
Occupational lung disease
45
Occupational lung disease CM Barber Consultant Respiratory Physician
Transcript of Occupational lung disease

Occupational lung disease
CM Barber
Consultant Respiratory Physician

Introduction
• What is occupational lung disease?
• What are the common conditions?
• Why is it important?
• What happens to people who get it?
• How should it be prevented?

Introduction
• What is occupational lung disease?

OLD – response to inhaling something at work
• Fume

OLD – response to inhaling something at work
• Dust

OLD – response to inhaling something at work
• Gas or vapour

OLD – response to inhaling something at work
• Mist/aerosol

Wide range of mechanisms • Direct injury (eg acute irritant asthma, pulmonary oedema)
• Infection (eg silicotuberculosis)
• Allergy (eg asthma, EAA)
• Chronic inflammation (eg COPD, bronchiolitis)
• Destruction of lung tissue (eg emphysema)
• Lung or pleural fibrosis (eg asbestos related disease)
• Carcinogenesis (eg lung cancer, mesothelioma)
Minutes
Years
Decades

OLD
Current exposure – Early recognition
– Accurate diagnosis
– Cessation of exposure
– Prognosis improved
– Health versus income
– Loss of employment
– Eg allergic OA
Historical exposure – Recognised years later
– Accurate diagnosis
– Supportive measures
– Little/no impact on prognosis
– Benefits advice
– Often retired
– Eg asbestosis
Wide range of effects
• Effects may be immediate or after a latent interval of months, years or decades
• Variable depending on individual susceptibility (? genetic)
• May occur whilst still at work or after retirement – E.g. silicosis and asbestosis may progress despite not being
exposed, due to lung retention of dust/fibres
• Effects range from mild to very severe (death)
• May be reversible or irreversible
• Some very old, some only recently described

Georgius Agricola.
De Re Metallica (16th Century)
• “If the dust has corrosive qualities, it eats away at the lungs, and implants consumption in the body. In the mines of the Carpathian mountains women are found who have married seven husbands, all of whom this terrible consumption has carried off to a premature death”

OLD
• What are the common conditions?

UK reporting figures

OLD cases
• Why is it important?
• What happens to people who get it?

Occupational
asthma

Occupational asthma - definition
• 90%- asthma induced by
sensitisation (allergy) to an
agent inhaled at work
OR
• 10%- asthma induced by
massive accidental irritant
exposure at work (direct
airway injury)
Occupational asthma
• 9-15% of all adult onset asthma
• UK estimate 1500-3000 new cases per year
• Risk of unemployment (up to one third)
• Loss of earnings
• Chronic ill health
• Early recognition
• Reduce/prevent exposures

Airway inflammation in farmers
Intervention n=32 Control n=10
Dressel et al, Eur Respir J 2007; 30: 545–548

Case study occupational asthma
• 42 male
• Adult-onset asthma
• Increasing severity and treatment
• Symptoms started 2 years after starting new job
• Symptoms better at weekend
• Worked as a baker
• Symptoms recognised within a year of onset due to health surveillance at work

• Normal spirometry
• Work-effect confirmed by PEF
• Positive immunology (flour IgE)
• Diagnosis of baker’s asthma
• OH dept advised to avoid exposure if possible
• Relocated to despatch room
• Asthma improved
• Medication reduced, remained employed
• i.e. good outcome with early diagnosis

Occupational COPD

Case study COPD
• 68 year old male
• Progressive dyspnoea over 5 years
• Breathless on one flight of stairs or carrying groceries
• Smoked age 14-30, max 25 pack years
• Irreversible airflow obstruction, low gas transfer
• CT - emphysema

Case study COPD
• Extremely dusty work (concrete dust)
• Grinding large concrete display tanks as an exhibit
preparatory in an aquarium.
• Also exposed to epoxies and fibreglass.
• Did 6-8 tanks per year x 7 years (1989-94)
• Less exposure 1994-1998, then retired.

Vo
lum
e in
Lit
ers
/Flo
w in
Lit
ers
Seco
nd
-1
F
EV
1 –
FV
C
F
EF
25-7
5
0
0.5
1
1.5
2
2.5
3
3.5
4
4.5
5
88
89
90
91
92
93
94
95
96
97
98
99
00
01
02
03
04
05
06
07
08
FVC
FEV
FEF

Case study - COPD • Patient found to be deficient in alpha 1 antitrypsin
• Genetic condition with increased risk of COPD
• Accelerated lung function decline due to dust exposure
• Fixed airway obstruction
• Permanent disability
• No longer working at time of presentation
• Bad outcome (opportunity to cease exposure missed)

FE
V1 (
% o
f valu
e a
t age 2
5) 100
75
50
25
0
25 50 75
Not exposed or
not susceptible
Stopped at 65
Stopped at 45
Disability
Exposed regularly to
FDGV and susceptible
Death
Age (years)
Lung function decline with time
FDGV = fume/dust/gas/vapour

EAA or HP
ppppppppppppppppppp

EAA or hypersensitivity pneumonitis
• Recognised since 1932 in farmers
• Allergic sensitisation
• Occupational or environmental
• Acute (self-limiting febrile response)
• Sub-acute
• Chronic (irreversible pulmonary fibrosis)

Occupational causes
• Microorganisms
– Farmers, wood pulp workers, sewage workers, mapple bark
strippers, cheese washers, paprika splitters, mushroom
workers, sequoiosis, suberosis, bagassosis, dog house
disease
• Animals
– Birds, wheat weevil, fish meal, rodent handlers
• Vegetation
– Coffee, wood
• Chemicals
– Vineyard sprayers, insecticide, isocyanates, anhydrides,
plastics

Bird Fanciers lung • 22 year old non-smoker
• SOBOE on exertion 2 years
• Weight loss of 1 stone
• Parrot in student house
• +ve avian precipitins
• HRCT sub-acute EAA
• Improvement over 3 years
• Gas transfer 52% to 78%
• Prognosis depends on early
recognition and avoiding exposure

Remove allergen to avoid irreversible fibrosis

Asbestos-related lung disease
• Benign pleural disease
• Pulmonary fibrosis
• Cancer

• Asbestos imported since 1880s
• Asbestosis described in 1920s
• Asbestos used widely in UK until 1980s

Pleural plaques
• Layers of collagen, often calcified
• Latency 30 years
• Harmless marker of exposure
• Not pre-malignant
• Aetiology unclear

Diffuse pleural thickening
• Follows benign effusion
• Obliteration of costophrenic angle
• Long latency
• Lung expansion restricted by thickened pleura
• Breathlessness, respiratory failure
• No effective treatment
• May progress slowly (without further exposure)

Asbestosis
• Scarring of lung tissue
• Long latency (decades)
• History of heavy exposure
• No effective treatment
• May progress (without further exposure)
• Progressive breathlessness
• Respiratory failure

Case study lung cancer
• 84 year old man
• GP abnormal CXRay
• Increasing breathlessness
• Ex-smoker (30 pack years)
• Retired electrician - 30 years
exposure to asbestos
• CT asbestosis and lung
cancer
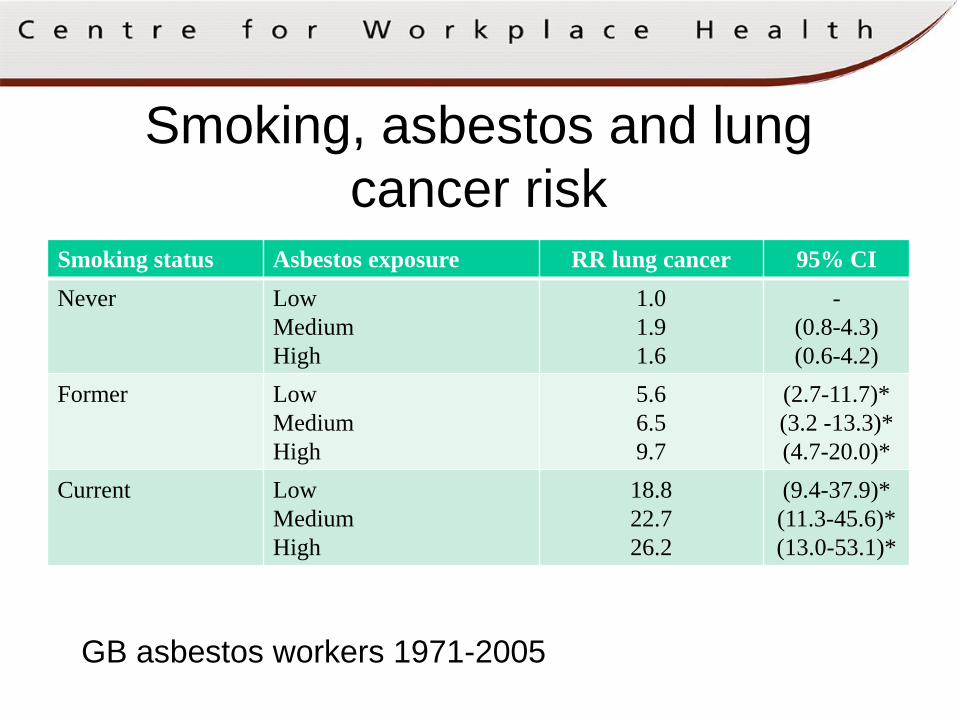
Smoking, asbestos and lung
cancer risk
GB asbestos workers 1971-2005
Smoking status Asbestos exposure RR lung cancer 95% CI
Never Low
Medium
High
1.0
1.9
1.6
-
(0.8-4.3)
(0.6-4.2)
Former Low
Medium
High
5.6
6.5
9.7
(2.7-11.7)*
(3.2 -13.3)*
(4.7-20.0)*
Current Low
Medium
High
18.8
22.7
26.2
(9.4-37.9)*
(11.3-45.6)*
(13.0-53.1)*

Mesothelioma
• Long latency (decades)
• Rapidly progressive and incurable
pleural cancer
• Lung encased by tumour
• Often presents as an unexplained
pleural effusion
• Progressive breathlessness, chest
pain, weight loss
• Average survival 8-14 months

Annual total number of mesothelioma deaths in GB was predicted to
peak at a level of 1950 to 2450 deaths during the period 2011 to 2015
Latest predictions peak 2025
OLD
• How should it be prevented?

Preventing OLD
• Risk assessment
• Legal requirement under COSHH
• Prevent or minimise exposures to harmful substances
– Elimination (eg asbestos)
– Substitution (eg latex to nitrile gloves)
– Engineering controls (eg exhaust ventilation)
– RPE (masks and respirators)

Preventing OLD
• If residual risk, monitor workers health (surveillance)
– Identify health problems early
– (eg yearly questionnaire/spirometry/CXR)
– Prevent further harm by reducing/preventing
exposure
– Review control measures to protect other
workers

Summary
• Avoidable
• Morbidity, mortality, loss of income
• Easily missed
• Seek specialist advice early
• Cure if early recognition and cease exposure
• Balance health and employment

Occupational asthma:
evidence based diagnosis and management
Interactive e-learning online module
Author: Chris Barber and Timothy Frank
Target audience:
Foundation programme
International
Practice nurse CPD
Hospital doctor CPD
GP CPD
GP trainee
Practice manager CPD















![Interstitial lung disease (ILD), or diffuse parenchymal lung disease … · 2018-10-28 · Interstitial lung disease (ILD), or diffuse parenchymal lung disease (DPLD),[[1] is a group](https://static.fdocuments.in/doc/165x107/5e7d31d2ec5074254471c7d0/interstitial-lung-disease-ild-or-diffuse-parenchymal-lung-disease-2018-10-28.jpg)


