: Rates of Discontinuation Due to Lack of Efficacy by Study Drug. .......................................................... 41 Table 16: Characteristics of the Available Evidence for KQ2. ............................................................................... 43 Table 17: Risk of Bias Summaries for RCTs Included for KQ2................................................................................ 44 Table 18: Risk of Bias Summary for Observational Studies Included for KQ2. ...................................................... 44 Table 19: Study Characteristics for all Studies Included for KQ2, the Investigated Outcomes and Risk of Bias Ratings. .................................................................................................................................................................. 47 Table 20: Reported Frequencies of Serious Adverse Events by Drug. .................................................................. 50 Table 21: Study Characteristics and Summary of Findings on Serious Adverse Events. ....................................... 54 Table 22: Drop-Out Rates and Risk for Specific Adverse Events During the Stable Phase of Treatment.............. 57 Table 23: Study Characteristics and Summary of Findings of Constipation. ......................................................... 62 Table 24: Study Characteristics and Summary of Findings o Nausea and Vomiting. ............................................ 72 Table 25: Studies Assessing Dizziness. .................................................................................................................. 78 Table 26: Studies Assessing Drowsiness, Somnolence, Fatigue, or Sedation. ...................................................... 81 Table 27: Studies Assessing Diarrhea. ................................................................................................................... 83
List of Figures Figure 1: WHO-Pain Ladder.(16) ............................................................................................................................. 9 Figure 2: Analytical Framework of the Comparative Efficacy, Effectiveness, and Risk for Harms of Extended-Release Opioids in Patients with Cancer-Related Pain. ........................................................................................ 18 Figure 3: PRISMA Flow Diagram of the Study Selection Process. ......................................................................... 27
List of Appendix-Tables Appendix-Table 1: Pharmaceutical Companies that were Contacted. ............................................................... 101 Appendix-Table 2: High Risk of Bias Studies and Reasons for the Poor Quality Rating. ..................................... 106 Appendix-Table 3: KQ1: GRADE Ratings for the Comparison Oral Morphine ER vs. Oral Hydromorphone ER, sorted by Outcomes for KQ1. .............................................................................................................................. 107 Appendix-Table 4: KQ1: GRADE Ratings for the Comparison Oral Hydromorphone ER vs. Oral Oxycodone ER, sorted by Outcomes for KQ1. .............................................................................................................................. 108

Appendix-Table 5: KQ1: GRADE Ratings for the Comparison Oral Oxycodone ER vs. Oxycodone plus Naloxone ER, sorted by Outcomes for KQ1. ........................................................................................................................ 109 Appendix-Table 6: KQ2: GRADE Ratings for the Comparison Oral Morphine ER vs. Oral Hydromorphone ER, sorted by Outcomes for KQ2. .............................................................................................................................. 110 Appendix-Table 7: KQ2: GRADE Ratings for the Comparison Oral Morphine ER vs. Oral Oxycodone ER, sorted by Outcomes for KQ2. .............................................................................................................................................. 111 Appendix-Table 8: KQ2: GRADE Ratings for the Comparison Oral Morphine ER vs. Transdermal Fentanyl ER, sorted by Outcomes For KQ2. ............................................................................................................................. 112 Appendix-Table 9: KQ2: GRADE Ratings for the Comparison Oral Hydromorphone ER vs. Oral Oxycodone ER sorted by Outcomes for KQ2. .............................................................................................................................. 113 Appendix-Table 10: KQ2: GRADE Ratings for the Comparison Oral Hydromorphone ER vs. Transdermal Fentanyl ER, sorted by Outcomes for KQ2. ........................................................................................................................ 114 Appendix-Table 11: KQ2: GRADE Ratings for the Comparison Oral Hydromorphone ER vs. Transdermal Buprenorphine ER, sorted by Outcomes for KQ2. .............................................................................................. 115 Appendix-Table 12: KQ2: GRADE Ratings for the Comparison Oral Oxycodone ER vs. Oral Oxycodone ER + Naloxone, sorted by Outcomes for KQ2. ............................................................................................................ 116 Appendix-Table 13: KQ2: GRADE Ratings for the Comparison Oral Oxycodone ER vs. Transdermal Fentanyl ER, sorted by Outcomes for KQ2. .............................................................................................................................. 117 Appendix-Table 14: KQ2: GRADE Ratings for the Comparison Transdermal Fentanyl ER vs. Transdermal Buprenorphine ER, sorted by Outcomes For KQ2. .............................................................................................. 118 Appendix-Table 15: Commonly Used Outcome Measures and Instruments. ..................................................... 119

Opioid Therapy for Cancer-Related Pain
1
1 Executive Summary
The PROSPERO (International Prospective Register of Systematic Reviews:
http://www.crd.york.ac.uk/prospero) registration number of this review is:
CRD42012002153
1.1 Background
Pain is one of the consequences cancer patients fear the most about their disease. Experts
estimate that up to 50% of patients afflicted with malignant tumors will experience pain
during the course of their disease. A recent pan-European survey of cancer-related pain
found that 56% of patients suffered moderate-to-severe pain at least monthly. Pain can
negatively affect a patient’s social life and functional psychology (cognitive, affective, and
behavioral). Inadequate pain control can not only affect a patient’s mood but can also trigger
feelings of anxiety and fear which can then lead to depression and a sense of hopelessness.
Whereas inadequate pain control can have a profound negative impact on quality of life,
some studies suggest that adequate pain control can result in improved survival rates.
Treatment of cancer-related pain is multidisciplinary and includes pharmacological therapy,
anti-tumor treatment (e.g., radiation, surgery and chemotherapy), supportive, non-
pharmacological techniques (including psychological support or behavioral therapy), and
invasive procedures (e.g., nerve blockades, neurolytic procedures, intra-thecal drug
therapy).
Recent guidelines for the pharmacological treatment of cancer pain still refer to the WHO’s
(World Health Organization’s) pain ladder, first published in 1986. The European Medicines
Agency (EMA) and U.S. Food and Drug Administration (FDA) have approved a wide variety of
opioids for relieving acute and chronic pain. In addition, several analgesic options are
available as long-acting medications which offer the promise of prolonged analgesia. Long-
acting opioids, also called sustained-release (SR), controlled-release (CR), modified-release
(MR) or extended-release (ER, XR or XL), are available in both oral and transdermal

Opioid Therapy for Cancer-Related Pain
2
formulations. They are administered at regularly scheduled times, for example every 12
hours.
The objective of this review was to compare the benefits and harms of oral or transdermal
extended-release opioids used for treatment of adults with moderate to severe cancer-
related pain. Specifically, we addressed the following research questions (KQs):
Key Question 1: How do extended-release opioids compare in their analgesic efficacy and
effectiveness in treating adult patients with cancer-related pain?
Key Question 2: How do extended-release opioids compare in their risk for harms in treating
adult patients with cancer-related pain?
Key Question 3: How do efficacy, effectiveness, or risk for harms of treatment with
extended-release opioids for cancer-related pain differ for the following subpopulations:
Patients with moderate vs. severe cancer pain?
Patients with breakthrough pain?
Patients with a neuropathic cancer pain component?
Different sex, or different age, ethnic or socioeconomic groups?
Patients taking other commonly prescribed co-analgesics (e.g., non-steroidal
anti-inflammatory drugs, antiepileptic drugs, antidepressants)?
1.2 Methods
During the course of topic development and refinement, we worked with the commissioner
of the report to develop a draft and final protocol for the systematic review process. We
generated an analytic framework, preliminary KQs, and preliminary inclusion/exclusion
criteria in the form of PICOTS (patient populations, interventions, comparators, outcomes,
timing, settings).
To identify articles relevant to each KQ, we searched PubMed, the Cochrane Library,
EMBASE, International Pharmaceutical Abstracts, CINAHL, BIOSIS, and Web of Science. We
Opioid Therapy for Cancer-Related Pain
3
used either Medical Subject Headings (MeSH) or major headings as search terms when
available and key words when appropriate. We limited the electronic searches to human and
adult populations. Sources were searched from 1980 to July 2012. We manually searched
reference lists of pertinent reviews, included trials, and background articles on this topic to
look for any relevant citations that our searches might have missed. We also explored
various sources for unpublished studies and contacted pharmaceutical companies
requesting any unpublished studies or data relevant for this review.
We developed eligibility (inclusion and exclusion) criteria with respect to patient
populations, interventions, comparators, outcomes, timing, settings, study designs, and
durations for each KQ. We included only studies that were published in English or German
language. For cross-over randomized-controlled studies (RCTs), we used data of the first
study period before the cross-over.
Two trained members of the research team independently reviewed all titles, abstracts, and
full-text articles for eligibility against our inclusion/exclusion criteria. If the reviewers
disagreed, they resolved conflicts by discussion and consensus or by consulting a third
member of the review team. To assess the risk of bias of RCTs for major outcomes of
interest, we used the Cochrane risk of bias tool. For observational studies we employed
predefined criteria based on established guidance.
For studies that met our inclusion criteria and were of low or unclear risk of bias, we
extracted important information into a structured data abstraction form. All data
abstractions were reviewed for completeness and accuracy by a second member of the
team. We recorded intention-to-treat (ITT) results if available.
Because quantitative synthesis was not appropriate (e.g., because of clinical heterogeneity,
insufficient number of similar studies, or variation in reported outcomes), we synthesized
the results qualitatively.
We graded the strength of the available evidence in a four-part hierarchy based on an
approach devised by the GRADE (Grading of Recommendations Assessment, Development
and Evaluation) working group. We used four grades: high, moderate, low, and very low.
Opioid Therapy for Cancer-Related Pain
4
Gradings reflect the strength of the body of evidence to answer KQs with respect to the
comparative efficacy, effectiveness, and risk of harms of extended-release opioids.
1.3 Results
We identified 5,135 citations from searches and reviews of reference lists and screened
3,390 records, after removal of duplicates. Out of those, we retrieved 211 articles for full-
text review for this report. Overall, nine studies met eligibility criteria for this systematic
review. Of the included studies, three were double-blind RCTs, two were non-blinded RCTs,
two were prospective cohort studies, and two were retrospective cohort studies.
Six out of the nine included studies that met eligibility criteria were rated as high risk of bias.
The main reasons for rating RCTs as high risk of bias were high attrition and lack of blinding.
We briefly discuss high risk of bias studies in the report because for many comparisons or
outcomes of interest no studies of better methodological quality were available.
The 12 included long-acting opioids allow for 66 possible drug-to-drug comparisons within
this drug class. For comparative efficacy, however, we found evidence on only three
comparisons; for comparative risk of harm on only nine comparisons. Consequently, we can
neither confirm nor rule out differences in the comparative efficacy and risk of harms for the
majority of comparisons. The available evidence often had serious methodological
shortcomings. Consequently, most of our conclusions have a very high degree of
uncertainty:
The comparative efficacy for improvement of pain intensity, quality of life, functional
capacity, and cognitive functioning was similar among compared drugs.
Discontinuation rates because of lack of evidence were also similar. The strength of
evidence supporting similar efficacy among compared drugs is very low.
We could not find eligible evidence on the comparative efficacy of transdermal
buprenorphine ER, oral dihydrocodeine ER, transdermal fentanyl ER, oral morphine
plus naltrexone ER, oral nalbuphine ER, oxymorphone ER, oral tapentadol
hydrochloride ER, and oral tramadol ER.
Opioid Therapy for Cancer-Related Pain
5
With few exceptions, the comparative risk of harms was also similar among reviewed
drugs. Discontinuation rates because of adverse events were similar. The strength of
evidence supporting a similar risk of harms with respect to serious adverse events,
constipation, nausea and vomiting, dizziness, and somnolence among compared
drugs is low or very low.
Oral oxycodone ER had higher risks of some adverse events than comparator drugs,
the strength of evidence, however, is low or very low:
o a higher risk of drowsiness than oral hydromorphone ER;
o a higher risk of constipation than oral oxycodone plus naloxone ER;
o a higher risk of nausea than oral morphine ER and transdermal fentanyl ER;
o and a higher risk of somnolence than transdermal fentanyl ER.
We did not find any studies that addressed the comparative efficacy and risk of harms of
extended-release opioids in subgroups with respect to sex, ethnicity, age, patients with
moderate vs. severe cancer pain, breakthrough pain, or pain with a neuropathic component.
Furthermore, no evidence on patients taking other commonly prescribed co-analgesics (e.g.,
non-steroidal anti-inflammatory drugs, antiepileptic drugs, antidepressants) was available.
1.4 Discussion
This systematic review assesses the comparative efficacy and risk of harms of extended-
release opioids for the treatment of moderate to severe cancer-related pain. Overall, for
most interventions and outcomes of interest, evidence was either lacking or insufficient to
draw conclusions. Furthermore, in the evidence available, the eligible studies often had
serious serious methodological shortcomings. Consequently, most of the conclusions have a
very high degree of uncertainty.
The available evidence indicates no substantial differences in efficacy and risk of harms
amongst extended-release opioids. Our confidence in these estimates, however, is very low.
We anticipate that future studies will change these estimates. Given the lack of reliable
evidence regarding the comparative benefits and harms of extended-release opioids,
clinicians should weigh clinical experience, patient preferences, and treatment costs when
choosing the optimal treatment for an individual cancer patient.

Opioid Therapy for Cancer-Related Pain
6
2 Introduction
2.1 Background
2.1.1 Cancer Pain
Pain is one of the consequences cancer patients fear the most about their disease. Experts
estimate that up to 50% of patients afflicted with malignant tumors will experience pain
during the course of their disease(1), although reported prevalence data set the range more
widely at 14 to 100%(2). In a quarter of all cancer patients, pain is the presenting symptom
at the time a tumor is diagnosed.(3) The incidence of pain, however, increases with the
progression of the underlying disease. Eventually two-thirds of patients with advanced,
metastatic cancer will suffer pain. In some types of cancer such as pancreatic cancer and
cancer of the head or neck, pain is especially prevalent.(4) Bone metastases (e.g., in lung,
prostatic or breast cancer) are usually also associated with intense pain conditions. A recent
pan-European survey of cancer-related pain found that 56% of patients suffered moderate-
to-severe pain at least monthly.(1) The International Association for the Study of Pain
defines pain as “an unpleasant sensory and emotional experience associated with actual or
potential tissue damage, or described in terms of such damage”.(5)
Pain can negatively affect a patient’s social life and functional psychology (cognitive,
affective and behavioral). When movement provokes pain, a patient’s daily activities and
mobility will be restricted. Inadequate pain control can not only affect a patient’s moods but
can also trigger feelings of anxiety and fear which can then lead to depression and a sense of
hopelessness.(6) Whereas inadequate pain control can have a profound negative impact on
quality of life, some studies suggest that adequate pain control can result in improved
survival rates.(1, 7)
Multiple causes exist for cancer-related pain. These can be roughly grouped into three
categories. First, the tumor or its metastases may directly cause pain. Second, in about 20%
of patients, cancer treatment results in painful sequelae such as painful peripheral
neuropathy after chemotherapy, persisting pelvic pain after radiation therapy or post-

Opioid Therapy for Cancer-Related Pain
7
thoracotomy pain after surgery.(8) Third, older patients in particular may suffer from pain
unrelated to the tumor that stems from preexisting chronic pain (e.g., chronic back pain
osteoarthritis or painful diabetic peripheral neuropathy). Sometimes patients report pain of
a fourth category - pain related to cancer such as muscle spasms, constipation, or
bedsores.(9)
Pain can be classified according to the underlying pathophysiology in nociceptive or
neuropathic pain. Direct tissue injury resulting in activation of nociceptors causes
nociceptive pain. Nociceptive pain can be further classified as either somatic or visceral.
Examples of conditions that cause nociceptive pain in cancer patients are bone metastases,
tissue inflammation and edema for somatic pain, or tumor invasion and distension of
internal organs as in peritoneal carcinosis or hepatic metastases for visceral pain.
Neuropathic pain on the other hand, is caused by infiltration or compression of peripheral or
central (e.g., spinal cord metastases) neuronal structures. While the distinction between
somatic and neuropathic pain has therapeutic implications – neuropathic pain usually does
not respond well to classical analgesics – the specification is also somewhat theoretical,
since patients suffering from cancer pain typically suffer from mixed types of pain in multiple
locations.(10) Assessment of pain quality can provide some clues as to the type of pain.
Somatic pain is usually localized and described as aching or throbbing, visceral pain is rather
diffuse, also described as cramping, whereas descriptions for neuropathic pain might include
shooting, burning or electrical sensations.
Caregivers and patients can also categorize pain according to its severity. Assessment of pain
intensity is usually based on self-reporting tools, using visual analogue scales (VAS) or
numerical rating scales (NRS), which are considered equally efficient.(11) On numerical
scales, scores from 0-4 generally indicate mild, 5-6 moderate, and 7-10 severe pain(12),
although some authors see the boundary between moderate and severe pain at >7.(13)
Verbal rating scales with four to seven adjectives describing pain intensity are used as well.
When assessments of pain focus solely on intensity, other dimensions of pain, particularly
pain induced impairment, are left unaccounted for. Multidimensional questionnaires are
more appropriate for assessing pain induced impairments.(14, 15)
Opioid Therapy for Cancer-Related Pain
8
Finally, pain assessments need to consider the time course of pain, especially if the pain is
stable or intermittent.
2.1.2 Treatment Strategies (Opioids)
Treatment of cancer-related pain is multidisciplinary and includes pharmacological therapy,
anti-tumor treatment (e.g., radiation, surgery and chemotherapy), supportive, non-
pharmacological techniques (including psychological support or behavioral therapy) and
invasive procedures (e.g., nerve blockades, neurolytic procedures, intra-thecal drug
therapy).
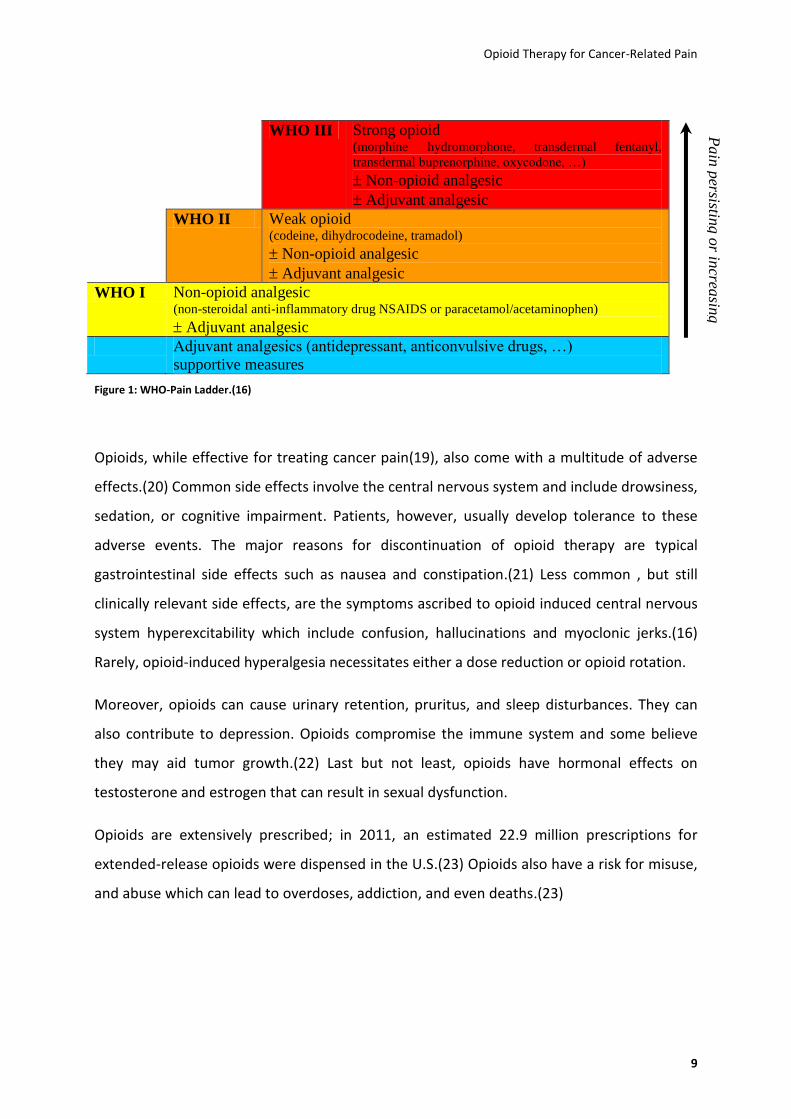
Recent guidelines for the pharmacological treatment of cancer pain(16) still refer to the
WHO’s (World Health Organization’s) pain ladder, first published in 1986 (see Figure 1).(17)
The WHO-ladder recommends a graded approach based on pain severity. For mild pain (NRS
1-4) non-opioid analgesics (non-steroidal anti-inflammatory drugs [NSAIDS] or
paracetamol/acetaminophen) might be sufficient in WHO-step I. When the pain is moderate
(up to NRS 5-7) WHO-step II suggests the addition of weak opioids (codeine, dihydrocodeine
or tramadol). Although not included in the original WHO pain ladder, some authors also
include strong opioids in low doses for WHO-step II.(16) For severe pain (NRS 8-10) strong
opioids replace codeine or tramadol (Figure 1). The ladder lists morphine as a “standard”
strong opioid although other drugs such as hydromorphone, transdermal fentanyl,
transdermal buprenorphine, or oxycodone are mentioned as well. The combination of
opioids with non-opioid analgesics is intended to reduce the side effects of opioids.(18)
Clinicians usually prefer the oral administration of pharmacological treatments.(17)
Transdermal opioid delivery systems (e.g., transdermal fentanyl or transdermal
buprenorphine), which take longer to reach a steady-state, may be more appropriate in
certain patients like those who have difficulty swallowing or adhering to treatment
regimens.(16) Clinicians reserve more invasive routes of opioid administration (e.g.,
subcutaneous, intravenous, or the spinal route) for patients in whom adequate analgesia
cannot be otherwise achieved. Drugs should be administered at fixed time intervals – “by
the clock”, using “rescue-medication” i.e., immediate-release preparations for breakthrough
pain. Adjuvants and co-analgesics (e.g., antidepressants or anti-convulsive drugs) might be
used at every step of the WHO ladder as clinically appropriate.(17)
Opioid Therapy for Cancer-Related Pain
9
WHO III Strong opioid (morphine hydromorphone, transdermal fentanyl,
transdermal buprenorphine, oxycodone, …)
Non-opioid analgesic
Adjuvant analgesic
WHO II Weak opioid (codeine, dihydrocodeine, tramadol)
Non-opioid analgesic
Adjuvant analgesic
WHO I Non-opioid analgesic (non-steroidal anti-inflammatory drug NSAIDS or paracetamol/acetaminophen)
Adjuvant analgesic
Adjuvant analgesics (antidepressant, anticonvulsive drugs, …)
supportive measures
Figure 1: WHO-Pain Ladder.(16)
Opioids, while effective for treating cancer pain(19), also come with a multitude of adverse
effects.(20) Common side effects involve the central nervous system and include drowsiness,
sedation, or cognitive impairment. Patients, however, usually develop tolerance to these
adverse events. The major reasons for discontinuation of opioid therapy are typical
gastrointestinal side effects such as nausea and constipation.(21) Less common , but still
clinically relevant side effects, are the symptoms ascribed to opioid induced central nervous
system hyperexcitability which include confusion, hallucinations and myoclonic jerks.(16)
Rarely, opioid-induced hyperalgesia necessitates either a dose reduction or opioid rotation.
Moreover, opioids can cause urinary retention, pruritus, and sleep disturbances. They can
also contribute to depression. Opioids compromise the immune system and some believe
they may aid tumor growth.(22) Last but not least, opioids have hormonal effects on
testosterone and estrogen that can result in sexual dysfunction.
Opioids are extensively prescribed; in 2011, an estimated 22.9 million prescriptions for
extended-release opioids were dispensed in the U.S.(23) Opioids also have a risk for misuse,
and abuse which can lead to overdoses, addiction, and even deaths.(23)
Pain
persistin
g o
r increa
sing
Opioid Therapy for Cancer-Related Pain
10
2.1.3 Pharmacology of Analgesic Opioids
Opioids produce their analgesic effects by binding to three major receptor families which are
called µ (mu), (kappa), and (delta) receptors. Although these receptors exist throughout
the body’s tissues, they are mainly located in the central nervous system.(24)
Classification of opioid analgesics as either pure agonists or agonist-antagonists is based on
their interaction with opioid receptors. The agonist-antagonists are divided into two
subtypes: partial agonists and mixed agonist-antagonists. Pure opioid agonists (morphine,
codeine, oxycodone, hydromorphone, fentanyl) bind to opioid receptors avidly and have no
ceiling in their analgesic effects. Opioids in the mixed agonist-antagonist subclass
(nalorphine, pentazocine) generally are not used for chronic pain because they have a ceiling
effect for antinociception and usage may result in the development of withdrawal
symptoms. Partial opioid agonists like buprenorphine have high affinity binding to opioid
receptors but low efficacy and produce a sub-maximal effect compared to pure agonists.(25-
27)
Tramadol can be considered an atypical opioid analgesic that acts through both an opioid
(mu agonist) and a nonopioid (serotonergic and noradrenergic) mechanism.(25-27)
Tapentadol is another narcotic pain reliever that has been marketed since 2008. It is a
centrally acting oral analgesic with two mechanisms of action within the same molecule: an
agonist activity at the mu-opioid receptor and a noradrenaline reuptake inhibition. The latter
characteristic makes it potentially more effective in treating neuropathic pain.(28)
Patient responses to opioid therapy vary remarkably, inter-individually from opioid to opioid
and also at different stages of treatment. Inadequate pain relief or intolerable side effects
are the main reasons for changes in treatment. Clinicians might recommend administration
of the same opioid through an alternative route or change to another agent.(29, 30)
The EMA and the FDA have approved a wide variety of opioids for relieving acute and
chronic pain. In addition, several analgesic options are available as long-acting medications
which offer the promise of prolonged analgesia. Long-acting opioids, also called sustained-
release (SR), controlled-release (CR), modified-release (MR), or extended-release (ER, XR, or
Opioid Therapy for Cancer-Related Pain
11
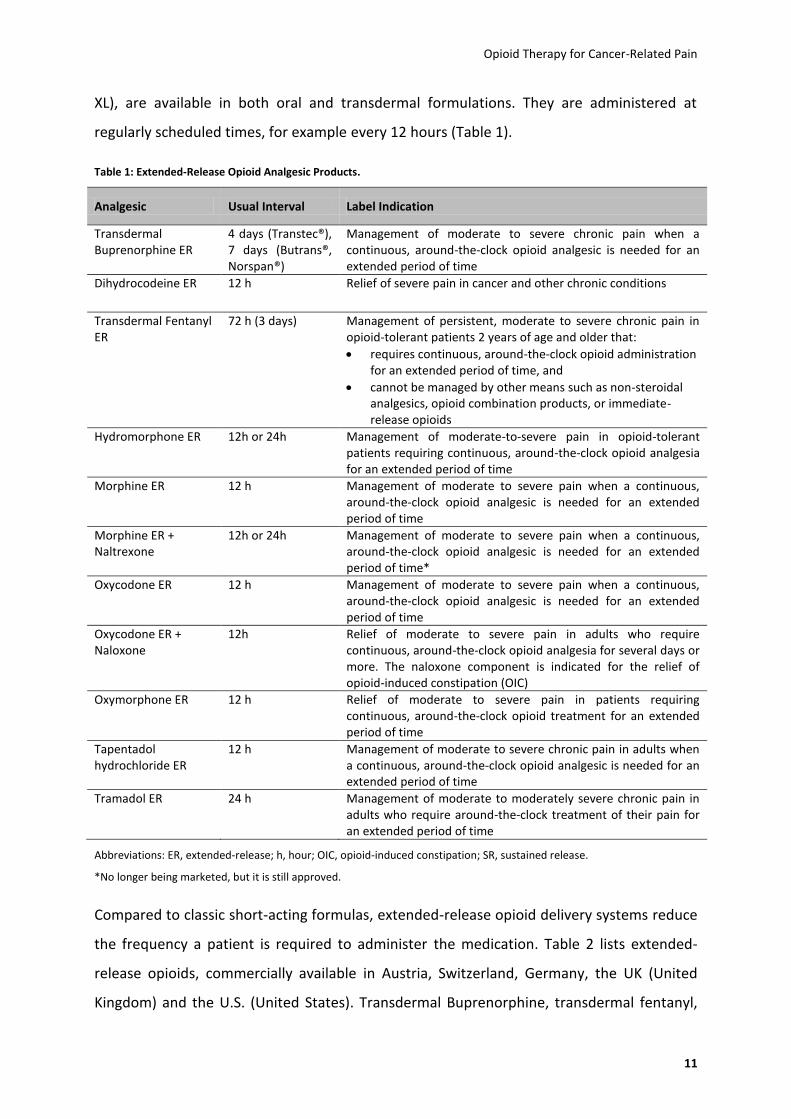
XL), are available in both oral and transdermal formulations. They are administered at
regularly scheduled times, for example every 12 hours (Table 1).
Table 1: Extended-Release Opioid Analgesic Products.
Analgesic Usual Interval Label Indication
Transdermal Buprenorphine ER
4 days (Transtec®), 7 days (Butrans®, Norspan®)
Management of moderate to severe chronic pain when a continuous, around-the-clock opioid analgesic is needed for an extended period of time
Dihydrocodeine ER 12 h Relief of severe pain in cancer and other chronic conditions
Transdermal Fentanyl ER
72 h (3 days) Management of persistent, moderate to severe chronic pain in opioid-tolerant patients 2 years of age and older that:
requires continuous, around-the-clock opioid administration for an extended period of time, and
cannot be managed by other means such as non-steroidal analgesics, opioid combination products, or immediate-release opioids
Hydromorphone ER 12h or 24h Management of moderate-to-severe pain in opioid-tolerant patients requiring continuous, around-the-clock opioid analgesia for an extended period of time
Morphine ER 12 h Management of moderate to severe pain when a continuous, around-the-clock opioid analgesic is needed for an extended period of time
Morphine ER + Naltrexone
12h or 24h Management of moderate to severe pain when a continuous, around-the-clock opioid analgesic is needed for an extended period of time*
Oxycodone ER 12 h Management of moderate to severe pain when a continuous, around-the-clock opioid analgesic is needed for an extended period of time
Oxycodone ER + Naloxone
12h Relief of moderate to severe pain in adults who require continuous, around-the-clock opioid analgesia for several days or more. The naloxone component is indicated for the relief of opioid-induced constipation (OIC)
Oxymorphone ER 12 h Relief of moderate to severe pain in patients requiring continuous, around-the-clock opioid treatment for an extended period of time
Tapentadol hydrochloride ER
12 h Management of moderate to severe chronic pain in adults when a continuous, around-the-clock opioid analgesic is needed for an extended period of time
Tramadol ER 24 h Management of moderate to moderately severe chronic pain in adults who require around-the-clock treatment of their pain for an extended period of time
Abbreviations: ER, extended-release; h, hour; OIC, opioid-induced constipation; SR, sustained release.
*No longer being marketed, but it is still approved.
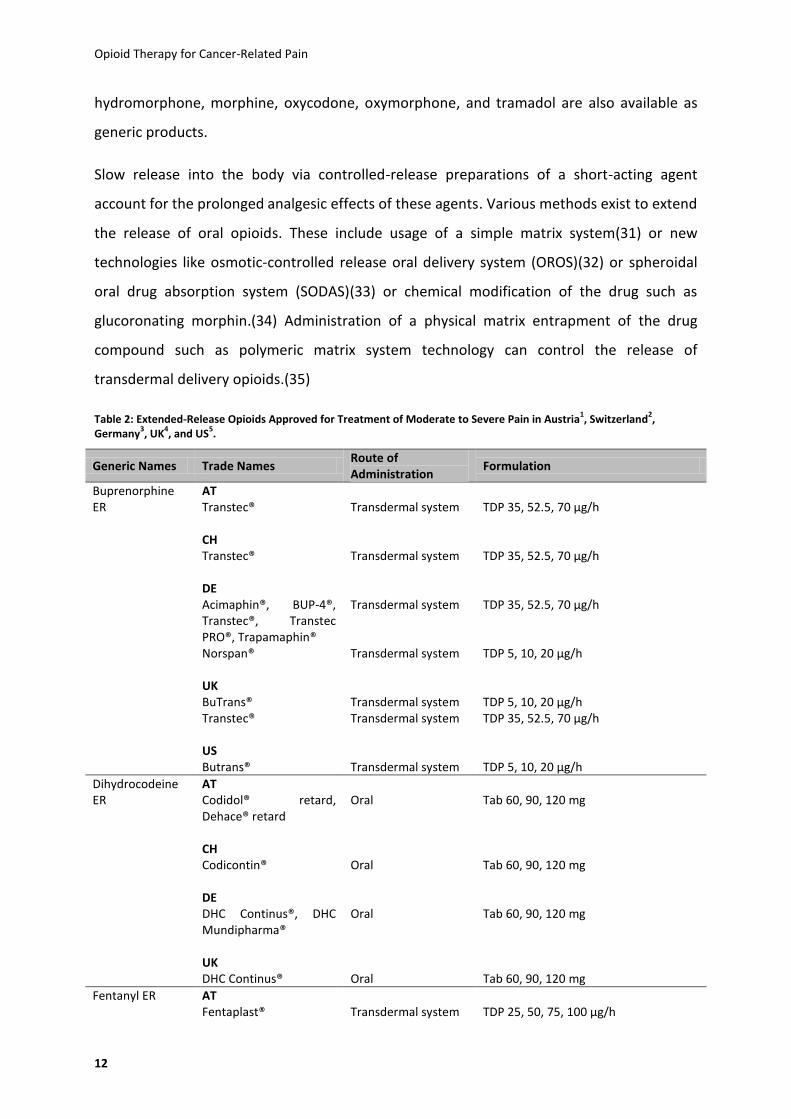
Compared to classic short-acting formulas, extended-release opioid delivery systems reduce
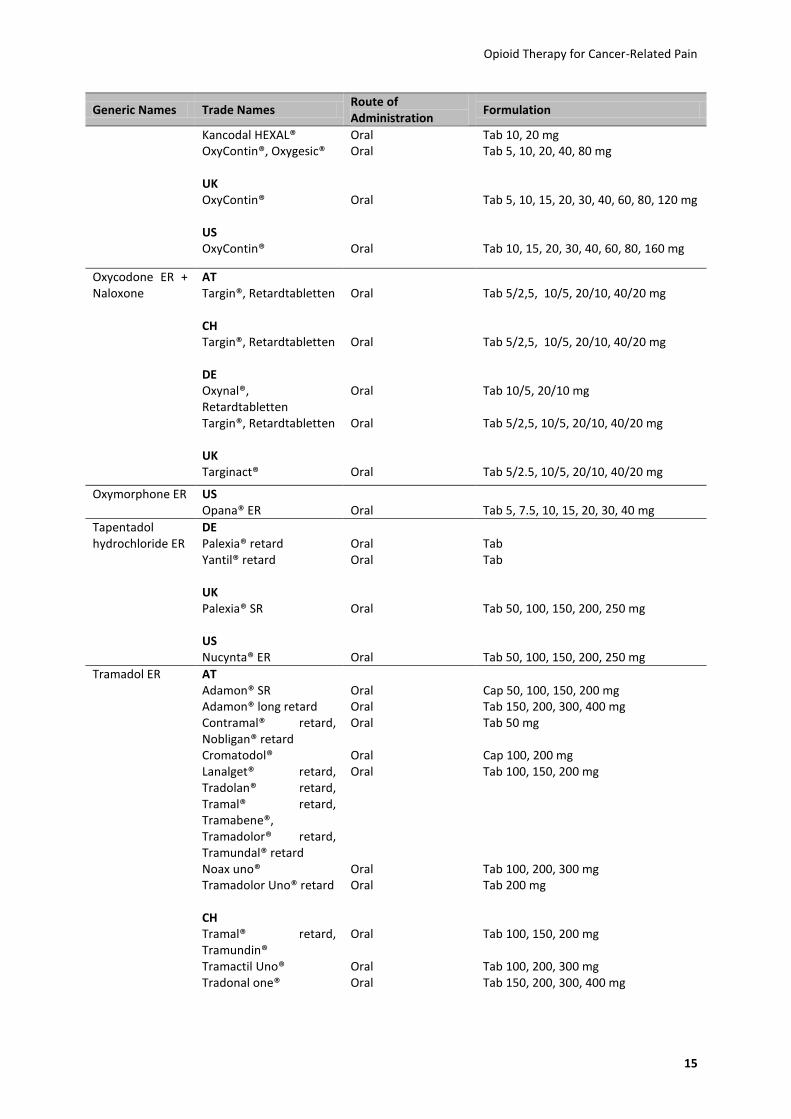
the frequency a patient is required to administer the medication. Table 2 lists extended-
release opioids, commercially available in Austria, Switzerland, Germany, the UK (United
Kingdom) and the U.S. (United States). Transdermal Buprenorphine, transdermal fentanyl,
Opioid Therapy for Cancer-Related Pain
12
hydromorphone, morphine, oxycodone, oxymorphone, and tramadol are also available as
generic products.
Slow release into the body via controlled-release preparations of a short-acting agent
account for the prolonged analgesic effects of these agents. Various methods exist to extend
the release of oral opioids. These include usage of a simple matrix system(31) or new
technologies like osmotic-controlled release oral delivery system (OROS)(32) or spheroidal
oral drug absorption system (SODAS)(33) or chemical modification of the drug such as
glucoronating morphin.(34) Administration of a physical matrix entrapment of the drug
compound such as polymeric matrix system technology can control the release of
transdermal delivery opioids.(35)
Table 2: Extended-Release Opioids Approved for Treatment of Moderate to Severe Pain in Austria1, Switzerland
2,
Germany3, UK
4, and US
5.
Generic Names Trade Names Route of Administration
Formulation
Buprenorphine ER
AT Transtec®
Transdermal system
TDP 35, 52.5, 70 μg/h
CH
Transtec®
Transdermal system
TDP 35, 52.5, 70 μg/h
DE
Acimaphin®, BUP-4®, Transtec®, Transtec PRO®, Trapamaphin®
Transdermal system
TDP 35, 52.5, 70 μg/h
Norspan® Transdermal system TDP 5, 10, 20 μg/h
UK
BuTrans®
Transdermal system
TDP 5, 10, 20 μg/h
Transtec® Transdermal system TDP 35, 52.5, 70 μg/h
US
Butrans®
Transdermal system
TDP 5, 10, 20 μg/h
Dihydrocodeine ER
AT Codidol® retard, Dehace® retard
Oral
Tab 60, 90, 120 mg
CH Codicontin®
Oral
Tab 60, 90, 120 mg
DE DHC Continus®, DHC Mundipharma®
Oral
Tab 60, 90, 120 mg
UK DHC Continus®
Oral
Tab 60, 90, 120 mg
Fentanyl ER AT Fentaplast®
Transdermal system
TDP 25, 50, 75, 100 μg/h

Opioid Therapy for Cancer-Related Pain
13
Generic Names Trade Names Route of Administration
Formulation
Fentarichtex® Transdermal system TDP 25, 37.5, 50, 75, 100 μg/h Durogesic®, Lafene®,
Fentoron®, Matrifen® Transdermal system TDP 12, 25, 50, 75, 100 μg/h
CH Durogesic Matrix®, Matrifen®
Transdermal system
TDP 12, 25, 50, 75, 100 μg/h
DE Fentavera®, Fentalupo Matrix®, Durogesic SMAT®, Fentaderm®, Fentadolon®, Fenylat®, Fentaquick Matrix®, Fentareu Matrix®, Matrifen®
Transdermal system
TDP 12, 25, 50, 75, 100 μg/h
FentaMat Sandoz® Transdermal system TDP 12, 25, 37.5, 50, 75, 100 μg/h Fenta Regiomedica
Matrix®, Durogesic®, Fentil®, Fentrix®, Lavifent Fentapatch Matrix®, Fentatrans®
Transdermal system TDP 25, 50, 75, 100 μg/h
UK Fencino®, Durogesic Dtrans®, Matrifen®, Mezolar Matrix®, Tilofyl®, Osmanil®
Transdermal system
TDP 12, 25, 50, 75, 100 μg/h
Victanyl® Transdermal system TDP 25, 50, 75, 100 μg/h
US Duragesic®
Transdermal system
TDP 12, 25, 50, 75, 100 μg/h
Hydromorphone ER
AT Jurnista®
Oral
Tab 4, 8, 16, 32, 64 mg
Hydal retard® Oral Cap 2, 4, 8, 16, 24 mg Mydrophostad® Oral Tab 4, 8, 16, 24 mg
CH Jurnista®
Oral
Tab 4, 8, 16, 32 mg
Palladon® Retard Oral Cap 4, 8, 16, 24 mg
DE Jurnista®
Oral
Tab 4, 8, 16, 32, 64 mg
Palladon Uno® Oral Cap 12, 16, 24, 32 mg Palladon® retard Oral Cap 4, 8, 16, 24 mg
UK Palladone® SR
Oral
Cap 2, 4, 8, 16, 24 mg
US Exalgo®
Oral
Tab 8, 12, 16 mg
Palladone®* Oral Cap 12, 16, 24, 32 mg
Morphine ER AT Compensan® retard
Oral
Tab 100, 200, 300 mg

Opioid Therapy for Cancer-Related Pain
14
Generic Names Trade Names Route of Administration
Formulation
Kapanol CSR® Oral Cap 50, 100 mg M - dolor® retard Oral Cap 10, 30, 60, 100, 200 mg Mundidol® retard,
Vendal® retard Oral Tab 10, 30, 60, 100, 200 mg
Mundidol Uno® retard Oral Cap 30, 60, 120, 200 mg Relimal® Oral Tab 200 mg Substitol® retard Oral Cap 120, 200 mg
CH Kapanol®
Oral
Cap 20, 50, 100 mg
M-retard Helvepharm® Oral Tab 10, 30, 60, 100, 200 mg MST Continus® Oral Susp 20, 30, 60, 100, 200 mg Sevre-Long® Oral Cap 30, 60, 120, 200 mg
DE Capros®
Oral
Cap 10, 20, 30, 60, 120, 200 mg
M-beta®, Morph Sandoz®, Morph® retard, Morphanton®, Morpholar®
Oral Tab 10, 30, 60, 100 mg
M-long® Oral Cap 10, 30, 60, 100 mg MST Mundipharma®,
MSTW Krugmann® Oral Tab 10, 30, 60, 100, 200 mg
Kapanol®, Morsan® Oral Cap 20, 50, 100 mg MST Continus® Oral Cap 30, 60, 100, 200 mg MST Retard-Granulat® Oral Gran 30, 60, 100, 200 mg M-Stada® Oral Tab 30, 60, 100, 200 mg Zomorph® Oral Cap 20, 40, 60, 120, 200 mg
UK Morphgesic® SR
Oral
Tab 10, 30, 60, 100 mg
MST Continus® Oral Tab 5, 10, 15, 30, 60, 100, 200 mg MST Continus® Oral Susp 20, 30, 60, 100, 200 mg MXL® Oral Cap 30, 60, 90, 120, 150, 200 mg Filnarine® SR, Zomorph® Oral Tab 10, 30, 60, 100, 200 mg
US Avinza®
Oral
Cap 3, 45, 60, 75, 90, 120 mg
Kadian® Oral Cap 10, 20, 30, 50, 60, 80, 100, 200 mg MS Contin® Oral Tab 15, 30, 60, 100, 200 mg Oramorph SR® Oral Tab 15, 30, 60, 100 mg
Morphine ER + Naltrexone
US Embeda®*
Oral
Cap 20/0.8, 30/1.2, 50/2, 60/2.4, 80/3.2, 100/4 mg
Oxycodone ER AT Carenox®
Oral
Tab 5, 10, 20 mg
Merlodon® Oral Tab 20, 30, 40, 50, 60, 80 mg Maridolor® Oral Tab 20, 40, 80 mg OxyGerolan®,
OxyContin® retard Oral Tab 5, 10, 20, 40, 80 mg
CH OxyContin® Retard
Oral
Tab 5, 10, 20, 40, 80 mg
DE
Opioid Therapy for Cancer-Related Pain
15
Generic Names Trade Names Route of Administration
Formulation
Kancodal HEXAL® Oral Tab 10, 20 mg OxyContin®, Oxygesic® Oral Tab 5, 10, 20, 40, 80 mg
UK OxyContin®
Oral
Tab 5, 10, 15, 20, 30, 40, 60, 80, 120 mg
US OxyContin®
Oral
Tab 10, 15, 20, 30, 40, 60, 80, 160 mg
Oxycodone ER + Naloxone
AT Targin®, Retardtabletten
Oral
Tab 5/2,5, 10/5, 20/10, 40/20 mg
CH Targin®, Retardtabletten
Oral
Tab 5/2,5, 10/5, 20/10, 40/20 mg
DE Oxynal®, Retardtabletten
Oral
Tab 10/5, 20/10 mg
Targin®, Retardtabletten Oral Tab 5/2,5, 10/5, 20/10, 40/20 mg
UK Targinact®
Oral
Tab 5/2.5, 10/5, 20/10, 40/20 mg
Oxymorphone ER US Opana® ER
Oral
Tab 5, 7.5, 10, 15, 20, 30, 40 mg
Tapentadol hydrochloride ER
DE Palexia® retard
Oral
Tab
Yantil® retard Oral Tab
UK Palexia® SR
Oral
Tab 50, 100, 150, 200, 250 mg
US Nucynta® ER
Oral
Tab 50, 100, 150, 200, 250 mg
Tramadol ER AT Adamon® SR
Oral
Cap 50, 100, 150, 200 mg
Adamon® long retard Oral Tab 150, 200, 300, 400 mg Contramal® retard,
Nobligan® retard Oral Tab 50 mg
Cromatodol® Oral Cap 100, 200 mg Lanalget® retard,
Tradolan® retard, Tramal® retard, Tramabene®, Tramadolor® retard, Tramundal® retard
Oral Tab 100, 150, 200 mg
Noax uno® Oral Tab 100, 200, 300 mg Tramadolor Uno® retard Oral Tab 200 mg
CH Tramal® retard, Tramundin®
Oral
Tab 100, 150, 200 mg
Tramactil Uno® Oral Tab 100, 200, 300 mg Tradonal one® Oral Tab 150, 200, 300, 400 mg

Opioid Therapy for Cancer-Related Pain
16
Generic Names Trade Names Route of Administration
Formulation
DE CG 315/1 long, Tramadura®, Tramdol® Retard
Oral
Tab 100 mg
Amadol® Retard, Nobligan® retard, Tramal® retard
Oral Tab 50, 100, 150, 200 mg
Amadol®, Tramabeta long®, Tramabeta® retard, Tramadolor ID®, Tramagit®, Tramal long®, Tramamed®, Tramil® RT, Tramol® RT, Tramundin® retard
Oral Tab 100, 150, 200 mg
Tramalgin® RT Oral Tab 150, 200 mg Hexamadol® Retard,
Hexatram® Retard, Tramasan® Retard
Oral Tab 200 mg
T-Long®, Tramabene Uno®
Oral Cap 100, 150, 200 mg
Tramadolor® einmal täglich
Oral Tab 100, 200, 300 mg
Travex One® Oral Tab 150, 200, 300, 400 mg
Tramadolor long®, Tramadura®, Travex® retard
Oral Cap 50, 100, 150, 200 mg
UK Larapam®, Mabron®, Marol®, Zeridame SR®, Zydol SR®
Oral
Tab 100, 150, 200 mg
Tradorec XL® Oral Tab 100, 200, 300 mg
Zamadol® 24hr, Zydol XL®
Oral Tab 150, 200, 300, 400 mg
Maxitram®SR Oral Tab 50, 100, 150, 200 mg Tramquel® SR,
Zamadol® SR Oral Cap 50, 100, 150, 200 mg
US Conzip®
Oral
Cap 50, 100, 150, 200 mg
Ryzolt®, Ultram® ER Oral Tab 100, 200, 300 mg
* No longer being marketed
Abbreviations: AT, Austria; Cap, capsule; CH, Switzerland; DE, Germany; ER, extended-release; Gran, Granule; h, hour; mg, milligram; RT, retard; SR, sustained-release; Susp, suspension; Tab, tablet; TDP, trans-dermal patch; UK, United Kingdom; US, United States; XL, extended length; μg, microgram. 1Austria: Austria Codex. Retrieved January 28, 2012 from http://www.univadis.at/ 2Switzerland: Medicinal product information. Swiss Agency for Therapeutic Products. Retrieved January 28, 2012 from http://swissmedinfo.oddb.org/ 3Germany: AMIS Drug Information System. German Institute of Medical Documentation and Information. Retrieved January 28, 2012 from http://www.dimdi.de/static/en/amg/amis/index.htm 4UK: British National Formulary. 61st edition. 2011. British Medical Association and Royal Pharmaceutical Society of Great Britain. UK: The electronic Medicines Compendium (eMC). Retrieved January 28, 2012 from http://www.medicines.org.uk/ 5US: Drugs@FDA: FDA Approved Drug Products. U.S. Food and Drug Administration. Retrieved January 28, 2012 from http://www.accessdata.fda.gov/scripts/cder/drugsatfda/index.cfm

Opioid Therapy for Cancer-Related Pain
17
2.2 Scope and Key Questions
This review compares the efficacy, efficacy and harms of oral or transdermal extended-
release opioids used for treatment of adults with moderate to severe cancer-related pain.
We also address the clinical importance of subgroup status that may affect efficacy, efficacy,
and harms; these include sex, age, ethnic or socioeconomic groups, intensity and quality of
pain, and patients taking various co-analgesics. We approach each key question by
considering the relevant populations, interventions, comparators, outcomes, timing, and
settings (PICOTS). In this review, we address the following Key Questions (KQs):
Key Question 1: How do extended-release opioids compare in their analgesic efficacy and
effectiveness in treating adult patients with cancer-related pain?
Key Question 2: How do extended-release opioids compare in their risk for harms in treating
adult patients with cancer-related pain?
Key Question 3: How do efficacy, effectiveness, or risk for harms of treatment with
extended-release opioids for cancer-related pain differ for the following subpopulations:
Patients with moderate vs. severe cancer pain?
Patients with breakthrough pain?
Patients with a neuropathic cancer pain component?
Different sex, or different age, ethnic or socioeconomic groups?
Patients taking other commonly prescribed co-analgesics (e.g., non-steroidal
anti-inflammatory drugs, antiepileptic drugs, antidepressants)?
Figure 2 depicts the analytic framework for the comparative efficacy, effectiveness and risk
of harms for extended-release opioids in adult patients with moderate to severe cancer pain.
KQs are displayed within the context of the PICOTS described in more detail in Methods.
Beginning with a population of adults with cancer-related pain, the figure illustrates the
comparative effects of extended-release opioids on health outcomes, including pain

Opioid Therapy for Cancer-Related Pain
18
intensity, quality of life, functional capacity, patient perceived effectiveness and cognitive
performance (KQ1). KQ2 addresses the comparative risks of opioid-related harms from these
interventions. Finally, subgroups within the overall population will be identified based on
sex, age, ethnic or socioeconomic groups, intensity and quality of pain, and patients taking
various co-analgesics (KQ3).
Figure 2: Analytical Framework of the Comparative Efficacy, Effectiveness, and Risk for Harms of Extended-Release Opioids in Patients with Cancer-Related Pain.
Adverse effects of intervention
(KQ2)
Serious adverse events
Constipation
Nausea and vomiting
and other adverse events
Discontinuation of
treatment:
Due to lack of
efficacy (KQ1)
Due to adverse
events (KQ2)
Differences in (KQ1):
Pain relief
Quality of life
Patient perceived
effectiveness
and other health-related
outcomes
Extended-release opioids
Adult patients with cancer-
related pain
Subgroups: (KQ3)
1 Sex
2 Age
3 Ethnic groups
4 Socioeconomic groups
5 Intensity and quality of pain
6 Patients taking co-analgesics

Opioid Therapy for Cancer-Related Pain
19
3 Methods
The PROSPERO (International Prospective Register of Systematic Reviews:
http://www.crd.york.ac.uk/prospero) registration number of this review is:
CRD42012002153
The main sections in this chapter reflect the elements of the protocol established for the
review. All methods and analyses were determined a priori.
3.1 Topic Refinement and Review Protocol
During the course of topic development and refinement, we worked with the commissioner
of the report to develop a draft and final protocol for the systematic review process. We
generated an analytic framework, preliminary KQs, and preliminary inclusion/exclusion
criteria in the form of PICOTS. The processes were guided by the information provided by
the funder of the review, a scan of the literature, and methods and content experts.
3.2 Search Strategy
To identify articles relevant to each KQ, we searched PubMed, the Cochrane Library,
EMBASE, International Pharmaceutical Abstracts, CINAHL, BIOSIS and Web of Science. The
full search strategy is presented in Appendix A. We used either Medical Subject Headings
(MeSH) or major headings as search terms when available and key words when appropriate,
focusing on terms to describe the relevant populations and interventions of interest. We
limited the electronic searches to human and adult populations. Sources were searched
from January 1980 to July 2012. We manually searched reference lists of pertinent reviews,
included trials, and background articles on this topic to look for any relevant citations that
our searches might have missed. We imported all citations into an EndNote® X4 electronic
database. Searches were run by an experienced information scientist.
We also searched for unpublished studies (i.e., grey literature) relevant to this review using
OpenGrey (http://www.opengrey.eu/), the GlaxoSmithKline Study Register (http://www.gsk-
clinicalstudyregister.com/), ClinicalTrials.gov (http://clinicaltrials.gov/), Drugs@FDA

Opioid Therapy for Cancer-Related Pain
20
(http://www.accessdata.fda.gov/scripts/cder/drugsatfda/), the World Health Organization’s
International Clinical Trials Registry Platform (http://www.who.int/ictrp/en/), and the
National Cancer Institute’s Clinical Trial Database (http://www.cancer.gov/clinicaltrials). In
addition, we contacted pharmaceutical companies requesting any unpublished studies or
data relevant for this review (see Appendix B). To include information from the
pharmaceutical industry, we required studies to meet all inclusion criteria and to contain
enough information on research methods to be able to assess risk of bias. Furthermore, we
contacted all authors from studies published only as abstracts to ascertain if these abstracts
were ever published as full papers and could be included in our study. Finally, in cases in
which relevant information was unclear or not reported, we contacted authors in an attempt
to obtain additional or unpublished information.
3.3 Eligibility Criteria
We developed eligibility (inclusion and exclusion) criteria with respect to patient
populations, interventions, comparators, outcomes, timing, settings, study designs, and
durations for each KQ. We included only studies that were published in English or German
language. For cross-over RCTs, we used data of the study period before the cross-over only.
3.3.1 Population
Adult patients with moderate or severe cancer-related pain of any aetiology; aetiology may
be primary or secondary malignancy from solid or haematological tumours. Studies
investigating the efficacy of medications for the treatment of breakthrough pain were
excluded.
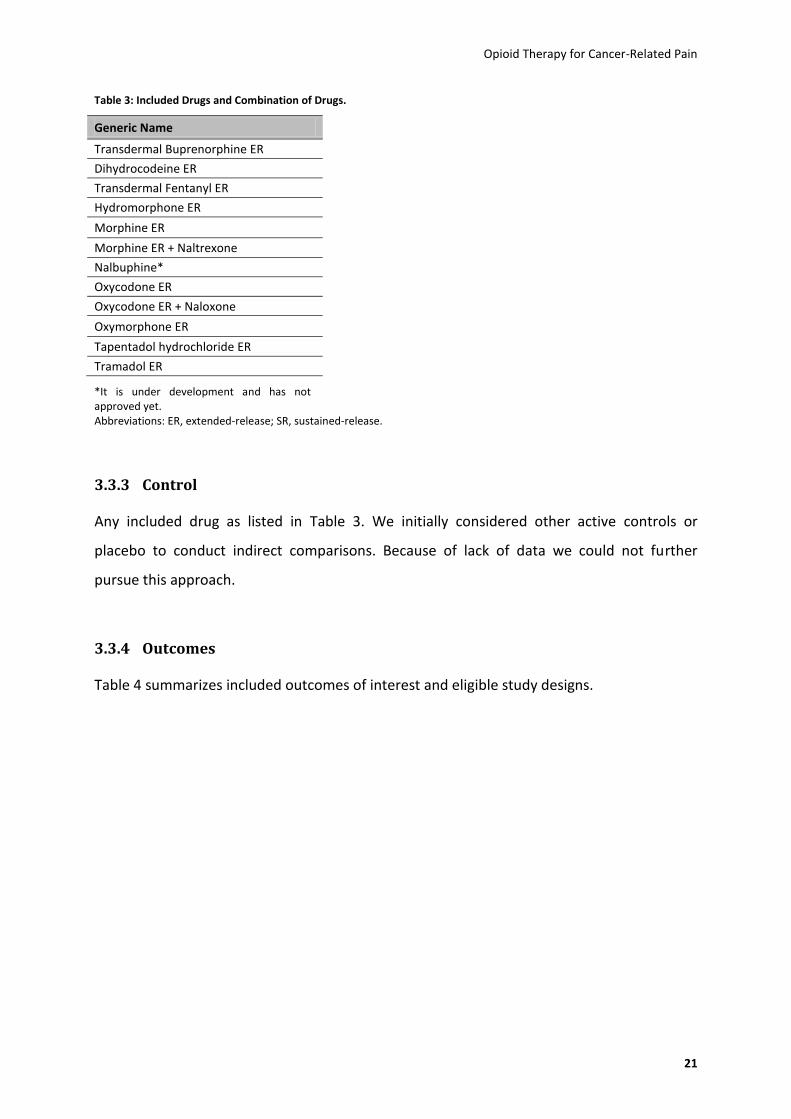
3.3.2 Intervention
Oral or transdermal extended-release opioids (WHO level III or WHO level II if approved for
moderate to severe pain in Germany, Austria, Switzerland, the United Kingdom, or the
United States; listed in Table 3)
Opioid Therapy for Cancer-Related Pain
21
Table 3: Included Drugs and Combination of Drugs.
Generic Name
Transdermal Buprenorphine ER
Dihydrocodeine ER
Transdermal Fentanyl ER
Hydromorphone ER
Morphine ER
Morphine ER + Naltrexone
Nalbuphine*
Oxycodone ER
Oxycodone ER + Naloxone
Oxymorphone ER
Tapentadol hydrochloride ER
Tramadol ER
*It is under development and has not approved yet. Abbreviations: ER, extended-release; SR, sustained-release.
3.3.3 Control
Any included drug as listed in Table 3. We initially considered other active controls or
placebo to conduct indirect comparisons. Because of lack of data we could not further
pursue this approach.
3.3.4 Outcomes
Table 4 summarizes included outcomes of interest and eligible study designs.

Opioid Therapy for Cancer-Related Pain
22
Table 4: Outcomes and Eligibility Criteria.
Outcome Study Eligibility Criteria
Efficacy / effectiveness
Health outcomes: o Pain intensity (patient-reported) o Quality of life (patient-reported) o Functional capacity o Patient perceived effectiveness o Cognitive performance
Discontinuation due to lack of efficacy / effect
Head-to-head double-blind RCTs1 or
systematic reviews +/- meta-analysis comparing 1 opioid to another o Low or unclear risk of bias o ≥ 1 week study duration
Risk for Harms
Overall adverse events
Serious adverse events
Specific adverse events, including: o Nausea and vomiting o Constipation o Dizziness o Drowsiness o Somnolence o Fatigue
Discontinuations due to adverse events
Head-to-head double-blind RCTs or systematic reviews +/- meta-analysis comparing 1 opioid to another o Low or unclear risk of bias o ≥ 1 week study duration
Open label or single-blinded RCTs (head-to-head), controlled observational studies (prospective and retrospective) o Low or unclear risk of bias o ≥ 1 week study duration o n ≥ 100
Abbreviations: n, number of participants; RCT, randomized controlled trial.
3.3.5 Timing
Studies with a duration of at least one week were eligible for this review.
3.3.6 Setting
We considered any setting.
3.4 Study Selection
We developed and pilot-tested literature review forms for abstract and full-text reviews (see
Appendix C). Two trained members of the research team independently reviewed all titles
and abstracts (identified through searches) for eligibility against our inclusion/exclusion
criteria. Studies marked for possible inclusion by either reviewer underwent a full-text
review. For studies that lacked adequate information to determine inclusion or exclusion, we
retrieved the full-text and then made the determination. If the necessary information in full-
1 for cross-over designs, we used only data after the first period before the cross-over.
Opioid Therapy for Cancer-Related Pain
23
text articles was unclear or missing, we contacted authors of the publications. All results
were tracked in an EndNote® database.
We retrieved the full-texts of all articles included during the title and abstract review phase.
Two trained members of the research team independently reviewed each full-text article for
inclusion or exclusion based on the eligibility criteria described above. If both reviewers
agreed that a study did not meet the eligibility criteria, we excluded it. If the reviewers
disagreed, they resolved conflicts by discussion and consensus or by consulting a third
member of the review team. All results were tracked in an EndNote® database. We recorded
the principal reason that each excluded full-text publication did not satisfy the eligibility
criteria (Appendix H).
3.5 Data Extraction
For studies that met our inclusion criteria and were of low or unclear risk of bias, we
extracted important information into a structured data abstraction form. We designed, pilot-
tested, and used structured data extraction forms to gather pertinent information from each
article; this included characteristics of study populations, settings, interventions,
comparators, study designs, methods, and results. Trained reviewers extracted the relevant
data from each included article into the data extraction forms. All data abstractions were
reviewed for completeness and accuracy by a second member of the team. We recorded
intention-to-treat (ITT) results if available. All data abstraction was performed using
Microsoft Excel® software. We did not extract complete data from studies that we rated as
high risk of bias.
3.6 Risk of Bias Assessment of Individual Studies
To assess the risk of bias (internal validity) of studies for major outcomes of interest, we
used the Cochrane risk of bias tool.(36) For observational studies we employed predefined
criteria as outlined by Deeks et al.(37) We assessed selection bias, confounding,
performance bias, detection bias, and attrition bias; we included questions about adequacy
of randomization, allocation concealment, similarity of groups at baseline, masking, attrition,

Opioid Therapy for Cancer-Related Pain
24
whether ITT analysis was used, method of handling dropouts, and treatment fidelity. We
rated the studies as low, unclear, or high risk of bias.
In general terms, a study categorized as low risk of bias implies confidence that results
represent the true treatment effects. A study with unclear risk of bias is susceptible to some
risk of bias but probably not enough to invalidate its results. A study assessed as high risk of
bias has significant flaws of various types (e.g., stemming from serious errors in design,
conduct, or analysis) that may invalidate its results.
Two independent reviewers assessed the risk of bias for each study; one of the two
reviewers was always an experienced or senior investigator. Disagreements between the
two reviewers were resolved by discussion and consensus or by consulting a third member
of the team. Appendix D lists studies rated as high risk of bias and reasons for the risk of bias
rating.
In addition to methodological shortcomings, we also assessed the dosing equivalence of
drugs compared within the same study. We used the equianalgesic dose calculator of the
Johns Hopkins University (www.hopweb.org).
3.7 Data Synthesis
Because quantitative synthesis was not appropriate (e.g., because of clinical heterogeneity,
insufficient number of similar studies, or variation in reported outcomes), we synthesized
the results qualitatively.
3.8 Strength of Body of Evidence
We graded the strength of the available evidence in a four-part hierarchy based on an
approach devised by the GRADE (Grading of Recommendations Assessment, Development
and Evaluation) working group.(38) As shown in Table 5 we used four grades: high,
moderate, low, and very low. Gradings reflect the strength of the body of evidence to
answer key questions with respect to the comparative efficacy, effectiveness, and risk of
harms of extended-release opioids.
Opioid Therapy for Cancer-Related Pain
25
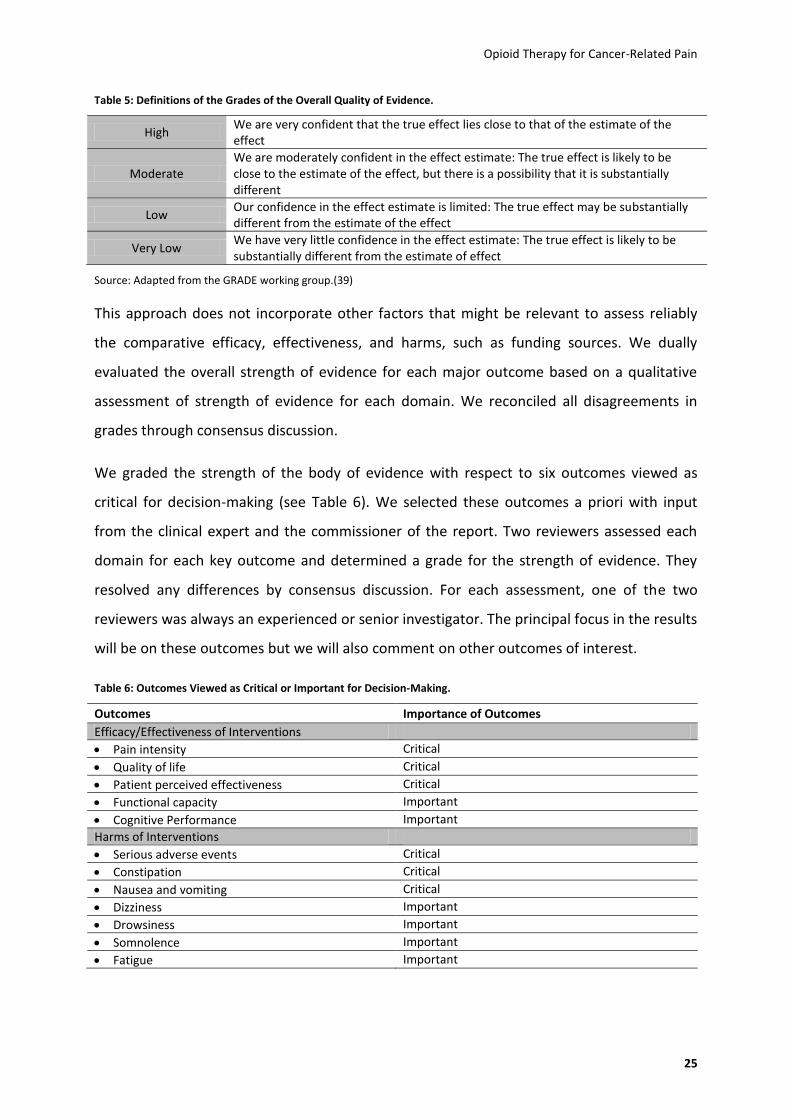
Table 5: Definitions of the Grades of the Overall Quality of Evidence.
High We are very confident that the true effect lies close to that of the estimate of the effect
Moderate We are moderately confident in the effect estimate: The true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different
Low Our confidence in the effect estimate is limited: The true effect may be substantially different from the estimate of the effect
Very Low We have very little confidence in the effect estimate: The true effect is likely to be substantially different from the estimate of effect
Source: Adapted from the GRADE working group.(39)
This approach does not incorporate other factors that might be relevant to assess reliably
the comparative efficacy, effectiveness, and harms, such as funding sources. We dually
evaluated the overall strength of evidence for each major outcome based on a qualitative
assessment of strength of evidence for each domain. We reconciled all disagreements in
grades through consensus discussion.
We graded the strength of the body of evidence with respect to six outcomes viewed as
critical for decision-making (see Table 6). We selected these outcomes a priori with input
from the clinical expert and the commissioner of the report. Two reviewers assessed each
domain for each key outcome and determined a grade for the strength of evidence. They
resolved any differences by consensus discussion. For each assessment, one of the two
reviewers was always an experienced or senior investigator. The principal focus in the results
will be on these outcomes but we will also comment on other outcomes of interest.
Table 6: Outcomes Viewed as Critical or Important for Decision-Making.
Outcomes Importance of Outcomes
Efficacy/Effectiveness of Interventions
Pain intensity Critical
Quality of life Critical
Patient perceived effectiveness Critical
Functional capacity Important
Cognitive Performance Important
Harms of Interventions
Serious adverse events Critical
Constipation Critical
Nausea and vomiting Critical
Dizziness Important
Drowsiness Important
Somnolence Important
Fatigue Important

Opioid Therapy for Cancer-Related Pain
26
4 Results
4.1 Introduction
This chapter is organized as follows: First, we discuss general results of the literature
searches and characteristics of included studies. Next, we present the available evidence by
KQ. Within each KQ we present results on the comparative efficacy, effectiveness, or risk of
harms first by outcome and second by individual drug-to-drug comparisons. In addition, we
present key points and a detailed synthesis in each KQ section. For each outcome deemed to
be critical for decision making, we rated the strength of evidence. Appendix E contains the
GRADE evidence profiles which present the ratings of each domain for each critical outcome.
Manufacturers of opioids use different terms to indicate extended-release formulations such
as sustained-release, controlled-release, prolonged-release, or long-acting. To ease
readability, we use only the term extended-release or the abbreviation ER. Unless otherwise
stated, the route of administration is oral. If not stated otherwise, the described extended
release opioids are administered orally.
Studies reviewed for this report employed a notable array of scales to assess outcomes of
interest. Most were pertinent to pain and specific adverse events, but some are considered
more generic instruments that assess aspects such as health-related quality of life, for
example. Appendix F summarizes commonly used instruments and the meaning of scores.
Appendix G defines commonly used abbreviations in this report.
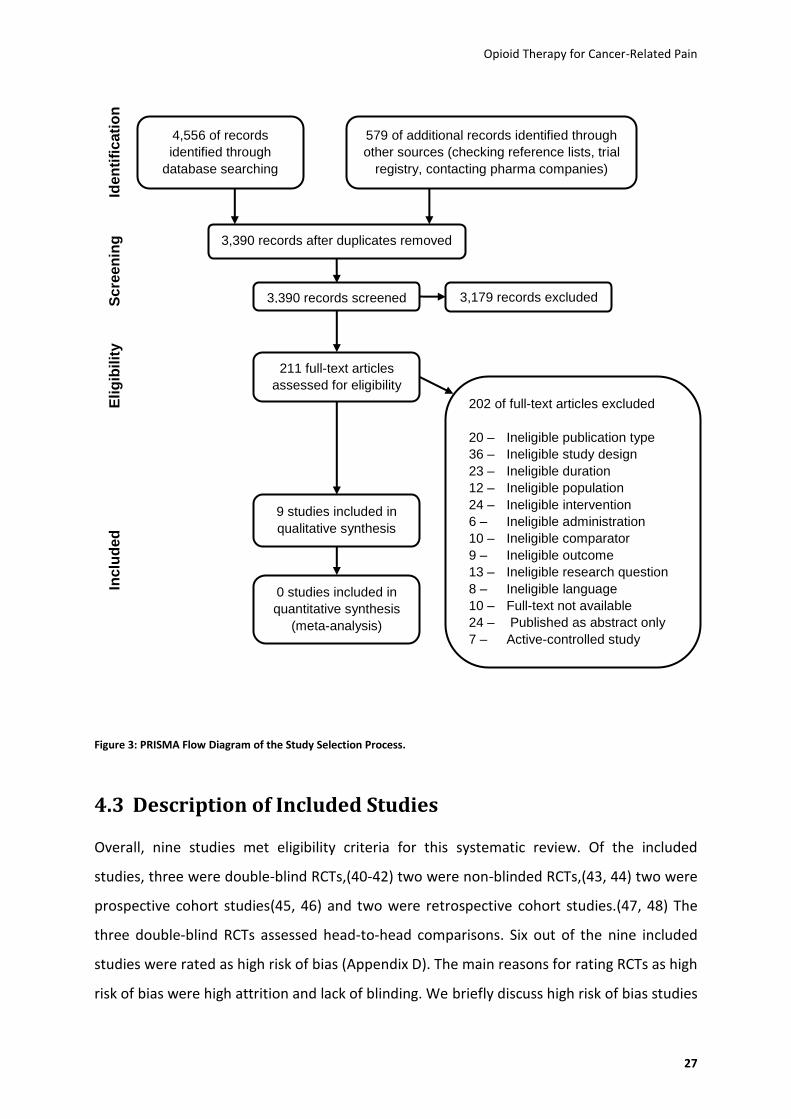
4.2 Results of Literature Searches
We identified 5,135 citations from searches and reviews of reference lists and screened
3,390 records, after removal of duplicates. Figure 3 documents the disposition of the 211
articles retrieved for full-text review for this report. Overall, we included nine studies, and
excluded 202 articles for various reasons. Articles excluded during full-text review are listed
in Appendix H with reasons for exclusions.
Opioid Therapy for Cancer-Related Pain
27
Figure 3: PRISMA Flow Diagram of the Study Selection Process.
4.3 Description of Included Studies
Overall, nine studies met eligibility criteria for this systematic review. Of the included
studies, three were double-blind RCTs,(40-42) two were non-blinded RCTs,(43, 44) two were
prospective cohort studies(45, 46) and two were retrospective cohort studies.(47, 48) The
three double-blind RCTs assessed head-to-head comparisons. Six out of the nine included
studies were rated as high risk of bias (Appendix D). The main reasons for rating RCTs as high
risk of bias were high attrition and lack of blinding. We briefly discuss high risk of bias studies
4,556 of records
identified through
database searching
579 of additional records identified through
other sources (checking reference lists, trial
registry, contacting pharma companies)
3,390 records after duplicates removed
3,390 records screened 3,179 records excluded
211 full-text articles
assessed for eligibility
9 studies included in
qualitative synthesis
0 studies included in
quantitative synthesis
(meta-analysis)
202 of full-text articles excluded
20 – Ineligible publication type
36 – Ineligible study design
23 – Ineligible duration
12 – Ineligible population
24 – Ineligible intervention
6 – Ineligible administration
10 – Ineligible comparator
9 – Ineligible outcome
13 – Ineligible research question
8 – Ineligible language
10 – Full-text not available
24 – Published as abstract only
7 – Active-controlled study
Iden
tifi
cati
on
S
cre
en
ing
E
lig
ibilit
y
Inclu
de
d

Opioid Therapy for Cancer-Related Pain
28
in the report because for many comparisons or outcomes of interest no studies of better
methodological quality were available.
Three(41, 42, 44) of the nine included studies were sponsored by the pharmaceutical
industry; in one case(40) funding was not explicitly reported but the second author was
affiliated with the manufacturer of the study medications. The other five studies did not
report their funding source.(43, 45-48)
We included extended-release opioids administered orally or transdermally. Only two
medications, transdermal fentanyl and transdermal buprenorphine are available as
transdermal applications. For most comparisons of interest, we could not find any studies.
Out of 66 possible comparisons for the 12 included extended-release opioids, we found
studies for only nine head-to-head comparisons.
4.4 Key Question 1: Comparative Efficacy and Effectiveness of
Extended-Release Opioids
4.4.1 Description of Included Studies
Three studies met eligibility criteria for KQ1, the comparative efficacy and effectiveness of
extended-release opioids.(40-42) Table 7 summarizes the characteristics of the available
body of evidence for KQ1.
Opioid Therapy for Cancer-Related Pain
29
Table 7: Characteristics of the Available Evidence for KQ1.
Characteristic Details
N studies: (N patients) 3 studies (428 patients)
Range of means of age in studies: 56 – 61.68
Sex: N patients (%) Female Male
220 (51.4%) 208 (48.6%)
Race: N patients (%) White Non-white NR
407 (95%) 6 (1.5%) 15 (3.5%)
Setting: N studies Inpatients, outpatients and day patients NR
1 2
Risk of Bias: N studies (%) High Unclear Low
3 (100%) 0 0
Comparisons: N studies (N patients randomized) Oral morphine ER vs. oral hydromorphone ER Oral hydromorphone ER vs. oral oxycodone ER Oral oxycodone ER vs. oral oxycodone ER plus naloxone
1 (200) 1 (44) 1 (184)
Abbreviations: ER, extended-release; N, number;NR, not reported vs., versus.
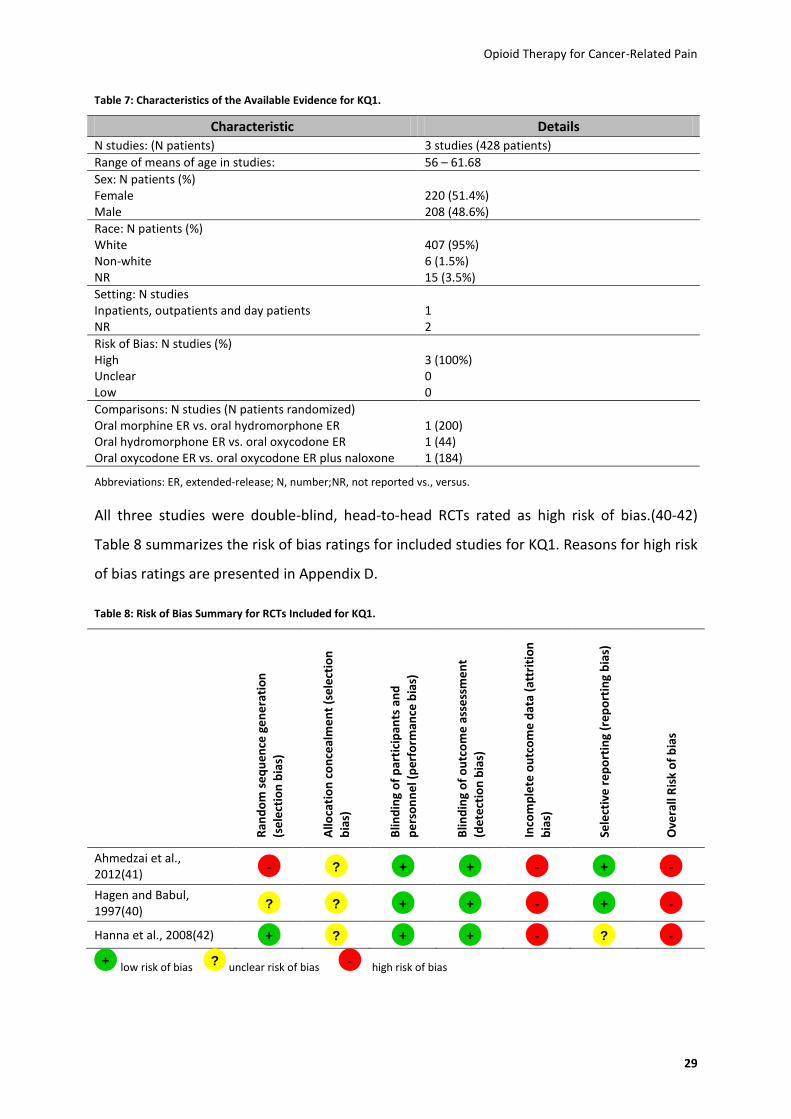
All three studies were double-blind, head-to-head RCTs rated as high risk of bias.(40-42)
Table 8 summarizes the risk of bias ratings for included studies for KQ1. Reasons for high risk
of bias ratings are presented in Appendix D.
Table 8: Risk of Bias Summary for RCTs Included for KQ1.
Ran
do
m s
eq
uen
ce g
en
era
tio
n
(se
lect
ion
bia
s)
Allo
cati
on
co
nce
alm
en
t (s
ele
ctio
n
bia
s)
Blin
din
g o
f p
arti
cip
ants
an
d
pe
rso
nn
el (
per
form
ance
bia
s)
Blin
din
g o
f o
utc
om
e a
sse
ssm
en
t
(de
tect
ion
bia
s)
Inco
mp
lete
ou
tco
me
dat
a (a
ttri
tio
n
bia
s)
Sele
ctiv
e r
ep
ort
ing
(re
po
rtin
g b
ias)
Ove
rall
Ris
k o
f b
ias
Ahmedzai et al., 2012(41)
Hagen and Babul, 1997(40)
Hanna et al., 2008(42)
low risk of bias unclear risk of bias high risk of bias
- ? + + - + -
? ? + + - + -
+ ? + + - ? -
+ ? -

Opioid Therapy for Cancer-Related Pain
30
4.4.2 Key Points
Out of 66 possible comparisons of extended-release opioids, we found information on
the comparative efficacy for only three comparisons.
For patients with cancer pain, morphine ER and hydromorphone ER led to similar
improvements of pain intensity, quality of life, functional capacity, and cognitive
functioning (very low strength of evidence, one study).
For patients with stable cancer pain, hydromorphone ER and oxycodone ER led to similar
improvements of pain intensity (very low strength of evidence, one study).
For patients with moderate or severe chronic cancer pain, oxycodone ER and oxycodone
plus naloxone ER led to similar improvements of pain intensity and quality of life (very
low strength of evidence, one study each).
Patients treated with morphine ER, hydromorphone ER, oxycodone ER, and oxycodone
plus naloxone ER had similar discontinuation rates because of lack of efficacy (very low
strength of evidence, three studies).
We could not find any eligible head-to-head evidence on transdermal buprenorphine ER,
dihydrocodeine ER, transdermal fentanyl ER, morphine plus naltrexone ER, nalbuphine
ER, oxymorphone ER, tapentadol hydrochloride ER, and tramadol ER.
4.4.3 Detailed Synthesis
Table 9 summarizes the characteristics of included studies for KQ1.
Because results at cross-over were not reported in the publication by Hagen and Babul(40),
we contacted authors to release unpublished data. Authors provided us with results on pain
intensity as the only outcome for KQ1 which is presented below.

Opioid Therapy for Cancer-Related Pain
31
Table 9: Study Characteristics for all Studies Included for KQ1, the Investigated Outcomes and Risk of Bias Ratings.
Study and Study Design
Country and Setting
Funding N Comparison Outcomes of Interest Risk of Bias Rating
Ahmedzai et al., 2012(41) double-blind RCT
International (Australia, Czech Republic, France, Germany, Hungary, Israel, Netherlands, Poland, United Kingdom), 64 study sites; setting NR
Mundipharma Research, Germany
184 Oral oxycodone ER vs. oral oxycodone plus naloxone ER
Pain intensity
Quality of life
High
Hagen and Babul, 1997(40) double-blind RCT
Canada; setting NR
NR 2
nd author
affiliated with Purdue Frederick, Canada (the producer of the study drugs)
44 Oral Hydromorphone ER vs. oral oxycodone ER
Pain intensity High
Hanna et al., 2008(42) double-blind RCT
International (Belgium, Canada, France, Germany, The Netherlands, Spain, Sweden, and the United Kingdom), 37 centres; inpatients, outpatients, and day patients
ALZA Corporation, USA
200 (IR phase) 163 (ER phase)
Oral morphine ER vs. oral hydromorphone ER
Pain intensity
Functional capacity
Quality of life
Patient perceived effectiveness
Cognitive performance
High
Abbreviations: ALZA, Alejandro Zaffaroni (portmanteau); IR, immediate-release; N, number of participants; NR, not reported; RCT, randomized controlled trial; vs., versus; ER, extended-release
In the following sections we present detailed analyses of head-to-head comparisons for each
outcome of interest. At the end of each outcome subchapter we summarize main results for
each outcome in a table. The order of the outcomes represents the importance of outcomes
as rated by our clinical experts – outcomes deemed to be critical for decision-making are
described first, followed by outcomes rated as important but not critical.
4.4.3.1 Pain Intensity
All three studies included for KQ1 assessed pain intensity.(40-42) Detailed results on pain
intensity are presented in Table 10.

Opioid Therapy for Cancer-Related Pain
32
Oral Morphine ER vs. Oral Hydromorphone ER
The only available evidence for this comparison was a double-blind head-to-head RCT by
Hanna et al.(42) We rated the study as high risk of bias because of an attrition rate of 34%.
Because the article reported only dosing ranges, we were unable to assess the dosing
equivalence. The study was sponsored by Alejandro Zaffaroni (ALZA) Corporation, a
producer of hydromorphone ER. Two hundred patients were initially randomized to
immediate-release (IR) morphine (n=101) or immediate-release hydromorphone (n=99).
Eighty-six patients completed the morphine IR phase and were then switched to morphine
ER. Seventy-seven patients completed the hydromorphone IR phase and then began taking
hydromorphone ER. The attrition rate because of lack of efficacy during the ER phase was
3.5% in the morphine ER group and 6.5% in the hydromorphone ER group.
During the extended-release phase, patients on both medications achieved a decrease in
pain intensity. The decrease in pain intensity was numerically smaller for patients treated
with morphine ER (decrease from 4.8 to 4.3 points) than hydromorphone ER (decrease from
5.0 to 3.5 points; p=NR) with respect to worst pain in the past 24 hours. Decreases were
similar between drugs for current pain in the morning (morphine ER: decrease from 3.4 to
2.8 points; hydromorphone ER: decrease from 3.3 to 2.4 points) and current pain in the
afternoon (morphine ER: decrease from 3.7 to 3.4 points; hydromorphone ER: decrease
from 3.6 to 2.6 points; p=NR, see Table 10). Both outcomes were measured on an 11-point
Brief Pain Inventory (BPI)-scale (0=no pain, 10=pain as bad as you can imagine). Differences,
however, did not reach statistical significance. Results of two other pain scales (least pain in
the last 24 hours and average pain in the last 24 hours (see Table 10) were also similar for
both study groups.
Because of methodological limitations, imprecision of results, and the fact that only a single
study assessed this outcome, the strength of evidence that morphine ER and
hydromorphone ER are equally efficacious with respect to pain intensity is very low (see
Appendix-Table 3).
Oral Hydromorphone ER vs. Oral Oxycodone ER
One study met our eligibility criteria for this comparison – a high risk of bias RCT(40) (n=44)
comparing the efficacy of hydromorphone ER with oxycodone ER during a study period of

Opioid Therapy for Cancer-Related Pain
33
seven days. Funding of this study was not reported but one author had an affiliation with the
producer of both study medications. The study employed a cross-over design; in the
following section we report comparisons of the two drugs before cross-over. The study was
rated as high risk of bias because of an attrition rate of 30% and a lack of ITT-analysis.
Results showed a numerically smaller reduction in pain intensity measured on a 100mm
visual analog scale (VAS) with hydromorphone ER compared with oxycodone ER after seven
days of treatment (difference of 4.3 mm; p=NR, see Table 10). When pain intensity was
measured with an ordinal scale (0=none, 1=mild, 2=moderate, 3=severe, 4=excruciating
pain), no difference in reduction of pain intensity between the groups was found (see Table
10). Results, however, have to be interpreted cautiously because the mean morphine-dose-
equivalent of oxycodone ER (124 mg/d) was 50% higher than that of hydromorphone ER (30
mg/d). The higher mean dosage for patients on oxycodone ER can partly be explained by a
higher mean pain score at baseline compared with patients on hydromorphone ER
(33.28mm vs. 27.87mm).
Because of methodological limitations, imprecision of results, and the fact that only a single
study assessed this outcome, the strength of evidence that hydromorphone ER and
oxycodone ER are equally efficacious with respect to pain intensity is very low (see
Appendix-Table 4).
Oral Oxycodone ER vs. Oral Oxycodone plus Naloxone ER
The only available evidence for this comparison was a double-blind head-to-head RCT by
Ahmedzai et al.with a high risk of bias.(41) This study investigated the comparative efficacy
and risk of harms of oxycodone ER and oxycodone plus naloxone ER in 184 patients with
chronic moderate or severe cancer pain. Because of lack of information, we were unable to
assess the dosing equivalence of drugs in this study. Findings showed similar changes in pain
scores after four weeks as measured on an 11-point BPI (oxycodone ER: decrease from 4.18
to 3.52 points, oxycodone plus naloxone ER: decrease from 4.16 to 3.50; p=NR) (see Table
10). The study was funded by Mundipharma Research, the producer of oxycodone plus
naloxone ER. This RCT was rated as high risk of bias because of the use of a pseudo-random
number generator for randomization, per-protocol analysis for some of the outcomes, and a
high attrition rate (28%).

Opioid Therapy for Cancer-Related Pain
34
Because of methodological limitations, imprecision of results, and the fact that only a single
study assessed this outcome, the strength of evidence that oxycodone ER and oxycodone
plus naloxone ER are equally efficacious with respect to pain intensity is very low (see
Appendix-Table 5).

Opioid Therapy for Cancer-Related Pain
35
Table 10: Study Characteristics and Summary of Findings on Pain Intensity.
Study N Duration Comparison and Dose
Outcome Measure Pain Intensity Risk of Bias
Oral Morphine ER vs. Oral Hydromorphone ER
Hanna et al., 2008(42)
200 (IR phase) 163 (SR phase)
10-15 days
Morphine ER: 60-540 mg/d
Hydromorphone ER: 16-96 mg/d
BPI for worst pain in the past 24h (0=no pain, 10=pain as bad as you can imagine)
Similar reduction of pain intensity for worst pain in the past 24h with morphine ER; Mean score change: morphine ER:- 0.5, hydromorphone ER: -1.5; p=NR
High
BPI for least pain in the past 24h Similar changes for least pain in the past 24h; Mean score change: morphine ER: -0.4, hydromorphone ER: 0; p=NR
BPI for average pain in the past 24h Similar changes for average pain in the past 24h with both study drugs; Mean score change: morphine ER: -0.4, hydromorphone ER: -0.2; p=NR
BPI for current pain (AM/PM) Similar reduction of current pain AM/PM with morphine ER; Mean score change (pain now AM/PM): morphine ER: -0.6/-0.3 hydromorphone ER: -0.9/-1; p=NR
Oral Hydromorphone ER vs. Oral Oxycodone ER
Hagen and Babul, 1997(40)
44 7 days Hydromorphone ER: mean final dose 30 ± 6 mg/d Oxycodone ER: 124 ± 22 mg/d
Pain intensity VAS 0-100mm (0=no pain, 100=excruciating pain)
Less reduction of pain intensity with hydromorphone ER Mean score change: hydromorphone ER: -2.38, oxycodone ER: -6.70; p=NR
High
Ordinal pain scale (0=none, 1=mild, 2=moderate, 3=severe, 4=excruciating)
Similar reduction in pain intensity with both study drugs Mean score change: hydromorphone ER: -0.25, oxycodone ER: -0.24; p=NR

Opioid Therapy for Cancer-Related Pain
36
Study N Duration Comparison and Dose
Outcome Measure Pain Intensity Risk of Bias
Oral Oxycodone ER vs. Oral Oxycodone plus Naloxone ER
Ahmedzai et al., 2012(41)
184 4 weeks Oxycodone ER: mean 43.09 (SD 19.31) mg/d Oxycodone plus naloxone ER: 46.59 (SD 22.58) mg/d
BPI-SF questionnaire (0=no pain, 10=pain as bad as you can imagine)
Similar pain scores at baseline and at 4 weeks in both study groups; Mean score change: Oxycodone ER: -0.66 Oxycodone plus naloxone ER: -0.66, p=NR
High
Abbreviations : AM, ante meridiem (meaning before midday); BPI, brief pain inventory; BPI-SF, Brief Pain Inventory-Short form; d, day; ER, extended-release; h, hour; IR, immediate-release; mg, milligram; mm, millimeter; N, number of participants; NR, not reported; p, probability; PM, post meridiem (meaning after midday); SD, standard deviation; SR, sustained-release; VAS, visual analogue scale; vs., versus; μg, microgram.

Opioid Therapy for Cancer-Related Pain
37
4.4.3.2 Quality of Life
Among the three studies analysed for KQ1, two head-to-head trials provided data on quality
of life.(41, 42) Table 11 summarizes results of the included studies.
Oral Morphine ER vs. Oral Hydromorphone ER
The only available evidence for this comparison was the double-blind, high risk of bias head-
to-head trial (n= 200) by Hanna et al.(42) which has been described in detail above (within
the section on pain intensity). Quality of life was measured with a BPI interference scale for
enjoyment of life. Results showed similar improvements in quality of life scores between
patients treated with morphine ER (decrease from 3.9 to 3.5 points; p=NR) and
hydromorphone ER (decrease from 4.1 to 3.5 points; p=NR). BPI score changes for
relationship (0.1 vs. 0.2 points; p=NR) and mood (0.2 vs. 0.2 points; p=NR) were also similar
between groups (see Table 11).
Because of methodological limitations, imprecision of results and the fact that only a single
study assessed this outcome, the strength of evidence that morphine ER and
hydromorphone ER are equally efficacious with respect to quality of life is very low (see
Appendix-Table 3).
Oral Oxycodone ER vs. Oral Oxycodone plus Naloxone ER
Only one study met our eligibility criteria for this comparison.(41) This high risk of bias RCT
(n=184) by Ahmedzai et al. has been described in more detail in the section on pain
intensity. After four weeks of treatment, patients in both treatment groups reported similar
quality of life scores on the European Quality of Life Instrument (EuroQoL EQ-5D) (0.49 vs.
0.50; p=NR, Table 11).
Because of methodological limitations, imprecision of results and the fact that only a single
study assessed this outcome, the strength of evidence that oxycodone ER and oxycodone
plus naloxone ER are equally efficacious with respect to quality of life is very low (see
Appendix-Table 5).

Opioid Therapy for Cancer-Related Pain
38
Table 11: Study Characteristics and Summary of Findings on Quality Of Life.
Study N Duration Comparison and Dose
Outcome Measure
Quality of Life Risk of Bias
Oral Morphine ER vs. Oral Hydromorphone ER
Hanna et al., 2008(42)
200 (IR phase) 163 (SR phase)
10-15 days
Morphine ER: 60-540 mg/d vs. Hydromorphone ER: 16.96 mg/d
BPI interference scale for enjoyment of life (0=no interference, 10=complete interference)
Similar improvement for enjoyment of life with both study drugs: Mean score change morphine ER: -0.4, hydromorphone ER: -0.6; p=NR
High/
BPI interference scale for relationships
Similar results for relationships with both study drugs: Mean score change morphine ER: 0.1, hydromorphone ER: 0.2; p=NR
BPI interference scale for mood
Similar slight improvement for mood with both study drugs: Mean score change morphine ER: -0.2, hydromorphone ER: - 0.2; p=NR
Oral Oxycodone ER vs. Oral Oxycodone plus Naloxone ER
Ahmedzai et al., 2012(41)
184 4 weeks Oxycodone ER: mean 43.09 (SD 19.31) mg/d Oxycodone plus naloxone ER: 46.59 (SD 22.58) mg/d
EuroQoL EQ-5D Similar QoL scores at baseline and at 4 weeks in both study groups: Mean score at endpoint oxycodone ER: 0.49, oxycodone plus naloxone ER: 0.50; p=NR
High
Abbreviations : BPI, brief pain inventory; d, day; ER, extended-release; EuroQoL EQ-5D, European Quality of Life instrument; IR, immediate-release; mg, milligram; N, number of participants; NR, not reported; p, probability; QoL, quality of life; SD, standard deviation; SR, sustained-release; vs., versus.
4.4.3.3 Functional Capacity
Among the three studies analysed for KQ1 only one study reported information on
functional capacity (see Table 12).(42)
Oral Morphine ER vs. Oral Hydromorphone ER
The only available evidence for this comparison was a two-phase (IR phase and ER phase)
RCT (n=200) determining the equivalency of morphine ER and hydromorphone ER.(42)

Opioid Therapy for Cancer-Related Pain
39
Details of this study by Hanna et al. have been described above in the section on pain
intensity. Results presented a similar improvement of general activity (BPI interference scale
for general activity) in patients treated with morphine ER (decrease from 4.3 to 4.1 points; p
= NR) or hydromorphone ER (decrease from 4.2 to 3.7 points; p=NR).
Because of methodological limitations, imprecision of results, and the fact that only a single
study assessed this outcome, the strength of evidence that morphine ER and
hydromorphone ER are equally efficacious with respect to functional capacity is very low.
Table 12: Study Characteristics and Summary of Findings on Functional Capacity.
Study N Duration Comparison and dose
Outcome measure Functional capacity
Risk of bias
Oral Morphine ER vs. Oral Hydromorphone ER
Hanna et al., 2008(42)
200 (IR phase) 163 (SR phase)
10-15 days
Morphine ER: 60-540 mg/d Hydromorphone ER: 16-96 mg/d
Brief Pain Inventory interference scale for general activity (0=no interference, 10=complete interference)
Similar improvement for general activity with both study drugs: Mean score change morphine ER: -0.2, hydromorphone ER: -0.5; p=NR
High
Abbreviations: d, day; ER, extended-release; IR, immediate-release; mg, milligram; N, number of participants; NR, not reported; p, probability; SR, sustained-release.
4.4.3.4 Patient Perceived Effectiveness
Among the three studies analysed for KQ1 only one study reported information on patient
perceived effectiveness, which means patients’ global assessments of treatment
effectiveness as good, very good, or excellent. Table 13 presents results for patient
perceived effectiveness.
Oral Morphine ER vs. Oral Hydromorphone ER
The only available evidence for this comparison was a double-blind head-to-head RCT by
Hanna et al. (42) with a high risk of bias, described in detail in the section on pain intensity.
At the end of the 10-15 days ER-phase numerically more patients (80.2%) in the morphine ER
group than in the hydromorphone ER group (73.4%) rated the treatment as good, very good
or excellent (p=NR). This outcome was measured on a 5-point scale (1=poor, 2=fair, 3=good,
4=very good, 5=excellent). Using the data from the study we calculated a statistically not

Opioid Therapy for Cancer-Related Pain
40
significant difference between the two treatment groups (Odds ratio [OR]: 1.42, 95% CI 0.68-
2.97)
Because of methodological limitations, imprecision of results, and the fact that only a single
study assessed this outcome, the strength of evidence that morphine ER and
hydromorphone ER are equally efficacious with respect to perceived effectiveness is very
low (see Appendix-Table 3).
Table 13: Study Characteristics and Summary of Findings on Patient Perceived Effectiveness.
Study N Duration Comparison and Dose
Outcome Measure
Evaluation of Treatment
Risk of Bias
Oral Morphine ER vs. Oral Hydromorphone ER
Hanna et al., 2008(42)
200 (IR phase) 163 (SR phase)
10-15 days
Morphine ER: 60-540 mg/d Hydromorphone ER: 16-96 mg/d
5-point scale (1=poor, 2=fair, 3=good, 4=very good, 5=excellent)
80.2% of participants in the morphine ER group and 73.4% in the hydromorphone ER group rated the treatment as good, very good or excellent (p=NR)
High
Abbreviations: d, day; ER, extended-release; IR, immediate-release; mg, milligram; N, number of participants; NR, not reported; p, probability; SR, sustained-release.
4.4.3.5 Cognitive Performance
Among the three studies analysed for KQ1, only one high risk of bias RCT reported on
cognitive performance associated with the use of extended-release opioids.(42) Table 14
presents the results for the outcome cognitive performance.
Oral Morphine ER vs. Oral Hydromorphone ER
The only available evidence for this comparison was the high risk of bias head-to-head trial
by Hanna et al.(42) which has been described in more detail in the section on pain intensity.
The Mini-Mental State Examination scores for measuring cognitive performance of 200
participants revealed similar scores between the two treatment groups at endpoint (29.2 vs.
28.9; p=NR), with a small identical decline of scores (0.4 points) from baseline to endpoint in
both groups (see Table 14).

Opioid Therapy for Cancer-Related Pain
41
Table 14: Study Characteristics and Summary of Findings on Cognitive Performance.
Study N Duration Comparison and Dose
Outcome Measure
Cognitive Performance
Risk of Bias
Oral Morphine ER vs. Oral Hydromorphone ER
Hanna et al., 2008(42)
200 (IR phase) 163 (ER phase)
10-15 days
Morphine ER: 60-540 mg/d Hydromorphone ER: 16-96 mg/d
MMSE scores (0-30); higher scores indicate better cognitive performance
Similar scores at endpoint: 29.2 vs. 28.9, p=NR
High
Abbreviations: d, day; ER, extended-release; IR, immediate-release; mg, milligram; MMSE, Mini-Mental State Examination; N, number of participants; NR, not reported; p, probability; vs., versus.
4.4.3.6 Discontinuation Due to Lack of Efficacy
The rate of discontinuation due to lack of efficacy was similar among drugs and ranged from
1.1% (oxycodone plus naloxone ER) to 6.5% (hydromorphone ER). Nevertheless, because of
small sample sizes, differences among drugs have to be interpreted cautiously.
Table 15 presents rates of discontinuation due to lack of efficacy for the included double-
blind head-to-head studies for the comparative efficacy and effectiveness of extended-
release opioids.
Table 15: Rates of Discontinuation Due to Lack of Efficacy by Study Drug.
Study N per Drug Discontinuation Due to Lack of Efficacy (N)
Discontinuation Due to Lack of Efficacy (%)
Oral Morphine ER
Hanna et al., 2008(42) 86* 3 3.5
Oral Hydromorphone ER
Hagen and Babul, 1997(40) 19 NR NR
Hanna et al., 2008(42) 77* 5 6.5
Oral Oxycodone ER
Ahmedzai et al., 2012(41) 92 4 4.3
Hagen and Babul, 1997(40) 12** NR NR
Oral Oxycodone plus Naloxone ER
Ahmedzai et al., 2012(41) 92 1 1.1
* only phase II with ER medication ** only first phase before cross-over; three patients discontinued due to inadequate pain control from the whole populationAbbreviations: ER, extended-release; N, number of participants; NR, not reported.

Opioid Therapy for Cancer-Related Pain
42
4.5 Key Question 2: Comparative Risk of Harms of Extended-
Release Opioids
This chapter is structured as follows: First, we discuss general results of the literature
searches and characteristics of included studies. Next, we present key points followed by a
detailed synthesis of the available evidence. The detailed synthesis is structured by adverse
events:
Serious adverse events (section 4.5.3.1)
Discontinuation rates and overall tolerability (section Discontinuation Rates and
Overall Tolerability4.5.3.2)
Constipation (section 4.5.3.3)
Nausea and vomiting (section 4.5.3.4)
Dizziness (section 4.5.3.5)
Drowsiness, Somnolence, Fatigue, Sedation (section 4.5.3.6)
Diarrhea (section 4.5.3.7)
4.5.1 Description of Included Studies
Overall, nine studies with more than 2600 patients provided data on the assessment of
adverse events of extended-release opioids.(40-48). Table 16 summarizes the characteristics
of the available body of evidence for KQ2.

Opioid Therapy for Cancer-Related Pain
43
Table 16: Characteristics of the Available Evidence for KQ2.
Characteristic Details N Studies: (N patients) 9 studies (2663 patients)
Range of means of age in studies: 52.8 – 67.8
Sex: N patients (%) Female Male
1411 (53.0%) 1252 (47.0%)
Race: N patients (%) White Non-white NR
1559 (58.5%) 120 (4.5%) 984 (37.0%)
Setting: N studies (%) Inpatients, outpatients and day patients NR
7 (78%) 2 (22%)
Risk of Bias: N studies (%) High Unclear Low
6 (67%) 3 (33%) 0
Comparisons: N studies (N patients randomized) Oral morphine ER vs. oral hydromorphone ER Oral morphine ER vs. oral oxycodone ER Oral morphine ER vs. transdermal fentanyl ER Oral hydromorphone ER vs. oral oxycodone ER Oral hydromorphone ER vs. transdermal fentanyl ER Oral hydromorphone ER vs. transdermal buprenorphine ER Oral oxycodone ER vs. oral oxycodone + naloxone ER Oral oxycodone ER vs. transdermal fentanyl ER Transdermal fentanyl ER vs. transdermal buprenorphine ER
2 (302) 2 (1072) 4 (1198) 1 (44) 1 (124) 1 (124) 1 (184) 2 (993) 1 (124)
Abbreviations: ER, extended-release; N, number; NR, not reported; vs, versus.
In addition to the three RCTs that we included for comparative efficacy in KQ1(40-42), two
RCTs(43, 44) and four observational studies(45-48) met our eligibility criteria for the
assessment of the risk of harms. The risk of bias summaries of the five RCTs included for KQ2
are presented in Table 17. The risk of bias summaries for observational studies included for
KQ2 are presented in Table 18.

Opioid Therapy for Cancer-Related Pain
44
Table 17: Risk of Bias Summaries for RCTs Included for KQ2.
Ran
do
m s
eq
uen
ce g
en
era
tio
n
(se
lect
ion
bia
s)
Allo
cati
on
co
nce
alm
en
t (s
ele
ctio
n
bia
s)
Blin
din
g o
f p
arti
cip
ants
an
d
pe
rso
nn
el (
per
form
ance
bia
s)
Blin
din
g o
f o
utc
om
e a
sse
ssm
en
t
(de
tect
ion
bia
s)
Inco
mp
lete
ou
tco
me
dat
a (a
ttri
tio
n
bia
s)
Sele
ctiv
e r
ep
ort
ing
(re
po
rtin
g b
ias)
Ove
rall
Ris
k o
f b
ias
Ahmedzai et al., 2012(41)
Hagen and Babul, 1997(40)
Hanna et al., 2008(42)
Mercadante et al., 2008(43)
van Seventer et al., 2003(44)
low risk of bias unclear risk of bias high risk of bias
Table 18: Risk of Bias Summary for Observational Studies Included for KQ2.
Pro
spe
ctiv
e s
tud
y d
esi
gn
Stu
dy
gro
up
s re
cru
ite
d f
rom
sam
e
sou
rce
po
pu
lati
on
(se
lect
ion
bia
s)
Par
tici
pan
ts in
all
stu
dy
gro
up
s re
cru
ite
d
ove
r sa
me
tim
e p
eri
od
Incl
usi
on
an
d e
xclu
sio
n c
rite
ria
eq
ual
ly
app
lied
in a
ll st
ud
y gr
ou
ps
Blin
din
g o
f o
utc
om
e a
sse
ssm
en
t
(de
tect
ion
bia
s)
Equ
al o
utc
om
e m
eas
ure
s am
on
g st
ud
y
gro
up
s
Val
id a
nd
re
liab
le o
utc
om
e m
eas
ure
s
Equ
al t
ime
of
follo
w-u
p in
all
stu
dy
gro
up
s
Dif
fere
nce
s b
etw
ee
n s
tud
y gr
ou
ps
take
n
into
acc
ou
nt
in s
tati
stic
al a
nal
ysis
Co
nfo
un
din
g ad
eq
uat
ely
acc
ou
nte
d f
or
Att
riti
on
<2
0%
Dif
fere
nti
al a
ttri
tio
n <
15
%
Excl
usi
on
of
par
tici
pan
ts
Ad
eq
uat
e m
eth
od
of
han
dlin
g d
rop
-ou
ts
Hartung et al., 2007(48)
* *
*
Okamoto et al., 2010(47)
* *
*
Wirz et al., 2008(45)
Wirz et al., 2009 (46)
low risk of bias unclear risk of bias high risk of bias
* Retrospective study, therefore no attrition
- ? + + - + -
? ? + + - + -
+ ? + + - ? -
+ ? - - - + -
? ? - - - ? -
+ ? - -
- + + + - + - ? + + ?
- + + + ? ? ? - ? ? -
+ + + + - + + + - - + ? + +
+ + + + ? + + - ? - + + ? ?
+ ? - -
Opioid Therapy for Cancer-Related Pain
45
4.5.2 Key Points
Out of 66 possible comparisons of extended-release opioids, we found information on the
comparative risk of harms for only nine comparisons.
For patients with cancer pain, available evidence indicates a similar risk of serious
adverse events among compared drugs:
o Morphine ER versus hydromorphone ER (very low strength of evidence, one
study)
o Morphine ER versus oxycodone ER (very low strength of evidence, one study)
o Morphine ER versus transdermal fentanyl ER (low strength of evidence, two
studies)
o Oxycodone ER versus oxycodone plus naloxone ER (very low strength of
evidence, one study)
The risk of constipation was similar amongst most compared drugs:
o Morphine ER versus hydromorphone ER (very low strength of evidence, one
study)
o Morphine ER versus oxycodone ER (very low strength of evidence, one study)
o Morphine ER versus transdermal fentanyl ER (low strength of evidence, three
studies)
o Hydromorphone ER versus transdermal fentanyl ER (very low strength of
evidence, one study)
o Hydromorphone ER versus transdermal buprenorphine ER (very low strength
of evidence, one study)
o Transdermal fentanyl ER versus transdermal buprenorphine ER (very low
strength of evidence, one study)
Oxycodone plus naloxone ER had a lower risk of constipation than oxycodone ER (low
strength of evidence, one study)
The risk for nausea and vomiting was similar amongst most compared drugs:
o Morphine ER versus transdermal fentanyl ER (very low strength of evidence,
three studies)
o Hydromorphone ER versus oxycodone ER (very low strength of evidence, one
study)

Opioid Therapy for Cancer-Related Pain
46
o Oxycodone ER versus oxycodone plus naloxone ER (very low strength of
evidence, one study)
o Transdermal fentanyl versus transdermal buprenorphine (very low strength of
evidence, one study)
Morphine ER had a higher risk of nausea and vomiting than hydromorphone ER (very
low strength of evidence, two studies)
Morphine ER had a lower risk of nausea than oxycodone ER (very low strength of
evidence, one study)
Hydromorphone ER had a similar risk of nausea but a higher risk of vomiting than
transdermal fentanyl ER (very low strength of evidence, one study) or transdermal
buprenophine ER (very low strength of evidence, one study)
Oxycodone ER had a higher risk of nausea than transdermal fentanyl ER (very low
strength of evidence, one study)
4.5.3 Detailed Synthesis
Table 19 summarizes characteristics of studies included for KQ2. In the following sections we
summarize results first on serious adverse events, second on discontinuation rates and
general tolerability, and third on the comparative risk of specific adverse events. Within each
section, we discuss findings by drug to drug comparisons.

Opioid Therapy for Cancer-Related Pain
47
Table 19: Study Characteristics for all Studies Included for KQ2, the Investigated Outcomes and Risk of Bias Ratings.
Study and Study Design Country and Setting Funding N Comparison Outcomes of Interest Risk of Bias Rating
Ahmedzai et al., 2012(41) double-blind RCT
International (Australia, Czech Republic, France, Germany, Hungary, Israel, Netherlands, Poland, United Kingdom), 64 study sites; setting NR
Mundipharma Research, Germany
184 Oral oxycodone ER vs. oral oxycodone ER plus naloxone
Nausea
Vomiting
Constipation
High
Hagen and Babul, 1997(40) double-blind RCT
Canada; setting NR
NR 2
nd author affiliated
with Purdue Frederick, Canada (the producer of the study drugs)
44 Oral hydromorphone ER vs. oral oxycodone ER
Nausea
Somnolence
High
Hanna et al., 2008(42) double-blind RCT
International (Belgium, Canada, France, Germany, The Netherlands, Spain, Sweden, and the United Kingdom), 37 centres; inpatients, outpatients, and day patients
ALZA Corporation, USA 200 (IR phase) 163 (ER phase)
Oral morphine ER vs. oral hydromorphone ER
Nausea
Vomiting
Constipation
Somnolence
Dizziness
Fatigue
High
Hartung et al., 2007(48) retrospective cohort study
USA, State Oregon fee-for-service recipients; Setting NR
NR 1295 Oral morphine ER vs. oral oxycodone ER vs. transdermal fentanyl ER
ED/hospitalization
Mortality
ED encounters
Hospitalization
Opioid poisoning
Overdose symptoms
Constipation (ED or hospital encounters for constipation)
Unclear
Mercadante et al., 2008(43) non-blinded RCT
Italy, multicenter study; setting NR
NR 108 Oral morphine ER vs. transdermal fentanyl ER
Constipation
Nausea/vomiting
Drowsiness
Confusion
High

Opioid Therapy for Cancer-Related Pain
48
Study and Study Design Country and Setting Funding N Comparison Outcomes of Interest Risk of Bias Rating
Okamoto et al., 2010(47) retrospective cohort study
Japan; hospital information system of the Osaka University Hospital
NR 413 Oral morphine ER vs. oral oxycodone ER vs. transdermal fentanyl ER
Nausea
Somnolence
High
van Seventer et al., 2003(44) non-blinded RCT
The Netherlands, multicentre Study (26 sites); setting NR
The Netherlands, Janssen-Cilag BV
131 Oral morphine ER vs. transdermal fentanyl ER
Nausea
Vomiting
Constipation
Daytime drowsiness
Daytime sleepiness
Respiratory depression
High
Wirz et al., 2008(45) prospective cohort study
Germany; ambulatory pain clinic
NR 102 Oral morphine ER vs. oral hydromorphone ER
Nausea
Vomiting
Constipation
Unclear
Wirz et al., 2009 (46) prospective cohort study
Germany; ambulatory pain clinic
NR 186 Oral hydromorphone ER vs. transdermal fentanyl ER vs. transdermal buprenorphine ER
Nausea
Vomiting
Constipation
Unclear
Abbreviations: ED, emergency department; ER, extended-release; IR, immediate-release; n, study participants; NR, not reported; RCT, randomized controlled trial; vs., versus.
Opioid Therapy for Cancer-Related Pain
49
4.5.3.1 Serious Adverse Events
The FDA defines a serious adverse event (SAE) in human drug trials as an undesirable
occurrence caused by any dose of a study treatment resulting in death, a threat to life,
hospitalization or prolongation of hospitalization, persistent or clinically significant
incapacity, substantial disruption of the ability to conduct normal life functions, or a
congenital anomaly or birth defect.(49) Similarily, the EMA defines a serious adverse event
as any untoward medical occurrence that at any dose: (1) results in death; (2) is life-
threatening; (3) requires inpatient hospitalisation or prolongation of existing hospitalisation;
(4) results in persistent or significant disability/incapacity; or (5) is a congenital
anomaly/birth defect.(50) To identify potential SAEs, we initially tried to use FDA and EMA
definitions. Unfortunately, SAEs in studies were either not clearly defined or definitions were
not in line with those of the FDA or EMA.As a result, we had to rely on guidance from a
clinical practitioner to determine which SAEs to report on. The practitioner recommended
reporting adverse events that led to hospital admission or prolongation of hospitalization
(e.g., due to severe dizziness, nausea, vomiting and constipation).
Less than half of our included studies reported on SAEs related to extended-release opioids
(SAEs such as death were often reported to have been caused by the progression of cancer
and not attributed to opioid treatment for pain). Overall, four studies with data on 1700
patients provided information on SAEs, including: death due to overdose, opioid poisoning,
hospitalization, and respiratory failure.(41, 42, 44, 48) However, data was often not clearly
presented and specific SAEs were rarely reported, which made comparisons of SAEs by
treatment difficult.
4.5.3.1.1 General Risk of Serious Adverse Events
Overall, the risk of SAEs (as reported by study authors) varied from 4.3% for oxycodone
ER(41) to 38% for morphine ER (9% due to progression of the underlying disease).(44) Table
20 summarizes frequencies of SAEs for extended-release opioids. Because definitions of SAEs
varied greatly among studies, frequencies cannot be compared across drugs.

Opioid Therapy for Cancer-Related Pain
50
Table 20: Reported Frequencies of Serious Adverse Events by Drug.
Generic name Frequency of serious adverse events
Transdermal Buprenorphine ER No data
Dihydrocodeine ER No data
Transdermal Fentanyl ER 30% (thereof 9% due to disease progression)
Hydromorphone ER 16%
Morphine ER 16% - 38% (thereof 9% due to disease progression)
Morphine + Naltrexone ER No data
Nalbuphine ER No data
Oxycodone ER 4.3%
Oxycodone + Naloxone ER 8.7%
Oxymorphone ER No data
Tapentadol hydrochloride ER No data
Tramadol ER No data Abbreviations: ER, extended-release.
4.5.3.1.2 Comparative Risk of Serious Adverse Events
Four studies provided data on the comparative risk of SAEs.(41, 42, 44, 48) Table 21
summarizes findings of these studies.
Oral Morphine ER vs. Oral Hydromorphone ER
In one high risk of bias study with two phases (IR phase, n=200 and ER phase, n=163),
patients were randomized to receive morphine ER or hydromorphone ER during 10-15
days.(42) Because the article reported only dosing ranges, we were unable to assess the
dosing equivalence. Overall, 12% (24/200) of patients experienced at least one SAE. The risk
of experiencing an SAE was similar between treatment groups. In the ER phase 10.5% (9/86)
of patients in the morphine ER group reported an SAE compared with 9% (7/77) in the
hydromorphone ER group. Authors reported that many of the SAEs were associated with the
underlying disease and that one-third were considered definitely or probably related to the
study therapy (n not reported). The study disclosed neither the nature of the SAEs nor the
definitions used for SAE classification. Therefore, we are unable to ascertain if the SAEs met
our criteria. Due to the limited evidence available, no inferences can be made about
differences between the two drugs in opioid-induced SAEs.
Because of methodological limitations, imprecision of results, and the fact that only a single
study assessed this outcome, the strength of evidence that morphine ER and
hydromorphone ER have a similar risk for SAEs is very low (see Appendix-Table 6).
Opioid Therapy for Cancer-Related Pain
51
Oral Morphine ER vs. Oral Oxycodone ER
A retrospective cohort study (n=810), with an unclear risk of bias, reported hazard ratios
(HR) for cancer patients who experienced opioid poisoning or who were admitted to the
hospital due to SAEs associated with the intake of morphine ER or oxycodone ER.(48) The HR
for the risk of hospital admission was adjusted for constipation, alteration of consciousness,
malaise, fatigue, lethargy, respiratory failure, and opioid poisoning. The drug dosages were
equivalent between morphine ER and oxycodone ER.
Morphine ER had a similar risk for hospital admissions due to SAEs compared with
oxycodone ER (HR 1.47, 95% CI: 0.58-3.7, p=0.411). Likewise, the risks for opioid poisoning
(HR 2.43, 95% CI: 0.12-50.0) and overdose symptoms (HR 0.95, 95% CI: 0.63-1.45) were not
statistically significantly different between morphine ER and oxycodone ER. Overdose
symptoms were summarized for alteration of consciousness, malaise, fatigue, lethargy and
respiratory failure. Confidence intervals of all estimates, however, are wide and encompass
differences that would be clinically meaningful. For example the risk for hospital admissions
due to SAEs comprises differences from a 42% lower to a 370% higher risk of oxycodone ER
than morphine ER. (HR 1.47, 95% CI 0.58-3.7, p=0.411) Therefore, findings should be viewed
as indeterminate.
Because of methodological limitations, imprecision of results, and the fact that only a single
study assessed this outcome, the strength of evidence that morphine ER and oxycodone ER
have a similar risk for opioid poisoning and hospital admission due to SAEs is very low (see
Appendix-Table 7).
Oral Morphine ER vs. Transdermal Fentanyl ER
A retrospective study (n=778)(48) with an unclear risk of bias and a high risk of bias RCT
(n=131)(44) described the risk of SAEs associated with the intake of morphine ER and
transdermal fentanyl ER. Both studies reported no statistically significant differences for the
risk of SAEs between morphine ER and transdermal fentanyl ER.
The retrospective study, described in the previous chapter, reported a similar risk for
hospital admissions due to SAEs of morphine ER (n=471) compared to transdermal fentanyl
ER (n=307): HR 0.93, 95% CI 0.36-2.33.(48) The hazard ratio for the risk of hospital admission

Opioid Therapy for Cancer-Related Pain
52
was adjusted for constipation, alteration of consciousness, malaise, fatigue, lethargy,
respiratory failure and opioid poisoning. The risk for overdose symptoms was also similar
between morphine ER and transdermal fentanyl ER (HR 0.95, 95% CI: 0.63-1.45). Overdose
symptoms were summarized for alteration of consciousness, malaise, fatigue, lethargy and
respiratory failure. The morphine-equivalent dose of transdermal fentanyl ER was 20%
higher than the morphine ER dose. Confidence intervals of all estimates, however, are wide
and encompass differences that would be clinically meaningful. The study was funded by
Janssen Cilag, the producer of a transdermal fentanyl patch.
The high risk of bias RCT reported 38% (24/64) SAEs in the morphine ER group and 30%
(20/67) SAEs in the transdermal fentanyl ER group.(44) The difference was not statistically
significant (OR 1.41, 95% CI: 0.68-2.92). For approximately 50% of the SAEs, specific reasons
were reported: in both treatment groups 9% of the SAEs were due to disease progression (6
patients in each treatment group) and 5-6% due to dyspnoea (morphine ER: 3/64,
transdermal fentanyl ER: 4/67). Both studies revealed no statistically significant difference
between morphine ER and transdermal fentanyl ER. However, due to the wide confidence
intervals of all estimates, reported findings should be viewed as indeterminate.
Because of methodological limitations and imprecision of results, the strength of evidence
that morphine ER and transdermal fentanyl ER have a similar risk of SAEs is low (see
Appendix-Table 8).
Oral Oxycodone ER vs. Oral Oxycodone ER plus Naloxone
Another RCT, rated as having a high risk of bias, reported numerically lower rates of SAEs for
oxycodone ER (4.3%) than oxycodone ER plus naloxone (8.7%).(41) Dosages were equivalent
between drugs. The difference, however was not statistically significant (OR 0.48; 95% CI:
0.14-1.64) No further information about the nature or the definition which lead to the
classification of SAEs was reported. The study was funded by Mundipharma, the producer of
the oxycodone ER plus naloxone combination drug. Due to the wide confidence interval and
an overall lack of available evidence, the comparative risk of SAEs between oral oxycodone
ER and oral oxycodone ER plus naloxone is indeterminate.
Opioid Therapy for Cancer-Related Pain
53
Because of methodological limitations, imprecision of results, and the fact that only a single
study assessed this outcome, the strength of evidence that oxycodone ER and oxycodone
plus naloxone ER have a similar risk for SAEs is very low (see Appendix-Table 12).

Opioid Therapy for Cancer-Related Pain
54
Table 21: Study Characteristics and Summary of Findings on Serious Adverse Events.
Study N Duration Comparison and Dose Outcome Measure Serious Adverse Events Risk of Bias
Oral Morphine ER vs. Oral Hydromorphone ER
Hanna et al., 2008(42)
200 (IR phase) 163 (ER phase)
10-15 days Morphine ER: 60-540 mg/d hydromorphine ER: 16-96 mg/d
SAE (not specified) Overall: 12% (24/200): IR-phase: 5 patients in each treatment group, ER-phase: morphine ER: 10.5% (9/86), hydromorphone ER: 9% (7/77) Many of the SAE were associated with the underlying disease: 1/3 were considered definitely or probably related to the study therapy
High
Oral Morphine ER vs. Oral Oxycodone ER
Hartung et al., 2007(48)
810 NR Morphine ER: mean±SD 85.1±60.0 mg/d oxycodone ER: morphine equivalent dose: 75.47±58.7 mg/d
ED encounters and hospitalization for constipation, alteration of consciousness, malaise, fatigue, lethargy, respiratory failure, opioid poisoning
Similar risk for ED encounters or hospital encounters (*HR 1.47, 95% CI: 0.58-3.7)
Unclear
Opioid poisoning Similar risk for opioid poisoning (*HR 2.43, 95% CI: 0.12-50.0)
Overdose symptoms (alteration of consciousness, malaise, fatigue, lethargy, respiratory failure)
Similar risk for overdose symptoms (*HR 0.95, 95% CI: 0.63-1.45)
Oral Morphine ER vs. Transdermal Fentanyl ER
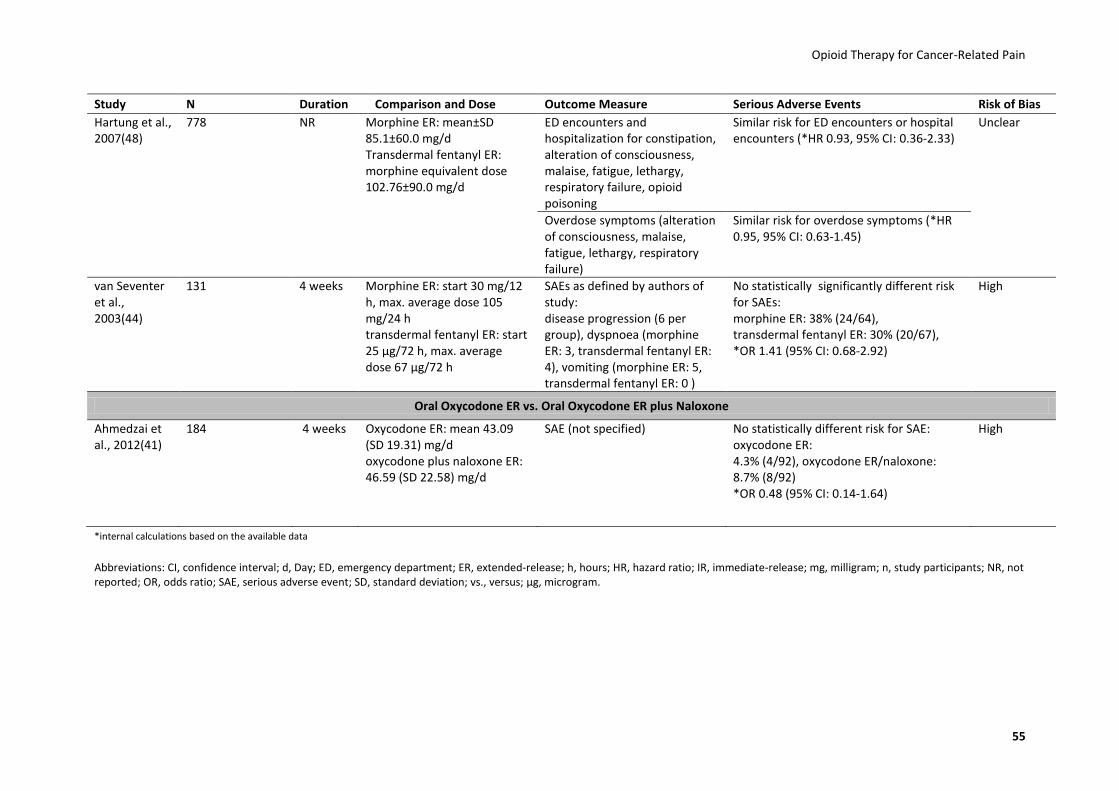
Opioid Therapy for Cancer-Related Pain
55
Study N Duration Comparison and Dose Outcome Measure Serious Adverse Events Risk of Bias
Hartung et al., 2007(48)
778 NR Morphine ER: mean±SD 85.1±60.0 mg/d Transdermal fentanyl ER: morphine equivalent dose 102.76±90.0 mg/d
ED encounters and hospitalization for constipation, alteration of consciousness, malaise, fatigue, lethargy, respiratory failure, opioid poisoning
Similar risk for ED encounters or hospital encounters (*HR 0.93, 95% CI: 0.36-2.33)
Unclear
Overdose symptoms (alteration of consciousness, malaise, fatigue, lethargy, respiratory failure)
Similar risk for overdose symptoms (*HR 0.95, 95% CI: 0.63-1.45)
van Seventer et al., 2003(44)
131 4 weeks Morphine ER: start 30 mg/12 h, max. average dose 105 mg/24 h transdermal fentanyl ER: start 25 µg/72 h, max. average dose 67 µg/72 h
SAEs as defined by authors of study: disease progression (6 per group), dyspnoea (morphine ER: 3, transdermal fentanyl ER: 4), vomiting (morphine ER: 5, transdermal fentanyl ER: 0 )
No statistically significantly different risk for SAEs: morphine ER: 38% (24/64), transdermal fentanyl ER: 30% (20/67), *OR 1.41 (95% CI: 0.68-2.92)
High
Oral Oxycodone ER vs. Oral Oxycodone ER plus Naloxone
Ahmedzai et al., 2012(41)
184 4 weeks Oxycodone ER: mean 43.09 (SD 19.31) mg/d oxycodone plus naloxone ER: 46.59 (SD 22.58) mg/d
SAE (not specified) No statistically different risk for SAE: oxycodone ER: 4.3% (4/92), oxycodone ER/naloxone: 8.7% (8/92) *OR 0.48 (95% CI: 0.14-1.64)
High
*internal calculations based on the available data
Abbreviations: CI, confidence interval; d, Day; ED, emergency department; ER, extended-release; h, hours; HR, hazard ratio; IR, immediate-release; mg, milligram; n, study participants; NR, not reported; OR, odds ratio; SAE, serious adverse event; SD, standard deviation; vs., versus; μg, microgram.

Opioid Therapy for Cancer-Related Pain
56
4.5.3.2 Discontinuation Rates and Overall Tolerability
The most common adverse events reported were constipation, nausea, vomiting, and
somnolence. If sufficient data were available, we calculated the weighted mean and 95%
confidence intervals from efficacy trials and observational studies to investigate the overall
discontinuation rates, discontinuation rates because of adverse events, and the mean
incidence of specific adverse events (Table 22). Discontinuation rates due to lack of efficacy
are presented in Table 15 (see chapter 4.4.3.6). Statistics are descriptive only and
comparisons across different drugs should not be made because of the small number of
included studies and the differences in reporting and assessing of adverse events across
studies.
The mean discontinuation rates because of adverse events for specific drugs vary between
4% (95% CI: 0%-9%) for patients treated with transdermal fentanyl ER and 22% (95% CI: 13%-
30%) for patients treated with oral oxycodone ER plus naloxone. We did not have any data
about discontinuation rates for morphine ER, dihydrocodeine ER, morphine ER plus
naltrexone, nalbuphine ER, oxymorphone ER, transdermal buprenorphine ER and tramadol
ER.
Overall, extended-release opioids led to a similar spectrum of adverse events. Results in
Table 22 are descriptive only and cannot prove a higher risk of a specific adverse event for a
particular drug over another.
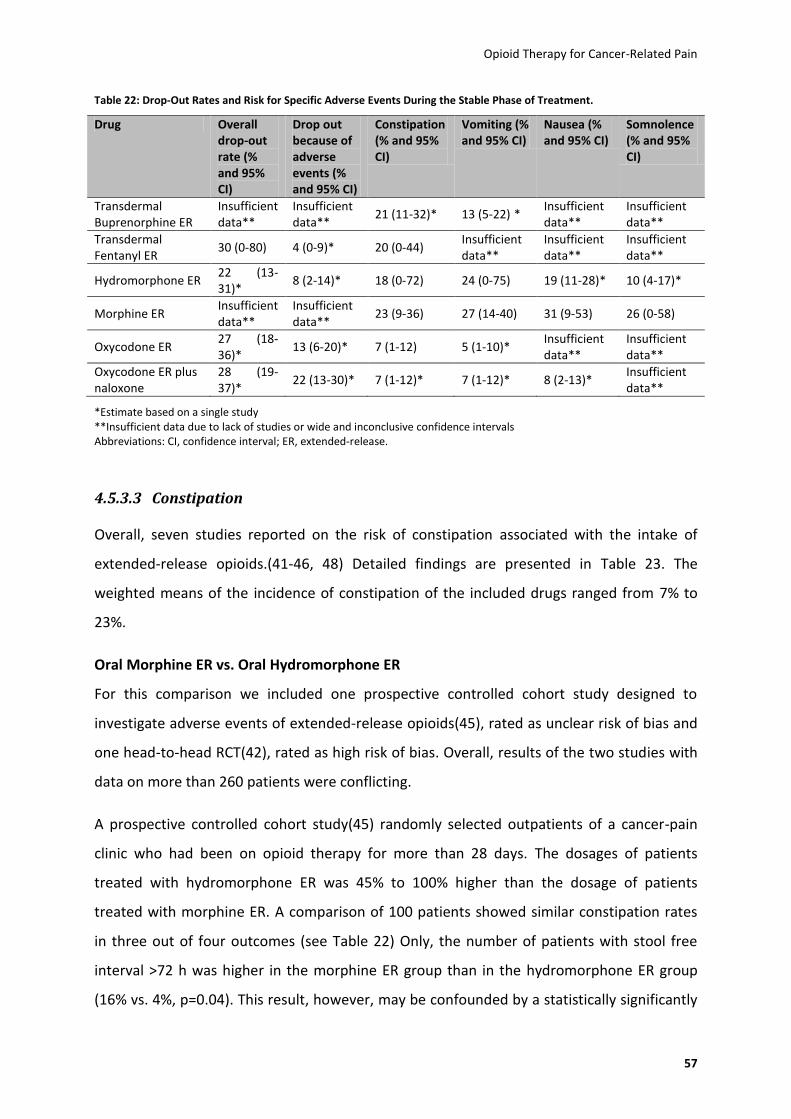
Opioid Therapy for Cancer-Related Pain
57
Table 22: Drop-Out Rates and Risk for Specific Adverse Events During the Stable Phase of Treatment.
Drug Overall drop-out rate (% and 95% CI)
Drop out because of adverse events (% and 95% CI)
Constipation (% and 95% CI)
Vomiting (% and 95% CI)
Nausea (% and 95% CI)
Somnolence (% and 95% CI)
Transdermal Buprenorphine ER
Insufficient data**
Insufficient data**
21 (11-32)* 13 (5-22) * Insufficient data**
Insufficient data**
Transdermal Fentanyl ER
30 (0-80) 4 (0-9)* 20 (0-44) Insufficient data**
Insufficient data**
Insufficient data**
Hydromorphone ER 22 (13-31)*
8 (2-14)*
18 (0-72) 24 (0-75) 19 (11-28)* 10 (4-17)*
Morphine ER Insufficient data**
Insufficient data**
23 (9-36) 27 (14-40) 31 (9-53) 26 (0-58)
Oxycodone ER 27 (18-36)*
13 (6-20)* 7 (1-12)
5 (1-10)* Insufficient data**
Insufficient data**
Oxycodone ER plus naloxone
28 (19-37)*
22 (13-30)* 7 (1-12)* 7 (1-12)* 8 (2-13)* Insufficient data**
*Estimate based on a single study **Insufficient data due to lack of studies or wide and inconclusive confidence intervals Abbreviations: CI, confidence interval; ER, extended-release.
4.5.3.3 Constipation
Overall, seven studies reported on the risk of constipation associated with the intake of
extended-release opioids.(41-46, 48) Detailed findings are presented in Table 23. The
weighted means of the incidence of constipation of the included drugs ranged from 7% to
23%.
Oral Morphine ER vs. Oral Hydromorphone ER
For this comparison we included one prospective controlled cohort study designed to
investigate adverse events of extended-release opioids(45), rated as unclear risk of bias and
one head-to-head RCT(42), rated as high risk of bias. Overall, results of the two studies with
data on more than 260 patients were conflicting.
A prospective controlled cohort study(45) randomly selected outpatients of a cancer-pain
clinic who had been on opioid therapy for more than 28 days. The dosages of patients
treated with hydromorphone ER was 45% to 100% higher than the dosage of patients
treated with morphine ER. A comparison of 100 patients showed similar constipation rates
in three out of four outcomes (see Table 22) Only, the number of patients with stool free
interval >72 h was higher in the morphine ER group than in the hydromorphone ER group
(16% vs. 4%, p=0.04). This result, however, may be confounded by a statistically significantly
Opioid Therapy for Cancer-Related Pain
58
higher proportion of patients treated with morphine ER who used other medications with a
risk for constipation (62% vs. 26%, p=0.0003). By contrast, the double-blind head-to-head
RCT(42) comparing morphine ER with hydromorphone ER in 163 patients during a duration
of 10-15 days revealed a lower incidence of patients reporting constipation in the morphine
ER group than in hydromorphone ER group (22.1% vs. 39.0%;p=NR).(42)
Because of methodological limitations, imprecision, and inconsistency of results, the
strength of evidence that morphine ER and hydromorphone ER have a similar risk for
constipation is very low (Appendix-Table 6).
Oral Morphine ER vs. Oral Oxycodone ER
The only evidence available for this comparison was a retrospective cohort study rated as
unclear risk of bias.(48) This study was based on Medicaid administrative claims data of 810
patients diagnosed with cancer that had at least one prescription of a 28 days or longer
supply of morphine ER or oxycodone ER. These dosages were comparable. Results showed a
similar risk of constipation for patients taking either drug (HR: 0.52, 95%: CI 0.19 to
1.39).(48)
Because of methodological limitations, imprecision of results, and the fact that only a single
study assessed this outcome, the strength of evidence that morphine ER and oxycodone ER
have a similar risk for constipation is very low (Appendix-Table 7).
Oral Morphine ER vs. Transdermal Fentanyl ER
Three studies, one retrospective cohort study (n=778)(48) with unclear risk of bias and two
non-blinded RCTs (n=203)(43, 44) rated as high risk of bias provided information on this
comparison. Overall, these studies reported similar rates of constipation for patients treated
with morphine ER or transdermal fentanyl ER.
The retrospective cohort study used Medicaid administrative claims data of 778 cancer
patients who had at least one prescription of a 28 days or longer supply of morphine ER or
transdermal fentanyl ER. Results indicated that patients treated with morphine ER and
transdermal fentanyl ER had a similar risk of constipation (HR 1.24, 95% CI: 0.51-2.99),
although the morphine-dose-equivalent for transdermal fentanyl was 20% higher in
comparison to the morphine treatment dosage.(48) Results of two non-blinded RCTs support

Opioid Therapy for Cancer-Related Pain
59
these findings although in one RCT(43) the morphine-dose equivalent for transdermal
fentanyl was 30% lower in comparison to the morphine treatment dosage.(43, 44)
Because of methodological limitations, and imprecision of results, the strength of evidence
that morphine ER and transdermal fentanyl ER have a similar risk for constipation is low
(Appendix-Table 8).
Oral Hydromorphone ER vs. Transdermal Fentanyl ER
The only evidence available for this comparison resulted from a prospective cohort study
(n=113) with unclear risk of bias designed to investigate adverse events.(46) This study
revealed that patients treated with hydromorphone ER and transdermal fentanyl ER had a
similar risk of constipation. An exception, however, the stool-free interval for more than 72
hours which was lower in patients on hydromorphone ER than transdermal fentanyl ER (2%
vs. 19%, p=NR). This result may be confounded by a shorter overall duration of opioid use of
hydromorphone ER-treated patients than patients on transdermal fentanyl ER (median use
60 days vs. 90 days).
Because of methodological limitations, imprecision of results, and the fact that only a single
study assessed this outcome, the strength of evidence that hydromorphone ER and
transdermal fentanyl ER have a similar risk for constipation is very low (Appendix-Table 10).
Oral Hydromorphone ER vs. Transdermal Buprenorphine ER
One study (n=119) compared the risk of constipation of hydromorphone ER and transdermal
buprenorphine ER.(46) Patients treated with hydromorphone ER or transdermal
buprenorphine ER had a similar risk of constipation despite a 60% higher morphine-dose
equivalence of hydromorphone ER than transdermal buprenorphine. An exception,
however, was the stool-free interval for more than 72 hours which was substantially lower in
patients on hydromorphone ER than transdermal buprenorphine ER (2% vs. 21%, p=NR).
Confounding, however, is conceivable because patients on hydromorphone ER had a shorter
duration of opioid use than patients on transdermal buprenorphine ER (median use 60 days
vs. 90 days).
Because of methodological limitations, inconsistency of results, and imprecision of results,
and the fact that only a single study assessed this outcome, the strength of evidence that

Opioid Therapy for Cancer-Related Pain
60
hydromorphone ER and transdermal buprenorphine ER have a similar risk for constipation is
very low (Appendix-Table 11).
Oral Oxycodone ER vs. Oral Oxycodone ER plus Naloxone
The only evidence available for this comparison was a high risk of bias RCT comparing the
self-reported symptoms of constipation in 184 patients treated with oral oxycodone ER and
oral oxycodone ER plus naloxone over a treatment period of four weeks.(41) Overall, the
study favoured oral oxycodone ER plus naloxone.
Constipation, as the primary outcome of this study, was measured by the Bowel Function
Index (51), the Patient Assessment of Constipation Symptoms and the European
Organisation of Research and Treatment of Cancer Quality of Life Questionnaire (EORTC
QLQ-C30) constipation subscore. After four weeks, patients receiving oral oxycodone ER
experienced a smaller improvement in bowel function than patients receiving oral
oxycodone plus naloxone ER (difference between the groups in the change in the Bowel
Function Index score from baseline to endpoint: -11.14, 95% CI: -19.03 to -3.24).(41)
Furthermore, patients receiving oral oxycodone ER showed a smaller improvement in the
Patient Assessment of Constipation Symptoms in terms of total symptom score (score mean
changes from baseline to four weeks: oxycodone ER -2.74 vs. oxycodone ER plus naloxone -
7.01; p=0.014) and frequency of symptoms (mean 2.03 vs. 1.47; p<0.01) and a clinically
important smaller improvement in EORTC QLQ-C30 constipation subscore (mean change -
13.1 vs. - 30.4, p=NR).(41)
Because of methodological limitations, some inconsistent findings, imprecision of results and
the fact that only a single study assessed this outcome, the strength of evidence that
oxycodone ER has a higher risk of constipation than oxycodone ER plus naloxone is low
(Appendix-Table 12).
Transdermal Fentanyl ER vs. Transdermal Buprenorphine ER
We found one prospective controlled cohort study(46) with unclear risk of bias comparing
the effects of transdermal fentanyl ER with transdermal buprenorphine ER in 116 patients.
Overall, the study reported no statistically significant differences in constipation among
patients although morphine-dose-equivalent for transdermal fentanyl was 100% higher than
for transdermal buprenorphine.(46)
Opioid Therapy for Cancer-Related Pain
61
Because of methodological limitations, imprecision of results, and the fact that only a single
study assessed this outcome, the strength of evidence that transdermal fentanyl ER and
transdermal buprenorphine ER have a similar risk for constipation is very low (Appendix-
Table 14).

Opioid Therapy for Cancer-Related Pain
62
Table 23: Study Characteristics and Summary of Findings of Constipation.
Study N Duration Comparison and Dose Outcome Measure Constipation Risk of Bias
Oral Morphine ER vs. Oral Hydromorphone ER
Hanna et al., 2008(42)
200 (IR phase) 163 (ER phase)
10-15 days Morphine ER: 60-540 mg/d Hydromorphone ER: 16-96 mg/d
Constipation reported by patients
Lower incidence of constipation for morphine ER: 22.1% vs. 39.0%; p=NR
High
Wirz et al., 2008(45)
100 Minimum 4 weeks treatment, 5 days observation of AE
Morphine ER: median (range) 60 (20-450) mg/d Hydromorphone ER (morphine equivalence 1:5): 80 (20-480) mg/d
Numerical rating scale for constipation (NRS, 0-10, 0=no symptom, 10=worst symptom imaginable)
Mean intensity of constipation was similar: 2.7% vs. 2.2%; p=0.35
Unclear
Four point EORTC QLQ 30 questionnaire, item on constipation (1=not at all, 2=a little, 3=quite a bit, 4=very much)
Mean scores for constipation were similar: 2.2% vs. 1.9%; p=0.18
Mean number of defecations of all patients per day
The mean defecation rate was similar: 1% vs. 0.9%; p=0.44
Stool free interval >72h More patients in the morphine ER group compared to the hydromorphone ER group had a stool free interval >72h: 16% vs., 4%; p=0.04
Oral Morphine ER vs. Oral Oxycodone ER
Hartung et al., 2007(48)
810 NR Morphine ER: mean±SD 85.1±60.0 mg/d Oxycodone ER: morphine equivalent dose: 75.47±58.7 mg/d
ED and hospitalization with an ICD-9 diagnosis code for constipation (564.0)
Similar risk for ED or hospital encounter for constipation: HR 0.52, 95% CI: 0.19-1.39
Unclear
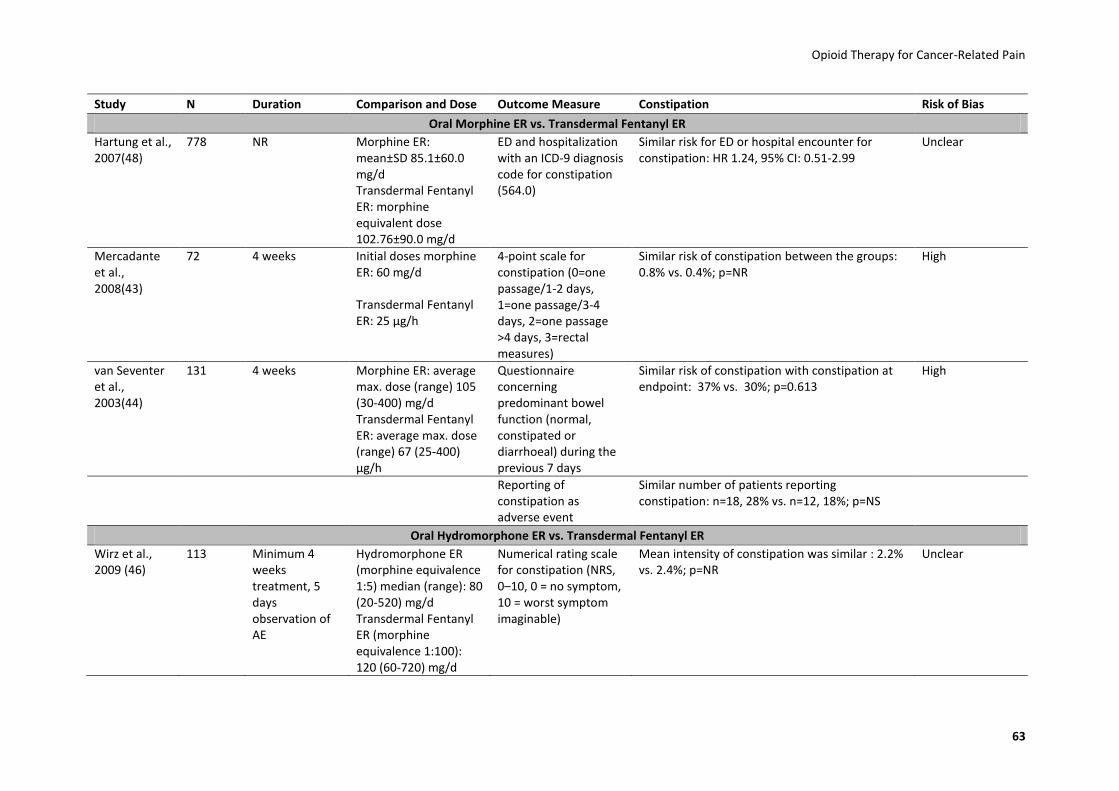
Opioid Therapy for Cancer-Related Pain
63
Study N Duration Comparison and Dose Outcome Measure Constipation Risk of Bias
Oral Morphine ER vs. Transdermal Fentanyl ER
Hartung et al., 2007(48)
778 NR Morphine ER: mean±SD 85.1±60.0 mg/d Transdermal Fentanyl ER: morphine equivalent dose 102.76±90.0 mg/d
ED and hospitalization with an ICD-9 diagnosis code for constipation (564.0)
Similar risk for ED or hospital encounter for constipation: HR 1.24, 95% CI: 0.51-2.99
Unclear
Mercadante et al., 2008(43)
72 4 weeks Initial doses morphine ER: 60 mg/d
Transdermal Fentanyl ER: 25 µg/h
4-point scale for constipation (0=one passage/1-2 days, 1=one passage/3-4 days, 2=one passage >4 days, 3=rectal measures)
Similar risk of constipation between the groups: 0.8% vs. 0.4%; p=NR
High
van Seventer et al., 2003(44)
131 4 weeks Morphine ER: average max. dose (range) 105 (30-400) mg/d Transdermal Fentanyl ER: average max. dose (range) 67 (25-400) µg/h
Questionnaire concerning predominant bowel function (normal, constipated or diarrhoeal) during the previous 7 days
Similar risk of constipation with constipation at endpoint: 37% vs. 30%; p=0.613
High
Reporting of constipation as adverse event
Similar number of patients reporting constipation: n=18, 28% vs. n=12, 18%; p=NS
Oral Hydromorphone ER vs. Transdermal Fentanyl ER
Wirz et al., 2009 (46)
113 Minimum 4 weeks treatment, 5 days observation of AE
Hydromorphone ER (morphine equivalence 1:5) median (range): 80 (20-520) mg/d Transdermal Fentanyl ER (morphine equivalence 1:100): 120 (60-720) mg/d
Numerical rating scale for constipation (NRS, 0–10, 0 = no symptom, 10 = worst symptom imaginable)
Mean intensity of constipation was similar : 2.2% vs. 2.4%; p=NR
Unclear
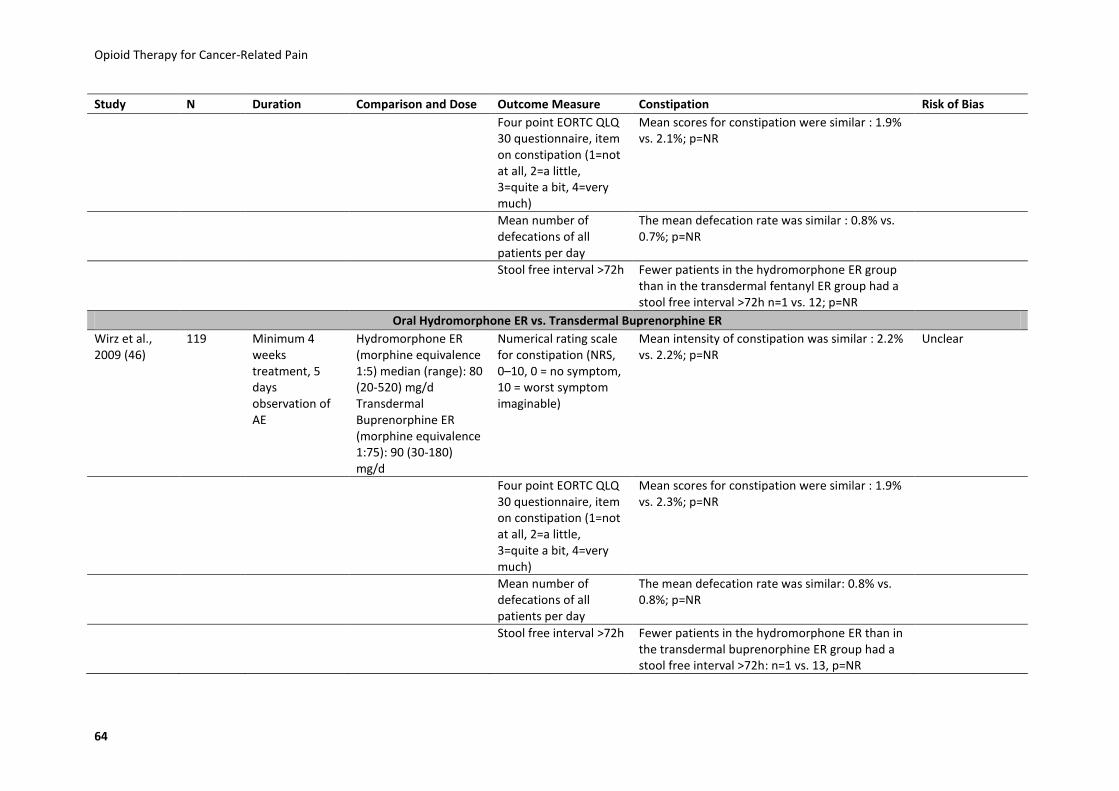
Opioid Therapy for Cancer-Related Pain
64
Study N Duration Comparison and Dose Outcome Measure Constipation Risk of Bias
Four point EORTC QLQ 30 questionnaire, item on constipation (1=not at all, 2=a little, 3=quite a bit, 4=very much)
Mean scores for constipation were similar : 1.9% vs. 2.1%; p=NR
Mean number of defecations of all patients per day
The mean defecation rate was similar : 0.8% vs. 0.7%; p=NR
Stool free interval >72h Fewer patients in the hydromorphone ER group than in the transdermal fentanyl ER group had a stool free interval >72h n=1 vs. 12; p=NR
Oral Hydromorphone ER vs. Transdermal Buprenorphine ER
Wirz et al., 2009 (46)
119 Minimum 4 weeks treatment, 5 days observation of AE
Hydromorphone ER (morphine equivalence 1:5) median (range): 80 (20-520) mg/d Transdermal Buprenorphine ER (morphine equivalence 1:75): 90 (30-180) mg/d
Numerical rating scale for constipation (NRS, 0–10, 0 = no symptom, 10 = worst symptom imaginable)
Mean intensity of constipation was similar : 2.2% vs. 2.2%; p=NR
Unclear
Four point EORTC QLQ 30 questionnaire, item on constipation (1=not at all, 2=a little, 3=quite a bit, 4=very much)
Mean scores for constipation were similar : 1.9% vs. 2.3%; p=NR
Mean number of defecations of all patients per day
The mean defecation rate was similar: 0.8% vs. 0.8%; p=NR
Stool free interval >72h Fewer patients in the hydromorphone ER than in the transdermal buprenorphine ER group had a stool free interval >72h: n=1 vs. 13, p=NR
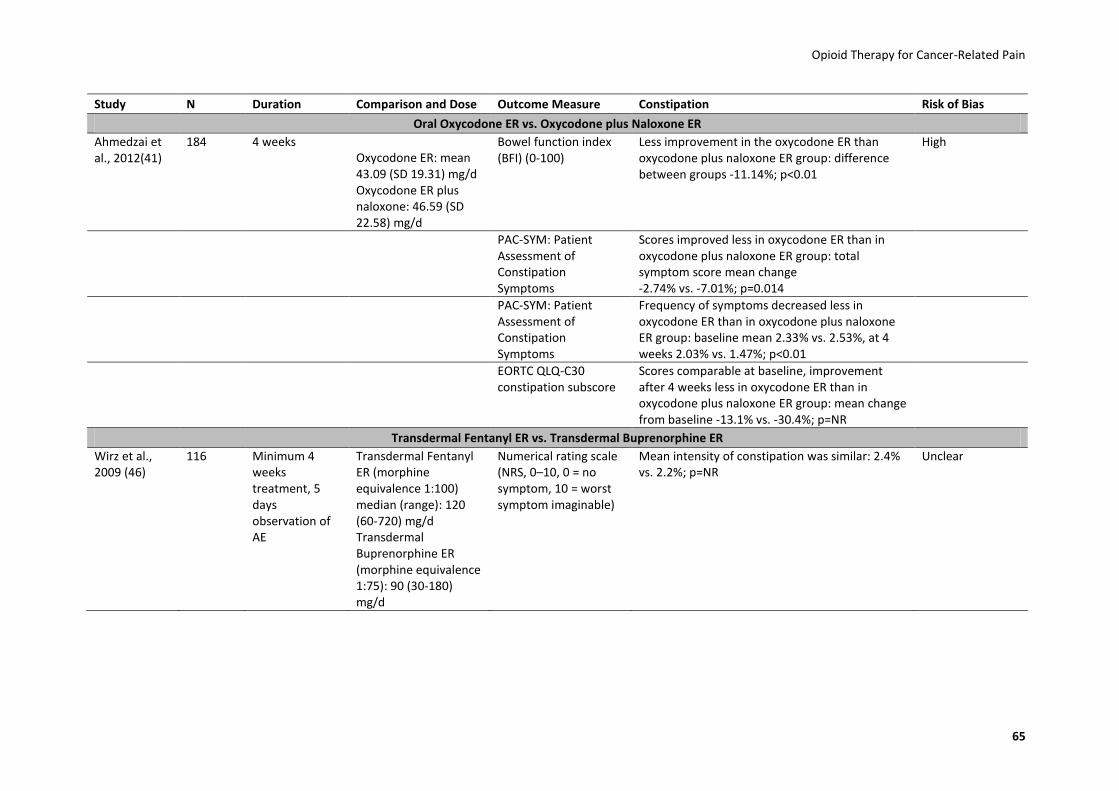
Opioid Therapy for Cancer-Related Pain
65
Study N Duration Comparison and Dose Outcome Measure Constipation Risk of Bias
Oral Oxycodone ER vs. Oxycodone plus Naloxone ER
Ahmedzai et al., 2012(41)
184 4 weeks Oxycodone ER: mean 43.09 (SD 19.31) mg/d Oxycodone ER plus naloxone: 46.59 (SD 22.58) mg/d
Bowel function index (BFI) (0-100)
Less improvement in the oxycodone ER than oxycodone plus naloxone ER group: difference between groups -11.14%; p<0.01
High
PAC-SYM: Patient Assessment of Constipation Symptoms
Scores improved less in oxycodone ER than in oxycodone plus naloxone ER group: total symptom score mean change -2.74% vs. -7.01%; p=0.014
PAC-SYM: Patient Assessment of Constipation Symptoms
Frequency of symptoms decreased less in oxycodone ER than in oxycodone plus naloxone ER group: baseline mean 2.33% vs. 2.53%, at 4 weeks 2.03% vs. 1.47%; p<0.01
EORTC QLQ-C30 constipation subscore
Scores comparable at baseline, improvement after 4 weeks less in oxycodone ER than in oxycodone plus naloxone ER group: mean change from baseline -13.1% vs. -30.4%; p=NR
Transdermal Fentanyl ER vs. Transdermal Buprenorphine ER
Wirz et al., 2009 (46)
116 Minimum 4 weeks treatment, 5 days observation of AE
Transdermal Fentanyl ER (morphine equivalence 1:100) median (range): 120 (60-720) mg/d Transdermal Buprenorphine ER (morphine equivalence 1:75): 90 (30-180) mg/d
Numerical rating scale (NRS, 0–10, 0 = no symptom, 10 = worst symptom imaginable)
Mean intensity of constipation was similar: 2.4% vs. 2.2%; p=NR
Unclear

Opioid Therapy for Cancer-Related Pain
66
Study N Duration Comparison and Dose Outcome Measure Constipation Risk of Bias
Four point EORTC QLQ 30 questionnaire, item on constipation (1=not at all, 2=a little, 3=quite a bit, 4=very much)
Mean scores for constipation were similar : 2.1% vs. 2.3%; p=NR
Mean number of defecations of all patients per day
The mean defecation rate was similar : 0.7% vs. 0.8%; p=NR
Stool free interval >72h Similar number of patients had a stool free interval >72h in both study groups: transdermal fentanyl ER: 12%, transdermal buprenorphine ER: 13%; p=NR
Abbreviations: AE, adverse events; BFI, bowel function index; CI, confidence interval; d, day; ED, emergency department; EORTC QLQ 30, European Organization for Research and Treatment of Cancer Quality of Life Questionnaire 30; ER, extended-release; h, hour; HR, hazard ratio; ICD, International Classification of Diseases; mg, milligram; n, number of participants; NR, not reported; NRS, numerical rating scale; NS, not significant; p, probability; PAC-SYM, Patient Assessment of Constipation Symptoms; SD, standard deviation; vs., versus; μg, microgram.

Opioid Therapy for Cancer-Related Pain
67
4.5.3.4 Nausea and Vomiting
Eight studies with more than 1500 patients provided data on the comparative risk of nausea
and vomiting of extended-release opioids.(40-47) Findings of these studies are presented in
Table 24.
Oral Morphine ER vs. Oral Hydromorphone ER
Two studies, a prospective cohort study (n=100)(45), rated as unclear risk of bias and a high
risk of bias RCT (n=200, ER-phase: 163)(42) reported data on the comparative risk of nausea
and vomiting for morphine ER and hydromorphone ER. In the prospective study the number
of patients with at least one episode of vomiting during an observation period of five days
did not differ significantly between the study groups (morphine ER: 30%, hydromorphone
ER: 36%, p=0.52).(45) The mean number of vomits per day was higher in the morphine ER
group than in the hydromorphone ER group (0.7 vs. 0.1; p=0.0001).(45) For nausea-intensity
two different scales were used: The numerical rating scale (0-10) showed statistically
significant differences (2.5 points for morphine ER vs. 1.5 points for hydromorphone ER;
p=0.01). The EORTC-questionnaire evaluated nausea on a scale from 1-4 and showed no
statistically different results between the two treatment groups (1.6 for morphine ER and 1.8
for hydromorphone ER, p=0.23). The mean morphine equivalent dose of hydromorphone ER
was 45% to 100% higher than in the morphine ER-group.
The second study, a high risk of bias RCT reported adverse events, based on patient reports.
In the ER-phase, nausea was reported by 29.1% (25/86) of patients taking morphine ER
versus 19.5% (15/77) of patients taking hydromorphone ER. We calculated the OR of the
difference which was not statistically significant (OR 1.69, 95% CI: 0.82-3.52).(42) Vomiting
rates, however, were statistically significant higher for patients taking morphine ER with
22.1% (19/86) versus 9.1% (7/77) for hydromorphone ER (OR 2.84, 95% CI: 1.17-7.18).
Nausea-intensity scores and the number of patients with at least one episode of vomiting in
the prospective study showed similar results for morphine ER and hydromorphone ER. The
authors of the study used two different ratios to define the morphine-equivalence of
hydromorphone ER (1:5 and 1:7.5). Depending on the ratio the mean morphine equivalent
dose of hydromorphone ER was from 45% to 100% higher than morphine ER. No data for

Opioid Therapy for Cancer-Related Pain
68
morphine-equivalency could be calculated for the high risk of bias RCT. The RCT showed no
statistically significant difference of nausea between morphine and hydromorphone but a
higher risk of vomiting for patients takingmorphine.
Because of methodological limitations, imprecision of results, and inconsistent findings of
the included studies, the strength of evidence that oral morphine ER has a higher risk of
nausea and vomiting than hydromorphone is very low (see Appendix-Table 6).
Oral Morphine ER vs. Oral Oxycodone ER
We found only one high risk of bias retrospective cohort study, based on a registry of the
Osaka University, which compared morphine ER with oxycodone ER.(47) This study enrolled
413 cancer patients, with data available on 262 patients for the morpine ER versus
oxycodone ER comparison. Results indicated numerically lower rates of nausea for patients
treated within morphine ER than oxycodone ER (22.6% vs. 35.4%). The difference, however,
did not reach statistical significance (OR 0.53, 95% CI: 0.27-1.05). We were unable to assess
the dosing equivalence for this study.
Because of substantial methodological shortcomings, results from this study cannot be used
to draw any conclusion about differences in the risk of nausea and vomiting between
morphine ER and oxycodone ER. The strength of evidence that morphine ER has a lower risk
of nausea than oxycodone ER is very low (see Appendix-Table 7).
Oral Morphine ER vs. Transdermal Fentanyl ER
Three high risk of bias studies, two non-blinded RCTs(43, 44) and one retrospective cohort
study(47), based on 397 patients reported inconsistent results concerning the comparative
risk of nausea and vomiting between morphine ER and transdermal fentanyl ER. For example
in one of the RCT´s 41% of patients in the morphine ER group reported nausea, compared
with 37% in the transdermal fentanyl ER group (OR 1.15, 95% CI, 0.57-2.32). Likewise, rates
of vomiting were similar (31% vs. 28%; OR 1.15, 95% CI, 0.54-2.43).(44) The second RCT also
reported similar ratings for nausea and vomiting although the mean morphine-equivalent
dose of transdermal fentanyl ER was 30% lower than morphine ER.(28)By contrast, the
retrospective cohort study with data on 194 patients, however, reported a statistically

Opioid Therapy for Cancer-Related Pain
69
significantly higher risk of nausea for patients treated with morphine ER than transdermal
fentanyl ER (22.6% vs. 6.8%, OR 3.99, 95% CI 1.62-9.82).(47)
Because of methodological limitations, imprecision of results, and inconsistent findings of
included studies, the strength of evidence that oral morphine ER and transdermal fentanyl
ER have a similar risk for nausea and vomiting is very low (see Appendix-Table 8).
Oral Hydromorphone ER vs. Oral Oxycodone ER
One double-blind RCT (n=44), rated as high risk of bias, showed similar mean nausea
intensity scores between hydromorphone ER and oxycodone ER (VAS: 16.05 vs. 16.68)
during a study period of seven days,(40) despite the fact that the the mean morphine-
eqivalent dose of oxycodone ER was 50% higher than that of hdromorphone ER.
Because of methodological limitations, imprecision of results, and the fact that only a single
study assessed this outcome, the strength of evidence that hydromorphone ER and
oxycodone ER have a similar risk for nausea and is very low (see Appendix-Table 9).
Oral Hydromorphone ER vs. Transdermal Fentanyl ER
Only one prospective cohort study of unclear risk of bias provided information on the
comparative risk of nausea and vomiting between hydromorphone ER and transdermal
fentanyl ER (n= 113).(46) Nausea was assessed using a numerical rating scale (NRS) from no
nausea (0), to worst imaginable nausea(10), and the four point EORTC QLQ 30 questionnaire.
Overall, results indicated similar nausea intensity-scores and vomiting scores (EORTC) in
patients treated with hydromorphone ER or transdermal fentanyl ER. The NRS – scale (0-10)
for nausea showed 1.5 points for hydromorphone ER and 1.3 points for transdermal fentanyl
ER. Patients on hydromorphone ER, however, reported statistically significantly higher rates
of vomiting than patients on transdermal fentanyl ER (33% vs. 16%; OR 2.49, 95% CI: 1.01-
6.13) during a 5-day follow-up period. The authors of the study used two different ratios to
define the morphine-equivalent dose of hydromorphone (1:5 and 1:7.5). Consequently, the
morphine-equivalent dose of hydromorphone ER varied from 20 % lower (for the 1:5 ratio)
to 20% higher (for the 1:7.5 ratio) compared with the morphine-equivalent dose of
transdermal fentanyl ER.

Opioid Therapy for Cancer-Related Pain
70
Because of methodological limitations, imprecision of results, and the fact that only a single
study assessed this outcome, the strength of evidence that hydromorphone ER transdermal
fentanyl ER have a similar risk for nausea is very low. In addition the strength of evidence,
that hydromorphone ER has a higher risk for vomiting than transdermal fentanyl ER is also
very low (see Appendix-Table 10).
Oral Hydromorphone ER vs. Transdermal Buprenorphine ER
The same prospective cohort study described in the previous section(46) showed similar
nausea and vomiting scores (NRS) for patients receiving hydromorphone ER (n=58) and
transdermal buprenorphine ER (n=61As mentioned above, authors defined two different
ratios of morphine-equivalence for hydromorphone ER (1:5 and 1:7.5). Consequently, the
mean morphine-equivalent dose of hydromorphone ER was from 60 % (for the 1:5 ratio) to
140% (for the 1:7.5 ratio) higher than the morphine equivalent dose of transdermal
buprenorphine ER.
Because of methodological limitations, imprecision of results, and the fact that only a single
study assessed this outcome, the strength of evidence that hydromorphone ER and have a
similar risk for nausea and higher risk for vomiting than transdermal buprenorphine ER is
very low.(see Appendix-Table 11)
Oral Oxycodone ER vs. Oral Oxycodone plus Naloxone ER
A high risk of bias double-blind RCT (n=184) with a duration of four weeks showed that
nausea was more frequent in patients receiving oxycodone ER (13%) compared to those on
oxycodone plus naloxone ER (7.6%), but the difference was not statistically significant (OR
1.82, 95% CI: 0.68-4.86).(41) Vomiting rates were similar among the study groups and
showed no statistically significant difference (oxycodone ER 5.4% and oxycodone plus
naloxone ER 6.5%; OR 0.82, 95% CI: 0.24-2.80).
Because of methodological limitations, imprecision of results, and the fact that only a single
study assessed this outcome, the strength of evidence that oxycodone ER and oxycodone
plus naloxone ER have a similar risk for nausea and vomiting is very low (see Appendix-Table
12).

Opioid Therapy for Cancer-Related Pain
71
Oral Oxycodone ER vs. Transdermal Fentanyl ER
One high risk of bias retrospective study with data of 296 patients showed that nausea
occurred more frequently in the oxycodone ER group (35.4%) than in the transdermal
fentanyl ER group (6.8%), OR 7.48, 95% CI: 3.54-15.81, based on internal calculations).(47)
Because of methodological limitations, imprecision of results, and the fact that only a single
study assessed this outcome, the strength of evidence that oxycodone ER has a higher risk of
nausea than transdermal fentanyl ER is very low (see Appendix-Table 13).
Transdermal Fentanyl ER vs. Transdermal Buprenorphine ER
The prospective cohort study with an unclear risk of bias, by Wirz et al. investigated 116
patients who received transdermal fentanyl ER or transdermal buprenorphine ER for at least
28 days prior to the five day data collection period.(46) Results showed similar low mean
nausea intensity-scores on a 0-10-scale with 1.3 points for transdermal fentanyl ER and 1.2
points for transdermal buprenorphine ER. The study reported also similar absolute numbers
of vomiting patients (transdermal fentanyl ER: 16% vs. transdermal buprenorphine ER: 13%,
OR 1.3, 95% CI: 0.46-3.63), although the mean morphine-eqivalent dose of transdermal
fentanyl ER was 100 % higher than that of transdermal buprenorphine ER-group.(46)
Because of methodological limitations, imprecision of results, and the fact that only a single
study assessed this outcome, the strength of evidence that transdermal fentanyl ER and
transdermal buprenorphine ER have a similar risk for nausea and vomiting is very low. (see
Appendix-Table 14)

Opioid Therapy for Cancer-Related Pain
72
Table 24: Study Characteristics and Summary of Findings o Nausea and Vomiting.
Study N Duration Comparison and Dose Outcome Measure Nausea and Vomiting Risk of Bias
Oral Morphine ER vs. Oral Hydromorphone ER
Hanna et al., 2008(42)
200 ER-phase: 163
10-15 days Morphine ER: 60-540 mg/d Hydromorphone ER: 16-96 mg/d
Nausea reported by patients
Higher incidence of nausea with ER morphine ER vs. hydromorphone ER (n=25, 29.1% vs. n=15, 19.5%; p=NR, *OR 1.69, 95% CI: 0.82-3.52)
High
Vomiting reported by patients
Higher incidence of vomiting with morphine ER vs. hydromorphone ER (n=19, 22.1% vs. n=7, 9.1%; p=NR, *OR 2.84, 95% CI: 1.17-7.18)
Wirz et al., 2008(45)
100 Minimum 4 weeks treatment, 5 days observation of AE
Morphine ER: median (range) 60 (20-450) mg/d Hydromorphone ER (morphine equivalence 1:5): 80 (20-480) mg/d
Numerical rating scale (NRS, 0-10, 0=no symptom, 10=worst symptom imaginable)
Mean intensity of nausea scores were higher in the morphine ER group compared to the hydromorphone ER group (2.5 vs. 1.5; p=0.01)
Unclear
Four point EORTC QLQ 30 questionnaire, item on nausea (1=not at all, 2=a little, 3=quite a bit, 4=very much)
Mean nausea scores were similar for both study groups (morphine ER: 1.6, hydromorphone ER: 1.8; p=0.23)
Four point EORTC QLQ 30 questionnaire, item on vomiting (1=not at all, 2=a little, 3=quite a bit, 4=very much)
Mean vomiting scores were similar for both study groups (morphine ER: 1.5, hydromorphone ER: 1.4; p=0.53)
Number of patients with at least 1 vomit during observation period
Similar number of patients with vomiting (morphine ER: n=15, 30%, hydromorphone ER: n=18, 36%; p=0.52)
Numbers of vomits/day Mean number of vomits per day was higher in the morphine ER group than in the hydromorphone ER group (0.7 vs. 0.1; p=0.0001)
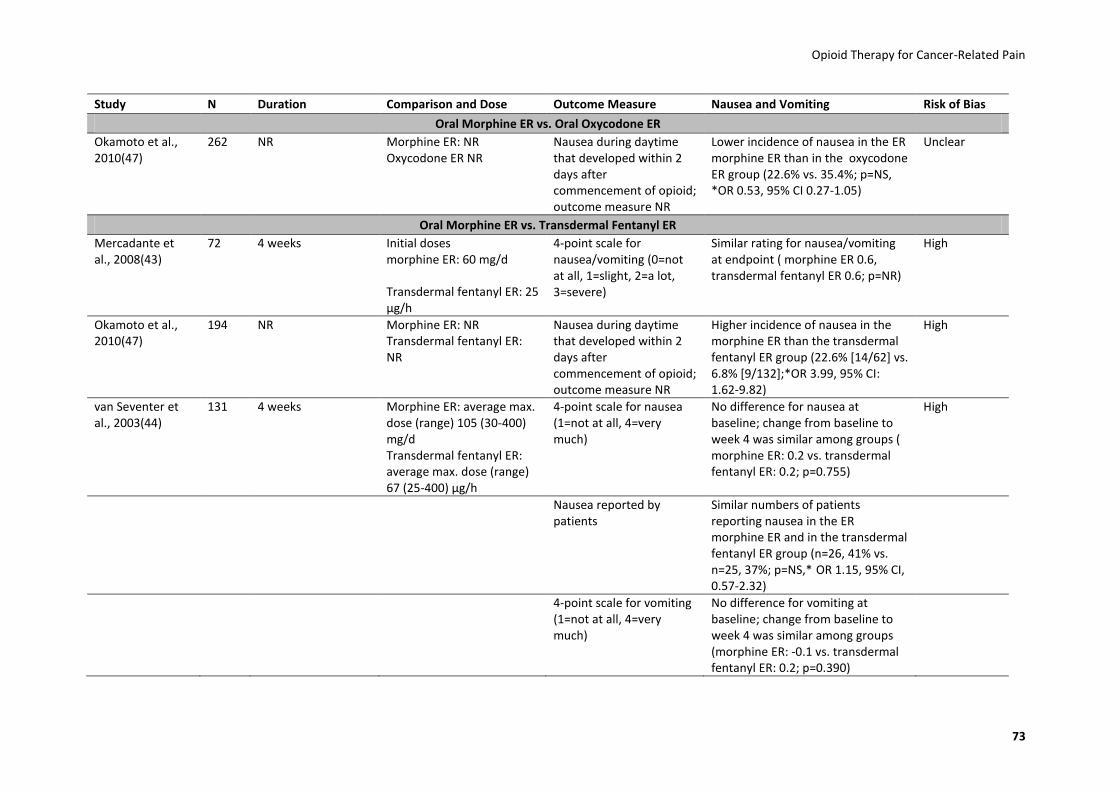
Opioid Therapy for Cancer-Related Pain
73
Study N Duration Comparison and Dose Outcome Measure Nausea and Vomiting Risk of Bias
Oral Morphine ER vs. Oral Oxycodone ER
Okamoto et al., 2010(47)
262 NR Morphine ER: NR Oxycodone ER NR
Nausea during daytime that developed within 2 days after commencement of opioid; outcome measure NR
Lower incidence of nausea in the ER morphine ER than in the oxycodone ER group (22.6% vs. 35.4%; p=NS, *OR 0.53, 95% CI 0.27-1.05)
Unclear
Oral Morphine ER vs. Transdermal Fentanyl ER
Mercadante et al., 2008(43)
72 4 weeks Initial doses morphine ER: 60 mg/d
Transdermal fentanyl ER: 25 µg/h
4-point scale for nausea/vomiting (0=not at all, 1=slight, 2=a lot, 3=severe)
Similar rating for nausea/vomiting at endpoint ( morphine ER 0.6, transdermal fentanyl ER 0.6; p=NR)
High
Okamoto et al., 2010(47)
194 NR Morphine ER: NR Transdermal fentanyl ER: NR
Nausea during daytime that developed within 2 days after commencement of opioid; outcome measure NR
Higher incidence of nausea in the morphine ER than the transdermal fentanyl ER group (22.6% [14/62] vs. 6.8% [9/132];*OR 3.99, 95% CI: 1.62-9.82)
High
van Seventer et al., 2003(44)
131 4 weeks Morphine ER: average max. dose (range) 105 (30-400) mg/d Transdermal fentanyl ER: average max. dose (range) 67 (25-400) µg/h
4-point scale for nausea (1=not at all, 4=very much)
No difference for nausea at baseline; change from baseline to week 4 was similar among groups ( morphine ER: 0.2 vs. transdermal fentanyl ER: 0.2; p=0.755)
High
Nausea reported by patients
Similar numbers of patients reporting nausea in the ER morphine ER and in the transdermal fentanyl ER group (n=26, 41% vs. n=25, 37%; p=NS,* OR 1.15, 95% CI, 0.57-2.32)
4-point scale for vomiting (1=not at all, 4=very much)
No difference for vomiting at baseline; change from baseline to week 4 was similar among groups (morphine ER: -0.1 vs. transdermal fentanyl ER: 0.2; p=0.390)

Opioid Therapy for Cancer-Related Pain
74
Study N Duration Comparison and Dose Outcome Measure Nausea and Vomiting Risk of Bias
Vomiting reported by patients
Similar numbers of patients reporting vomiting in the morphine ER and in the transdermal fentanyl ER group (n=20, 31% vs. n=19, 28%; p=NS, *OR 1.15, 95% CI: 0.54-2.43)
Oral Hydromorphone ER vs. Oral Oxycodone ER
Hagen and Babul, 1997(40)
44 7 days Hydromorphone ER: mean final dose 30 ± 6 mg/d oxycodone ER: 124 ± 22 mg/d
VAS 0-100mm for nausea (0=no nausea, 100=severe nausea)
Overall mean nausea scores similar for both groups (hydromorphone ER: 16.05 vs. oxycodone ER: 16.68; p=NR)
High
Oral Hydromorphone ER vs. Transdermal Fentanyl ER
Wirz et al., 2009 (46)
113 Minimum 4 weeks treatment, 5 days observation of AE
Hydromorphone ER (morphine equivalence 1:5) median (range): 80 (20-520) mg/d Transdermal fentanyl ER (morphine equivalence 1:100): 120 (60-720) mg/d
Numerical rating scale for nausea (NRS, 0-10, 0=no symptom, 10=worst symptom imaginable)
Mean intensity of nausea scores were similar for both study groups (hydromorphone ER: 1.5, transdermal fentanyl ER: 1.3; p=NR)
Unclear
Four point EORTC QLQ 30 questionnaire, item on nausea (1=not at all, 2=a little, 3=quite a bit, 4=very much)
Mean nausea scores were similar for both study groups ( hydromorphone ER: 1.8, transdermal fentanyl ER: 1.8; p=NR)
Four point EORTC QLQ 30 questionnaire, item on vomiting (1=not at all, 2=a little, 3=quite a bit, 4=very much)
Mean vomiting scores were similar for both study groups ( hydromorphone ER: 1.4, transdermal fentanyl ER: 1.6; p=NR)
Number of patients with at least 1 vomit during observation period
Higher number of patients with vomiting (hydromorphone ER: n=19, 33%, transdermal fentanyl ER: n=9, 16%; p=NR, * OR 2.49, 95% CI: 1.01-6.13)

Opioid Therapy for Cancer-Related Pain
75
Study N Duration Comparison and Dose Outcome Measure Nausea and Vomiting Risk of Bias
Numbers of vomits/day Mean number of vomits per day were similar for both study groups (hydromorphone ER: 0.1, transdermal fentanyl ER: 0.1; p=NR)
Oral Hdromorphone ER vs. Transdermal Buprenorphine ER
Wirz et al., 2009 (46)
119 Minimum 4 weeks treatment, 5 days observation of AE
Hydromorphone ER (morphine equivalence 1:5) median (range): 80 (20-520) mg/d Transdermal buprenorphine ER (morphine equivalence 1:75): 90 (30-180) mg/d
Numerical rating scale for nausea (NRS, 0-10, 0=no symptom, 10=worst symptom imaginable)
Mean intensity of nausea scores were similar for both study groups (hydromorphone ER: 1.5, transdermal buprenorphine ER: 1.2; p=NR)
Unclear
Four point EORTC QLQ 30 questionnaire, item on nausea (1=not at all, 2=a little, 3=quite a bit, 4=very much)
Mean nausea scores were similar for both study groups (hydromorphone ER: 1.8, transdermal buprenorphine ER: 1.7; p=NR)
Four point EORTC QLQ 30 questionnaire, item on vomiting (1=not at all, 2=a little, 3=quite a bit, 4=very much)
Mean vomiting scores were similar for both study groups (hydromorphone ER: 1.4, transdermal buprenorphine ER: 1.4; p=NR)
Number of patients with at least 1 vomit during observation period
Higher number of patients with vomiting (hydromorphone ER: n=19, 33%, transdermal buprenorphine ER: n=8, 13%; p=NR, *OR 3.23, 95% CI: 1.28-8.13)
Numbers of vomits/day Mean number of vomits per day were similar for both study groups (hydromorphone ER: 0.1, transdermal buprenorphine ER: 0.1; p=NR)
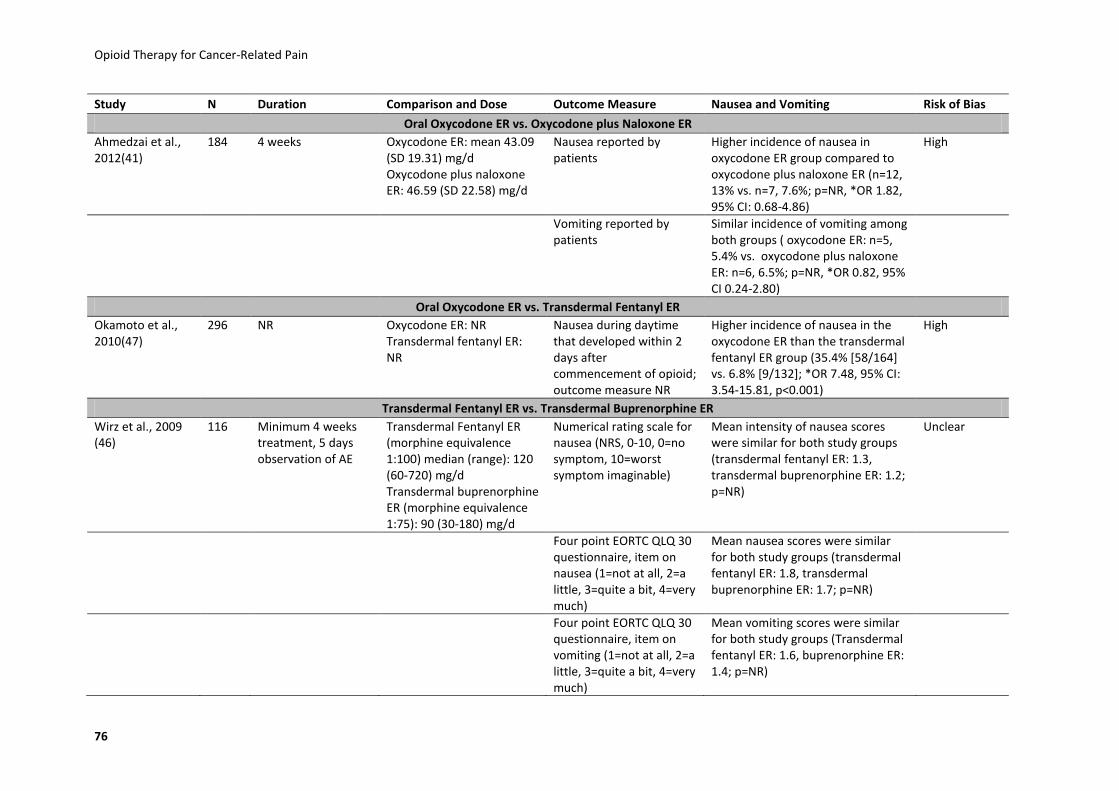
Opioid Therapy for Cancer-Related Pain
76
Study N Duration Comparison and Dose Outcome Measure Nausea and Vomiting Risk of Bias
Oral Oxycodone ER vs. Oxycodone plus Naloxone ER
Ahmedzai et al., 2012(41)
184 4 weeks Oxycodone ER: mean 43.09 (SD 19.31) mg/d Oxycodone plus naloxone ER: 46.59 (SD 22.58) mg/d
Nausea reported by patients
Higher incidence of nausea in oxycodone ER group compared to oxycodone plus naloxone ER (n=12, 13% vs. n=7, 7.6%; p=NR, *OR 1.82, 95% CI: 0.68-4.86)
High
Vomiting reported by patients
Similar incidence of vomiting among both groups ( oxycodone ER: n=5, 5.4% vs. oxycodone plus naloxone ER: n=6, 6.5%; p=NR, *OR 0.82, 95% CI 0.24-2.80)
Oral Oxycodone ER vs. Transdermal Fentanyl ER
Okamoto et al., 2010(47)
296 NR Oxycodone ER: NR Transdermal fentanyl ER: NR
Nausea during daytime that developed within 2 days after commencement of opioid; outcome measure NR
Higher incidence of nausea in the oxycodone ER than the transdermal fentanyl ER group (35.4% [58/164] vs. 6.8% [9/132]; *OR 7.48, 95% CI: 3.54-15.81, p<0.001)
High
Transdermal Fentanyl ER vs. Transdermal Buprenorphine ER
Wirz et al., 2009 (46)
116 Minimum 4 weeks treatment, 5 days observation of AE
Transdermal Fentanyl ER (morphine equivalence 1:100) median (range): 120 (60-720) mg/d Transdermal buprenorphine ER (morphine equivalence 1:75): 90 (30-180) mg/d
Numerical rating scale for nausea (NRS, 0-10, 0=no symptom, 10=worst symptom imaginable)
Mean intensity of nausea scores were similar for both study groups (transdermal fentanyl ER: 1.3, transdermal buprenorphine ER: 1.2; p=NR)
Unclear
Four point EORTC QLQ 30 questionnaire, item on nausea (1=not at all, 2=a little, 3=quite a bit, 4=very much)
Mean nausea scores were similar for both study groups (transdermal fentanyl ER: 1.8, transdermal buprenorphine ER: 1.7; p=NR)
Four point EORTC QLQ 30 questionnaire, item on vomiting (1=not at all, 2=a little, 3=quite a bit, 4=very much)
Mean vomiting scores were similar for both study groups (Transdermal fentanyl ER: 1.6, buprenorphine ER: 1.4; p=NR)
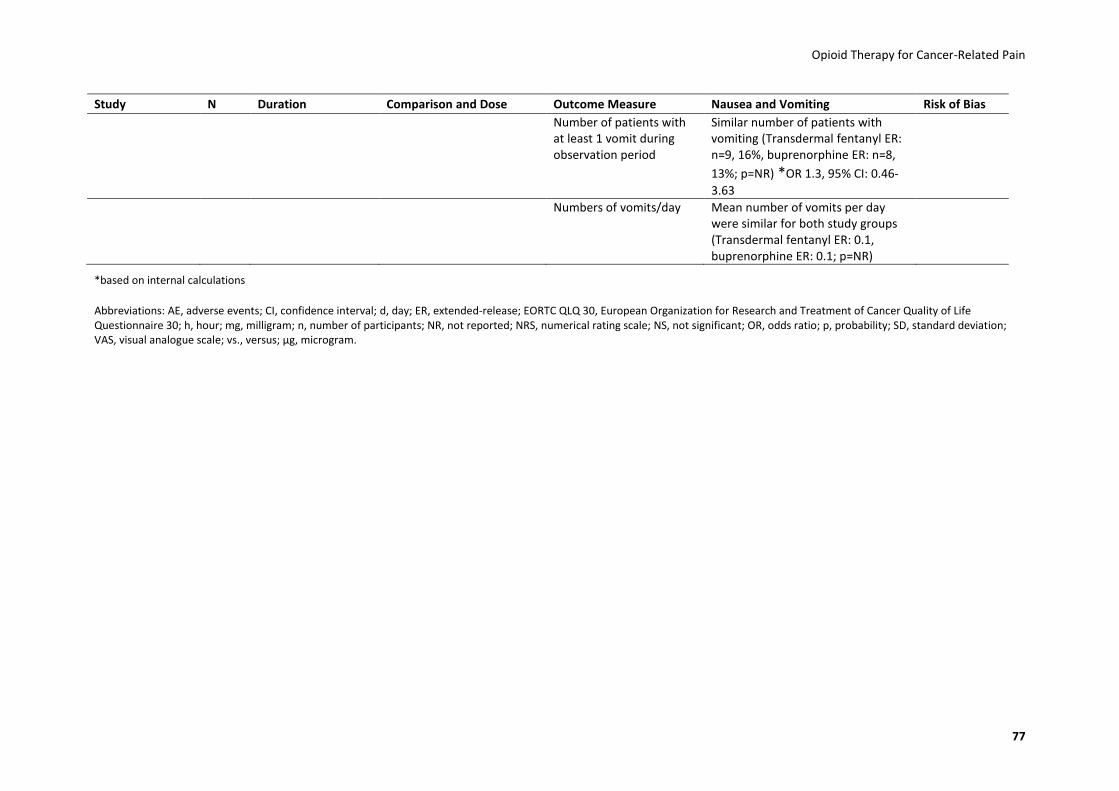
Opioid Therapy for Cancer-Related Pain
77
Study N Duration Comparison and Dose Outcome Measure Nausea and Vomiting Risk of Bias
Number of patients with at least 1 vomit during observation period
Similar number of patients with vomiting (Transdermal fentanyl ER: n=9, 16%, buprenorphine ER: n=8,
13%; p=NR) *OR 1.3, 95% CI: 0.46-
3.63
Numbers of vomits/day Mean number of vomits per day were similar for both study groups (Transdermal fentanyl ER: 0.1, buprenorphine ER: 0.1; p=NR)
*based on internal calculations
Abbreviations: AE, adverse events; CI, confidence interval; d, day; ER, extended-release; EORTC QLQ 30, European Organization for Research and Treatment of Cancer Quality of Life Questionnaire 30; h, hour; mg, milligram; n, number of participants; NR, not reported; NRS, numerical rating scale; NS, not significant; OR, odds ratio; p, probability; SD, standard deviation; VAS, visual analogue scale; vs., versus; μg, microgram.
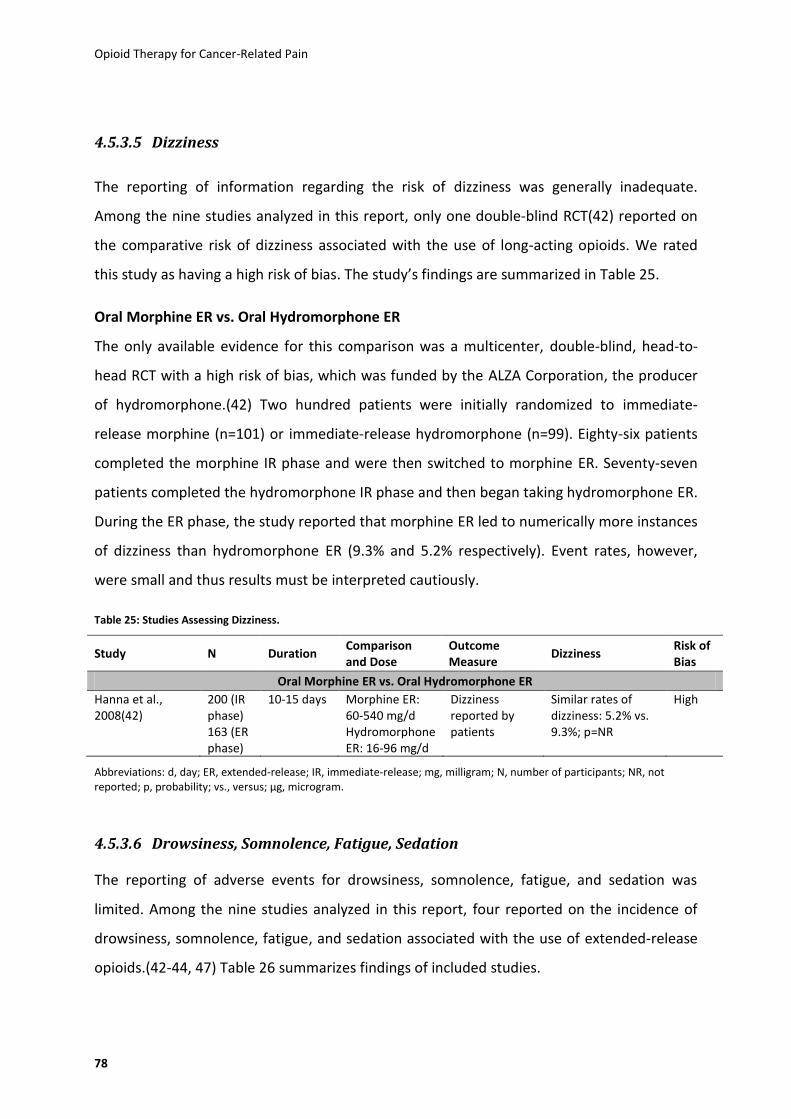
Opioid Therapy for Cancer-Related Pain
78
4.5.3.5 Dizziness
The reporting of information regarding the risk of dizziness was generally inadequate.
Among the nine studies analyzed in this report, only one double-blind RCT(42) reported on
the comparative risk of dizziness associated with the use of long-acting opioids. We rated
this study as having a high risk of bias. The study’s findings are summarized in Table 25.
Oral Morphine ER vs. Oral Hydromorphone ER
The only available evidence for this comparison was a multicenter, double-blind, head-to-
head RCT with a high risk of bias, which was funded by the ALZA Corporation, the producer
of hydromorphone.(42) Two hundred patients were initially randomized to immediate-
release morphine (n=101) or immediate-release hydromorphone (n=99). Eighty-six patients
completed the morphine IR phase and were then switched to morphine ER. Seventy-seven
patients completed the hydromorphone IR phase and then began taking hydromorphone ER.
During the ER phase, the study reported that morphine ER led to numerically more instances
of dizziness than hydromorphone ER (9.3% and 5.2% respectively). Event rates, however,
were small and thus results must be interpreted cautiously.
Table 25: Studies Assessing Dizziness.
Study N Duration Comparison and Dose
Outcome Measure
Dizziness Risk of Bias
Oral Morphine ER vs. Oral Hydromorphone ER
Hanna et al., 2008(42)
200 (IR phase) 163 (ER phase)
10-15 days Morphine ER: 60-540 mg/d Hydromorphone ER: 16-96 mg/d
Dizziness reported by patients
Similar rates of dizziness: 5.2% vs. 9.3%; p=NR
High
Abbreviations: d, day; ER, extended-release; IR, immediate-release; mg, milligram; N, number of participants; NR, not reported; p, probability; vs., versus; μg, microgram.
4.5.3.6 Drowsiness, Somnolence, Fatigue, Sedation
The reporting of adverse events for drowsiness, somnolence, fatigue, and sedation was
limited. Among the nine studies analyzed in this report, four reported on the incidence of
drowsiness, somnolence, fatigue, and sedation associated with the use of extended-release
opioids.(42-44, 47) Table 26 summarizes findings of included studies.
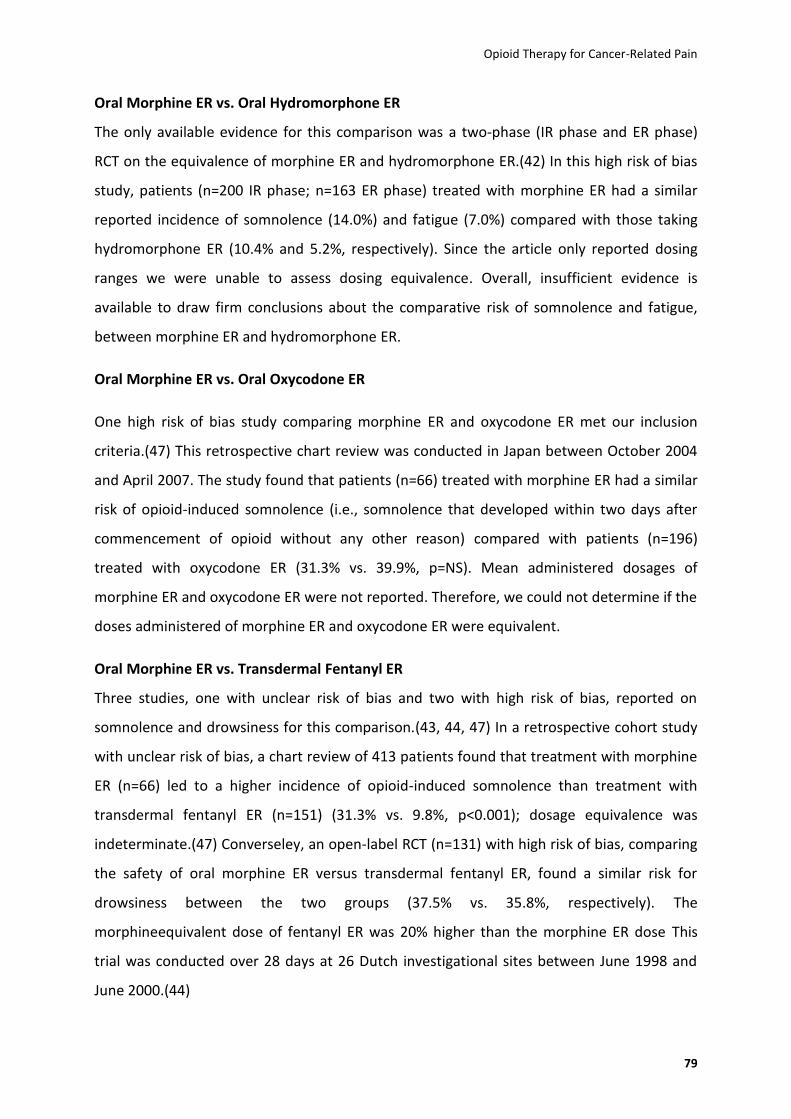
Opioid Therapy for Cancer-Related Pain
79
Oral Morphine ER vs. Oral Hydromorphone ER
The only available evidence for this comparison was a two-phase (IR phase and ER phase)
RCT on the equivalence of morphine ER and hydromorphone ER.(42) In this high risk of bias
study, patients (n=200 IR phase; n=163 ER phase) treated with morphine ER had a similar
reported incidence of somnolence (14.0%) and fatigue (7.0%) compared with those taking
hydromorphone ER (10.4% and 5.2%, respectively). Since the article only reported dosing
ranges we were unable to assess dosing equivalence. Overall, insufficient evidence is
available to draw firm conclusions about the comparative risk of somnolence and fatigue,
between morphine ER and hydromorphone ER.
Oral Morphine ER vs. Oral Oxycodone ER
One high risk of bias study comparing morphine ER and oxycodone ER met our inclusion
criteria.(47) This retrospective chart review was conducted in Japan between October 2004
and April 2007. The study found that patients (n=66) treated with morphine ER had a similar
risk of opioid-induced somnolence (i.e., somnolence that developed within two days after
commencement of opioid without any other reason) compared with patients (n=196)
treated with oxycodone ER (31.3% vs. 39.9%, p=NS). Mean administered dosages of
morphine ER and oxycodone ER were not reported. Therefore, we could not determine if the
doses administered of morphine ER and oxycodone ER were equivalent.
Oral Morphine ER vs. Transdermal Fentanyl ER
Three studies, one with unclear risk of bias and two with high risk of bias, reported on
somnolence and drowsiness for this comparison.(43, 44, 47) In a retrospective cohort study
with unclear risk of bias, a chart review of 413 patients found that treatment with morphine
ER (n=66) led to a higher incidence of opioid-induced somnolence than treatment with
transdermal fentanyl ER (n=151) (31.3% vs. 9.8%, p<0.001); dosage equivalence was
indeterminate.(47) Converseley, an open-label RCT (n=131) with high risk of bias, comparing
the safety of oral morphine ER versus transdermal fentanyl ER, found a similar risk for
drowsiness between the two groups (37.5% vs. 35.8%, respectively). The
morphineequivalent dose of fentanyl ER was 20% higher than the morphine ER dose This
trial was conducted over 28 days at 26 Dutch investigational sites between June 1998 and
June 2000.(44)

Opioid Therapy for Cancer-Related Pain
80
An open-label RCT (n=72) also compared morphine ER versus transdermal fentanyl ER.
However, due to the high risk of bias and low quality of evidence (for adverse events only,
within group comparisons were presented), no inferences can be made from this study
about differences between the two drugs in opioid-induced drowsiness in cancer
patients.(43)
Oral Hydromorphone ER vs. Oral Oxycodone ER
One study met our eligibility criteria for this comparison - a high risk of bias RCT (n=44)
comparing the safety of hydromorphone ER versus oxycodone ER over a study period of
seven days.(40)
There were no significant differences between treatments in sedation VAS when tested by
time of day (p=0.11) and by day of treatment (p=0.1114). Patients who received
hydromorphone ER, however, had fewer overall reported incidents of sedation than patients
who took oxycodone ER (19.92% vs. 24.81%; p=NR). Results should be interepreted with
caution because the mean morphine-dose-equivalent of oxycodone ER (124 mg/d) was 50%
higher than that of hydromorphone ER (30 mg/d).
Oral Oxycodone ER vs. Transdermal Fentanyl ER
The only available evidence for this comparison was a high risk of bias retrospective chart
review that collected data on somnolence from the Japanese medical records of patients
suffering from cancer pain. Patients (n=196) treated with oxycodone ER had a higher
incidence of opioid-induced somnolence than patients (n=151) treated with transdermal
fentanyl ER (39.9% vs. 9.8%, p<0.001).(47) Dosgae equivallencies could not be determined
because mean adminstered dosages were not reported (only ranges).

Opioid Therapy for Cancer-Related Pain
81
Table 26: Studies Assessing Drowsiness, Somnolence, Fatigue, or Sedation.
Study N Duration Comparison and Dose Outcome Measure Drowsiness, Somnolence or Fatigue
Risk of Bias
Oral Morphine ER vs. oral Hydromorphone ER
Hanna et al., 2008(42)
200 (IR phase) 163 (ER phase)
10-15 days Morphine ER: 60-540 mg/dHydromorphone ER: 16-96 mg/d
Somnolence reported by patients
Similar incidence of somnolence: 14.0% vs. 10.4%; p=NR
High
Fatigue reported by patients
Similar numbers of patients reporting fatigue: 7.0% vs. 5.2%; p=NR
Oral Morphine ER vs. oral Oxycodone ER
Okamoto et al., 2010(47)
262 NR Morphine ER: 48.0±34.7 mg/d Oxycodone ER (oral morphine equivalent): 21.4±12.1 mg/d
Somnolence during daytime that developed within 2 days after commencement of opioid; outcome measure NR
Similar incidence of somnolence: 31.3% vs. 39.9%; p=NS
High
Oral Morphine ER vs. Transdermal Fentanyl ER
Mercadante et al., 2008(43)
72 4 weeks Morphine ER: 60 mg/d Transdermal Fentanyl ER: 25 µg/h
4-point scale for drowsiness (0=not at all, 1=slight, 2=a lot, 3=severe)
Similar ratings for drowsiness: 0.6% vs. 0.9%; p=NR
High
Okamoto et al., 2010(47)
217 NR Morphine ER: 48.0±34.7 mg/d Transdermal Fentanyl ER (oral morphine equivalent): 92.5±65.7 mg/d
Somnolence during daytime that developed within 2 days after commencement of opioid; outcome measure NR
Higher incidence of somnolence for patients treated with Morphine ER: 31.3% vs. 9.8%; p<0.001
High
van Seventer et al., 2003(44)
131 4 weeks Morphine ER: average max. dose (range) 105 (30-400) mg/d Transdermal Fentanyl ER: 67 (25-400) µg/h
4-point scale for daytime drowsiness (1=not at all, 4=very much)
No difference for daytime drowsiness: 0.5% vs. 0.4%; p=0.973
High

Opioid Therapy for Cancer-Related Pain
82
Study N Duration Comparison and Dose Outcome Measure Drowsiness, Somnolence or Fatigue
Risk of Bias
Drowsiness reported by patients
Similar numbers of patients reporting drowsiness: n=24, 37.5% vs. n=24, 35.8%; p=NS
Epworth Sleepiness Scale: 4-point scale for 8 items (0=would never doze, 3=high chance of dozing)
No difference for daytime sleepiness: 4.8% vs. 2.9%; p=0.175
Oral Hydromorphone ER vs. Oral Oxycodone ER
Hagen and Babul, 1997(40)
44 7 days Hydromorphone ER: mean final dose 30 ± 6 mg/d Oxycodone ER: 124 ± 22 mg/d
VAS 0-100mm for sedation (0=no sedation, 100=extreme sedation), assessed 4 times a day
Lower overall mean sedation score for patients treated with Hydromorphone ER: 19.92% vs. 24.81%; p=NR
High
Oral Oxycodone ER vs. Transdermal Fentanyl ER
Okamoto et al., 2010(47)
347 NR Oxycodone ER (oral morphine equivalent): 21.4±12.1 mg/d Transdermal Fentanyl ER (oral morphine equivalent): 92.5±65.7 mg/d
Somnolence during daytime that developed within 2 days after commencement of opioid; outcome measure NR
Higher incidence of somnolence for patients treated with Oxycodone ER: 39.9% vs. 9.8%; p<0.001
High
Abbreviations: d, day; ER, extended-release; h, hour; IR, immediate-release; mg, milligram; n, number of participants; NR, not reported; NS, not significant; p, probability; VAS, visual analog scale; vs., versus; μg, microgram.

Opioid Therapy for Cancer-Related Pain
83
4.5.3.7 Diarrhea
Diarrhea has been reported as an adverse event of naloxone, an opioid antagonist. Only one
study addressed the risk of diarrhea.(41) Table 27 summarizes findings of the included study.
Oral Oxycodone ER vs. Oxycodone plus Naloxone ER
A high risk of bias RCT compared the reported symptoms of diarrhea in 184 patients treated
with oral oxycodone ER or oral oxycodone plus naloxone ER over a treatment period of four
weeks and showed no difference between the groups (4.3% vs. 4.3%).(41) We were unable
to assess the dosing equivalence of the administered drugs in this study because mean
dosages were not reported.
Table 27: Studies Assessing Diarrhea.
Study N Duration Comparison and Dose
Outcome Measure
Diarrhea Risk of Bias
Oral Oxycodone ER vs. Oxycodone plus Naloxone ER
Ahmedzai et al., 2012(41)
184 4 weeks Oxycodone ER: mean 43.09 (SD 19.31) mg/d oxycodone plus naloxone ER: 46.59 (SD 22.58) mg/d
Diarrhea reported by patients
Same number of patients reported diarrhea (n=4, 4.3% in both study groups; p=NR)
High
Abbreviations: d, day; ER, extended-release; mg, milligram; n, number of participants; NR, not reported; SD, standard deviation; vs., versus.
4.6 Key Question 3: Efficacy, Effectiveness, or Risk for Harms
in Subpopulations
We did not identify any study that addressed this key question.
Opioid Therapy for Cancer-Related Pain
84
5 Discussion
5.1 Key Findings and Strength of Evidence
This systematic review assesses the comparative efficacy, effectiveness and risk of harms of
extended-release opioids for the treatment of cancer-related pain. Overall, for most
interventions and outcomes of interest, evidence was either lacking or insufficient to draw
conclusions. Furthermore, in the evidence available, the eligible studies were fraught with
serious methodological shortcomings. Consequently, most of the conclusions have a very
high degree of uncertainty:
The comparative efficacy for improvement of pain intensity, quality of life, functional
capacity, and cognitive functioning was similar among compared drugs.
Discontinuation rates because of lack of efficacy were also similar. The strength of
evidence supporting similar efficacy among compared drugs is very low.
We could not find eligible evidence on the comparative efficacy of transdermal
buprenorphine ER, dihydrocodeine ER, transdermal fentanyl ER, morphine plus
naltrexone ER, nalbuphine ER, oxymorphone ER, tapentadol hydrochloride ER, and
tramadol ER.
With few exceptions, the comparative risk of harms was also similar among reviewed
drugs. Discontinuation rates because of adverse events were similar. The strength of
evidence supporting a similar risk of harms with respect to serious adverse events,
constipation, nausea and vomiting, dizziness, and somnolence among compared
drugs is low or very low.
A notable exception, albeit based on weak evidence, is that oxycodone ER had higher
risks of some adverse events than comparator drugs:
o a higher risk of drowsiness than hydromorphone ER;
o a higher risk of constipation than oxycodone plus naloxone ER;
o a higher risk of nausea than morphine ER and transdermal fentanyl ER;
o and a higher risk of somnolence than transdermal fentanyl ER.

Opioid Therapy for Cancer-Related Pain
85
GRADE Evidence Profiles with strength of evidence ratings for all outcomes within each
comparison can be found in Appendix E (Appendix-Table 3 to Appendix-Table 14).
5.2 Gaps in the Evidence
Three main drawbacks posed challenges for this review and limit findings about the
comparative efficacy and risk of harms of extended-release opioids. First, no studies existed
for many interventions. Out of 66 possible comparisons for this drug class, we found no
evidence on 75 comparisons for comparative efficacy, and 69 for comparative risk of harms.
Consequently, we can neither confirm nor rule out differences in the comparative efficacy
and risk of harms for the majority of comparisons. Second, the available evidence was often
limited to a single study with methodological shortcomings. Many of these studies did not
publish details about some attributes of their subjects (e.g., race or ethnicity); and generally
investigators did not report whether interventions were efficacious for subgroups.
Therefore, whether findings can be applied to subgroups with respect to sex, ethnicity, age,
moderate vs. severe cancer pain, breakthrough pain, or pain with a neuropathic component
is unclear. Furthermore, no evidence on patients taking other commonly prescribed co-
analgesics (e.g., non-steroidal anti-inflammatory drugs, antiepileptic drugs, antidepressants)
was available. Third, the few interventions with somewhat reliable evidence for the risk of
harms often had wide confidence intervals which lead to inconclusive results.

Opioid Therapy for Cancer-Related Pain
86
6 Conclusions
The evidence available indicates no substantial differences in efficacy and risk of harms
amongst extended-release opioids. The body of evidence, however, is limited to few
comparisons and fraught with methodological shortcomings. Generally, our confidence in
the available estimates is very low. We anticipate that future studies will change these
estimates. Given the lack of reliable evidence regarding the comparative benefits and harms
of extended-release opioids, clinicians should weigh clinical experience, patient preferences,
and treatment costs when choosing the optimal treatment for an individual cancer patient.
Opioid Therapy for Cancer-Related Pain
87
7 References
1. Breivik H, Cherny N, Collett B, de Conno F, Filbet M, Foubert AJ, et al. Cancer-related pain: a pan-European survey of prevalence, treatment, and patient attitudes. Ann Oncol. 2009;20(8):1420-33. Epub 2009/02/27. 2. Patrick DL, Ferketich SL, Frame PS, Harris JJ, Hendricks CB, Levin B, et al. National Institutes of Health State-of-the-Science Conference Statement: Symptom management in cancer: pain, depression, and fatigue, July 15-17, 2002. J Natl Cancer Inst Monogr. 2004(32):9-16. Epub 2004/07/21. 3. Paice JA, Ferrell B. The management of cancer pain. CA: a cancer journal for clinicians. 2011;61(3):157-82. Epub 2011/05/06. 4. van den Beuken-van Everdingen MHJ, de Rijke JM, Kessels AG, Schouten HC, van Kleef M, Patijn J. Prevalence of pain in patients with cancer: A systematic review of the past 40 years. Annals of Oncology. 2007;18(9):1437-49. 5. Meresky H, Bogduk N. Classification of Chronic Pain. Descriptions of Chronic Pain Syndromes and Definitions of Pain Terms. IASP Press. 1994;2nd ed. Seattle. 6. Strang P. Annals of Oncology. 1998;37:641-44. 7. Temel JS, Greer JA, Muzikansky A, Gallagher ER, Admane S, Jackson VA, et al. Early palliative care for patients with metastatic non-small-cell lung cancer. N Engl J Med. 2010;363(8):733-42. Epub 2010/09/08. 8. Jost L, Roila F. Management of cancer pain: ESMO Clinical Practice Guidelines. Ann Oncol. 2010;21 Suppl 5:v257-60. Epub 2010/06/29. 9. WHO. Cancer pain relief and palliative care. Geneva: 1990. 10. Vadalouca A, Raptis E, Moka E, Zis P, Sykioti P, Siafaka I. Pharmacological treatment of neuropathic cancer pain: a comprehensive review of the current literature. Pain Pract. 2012;12(3):219-51. Epub 2011/07/30. 11. Hjermstad MJ, Fayers PM, Haugen DF, Caraceni A, Hanks GW, Loge JH, et al. Studies Comparing Numerical Rating Scales, Verbal Rating Scalens, and Visual Analogue Scales for Assessment of Pain Intensity in Adults: A Systematic Literature Review. J Pain Symptom Manage. 2011;41:1073-93. 12. Li KK, Harris K, Hadi S, Chow E. What should be the optimal cut points for mild, moderate, and severe pain? J Palliat Med. 2007;10(6):1338-46. Epub 2007/12/22. 13. Paul SM, Zelman DC, Smith M, Miaskowski C. Categorizing the severity of cancer pain: further exploration of the establishment of cutpoints. Pain. 2005;113(1-2):37-44. Epub 2004/12/29. 14. Ripamonti CI, Bandieri E, Roila F. Management of cancer pain: ESMO Clinical Practice Guidelines. Ann Oncol. 2011;22 Suppl 6:vi69-77. Epub 2011/10/20. 15. Holen JC, Hjermstad MJ, Loge JH, Fayers PM, Caraceni A, De Conno F, et al. Pain assessment tools: is the content appropriate for use in palliative care? J Pain Symptom Manage. 2006;32(6):567-80. Epub 2006/12/13. 16. Caraceni A, Hanks G, Kaasa S, Bennett MI, Brunelli C, Cherny N, et al. Use of opioid analgesics in the treatment of cancer pain: evidence-based recommendations from the EAPC. Lancet Oncol. 2012;13(2):e58-68. Epub 2012/02/04. 17. WHO. Cancer pain relief. Second Edition. With a guide to opioid availability. Geneva: 1996. 18. Nabal M, Librada S, Redondo MJ, Pigni A, Brunelli C, Caraceni A. The role of paracetamol and nonsteroidal anti-inflammatory drugs in addition to WHO Step III opioids in the control of pain in advanced cancer. A systematic review of the literature. Palliat Med. 2012;26(4):305-12. Epub 2011/12/01. 19. Colson J, Koyyalagunta D, Falco FJ, Manchikanti L. A systematic review of observational studies on the effectiveness of opioid therapy for cancer pain. Pain Physician. 2011;14(2):E85-102. Epub 2011/03/18. 20. US Food and Drug Administration. EXTENDED-RELEASE (ER) AND LONG-ACTING (LA) OPIOID ANALGESICS RISK EVALUATION AND MITIGATION STRATEGY (REMS). 2012 [08.08.2012]; Available from: http://www.fda.gov/downloads/Drugs/DrugSafety/PostmarketDrugSafetyInformationforPatientsandProviders/UCM311290.pdf. 21. Porreca F, Ossipov MH. Nausea and vomiting side effects with opioid analgesics during treatment of chronic pain: mechanisms, implications, and management options. Pain Med. 2009;10(4):654-62. Epub 2009/03/24. 22. Gupta K, Kshirsagar S, Chang L, Schwartz R, Law PY, Yee D, et al. Morphine stimulates angiogenesis by activating proangiogenic and survival-promoting signaling and promotes breast tumor growth. Cancer Res. 2002;62(15):4491-8. Epub 2002/08/03.

Opioid Therapy for Cancer-Related Pain
88
23. FDA US Department of Health and Human Services. FDA NEWS RELEASE. FDA, U.S. Department of Health and Human Services,; 2012 [08.08.2012]; Available from: http://www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm310870.htm. 24. Harvey RA, Champe PC. Lippincott's Illustrated Review - Pharmacology (4th ed). Philadelphia: Lippincott Williams & Wilkins, 2009. 25. Vallejo R, Barkin RL, Wang VC. Pharmacology of opioids in the treatment of chronic pain syndromes. Pain Physician. 2011;14(4):E343-60. Epub 2011/07/26. 26. Trivedi M, Shaikh S, Gwinnut C. Pharmacology of Opioids. Update in Anaesthesia (special edition). Update in Anaesthesia. 2008;24(2):118-24. 27. Inturrisi C, Lipman AG. Bonica's Management of Pain (4th ed). Philadelphia: Lippincott Williams & Wilkins, 2009. 28. Hartrick CT, Rozek RJ. Tapentadol in pain management: a mu-opioid receptor agonist and noradrenaline reuptake inhibitor. CNS Drugs. 2011;25(5):359-70. Epub 2011/04/12. 29. Slatkin NE. Opioid switching and rotation in primary care: Implementation and clinical utility. Current Medical Research and Opinion. 2009;25(9):2133-50. 30. Fukshansky M, Are M, Burton AW. The role of opioids in cancer pain management. Pain Pract. 2005;5(1):43-53; quiz -4. Epub 2006/12/13. 31. Balch RJ, Trescot A. Extended-release morphine sulfate in treatment of severe acute and chronic pain. Journal of pain research. 2010;3:191-200. Epub 2011/01/05. 32. Guay DR. Oral hydromorphone extended-release. The Consultant pharmacist : the journal of the American Society of Consultant Pharmacists. 2010;25(12):816-28. Epub 2010/12/22. 33. Semenchuk MR. Avinza Elan. Curr Opin Investig Drugs. 2002;3(9):1369-72. Epub 2002/12/25. 34. Hanna MH, Elliott KM, Fung M. Randomized, double-blind study of the analgesic efficacy of morphine-6-glucuronide versus morphine sulfate for postoperative pain in major surgery. Anesthesiology. 2005;102(4):815-21. 35. Ammar HO, Ghorab M, El-Nahhas SA, Kamel R. Polymeric matrix system for prolonged delivery of tramadol hydrochloride, part I: physicochemical evaluation. AAPS PharmSciTech. 2009;10(1):7-20. Epub 2009/01/10. 36. Higgins J, Green S. Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 [updated September 2008]. The Cochrane Collaboration, 2008; 2008 [06.07.2011]; Available from: http://www.cochrane-handbook.org/. 37. Deeks JJ, Dinnes J, D'Amico R, Sowden AJ, Sakarovitch C, Song F, et al. Evaluating non-randomised intervention studies. Health Technol Assess. 2003;7(27):iii-x, 1-173. 38. Guyatt GH, Oxman AD, Vist GE, Kunz R, Falck-Ytter Y, Alonso-Coello P, et al. GRADE: an emerging consensus on rating quality of evidence and strength of recommendations. BMJ. 2008;336(7650):924-6. Epub 2008/04/26. 39. Balshem H, Helfand M, Schunemann HJ, Oxman AD, Kunz R, Brozek J, et al. GRADE guidelines: 3. Rating the quality of evidence. Journal of Clinical Epidemiology. 2011;64(4):401-6. 40. Hagen NA, Babul N. Comparative clinical efficacy and safety of a novel controlled-release oxycodone formulation and controlled-release hydromorphone in the treatment of cancer pain. Cancer. 1997;79(7):1428-37. Epub 1997/04/01. 41. Ahmedzai SH, Nauck F, Bar-Sela G, Bosse B, Leyendecker P, Hopp M. A randomized, double-blind, active-controlled, double-dummy, parallel-group study to determine the safety and efficacy of oxycodone/naloxone prolonged-release tablets in patients with moderate/severe, chronic cancer pain. Palliat Med. 2012;26(1):50-60. Epub 2011/09/23. 42. Hanna M, Thipphawong J. A randomized, double-blind comparison of OROS® hydromorphone and controlled-release morphine for the control of chronic cancer pain. BMC Palliative Care. 2008;7(1). 43. Mercadante S, Porzio G, Ferrera P, Fulfaro F, Aielli F, Verna L, et al. Sustained-release oral morphine versus transdermal fentanyl and oral methadone in cancer pain management. Eur J Pain. 2008;12(8):1040-6. Epub 2008/03/21. 44. van Seventer R, Smit JM, Schipper RM, Wicks MA, Zuurmond WW. Comparison of TTS-fentanyl with sustained-release oral morphine in the treatment of patients not using opioids for mild-to-moderate pain. Curr Med Res Opin. 2003;19(6):457-69. Epub 2003/11/05. 45. Wirz S, Wartenberg HC, Nadstawek J. Less nausea, emesis, and constipation comparing hydromorphone and morphine? A prospective open-labeled investigation on cancer pain. Support Care Cancer. 2008;16(9):999-1009. Epub 2007/12/21.

Opioid Therapy for Cancer-Related Pain
89
46. Wirz S, Wittmann M, Schenk M, Schroeck A, Schaefer N, Mueller M, et al. Gastrointestinal symptoms under opioid therapy: a prospective comparison of oral sustained-release hydromorphone, transdermal fentanyl, and transdermal buprenorphine. Eur J Pain. 2009;13(7):737-43. Epub 2008/11/04. 47. Okamoto Y, Tsuneto S, Tsugane M, Takagi T, Uejima E. A retrospective chart review of opioid-induced nausea and somnolence on commencement for cancer pain treatment. J Opioid Manag. 2010;6(6):431-4. Epub 2011/01/29. 48. Hartung DM, Middleton L, Haxby DG, Koder M, Ketchum KL, Chou R. Rates of adverse events of long-acting opioids in a state Medicaid program. Ann Pharmacother. 2007;41(6):921-8. Epub 2007/05/17. 49. Sherman RB, Woodcock J, Norden J, Grandinetti C, Temple RJ. New FDA regulation to improve safety reporting in clinical trials. N Engl J Med. 2011;365(1):3-5. Epub 2011/06/10. 50. European Medicines Agency. Clinical Safety Data Management: Definitions and Standards for Expedited Reporting. 1995 [04.10.2012]; Available from: http://www.emea.europa.eu/docs/en_GB/document_library/Scientific_guideline/2009/09/WC500002749.pdf. 51. Rentz AM, van Hanswijck de Jonge P, Leyendecker P, Hopp M. Observational, nonintervention, multicenter study for validation of the Bowel Function Index for constipation in European countries. Curr Med Res Opin. 2011;27(1):35-44. Epub 2010/11/19.
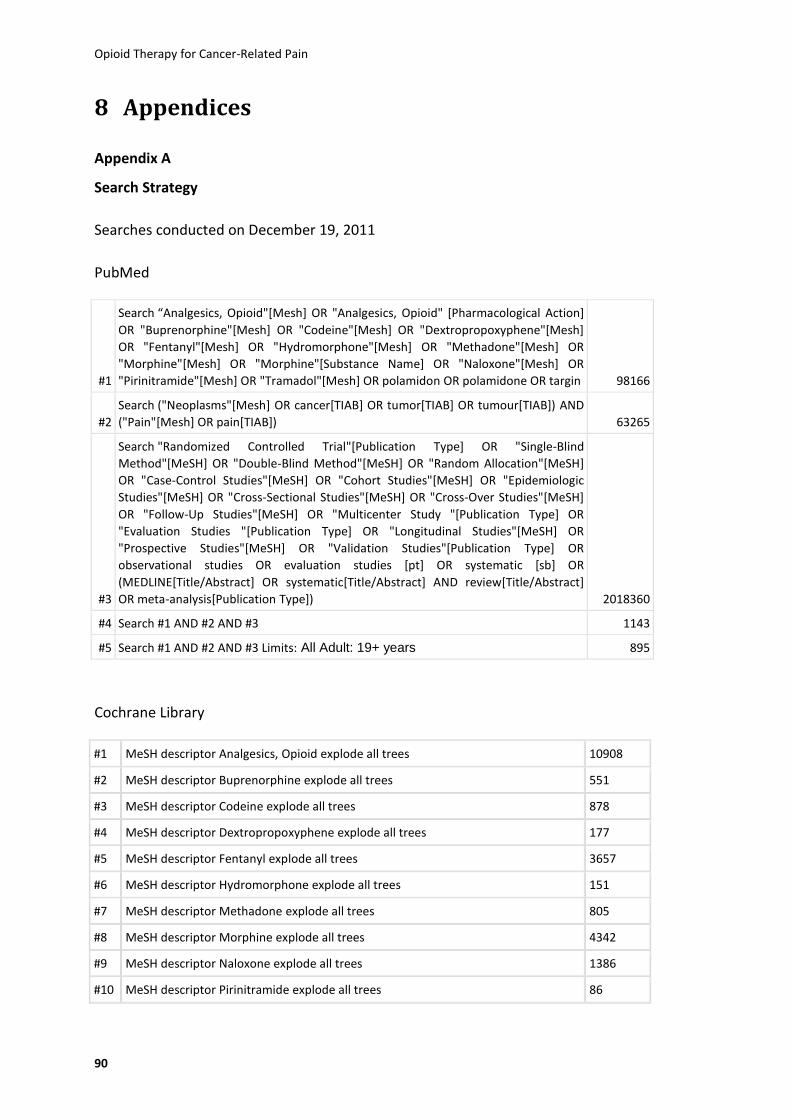
Opioid Therapy for Cancer-Related Pain
90
8 Appendices
Appendix A
Search Strategy
Searches conducted on December 19, 2011
PubMed
#1
Search “Analgesics, Opioid"[Mesh] OR "Analgesics, Opioid" [Pharmacological Action]
OR "Buprenorphine"[Mesh] OR "Codeine"[Mesh] OR "Dextropropoxyphene"[Mesh]
OR "Fentanyl"[Mesh] OR "Hydromorphone"[Mesh] OR "Methadone"[Mesh] OR
"Morphine"[Mesh] OR "Morphine"[Substance Name] OR "Naloxone"[Mesh] OR
"Pirinitramide"[Mesh] OR "Tramadol"[Mesh] OR polamidon OR polamidone OR targin 98166
#2
Search ("Neoplasms"[Mesh] OR cancer[TIAB] OR tumor[TIAB] OR tumour[TIAB]) AND
("Pain"[Mesh] OR pain[TIAB]) 63265
#3
Search "Randomized Controlled Trial"[Publication Type] OR "Single-Blind
Method"[MeSH] OR "Double-Blind Method"[MeSH] OR "Random Allocation"[MeSH]
OR "Case-Control Studies"[MeSH] OR "Cohort Studies"[MeSH] OR "Epidemiologic
Studies"[MeSH] OR "Cross-Sectional Studies"[MeSH] OR "Cross-Over Studies"[MeSH]
OR "Follow-Up Studies"[MeSH] OR "Multicenter Study "[Publication Type] OR
"Evaluation Studies "[Publication Type] OR "Longitudinal Studies"[MeSH] OR
"Prospective Studies"[MeSH] OR "Validation Studies"[Publication Type] OR
observational studies OR evaluation studies [pt] OR systematic [sb] OR
(MEDLINE[Title/Abstract] OR systematic[Title/Abstract] AND review[Title/Abstract]
OR meta-analysis[Publication Type]) 2018360
#4 Search #1 AND #2 AND #3 1143
#5 Search #1 AND #2 AND #3 Limits: All Adult: 19+ years 895
Cochrane Library
#1 MeSH descriptor Analgesics, Opioid explode all trees 10908
#2 MeSH descriptor Buprenorphine explode all trees 551
#3 MeSH descriptor Codeine explode all trees 878
#4 MeSH descriptor Dextropropoxyphene explode all trees 177
#5 MeSH descriptor Fentanyl explode all trees 3657
#6 MeSH descriptor Hydromorphone explode all trees 151
#7 MeSH descriptor Methadone explode all trees 805
#8 MeSH descriptor Morphine explode all trees 4342
#9 MeSH descriptor Naloxone explode all trees 1386
#10 MeSH descriptor Pirinitramide explode all trees 86
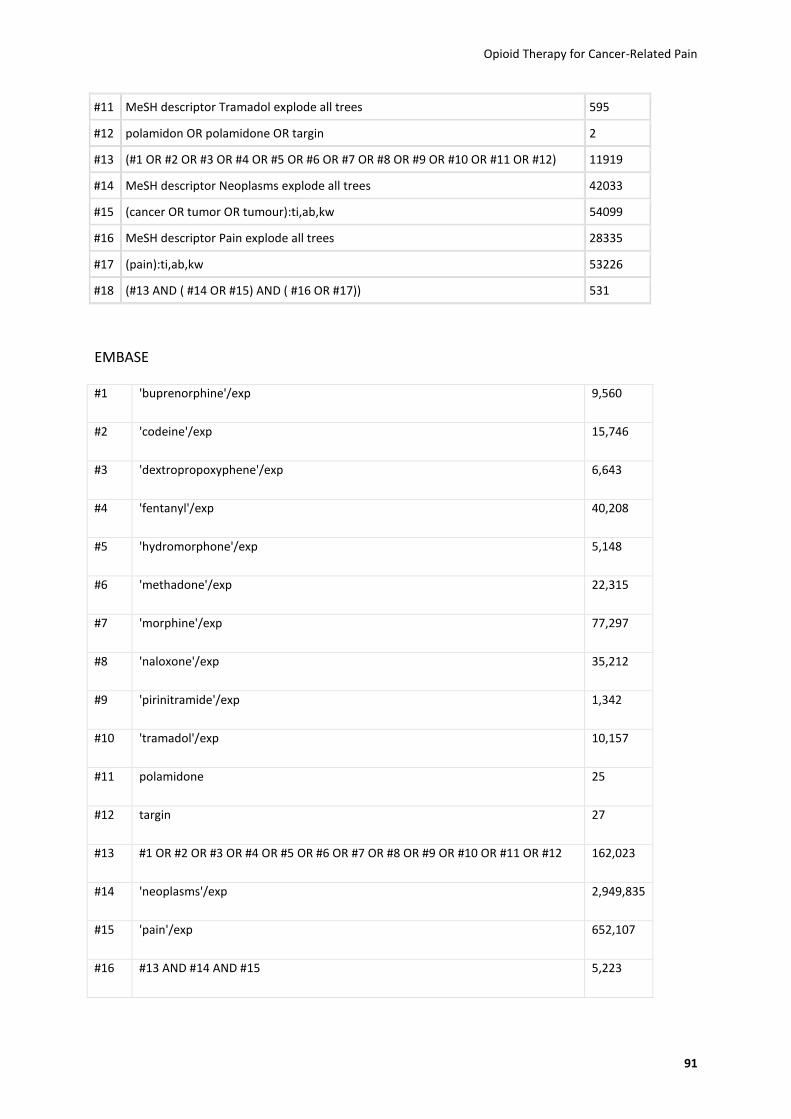
Opioid Therapy for Cancer-Related Pain
91
#11 MeSH descriptor Tramadol explode all trees 595
#12 polamidon OR polamidone OR targin 2
#13 (#1 OR #2 OR #3 OR #4 OR #5 OR #6 OR #7 OR #8 OR #9 OR #10 OR #11 OR #12) 11919
#14 MeSH descriptor Neoplasms explode all trees 42033
#15 (cancer OR tumor OR tumour):ti,ab,kw 54099
#16 MeSH descriptor Pain explode all trees 28335
#17 (pain):ti,ab,kw 53226
#18 (#13 AND ( #14 OR #15) AND ( #16 OR #17)) 531
EMBASE
#1 'buprenorphine'/exp 9,560
#2 'codeine'/exp 15,746
#3 'dextropropoxyphene'/exp 6,643
#4 'fentanyl'/exp 40,208
#5 'hydromorphone'/exp 5,148
#6 'methadone'/exp 22,315
#7 'morphine'/exp 77,297
#8 'naloxone'/exp 35,212
#9 'pirinitramide'/exp 1,342
#10 'tramadol'/exp 10,157
#11 polamidone 25
#12 targin 27
#13 #1 OR #2 OR #3 OR #4 OR #5 OR #6 OR #7 OR #8 OR #9 OR #10 OR #11 OR #12 162,023
#14 'neoplasms'/exp 2,949,835
#15 'pain'/exp 652,107
#16 #13 AND #14 AND #15 5,223
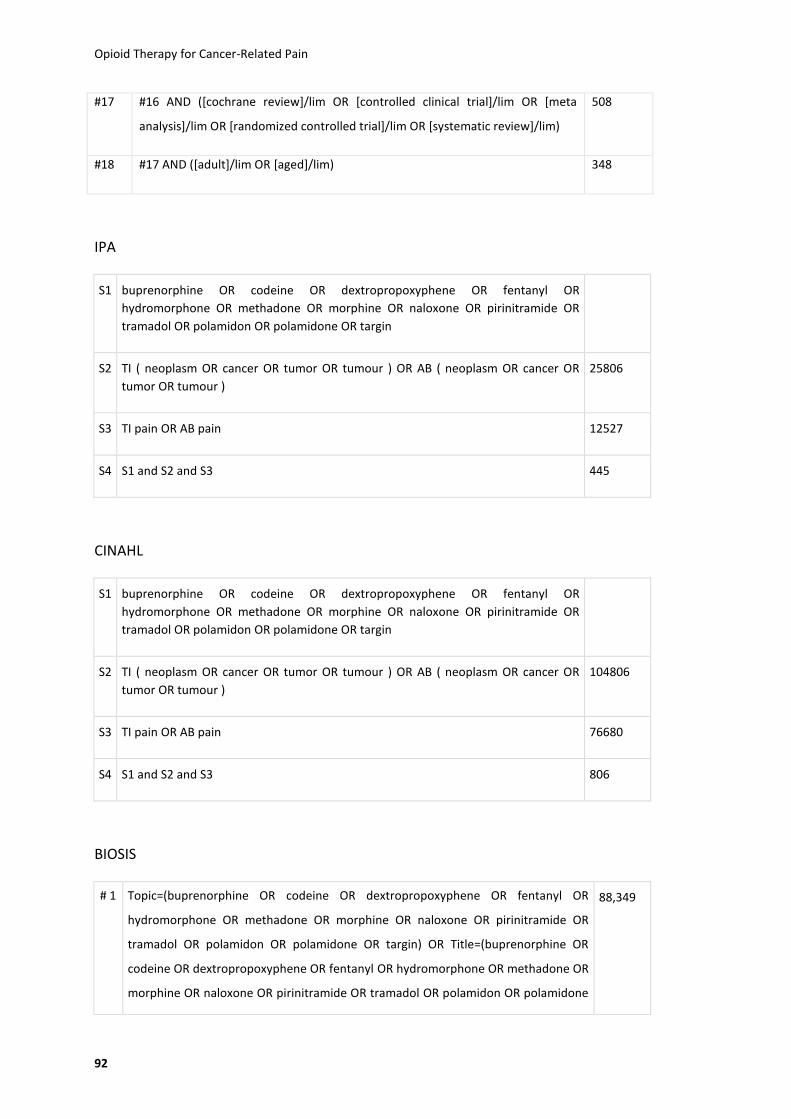
Opioid Therapy for Cancer-Related Pain
92
#17 #16 AND ([cochrane review]/lim OR [controlled clinical trial]/lim OR [meta
analysis]/lim OR [randomized controlled trial]/lim OR [systematic review]/lim)
508
#18 #17 AND ([adult]/lim OR [aged]/lim) 348
IPA
S1 buprenorphine OR codeine OR dextropropoxyphene OR fentanyl OR
hydromorphone OR methadone OR morphine OR naloxone OR pirinitramide OR
tramadol OR polamidon OR polamidone OR targin
S2 TI ( neoplasm OR cancer OR tumor OR tumour ) OR AB ( neoplasm OR cancer OR
tumor OR tumour )
25806
S3 TI pain OR AB pain 12527
S4 S1 and S2 and S3 445
CINAHL
S1 buprenorphine OR codeine OR dextropropoxyphene OR fentanyl OR
hydromorphone OR methadone OR morphine OR naloxone OR pirinitramide OR
tramadol OR polamidon OR polamidone OR targin
S2 TI ( neoplasm OR cancer OR tumor OR tumour ) OR AB ( neoplasm OR cancer OR
tumor OR tumour )
104806
S3 TI pain OR AB pain 76680
S4 S1 and S2 and S3 806
BIOSIS
# 1 Topic=(buprenorphine OR codeine OR dextropropoxyphene OR fentanyl OR
hydromorphone OR methadone OR morphine OR naloxone OR pirinitramide OR
tramadol OR polamidon OR polamidone OR targin) OR Title=(buprenorphine OR
codeine OR dextropropoxyphene OR fentanyl OR hydromorphone OR methadone OR
morphine OR naloxone OR pirinitramide OR tramadol OR polamidon OR polamidone
88,349

Opioid Therapy for Cancer-Related Pain
93
OR targin)
Databases=BIOSIS Previews Timespan=All Years
# 2 Title=(neoplasm OR cancer OR tumor OR tumour)
Databases=BIOSIS Previews Timespan=All Years
716,532
# 3 Title=(pain)
Databases=BIOSIS Previews Timespan=All Years
58,887
# 4 #1 AND #2 AND #3
Databases=BIOSIS Previews Timespan=All Years
917
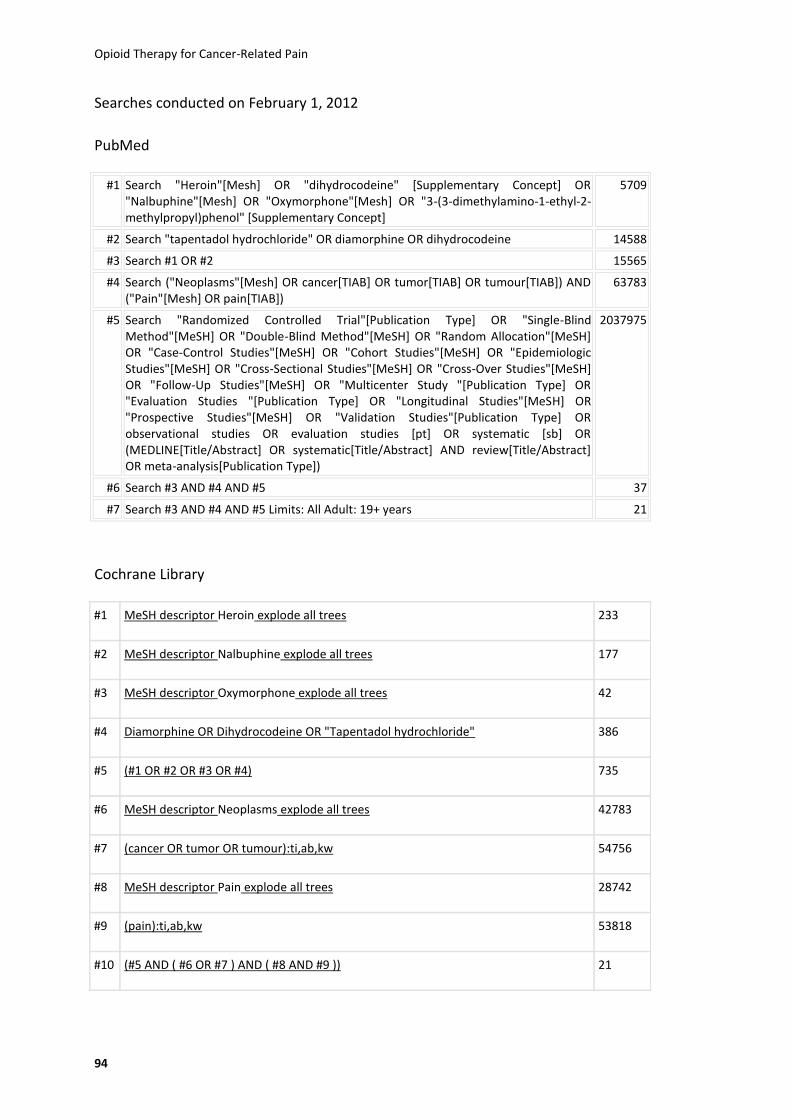
Opioid Therapy for Cancer-Related Pain
94
Searches conducted on February 1, 2012
PubMed
#1 Search "Heroin"[Mesh] OR "dihydrocodeine" [Supplementary Concept] OR "Nalbuphine"[Mesh] OR "Oxymorphone"[Mesh] OR "3-(3-dimethylamino-1-ethyl-2-methylpropyl)phenol" [Supplementary Concept]
5709
#2 Search "tapentadol hydrochloride" OR diamorphine OR dihydrocodeine 14588
#3 Search #1 OR #2 15565
#4 Search ("Neoplasms"[Mesh] OR cancer[TIAB] OR tumor[TIAB] OR tumour[TIAB]) AND ("Pain"[Mesh] OR pain[TIAB])
63783
#5 Search "Randomized Controlled Trial"[Publication Type] OR "Single-Blind Method"[MeSH] OR "Double-Blind Method"[MeSH] OR "Random Allocation"[MeSH] OR "Case-Control Studies"[MeSH] OR "Cohort Studies"[MeSH] OR "Epidemiologic Studies"[MeSH] OR "Cross-Sectional Studies"[MeSH] OR "Cross-Over Studies"[MeSH] OR "Follow-Up Studies"[MeSH] OR "Multicenter Study "[Publication Type] OR "Evaluation Studies "[Publication Type] OR "Longitudinal Studies"[MeSH] OR "Prospective Studies"[MeSH] OR "Validation Studies"[Publication Type] OR observational studies OR evaluation studies [pt] OR systematic [sb] OR (MEDLINE[Title/Abstract] OR systematic[Title/Abstract] AND review[Title/Abstract] OR meta-analysis[Publication Type])
2037975
#6 Search #3 AND #4 AND #5 37
#7 Search #3 AND #4 AND #5 Limits: All Adult: 19+ years 21
Cochrane Library
#1 MeSH descriptor Heroin explode all trees 233
#2 MeSH descriptor Nalbuphine explode all trees 177
#3 MeSH descriptor Oxymorphone explode all trees 42
#4 Diamorphine OR Dihydrocodeine OR "Tapentadol hydrochloride" 386
#5 (#1 OR #2 OR #3 OR #4) 735
#6 MeSH descriptor Neoplasms explode all trees 42783
#7 (cancer OR tumor OR tumour):ti,ab,kw 54756
#8 MeSH descriptor Pain explode all trees 28742
#9 (pain):ti,ab,kw 53818
#10 (#5 AND ( #6 OR #7 ) AND ( #8 AND #9 )) 21

Opioid Therapy for Cancer-Related Pain
95
EMBASE
#1 'diamorphine'/exp OR 'dihydrocodeine'/exp OR 'oxymorphone'/exp OR
'tapentadol'/exp OR 'nalbuphine'/exp
22,348
#2 'neoplasm'/exp 2,974,9
16
#3 'pain'/exp 659,81
5
#4 #1 AND #2 AND #3
434
#5 #4 AND ([cochrane review]/lim OR [controlled clinical trial]/lim OR [meta
analysis]/lim OR [randomized controlled trial]/lim OR [systematic review]/lim)
23
CINAHL
S1 TI ( neoplasm OR cancer OR tumor OR tumour ) OR AB ( neoplasm OR cancer OR
tumor OR tumour )
105935
S2 TI pain OR AB pain 77289
S3
Diamorphine OR Dihydrocodeine OR Oxymorphone OR Tapentadol hydrochloride
OR Nalbuphine 241
S4 (Diamorphine OR Dihydrocodeine OR Oxymorphone OR Tapentadol hydrochloride
OR Nalbuphine) and (S1 and S2 and S3)
17
BIOSIS
#1 Topic=(Diamorphine OR Dihydrocodeine OR Oxymorphone OR Tapentadol hydrochloride OR Nalbuphine) Databases=BIOSIS Previews Timespan=All Years Lemmatization=On
1,822
# 2 Title=(neoplasm OR cancer OR tumor OR tumour) Databases=BIOSIS Previews Timespan=All Years Lemmatization=On
719,688
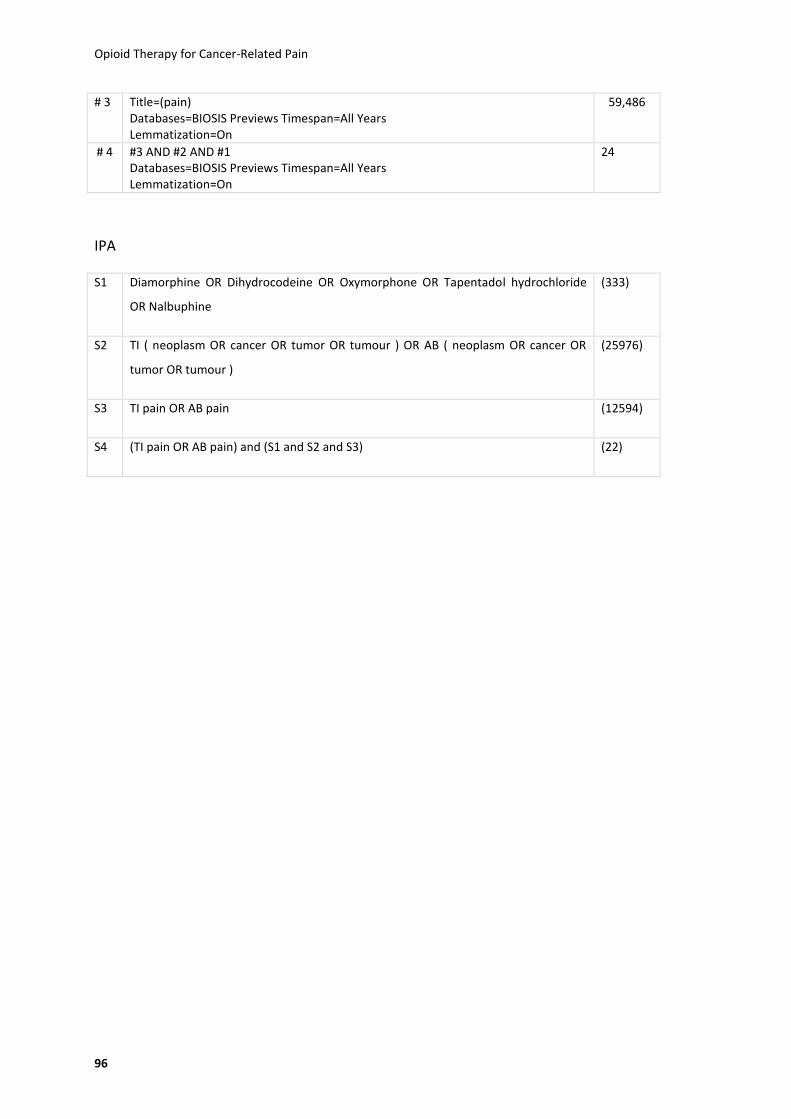
Opioid Therapy for Cancer-Related Pain
96
# 3 Title=(pain) Databases=BIOSIS Previews Timespan=All Years Lemmatization=On
59,486
# 4 #3 AND #2 AND #1 Databases=BIOSIS Previews Timespan=All Years Lemmatization=On
24
IPA
S1 Diamorphine OR Dihydrocodeine OR Oxymorphone OR Tapentadol hydrochloride
OR Nalbuphine
(333)
S2 TI ( neoplasm OR cancer OR tumor OR tumour ) OR AB ( neoplasm OR cancer OR
tumor OR tumour )
(25976)
S3 TI pain OR AB pain (12594)
S4 (TI pain OR AB pain) and (S1 and S2 and S3) (22)
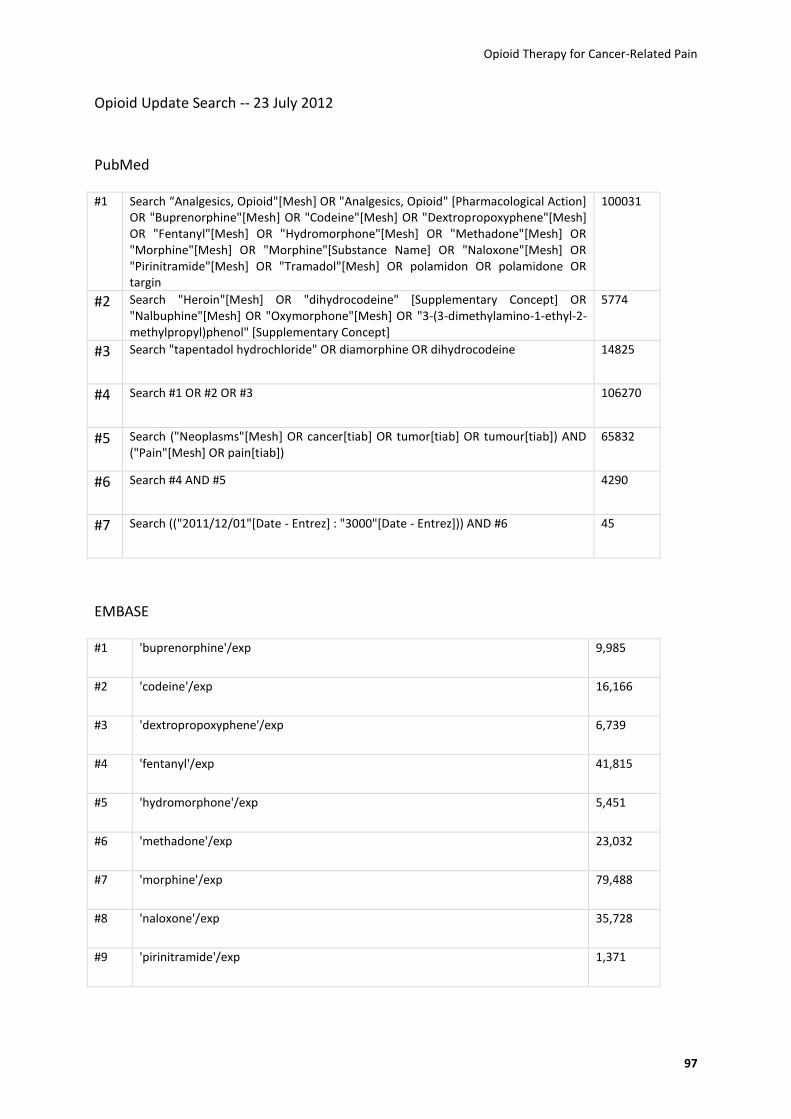
Opioid Therapy for Cancer-Related Pain
97
Opioid Update Search -- 23 July 2012
PubMed
#1 Search “Analgesics, Opioid"[Mesh] OR "Analgesics, Opioid" [Pharmacological Action] OR "Buprenorphine"[Mesh] OR "Codeine"[Mesh] OR "Dextropropoxyphene"[Mesh] OR "Fentanyl"[Mesh] OR "Hydromorphone"[Mesh] OR "Methadone"[Mesh] OR "Morphine"[Mesh] OR "Morphine"[Substance Name] OR "Naloxone"[Mesh] OR "Pirinitramide"[Mesh] OR "Tramadol"[Mesh] OR polamidon OR polamidone OR targin
100031
#2 Search "Heroin"[Mesh] OR "dihydrocodeine" [Supplementary Concept] OR "Nalbuphine"[Mesh] OR "Oxymorphone"[Mesh] OR "3-(3-dimethylamino-1-ethyl-2-methylpropyl)phenol" [Supplementary Concept]
5774
#3 Search "tapentadol hydrochloride" OR diamorphine OR dihydrocodeine 14825
#4 Search #1 OR #2 OR #3 106270
#5 Search ("Neoplasms"[Mesh] OR cancer[tiab] OR tumor[tiab] OR tumour[tiab]) AND ("Pain"[Mesh] OR pain[tiab])
65832
#6 Search #4 AND #5 4290
#7 Search (("2011/12/01"[Date - Entrez] : "3000"[Date - Entrez])) AND #6 45
EMBASE
#1 'buprenorphine'/exp 9,985
#2 'codeine'/exp 16,166
#3 'dextropropoxyphene'/exp 6,739
#4 'fentanyl'/exp 41,815
#5 'hydromorphone'/exp 5,451
#6 'methadone'/exp 23,032
#7 'morphine'/exp 79,488
#8 'naloxone'/exp 35,728
#9 'pirinitramide'/exp 1,371
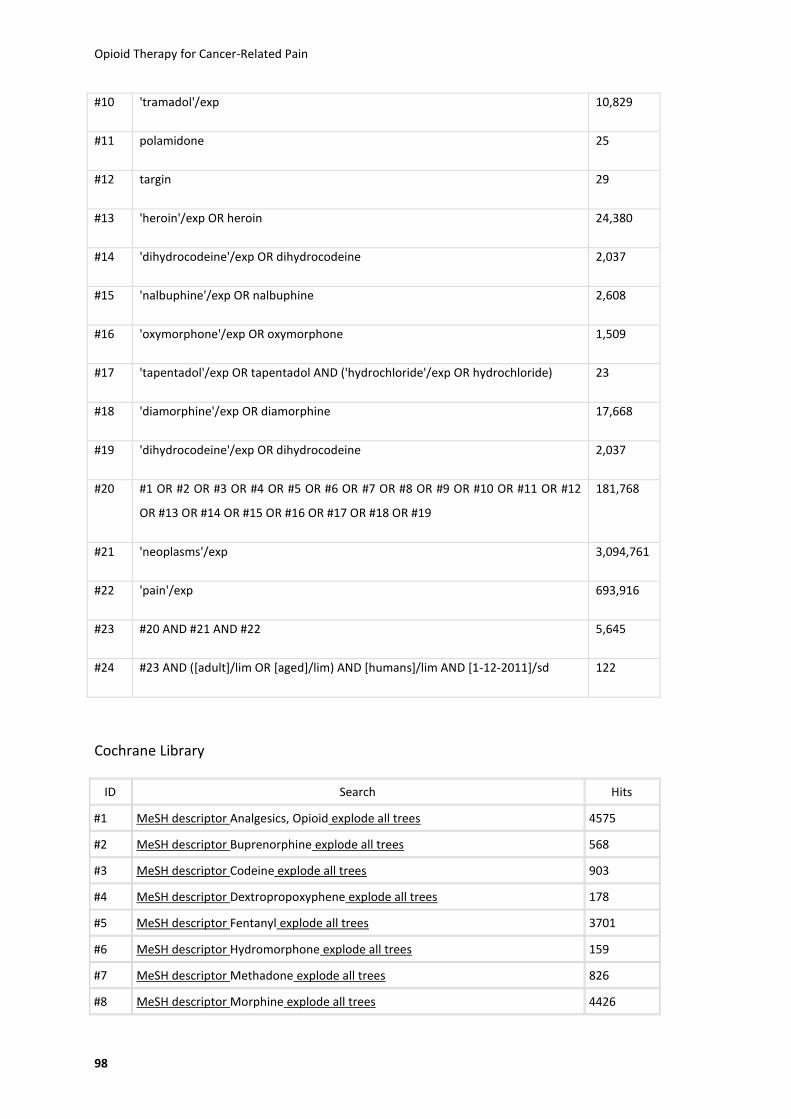
Opioid Therapy for Cancer-Related Pain
98
#10 'tramadol'/exp 10,829
#11 polamidone 25
#12 targin 29
#13 'heroin'/exp OR heroin 24,380
#14 'dihydrocodeine'/exp OR dihydrocodeine 2,037
#15 'nalbuphine'/exp OR nalbuphine 2,608
#16 'oxymorphone'/exp OR oxymorphone 1,509
#17 'tapentadol'/exp OR tapentadol AND ('hydrochloride'/exp OR hydrochloride) 23
#18 'diamorphine'/exp OR diamorphine 17,668
#19 'dihydrocodeine'/exp OR dihydrocodeine 2,037
#20 #1 OR #2 OR #3 OR #4 OR #5 OR #6 OR #7 OR #8 OR #9 OR #10 OR #11 OR #12
OR #13 OR #14 OR #15 OR #16 OR #17 OR #18 OR #19
181,768
#21 'neoplasms'/exp 3,094,761
#22 'pain'/exp 693,916
#23 #20 AND #21 AND #22 5,645
#24 #23 AND ([adult]/lim OR [aged]/lim) AND [humans]/lim AND [1-12-2011]/sd 122
Cochrane Library
ID Search Hits
#1 MeSH descriptor Analgesics, Opioid explode all trees 4575
#2 MeSH descriptor Buprenorphine explode all trees 568
#3 MeSH descriptor Codeine explode all trees 903
#4 MeSH descriptor Dextropropoxyphene explode all trees 178
#5 MeSH descriptor Fentanyl explode all trees 3701
#6 MeSH descriptor Hydromorphone explode all trees 159
#7 MeSH descriptor Methadone explode all trees 826
#8 MeSH descriptor Morphine explode all trees 4426

Opioid Therapy for Cancer-Related Pain
99
#9 MeSH descriptor Naloxone explode all trees 1414
#10 MeSH descriptor Pirinitramide explode all trees 87
#11 MeSH descriptor Tramadol explode all trees 621
#12 polamidon OR polamidone OR targin 2
#13 MeSH descriptor Heroin explode all trees 237
#14 MeSH descriptor Nalbuphine explode all trees 177
#15 MeSH descriptor Oxymorphone explode all trees 42
#16 Diamorphine OR Dihydrocodeine OR "Tapentadol hydrochloride" 394
#17 (#1 OR #2 OR #3 OR #4 OR #5 OR #6 OR #7 OR #8 OR #9 OR #10 OR #11 OR #12 OR #13 OR #14 OR #15 OR #16)
11625
#18 MeSH descriptor Neoplasms explode all trees 43907
#19 (cancer OR tumor OR tumour):ti,ab,kw 55964
#20 MeSH descriptor Pain explode all trees 29079
#21 (pain):ti,ab,kw 55147
#22 (#17 AND ( ( #18 OR #19 ) AND ( #20 OR #21 ) )) 548
#23 (#22), in 2012 2
IPA/CINAHL
S11 S10 Limiters - Published Date from: 20111201-20120831; Human 21
S10 S3 and S8 and S9 1683
S9 pain 121133
S8 S4 or S5 or S6 or S7 167507
S7 Tumour 29676
S6 Tumor 49148
S5 Cancer 132147
S4 Neoplasm 46264
S3 S1 or S2 16538
S2 Diamorphine OR Dihydrocodeine OR Oxymorphone OR Tapentadol hydrochloride OR Nalbuphine
584
S1 buprenorphine OR codeine OR dextropropoxyphene OR fentanyl OR hydromorphone OR methadone OR morphine OR naloxone OR pirinitramide OR tramadol OR polamidon OR polamidone OR targin
16235

Opioid Therapy for Cancer-Related Pain
100
BIOSIS
#13 #12 Databases=BIOSIS Previews Timespan=2012 Lemmatization=On
47
#12 #11 AND #8 AND #5 Databases=BIOSIS Previews Timespan=All Years Lemmatization=On
2,297
#11 #10 OR #9 Databases=BIOSIS Previews Timespan=All Years Lemmatization=On
223,754
#10 TS=(pain) Databases=BIOSIS Previews Timespan=All Years Lemmatization=On
223,754
#9 TI=(pain) Databases=BIOSIS Previews Timespan=All Years Lemmatization=On
62,930
#8 #7 OR #6 Databases=BIOSIS Previews Timespan=All Years Lemmatization=On
2,781,310
#7 TS=(neoplasm OR cancer OR tumor OR tumour) Databases=BIOSIS Previews Timespan=All Years Lemmatization=On
2,781,310
#6 TI=(neoplasm OR cancer OR tumor OR tumour) Databases=BIOSIS Previews Timespan=All Years Lemmatization=On
771,702
#5 #4 OR #3 OR #2 OR #1 Databases=BIOSIS Previews Timespan=All Years Lemmatization=On
95,234
#4
TI=(Diamorphine OR Dihydrocodeine OR Oxymorphone OR Tapentadol hydrochloride OR Nalbuphine) Databases=BIOSIS Previews Timespan=All Years Lemmatization=On
720
#3
TS=(Diamorphine OR Dihydrocodeine OR Oxymorphone OR Tapentadol hydrochloride OR Nalbuphine) Databases=BIOSIS Previews Timespan=All Years Lemmatization=On
1,901
#2
TI=(buprenorphine OR codeine OR dextropropoxyphene OR fentanyl OR hydromorphone OR methadone OR morphine OR naloxone OR pirinitramide OR tramadol OR polamidon OR polamidone OR targin) Databases=BIOSIS Previews Timespan=All Years Lemmatization=On
42,757
#1
TS=(buprenorphine OR codeine OR dextropropoxyphene OR fentanyl OR hydromorphone OR methadone OR morphine OR naloxone OR pirinitramide OR tramadol OR polamidon OR polamidone OR targin) Databases=BIOSIS Previews Timespan=All Years Lemmatization=On
94,550

Opioid Therapy for Cancer-Related Pain
101
Appendix B
Appendix-Table 1: Pharmaceutical Companies that were Contacted.
Marketing Authorization Holder Active Ingredient Country Received
Reply
ACINO AG Transdermal Buprenorphine Transdermal Fentanyl Oxycodone
Germany No
Actavis Morphine US Yes
Actavis Deutschland GmbH & Co Morphine Germany Yes
Actavis UK Ltd Transdermal Fentanyl Tramadol
UK No
Amdipharm Plc Morphine UK Yes
AWD.pharma GmbH & Co.
Hydromorphone Morphine Transdermal Buprenorphine Transdermal Fentanyl Tramadol
Germany Yes
BC Biochemie Pharma GmbH Morphine Germany No
Beechmere Pharmaceuticals Ltd Tramadol UK No
BERAGENA Arzneimittel GmbH/ Pharma Westen GmbH/ Grünenthal GmbH/ EMRA-MED Arzneimittel GmbH/ AxiCorp Pharma GmbH/ EurimPharm Arzneimittel GmbH/ Pharma Gerke Arzneimittelvertriebs GmbH/ kohlpharma GmbH
Tramadol Germany No
betapharm Arzneimittel GmbH
Transdermal Fentanyl Hydromorphone Morphine Oxycodone Tramadol
Germany No
Chiesi Limited Tramadol UK Yes
CIPHER PHARMS INC Tramadol US No
Dallas Burston Ashbourne Ltd Transdermal Fentanyl UK No
Endo Pharma Oxymorphone US No
Ethypharm Morphine Austria No
Ethypharm Morphine France No
Ethypharm Morphine Tramadol
Germany No
EurimPharm Arzneimittel GmbH Tramadol Germany No
EurimPharm Arzneimittel GmbH/ Mundipharma GmbH/ EurimPharm Arzneimittel GmbH
Tramadol Germany No
G. L. Pharma GmbH Morphine Oxycodone Dihydrocodeine
Austria Yes
Gebro Pharma AG Tramadol Switzerland No
GlaxoSmithKline AG Morphine Switzerland No
GlaxoSmithKline GmbH & Co. Morphine Germany Yes
GlaxoSmithKline Pharma GmbH Morphine Austria Yes
GRUENENTHAL GMBH Tramadol Austria No
Grünenthal GmbH
Transdermal Buprenorphine Morphine Tapentadol hydrochloride Tramadol
Germany No

Opioid Therapy for Cancer-Related Pain
102
Marketing Authorization Holder Active Ingredient Country Received
Reply
Grünenthal Ltd Tapentadol hydrochloride Tramadol
UK No
Grünenthal Pharma AG Transdermal Buprenorphine Tramadol
Switzerland No
Halvepharm AG Morphine Switzerland No
Helm AG Transdermal Fentanyl Germany Yes
Hennig Arzneimittel GmbH & Co.KG Transdermal Fentanyl Germany Yes
Hexal AG Transdermal Fentanyl Austria No
HEXAL AG Hydromorphone Morphine Oxycodone
Germany Yes
Janssen - Cilag Pharma GmbH Hydromorphone Austria Yes
Janssen - Cilag Pharma GmbH Hydromorphone Germany No
Janssen Pharmaceuticals Tapentadol hydrochloride US No
Janssen-Cilag AG Transdermal Fentanyl Hydromorphone
Switzerland No
Janssen-Cilag Ltd Fentanyl UK No
Juta Pharma GmbH Morphine Tramadol
Germany Yes
King Pharms Morphine Morphine and naltrexone
US No
kohlpharma GmbH Dihydrocodeine Germany Yes
Krewel Meuselbach GmbH Transdermal Fentanyl Morphine Tramadol
Germany No
LABOPHARM EUROPE LTD, Tramadol Ireland Yes
Lannacher Heilmittel GmbH Morphine Tramadol
Austria No
LAVIPHARM S.A. Transdermal Fentanyl Greece No
Libra-Pharm GmbH Transdermal Buprenorphine Tramadol
Germany Yes
COVIDIEN Hydromorphone US No
MEDA Pharma GmbH Tramadol Switzerland Yes
MEDA Pharma GmbH & Co. KG Tramadol Germany No
Meda Pharmaceuticals Tramadol UK No
medac Gesellschaft für klinische Spezialpräparate mbH
Morphine Germany Yes
Merck Sharp & Dohme Limited Tramadol UK Yes
mibe GmbH Arzneimittel Transdermal Fentanyl Germany No
Morningside Livery Tramadol UK No
MUNDIPHARMA GMBH
Dihydrocodeine Hydromorphone Morphine Oxycodone Oxycodone + naloxone Tramadol
Austria Yes
Mundipharma GmbH
Dihydrocodeine Hydromorphone Morphine Oxycodone Oxycodone + naloxone Tramadol
Germany Yes

Opioid Therapy for Cancer-Related Pain
103
Marketing Authorization Holder Active Ingredient Country Received
Reply
Mundipharma GmbH/ PB Pharma GmbH Hydromorphone Germany Yes
Mundipharma Medical Company
Dihydrocodeine Hydromorphone Morphine Oxycodone Oxycodone + naloxone Tramadol
Switzerland No
Napp Pharmaceuticals Limited
Transdermal Buprenorphine Dihydrocodeine hydromorphone Morphine Oxycodone Oxycodone + naloxone
UK No
NYCOMED DANMARK A/S, DK-ROSKILDE Transdermal Fentanyl Denmark No
Nycomed GmbH Transdermal Fentanyl Germany Yes
Nycomed Pharma AG Transdermal Fentanyl Switzerland No
Nycomed UK Ltd Transdermal Fentanyl UK Yes
Janssen Pharmaceuticals, Inc. Transdermal Fentanyl US No
Pfizer GmbH Morphine Germany No
PHARBIL PHARMA GMBH Hydromorphone Germany Yes
Pharmachemie B.V. Morphine Austria No
Purdue Pharma
Transdermal Buprenorphine Hydromorphone Morphine Oxycodone Tramadol
US Yes
Riemser Arzneimittel AG Transdermal Fentanyl Germany Yes
SMB TECHNOLOGY SA Tramadol Belgium Yes
Stadapharm GmbH
Transdermal Fentanyl Hydromorphone Morphine Oxycodone Tramadol
Germany Yes
TAD Pharma GmbH Transdermal Fentanyl Tramadol
Germany Yes
TEMMLER-PHARMA GMBH Tramadol Germany Yes
Teva Uk Limited Morphine UK No
Tillomed Laboratories Ltd Transdermal Fentanyl UK No
VALEANT INTL Tramadol US No
VEMEDIA MANUFACTURING B.V., Tramadol Netherlands No
Xanodyne Pharms Morphine US Yes
Yes Pharmaceutical Development Oxycodone Germany Yes
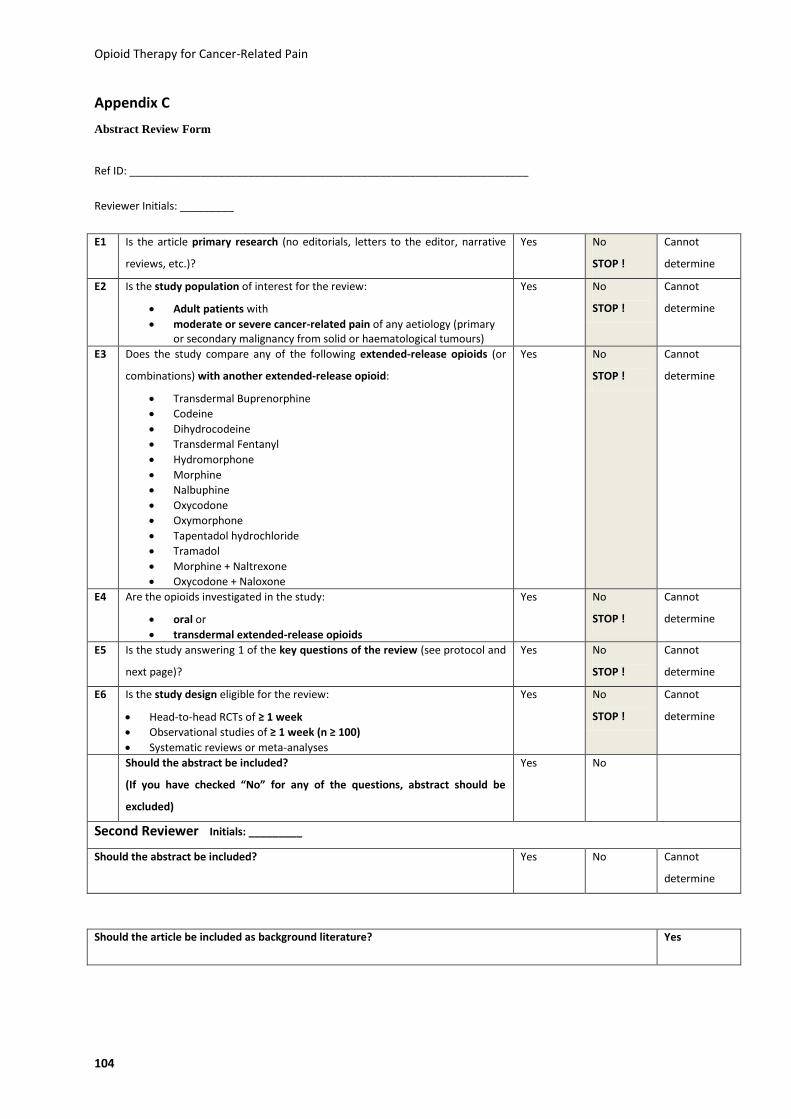
Opioid Therapy for Cancer-Related Pain
104
Appendix C
Abstract Review Form
Ref ID: ___________________________________________________________________
Reviewer Initials: _________
E1 Is the article primary research (no editorials, letters to the editor, narrative
reviews, etc.)?
Yes No
STOP !
Cannot
determine
E2 Is the study population of interest for the review:
Adult patients with
moderate or severe cancer-related pain of any aetiology (primary or secondary malignancy from solid or haematological tumours)
Yes No
STOP !
Cannot
determine
E3 Does the study compare any of the following extended-release opioids (or
combinations) with another extended-release opioid:
Transdermal Buprenorphine
Codeine
Dihydrocodeine
Transdermal Fentanyl
Hydromorphone
Morphine
Nalbuphine
Oxycodone
Oxymorphone
Tapentadol hydrochloride
Tramadol
Morphine + Naltrexone
Oxycodone + Naloxone
Yes No
STOP !
Cannot
determine
E4 Are the opioids investigated in the study:
oral or
transdermal extended-release opioids
Yes No
STOP !
Cannot
determine
E5 Is the study answering 1 of the key questions of the review (see protocol and
next page)?
Yes No
STOP !
Cannot
determine
E6 Is the study design eligible for the review:
Head-to-head RCTs of ≥ 1 week
Observational studies of ≥ 1 week (n ≥ 100)
Systematic reviews or meta-analyses
Yes No
STOP !
Cannot
determine
Should the abstract be included?
(If you have checked “No” for any of the questions, abstract should be
excluded)
Yes No
Second Reviewer Initials: _________
Should the abstract be included? Yes No Cannot
determine
Should the article be included as background literature? Yes
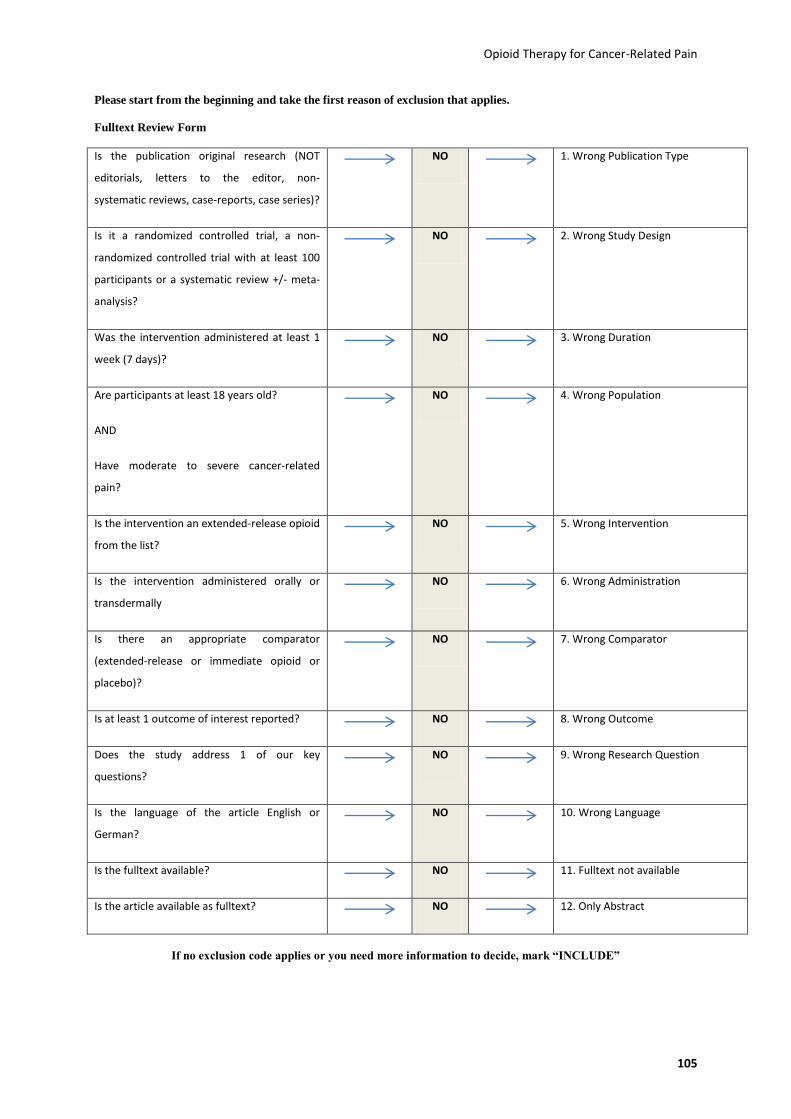
Opioid Therapy for Cancer-Related Pain
105
Please start from the beginning and take the first reason of exclusion that applies.
Fulltext Review Form
Is the publication original research (NOT
editorials, letters to the editor, non-
systematic reviews, case-reports, case series)?
NO 1. Wrong Publication Type
Is it a randomized controlled trial, a non-
randomized controlled trial with at least 100
participants or a systematic review +/- meta-
analysis?
NO 2. Wrong Study Design
Was the intervention administered at least 1
week (7 days)?
NO 3. Wrong Duration
Are participants at least 18 years old?
AND
Have moderate to severe cancer-related
pain?
NO 4. Wrong Population
Is the intervention an extended-release opioid
from the list?
NO 5. Wrong Intervention
Is the intervention administered orally or
transdermally
NO 6. Wrong Administration
Is there an appropriate comparator
(extended-release or immediate opioid or
placebo)?
NO 7. Wrong Comparator
Is at least 1 outcome of interest reported? NO 8. Wrong Outcome
Does the study address 1 of our key
questions?
NO 9. Wrong Research Question
Is the language of the article English or
German?
NO 10. Wrong Language
Is the fulltext available? NO 11. Fulltext not available
Is the article available as fulltext? NO 12. Only Abstract
If no exclusion code applies or you need more information to decide, mark “INCLUDE”

Opioid Therapy for Cancer-Related Pain
106
Appendix D
Appendix-Table 2: High Risk of Bias Studies and Reasons for the Poor Quality Rating.
Study Design Reasons for High Risk of Bias Rating
Ahmedzai et al., 2012(41) RCT Pseudo-random number generator for randomization; partial ITT analysis; 28% attrition (27% and 28%)
Hagen and Babul, 1997(40)
RCT 30% attrition; no ITT analysis; unclear risk for selection bias
Hanna et al., 2008(42) RCT 33.5% attrition (39.4% and 27.7%); unclear risk of selection bias
Mercadante et al., 2008(43)
RCT Non-blinded study; 35.2% attrition (38.9% and 30.6%); no ITT analysis
Okamoto et al., 2010(47) Retrospective cohort study
Retrospective design; no information on duration of follow-up, opioid doses, blinding, outcome measures
van Seventer et al., 2003(44)
RCT Non-blinded study; 39% attrition (55% and 24%); no ITT analysis
Abbreviations: ITT, intent to treat analysis; RCT, randomized controlled trial.
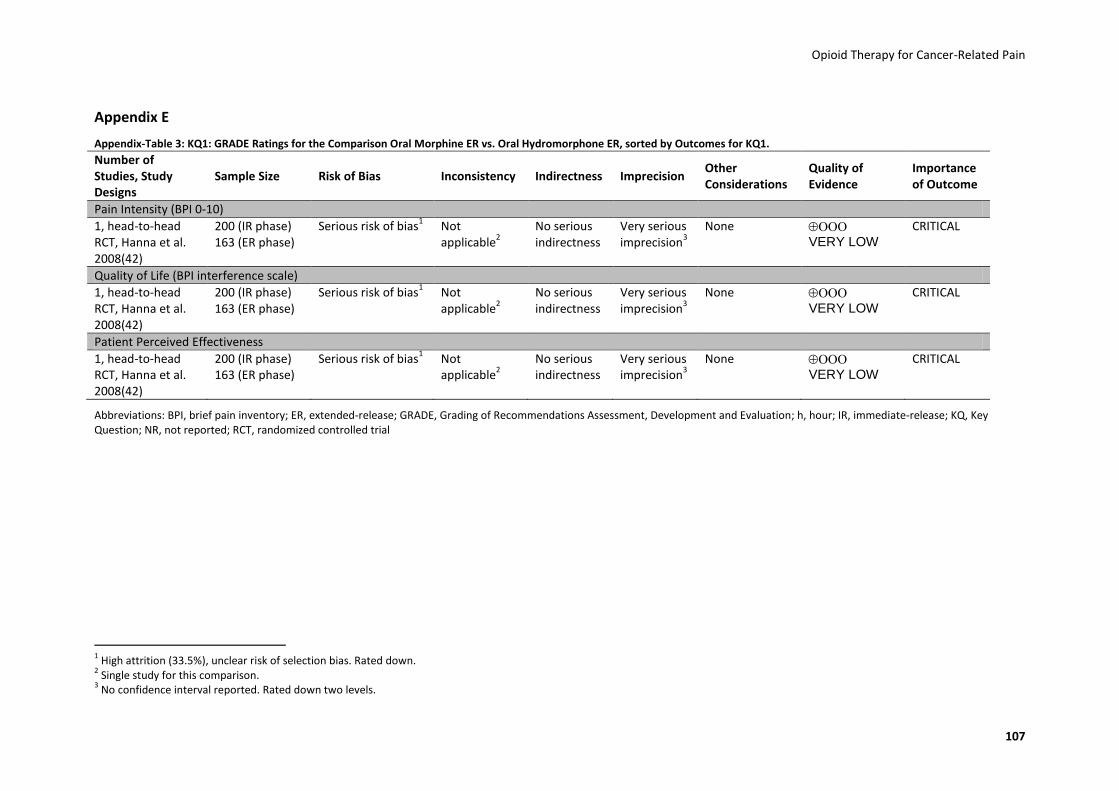
Opioid Therapy for Cancer-Related Pain
107
Appendix E
Appendix-Table 3: KQ1: GRADE Ratings for the Comparison Oral Morphine ER vs. Oral Hydromorphone ER, sorted by Outcomes for KQ1.
Number of Studies, Study Designs
Sample Size Risk of Bias Inconsistency Indirectness Imprecision Other Considerations
Quality of Evidence
Importance of Outcome
Pain Intensity (BPI 0-10)
1, head-to-head RCT, Hanna et al. 2008(42)
200 (IR phase) 163 (ER phase)
Serious risk of bias1 Not
applicable2
No serious indirectness
Very serious imprecision
3
None VERY LOW
CRITICAL
Quality of Life (BPI interference scale)
1, head-to-head RCT, Hanna et al. 2008(42)
200 (IR phase) 163 (ER phase)
Serious risk of bias1 Not
applicable2
No serious indirectness
Very serious imprecision
3
None VERY LOW
CRITICAL
Patient Perceived Effectiveness
1, head-to-head RCT, Hanna et al. 2008(42)
200 (IR phase) 163 (ER phase)
Serious risk of bias1 Not
applicable2
No serious indirectness
Very serious imprecision
3
None VERY LOW
CRITICAL
Abbreviations: BPI, brief pain inventory; ER, extended-release; GRADE, Grading of Recommendations Assessment, Development and Evaluation; h, hour; IR, immediate-release; KQ, Key Question; NR, not reported; RCT, randomized controlled trial
1 High attrition (33.5%), unclear risk of selection bias. Rated down.
2 Single study for this comparison.
3 No confidence interval reported. Rated down two levels.
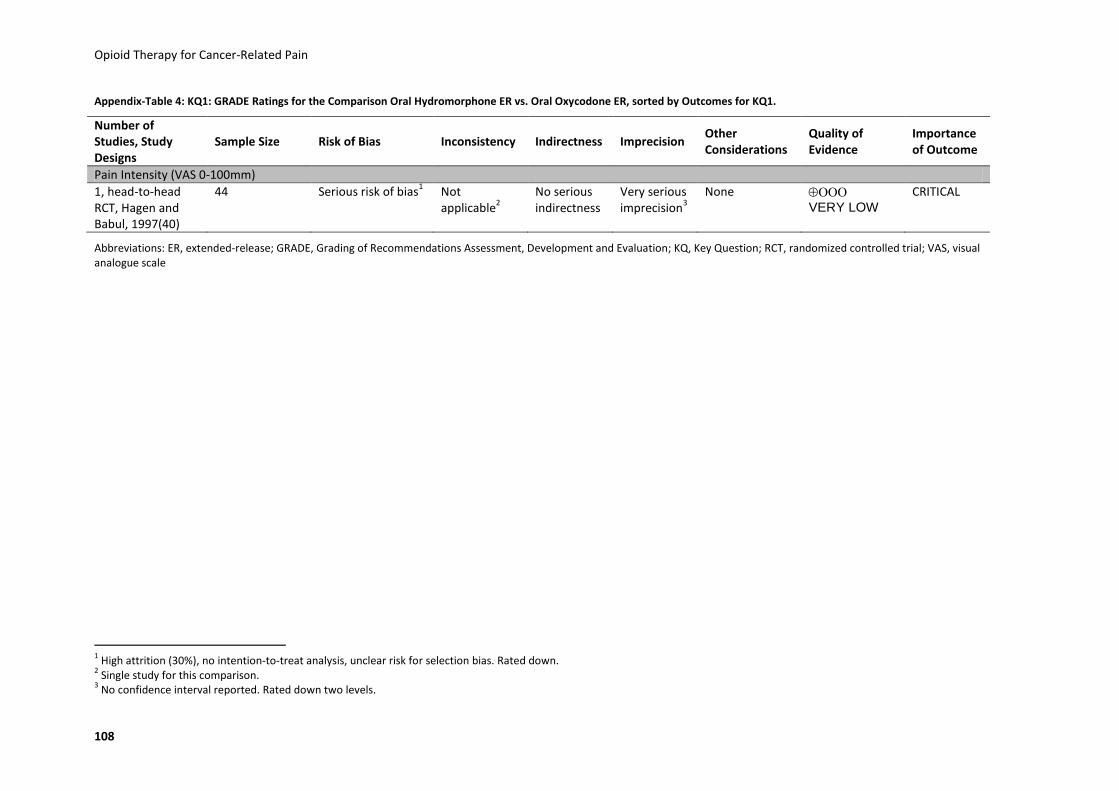
Opioid Therapy for Cancer-Related Pain
108
Appendix-Table 4: KQ1: GRADE Ratings for the Comparison Oral Hydromorphone ER vs. Oral Oxycodone ER, sorted by Outcomes for KQ1.
Number of Studies, Study Designs
Sample Size Risk of Bias Inconsistency Indirectness Imprecision Other Considerations
Quality of Evidence
Importance of Outcome
Pain Intensity (VAS 0-100mm)
1, head-to-head RCT, Hagen and Babul, 1997(40)
44 Serious risk of bias1 Not
applicable2
No serious indirectness
Very serious imprecision
3
None VERY LOW
CRITICAL
Abbreviations: ER, extended-release; GRADE, Grading of Recommendations Assessment, Development and Evaluation; KQ, Key Question; RCT, randomized controlled trial; VAS, visual analogue scale
1 High attrition (30%), no intention-to-treat analysis, unclear risk for selection bias. Rated down.
2 Single study for this comparison.
3 No confidence interval reported. Rated down two levels.
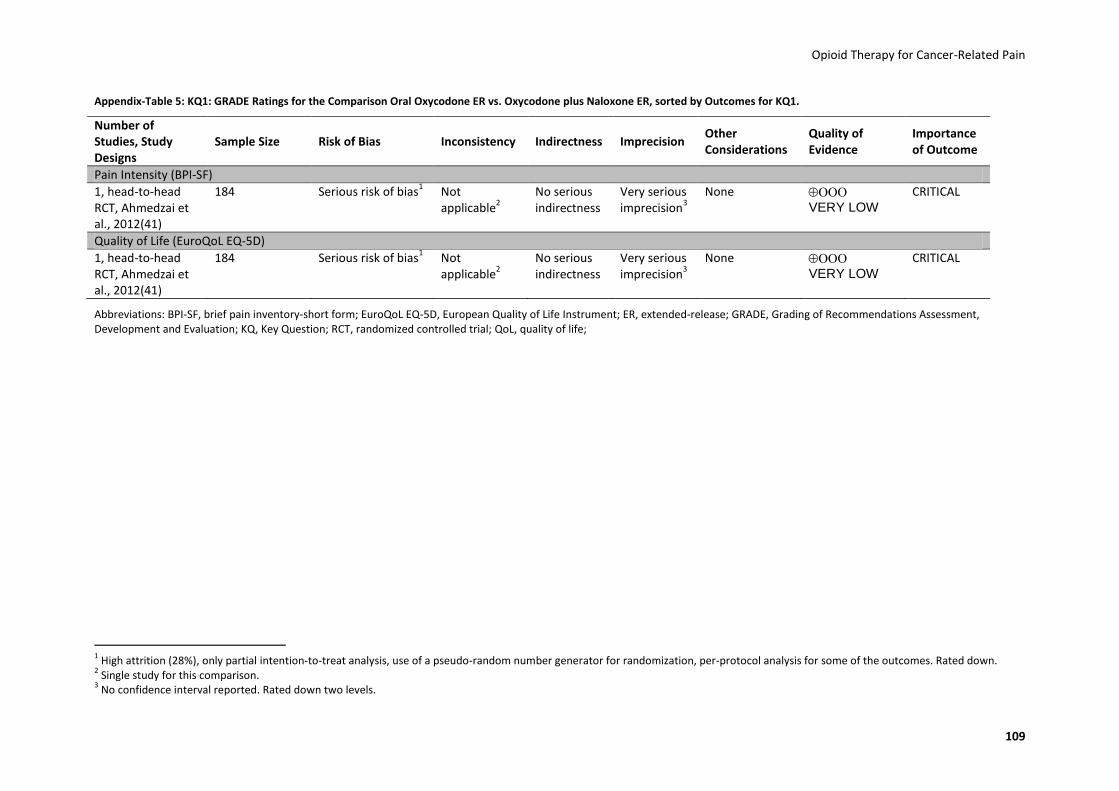
Opioid Therapy for Cancer-Related Pain
109
Appendix-Table 5: KQ1: GRADE Ratings for the Comparison Oral Oxycodone ER vs. Oxycodone plus Naloxone ER, sorted by Outcomes for KQ1.
Number of Studies, Study Designs
Sample Size Risk of Bias Inconsistency Indirectness Imprecision Other Considerations
Quality of Evidence
Importance of Outcome
Pain Intensity (BPI-SF)
1, head-to-head RCT, Ahmedzai et al., 2012(41)
184 Serious risk of bias1 Not
applicable2
No serious indirectness
Very serious imprecision
3
None VERY LOW
CRITICAL
Quality of Life (EuroQoL EQ-5D)
1, head-to-head RCT, Ahmedzai et al., 2012(41)
184 Serious risk of bias1 Not
applicable2
No serious indirectness
Very serious imprecision
3
None VERY LOW
CRITICAL
Abbreviations: BPI-SF, brief pain inventory-short form; EuroQoL EQ-5D, European Quality of Life Instrument; ER, extended-release; GRADE, Grading of Recommendations Assessment, Development and Evaluation; KQ, Key Question; RCT, randomized controlled trial; QoL, quality of life;
1 High attrition (28%), only partial intention-to-treat analysis, use of a pseudo-random number generator for randomization, per-protocol analysis for some of the outcomes. Rated down.
2 Single study for this comparison.
3 No confidence interval reported. Rated down two levels.

Opioid Therapy for Cancer-Related Pain
110
Appendix-Table 6: KQ2: GRADE Ratings for the Comparison Oral Morphine ER vs. Oral Hydromorphone ER, sorted by Outcomes for KQ2.
Number of Studies, Study Designs
Sample Size Risk of Bias Inconsistency Indirectness Imprecision Other Considerations
Quality of Evidence
Importance of Outcome
Serious Adverse Events
1, head-to-head RCT, Hanna et al. 2008(42)
200 (IR phase) 163 (ER phase)
Serious risk of bias1 Not
applicable2
No serious indirectness
Very serious imprecision
3
None VERY LOW
CRITICAL
Constipation
1, head-to-head RCT, Hanna et al. 2008(42)
200 (IR phase) 163 (ER phase)
Serious risk of bias1 Serious
inconsistency4
No serious indirectness
Very serious imprecision
5
None
VERY LOW
CRITICAL 1, prospective cohort study Wirz et al. 2008(45)
100 No serious risk of bias
6
Nausea and Vomiting
1, head-to-head RCT, Hanna et al. 2008(42)
200 (IR phase) 163 (ER phase)
Serious risk of bias1 Serious
inconsistency4
No serious indirectness
Very serious imprecision
5
None
VERY LOW
CRITICAL 1, prospective cohort study, Wirz et al. 2008(45)
100 No serious risk of bias
6
Abbreviations: ER, extended-release; GRADE, Grading of Recommendations Assessment, Development and Evaluation; IR, immediate-release; KQ, Key Question; RCT, randomized controlled trial;
1 High overall attrition for the IR phase (33.5%), unclear risk of selection bias. Rated down.
2 Single study for this comparison.
3 No confidence interval reported. Rated down two levels.
4 Different results according to different outcome measures in one observational study. Inconsistent results between RCT and observational study. Rated down.
5 No confidence interval reported. Rated down two levels.
6 Different time spans of using opioids before entering the study and lack of blinding of outcome assessment, lack of adjustment for confounding.

Opioid Therapy for Cancer-Related Pain
111
Appendix-Table 7: KQ2: GRADE Ratings for the Comparison Oral Morphine ER vs. Oral Oxycodone ER, sorted by Outcomes for KQ2.
Number of Studies, Study Designs
Sample Size Risk of Bias Inconsistency Indirectness Imprecision Other Considerations
Quality of Evidence
Importance of Outcome
Serious Adverse Events
1, retrospective cohort study, Hartung et al. 2007(48)
810 No serious risk of bias
1
Not applicable
2
No serious indirectness
Serious imprecision
3
None VERY LOW
CRITICAL
Constipation
1, retrospective cohort study, Hartung et al. 2007(48)
810 No serious risk of bias
1
Not applicable
2
No serious indirectness
Serious imprecision
3
None VERY LOW
CRITICAL
Nausea and Vomiting
1, retrospective cohort study, Okamoto et al., 2010(47, 48)
226 Very serious risk of bias
4
Not applicable
2
No serious indirectness
Serious imprecision
5
None VERY LOW
CRITICAL
Abbreviations: ER, extended-release; GRADE, Grading of Recommendations Assessment, Development and Evaluation; KQ, Key Question;
1 No blinding of outcome assessment, no valid and reliable outcome measures.
2 Single study for this comparison.
3 Event rate below optimal information size; confidence intervals cross clinically important thresholds. Rated down.
4 Exclusion of participants, no comment about time to follow-up in all study groups, no information about opioid-doses. Rated down two levels.
5 Event rate below optimal information size; No confidence interval reported; Rated down.

Opioid Therapy for Cancer-Related Pain
112
Appendix-Table 8: KQ2: GRADE Ratings for the Comparison Oral Morphine ER vs. Transdermal Fentanyl ER, sorted by Outcomes For KQ2.
Number of Studies, Study Designs
Sample Size
Risk of Bias Inconsistency Indirectness Imprecision Other Considerations
Quality of Evidence
Importance of Outcome
Serious Adverse Events
1, head-to head RCT(44) van Seventer et al. 2003(44)
131 Serious risk of bias1 No serious
inconsistency No serious indirectness
Serious imprecision
2
None
LOW
CRITICAL 1, retrospective cohort study, Hartung et al. 2007(48)
778 No serious risk of bias
3
Constipation
2, head-to-head RCT, Mercadante et al. 2008(43), van Seventer et al. 2003(44)
203 Serious risk of bias4 No serious
inconsistency No serious indirectness
Serious imprecision
5
None
LOW
CRITICAL 1, retrospective cohort study, Hartung et al. 2007(48)
778 No serious risk of bias
3
Nausea and Vomiting
2, head-to-head RCT, Mercadante et al. 2008(43), van Seventer et al. 2003(44)
203 Serious risk of bias4 Serious
inconsistency6
No serious indirectness
Very serious imprecision
7
None
VERY LOW
CRITICAL 1, retrospective cohort study, Okamoto et al. 2010(47)
194 Very serious risk of bias
8
Abbreviations: ER, extended-release; GRADE, Grading of Recommendations Assessment, Development and Evaluation; KQ, Key Question; RCT, randomized controlled trial;
1 Lack of blinding of participants and personnel as well as outcomes assessors, high attrition (van Seventer (48) et al.: 39%) and lack of intention-to-treat-analyses. Rated down.
2 Studies do not meet optimal information size; wide confidence intervals for all estimates, Rated down.
3 No blinding of outcome assessment, no valid and reliable outcome measures.
4 Lack of blinding of participants and personnel as well as outcomes assessors, high attrition (van Seventer et al. 44. van Seventer R, Smit JM, Schipper RM, Wicks MA, Zuurmond WW.
Comparison of TTS-fentanyl with sustained-release oral morphine in the treatment of patients not using opioids for mild-to-moderate pain. Curr Med Res Opin. 2003;19(6):457-69. Epub 2003/11/05.: 39%; Mercadante et al. 28: 35,2%) and lack of intention-to-treat-analyses. Rated down. 5 No confidence interval reported for RCTs; Confidence intervals for cohort study cross clinically important thresholds. Rated down.
6 Inconsistent results. Rated down.
7 Event rate below optimal information size; No confidence interval reported. Rated down two levels.
8 Exclusion of participants, No comment about time to follow-up in all study groups, no information about opioid-doses . Rated down two levels.
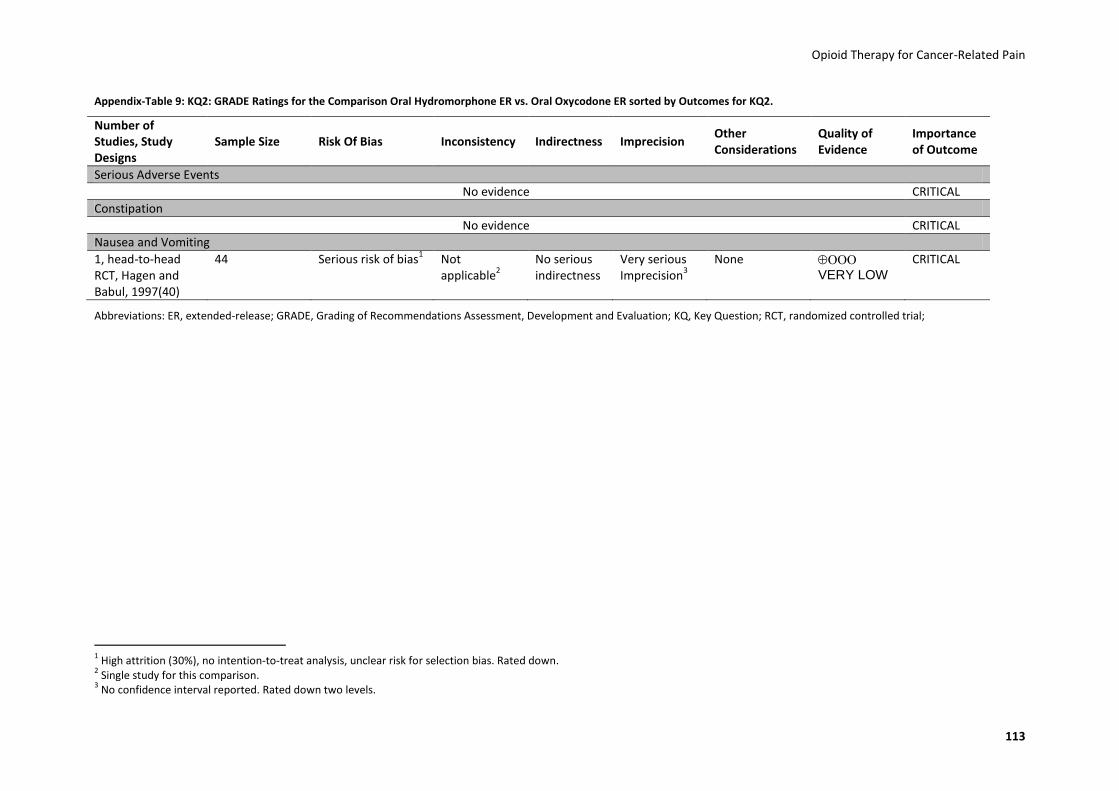
Opioid Therapy for Cancer-Related Pain
113
Appendix-Table 9: KQ2: GRADE Ratings for the Comparison Oral Hydromorphone ER vs. Oral Oxycodone ER sorted by Outcomes for KQ2.
Number of Studies, Study Designs
Sample Size Risk Of Bias Inconsistency Indirectness Imprecision Other Considerations
Quality of Evidence
Importance of Outcome
Serious Adverse Events
No evidence CRITICAL
Constipation
No evidence CRITICAL
Nausea and Vomiting
1, head-to-head RCT, Hagen and Babul, 1997(40)
44 Serious risk of bias1 Not
applicable2
No serious indirectness
Very serious Imprecision
3
None VERY LOW
CRITICAL
Abbreviations: ER, extended-release; GRADE, Grading of Recommendations Assessment, Development and Evaluation; KQ, Key Question; RCT, randomized controlled trial;
1 High attrition (30%), no intention-to-treat analysis, unclear risk for selection bias. Rated down.
2 Single study for this comparison.
3 No confidence interval reported. Rated down two levels.
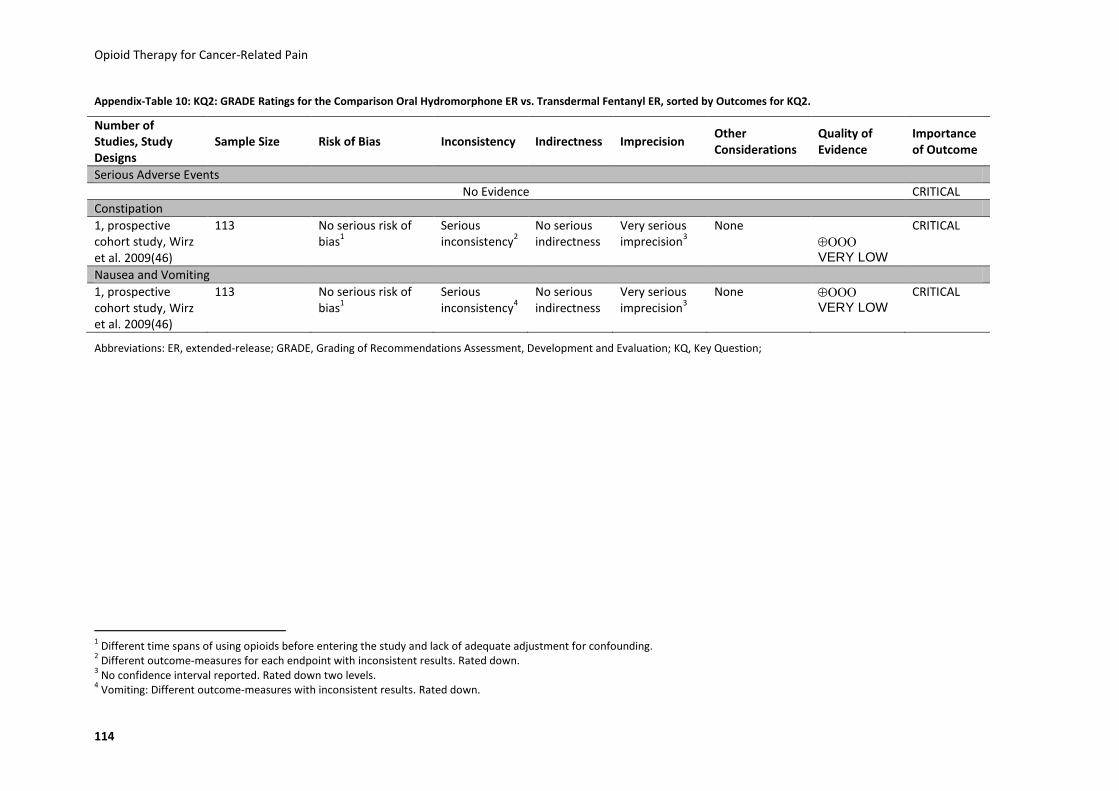
Opioid Therapy for Cancer-Related Pain
114
Appendix-Table 10: KQ2: GRADE Ratings for the Comparison Oral Hydromorphone ER vs. Transdermal Fentanyl ER, sorted by Outcomes for KQ2.
Number of Studies, Study Designs
Sample Size Risk of Bias Inconsistency Indirectness Imprecision Other Considerations
Quality of Evidence
Importance of Outcome
Serious Adverse Events
No Evidence CRITICAL
Constipation
1, prospective cohort study, Wirz et al. 2009(46)
113 No serious risk of bias
1
Serious inconsistency
2
No serious indirectness
Very serious imprecision
3
None
VERY LOW
CRITICAL
Nausea and Vomiting
1, prospective cohort study, Wirz et al. 2009(46)
113 No serious risk of bias
1
Serious inconsistency
4
No serious indirectness
Very serious imprecision
3
None VERY LOW
CRITICAL
Abbreviations: ER, extended-release; GRADE, Grading of Recommendations Assessment, Development and Evaluation; KQ, Key Question;
1 Different time spans of using opioids before entering the study and lack of adequate adjustment for confounding.
2 Different outcome-measures for each endpoint with inconsistent results. Rated down.
3 No confidence interval reported. Rated down two levels.
4 Vomiting: Different outcome-measures with inconsistent results. Rated down.

Opioid Therapy for Cancer-Related Pain
115
Appendix-Table 11: KQ2: GRADE Ratings for the Comparison Oral Hydromorphone ER vs. Transdermal Buprenorphine ER, sorted by Outcomes for KQ2.
Number of Studies, Study Designs
Sample size Risk of Bias Inconsistency Indirectness Imprecision Other Considerations
Quality of Evidence
Importance of Outcome
Serious Adverse Events
No Evidence CRITICAL
Constipation
1, prospective cohort study, Wirz et al. 2009 (46)
119 No serious risk of bias
1
Serious inconsistency
2
No serious indirectness
Very serious imprecision
3
None VERY LOW
CRITICAL
Nausea and Vomiting
1, prospective cohort study, Wirz et al. 2009 (46)
119 No serious risk of bias
1
Serious inconsistency
4
No serious indirectness
Very serious imprecision
3
None VERY LOW
CRITICAL
Abbreviations: ER, extended-release; GRADE, Grading of Recommendations Assessment, Development and Evaluation; KQ, Key Question;
1 Different time spans of using opioids before entering the study and lack of adequate adjustment for confounding.
2 Different outcome-measures for each endpoint with inconsistent results in one observational study. Rated down.
3 No confidence interval reported. Rated down two levels.
4 Vomiting: Different outcome-measures with inconsistent results. Rated down.

Opioid Therapy for Cancer-Related Pain
116
Appendix-Table 12: KQ2: GRADE Ratings for the Comparison Oral Oxycodone ER vs. Oral Oxycodone ER + Naloxone, sorted by Outcomes for KQ2.
Number of Studies, Study Designs
Sample Size Risk of Bias Inconsistency Indirectness Imprecision Other Considerations
Quality of Evidence
Importance of Outcome
Serious Adverse Events
1, head-to-head RCT, Ahmedzai et al., 2012(41)
184 Serious risk of bias1 Not
applicable2
No serious indirectness
Very serious Imprecision
3
None VERY LOW
CRITICAL
Constipation
1, head-to-head RCT, Ahmedzai et al., 2012(41)
184 Serious risk of bias1 Not
applicable2
No serious indirectness
Serious imprecision
4
None LOW
CRITICAL
Nausea and Vomiting
1, head-to-head RCT, Ahmedzai et al., 2012(41)
184 Serious risk of bias1 Not
applicable2
No serious indirectness
Very serious Imprecision
3
None VERY LOW
CRITICAL
Abbreviations: ER, extended-release; GRADE, Grading of Recommendations Assessment, Development and Evaluation; KQ, Key Question; RCT, randomized controlled trial;
1 Lack of random sequence generation and high attrition rates (27,7%) and only partial intention-to-treat analysis. Rated down.
2 Single study for this comparison.
3 No confidence interval reported. Rated down two levels.
4 Confidence interval for primary outcome cross clinically important thresholds. Rated down.
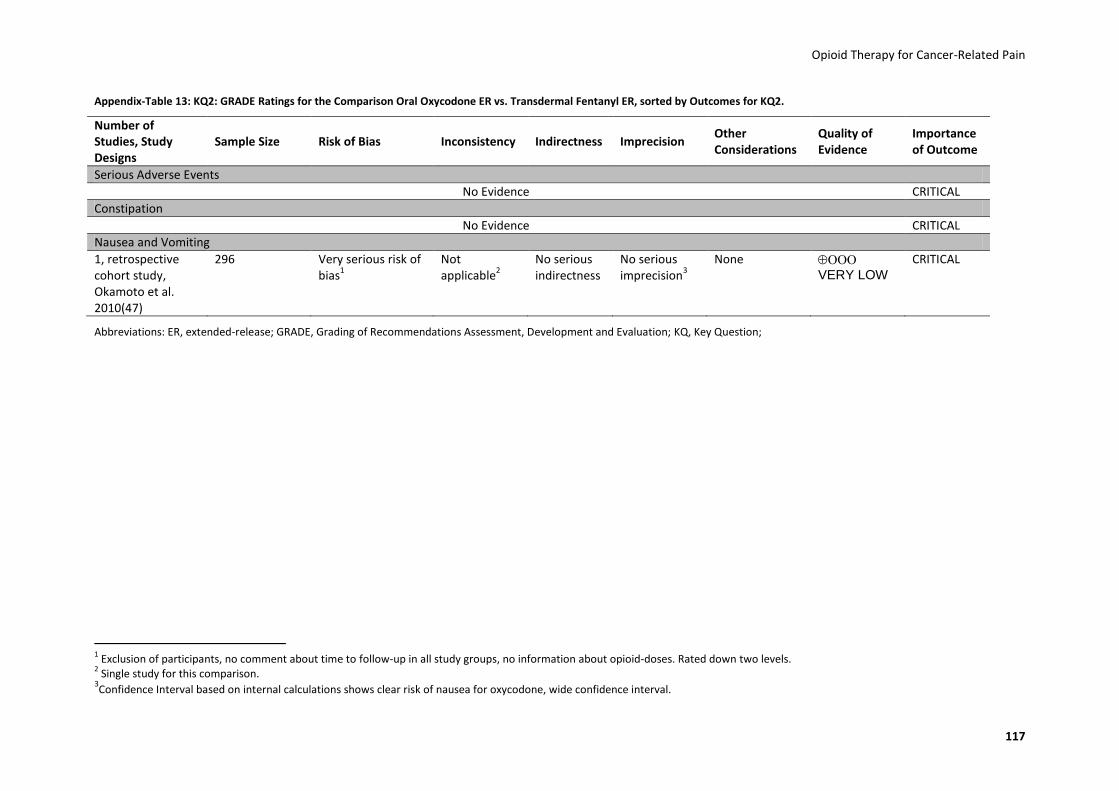
Opioid Therapy for Cancer-Related Pain
117
Appendix-Table 13: KQ2: GRADE Ratings for the Comparison Oral Oxycodone ER vs. Transdermal Fentanyl ER, sorted by Outcomes for KQ2.
Number of Studies, Study Designs
Sample Size Risk of Bias Inconsistency Indirectness Imprecision Other Considerations
Quality of Evidence
Importance of Outcome
Serious Adverse Events
No Evidence CRITICAL
Constipation
No Evidence CRITICAL
Nausea and Vomiting
1, retrospective cohort study, Okamoto et al. 2010(47)
296 Very serious risk of bias
1
Not applicable
2
No serious indirectness
No serious imprecision
3
None VERY LOW
CRITICAL
Abbreviations: ER, extended-release; GRADE, Grading of Recommendations Assessment, Development and Evaluation; KQ, Key Question;
1 Exclusion of participants, no comment about time to follow-up in all study groups, no information about opioid-doses. Rated down two levels.
2 Single study for this comparison.
3Confidence Interval based on internal calculations shows clear risk of nausea for oxycodone, wide confidence interval.
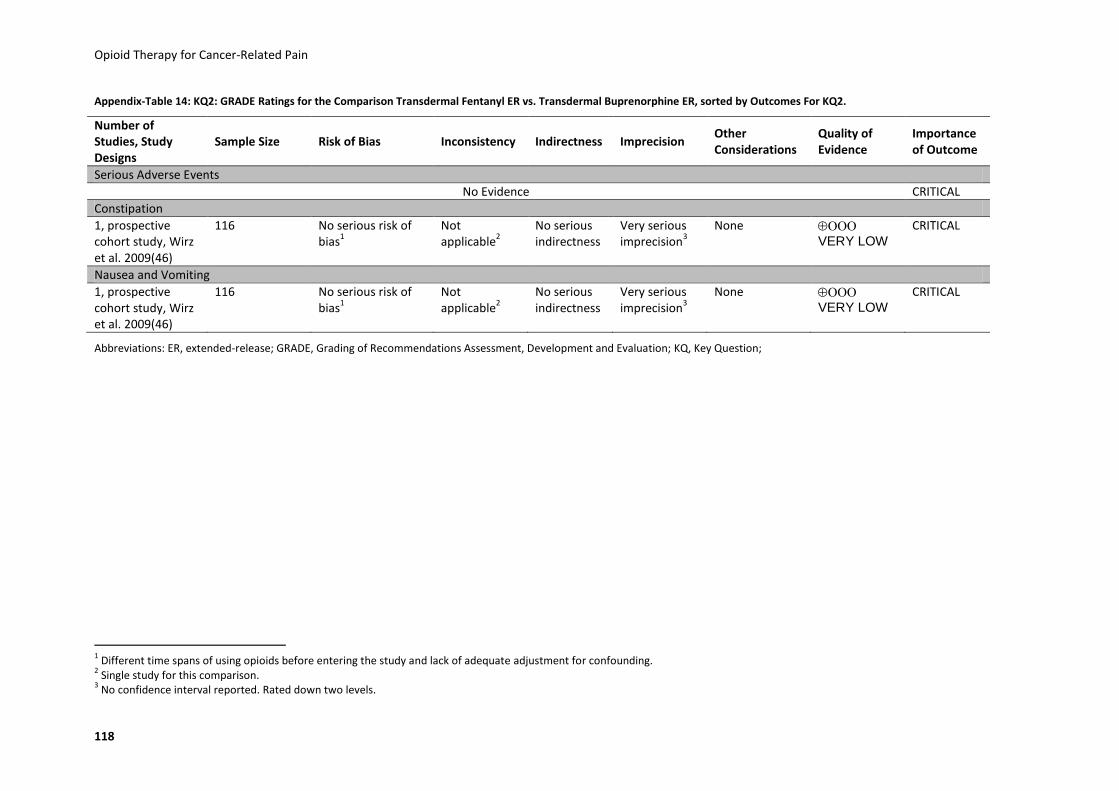
Opioid Therapy for Cancer-Related Pain
118
Appendix-Table 14: KQ2: GRADE Ratings for the Comparison Transdermal Fentanyl ER vs. Transdermal Buprenorphine ER, sorted by Outcomes For KQ2.
Number of Studies, Study Designs
Sample Size Risk of Bias Inconsistency Indirectness Imprecision Other Considerations
Quality of Evidence
Importance of Outcome
Serious Adverse Events
No Evidence CRITICAL
Constipation
1, prospective cohort study, Wirz et al. 2009(46)
116 No serious risk of bias
1
Not applicable
2
No serious indirectness
Very serious imprecision
3
None VERY LOW
CRITICAL
Nausea and Vomiting
1, prospective cohort study, Wirz et al. 2009(46)
116 No serious risk of bias
1
Not applicable
2
No serious indirectness
Very serious imprecision
3
None VERY LOW
CRITICAL
Abbreviations: ER, extended-release; GRADE, Grading of Recommendations Assessment, Development and Evaluation; KQ, Key Question;
1 Different time spans of using opioids before entering the study and lack of adequate adjustment for confounding.
2 Single study for this comparison.
3 No confidence interval reported. Rated down two levels.
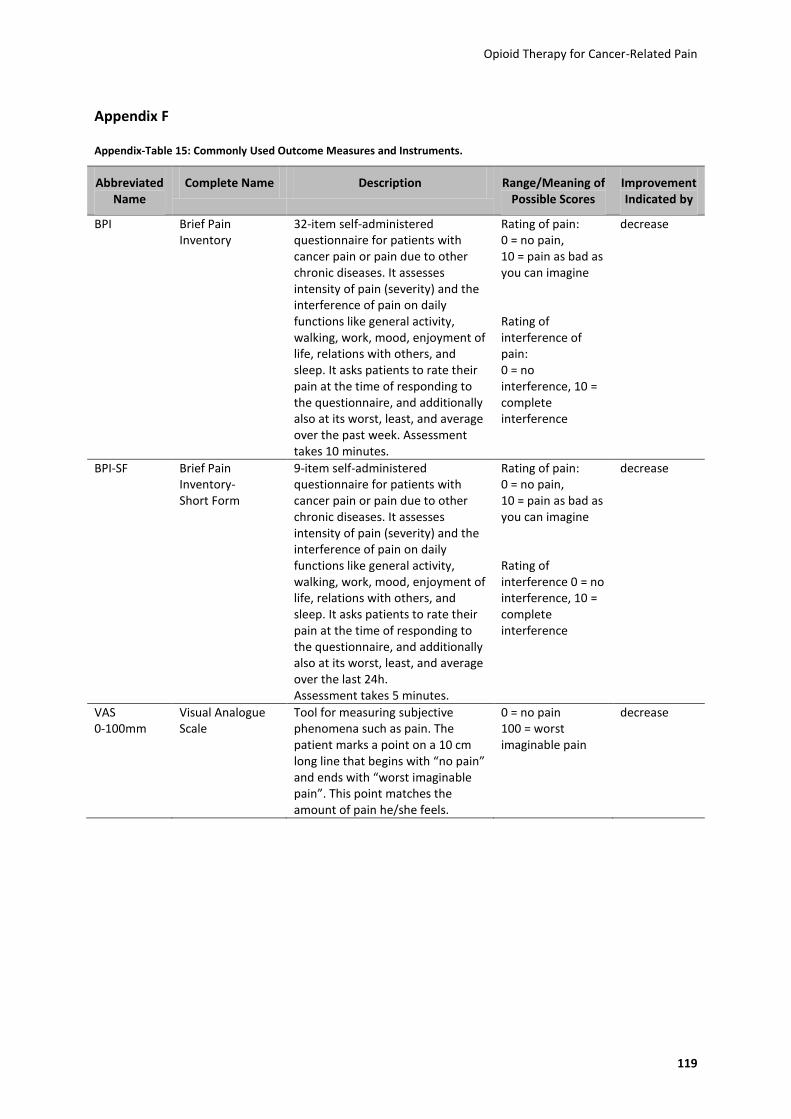
Opioid Therapy for Cancer-Related Pain
119
Appendix F
Appendix-Table 15: Commonly Used Outcome Measures and Instruments.
Abbreviated Name
Complete Name Description Range/Meaning of Possible Scores
Improvement Indicated by
BPI Brief Pain Inventory
32-item self-administered questionnaire for patients with cancer pain or pain due to other chronic diseases. It assesses intensity of pain (severity) and the interference of pain on daily functions like general activity, walking, work, mood, enjoyment of life, relations with others, and sleep. It asks patients to rate their pain at the time of responding to the questionnaire, and additionally also at its worst, least, and average over the past week. Assessment takes 10 minutes.
Rating of pain: 0 = no pain, 10 = pain as bad as you can imagine Rating of interference of pain: 0 = no interference, 10 = complete interference
decrease
BPI-SF Brief Pain Inventory- Short Form
9-item self-administered questionnaire for patients with cancer pain or pain due to other chronic diseases. It assesses intensity of pain (severity) and the interference of pain on daily functions like general activity, walking, work, mood, enjoyment of life, relations with others, and sleep. It asks patients to rate their pain at the time of responding to the questionnaire, and additionally also at its worst, least, and average over the last 24h. Assessment takes 5 minutes.
Rating of pain: 0 = no pain, 10 = pain as bad as you can imagine Rating of interference 0 = no interference, 10 = complete interference
decrease
VAS 0-100mm
Visual Analogue Scale
Tool for measuring subjective phenomena such as pain. The patient marks a point on a 10 cm long line that begins with “no pain” and ends with “worst imaginable pain”. This point matches the amount of pain he/she feels.
0 = no pain 100 = worst imaginable pain
decrease
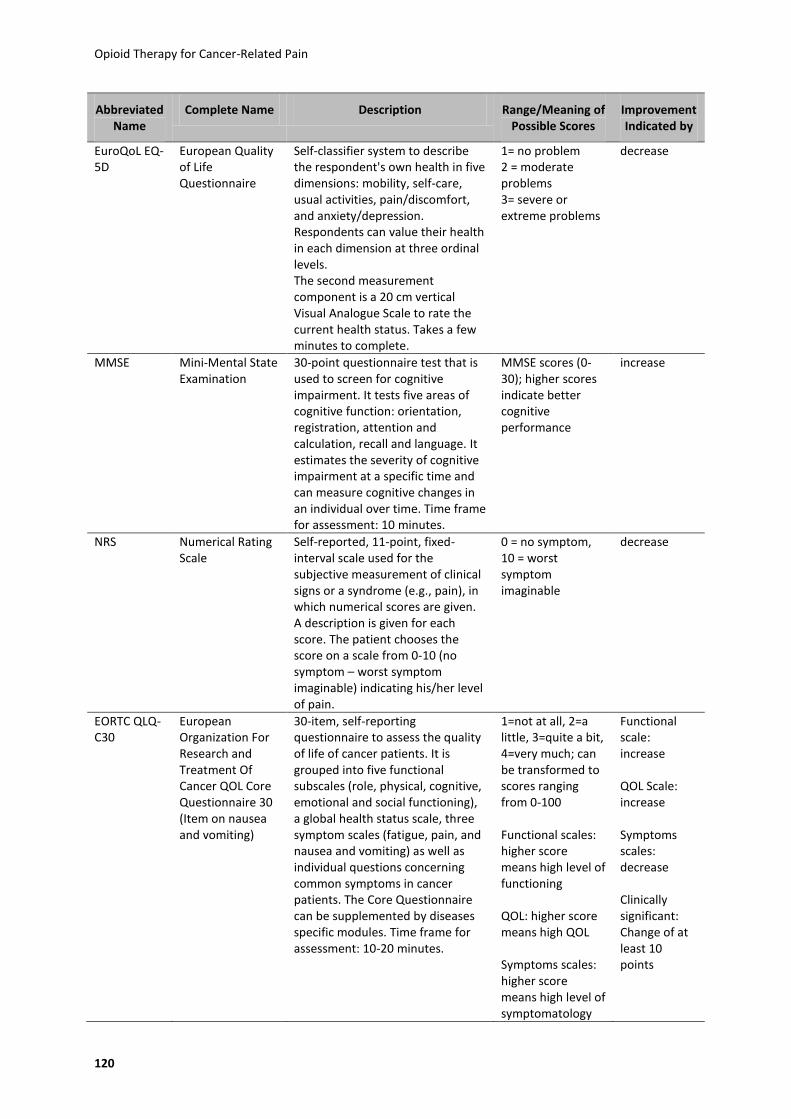
Opioid Therapy for Cancer-Related Pain
120
Abbreviated Name
Complete Name Description Range/Meaning of Possible Scores
Improvement Indicated by
EuroQoL EQ-5D
European Quality of Life Questionnaire
Self-classifier system to describe the respondent's own health in five dimensions: mobility, self-care, usual activities, pain/discomfort, and anxiety/depression. Respondents can value their health in each dimension at three ordinal levels. The second measurement component is a 20 cm vertical Visual Analogue Scale to rate the current health status. Takes a few minutes to complete.
1= no problem 2 = moderate problems 3= severe or extreme problems
decrease
MMSE Mini-Mental State Examination
30-point questionnaire test that is used to screen for cognitive impairment. It tests five areas of cognitive function: orientation, registration, attention and calculation, recall and language. It estimates the severity of cognitive impairment at a specific time and can measure cognitive changes in an individual over time. Time frame for assessment: 10 minutes.
MMSE scores (0-30); higher scores indicate better cognitive performance
increase
NRS Numerical Rating Scale
Self-reported, 11-point, fixed-interval scale used for the subjective measurement of clinical signs or a syndrome (e.g., pain), in which numerical scores are given. A description is given for each score. The patient chooses the score on a scale from 0-10 (no symptom – worst symptom imaginable) indicating his/her level of pain.
0 = no symptom, 10 = worst symptom imaginable
decrease
EORTC QLQ-C30
European Organization For Research and Treatment Of Cancer QOL Core Questionnaire 30 (Item on nausea and vomiting)
30-item, self-reporting questionnaire to assess the quality of life of cancer patients. It is grouped into five functional subscales (role, physical, cognitive, emotional and social functioning), a global health status scale, three symptom scales (fatigue, pain, and nausea and vomiting) as well as individual questions concerning common symptoms in cancer patients. The Core Questionnaire can be supplemented by diseases specific modules. Time frame for assessment: 10-20 minutes.
1=not at all, 2=a little, 3=quite a bit, 4=very much; can be transformed to scores ranging from 0-100 Functional scales: higher score means high level of functioning QOL: higher score means high QOL Symptoms scales: higher score means high level of symptomatology
Functional scale: increase QOL Scale: increase Symptoms scales: decrease Clinically significant: Change of at least 10 points
Opioid Therapy for Cancer-Related Pain
121
Appendix G
Commonly Used Abbreviations
Abbreviation Description
AE Adverse Events
BFI Bowel Function Index
BPI Brief Pain Inventory
BPI-SF Brief Pain Inventory-Short Form
CI Confidence Interval
d Day
ED Emergency Department
EORTC QLQ 30 European Organization for Research and Treatment of Cancer Quality of Life Questionnaire 30
ER Extended-Release
EuroQoL EQ-5D European Quality of Life Instrument
h Hours
HR Hazard Ratio
ICD International Classification of Diseases
IR Immediate-Release
KQ Key Question
mg Milligram
MMSE Mini-Mental State Examination
n Number of Participants
NR Not Reported
NRS Numerical Rating Scale
OR Odds Ratio
p Probability
PAC-SYM Patient Assessment of Constipation Symptoms
QoL Quality of Life
RCT Randomized Controlled Trial
SAE Serious Adverse Events
SD Standard Deviation
SR Sustained-Release
VAS Visual Analogue Scale
vs. Versus
μg Microgram

Opioid Therapy for Cancer-Related Pain
122
Appendix H
Excluded studies
Ineligible Publication Type (19):
1. Caraceni A, Pigni A, Brunelli C. Is oral morphine still the first choice opioid for moderate to severe cancer pain? A systematic review within the European Palliative Care Research Collaborative guidelines project. Palliative medicine. 2011;25(5):402-409.
2. Chwieduk CM, McKeage K. Fentanyl sublingual: in breakthrough pain in opioid-tolerant adults with cancer. Drugs. 2010;70(17):2281-2288.
3. Comerford T, Bruera E. Efficacy of controlled-release oxycodone [5] (multiple letters). Journal of Clinical Oncology. 1999;17(2):738.
4. Cormie PJ, Nairn M, Welsh J, Guideline Dev G. Control of pain in adults with cancer: summary of SIGN guidelines. British Medical Journal (England). 2008;337(NOV 5):NIL-NIL.
5. Gordon DB. Journal club. Oral transmucosal fentanyl citrate for cancer breakthrough pain: a review. Oncology nursing forum. 2006;33(2):257-264.
6. Gourlay GK. Treatment of cancer pain with transdermal fentanyl. Lancet Oncology. 2001;2(3):165-172.
7. Hair PI, Keating GM, McKeage K. Transdermal matrix fentanyl membrane patch (MATRIFEN): in severe cancer-related chronic pain. Drugs. 2008;68(14):2001-2009.
8. Hoy SM, Keating GM. Fentanyl Transdermal Matrix Patch (DUROTEP MT patch; DUROGESIC DTRANS; DUROGESIC SMAT): in adults with cancer-related pain. Drugs. 2008;68(12):1711-1721.
9. King S, Forbes K, Hanks G, Ferro C, Chambers E. A systematic review of the use of opioid medication for those with moderate to severe cancer pain and renal impairment: A European Palliative Care Research Collaborative opioid guidelines project. Palliative medicine. 2011;25(5):525-552.
10. King SJ, Reid C, Forbes K, Hanks G. A systematic review of oxycodone in the management of cancer pain. Palliative medicine. 2011;25(5):454-470.
11. Klepstad P, Kaasa S, Borchgrevink PC. Starting Step III opioids for moderate to severe pain in cancer patients: Dose titration: A systematic review. Palliative medicine. 2011;25(5):424-430.
12. McNicol E, Horowicz-Mehler N, Fisk RA, Bennett K, Carr D, et al. Management of opioid side effects in cancer-related and chronic noncancer pain: a systematic review. Journal of Pain (USA). 2003;4(May):231-256.
13. Pigni A, Brunelli C, Caraceni A. The role of hydromorphone in cancer pain treatment: a systematic review. Palliative medicine. 2011;25(5):471-477.
14. Ruiz-Garcia V, Lopez-Briz E. Breakthrough cancer pain: morphine remains gold standard in breakthrough cancer pain. BMJ: British Medical Journal (Overseas & Retired Doctors Edition). 2009;338(7685):7-8.
15. Tassinari D, Drudi F, Rosati M, Tombesi P, Sartori S, Maltoni M. The second step of the analgesic ladder and oral tramadol in the treatment of mild to moderate cancer pain: A systematic review. Palliative medicine. 2011;25(5):410-423.
16. Twycross RG. Controlled release morphine tablets. Lancet (England). 1981;1(Apr 18):892.
17. Vissers D, Stam W, Nolte T, Lenre M, Jansen J. Efficacy of intranasal fentanyl spray versus other opioids for breakthrough pain in cancer. Vol 26:1037.

Opioid Therapy for Cancer-Related Pain
123
18. Xu GZ, Cai ZJ, Deng YP, Hou J, Liu SJ, Et. Clinical evaluation of the analgesic effect of sustained-release morphine sulfate microgranules in patients with terminal cancer. Clinical Drug Investigation (New Zealand). 1997;14(Suppl 1):34-42.
19. Yu S, Sun Y. A large-scale study of OxyContin® tablets for relieving moderate to severe cancer pain. European Journal of Pain Supplements. 2007;1(1):99-100.
Ineligible Study Design (36):
1. Ahmedzai S, Brooks D. Transdermal fentanyl versus sustained-release oral morphine in cancer pain: preference, efficacy, and quality of life. The TTS-Fentanyl Comparative Trial Group. J Pain Symptom Manage. May 1997;13(5):254-261.
2. Anonymous. Abstral(R) (Fentanyl Sublingual Tablets for Breakthrough Cancer Pain). Vol 36:2.
3. Beaver WT, Wallenstein SL, Rogers A, Houde RW. Analgesic studies of codeine and oxycodone in patients with cancer. I. Comparisons of oral with intramuscular codeine and of oral with intramuscular oxycodone. J Pharmacol Exp Ther. Oct 1978;207(1):92-100.
4. Brooks I, De Jager R, Blumenreich M, George E, Savarese JJ. PRINCIPLES OF CANCER PAIN MANAGEMENT USE OF LONG-ACTING ORAL MORPHINE. Journal of Family Practice. 1989;28(3):275-280.
5. Chen HP, Jiang JJ, Li JX. Efficacy and safety of oxycodone-acetaminophen for moderate and severe visceral pain in advanced cancer patients. Vol 18:920.
6. Clark AJ, Ahmedzai SH, Allan LG, et al. Efficacy and safety of transdermal fentanyl and sustained-release oral morphine in patients with cancer and chronic non-cancer pain. Curr Med Res Opin. Sep 2004;20(9):1419-1428.
7. Clemens KE, Klaschik E. Clinical experience with transdermal and orally administered opioids in palliative care patients--a retrospective study. Jpn J Clin Oncol. Apr 2007;37(4):302-309.
8. De Stoutz ND, Bruera E, Suarez-Almazor M. Opioid rotation for toxicity reduction in terminal cancer patients. Journal of Pain and Symptom Management. 1995;10(5):378-384.
9. Gamallo A, Monescillo MA, Pereira MA, et al. Transdermal fentanyl for the treatment of chronic cancer pain in patients under home palliative care. European Journal of Cancer. Sept. 1999;35(SUPPL. 4):S368.
10. Grond S, Radbruch L, Meuser T, Loick G, Sabatowski R, Lehmann KA. High-dose tramadol in comparison to low-dose morphine for cancer pain relief. J Pain Symptom Manage. Sep 1999;18(3):174-179.
11. Hanna M, Tuca A, Thipphawong J. An open-label, 1-year extension study of the long-term safety and efficacy of once-daily OROS1 hydromorphone in patients with chronic cancer pain. BMC Palliative Care. 2009;8.
12. Hays H, Hagen N, Thirlwell M, et al. Comparative clinical efficacy and safety of immediate release and controlled release hydromorphone for chronic severe cancer pain. Cancer. Sep 15 1994;74(6):1808-1816.
13. Kanamori C, Kanamori T, Hayashi M, Yorioka H, Kanzaki H. Three-cycle fentanyl patch system significantly improves pain control in gynecologic cancer. Journal of Obstetrics & Gynaecology Research. 2006;32(6):605-609.
14. Khojasteh A, Evans W, Reynolds RD, Thomas G, Savarese JJ. Controlled-release oral morphine sulfate in the treatment of cancer pain with pharmacokinetic correlation. J Clin Oncol. Jun 1987;5(6):956-961.
15. Lauretti GR, Oliveira GM, Pereira NL. Comparison of sustained-release morphine with sustained-release oxycodone in advanced cancer patients. Br J Cancer. Dec 1 2003;89(11):2027-2030.
Opioid Therapy for Cancer-Related Pain
124
16. Leelanuntakit S. Management of cancer-related pain with transdermal fentanyl. J Med Assoc Thai. Jun 1996;79(6):341-346.
17. Leppert W. Analgesic efficacy and side effects of oral tramadol and morphine administered orally in the treatment of cancer pain. Nowotwory. 2001;51(3):257-266.
18. Leppert W, Majkowicz M. The impact of tramadol and dihydrocodeine treatment on quality of life of patients with cancer pain. Int J Clin Pract. Nov 2010;64(12):1681-1687.
19. Likar R, Wittels M, Molnar M, Kager I, Ziervogel G, Sittl R. Pharmacokinetic and pharmacodynamic properties of tramadol IR and SR in elderly patients: A prospective, age-group-controlled study. Clinical therapeutics. 2006;28(12):2022-2039.
20. Mercadante S, Casuccio A, Agnello A, Serretta R, Calderone L, Barresi L. Morphine versus methadone in the pain treatment of advanced-cancer patients followed up at home. J Clin Oncol. Nov 1998;16(11):3656-3661.
21. Mercadante S, Ferrera P, Villari P, Casuccio A. Rapid switching between transdermal fentanyl and methadone in cancer patients. J Clin Oncol. Aug 1 2005;23(22):5229-5234.
22. Mercadante S, Tirelli W, David F, et al. Morphine versus oxycodone in pancreatic cancer pain: a randomized controlled study. Clin J Pain. Nov-Dec 2010;26(9):794-797.
23. Miyazaki T, Hanaoka K, Namiki A, et al. Efficacy, safety and pharmacokinetic study of a novel fentanyl-containing matrix transdermal patch system in Japanese patients with cancer pain. Clinical drug investigation. 2008;28(5):313-325.
24. Morita T, Takigawa C, Onishi H, et al. Opioid rotation from morphine to fentanyl in delirious cancer patients: an open-label trial. Journal of Pain & Symptom Management. 2005;30(1):96-103.
25. Pace MC, Passavanti MB, Grella E, et al. Buprenorphine in long-term control of chronic pain in cancer patients. Front Biosci. 2007;12:1291-1299.
26. Panich A, Charnvej L. Comparison of morphine slow release tablet (MST) and morphine sulphate solution (MSS) in the treatment of cancer pain. J Med Assoc Thai. Dec 1993;76(12):672-676.
27. Payne R, Mathias SD, Pasta DJ, Wanke LA, Williams R, Mahmoud R. Quality of life and cancer pain: satisfaction and side effects with transdermal fentanyl versus oral morphine. J Clin Oncol. Apr 1998;16(4):1588-1593.
28. Reid CM, Martin RM, Sterne JA, Davies AN, Hanks GW. Oxycodone for cancer-related pain - Meta-analysis of randomized controlled trials. Archives of Internal Medicine (USA). 2006;166(Aug):837-843.
29. Salzman RT, Roberts MS, Wild J, Fabian C, Reder RF, Goldenheim PD. Can a controlled-release oral dose form of oxycodone be used as readily as an immediate-release form for the purpose of titrating to stable pain control? J Pain Symptom Manage. Oct 1999;18(4):271-279.
30. Sittl R, Nuijten M, Nautrup BP. Changes in prescribed daily doses of transdermal fentanyl and transdermal buprenorphine during treatment of patients with cancer and noncancer pain in Germany: results of a retrospective cohort study. Clinical therapeutics. 2005;27(7):1022-1031.
31. Sloan P, Slatkin N, Ahdieh H. Effectiveness and safety of oral extended-release oxymorphone for the treatment of cancer pain: a pilot study. Support Care Cancer. Jan 2005;13(1):57-65.
32. Ventaffrida V, Oliveri E, Caraceni A, et al. A retrospective study on the use of oral morphine in cancer pain. J Pain Symptom Manage. Spring 1987;2(2):77-81.
33. Weinstein SM, Messina J, Xie F. Fentanyl Buccal Tablet for the Treatment of Breakthrough Pain in Opioid-Tolerant Patients With Chronic Cancer Pain: A Long-term, Open-Label Safety Study. (vol 115, pg 2571, 2009). Cancer. Jul 15 2009;115(14):3372.

Opioid Therapy for Cancer-Related Pain
125
34. Weinstein SM, Shi M, Buckley BJ, Kwarcinski MA. Multicenter, open-label, prospective evaluation of the conversion from previous opioid analgesics to extended-release hydromorphone hydrochloride administered every 24 hours to patients with persistent moderate to severe pain. Clin Ther. Jan 2006;28(1):86-98.
35. Wilkinson TJ, Robinson BA, Begg EJ, Duffull SB, Ravenscroft PJ, Schneider JJ. Pharmacokinetics and efficacy of rectal versus oral sustained-release morphine in cancer patients. Cancer Chemother Pharmacol. 1992;31(3):251-254.
36. Wong JO, Chiu GL, Tsao CJ, Chang CL. Comparison of oral controlled-release morphine with transdermal fentanyl in terminal cancer pain. Acta Anaesthesiol Sin. Mar 1997;35(1):25-32.
Ineligible Duration (22):
1. Bono AV, Cuffari S. Efficacy and tolerability of tramadol in neoplastic pain: A comparative study with buprenorphine. Drugs. 1997;53(SUPPL. 2):40-49.
2. Chrubasik S, Friedrich G, Yucel A, Aykut G, Chrubasik J, Ziegler R. Replacement of oral slow release morphine by morphine sulphate suppositories in patients suffering from intractable cancer pain. Regional Anesthesia. 1997;22(2 SUPPL.):102.
3. Cundiff D, McCarthy K, Savarese JJ, et al. Evaluation of a cancer pain model for the testing of long-acting analgesics. The effect of MS Contin in a double-blind, randomized crossover design. Cancer. Jun 1 1989;63(11 Suppl):2355-2359.
4. Finn JW, Walsh TD, MacDonald N, Bruera E, Krebs LU, Shepard KV. Placebo-blinded study of morphine sulfate sustained-release tablets and immediate-release morphine sulfate solution in outpatients with chronic pain due to advanced cancer. J Clin Oncol. May 1993;11(5):967-972.
5. Grosset AB, Roberts MS, Woodson ME, et al. Comparative efficacy of oral extended-release hydromorphone and immediate-release hydromorphone in patients with persistent moderate to severe pain: two randomized controlled trials. J Pain Symptom Manage. Jun 2005;29(6):584-594.
6. Hanks GW, Twycross RG, Bliss JM. Controlled release morphine tablets: a double-blind trial in patients with advanced cancer. Anaesthesia. Aug 1987;42(8):840-844.
7. Heiskanen T, Kalso E. Controlled-release oxycodone and morphine in cancer related pain. Pain. Oct 1997;73(1):37-45.
8. Heiskanen TE, Ruismaki PM, Seppala TA, Kalso EA. Morphine or oxycodone in cancer pain? Acta Oncol. 2000;39(8):941-947.
9. Kalso E, Vainio A. Morphine and oxycodone hydrochloride in the management of cancer pain. Clin Pharmacol Ther. May 1990;47(5):639-646.
10. Mercadante S, Arcuri E, Fusco F, et al. Randomized double-blind, double-dummy crossover clinical trial of oral tramadol versus rectal tramadol administration in opioid-naive cancer patients with pain. Support Care Cancer. Sep 2005;13(9):702-707.
11. Moertel CG, Ahmann DL, Taylor WF, Schwartau N. Relief of pain by oral medications: a controlled evaluation of analgesic combinatioms. J. Am. Med. Assoc. 1974;229(Jul 1):55-59.
12. Moolenaar F, Meijler WJ, Frijlink HW, Visser J, Proost JH. Clinical efficacy, safety and pharmacokinetics of a newly developed controlled release morphine sulphate suppository in patients with cancer pain. Eur J Clin Pharmacol. Jun 2000;56(3):219-223.
13. Mucci-LoRusso P, Berman BS, Silberstein PT, et al. Controlled-release oxycodone compared with controlled-release morphine in the treatment of cancer pain: A randomized, double-blind, parallel-group study. European Journal of Pain. 1998;2(3):239-249.
Opioid Therapy for Cancer-Related Pain
126
14. Parris WC, Johnson BW, Jr., Croghan MK, et al. The use of controlled-release oxycodone for the treatment of chronic cancer pain: a randomized, double-blind study. J Pain Symptom Manage. Oct 1998;16(4):205-211.
15. Savarese JJ, Thomas GB, Homesley H, Hill CS. Rescue factor: design for evaluating long acting analgesics. Clinical Pharmacology and Therapeutics (USA). 1988;43(Apr):376-380.
16. Sawe J, Dahlstrom B, Rane A. Steady-state kinetics and analgesic effect of oral morphine in cancer patients. Eur J Clin Pharmacol. 1983;24(4):537-542.
17. Stambaugh JE, Reder RF, Stambaugh MD, Stambaugh H, Davis M. Double-blind, randomized comparison of the analgesic and pharmacokinetic profiles of controlled- and immediate-release oral oxycodone in cancer pain patients. J Clin Pharmacol. May 2001;41(5):500-506.
18. Staquet M. Double blind study of dezocine in cancer pain. Journal of Clinical Pharmacology (USA). 1979;19(Jul):392-394.
19. Walsh TD. A controlled study of MST Continuos tablets for chronic pain in advanced cancer. Advances in Morphine Therapy. the 1983 International Symposium on Pain Control. 1984:99-102.
20. Wilder-Smith CH, Schimke J, Osterwalder B, Senn HJ. Oral tramadol, a mu-opioid agonist and monoamine reuptake-blocker, and morphine for strong cancer-related pain. Ann Oncol. Feb 1994;5(2):141-146.
21. Wirz S, Wartenberg HC, Elsen C, Wittmann M, Nadstawek J, et al. Managing cancer pain and symptoms of outpatients by rotation to sustained-release hydromorphone - A prospective clinical trial. Clinical Journal of Pain. 2006;22(Sep):770-775.
22. Zech D, Dauer HG, Stollenwerk B, Lehmann KA. PCA AND TTS FENTANYL IN THE TREATMENT OF CANCER PAIN. Pain. 1990(SUPPL. 5):S356.
Ineligible Population (11):
1. Eisenberg E, McNicol ED, Carr DB. Efficacy and safety of opioid agonists in the treatment of neuropathic pain of nonmalignant origin: Systematic review and meta-analysis of randomized controlled trials. Journal of the American Medical Association. 2005;293(24):3043-3052.
2. Galer BS, Lee D, Ma T, Nagle B, Schlagheck TG. MorphiDex® (morphine sulfate/dextromethorphan hydrobromide combination) in the treatment of chronic pain: Three multicenter, randomized, double-blind, controlled clinical trials fail to demonstrate enhanced opioid analgesia or reduction in tolerance. Pain. 2005;115(3):284-295.
3. Mayyas F, Fayers P, Kaasa S, Dale O. A systematic review of oxymorphone in the management of chronic pain. Journal of Pain & Symptom Management. 2010;39(2):296-308.
4. Portenoy RK, Payne R, Coluzzi P, et al. Oral transmucosal fentanyl citrate (OTFC) for the treatment of breakthrough pain in cancer patients: a controlled dose titration study. Pain. Feb 1999;79(2-3):303-312.
5. Quigley C. Hydromorphone for acute and chronic pain. Cochrane Database of Systematic Reviews. 2002(1).
6. Sidebotham D, Dijkhuizen MRJ, Schug SA. The safety and utilization of patient-controlled analgesia. Journal of Pain & Symptom Management. 1997;14(4):202-209.
7. Sittl R, Griessinger N, Likar R. Analgesic efficacy and tolerability of transdermal buprenorphine in patients with inadequately controlled chronic pain related to cancer and other disorders: a multicenter, randomized, double-blind, placebo-controlled trial. Clin Ther. Jan 2003;25(1):150-168.
Opioid Therapy for Cancer-Related Pain
127
8. Sorge J, Sittl R. Transdermal buprenorphine in the treatment of chronic pain: results of a phase III, multicenter, randomized, double-blind, placebo-controlled study. Clin Ther. Nov 2004;26(11):1808-1820.
9. Tassinari D, Sartori S, Tamburini E, et al. Transdermal fentanyl as a front-line approach to moderate-severe pain: a meta-analysis of randomized clinical trials. Journal of Palliative Care. 2009;25(3):172-180.
10. Zeppetella G. Opioids for the management of breakthrough cancer pain in adults: A systematic review undertaken as part of an EPCRC opioid guidelines project. Palliative medicine. 2011;25(5):516-524.
11. Zhao SZ, Chung F, Hanna DB, Raymundo AL, Cheung RY, Chen C. Dose-response relationship between opioid use and adverse effects after ambulatory surgery. Journal of Pain & Symptom Management. 2004;28(1):35-46.
Ineligible Intervention (23):
1. Anonymous. Fentanyl Buccal Soluble Film (<it>Onsolis</it>) for Breakthrough Cancer Pain. Vol 52:30.
2. Arbaiza D, Vidal O. Tramadol in the treatment of neuropathic cancer pain: a double-blind, placebo-controlled study. Clin Drug Investig. 2007;27(1):75-83.
3. Bruera E, Belzile M, Pituskin E, et al. Efficacy and safety of morphine sulfate controlled-release suppositories (MS-CRS) administered once daily and twice daily for severe cancer pain. Journal of Palliative Care. Fal 1998;14(3):117-117.
4. Chary S, Goughnour BR, Moulin DE, Thorpe WR, Harsanyi Z, Darke AC. The dose-response relationship of controlled-release codeine (Codeine Contin) in chronic cancer pain. J Pain Symptom Manage. Aug 1994;9(6):363-371.
5. Clemons M, Regnard C, Appleton T. Alertness, cognition and morphine in patients with advanced cancer. Cancer Treatment Reviews. 1996;22(6):451-468.
6. Coluzzi PH, Schwartzberg L, Conroy JD, et al. Breakthrough cancer pain: a randomized trial comparing oral transmucosal fentanyl citrate (OTFC) and morphine sulfate immediate release (MSIR). Pain. Mar 2001;91(1-2):123-130.
7. De Conno F, Ripamonti C, Sbanotto A, et al. A clinical study on the use of codeine, oxycodone, dextropropoxyphene, buprenorphine, and pentazocine in cancer pain. Journal of Pain & Symptom Management. 1991;6(7):423-427.
8. Dhaliwal HS, Sloan P, Arkinstall WW, et al. Randomized evaluation of controlled-release codeine and placebo in chronic cancer pain. J Pain Symptom Manage. Nov 1995;10(8):612-623.
9. Ferrell B, Wisdom C, Wenzl C, Brown J. Effects of controlled-released morphine on quality of life for cancer pain. Oncol Nurs Forum. Jul-Aug 1989;16(4):521-526.
10. Gourlay GK, Cherry DA, Cousins MJ. A comparative study of the efficacy and pharmacokinetics of oral methadone and morphine in the treatment of severe pain in patients with cancer. Pain. Jun 1986;25(3):297-312.
11. Kanner RM, Foley KM. Patterns of narcotic drug use in a cancer pain clinic. Ann N Y Acad Sci. 1981;362:161-172.
12. Marinangeli F, Ciccozzi A, Leonardis M, et al. Use of strong opioids in advanced cancer pain: a randomized trial. J Pain Symptom Manage. May 2004;27(5):409-416.
13. Reid. Oxycodone for cancer-related pain: Meta-analysis of randomized controlled trials (vol 166, pg 837, 2006). Archives of internal medicine. Nov 27 2006;166(21):2387.
Opioid Therapy for Cancer-Related Pain
128
14. Rodriguez RF, Bravo LE, Castro F, et al. Incidence of weak opioids adverse events in the management of cancer pain: a double-blind comparative trial. J Palliat Med. Feb 2007;10(1):56-60.
15. Rodriguez RF, Castillo JM, Castillo MP, et al. Hydrocodone/acetaminophen and tramadol chlorhydrate combination tablets for the management of chronic cancer pain: a double-blind comparative trial. Clin J Pain. Jan 2008;24(1):1-4.
16. Rodriguez RF, Castillo JM, Del Pilar Castillo M, et al. Codeine/acetaminophen and hydrocodone/acetaminophen combination tablets for the management of chronic cancer pain in adults: a 23-day, prospective, double-blind, randomized, parallel-group study. Clin Ther. Apr 2007;29(4):581-587.
17. Rodriguez RF, Castillo JM, Mdp C. Codeine/paracetamol and hydrocodone/paracetamol combination tablets for the management of chronic cancer pain in adults: A 23-days, prospective, double-blind, randomized, parallel-group study. Clin Ther. 2007;29:582-587.
18. Stambaugh JE, Jr., McAdams J. Comparison of the analgesic efficacy and safety oral ciramadol, codeine, and placebo in patients with chronic cancer pain. J Clin Pharmacol. Feb 1987;27(2):162-166.
19. Twycross RG. Choice of strong analgesic in terminal cancer: diamorphine or morphine? Pain. 1977(2):93-104. http://www.mrw.interscience.wiley.com/cochrane/clcentral/articles/312/CN-00016312/frame.html.
20. Twycross RG. Comparison of diamorphine with cocaine and methadone. British Journal of Clinical Pharmacology (England). 1977;4(Dec):691-693.
21. Ventafridda V, De Conno F, Guarise G, Tamburini M, Savio G. Chronic analgesic study on buprenorphine action in cancer pain. Comparison with pentazocine. Arzneimittelforschung. 1983;33(4):587-590.
22. Ventafridda V, Ripamonti C, Bianchi M, Sbanotto A, De Conno F. A randomized study on oral administration of morphine and methadone in the treatment of cancer pain. Journal of Pain & Symptom Management. 1986;1(4):203-207.
23. Zeppetella G, Ribeiro Maria DC. Opioids for the management of breakthrough (episodic) pain in cancer patients. Cochrane Database of Systematic Reviews. 2006(1). http://www.mrw.interscience.wiley.com/cochrane/clsysrev/articles/CD004311/frame.html.
Ineligible Administration (6):
1. Beaver WT, Wallenstein SL, Houde RW, Rogers A. A comparison of the analgesic effects of pentazocine and morphine in patients with cancer. Clinical pharmacology and therapeutics. 1966(6):740-751. http://www.mrw.interscience.wiley.com/cochrane/clcentral/articles/061/CN-00296061/frame.html.
2. Bruera E, Belzile M, Neumann CM, Ford I, Harsanyi Z, Darke A. Twice-daily versus once-daily morphine sulphate controlled-release suppositories for the treatment of cancer pain. A randomized controlled trial. Support Care Cancer. Jul 1999;7(4):280-283.
3. Elsner F, Radbruch L, Loick G, Gartner J, Sabatowski R. Intravenous versus subcutaneous morphine titration in patients with persisting exacerbation of cancer pain. J Palliat Med. Aug 2005;8(4):743-750.
4. Frankendal B, Kjellgren O. Severe pain in gynecologic cancer. Trial of pentazocine, morphine, and a placebo. Cancer. 1971(4):842-847. http://www.mrw.interscience.wiley.com/cochrane/clcentral/articles/687/CN-00005687/frame.html.
5. Osipova NA, Novikov GA, Beresnev VA, Loseva NA. ANALGESIC EFFECT OF TRAMADOL IN CANCER PATIENTS WITH CHRONIC PAIN A COMPARISON WITH PROLONGED-ACTION MORPHINE SULFATE. Current Therapeutic Research. 1991;50(6):812-821.

Opioid Therapy for Cancer-Related Pain
129
6. Quigley C, Wiffen P. A systematic review of hydromorphone in acute and chronic pain. Journal of Pain & Symptom Management. 2003;25(2):169-178.
Ineligible Comparator (9):
1. A randomized study to assess the efficacy and safety of fentanyl-TTS versus minor opioids in patients with moderate to severe chronic oncological pain previously treated with NSAIDs.: Janssen-Cilag, S.A.; Access Date: 20.06.2012 2007.
2. Apolone G, Corli O, Negri E, et al. Effects of transdermal buprenorphine on patients-reported outcomes in cancer patients: results from the Cancer Pain Outcome Research (CPOR) Study Group. Clin J Pain. Oct 2009;25(8):671-682.
3. Kerr RO, Tester WJ. Patient preference study comparing two extended-release morphine sulfate formulations (once daily Kadian versus twice daily MS Contin) for cancer pain. Clinical Drug Investigation (New Zealand). 2000;19(Jan):25-32.
4. Kress HG, Von der Laage D, Hoerauf KH, et al. A randomized, open, parallel group, multicenter trial to investigate analgesic efficacy and safety of a new transdermal fentanyl patch compared to standard opioid treatment in cancer pain. J Pain Symptom Manage. Sep 2008;36(3):268-279.
5. Moertel CG, Ahmann DL, Taylor WF, Schwartau N. Comparative evaluation of marketed analgesic drugs. New England Journal of Medicine (USA). 1972;286(Apr 13):813-815.
6. Mystakidou K, Katsouda E, Kouloulias V, Kouvaris J, Tsiatas M, Vlahos L. Comparison of transdermal fentanyl with codeine/paracetamol, in combination with radiotherapy, for the management of metastatic bone pain. J Opioid Manag. Sep-Oct 2005;1(4):204-210.
7. Pistevou-Gompaki K, Kouloulias VE, Varveris C, et al. Radiotherapy plus either transdermal fentanyl or paracetamol and codeine for painful bone metastases: a randomised study of pain relief and quality of life. Curr Med Res Opin. 2004;20(2):159-163.
8. Tooley PJH, Cookson RF, Jones M, Nuyts GD. Medical events and resource utilisation in cancer-pain patients treated with strong opioids: an analysis of the UK General Practice Research Database. Journal of Drug Assessment. 2000;3(Part 3):221-234.
9. Wiffen PJ, McQuay HJ. Oral morphine for cancer pain. Cochrane Database Syst Rev. 2007(4):CD003868.
Ineligible Outcome (9):
1. Bruera E, Belzile M, Pituskin E, et al. Randomized, double-blind, cross-over trial comparing safety and efficacy of oral controlled-release oxycodone with controlled-release morphine in patients with cancer pain. J Clin Oncol. Oct 1998;16(10):3222-3229.
2. Gabrail NY, Dvergsten C, Ahdieh H. Establishing the dosage equivalency of oxymorphone extended-release and oxycodone controlled release in patients with cancer pain: a randomized controlled study. Curr Med Res Opin. Jun 2004;20(6):911-918.
3. Goughnour BR, Arkinstall WW, Stewart JH. Analgesic response to single and multiple doses of controlled-release morphine tablets and morphine oral solution in cancer patients. Cancer. Jun 1 1989;63(11 Suppl):2294-2297.
4. Guest JF, Ruiz FJ, Russ J, Gupta RD, Mihai A, Greener M. A comparison of the resources used in advanced cancer care between two different strong opioids: an analysis of naturalistic practice in the UK. Curr Med Res Opin. Feb 2005;21(2):271-280.
5. Hagen N, Thirlwell MP, Dhaliwal HS, Babul N, Harsanyi Z, Darke AC. Steady-state pharmacokinetics of hydromorphone and hydromorphone-3-glucuronide in cancer patients after immediate and controlled-release hydromorphone. J Clin Pharmacol. Jan 1995;35(1):37-44.

Opioid Therapy for Cancer-Related Pain
130
6. Henriksen H, Knudsen J. MST Continuos tablets in pain of advanced cancer: A controlled study. Advances in Morphine Therapy. The 1983 International Symposium on Pain Control. 1984:123-126.
7. Sittl R, Likar R, Nautrup BP. Equipotent doses of transdermal fentanyl and transdermal buprenorphine in patients with cancer and noncancer pain: results of a retrospective cohort study. Clin Ther. Feb 2005;27(2):225-237.
8. Tassinari D, Sartori S, Tamburini E, et al. Adverse effects of transdermal opiates treating moderate-severe cancer pain in comparison to long-acting morphine: a meta-analysis and systematic review of the literature. Journal of Palliative Medicine. 2008;11(3):492-501.
9. Welsh J, Stuart JHB, Haveshaw T, Billiaert P, Caiman KC. A double blind cross-over study of two oral formulations of morphine. Cancer Chemotherapy and Selective Drug Development. 1984:153-158.
Ineligible Research Question (12):
1. Boureau F, Saudubray F, d'Arnoux C, et al. A comparative study of controlled-release morphine (CRM) suspension and CRM tablets in chronic cancer pain. J Pain Symptom Manage. Oct 1992;7(7):393-399.
2. Gourlay GK, Cherry DA, Onley MM, et al. Pharmacokinetics and pharmacodynamics of twenty-four-hourly Kapanol compared to twelve-hourly MS Contin in the treatment of severe cancer pain. Pain. Feb 1997;69(3):295-302.
3. Hagen NA, Thirlwell M, Eisenhoffer J, Quigley P, Harsanyi Z, Darke A. Efficacy, safety, and steady-state pharmacokinetics of once-a-day controlled-release morphine (MS Contin XL) in cancer pain. J Pain Symptom Manage. Jan 2005;29(1):80-90.
4. Hasselstrom J, Alexander N, Bringel C, Svensson JO, Sawe J. Single-dose and steady-state kinetics of morphine and its metabolites in cancer patients--a comparison of two oral formulations. Eur J Clin Pharmacol. 1991;40(6):585-591.
5. Kim DY, Song HS, Ahn JS, et al. The dosing frequency of sustained-release opioids and the prevalence of end-of-dose failure in cancer pain control: a Korean multicenter study. Support Care Cancer. Feb 2010;19(2):297-301.
6. Lorenz KA, Lynn J, Dy SM, et al. Evidence for improving palliative care at the end of life: A systematic review. Annals of Internal Medicine. 2008;148(2):147-159.
7. Maltoni M, Scarpi E, Modonesi C, et al. A validation study of the WHO analgesic ladder: a two-step vs three-step strategy. Support Care Cancer. Nov 2005;13(11):888-894.
8. Mercadante S, Caraceni A. Conversion ratios for opioid switching in the treatment of cancer pain: a systematic review. Palliative medicine. 2011;25(5):504-515.
9. Mercadante S, Fulfaro F, Casuccio A. Pattern of drug use by advanced cancer patients followed at home. Journal of Palliative Care. Spr 2001;17(1):37-40.
10. O'Brien T, Mortimer PG, McDonald CJ, Miller AJ. A randomized crossover study comparing the efficacy and tolerability of a novel once-daily morphine preparation (MXL capsules) with MST Continus tablets in cancer patients with severe pain. Palliat Med. Nov 1997;11(6):475-482.
11. Ridgway D, Sopata M, Burneckis A, Jespersen L, Andersen C. Clinical efficacy and safety of once-daily dosing of a novel, prolonged-release oral morphine tablet compared with twice-daily dosing of a standard controlled-release morphine tablet in patients with cancer pain: a randomized, double-blind, exploratory crossover study. J Pain Symptom Manage. Apr 2010;39(4):712-720.
12. Sittl R, Nuijten M, Nautrup BP. Patterns of dosage changes with transdermal buprenorphine and transdermal fentanyl for the treatment of noncancer and cancer pain: a retrospective data analysis in Germany. Clin Ther. Aug 2006;28(8):1144-1154.

Opioid Therapy for Cancer-Related Pain
131
Ineligible Language (8):
1. Bono AV, Cuffari S. [Effectiveness and tolerance of tramadol in cancer pain. A comparative study with respect to buprenorphine]. Drugs. 1997;53 Suppl 2:40-49.
2. Knudsen J, Mortensen SM, Eikard B, Henriksen H. Slow-release morphine tablets compared with conventional morphine tablets in the treatment of cancer pain. Ugeskrift for Laeger. 1985;147(9):780-784.
3. Li T-D, Ding, Yong W, Huang, Zhu H. Analgesic Effect of Lysinipinum, Codeine and Pethidine on Cancer Pain. Zhongguo Zhongliu Linchuang. 1995;22(1):39-42.
4. Ozturk T, Karadibak K, Catal D, Cakan A, Tugsavul F, Cirak K. [Comparison of TD-fentanyl with sustained-release morphine in the pain treatment of patients with lung cancer]. Agri. Jul 2008;20(3):20-25.
5. Qiu H, Wang J, Bao J. Clinical evaluation of durogesic in treatment of severe cancer pain. Zhongguo Zhongliu Linchuang. Jan. 20 2001;28(2):118-120.
6. Vaisman MA, Gantsev SK, Gazilov AA, Rudoi SV. [Comparative assessment of chronic pain syndrome treatment methods in patients with small pelvis neoplasms]. Anesteziol Reanimatol. Jul-Aug 1996(4):31-35.
7. Xu G, Duan L, Deng Y, et al. Post-market evaluation of fentanyl transdermal system on cancer pain. Zhongguo Zhongliu Linchuang. Apr. 20 2003;30(4):264-272.
8. Yao WX, Zhou H, Wang LY, Wei Y, Liu XY. [Efficacy comparison between morphine sulfate controlled-released tablet and morphine hydrochloride sustained-released tablet in treating cancer pain]. Ai Zheng. Dec 2007;26(12):1357-1359.
Full-text Not Available (10):
1. A comparative efficacy and tolerability study of palladone capsules and MST continus tablets in patients with cancer pain. Data on File. 2000.
2. De Conno F, Ripamonti C, Bianchi M, Gallucci M, Tamburini M, Ventafridda V. A CLINICAL COMPARISON BETWEEN ORAL MORPHINE AND METHADONE IN CANCER PAIN TREATMENT1986.
3. Goudas L, Carr DB, Bloch R, et al. Management of cancer pain. Volume 1. Volume 2: evidence tables (Structured abstract). Agency for Healthcare Research and Quality. 2001:196. http://www.mrw.interscience.wiley.com/cochrane/cldare/articles/DARE-12002008296/frame.html.
4. Houde RW. Clinical analgesic studies of hydromorphone. Advances in Pain Research and Therapy. 1986;8:129-135.
5. Kaiko RF, Savarese JJ, Goldenheim PD. CONTROLLED-RELEASED MORPHINE IN CHRONIC CANCER PAIN1986.
6. Moriarty M, McDonald CJ, Miller AJ. A randomised crossover comparison of controlled release hydromorphone tablets with controlled release morphine tablets in patients with cancer pain. Journal of Clinical Research. 1999;2(1-8):1-8.
7. Pan HJ, Zhou RY, Du M, Zhang RF, Lu YY. Comparative study of the analgesic effect of morphine sulfate and morphine HCl tablets in treatment of 84 patients with moderate to severe cancer pain. Chinese Journal of New Drugs. 2004;13(Jan):68-69.
8. Song H, Kim D, Ahn J, et al. The dosing frequency of sustained-release opioids and the prevalence of end-of-dose failure in cancer pain control: a Korean multicenter study. EJC Supplements. Sep 2009;7(2):184.

Opioid Therapy for Cancer-Related Pain
132
9. Stambaugh JEJ, McAdams J. COMPARISON OF THE ANALGESIC EFFICACY AND SAFETY OF ORAL DOSES OF NALBUPHINE AND ACETAMINOPHEN ALONE AND IN COMBINATION TO PLACEBO IN PATIENTS WITH CHRONIC CANCER PAIN. Clinical pharmacology and therapeutics. 1985;37(2):231.
10. Xue P, Cai X, Wang LW. Analysis of therapeutic effects and pharmacoeconomics of oxycodone acetaminophen tablets and morphine sulfate controlled-release tablets in the treatment of advanced cancer pain. Vol 17:1967.
Published As Abstract Only (24):
1. Ahmedzai S, Brooks DJ. Transdermal fentanyl vs oral morphine in cancer pain. Journal of Palliative Care. Win 1995;11(4):62-62.
2. Babul N, Dhaliwal H, Sloan P, et al. Analgesic efficacy and safety of controlled release codeine and placebo in cancer pain. Clinical pharmacology and therapeutics. 1995;57(2):137.
3. Blokker MB. Methadone experience in opioid rotation for patients with cancer pain. Journal of Palliative Care. Fal 1999;15(3):61-61.
4. Brooks IM, Clark V, Blumenreich MS, Dejager RL. CONTINUOUS RELEASE MORPHINE SULFATE TABLETS IN CANCER PATIENTS WITH CHRONIC PAIN. Proceedings American Society of Clinical Oncology Annual Meeting. 1986;5:251.
5. Cherry DA, Gourlay GK, Cousins MJ. A COMPARATIVE STUDY OF THE EFFICACY AND PHARMACOKINETICS OF ORAL METHADONE AND MORPHINE IN THE TREATMENT OF CANCER PAIN. Pain. 1984(SUPPL. 2):S202.
6. Darke A, Moulin D, Provencher L, Laberge F, Harsanyi Z, Babul N. Efficacy, safety and pharmacokinetics of controlled release morphine suppositories and tablets in cancer pain. Clinical pharmacology and therapeutics. 1995;57(2):165.
7. Goldenheim PD, Savarese JJ, George E. MANAGEMENT OF LUNG-THORACIC CANCER PAIN WITH CONTROLLED-RELEASE MORPHINE SULFATE TABLETS. American Review of Respiratory Disease. 1987;135(4 PART 2):A243.
8. Hanks GW, Trueman T. CONTROLLED RELEASE MORPHINE TABLETS IN CHRONIC CANCER PAIN. Pain. 1984(SUPPL. 2):S406.
9. Holdsworth MT, Plezia PM, Davis A, Harinder RN, Garewal S, Clements W. AN EVALUATION OF SUSTAINED-RELEASE MORPHINE IN CHRONIC CANCER PAIN. Pharmacotherapy. 1989;9(3):178.
10. Kaiko R, Lacouture P, Hopf K. Analgesic onset and potency of oral controlled-release (CR) oxycodone and CR morphine. Clin Pharmacol Ther. 1996;59:130.
11. Khojasteh A, Evans W, Reynolds RD, Savarese J, Thomas G. SAFETY AND EFFICACY OF SLOW-RELEASE MORPHINE SULFATE TABLETS IN CANCER PAIN THERAPY. Proceedings American Society of Clinical Oncology Annual Meeting. 1986;5:256.
12. Krant M, Shepherd L. CANCER PAIN MANAGEMENT WITH CONTROLLED-RELEASE ORAL MORPHINE. Proceedings American Society of Clinical Oncology Annual Meeting. 1986;5:251.
13. Krawczeniuk MM, Davis LE, Abraham JL, et al. Controlled-release morphine (MS Contin) tablets vs fentanyl transdermal system (Duragesic) for the outpatient treatment of chronic cancer pain. Pharmacotherapy. 1996;16(3):500.
14. Leppert W. Assessment of analgesia, side effects and quality of life during cancer pain treatment with controlled release tramadol and dihydrocodeine - A prospective, randomized, cross-over trial. Psycho-Oncology. Sep 2007;16(9):S160-S161.
Opioid Therapy for Cancer-Related Pain
133
15. Leppert W. Quality of life during cancer pain treatment with controlled release dihydrocodeine and tramadol. Psycho-Oncology. Jun 2008;17:S218-S218.
16. Levine MN, Sackett DL. CANCER PAIN HEROIN VS. MORPHINE. Clinical Research. 1985;33(2 PART 1):257A.
17. Meissner W, Schwittay A, Lux E, Kleeberg UR, Schneid H. A Pan-European Phase IV Open-label Multicentre Study in Patients With Breakthrough Cancer Pain (BTcP) Treated With Fentanyl Buccal Tablet (FBT) - Preliminary Data From Germany. European Journal of Cancer. Sep 2011;47(Suppl. 1):S226.
18. Sloan P, Dhaliwal H, Arkinstall W, et al. Evaluation of the efficacy and safety of controlled-released codeine and placebo in cancer pain. Anesthesia and analgesia. 1995;80(2 SUPPL.):S453.
19. Sunshine A, Olson N, Colon A, Rivera J, Fitzmartin R, Grandy R. Onset and duration of analgesia for controlled-release vs. immediate-release oxycodone alone and in combination with acetaminophen in postoperative pain. Clin Pharmacol Ther. 1995;57:137.
20. Tawfik M, Elborolossy K, Nasr F. TRAMADOL HYDROCHLORIDE IN THE RELIEF OF CANCER PAIN A DOUBLE BLIND COMPARISON AGAINST SUSTAINED RELEASE MORPHINE. Pain. 1990(SUPPL. 5):S377.
21. Ventafridda V, De Conno F, Tamburini M, Rocca E, Guarise G, Gallucci M. BUPRENORPHINE IN CANCER PAIN A CROSSOVER COMPARISON WITH PENTAZOCINE. Pain. 1984(SUPPL. 2):S408.
22. Ventafridda V, Saita L, Oliveri E, et al. A RANDOMIZED STUDY ON ORAL ADMINISTRATION OF MORPHINE SOLUTION AND SLOW RELEASE MORPHINE SULFATE TABLETS MST IN THE TREATMENT OF CANCER PAIN. Pain. 1987(SUPPL. 4):S157.
23. Walsh TD. CONTROLLED STUDY OF SLOW RELEASE MORPHINE FOR CHRONIC PAIN IN ADVANCED CANCER. Pain. 1984(SUPPL. 2):S202.
24. Watanabe S, Bruera E, Belzile M, Kuehn N, Hanson J. Capsules and suppositories of methadone for patients on high dose opioids for cancer pain. Clinical and Investigative Medicine. 1995;18(4 SUPPL.):B91.
Active Controlled Study (7):
1. Babul N, Provencher L, Laberge F, Harsanyi Z, Moulin D. Comparative efficacy and safety of controlled-release morphine suppositories and tablets in cancer pain. J Clin Pharmacol. Jan 1998;38(1):74-81.
2. Brema F, Pastorino G, Martini MC, et al. Oral tramadol and buprenorphine in tumour pain. An Italian multicentre trial. Int J Clin Pharmacol Res. 1996;16(4-5):109-116.
3. Broomhead A, Kerr R, Tester W, et al. Comparison of a once-a-day sustained-release morphine formulation with standard oral morphine treatment for cancer pain. J Pain Symptom Manage. Aug 1997;14(2):63-73.
4. Bruera E, Palmer JL, Bosnjak S, et al. Methadone versus morphine as a first-line strong opioid for cancer pain: a randomized, double-blind study. J Clin Oncol. Jan 1 2004;22(1):185-192.
5. Deschamps M, Band PR, Hislop TG, Rusthoven J, Iscoe N, Warr D. The evaluation of analgesic effects in cancer patients as exemplified by a double-blind, crossover study of immediate-release versus controlled-release morphine. J Pain Symptom Manage. Oct 1992;7(7):384-392.
6. Klepstad P, Kaasa S, Jystad A, Hval B, Borchgrevink PC. Immediate- or sustained-release morphine for dose finding during start of morphine to cancer patients: a randomized, double-blind trial. Pain. Jan 2003;101(1-2):193-198.
7. Mercadante S, Salvaggio L, Dardanoni G, Agnello A, Garofalo S. Dextropropoxyphene versus morphine in opioid-naive cancer patients with pain. J Pain Symptom Manage. Feb 1998;15(2):76-81.


















