Classifications of etio pathogenesis of uveitis, anterior uveitis- dr.k.srikanth, 17.03.16
Upload
elinor-powersCategory
view
222download
3
Ocular Immunology/ Uveitis
Kyle C. McKenna, Ph. D.Associate Professor of Biology and Ophthalmology

HypopyonOcular infiltrate of white blood cells(leukocytes) which settle via gravityto the bottom of the anterior chamber“like sands through the hour glass”
How did the leukocytes get there?
Leukocytes (cells of the immune system travelVia blood and enter the eye via vessels in theiris, ciliary body, choroid, retina, and sclera

Blood Smear
Basophil
MonocyteBand Cell
Eosinophil
Lymphocyte
Lymphocyte
Neutrophil
Neutrophil
1
2
34 5
65
1

Granulocytes
Neutrophil Eosinophil Basophil
Mast Cells
Monocytes
Macrophages
Lymphocytes
B CellsT Cells
T T
CD4+Thelper
CD8+CTL
Innate Immunity Adaptive Immunity
Complement
Antibody

• Immediate• Includes anatomical
and biochemical barriers
• Recognition of conserved pathogen associated molecular patterns (PAMPs)
• No memory generation
• Delayed• Specific recognition of
pathogenic molecules• Memory Generation
Innate Adaptive

PAMP PRRPathogen Recognition Receptor
Lipopolysaccharide (LPS) TLR 4Toll Like Receptor
Double Stranded RNA TLR 3
DAMPDamage associated molecular pattern
DRRDamage Recognition Receptor
HMGB1(High MobilityGroup box 1)
RAGE, TLR 2, 4 and 9Receptor of advanced glycation endproduct
Nonoxidized (reduced) HMGB1 is released by normal cells upon necrotic butNot apoptotic cell death

PAMPs and DAMPs promote inflammation
IL-1IL-6
TNFNitric oxide
IL-8
Increased Cell Surface moleculesMHC Class I & IICD40, CD80, CD86
Produce inflammatory cytokinesIL-12TNF
Activated Antigen PresentingCells Leave via afferent lymphatics
MacsDC
RednessSWELLINGPAIN

Spleen
Secondary Lymphoid Organs

Innate immunity is immediate but alone insufficient for pathogen control

Adaptive ImmunityB-Cells T-Cells
Antigen Receptor: Immunoglobulin TCRRecognition: Proteins, Carbohydrates
Lipids, most any moleculeProcessed Proteins Presented as
Peptides via MHC molecules by APC
ExogenousProteins via
MHC Class II
EndogenousProteins via
MHC Class I
ProfessionalAPC
All Cells inBody
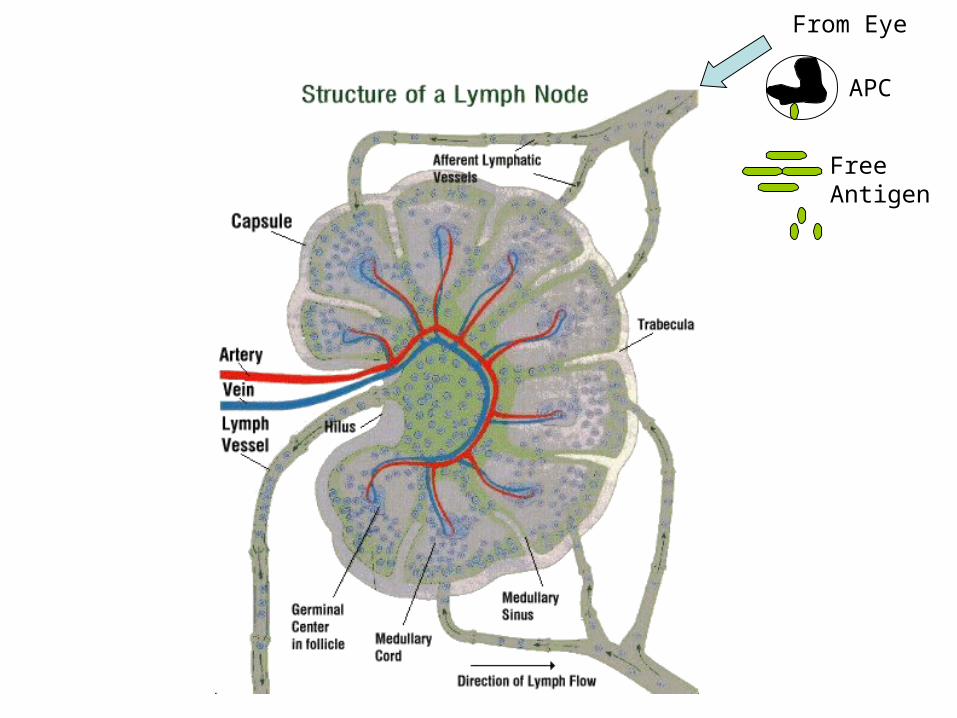
From Eye
APC
FreeAntigen

B
B
B
BB
B
B
B
B
T
T
T
T
T
T
T
T
T
T
TT
T
T
FDC
More ProliferationHere

Clonal Expansion
Diverse RepertoireOf B cells and T cell
Increase NumbersOf Antigen Specific
Clones
Differentiation
Memory Cells
Antibody SecretingPlasma Cells
T helper Subsets
CTL
Process of Expansion and Differentiation takes time which is why AdaptiveImmunity is Delayed
Eff
ecto
rs
APC

CD4+T helper
IL-2
IL-2IFN
CD8+CTL
Lytic granulesContaining Granzyme B Lysis of infected Cells
IFN
B cells
IgG2aViral and Bacterial infections
IL-4, 5, 6, 10
B cells
IgG, IgEExtracellular Helminthic Infections
What determines uniqueThelper differentiation?
PAMPS / APC
APCIL-12
LPS/TLR4
TH1
APCIL-4
Filaria?
TH2

Infections Activate InnateImmunity via PAMPS
T and B cell expansionAnd differentiation occur
Blood Stream
Activated APCLeave eye CarryingPathogenic Molecules
AfferentLymphatics
LymphNode
EfferentLymphatics

What is Type I Hypersensitivity?
Immediate Hypersensitivity
Antibody Mediated (IgE)
IgE molecules are bound by FcEpsilon receptors on Mast Cells
Mast Cells release histamines which promote inflammation
Allergic Conjunctivitis

What is Type II Hypersensitivity?
Antibody Mediated
Cell lysis via Antibody Dependent Cellular Cytotoxicity
Rh Hemolytic anemia in newborns
Sympathetic ophthalmia, Uveitis
CompMAC
Phagocytosis
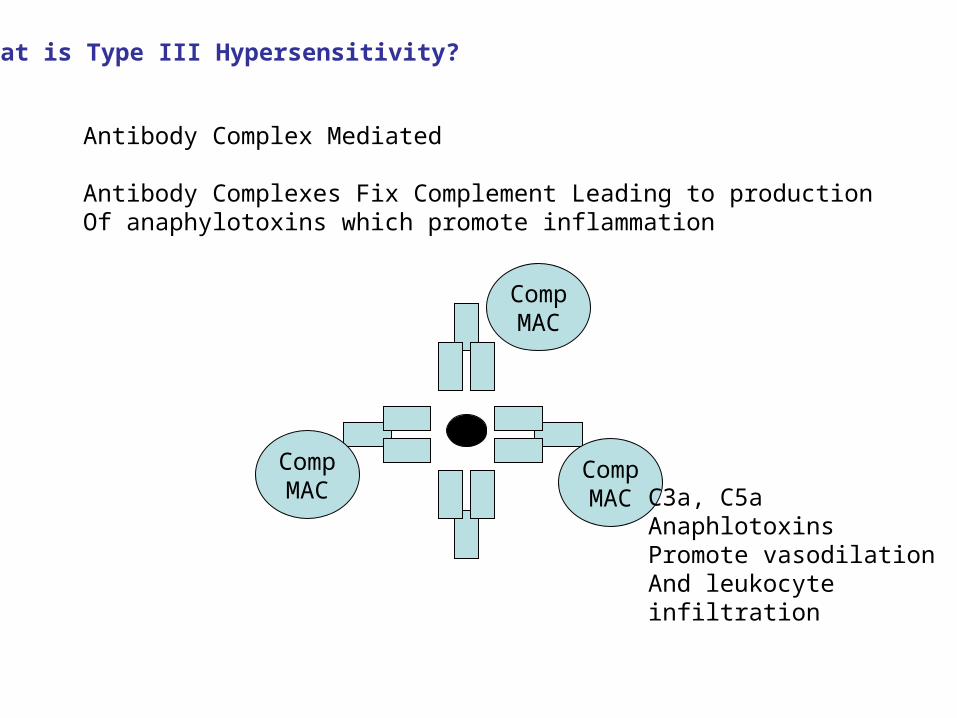
What is Type III Hypersensitivity?
Antibody Complex Mediated
Antibody Complexes Fix Complement Leading to productionOf anaphylotoxins which promote inflammation
CompMAC
CompMAC
CompMAC C3a, C5a
AnaphlotoxinsPromote vasodilationAnd leukocyteinfiltration

What is Type IV Hypersensitivity?
Delayed Type Hypersensitivity
T cell mediated (CD4 TH1 cells)
CD4+ T cells activate macrophages to release inflammatory mediators(TNFa, Nitric Oxide) which causes nonspecific damage of innocent bystanderTissues
Promote infiltration of neutrophils which further enhance inflammation
CD4+T helper MAC
IFN
Nitric OxideTNF

What is Type V Hypersensitivity?
Antibodies are generated which are stimulatory
Graves DiseaseAnti-thyroid stimulating hormone receptor antibodiesstimulate the effects of Thyroid Stimulating Hormone
TSH
TSHR
Antibody

TCR and Immunoglobulin molecules are generated by Random Somatic Rearrangement of gene segments
What is the potential complication of this process?
Generation of TCR and Immunoglobulin molecules that recognize self tissues

T cells expressing TCR with strong reactivity to self antigens are deletedIn the Thymus during T cell development
What is the consequence of overly stringent negative selection?
Decreased Repertoire of the T cell pool
Fact: T cells and B cells are generated with receptors that demonstratesome affinity for self antigens.
Why are we not in a constant state of autoimmunity?
Peripheral tolerance mechanisms

Three Signals are Required for Full T cell activation
3
Cytokines
1. TCR : MHC/peptide2. Costimulatory Molecules3. Cytokine Production
In the absence of three signalsT cell anergy or tolerance is generated
How do PAMPS break tolerance toSelf antigens?
PAMPS increase costimulatory moleculesAnd cytokine expression

UveitisClassic T cell dependent Type IV hypersensitivity response
Infectious (syphilis, tuberculosis, toxoplasma gondii)Noninfectious (self antigens)[mouse models via immunization with IRBP, Retinal S-ag]
Disease Associations made with particular MHC moleculesHLA-B27 : Reiter’s syndromeHLA-B5: Behcet’s DiseaseHLA-29: Birdshot Choroidopathy
How could an immune response to an ocular antigen develop toCause autoimmune uveitis?
Retention of T cells with specificity to ocular antigens due toWeak negative selection in individuals with particular HLA types
Previous infection or trauma primed for ocular antigens in anInflammatory context
Molecular Mimicry (Klebsiella, Chlymidia, Yersinia?)

Ocular Immune PrivilegeCharacterized by prolonged acceptance of foreign immunogenic graftsIn comparison to conventional sites
Corneal Allografts most successful (no matching, minimal immunosuppression required)
Experimentally immunogenic tumors grow progressively in the anteriorChamber but are eliminated by CD8+ T cells when transplanted in theskin

Anatomical Barriers to Host Immune Response
Cornea is avascular
Interior of Eye lacks demonstrable lymphatic drainage
Blood Aqueous Barrier
Blood Retinal Barrier

Biochemical Barriers to Host Immune Response
Aqueous Humor contains Immunosuppressive soluble factors(TGF-b, a-MSH, IL-10, MIF, CGRP, VIP, somatostatin)
Interior Cell Surface expresses Death inducing Molecules(FasL, Trail, PD-1 and PD-2L)
T cell anergy, T cell death, T regulatory generation

Tolerance Induction to Ocular Antigens
Introduction of foreign antigens into the anterior chamber, subretinal spaceAnd vitreous cavity induces systemic tolerance to these antigens
Mediated by the generation of Tregulatory cellsCD4, CD8+