
Operative and Nonoperative Treatment Approaches for … and Nonoperative Treatment Approaches for...
7
Operative and Nonoperative Treatment Approaches for Lumbar Degenerative Disc Disease Have Similar Long-Term Clinical Outcomes Among Patients with Positive Discography Q3 Justin S. Smith 1 , Gursukhman Sidhu 2 , Ken Bode 2 , David Gendelberg 3 , Mitchell Maltenfort 2 , David Ibrahimi 1 , Christopher I. Shaffrey 1 , Alexander R. Vaccaro 2 INTRODUCTION Chronic back pain, with an annual preva- lence of 15%e45%, results in enormous health-related expenditure without a consistent improvement in physical, mental, and functional health-related outcomes (32). Chronic low back pain has been attributed to degenerative disc disease (DDD) in a subset of patients, and provocative discography has been proposed as a decision-making guide to better select patients who could potentially benefit from interventional/surgical procedures for relief of back pain thought to be secondary to DDD (31). Discography involves injection of a “contrast” material into the disc space to provide information on disk morphology and to assess whether the injection elicits a “provoked” pain response. Although morphologic alter- ations may be readily appreciated on discography, their presence alone does not necessarily implicate the disc as a pain generator (1, 31, 33). As a result, consid- erable importance is given to the provoked pain response, which, when reported by the patient to be similar to their symptomatic pain, is considered as evidence of a symptomatic disk. There is extensive debate in the spine literature with regard to discography, with one of the major concerns being a high false-positive rate of the provoked pain response in asymptomatic and symptomatic individ- uals (5, 7, 8, 24, 40, 52). However, a recent meta-analysis of false-positive studies using the International Spine Intervention Society standard suggested that discog- raphy has a specificity of 0.94, after setting certain patient selection criteria (52). - OBJECTIVE: It remains unclear whether fusion for lumbar degenerative disc disease with positive discography produces better outcomes compared with nonoperative treatment. The aim of this study was to compare outcomes of patients with discography-concordant lumbar degenerative disc disease elect- ing for fusion versus nonoperative treatment. - METHODS: We retrospectively reviewed consecutive patients with back pain and concordant lumbar discogram who were offered fusion. Follow-up ques- tionnaires included pain score, Oswestry disability index, short form-12, and satisfaction scale. Patients were stratified based on whether they elected for fusion or nonoperative treatment. - RESULTS: Overall follow-up was 48% (96/200). Patients lacking follow-up were slightly older (P [ 0.021) and less likely to be smokers (P [ 0.013). Between patients with and without follow-up, there were no significant differences in pain score at initial visit, body mass index, or gender (P ‡ 0.40). The 96 patients for whom follow-up was obtained included 53 in the operative and 43 in the nonoperative groups. At baseline, there were no significant differences between these groups based on age, pain score, body mass index, smoking, or gender (P ‡ 0.25). Mean follow-up was 63 months for operative and 58 months for nonoperative patients (P [ 0.20). The mean pain score at last follow-up improved significantly for operative and nonoperative patients (P < 0.001). At follow-up, operative and nonoperative groups did not differ signifi- cantly with regard to pain scores, Oswestry disability index, short form-12, or satisfaction scale. - CONCLUSIONS: Comparison of long-term outcomes for patients with back pain and concordant discography did not demonstrate a significant difference in outcome measures of pain, health status, satisfaction, or disability based on whether the patient elected for fusion or nonoperative treatment. Key words - Degenerative disc disease - Discogram - Discography - Fusion - Lumbar - Outcomes - Spine - Surgery Abbreviations and Acronyms BMI: Body mass index DDD: Degenerative disc disease HRQOL: Health-related quality of life MCS: Mental component score MRI: Magnetic resonance imaging NRS: Numerical rating scale ODI: Oswestry disability index PCS: Physical component score SF-12: Short form-12 From the 1 Department of Neurosurgery, University of Virginia, Charlottesville, Virginia; 2 Department of Orthopedic Surgery, Thomas Jefferson University, Philadelphia, Pennsylvania; and 3 Department of Orthopedic Surgery, Penn State Milton S. Hershey Medical Center, Hershey, Pennsylvania, USA To whom correspondence should be addressed: Justin S. Smith, M.D., Ph.D. [E-mail: [email protected]] Citation: World Neurosurg. (2013). http://dx.doi.org/10.1016/j.wneu.2013.09.013 Journal homepage: www.WORLDNEUROSURGERY.org Available online: www.sciencedirect.com 1878-8750/$ - see front matter ª 2013 Elsevier Inc. All rights reserved. WORLD NEUROSURGERY - [ -]: -- -,MONTH 2013 www.WORLDNEUROSURGERY.org 1 REV 5.2.0 DTD ĸ WNEU2106_proof ĸ 23 October 2013 ĸ 7:23 pm ĸ ce Peer-Review Reports 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 55 56 57 58 59 60 61 62 63 64 65 66 67 68 69 70 71 72 73 74 75 76 77 78 79 80 81 82 83 84 85 86 87 88 89 90 91 92 93 94 95 96 97 98 99 100 101 102 103 104 105 106 107 108 109 110 111 112 113 114 115 116
Transcript of Operative and Nonoperative Treatment Approaches for … and Nonoperative Treatment Approaches for...

Q3
Peer-Review Reports
12345678910111213141516171819202122232425262728293031323334353637383940414243444546474849505152535455565758
596061
Operative and Nonoperative Treatment Approaches for Lumbar Degenerative Disc6263646566
Disease Have Similar Long-Term Clinical Outcomes Among Patients with Positive
Discography
Justin S. Smith1, Gursukhman Sidhu2, Ken Bode2, David Gendelberg3, Mitchell Maltenfort2, David Ibrahimi1,Christopher I. Shaffrey1, Alexander R. Vaccaro2
-OBJECTIVE: It remains unclear whether fusion for lumbar degenerative discdisease with positive discography produces better outcomes compared withnonoperative treatment. The aim of this study was to compare outcomes ofpatients with discography-concordant lumbar degenerative disc disease elect-ing for fusion versus nonoperative treatment.
-METHODS: We retrospectively reviewed consecutive patients with back painand concordant lumbar discogram who were offered fusion. Follow-up ques-tionnaires included pain score, Oswestry disability index, short form-12, andsatisfaction scale. Patients were stratified based on whether they elected forfusion or nonoperative treatment.
-RESULTS: Overall follow-up was 48% (96/200). Patients lacking follow-upwere slightly older (P [ 0.021) and less likely to be smokers (P [ 0.013).Between patients with and without follow-up, there were no significantdifferences in pain score at initial visit, body mass index, or gender (P ‡ 0.40).The 96 patients for whom follow-up was obtained included 53 in the operativeand 43 in the nonoperative groups. At baseline, there were no significantdifferences between these groups based on age, pain score, body mass index,smoking, or gender (P ‡ 0.25). Mean follow-up was 63 months for operative and58 months for nonoperative patients (P [ 0.20). The mean pain score at lastfollow-up improved significantly for operative and nonoperative patients (P <0.001). At follow-up, operative and nonoperative groups did not differ signifi-cantly with regard to pain scores, Oswestry disability index, short form-12, orsatisfaction scale.
-CONCLUSIONS: Comparison of long-term outcomes for patients with backpain and concordant discography did not demonstrate a significant difference inoutcome measures of pain, health status, satisfaction, or disability based onwhether the patient elected for fusion or nonoperative treatment.
Key words- Degenerative disc disease- Discogram- Discography- Fusion- Lumbar- Outcomes- Spine- Surgery
Abbreviations and AcronymsBMI: Body mass indexDDD: Degenerative disc diseaseHRQOL: Health-related quality of lifeMCS: Mental component scoreMRI: Magnetic resonance imagingNRS: Numerical rating scaleODI: Oswestry disability indexPCS: Physical component scoreSF-12: Short form-12
From the 1Department of Neurosurgery,University of Virginia, Charlottesville, Virginia;
2Department of Orthopedic Surgery, Thomas JeffersonUniversity, Philadelphia, Pennsylvania; and 3Department ofOrthopedic Surgery, Penn State Milton S. Hershey MedicalCenter, Hershey, Pennsylvania, USA
To whom correspondence should be addressed:Justin S. Smith, M.D., Ph.D.[E-mail: [email protected]]
Citation: World Neurosurg. (2013).http://dx.doi.org/10.1016/j.wneu.2013.09.013
Journal homepage: www.WORLDNEUROSURGERY.org
Available online: www.sciencedirect.com
1878-8750/$ - see front matter ª 2013 Elsevier Inc.
676869707172737475767778798081828384858687888990919293949596979899100101102103104105106107108109110111112113114115116
INTRODUCTION
Chronic back pain, with an annual preva-lence of 15%e45%, results in enormoushealth-related expenditure withouta consistent improvement in physical,mental, and functional health-relatedoutcomes (32). Chronic low back pain hasbeen attributed to degenerative discdisease (DDD) in a subset of patients, andprovocative discography has beenproposed as a decision-making guide tobetter select patients who could potentiallybenefit from interventional/surgicalprocedures for relief of back pain thought
All rights reserved.
WORLD NEUROSURGERY- [-]: ---, MON
REV 5.2.0 DTD �
to be secondary to DDD (31). Discographyinvolves injection of a “contrast” materialinto the disc space to provide informationon disk morphology and to assess whetherthe injection elicits a “provoked” painresponse. Although morphologic alter-ations may be readily appreciated ondiscography, their presence alone does notnecessarily implicate the disc as a paingenerator (1, 31, 33). As a result, consid-erable importance is given to the provokedpain response, which, when reported bythe patient to be similar to their
TH 2013
WNEU2106_proof � 23 October 2013 � 7:23 pm
symptomatic pain, is considered asevidence of a symptomatic disk. There isextensive debate in the spine literaturewith regard to discography, with one of themajor concerns being a high false-positiverate of the provoked pain response inasymptomatic and symptomatic individ-uals (5, 7, 8, 24, 40, 52). However, a recentmeta-analysis of false-positive studiesusing the International Spine InterventionSociety standard suggested that discog-raphy has a specificity of 0.94, after settingcertain patient selection criteria (52).
www.WORLDNEUROSURGERY.org 1
� ce

117118119120121122123124125126127128129130131132133134135136137138139140141142143144145146147148149150151152153154155156157158159160161162163164165166167168169170171172173174
175176177178179180181182183184185186187188189190191192193194195196197198199200201202203204205206207208209210
PEER-REVIEW REPORTS
JUSTIN S. SMITH ET AL. DISCOGRAPHY AND FUSION FOR LUMBAR DDD
Multiple studies have tried to determinethe correlation between discographyresults and treatment outcomes (9, 10, 20,26, 30, 37, 46, 51). The results have beeninconsistent, with variable outcomesregarding pain, functionality, and qualityof life. The question whether surgeryshould be performed for back pain relieffor those with a positive discogram stillremains without a clear answer. Someinvestigators recommend surgical inter-vention after a positive discogram only forpatients who also have associatedabnormal magnetic resonance imaging(MRI) findings (37-39). The controversy isfurther compounded by recent trans-lational and clinical evidence documentingdamage and progression of disc degener-ation as a result of dye injection as part ofthe discography procedure (6, 21, 22, 25).Interpretation of evidence regarding effi-cacy of presurgical discography becomesdifficult with divergent views amongvarious investigators.Our objective in the present study was
to assess the long-term clinical outcomesof patients with a positive, concordantlumbar discogram who were offered spinalfusion and either accepted or declined thissurgical treatment. Our hypothesis wasthat, compared with the patients electingfor nonoperative treatment, the patientstreated with lumbar fusion would havebetter health-related quality of life(HRQOL) and satisfaction scores at long-term follow-up.
211212213214215216217218219220221222223224225226227228229230231232
METHODS
This study was a retrospective review ofconsecutive patients who were referred fora diagnostic lumbar discography procedurebetween 2003 and 2009 at a single institu-tion (Thomas Jefferson University, Phila-delphia, Pennsylvania, USA). Inclusioncriteria for the present study were symp-toms of axial low back pain, attemptedconservative therapy for a minimum of 6weeks, and a one level or a two adjacentlevel positive discogram that was concor-dant with lumbar DDD based on MRI. Allpatients expressed interest in surgery andfelt to be surgical candidates beforeobtaining discography. Patients presentingwith discogenic back pain along with othersurgical indications (e.g., spondylolis-thesis, tumor, infection, and stenosis, andpatients who had undergone previous
2 www.SCIENCEDIRECT.com
REV 5.2.0 DTD �
lumbar decompression/discectomy ora previous lumbar fusion) were excluded. Ingeneral, a discogram was ordered afterdocumentation of abnormal MRI findings,and surgery (instrumented lumbar fusion)was subsequently offered to those who hada one level or a two adjacent level positivediscogram that was concordant withlumbar DDD based on MRI scans. Patientswho declined surgical intervention weregenerally offered nonoperative treatmentmodalities, including physical therapy,epidural injections, and medications.Before study initiation, internal reviewboard approval was obtained throughThomas Jefferson University MedicalCenter.For patients meeting inclusion criteria,
medical records from initial presentationwere reviewed, and extracted informationincluded patient age, gender, body massindex (BMI), smoking status, surgicaldates if surgery was performed, andbaseline back pain numerical rating scale(NRS) score. The NRS score ranged from0 to 10, with 0 representing no pain and 10representing the most unbearable pain.This information was collected as part ofthe standard medical record.For the present study, patients were
contacted by telephone and/or mail andasked to complete disability and func-tionality questionnaires including Oswes-try disability index (ODI) (18), satisfactionscale (14, 29), and the short form-12(SF-12) surveys (48). Patients whoprovided incomplete information, denieda telephone interview, or could not becontacted were not included in the presentstudy. Baseline parameters were comparedbetween patients for whom follow-up wasachieved and those for whom follow-upcould not be obtained to assess forpotential confounding factors related tofollow-up.The satisfaction scale includes six
questions regarding satisfaction with theoverall result of the back operation,including pain relief, walking ability,ability to do housework or employment,and strength in the lower extremities andsteadiness in an upright posture (14, 29).These questions are each scored on a 4-point scale: 1 (very satisfied), 2 (somewhatsatisfied), 3 (somewhat dissatisfied), and 4(very dissatisfied). The satisfaction scalescore is obtained by summing the scorefor each answered question and dividing
WORLD NEUROSURGERY, http://
WNEU2106_proof � 23 October 2013 � 7:23 pm
by the number of answered questions.Thus, the final score can range from oneto four.Baseline demographics and NRS pain
scores, as well as outcomes scores atfollow-up, were compared between thepatients treated with lumbar fusion versusthose who declined surgical treatment.Because patients who initially declinedsurgical treatment could subsequentlyelect for surgical treatment, we chose toanalyze the data using two differentapproaches. For the first data analysisapproach, patients were classified into theoperative and nonoperative groups basedon the initial management plan; specifi-cally, patients were classified as operativeonly if they underwent lumbar fusionwithin 6 months of the initial evaluationand discography. All other patients wereclassified into the nonoperative group,including those who elected for lumbarfusion more than 6 months after initialevaluation. For the second data analysisapproach, patients were classified into theoperative group if they were treated withlumbar fusion at any point between thetime of initial evaluation and the time oflast follow-up. Only patients who had notundergone lumbar fusion as of the time oflast follow-up were classified into thenonoperative group.
Statistical AnalysisFrequency distributions and summarystatistics were calculated for all clinical,operative, and radiographic variables. Forcategorical variables, cross-tabulationswere generated, and the Fisher’s exact orPearson c2 test were used to comparedistributions. For continuous variables, t-tests were used to investigate differencesbetween subsets of patients classified bycategorical data. Multiple regressionanalyses were performed using each of theoutcomes measures (NRS pain score, ODI,SF-12 mental component score [MCS], SF-12 physical component score [PCS], andsatisfaction score) as a dependent variableand patient demographic and clinicalparameters as independent variables.Statistical tests were two-sided, and P <0.05 was considered statistically signifi-cant. All data recorded were analyzed by Rversion 2.15.2 software (R Foundation forStatistical Computing, Vienna, Austria;available at: http://www.r-project.org/).
dx.doi.org/10.1016/j.wneu.2013.09.013
� ce
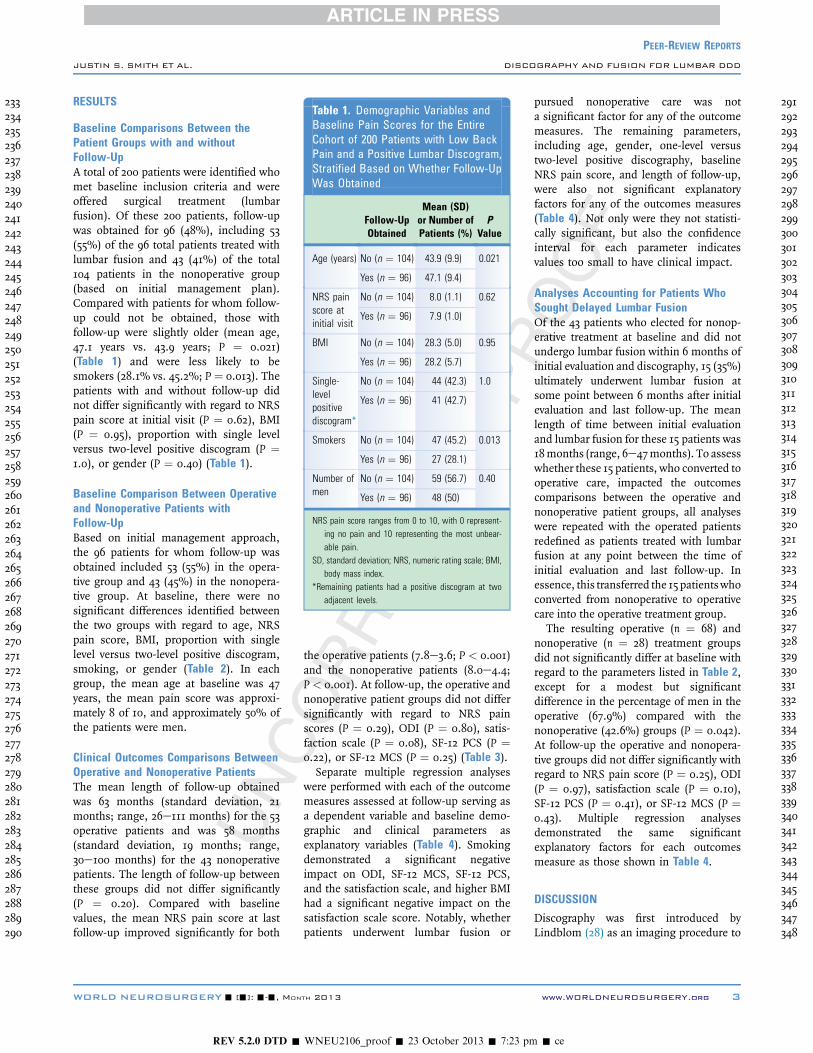
Table 1. Demographic Variables andBaseline Pain Scores for the EntireCohort of 200 Patients with Low BackPain and a Positive Lumbar Discogram,Stratified Based on Whether Follow-UpWas Obtained
Follow-UpObtained
Mean (SD)or Number ofPatients (%)
PValue
Age (years) No (n ¼ 104) 43.9 (9.9) 0.021
Yes (n ¼ 96) 47.1 (9.4)
NRS painscore atinitial visit
No (n ¼ 104) 8.0 (1.1) 0.62
Yes (n ¼ 96) 7.9 (1.0)
BMI No (n ¼ 104) 28.3 (5.0) 0.95
Yes (n ¼ 96) 28.2 (5.7)
Single-levelpositivediscogram*
No (n ¼ 104) 44 (42.3) 1.0
Yes (n ¼ 96) 41 (42.7)
Smokers No (n ¼ 104) 47 (45.2) 0.013
Yes (n ¼ 96) 27 (28.1)
Number ofmen
No (n ¼ 104) 59 (56.7) 0.40
Yes (n ¼ 96) 48 (50)
NRS pain score ranges from 0 to 10, with 0 represent-ing no pain and 10 representing the most unbear-able pain.
SD, standard deviation; NRS, numeric rating scale; BMI,body mass index.
*Remaining patients had a positive discogram at twoadjacent levels.
233234235236237238239240241242243244245246247248249250251252253254255256257258259260261262263264265266267268269270271272273274275276277278279280281282283284285286287288289290
291292293294295296297298299300301302303304305306307308309310311312313314315316317318319320321322323324325326327328329330331332333334335336337338339340341342343344345346347348
PEER-REVIEW REPORTS
JUSTIN S. SMITH ET AL. DISCOGRAPHY AND FUSION FOR LUMBAR DDD
RESULTS
Baseline Comparisons Between thePatient Groups with and withoutFollow-UpA total of 200 patients were identified whomet baseline inclusion criteria and wereoffered surgical treatment (lumbarfusion). Of these 200 patients, follow-upwas obtained for 96 (48%), including 53(55%) of the 96 total patients treated withlumbar fusion and 43 (41%) of the total104 patients in the nonoperative group(based on initial management plan).Compared with patients for whom follow-up could not be obtained, those withfollow-up were slightly older (mean age,47.1 years vs. 43.9 years; P ¼ 0.021)(Table 1) and were less likely to besmokers (28.1% vs. 45.2%; P ¼ 0.013). Thepatients with and without follow-up didnot differ significantly with regard to NRSpain score at initial visit (P ¼ 0.62), BMI(P ¼ 0.95), proportion with single levelversus two-level positive discogram (P ¼1.0), or gender (P ¼ 0.40) (Table 1).
Baseline Comparison Between Operativeand Nonoperative Patients withFollow-UpBased on initial management approach,the 96 patients for whom follow-up wasobtained included 53 (55%) in the opera-tive group and 43 (45%) in the nonopera-tive group. At baseline, there were nosignificant differences identified betweenthe two groups with regard to age, NRSpain score, BMI, proportion with singlelevel versus two-level positive discogram,smoking, or gender (Table 2). In eachgroup, the mean age at baseline was 47years, the mean pain score was approxi-mately 8 of 10, and approximately 50% ofthe patients were men.
Clinical Outcomes Comparisons BetweenOperative and Nonoperative PatientsThe mean length of follow-up obtainedwas 63 months (standard deviation, 21months; range, 26e111 months) for the 53operative patients and was 58 months(standard deviation, 19 months; range,30e100 months) for the 43 nonoperativepatients. The length of follow-up betweenthese groups did not differ significantly(P ¼ 0.20). Compared with baselinevalues, the mean NRS pain score at lastfollow-up improved significantly for both
WORLD NEUROSURGERY- [-]: ---, MON
REV 5.2.0 DTD �
the operative patients (7.8e3.6; P < 0.001)and the nonoperative patients (8.0e4.4;P < 0.001). At follow-up, the operative andnonoperative patient groups did not differsignificantly with regard to NRS painscores (P ¼ 0.29), ODI (P ¼ 0.80), satis-faction scale (P ¼ 0.08), SF-12 PCS (P ¼0.22), or SF-12 MCS (P ¼ 0.25) (Table 3).Separate multiple regression analyses
were performed with each of the outcomemeasures assessed at follow-up serving asa dependent variable and baseline demo-graphic and clinical parameters asexplanatory variables (Table 4). Smokingdemonstrated a significant negativeimpact on ODI, SF-12 MCS, SF-12 PCS,and the satisfaction scale, and higher BMIhad a significant negative impact on thesatisfaction scale score. Notably, whetherpatients underwent lumbar fusion or
TH 2013
WNEU2106_proof � 23 October 2013 � 7:23 pm
pursued nonoperative care was nota significant factor for any of the outcomemeasures. The remaining parameters,including age, gender, one-level versustwo-level positive discography, baselineNRS pain score, and length of follow-up,were also not significant explanatoryfactors for any of the outcomes measures(Table 4). Not only were they not statisti-cally significant, but also the confidenceinterval for each parameter indicatesvalues too small to have clinical impact.
Analyses Accounting for Patients WhoSought Delayed Lumbar FusionOf the 43 patients who elected for nonop-erative treatment at baseline and did notundergo lumbar fusion within 6 months ofinitial evaluation and discography, 15 (35%)ultimately underwent lumbar fusion atsome point between 6 months after initialevaluation and last follow-up. The meanlength of time between initial evaluationand lumbar fusion for these 15 patients was18months (range, 6e47months). To assesswhether these 15 patients, who converted tooperative care, impacted the outcomescomparisons between the operative andnonoperative patient groups, all analyseswere repeated with the operated patientsredefined as patients treated with lumbarfusion at any point between the time ofinitial evaluation and last follow-up. Inessence, this transferred the 15 patientswhoconverted from nonoperative to operativecare into the operative treatment group.The resulting operative (n ¼ 68) and
nonoperative (n ¼ 28) treatment groupsdid not significantly differ at baseline withregard to the parameters listed in Table 2,except for a modest but significantdifference in the percentage of men in theoperative (67.9%) compared with thenonoperative (42.6%) groups (P ¼ 0.042).At follow-up the operative and nonopera-tive groups did not differ significantly withregard to NRS pain score (P ¼ 0.25), ODI(P ¼ 0.97), satisfaction scale (P ¼ 0.10),SF-12 PCS (P ¼ 0.41), or SF-12 MCS (P ¼0.43). Multiple regression analysesdemonstrated the same significantexplanatory factors for each outcomesmeasure as those shown in Table 4.
DISCUSSION
Discography was first introduced byLindblom (28) as an imaging procedure to
www.WORLDNEUROSURGERY.org 3
� ce

Q1
Table 2. Demographic Variables and Baseline Pain Scores for the 96 Patients with LowBack Pain and Positive Discogram for Whom Follow-Up Was Obtained, Stratified Basedon Whether or Not Lumbar Fusion Was Performed as Part of Initial Management Plan(within 6 months of positive discogram)
Treatment Number of PatientsMean (SD) or Number
of Patients (%) P Value
Age (years) Nonoperative 43 47.3 (10.0) 0.87
Operative 53 47.0 (8.9)
NRS pain score at initial visit Nonoperative 43 8.0 (1.2) 0.41
Operative 53 7.8 (0.9)
BMI Nonoperative 43 27.9 (6.6) 0.64
Operative 53 28.5 (4.9)
Single-level positive discogram* Nonoperative 43 17 (39.5%) 0.68
Operative 53 24 (45.3%)
Smokers Nonoperative 43 15 (34.9%) 0.25
Operative 53 12 (22.6%)
Number of men Nonoperative 43 23 (53.5%) 0.68
Operative 53 25 (47.2%)
NRS pain score ranges from 0 to 10, with 0 representing no pain and 10 representing the most unbearable pain.SD, standard deviation; NRS, numeric rating scale; BMI, body mass index.*Remaining patients had a positive discogram at two adjacent levels.
349350351352353354355356357358359360361362363364365366367368369370371372373374375376377378379380381382383384385386387388389390391392393394395396397398399400401402403404405406
407408409410411412413414415416417418419420421422423424425426427428429430431432433434435436437438
PEER-REVIEW REPORTS
JUSTIN S. SMITH ET AL. DISCOGRAPHY AND FUSION FOR LUMBAR DDD
visualize the herniated nucleus pulposusin the 1940s. At present, discography isused by some physicians as a diagnostic
Table 3. Comparison of Clinical Outcome Meand Nonoperative Groups, with the OperativeLumbar Fusion Performed as Part of Initial Mpositive discogram)
Treatment Number
NRS pain score at follow-up Nonoperative
Operative
Oswestry disability index Nonoperative
Operative
Satisfaction scale (1e4) Nonoperative
Operative
SF-12 PCS Nonoperative
Operative
SF-12 MCS Nonoperative
Operative
Pain score ranges from 0 to 10, with 0 representing no pain aSD, standard deviation; NRS, numeric rating scale; SF, Short Form
score.
4 www.SCIENCEDIRECT.com
REV 5.2.0 DTD �
test to help determine whether a patientwith back pain with degenerative diskdisease may be a candidate for surgical
asures at Follow-Up Between OperativeGroup Defined as Those Treated withanagement plan (within 6 months of
of PatientsMean (SD) or Number
of Patients (%) P Value
43 4.4 (2.7) 0.29
53 3.6 (3.0)
43 34.2 (19.3) 0.80
53 35.3 (25.5)
43 2.3 (0.9) 0.08
53 1.9 (1.0)
43 43.8 (7.1) 0.22
53 45.7 (8.0)
43 48.7 (9.9) 0.25
53 46.1 (11.9)
nd 10 representing the most unbearable pain.; PCS, physical component score; MCS, mental component
WORLD NEUROSURGERY, http://
WNEU2106_proof � 23 October 2013 � 7:23 pm
439440441442443444445446447448449450451452453454455456457458459460461462463464
intervention. According to Derby et al.(12), a positive discogram is determined bythe following criteria: a pain severity morethan 6/10, which is concordant with thepatient’s presenting pain, a pressure limitof less than 50 psi, a grade 3 annular tear,and a control disc with pain severity lessthan 6/10. All patients in our study metthese defined criteria and were offeredsurgery for their discogenic pain. Theresults of our study demonstrate signifi-cantly improved pain scores at follow-upfor both the operative and nonoperativetreatment groups and do not demonstratea significant difference for standardizedoutcomes measures of pain, generalizedhealth status, satisfaction, or disabilitybetween the two groups. Collectively,these findings do not support our initialhypothesis, which compared with thepatients electing for nonoperative treat-ment the patients treated with lumbarfusion would have better HRQOL andsatisfaction scores at long-term follow-up.It is important to appropriately interpret
and apply the findings of the present studyas these data only reflect lumbar fusion forDDD. Spinal fusion is commonly used totreat several other conditions, includingtraumatic spinal injuries, spondylolis-thesis, spinal deformities, spine tumors,and spinal instability created by the needfor aggressive bony decompression. Thepresent study does not apply to theseconditions, and many other reportsaddress the application and effectivenessof spinal fusion for these conditions (3, 4,11, 35, 42-45, 49, 50, 53).Treatment options for low back pain
that is attributed to DDD are varied andmay include physical therapy, epiduralinjections, intradiscal electrothermaltherapy, nucleoplasty, and surgery.However, each of these treatments hasmixed results reported in the literature,with inconclusive evidence regardingfunctional outcomes. A systematic reviewof five randomized controlled trialscomparing lumbar fusion surgery tononoperative care for low back paindemonstrated that fusion may not be moreeffective than a structured rehabilitationprogram (17, 34). Surgical managementalso comes with associated risk such asjunctional degeneration (17), pseudarth-rosis, and need for reoperation (15).Clinical utility of a positive discogram is
a controversial topic. Multiple studies have
dx.doi.org/10.1016/j.wneu.2013.09.013
� ce

Table 4. Multiple Regression Analyses of Clinical Outcome Measures Based on Demographic, Clinical, and Treatment Factors Amongthe Combined Cohort of Operative and Nonoperative Patients, with the Operative Group Defined as Those Treated with Lumbar FusionPerformed as Part of Initial Management Plan (within 6 months of positive discogram)
Clinical Outcome Measure at Last Follow-UpCoefficient � standard error (P value)
NRS Pain Score ODI SF-12 MCS SF-12 PCS Satisfaction Scale Score
Smoker 0.599 � 0.345 (0.086) 13.004 � 5.506 (0.020) �6.477 � 2.650 (0.017) �4.845 � �1.799 (0.0085) 0.777 � 0.224 (0.00083)
Age 0.002 � 0.017 (0.89) 0.231 � 0.274 (0.40) �0.035 � 0.132 (0.79) �0.089 � 0.089 (0.32) 0.0006 � �0.011 (0.96)
Men 0.022 � 0.297 (0.94) �2.757 � 4.736 (0.56) 1.487 � 2.279 (0.52) 0.876 � 1.547 (0.57) �0.041 � 0.190 (0.83)
Single-level positivediscogram*
0.033 � 0.329 (0.92) �0.351 � 5.254 (0.95) 2.063 � 2.529 (0.42) �0.187 � 1.716 (0.91) 0.085 � 0.212 (0.69)
NRS pain scoreat initial visit
0.158 � 0.141 (0.27) 1.788 � 2.257 (0.43) �0.839 � 1.086 (0.44) �0.531 � 0.737 (0.47) 0.103 � 0.091 (0.26)
BMI 0.0118 � 0.028 (0.68) 0.515 � 0.452 (0.26) �0.147 � 0.218 (0.50) �0.267 � 0.148 (0.075) 0.038 � 0.018 (0.040)
Length of follow-up 0.006 � 0.008 (0.47) 0.043 � 0.125 (0.73) 0.025 � 0.060 (0.68) 0.032 � 0.041 (0.44) �0.006 � 0.005 (0.22)
Operative treatment �0.231 � 0.299 (0.44) 2.423 � 4.777 (0.61) �3.360 � 2.299 (0.15) 1.223 � 1.560 (0.44) �0.240 � 0.192 (0.21)
Intercept �0.214 � 1.680 (0.90) �10.341 � 26.824 (0.70) 57.850 � 12.909 (< 0.001) 59.349 � 8.763 (< 0.001) 0.379 � 1.076 (0.73)
Gray shading is used to highlight parameters with significant P values.NRS, numeric rating scale for pain (ranges from 0 to 10, with 0 representing no pain and 10 representing the most unbearable pain); ODI, Oswestry disability index; SF, Short Form; PCS, physical
component score; MCS, mental component score; BMI, body mass index.*Remaining patients had a positive discogram at two adjacent levels.
465466467468469470471472473474475476477478479480481482483484485486487488489490491492493494495496497498499500501502503504505506507508509510511512513514515516517518519520521522
523524525526527528529530531532533534535536537538539540541542543544545546547548549550551552553554555556557558559560561562563564565566567568569570571572573574575576577578579580
PEER-REVIEW REPORTS
JUSTIN S. SMITH ET AL. DISCOGRAPHY AND FUSION FOR LUMBAR DDD
examined the role of surgery for patientswith discogram-concordant pain. Ina study conducted by Colhoun et al. (10)the surgical outcomes of patients who hadsurgery after a discogram were assessed.Of the 137 patients who had a positivediscogram, they reported that 89% hada sustained and significant benefit aftersurgical treatment. In contrast, among the25 patients who did not have provocationof symptoms during the discogram, only52% had a sustained and significantbenefit after surgical treatment. Anotherstudy determined surgery for discogram-positive back pain to have satisfactoryoutcomes if associated with a solidarthrodesis (51). Knox and Chapman (26)reported that a single-level anteriorlumbar interbody fusion, when performedfor discogenic back pain, only improvedoutcomes in 53% of the patients. Inanother study that compared patients whounderwent surgery for discogenic backpain, with and without a presurgicalscreening discography, there was nosignificant difference in the degree ofimprovement in ODI scores between thegroups (30). In a retrospective study,Smith et al. (46) assessed outcomes of
WORLD NEUROSURGERY- [-]: ---, MON
REV 5.2.0 DTD �
patients with documented single-leveldiscogenic pain with a positive discogramwho were considered candidates forsurgery but chose conservative therapy andreported improvements in pain anddisability scores in 68% of these patientsat a mean follow-up of 4.9 years. Thislatter study is consistent with the presentstudy, in which patients with a positivediscogram who elected for nonsurgicaltreatment also experienced, on average,significant clinical improvement at long-term follow-up.There have also been studies indicating
that this procedure could potentially harmthe patient. Studies have suggested thatdiscography can cause accelerated discdegeneration. For example, Gruber et al.(23) demonstrated that the radiocontrastdye used for discography may have dele-terious effects affecting viability of humandisc cells.Multivariate analyses in the present
study suggest that smoking significantlynegatively impacts HRQOL as assessed byODI, SF-12 MCS, SF-12 PCS, and satisfac-tion scale score. This is consistent withprevious studies in which smoking hasbeen linked to poorer surgical outcomes
TH 2013
WNEU2106_proof � 23 October 2013 � 7:23 pm
for cervical spine procedures (36) and forlumbar spinal procedures (13, 27, 41, 45,47), including instrumented and non-instrumented. In addition, in the presentstudy, increased BMI was associated withpoorer satisfaction scale scores, but wasnot significantly associated with otheroutcome measures, including NRS painscore, ODI, SF-12 MCS, or SF-12 PCS. Thisis consistent with previous studies sug-gesting that obese patients, surgicallytreated for degenerative lumbar disease,do not have poorer pain, disability andgeneral health outcomes compared withnonobese patients (2, 16, 19), but contrastswith the study of Gepstein et al. (19), inwhich patient satisfaction was assessedand did not appear to be impacted byobesity. Smith et al. (45) reported onfactors that distinguished between thebest and worst outcomes for adult spinaldeformity surgery, and among the fewfactors that distinguished these groupswere smoking and BMI.The primary limitations of the present
study include the retrospective design andthe modest follow-up rate of approxi-mately 50%. However, except for a modestdifference in mean patient age and
www.WORLDNEUROSURGERY.org 5
� ce

581582583584585586587588589590591592593594595596597598599600601602603604605606607608609610611612613614615616617618619620621622623624625626627628629630631632633634635636637638
639640641642643644645646647648649650651652653654655656657658659660661662663664665
PEER-REVIEW REPORTS
JUSTIN S. SMITH ET AL. DISCOGRAPHY AND FUSION FOR LUMBAR DDD
differences in smoking rates, the patientgroups for which follow-up was and wasnot achieved were similar. Because thiswas a retrospective evaluation, there wereno preoperative ODI or SF-12 scoresavailable, but the baseline NRS painscores suggest that the operative andnonoperative groups had similar preoper-ative pain levels. In addition, although theoperative and nonoperative patientsdemonstrated similar outcomes measuresat last follow-up, our data do not permitassessment of the time course over whichthese improvements occurred. It ispossible that patients in either the opera-tive or nonoperative groups may haveachieved improvement faster.A key strength of the present study is
that all patients were evaluated and caredfor by the same physiatrist. In addition,analyses were performed using twoapproaches (with patients grouped basedon initial operative versus nonoperativemanagement plan and with patientsgrouped based on whether surgery was orwas not performed at any point before thelast follow-up).
666667668669670671672673674675676677678679680681682683684685686687688689690691692693694695696
CONCLUSIONS
The present study provides comparison oflong-term outcomes for patients with lowback pain and a positive concordantdiscography and who either elected for oragainst lumbar fusion. The results of ourstudy demonstrate significantly improvedpain scores at follow-up for the operativeand nonoperative treatment groups and donot demonstrate a significant differencefor standardized outcome measures ofpain, generalized health status, satisfac-tion, or disability. Collectively, thesefindings do not support our initialhypothesis comparing the patients elect-ing for nonoperative treatment and thepatients treated with lumbar fusion, whichgroup would have better HRQOL andsatisfaction scores at long-term follow-up.
REFERENCES
1. Agorastides ID, Lam KS, Freeman BJ,Mulholland RC: The Adams classification forcadaveric discograms: inter- and intra-observererror in the clinical setting. Eur Spine J 11:76-79,2002.
2. Andreshak TG, An HS, Hall J, Stein B: Lumbarspine surgery in the obese patient. J Spinal Disord10:376-379, 1997.
6 www.SCIENCEDIRECT.com
REV 5.2.0 DTD �
3. Bridwell KH, Baldus C, Berven S, Edwards C 2nd,Glassman S, Hamill C, Horton W, Lenke LG,Ondra S, Schwab F, Shaffrey C, Wootten D:Changes in radiographic and clinical outcomeswith primary treatment adult spinal deformitysurgeries from two years to three to five years offollow-up. Spine (Phila Pa 1976) 35:1849-1854,2010.
4. Bridwell KH, Glassman S, Horton W, Shaffrey C,Schwab F, Zebala LP, Lenke LG, Hilton JF,Shainline M, Baldus C, Wootten D: Does treat-ment (nonoperative and operative) improve thetwo-year quality of life in patients with adultsymptomatic lumbar scoliosis: a prospectivemulticenter evidence-based medicine study. Spine(Phila Pa 1976) 34:2171-2178, 2009.
5. Carragee EJ, Chen Y, Tanner CM, Truong T,Lau E, Brito JL: Provocative discography inpatients after limited lumbar discectomy:a controlled, randomized study of pain responsein symptomatic and asymptomatic subjects. Spine(Phila Pa 1976) 25:3065-3071, 2000.
6. Carragee EJ, Don AS, Hurwitz EL, Cuellar JM,Carrino JA, Herzog R: 2009 ISSLS Prize Winner.Does discography cause accelerated progressionof degeneration changes in the lumbar disc?:a ten-year matched cohort study. Spine (Phila Pa1976) 34:2338-2345, 2009.
7. Carragee EJ, Tanner CM, Khurana S, Hayward C,Welsh J, Date E, Truong T, Rossi M, Hagle C: Therates of false-positive lumbar discography in selectpatients without low back symptoms. Spine (PhilaPa 1976) 25:1373-1380 [discussion 1381], 2000.
8. Carragee EJ, Tanner CM, Yang B, Brito JL,Truong T: False-positive findings on lumbardiscography. Reliability of subjective concordanceassessment during provocative disc injection.Spine (Phila Pa 1976) 24:2542-2547, 1999.
9. Cohen SP, Larkin TM, Barna SA, Palmer WE,Hecht AC, Stojanovic MP: Lumbar discography:a comprehensive review of outcome studies,diagnostic accuracy, and principles. Reg AnesthPain Med 30:163-183, 2005.
10. Colhoun E, McCall IW, Williams L: Cassar Pull-icino VN: Provocation discography as a guide toplanning operations on the spine. J Bone JointSurg Br 70:267-271, 1988.
11. Dai LY, Jiang LS, Jiang SD: Anterior-only stabili-zation using plating with bone structural autograftversus titanium mesh cages for two- or three-column thoracolumbar burst fractures: a prospec-tive randomized study. Spine (Phila Pa 1976) 34:1429-1435, 2009.
12. Derby R, Kim BJ, Lee SH, Chen Y, Seo KS,Aprill C: Comparison of discographic findings inasymptomatic subject discs and the negative discsof chronic LBP patients: can discography distin-guish asymptomatic discs among morphologicallyabnormal discs? Spine J 5:389-394, 2005.
13. Dewing CB, Provencher MT, Riffenburgh RH,Kerr S, Manos RE: The outcomes of lumbarmicrodiscectomy in a young, active population:correlation by herniation type and level. Spine(Phila Pa 1976) 33:33-38, 2008.
WORLD NEUROSURGERY, http://
WNEU2106_proof � 23 October 2013 � 7:23 pm
14. Deyo RA, Diehl AK: Patient satisfaction withmedical care for low-back pain. Spine (Phila Pa1976) 11:28-30, 1986.
15. Deyo RA, Martin BI, Kreuter W, Jarvik JG,Angier H, Mirza SK: Revision surgery followingoperations for lumbar stenosis. J Bone Joint SurgAm 93:1979-1986, 2011.
16. Djurasovic M, Bratcher KR, Glassman SD,Dimar JR, Carreon LY: The effect of obesity onclinical outcomes after lumbar fusion. Spine(Phila Pa 1976) 33:1789-1792, 2008.
17. Ekman P, Moller H, Shalabi A, Yu YX, Hedlund R:A prospective randomised study on the long-termeffect of lumbar fusion on adjacent disc degener-ation. Eur Spine J 18:1175-1186, 2009.
18. Fairbank JC, Pynsent PB: The Oswestry DisabilityIndex. Spine (Phila Pa 1976) 25:2940-2952[discussion 2952], 2000.
19. Gepstein R, Shabat S, Arinzon ZH, Berner Y,Catz A, Folman Y: Does obesity affect the resultsof lumbar decompressive spinal surgery in theelderly? Clin Orthop Relat Res:138-144, 2004.
20. Gill K, Blumenthal SL: Functional results afteranterior lumbar fusion at L5-S1 in patients withnormal and abnormal MRI scans. Spine (Phila Pa1976) 17:940-942, 1992.
21. Goldie I: Invertebral disc changes after discog-raphy. Acta Chir Scand 113:438-439, 1957.
22. Goldie I: Changes observed in the intervertebraldisc after discography. Acta Pathol MicrobiolScand 42:193-197, 1958.
23. Gruber HE, Rhyne AL 3rd, Hansen KJ,Phillips RC, Hoelscher GL, Ingram JA, Norton HJ,Hanley EN Jr: Deleterious effects of discographyradiocontrast solution on human annulus cell invitro: changes in cell viability, proliferation, andapoptosis in exposed cells. Spine J 12:329-335,2012.
24. Holt EP Jr: The question of lumbar discography.J Bone Joint Surg Am 50:720-726, 1968.
25. Johnson RG: Does discography injure normaldiscs? An analysis of repeat discograms. Spine(Phila Pa 1976) 14:424-426, 1989.
26. Knox BD, Chapman TM: Anterior lumbar inter-body fusion for discogram concordant pain.J Spinal Disord 6:242-244, 1993.
27. Krebs EE, Lurie JD, Fanciullo G, Tosteson TD,Blood EA, Carey TS, Weinstein JN: Predictors oflong-term opioid use among patients with painfullumbar spine conditions. J Pain 11:44-52, 2010.
28. Lindblom K: Technique and results of diagnosticdisc puncture and injection (discography) in thelumbar region. Acta Orthop Scand 20:315-326,1951.
29. Longo UG, Loppini M, Denaro L, Maffulli N,Denaro V: Rating scales for low back pain. Br MedBull 94:81-144, 2010.
30. Madan S, Gundanna M, Harley JM, Boeree NR,Sampson M: Does provocative discographyscreening of discogenic back pain improve
dx.doi.org/10.1016/j.wneu.2013.09.013
� ce

2
697698699700701702703704705706707708709710711712713714715716717718719720721722723724725726727728729730731732733734735736737738739740741742743744745746747748749750751752753754755756757758759760761762763764765766767768769
770771772773774775776777778779780781782783784785786787788789790791792793794795796797798799800801802803804805806807808809810811812813814815816817818819820821822823824825826827828829830831832833834835836837838839840841842
PEER-REVIEW REPORTS
JUSTIN S. SMITH ET AL. DISCOGRAPHY AND FUSION FOR LUMBAR DDD
surgical outcome? J Spinal Disord Tech 15:245-251,2002.
31. Manchikanti L, Glaser SE, Wolfer L, Derby R,Cohen SP: Systematic review of lumbar discog-raphy as a diagnostic test for chronic low backpain. Pain Physician 12:541-559, 2009.
32. Martin BI, Turner JA, Mirza SK, Lee MJ,Comstock BA, Deyo RA: Trends in health careexpenditures, utilization, and health status amongUS adults with spine problems, 1997e2006. Spine(Phila Pa 1976) 34:2077-2084, 2009.
33. Milette PC, Fontaine S, Lepanto L, Cardinal E,Breton G: Differentiating lumbar disc protrusions,disc bulges, and discs with normal contour butabnormal signal intensity. Magnetic resonanceimaging with discographic correlations. Spine(Phila Pa 1976) 24:44-53, 1999.
34. Mirza SK, Deyo RA: Systematic review ofrandomized trials comparing lumbar fusionsurgery to nonoperative care for treatment ofchronic back pain. Spine (Phila Pa 1976) 32:816-823, 2007.
35. Pearson A, Blood E, Lurie J, Tosteson T,Abdu WA, Hillibrand A, Bridwell K, Weinstein J:Degenerative spondylolisthesis versus spinalstenosis: does a slip matter? Comparison ofbaseline characteristics and outcomes (SPORT).Spine (Phila Pa 1976) 35:298-305, 2010.
36. Peolsson A, Peolsson M: Predictive factors forlong-term outcome of anterior cervical decom-pression and fusion: a multivariate data analysis.Eur Spine J 17:406-414, 2008.
37. Resnick DK: Evidence-based guidelines for theperformance of lumbar fusion. Clin Neurosurg 53:279-284, 2006.
38. Resnick DK, Choudhri TF, Dailey AT, Groff MW,Khoo L, Matz PG, Mummaneni P,Watters WC 3rd, Wang J, Walters BC, Hadley MN:Guidelines for the performance of fusion proce-dures for degenerative disease of the lumbarspine. Part 6: magnetic resonance imaging anddiscography for patient selection for lumbarfusion. J Neurosurg Spine 2:662-669, 2005.
39. Resnick DK, Malone DG, Ryken TC: Guidelinesfor the use of discography for the diagnosis ofpainful degenerative lumbar disc disease. Neuro-surg Focus 13:E12, 2002.
40. Simmons JW, Aprill CN, Dwyer AP, Brodsky AE:A reassessment of Holt’s data on: “The questionof lumbar discography”. Clin Orthop Relat Res237:120-124, 1988.
41. Slover J, Abdu WA, Hanscom B, Weinstein JN:The impact of comorbidities on the change inshort-form 36 and oswestry scores followinglumbar spine surgery. Spine (Phila Pa 1976) 31:1974-1980, 2006.
42. Smith JS, Shaffrey CI, Berven S, Glassman S,Hamill C, Horton W, Ondra S, Schwab F,Shainline M, Fu KM, Bridwell K: Improvement ofback pain with operative and nonoperative treat-ment in adults with scoliosis. Neurosurgery 65:86-93 [discussion 93-94], 2009.
WORLD NEUROSURGERY- [-]: ---, MON
REV 5.2.0 DTD �
43. Smith JS, Shaffrey CI, Berven S, Glassman S,Hamill C, Horton W, Ondra S, Schwab F,Shainline M, Fu KM, Bridwell K: Operative versusnonoperative treatment of leg pain in adults withscoliosis: a retrospective review of a prospectivemulticenter database with two-year follow-up.Spine (Phila Pa 1976) 34:1693-1698, 2009.
44. Smith JS, Shaffrey CI, Glassman SD, Berven SH,Schwab FJ, Hamill CL, Horton WC, Ondra SL,Sansur CA, Bridwell KH: Risk-benefit assessmentof surgery for adult scoliosis: an analysis based onpatient age. Spine (Phila Pa 1976) 36:817-824,2011.
45. Smith JS, Shaffrey CI, Glassman SD, Carreon LY,Schwab FJ, Lafage V, Arlet V, Fu KM, Bridwell KH:Clinical and radiographic parameters that distin-guish between the best and worst outcomes ofscoliosis surgery for adults. Eur Spine J 22:402-410, 2013.
46. Smith SE, Darden BV, Rhyne AL, Wood KE:Outcome of unoperated discogram-positive lowback pain. Spine (Phila Pa 1976) 20:1997-2000[discussion 2000-2001], 1995.
47. Trief PM, Ploutz-Snyder R, Fredrickson BE:Emotional health predicts pain and function afterfusion: a prospective multicenter study. Spine(Phila Pa 1976) 31:823-830, 2006.
48. Ware J Jr, Kosinski M, Keller SD: A 12-Item Short-Form Health Survey: construction of scales andpreliminary tests of reliability and validity. MedCare 34:220-233, 1996.
49. Weinstein JN, Lurie JD, Tosteson TD, Hanscom B,Tosteson AN, Blood EA, Birkmeyer NJ,Hilibrand AS, Herkowitz H, Cammisa FP,Albert TJ, Emery SE, Lenke LG, Abdu WA,Longley M, Errico TJ, Hu SS: Surgical versusnonsurgical treatment for lumbar degenerativespondylolisthesis. N Engl J Med 356:2257-2270,2007.
50. Weinstein JN, Lurie JD, Tosteson TD, Zhao W,Blood EA, Tosteson AN, Birkmeyer N,Herkowitz H, Longley M, Lenke L, Emery S,Hu SS: Surgical compared with nonoperativetreatment for lumbar degenerative spondylolis-thesis. Four-year results in the Spine PatientOutcomes Research Trial (SPORT) randomizedand observational cohorts. J Bone Joint Surg Am91:1295-1304, 2009.
51. Wetzel FT, LaRocca SH, Lowery GL, Aprill CN:The treatment of lumbar spinal pain syndromesdiagnosed by discography. Lumbar arthrodesis.Spine (Phila Pa 1976) 19:792-800, 1994.
52. Wolfer LR, Derby R, Lee JE, Lee SH: Systematicreview of lumbar provocation discography inasymptomatic subjects with a meta-analysis offalse-positive rates. Pain Physician 11:513-538,2008.
53. Xu R, Garces-Ambrossi GL, McGirt MJ,Witham TF, Wolinsky JP, Bydon A, Gokaslan ZL,Sciubba DM: Thoracic vertebrectomy and spinalreconstruction via anterior, posterior, orcombined approaches: clinical outcomes in 91
TH 2013
WNEU2106_proof � 23 October 2013 � 7:23 pm
consecutive patients with metastatic spinaltumors. J Neurosurg Spine 11:272-284, 2009.
Conflict of interest statement: Approval for the present studywas obtained through the institutional review board ofThomas Jefferson University. Justin S. Smith is a consultantfor Medtronic, Biomet, Globus; received honoraria forteaching: Medtronic, Depuy, Biomet; Research study groupsupport: Depuy. Christopher Shaffrey is a consultant, patentfor Biomet; received royalties, patent from Medtronic; isa consultant for Depuy; got grant funding from NIH and DOD.Alexander Vaccaro received Health Care Entity Relationshipsand Investments from the following companies: ReplicationMedica / Stock/ Stock Option Ownership Interests; DePuy /Receipt of Royalty Payments; Medtronics / Receipt ofRoyalty Payments; Stryker Spine / Receipt of RoyaltyPayments, Institutional/ Educational Grant; Biomet Spine /Receipt of Royalty Payments; Globus / Receipt of RoyaltyPayments, Stock/ Stock Option Ownership Interests; K-2Medical / Stock/ Stock Option Ownership Interests;Paradigm Spine / Stock/ Stock Option Ownership Interests;Stout Medical / Consulting/Independent Contractor, Stock/Stock Option Ownership Interests; Aesculap / Receipt ofRoyalty Payments; Spine Medica / Stock/ Stock OptionOwnership Interests; Computational Biodynamics / Stock/Stock Option Ownership Interests; Progressive SpinalTechnologies / Stock/ Stock Option Ownership Interests;Spinology / Stock/ Stock Option Ownership Interests; SmallBone Innovations / Stock/ Stock Option Ownership Interests;NeuCore / Stock/ Stock Option Ownership Interests; CrossCurrent / Stock/ Stock Option Ownership Interests;Syndicom / Stock/ Stock Option Ownership Interests; InVivo / Stock/ Stock Option Ownership Interests; FlagshipSurgical / Stock/ Stock Option Ownership Interests;Advanced Spinal Intellectual Properties / Stock/ StockOption Ownership Interests; Cytonics / Stock/ Stock OptionOwnership Interests; Bonovo Orthopaedics / Stock/ StockOption Ownership Interests; Electrocore Stock/ Stock OptionOwnership Interests; Nuvasive / Receipt of RoyaltyPayments, Institutional/ Educational Grant; Gamma Spine /Stock/ Stock Option Ownership Interests; Location BasedIntelligence / Stock/ Stock Option Ownership Interests;FlowPharma / Stock/ Stock Option Ownership Interests;R.S.I Q. /??; Gerson Lehrman Group / Consulting/IndependentContractor; Guidepoint Global / Consulting/IndependentContractor; Medacorp / Consulting/Independent Contractor;Cerapedics / Institutional/ Educational Grant; RothmanInstitute and Related Properties / Stock/ Stock OptionOwnership Interests; AO Spine / Service on ScientificAdvisory Board/Board of Directors/Service on Committees;Innovative Surgical Design / Consulting/IndependentContractor, Service on Scientific Advisory Board/Board ofDirectors/Service on Committees, Stock/ Stock OptionOwnership Interests; Association of Collaborative SpineResearch / Service on Scientific Advisory Board/Board ofDirectors/Service on Committees; Spinicity / Service onScientific Advisory Board/Board of Directors/Service onCommittees, Stock/ Stock Option Ownership Interests.Gursukhman Sidhu, Ken Bode, David Gendelberg, MitchellMaltenfort, David Ibrahimi have nothing to disclose.
Received 9 August 2013; accepted 9 September 2013
Citation: World Neurosurg. (2013).http://dx.doi.org/10.1016/j.wneu.2013.09.013
Journal homepage: www.WORLDNEUROSURGERY.org
Available online: www.sciencedirect.com
1878-8750/$ - see front matter ª 2013 Elsevier Inc.All rights reserved.
www.WORLDNEUROSURGERY.org 7
� ce












![Operative versus Nonoperative Treatment of Acute …...treatment following Achilles tendon rupture and reported a relativeriskofreruptureof0.32(95%confidenceinterval[CI], 0.14 to](https://static.fdocuments.in/doc/165x107/5fa052da28595e20265c2b35/operative-versus-nonoperative-treatment-of-acute-treatment-following-achilles.jpg)





