
Olivier Langeron, MD, PhD Department of Anesthesiology and Intensive Care Pitié-Salpêtrière...
34
Olivier Langeron, MD, PhD Department of Anesthesiology and Intensive Care Pitié-Salpêtrière Hospital Paris, France Guidelines of difficult airway : what’s new ?
-
Upload
jonas-doyle -
Category
Documents
-
view
218 -
download
1
Transcript of Olivier Langeron, MD, PhD Department of Anesthesiology and Intensive Care Pitié-Salpêtrière...

Olivier Langeron, MD, PhD
Department of Anesthesiology and Intensive CarePitié-Salpêtrière Hospital
Paris, France
Guidelines of difficult airway :
what’s new ?

Disclosures
BAXTER
COOK medical
COVIDIEN

Difficult airway management guidelines
SFAR difficult intubation : a collective expertise Ann Fr Anesth Réanim 1996, 2007 (2014)
ASA practice guidelines for management of the difficult airway Anesthesiology 1993, 2003, 2013
Canada the anticipated difficult airway with recommendations for management
Can J Anaesth 1998
UK difficult airway society guidelines for management of unanticipated difficult intubation
Anaesthesia 2004

Difficult airway issues
Anticipate it, to manage it !
How ?
difficult airway algorithms
difficult airway risk factors

Definition of DMV
1993
2003
2000
2005
2006
S
No universal definition
Simplification over time
2 main criteria despite lack of objectivity:
-Difficulties to maintain oxygenation
-Necessity of additional support to perform MV
El-Orbany M and Woehlck HJ Anesth Analg 2009
Definition of difficult intubation (DI)
ASA 2003 : DI if conventionnal laryngoscopy
> 3 attempts or >
10 minutes multiples attempts
SFAR 1996 : DI if conventionnal laryngoscopy > 2
attempts or > 10 minutes and/or alternative technique required after optimization of head position, with or without external laryngeal maneuver
2013 2006

Anticipated DMV
Impossible : - lingual tonsill hyperplasia (LTH) +++
Ovassapian A et al. Anesthesiology 2002
- increased risk after tracheal intubation failures (≥3) Mort T. Anesth Analg 2004
- laryngospasm / bronchospasm
Possible : prediction of DMV Langeron O et al. Anesthesiology 2000
Kheterpal S et al. Anesthesiology 2006

Hypertrophied Lingual Tonsil
Sagittal Sectionof normal Tongueand Larynx
From Jones DH et al. Anesth Analg 1993

Comparison of DMV prediction studies
Langeron 2000
Kheterpal 2006

DMV risk factors
http://www.sfar.org/cexpintubdifficile.html
Increasing risk if at least 2 of these factors:
• Age >55 yr• BMI >26kg/m2
• Jaw protrusion severely limited• Lack of teeth• Snoring• Beard
X 4 risk of difficult intubation with a DMV

0
0
88
Mask ventilation
Laryngoscopy - Intubation
easy impossibleCerebral damageDeath
Benumof JL Anesthesiology 1991
Definition of a difficult airway
Interaction
DMV could be a dynamic process

Multiple TI attempts
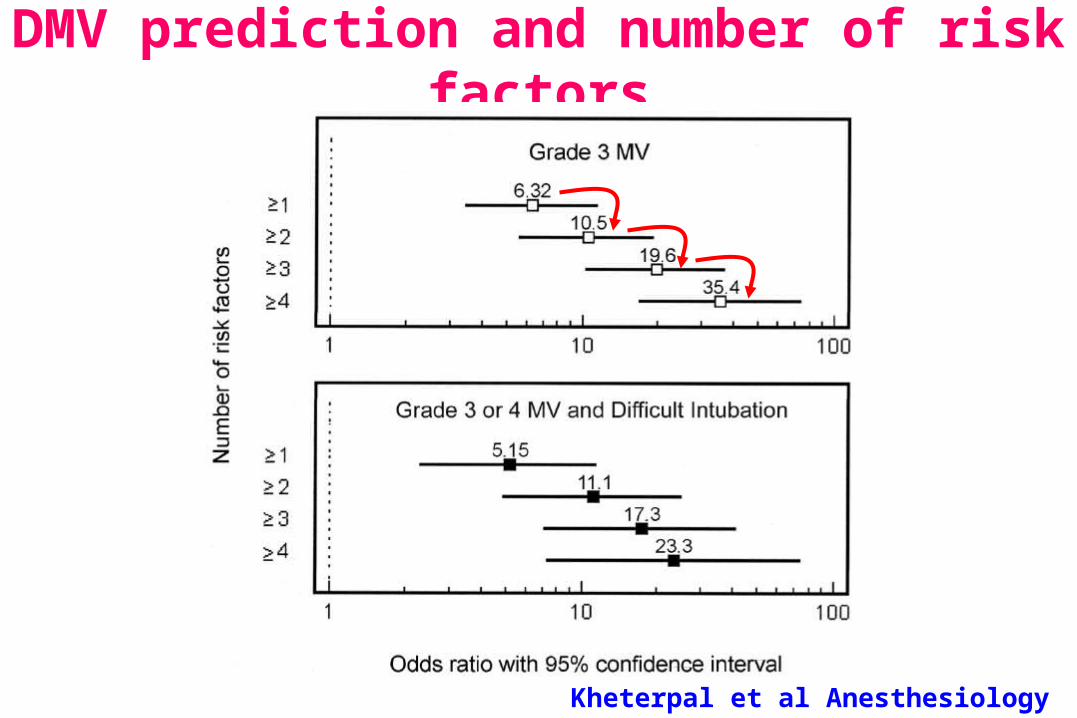
DMV prediction and number of risk factors
Kheterpal et al Anesthesiology 2006

Johnson JO et al Anesthesiology 1999
DMV risk factor and clinical relevance
Patient information +++
Ask to shave the beard ?

Optimization of mask ventilation
Better mask seal : appropriate face mask size, mask ventilation achieved by two persons with a two-handed mask ventilation technique
Use of large oral-pharyngeal / nasal-pharyngeal airways
One person assigned to O2 administration (flush valve…) and patient monitoring (SpO2 …)

DMV risk factor and clinical relevance
lower lip placement standard face mask ventilation

DMV risk factor and clinical relevance
lower lip placement standard face mask ventilation
Expired tidal volume (ml)
median value 0 ml (0–50ml) 400 ml (365–485 ml)
P < 0.001

DI risk factors
http://www.sfar.org/cexpintubdifficile.html
History of a DI ++++Recommended criteria (mandatory +++) :
Mallampati class >IITMD <65mmMO <35mm
Supplementary criteriaLimited jaw protrusion Limited cervical spine mobility
Criteria dependent on context BMI > 35kg/m2
OSA with neck circumference > 45.6cmNeck and/or facial pathologyPre-eclampsia
Strategy
Techniques
Algorithms

Strategy = Algorithms
Oygenation maintenance
Altenative techniques to control the airway
Rationale to use algorithms
To Analyze the difficult airway situation
To elaborate (local) solutions
To broadcast information

90 % ID solved with GEB
98 % patients intubated
100 % patients oxygenated
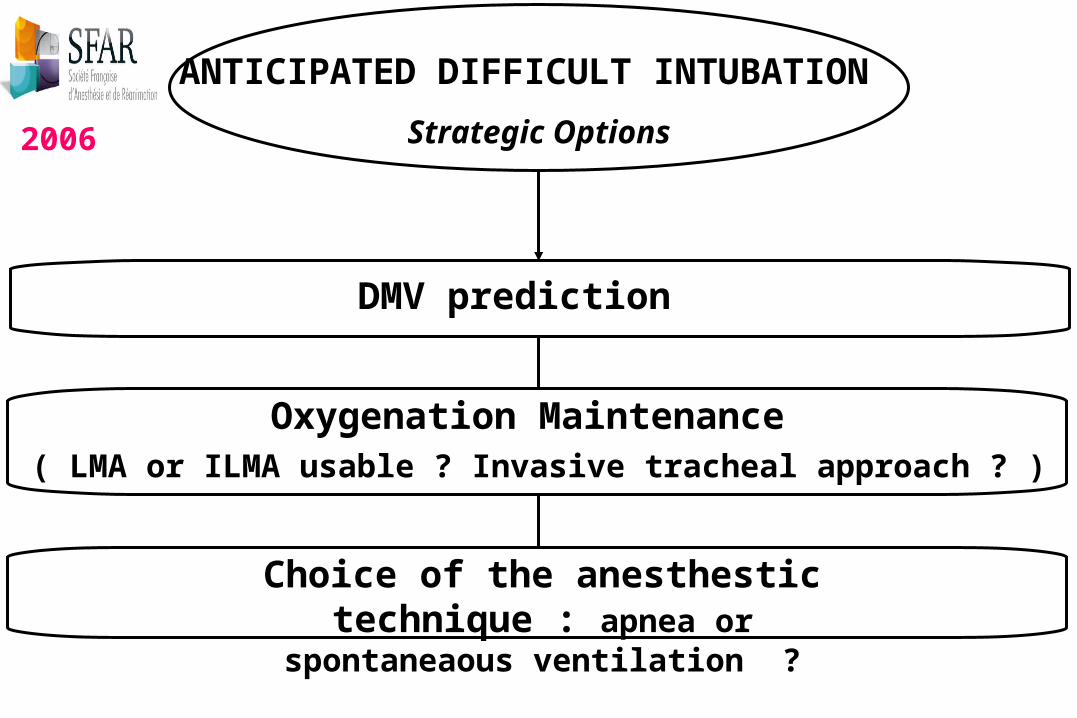
ANTICIPATED DIFFICULT INTUBATION
Strategic Options
DMV prediction
Oxygenation Maintenance ( LMA or ILMA usable ? Invasive tracheal approach ? )
Choice of the anesthestic technique : apnea or spontaneaous ventilation ?
SFAR 20062006

INTUBATION
FAILURE
ILMALMA <30 kg
FAILURE
FIBERSCOPE
FAILURE
Apnea possible Spontaneous Ventilation
Anticipated support
RecoveryTracheal access
If impossible
Mask ventilation efficientSFAR 2006
IntubationIntubation± fiberscope
Intubation
Recovery Recovery
Laryngoscopy 2 trials –
Gum elastic bougie
SFAR 20062006
Videoloaryngoscope

ILMALMA <30 kg
Transtracheal O2
Intubation
FAILURE Contre Indication
Recovery
Success
Others intubation techniques
Intubation
FAILURE
Failure
CRICOTHYROIDOTOMY TRACHEOTOMY
Recovery
OXYGENATIONMask ventilation and/or intubation failures
= SUPPORT IN ANY CASES
Recovery
2006

UNANTICIPATED DIFFICULT INTUBATION
Intubation
Failure ILMA LMA <30 kg
Mask Ventilation
= SUPPORTand DI trolley and Anesthesia maintenance +++
INTUBATION ALGORITHM
OXYGENATION ALGORITHM
efficient inefficient
Laryngoscopy 2 trials - Gum elastic bougie
Ventilation ILMA
inefficientefficient
SFAR 20062006
Videoloaryngoscope

ASA DIFFICULT AIRWAY ALGORITHM Anesthesiology 1993 / 2003 /
Consider attempt LMA

ASA DIFFICULT AIRWAY ALGORITHM Anesthesiology 2013
Videolaryngoscopes added

Algorithm Basic Rules
At each step : consider awaken patient option
Never go a “bridge too far”, never try the “last” option
Algorithm fitting with the patient case, local means and operator abilities
Logistics (material, human resources and task organization) are mandatory

Strategy to manage a difficult airway : what remains !!!
Algorithm (ASA /SFAR) :
Mask ventilation adequate or not ?
Intubation algorithm or oxygenation algorithm
The good question
The good option

Basic airway management
Preoxygenation, SpO2 monitoring
Chin lift and Jaw thrust
Oral / nasopharyngeal airway devices
Limited tracheal intubation attempts (<3)

Conclusion
DMV prediction is mandatory (SFAR guidelines for ex), and the patient should be informed about the risk and the solutions to decrease it
The main goal of airway management is patient oxygenation and not necessary endotracheal intubation
A strategy (including DMV prediction and anesthesia techniques) arising from guidelines and algorithms is always the first step in a difficult airway management

DMV
DI
Oxygenation maintenance

http://www.sfar.org/cexpintubdifficile.html


















