Airway and respiratory management in trauma patientsfiles.medmeeting.org/4783/20.pdf · Pr Olivier...
31
Pr Olivier Langeron MD, PhD Head of Multidisciplinary Intensive Care Unit Hôpital de la Pitié-Salpêtrière Université Pierre et Marie Curie –Paris VI Airway and respiratory management in trauma patients
Transcript of Airway and respiratory management in trauma patientsfiles.medmeeting.org/4783/20.pdf · Pr Olivier...

Pr Olivier Langeron MD, PhD
Head of Multidisciplinary Intensive Care UnitHôpital de la Pitié-Salpêtrière
Université Pierre et Marie Curie –Paris VI
Airway and respiratory management in trauma patients

o Airway management :- Special issues in trauma patient- Basic airway management- Advanced airway management
o Respiratory management - Focus in chest trauma patient
Agenda

Trauma and cause of death
Airway and respiratory management are both mandatory
Sauaia A et al., J Trauma 1995

Difficult environmental situation, prehospital and emergency setting
Head or facial trauma with potential difficult airway access (oedema, hematoma or active bleeding)
Airway and Respiratory management in trauma : What are the issues ?


Scheduled surgery : IDS > 5 : 6%vs
Emergency : IDS > 5 : 16%
%

Mortality related to airway management
(Number of events)
ED 8 % (72%) of all events 11% (41%) of all deaths/BD
TOTAL 184

Airway complications and Causes
Difficult airway and difficult oxygenation

Basic Airway Management
Advanced Airway Management
Airway patencyCervical spine immobilization Mask Ventilation Use of oral or nasal canules Transtracheal O2 Intubation
IntubationLMAFastrachVideolaryngoscopeCricothyroidotomyTracheotomy

Basic airway management
o Chin lift and Jaw thrust, oral / nasopharyngeal airway devices
o Preoxygenation, SpO2 monitoring
o Pulmonary regurgitation prevention (Sellick)
o Limited tracheal intubation attempts (<3)

Benumof JL et al Anesthesiology. 1997
FRC
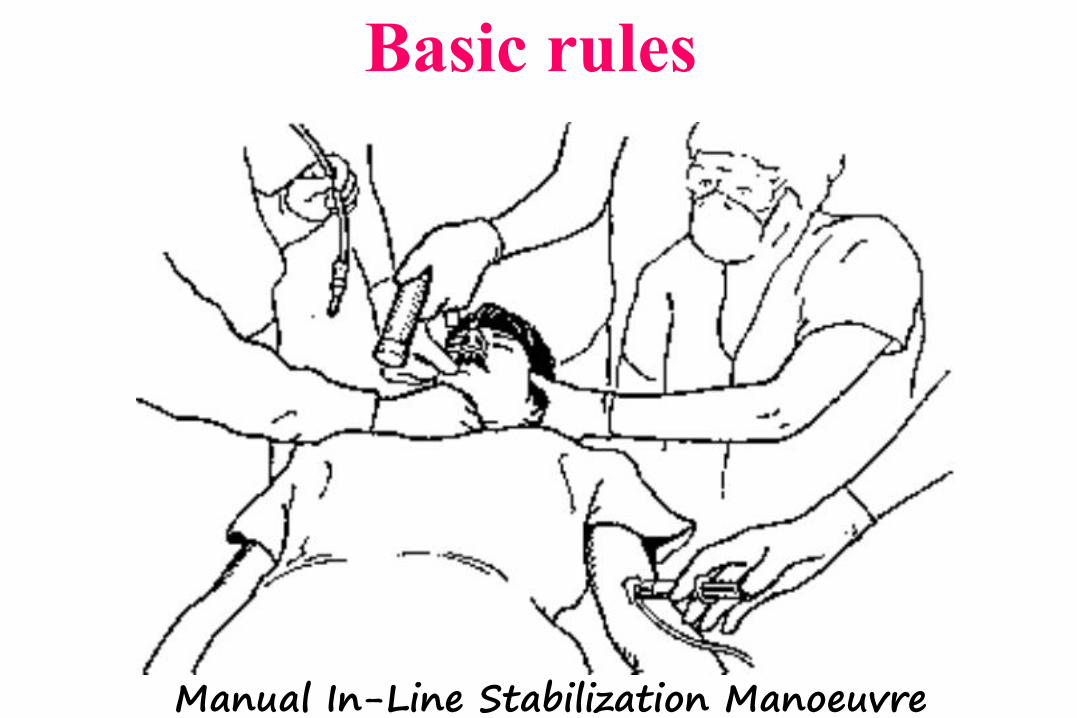
Basic rules
Manual In-Line Stabilization Manoeuvre

Adnet F et al Eur J Emerg Med. 1998
Difficult intubation depending of consciousness level

failed intubation increased significantly in plastic blade group :
17 vs. 3%; P < 0.01

Basic Airway Management
Advanced Airway Management
Airway patencyCervical spine immobilization Mask Ventilation Use of oral or nasal canules Transtracheal O2 Intubation
IntubationLMAFastrachVideolaryngoscopeCricothyroidotomyTracheotomy

Advanced Airway Management : Fastrach



Difficult environmental situation and emergency
Head or facial trauma with potential difficult airway access (oedema, hematoma or active bleeding)
Airway and Respiratory management in trauma : What are the issues ?
Makes tracheal intubation much more difficult !
A strategy should be implemented according oxygenation techniques

Airway control and clinical setting Initially
After surgery
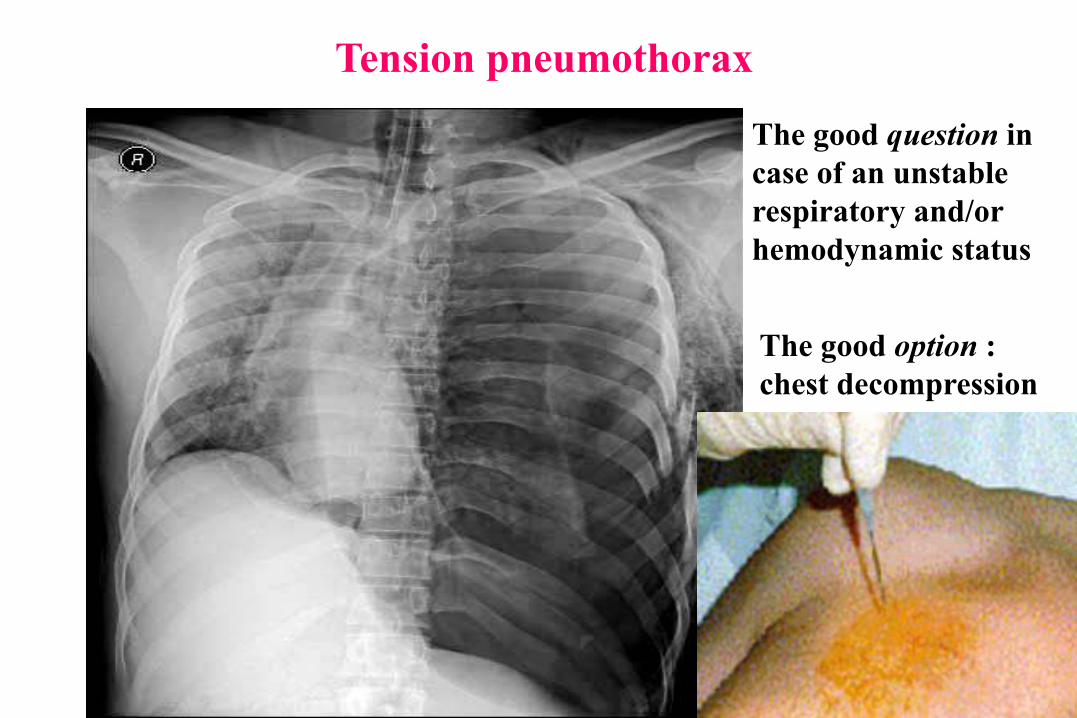
Tension pneumothorax
The good question in case of an unstable respiratory and/or hemodynamic status
The good option : chest decompression

EMERGENCY DECISIONS
INITIAL ASSESSMENT

Imaging in chest trauma : what do we have ? what do we need ?
Bedside techniques
Computed tomography (CT) techniques
Diagnosis
Monitoring
Better understanding disease mechanism
Complementary techniques

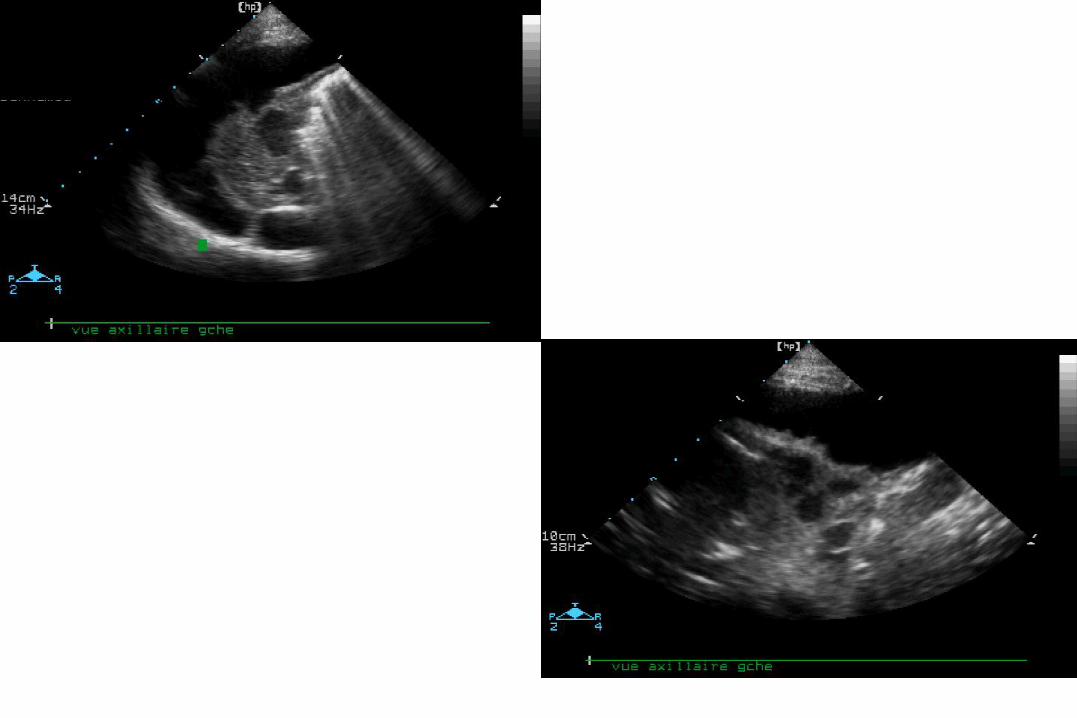
Pneumothorax
Chest X-ray
Tension pneumothorax
Hemothorax

Estimated Volume (ml) = section x h
0 200 400 600 800 1000 1200
Volume drained (ml)
0200400600800
10001200
r2 = 0.722p < 0.001
Remerand F et al. Intensive Care Med 2010
Section
Multiplane ultrasound approach to quantify pleural effusion at the bedside

Chest spiral CT
Pulmonary contusion underestimated by chest X-ray better assessed by Computed Tomography

PEEP should be adjusted to lung morphology
Cqs 41 ml/cmH2O PaO2/FIO2 98 mmHg
Cqs 39 ml/cmH2O PaO2/FIO2 98 mmHg
High PEEP ≥ 15 cmH2O
to recruit the lung
Moderate PEEP ≤ 10 cmH2O

1000
00
250
500
750
10 20 30
Lung volume (ml)
ZEEP
P-V curve depends on :
- the mecanical properties of the lung remaining aerated at end-expiration
- the recruitment curve of nonaerated lung areas
Patients with a « focal » loss of aeration
interpretation of the P-V curve is much more complex
Airway pressure (cmH2O)
Lung overinflation occurs together with recruitment and cannot be detected from the global PV curve
Rouby et al., European Resp Journal, 22 (suppl 42) : 27s-36s , 2003

PULMONARY CONTUSION
Prone position
PEEP trial

Conclusiono Emergency makes airway management more difficult
o A strategy arising from guidelines and algorithms are always the first step to solve a difficult airway
(Maintenance of oxygenation +++)
o Initial chest X-ray/pulmonary echography are useful and respiratory setting is performed at best with CT-scan