Ophthalmology 2021 - CONTi Symposium
28
10/16/21 1 CONTI Symposium Ophthalmology 2021 1 Animal Ophthalmology Clinic Dallas and Grapevine, TX Robert J. Munger, DVM, DACVO 2 3
Transcript of Ophthalmology 2021 - CONTi Symposium

10/16/21
1
CONTI SymposiumOphthalmology 2021
1
Animal Ophthalmology ClinicDallas and Grapevine, TX
Robert J. Munger, DVM, DACVO
2
3

10/16/21
2
Truth or Dare
A conclusion is the place you got tired of thinking.
4
Corneal Ulcers:When Corneal Ulcers Won’t
Heal or
Understanding Mistakes Before They Happen
5
Problem CorneasThis #*@! cornea just wont heal!
6

10/16/21
3
Problem Corneas
7
Problem CorneasTrue or False?
In this case from the preceding slide the problem has been present for 5 weeks.
Multiple punctate or grid keratotomy would be a good treatment for this ulcer?
8
Problem Corneas
This is a cat that has ongoing keratitis of 3 weeks duration and is developing corneal erosions. True or False. MPK would be a good treatment for this ulcer?
9

10/16/21
4
Problem CorneasThis corneal ulcer has been present for 48 hours. True or false?MPK would be a good treatment for this ulcer.
10
Problem Corneas
This is the eye of a 14 year old dog with recurrent corneal erosions/ulcers.True or False? MPK would be a good treatment for this ulcer?
11
Problem CorneasThis is the eye of a 14year-old shepherd cross with a corneal ulcer of 1 week duration. True or False? MPK would be a good treatment for this ulcer?
12

10/16/21
5
Problem Corneas
13
Problem Corneas
True or False?In the cases from the preceding slide
multiple punctate or grid keratotomy would be a good treatment for those ulcers?
FALSE!!!
14
What’s the Point?! Multiple punctate keratotomy (MPK) or grid
keratectomy (GK) has become one of the most overused and misused treatments of corneal ulcers; lately this includes Alger Brush Debridement (ABD)
! Often detrimental when not used appropriately! Use confined only to true recurrent corneal
erosions ! Should NEVER be used in any
other types of corneal ulcers
15
10/16/21
6
Most Common Mistakes
! Trial and error antibiotic therapy! Failure to recognize the type/origin of an ulcer! Failure to recheck promptly! Inappropriate debridement and treatments– Failure to recognize underlying cause (eg. repeated
debridement of eye with KCS, exposure keratitis, etc.)
– Herpetic disease in cats– Rare fungal infetions
16
What Prevents Healing?! Infection! Foreign bodies and other irritants! Conformation! Physiologic interference– Recurrent erosions– Corneal degeneration– Host factors – MMPs, proteolytic enzymes
17
Target Identification
18
10/16/21
7
Problem Corneas: Goals
!Understand common and potential pathogens!Understand pathophysiology (disease process)!Understand species and breed variations!Develop rational therapeutic measures!Evaluate response to your plan
19
Problem Corneas: Mode of Infection
!Primary infections rare – except viral disease
!Bacteria and fungi require pre-existing damage to cornea
20
Problem Corneas: Pathogens
! Viral – Rare with dendritic or geographic erosions
! Bacteria – Pseudomonas, E. coli, Proteus, Streptococcal Staphylococci
! Fungi - Rare
! Viral – Common! Dendritic and geographic erosions
! Mycoplasma; Chlamydophila
! Bacteria – similar to dogs
! Fungi - Rare
Canine Feline
21
10/16/21
8
Secondary Refractory Erosions
! Trichiasis, distichiasis, ectopic cilia, foreign body
! Entropion, lagophthalmos, exposure keratitis! Tear film abnormalities! Neurotrophic or neuroparalytic keratitis! Corneal sequestrum! Herpetic keratitis! Corneal edema/bullous keratopathy
22
What’s In A Name?Recurrent Erosions
! a.k.a. recurrent epithelial erosions, Boxer ulcers, spontaneous chronic corneal epithelial defects (SCCED)
! Middle-aged dogs! Loose epithelial edges! Stroma not involved! Usually present >1-2 weeks
Indolent Ulcers! Slow to develop, heal or
progress ± pain; persistent! For this lecture: Any slow-
healing ulcers that are not recurrent epithelial erosions
! No loose edges; stroma may be affected
! Any age may be affected
23
Recurrent Corneal Erosions: Classical Features
! Erosions may be quite large when loose epithelium is debrided.
! Fluorescein spreads under loose epithelium.! Corneal vascularization may be mild to severe.! When final healing occurs it is rare for the same
eye to be involved twice.! Fellow eye within a year.
24

10/16/21
9
Recurrent Corneal Erosions
25
Recurrent Erosions
26
Recurrent Erosions
27
10/16/21
10
Pathogenesis of Recurrent Erosions
! Incompletely defined! Disorganized epithelial architecture
(dysmaturation)! Absent or poorly organized basement
membrane and adhesion complexes! Acellular adjacent stromal ! Variable stromal fibroplasia, cellular infiltrates,
& vascularization
28
True or False – If a recurrent erosion is not healing, a different antibiotic should be initiated.
FALSE! They are not infected!!!
29
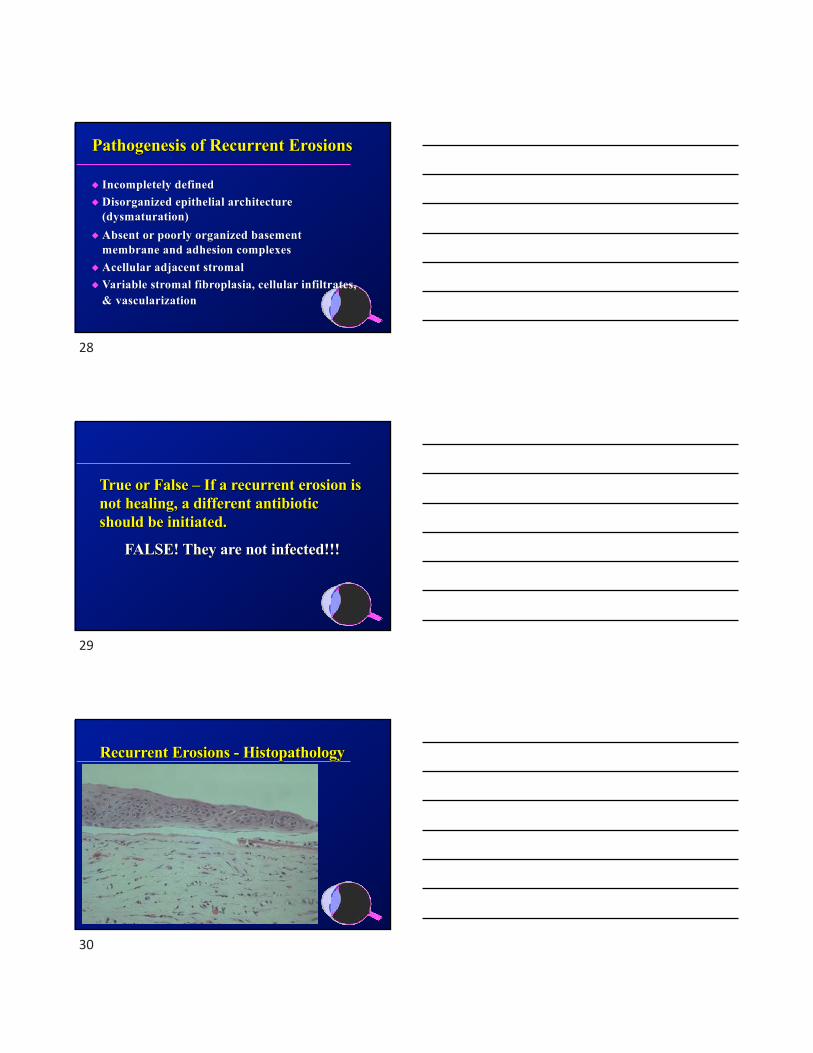
Recurrent Erosions - Histopathology
30

10/16/21
11
EM – Basement Membrane DZ
31
MPK & Grid Keratotomy
32
MPK & Grid Keratotomy
33

10/16/21
12
Alger Brush with Diamond Burr
34
True or False - When a recurrent erosion has not healed within 5 days after performing a multiple punctate keratotomy the procedure should then be repeated.
False!Allow at least 2 weeks to pass before
repeating.
35
Refractory Erosions – Herpetic
36

10/16/21
13
True or False – Multiple punctate keratotomy or grid keratotomy should be
performed when a cat has a chronic recurrent erosion.
FALSE!!! Put down the needle and step away from
the cat!
37
Which of the following is the best topical antibiotics for cats?
A. Neomycin, polymyxin B, bacitracin
A. Erythromycin
B. Terramycin
C. Neomycin, polymyxin B, 0.1% dexamethasone
38
Secondary Refractory Erosions
39

10/16/21
14
Secondary Refractory Ulcers
40
Senile Corneal Degeneration
"Calcium &/or lipid depositions.
"Initial superficial ulcers
"Deep slough ±corneal perforation
41
Rx: Senile Corneal Degeneration
" Topical 1% EDTA
" Topical antibiotics
" Keratectomy +/-
corneal graft or
conjunctival flap
42

10/16/21
15
Problem CorneasCorneal Endothelial Decompensation
(Degeneration/Dystrophy or Secondary to Damage to Endothelium
43
Corneal Endothelial Dystrophy! Boston terriers (5-9 years)! Chihuahuas (6-13 years) ! Dachshunds (8-11 years) ! Possibly in Basset hounds ! Familial - unknown mode of inheritance
44
Corneal Endothelial Dystrophy
45

10/16/21
16
Corneal Endothelial Dystrophy/Degeneration
! Hypertonic saline (5%) - Muro 128â
! Topical/systemic steroids in immune mediated disease and inflammation
! Systemic doxycycline
Medical Therapy Disappointing
46
Corneal Endothelial Dystrophy/Degeneration
Past! Thermal keratoplasty in refractory cases! Homologous penetrating keratoplasty (high risk of
graft rejection)Present
! Keratoleptynsis (Gundersen Flaps)Future
! Corneal Endothelial Transplant EK – DSEK vs. DMEK)
Surgical Therapy
47
Thermal Keratoplasy
48

10/16/21
17
Keratoleptynsis
! 15 year old FS G. Ret.
! 6 weeks postop.! Treated initially for REE! Painful bullous
keratopathy resolved
49
Keratoleptynsis
Mandy – 9 year-old FS Boston terrier 5 months postop.
50
Gundersen flaps deteriorate over time !!!
! Superficial Keratectomy and Conjunctival Advancement Hood Flap (SKCAHF) for the
Management of Bullous Keratopathy: Validation in Dogs With Spontaneous Disease! Horikawa, T; Thomasy, S; et al. Cornea:
2016:35(10); 1295-1304Conclusions: ”…The increase in corneal thickness
over time, after performing SKCAHF, is likely because of progressive endothelial
decompensation.…”
WE AREN’T CURING ANYTHING !!!
51
51

10/16/21
18
DSEK vs. DMEK! Advantages – Replaces defective endothelium.
Lower graft rejection than full-thickness corneal transplant
! DSEK (Descemet’s Stripping Endothelial Keratoplasty) – Implants the back 20-30% of donor cornea
! DMEK (Descemet’s Membrane Endothelial Keratoplasty) – Implants Descemet’s membrane and endothelium.
52
DMEK in Human
53
“Lucky” Stroup10y old Boston Terrier
After3/26/19
790Microns
1-day post graft7/26/17
Courtesy of Dr. Micki Armour
54

10/16/21
19
“Tebah” Stineman1y old Tibetan Terrier
Before 8/21/18
After4/12/19
1,670 microns
660microns
Courtesy of Dr. Micki Armour
55
Graft Rejections - All is Not Roses! Poor patient and client selection– Ability to perform follow up appointments
effectively– Compliance with eye drops and medical protocol– Excessive keratitis
! Inability to visualize ! Other causes
Courtesy of Dr. Micki Armour
56
Luna Mosser: July 2018Courtesy of Dr. Micki Armour
57

10/16/21
20
Luna Mosser: August 2018Courtesy of Dr. Micki Armour
58
Corneal Infection! Preceded by epithelial damage! Bacterial production of proteolytic &
collagenolytic enzymes and toxins - progression of the ulcer
! Neutrophils, degenerate epithelial cells & fibroblasts produce proteolytic enzymes which can contribute to keratomalacia
! Fungi can penetrate into healthy stroma
59
Deep Corneal Ulcers
Progression of ulcers due to degeneration of the cornea
and/or infection with production of enzymes & toxins which destroy the
corneal stroma
60

10/16/21
21
Deep Progressive Ulcers!Always assume infection but remember host
defense factors as well!No room for half measures!Aggressive therapy and timely rechecks
#Anti-collagenolytic/anti-proteolytic therapy#Antibiotics – Topical and systemic#Recheck in 24 hours#Anti-inflammatory and pain therapy#Surgery preferably when infection controlled
61
Potentiation of Infection! Corticosteroids and NSAID’s inhibit immune
response and potentiate activity of proteolytic and collagenolytic enzymes
! Cyclosporine inhibits cell mediated immunity but not acute inflammatory response > contraindicated in fungal and viral keratitis but not in bacterial infections
62
Bacterial Ulcers - Diagnosis
! Clinical signs: pain, exudates and infiltrates, hypopyon, blepharospasm, photophobia, miosis
! Gram stains of corneal scrapings of ulcer edge! Culture and sensitivity early whenever you
suspect infections!!!! There can be some wicked bacteria involved!MRSA and MRSP!Stenotrophomonas maltophilia (Gm -)!Capnocytophaga sp. (Say whaaaatttt???)
63

10/16/21
22
Antibiotic Rx of Bacterial Ulcers! Initial intense topical broad spectrum antibiotic
altered as indicated by culture sensitivity! Staphylococci - Cephalothins, quinolones,
bacitracin, gentamicin! Streptococci - CHPC, erythromycin, penicillins,
quinolones! Pseudomonas & E. coli - gentamicin,
tobramycin, quinolones, amikacin
64
Adjunctive Rx of Bacterial Ulcers
! Systemic antibiotics! Topical atropine! Inhibit proteolytic and collagenolytic
enzymes: autologous serum, 5-10% acetylcysteine, 1% EDTA
! Remove necrotic debris! 360-degree conjunctival flaps,
conjunctival pedicle flaps, and other grafts
65
Mycotic Keratitis
!Most common in horses!History of topical inhibitors of cell-
mediated immunity (steroids, CSA)!Injury with vegetative matter or other
source of fungal spores - especially deep penetrating wounds
66

10/16/21
23
Mycotic Keratitis - Diagnosis
! Clinical signs - insidious onset, slow healing erosion, typical appearance of fungal colony -interlacing branches or fuzzy appearance, stromal abscess or yellow-white plaque, severe corneal vascularization, keratouveitis, hypopyon
! Corneal scrapings: center and edges of ulcer, cultures and cytology
67
Diagnostics!Viral – Problematic; false negatives and false
positives with PCR, IFA, etc.; !Bacterial – Gram stains, cytology, culture and
sensitivity on corneal scrapings!Fungal – Cytology; culture on Saborauds-
dextrose slants; sensitivities expensive
68
Superficial Ulcers
69

10/16/21
24
Bacterial Ulcers
70
Bacterial Ulcers
71
Canine Mycotic Keratitis
72

10/16/21
25
Equine Mycotic Keratitis
73
Topical Support Therapy! I-drop™Vet Gel! Optixcare Eye Health;
Lubricant Gels! EyeQ™ Amniotic
Eyedrops! Artificial Tears! Vizoovet™! Remend™ Corneal
Repair Gel
74
Optixcare For Cleaning Lids
75

10/16/21
26
Surgical Options for Ulcers! Conjunctival flaps – pedicle flap/graft, 360-degree flaps! Autologous (transpositional – CCT, etc.) and homologous (free)
corneal grafts ! Amnion and other extracellular matrix (ECM) technology
xenografts– Vetrix® BioSIS - small intestinal mucosa– Acell® - acellular porcine bladder submucosa – Vetrix® EyeQ Ocular Discs and grafts are decellularized
amniotic membrane discs, carefully processed to remove cells and other immunogens.
! Alternatives to surgery?
76
Amnion Allografts in Humans“Amniotic membrane-based allografts are classified as a naturally derived biomaterial and are currently being used in wound and soft tissue repair applications. Characterization of this tissue has revealed many growth factors, cytokines, and protease inhibitors that can play a role in wound repair. Amnion has been shown to stimulate cellular activity including proliferation, migration, and secretion of soluble paracrine factors in vitro, and has also demonstrated the ability to recruit reparative adult stem cells to the site of implantation in vivo. In addition, these allografts have been shown in randomized clinical trials to be effective in healing various dermal and soft tissue wounds.”
(Lei, "Dehydrated Human Amnion/Chorion Membrane (dHACM) Allografts as a Therapy for Orthopedic Tissue Repair", 2017)
77
Amnionic Membrane Grafts! The clinical efficacy has been attributed to its anti-
inflammatory, anti-scarring, and immuno-privileged components that promote rapid corneal re-epithelialization.
! Can be used as either a tissue to be sutured, as an inlay, or as a temporary patch graft as an onlay to cover the damaged ocular surface.
! Vetrix® EyeQ Ocular Discs and grafts are decellularized amniotic membrane discs, carefully processed to remove cells and other immunogens.
78

10/16/21
27
Vetrix® EyeQ Amniotic Eye Drops! Store at room temperature until reconstituted
them refrigerate; discard after 1 month; do not lay on side
! Cost to client ~ $130.00 / vial! “Provides scaffolding for healing”! As an alternative to or an adjunct to surgery
79
Corneal Ulcers - The Bottom Line! Ulcers may progress rapidly (24 hours) to
perforation given the right circumstances! Aggressive early therapy is imperative! Follow up within 24-48 hours ! Use of 3rd ELF’s for progressing ulcers is
poorly conceived.
80
Questions?
81

10/16/21
28
Questions?
82