
Obscure Upper GI Bleeding a result of his recurrent UGIB, he had chronic anemia and he was對...
25
Obscure Upper GI Bleeding Finding the Bloody Mess Marilyn Ng, MD Dept. of Surgery M&M Conference Downstate Medical Center December 22, 2011 www.downstatesurgery.org
Transcript of Obscure Upper GI Bleeding a result of his recurrent UGIB, he had chronic anemia and he was對...

Obscure Upper GI Bleeding Finding the Bloody Mess
Marilyn Ng, MD
Dept. of Surgery M&M Conference
Downstate Medical Center
December 22, 2011
www.downstatesurgery.org

Case Presentation
Xx yo cachetic man admitted to
Medicine service for weakness
Coffee – ground emesis
Profound anemia with Hct 17
On octreotide & iron therapy
www.downstatesurgery.org
Presenter
Presentation Notes
This is a case of 75 yo cachetic man who was admitted from the PMD office to the Medicine service for weakness and intermittent episodes of coffee-ground emesis without melena at home. Laboratory work revealed profound anemia with Hct 17. He was already on octreotide and iron replacement therapy with a fair response following an extensive negative diagnostic workup for obscure GI bleeding.

AF BP 75/46 HR 73 PO2 100% RA
NAD, pallor, AAO x 3
Chest: RR, barrel chest
Lungs: decreased BS @ right base
Abd: normal
On Physical Exam www.downstatesurgery.org
Presenter
Presentation Notes
On physical exam he was afebrile, hypotensive and saturating at 100% on RA. He was pale and had decreased breath sounds at the right base, but otherwise had a normal exam.

Case Presentation
PMHx: CAD s/p PCI, CHF, A-fib, HTN,
anemia, mitral regurgitation, chronic
hyponatremia, pneumonia
SHx: MV & AV repair; PPM / AICD;
right CEA; appendectomy
SocHx: denies
www.downstatesurgery.org
Presenter
Presentation Notes
He had an extensive past medical history, which included CAD, CHF, atrial fibrillation not on anticoagulants, HTN, chronic IDA, severe mitral regurgitation, chronic hypnatremia and pneumonia. Not to mention his GI bleeding history, which we review shortly. His past surgical history included mitral and aortic valve repair, right carotid endartectomy and appendectomy. He denied any toxic habits.

His Upper GI Maladies ….
Esophagitis & erosive gastritis
Diffuse gastric & duodenal AVM (2009)
30 subsequent EGD + APC / cautery
Weekly PRBC transfusions = 100+ units!
www.downstatesurgery.org
Presenter
Presentation Notes
He had long suffered from episodes of esophagitis and erosive gastritis and was initially diagnosed in 2009 with angiodysplasia in his stomach and duodenum. As time progressed, his gastric angiodysplasia developed multiple, diffuse with some angiodysplasia noted in his duodenum. He underwent 30 subsequent EGDs (at monthly intervals) with argon plasma coagulation and bipolar cauterization of bleeding ulcers and angiodysplastic lesion. As a result of his recurrent UGIB, he had chronic anemia and he was started on iron replacement therapy and octreotide therapy. However, he still required near weekly PRBC transfusions totally 100+ units over the past 2 years.

Surgical Intervention
Negative EGD & bleeding scan
Pre-op PRBC transfusions
Total gastrectomy
Roux - en - Y reconstruction
Hunt – Lawrence pouch
www.downstatesurgery.org
Presenter
Presentation Notes
Cardiac risk stratification was obtained in anticipation of surgery, and he was deemed fit by the cardiologist. During his hospitalization, he received multiple PRBC transfusions and had a repeat EGD and a bleeding scan that were both negative Surgery consult was obtained and we performed an open total gastrectomy with a Roux-en-Y reconstruction and J-pouch (aka Hunt-Lawrence pouch). The roux limb was 60 cm long and the J-pouch was 20 cm long.

Post - Op Course POD #1: TPN
POD #2: Extubated
POD #4: Negative UGI series
POD #9: Tolerated nectars
POD #10: Transferred to Medicine
POD #14: Negative EGD & stable Hct
www.downstatesurgery.org
Presenter
Presentation Notes
The patient’s post-op course was as follows: On POD#1 he was started on TPN to improve his malnutrition while remaining NPO (Pre-op prealbumin 14.1 and albumin 2.8). He was extubated on POD#2. On POD#4, he underwent a upper GI series, which was negative for leak but did show reflux from the pouch. He was advanced to nectars as suggested by speech & swallowon POD#9. He was transferred the following day with stable Hct. Of note, GI repeated an EGD on POD#14, which demonstrated no bleeding.

Obscure GI Bleeding (OGIB)
Bleeding of unknown source
Negative upper & lower endoscopy
Occult OGIB Iron – deficient anemia (IDA)
Positive FOBT
Overt OGIB Visible bleeding Pasha SF, et al. Gastroenterol Hepatol, 2009.
www.downstatesurgery.org
Presenter
Presentation Notes
OGIB is defined as: bleeding of unknown origin that persists or recurs after a negative initial upper endoscopy and colonoscopy. OGIB may be categorized into occult OGIB and overt OGIB. Occult OGIB may manifest itself as iron-deficiency anemia and/or with positive a fecal occult blood test. Overt OGIB is high-volume bleeding manifesting as hematemesis, melena or hematochezia without an identified source after initial endoscopy.

Presentation
Prior procedures
Radiation therapy
Family history
Nature of bleeding
Bleeding diathesis
Medication use
Comorbidities
www.downstatesurgery.org
Presenter
Presentation Notes
On presentation, a good history and physical may elucidate possible causes for GI bleeding. What is the nature of the bleeding? Is there hematemesis, coffee-ground emesis, melena? Is there a history of bleeding diathesis or chronic aspirin or NSAID use? Does the patient have other comorbidities (valvular heart disease or vasculitis) that increase the risk of GI bleeding. Had there been recent surgical procedures or radiation therapy that account for the GI bleeding. It’s also important to inquire about family history, such as inflammatory bowel disease.

All Things Considered …
Bleeding type
Duration & frequency
Severity & acuity
Transfusion requirement
Iron-deficient anemia
www.downstatesurgery.org
Presenter
Presentation Notes
After obtaining the patient’s history, patient’s management should be individualized based on several factors, including duration and frequency of bleeding, severity and acuity of bleeding, need for packed red blood cell transfusions, and the presence or absence of iron-deficiency anemia. The initial management in patients with obscure upper GI bleeding is to obtain an EGD and colonoscopy to diagnosis and potentially stop the site of bleeding.

OGIB Frequency
10 - 20% no identifiable etiology
5% of recurrent GI bleeding with no identifiable etiology
~ 75% small bowel source
70% vascular lesions
Pasha SF, et al. Gastroenterol Hepatol, 2009.
www.downstatesurgery.org
Presenter
Presentation Notes
GI bleeding leads to more than 300,000 hospitalizations per year. Despite initial upper and lower endoscopy, approximately 10-20% of these patients do not have an identified bleeding source, leading to extensive testing. Of these patient, approximately half (or 5%) of patients presenting with recurrent GI bleeding have no identifiable etiology. Almost 75% of identified sources arise from the small bowel and over 2/3 are due to vascular lesions.

Upper GI Etiology
Mitchell R, et al. J Clin Gastroenterol, 2007.
www.downstatesurgery.org
Presenter
Presentation Notes
Some identifiable causes of upper GI bleeding are the following: Esophagitis Cameron ulcers = ulcer associated with a hiatal hernia Dieulafoy lesion= large tortuous artery at the level of the the submucosa Angiodysplasias Gastric antral vascular ectasia aka watermelon stomach as seen here on endoscopy As well as the following duodenal causes: Ampullary neoplasm, distal duodenal neoplasia, aortoenteric fistula, Hemosuccus pancreaticus = GI bleeding via pancreatic duct usually 2’ pseudoaneurysm of peripancreatic arteries (GDA, RHA) and Hemobilia

Management
Iron & transfusion therapy
Estrogen
Octreotide
Bidirectional endoscopy
Imaging & angiography Concha R. J Clin Gastroenterol, 2007. Pasha SF, et al. Gastroenterol Hepatol, 2009.
www.downstatesurgery.org
Presenter
Presentation Notes
Because nearly 50% of patients with OGIB have no identifiable source after comprehensive negative diagnostic evaluation, a reasonable option of management is primarily supportive with iron replacement. Hg concentration should rise 2 after 3 to 4 weeks of supplementation, which should continue for 3 months after correction of anemia to replenish iron stores. (Elemental iron in: Ferrous fumarate 33%, ferrous sulfate 20%, ferrous gluconate 12%) PRBC transfusions is started if the patient is unresponsive to iron replacement. Criteria for transfusion in elderly: symptomatic CV deterioration, Hct <26, Hg<9 associated with history of CV disorder, and Hg<8 if an ESRD patient Medical management with hormonal and somatostatin analogues have been successful, but its use is limited in the long-term management of OGIB as 46% of patients rebleed. Use of estrogen in studies demonstrate a significant reduction of the need for blood transfusions among patients with OGIB. (The adverse side effects include gynecomastia, fluid retention, and heart failure.) Octreotide has also been shown to reduce if not eliminate transfusion requirements and is an option for those reluctant to take hormone therapy or who have not responded to it. (The mechanism of action include reducing splanchnic blood flow by inhibiting release of CCK, secretin, and vasoactive intestinal polypeptide. (Vasopressin is no longer used.) Repeat look endoscopy is warranted as there is a high rate of missed lesions on initial endoscopy and has a diagnostic yield of 35-75% for EGD and 6% for colonoscopy. If the lesion is found, cauterization of actively bleeding angiodysplasia in OGIB decreases transfusion requirements. However, the rate of rebleeding is significant even after therapeutic endoscopy, ranging from 13-34% Of note, approximately 50% (44-58%) of GI bleeding from angiodysplastic GI bleeding stops spontaneously. If the source is not found on endoscopy, further imaging may be obtained. While the above maneuvers may help, patients with OGIB present as a diagnostic and therapeutic challenge that often require repeated evaluation for recurrent bleeding and/or anemia.

Rockey, DC. Nat Rev Gastroenterol Hepatol, 2010.
In With the New … www.downstatesurgery.org
Presenter
Presentation Notes
Among the various diagnostic and therapeutic maneuvers, small bowel follow through, conventional enteroclysis and push enteroscopy (while safe) having fallen out of use secondary to poor diagnostic yield and with the introduction of better yielding modalities. These new modalities include CT enterography, enteroclysis and angiography; capsule endoscopy and balloon-assisted enteroscopy. CT scan technology for enterography, enteroclysis utilizes oral contrast for luminal distention for specific evaluation of the small bowel and its use are indicated in occult OGIB. The advantages and disadvantages of each technique are listed above.

www.downstatesurgery.org
Presenter
Presentation Notes
The development of capsule endoscopy has permitted direct visualization of the entire small bowel and OGIB is the main clinical indication for it’s use. About 79-80% of patients undergoing OGIB have OGIB. A plastic capsule containing light-emitting diodes, a lens, a camera, batteries and a RF transmitter is passively propelled by peristalsis while capturing 2 frames per second. CE’s diagnostic yield of 50-83% in OGIB. After CE-directed interventions, 50-66% pts remain transfusion free and without recurrent bleeding. There is a higher likelihood of positive findings with Hg <10, longer duration of bleeding (>6 months), more than 1 episode of bleeding, overt GIB (60 vs 46%), use of CE within 2 wks of the bleeding episode (91 vs 34%). Its use is limited by a lack of therapeutic capabilities and may be complicated by possible retention (1%), disintegration and perforation, which precludes its use in patients with obstruction or strictures. This concern may be ruled out with pre-study small bowel series or CTE. The advantages of CE are that it’s painless, requires no sedation, and may direct further therapeutics.
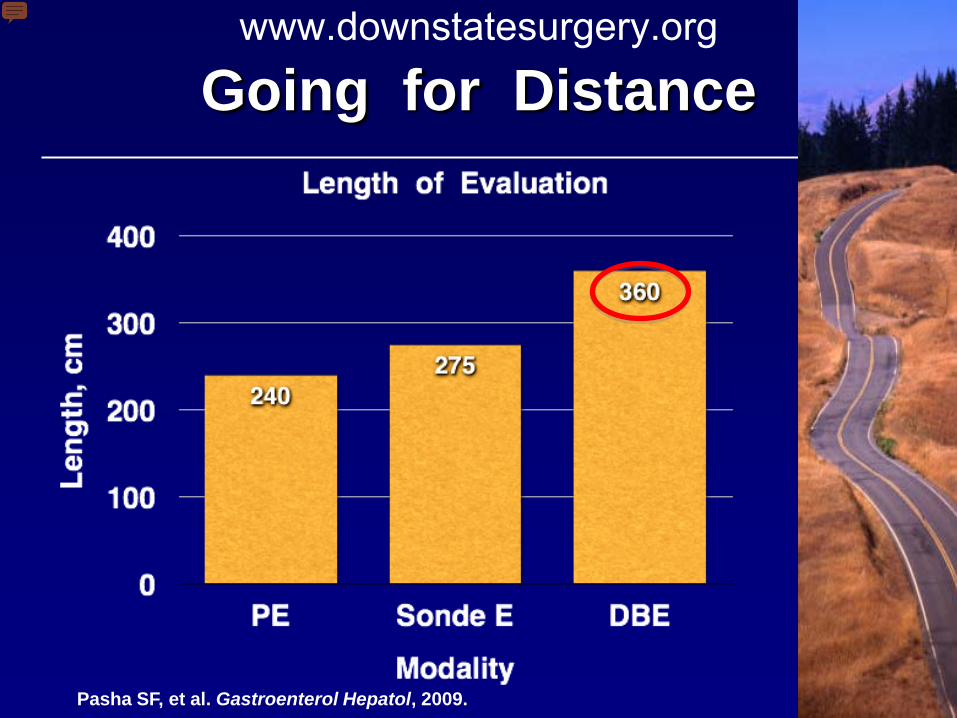
Going for Distance
Pasha SF, et al. Gastroenterol Hepatol, 2009.
www.downstatesurgery.org
Presenter
Presentation Notes
Via catheter-directed angiography or therapeutic endoscopy. While traditional endoscopy is limited by the length of the scope, even with bidirectional evaluation. Newer endoscopic devices now go the distance. The median small bowel length in humans is approximately 575 cm. Push enteroscopy allows evaluation up 10 to 50 cm of jejunum beyond the ligament of Treitz, or total length of evaluation measuring 240 cm. PE’s diagnostic yield ranges from 3-70%. Sonde enteroscopy use peristalsis to propagate the scope forward and has a longer reach, but is no longer used due to patient discomfort And now with the development of double-balloon enteroscopy (DBE), which enables the scope to be advanced and the overtube to be pulled forward, has increased evaluation of SB another 90 cm. The diagnostic yield of DBE is 60-80% and has the advantage of therapeutic capabilities. Complication rates for diagnostic procedures are 0.4% and 4% if therapeutic interventions are performed. When CE is used a prior to DBE, it has be shown to increase diagnostic yield (73-93%) and therapeutic yields (57-73%)

Pasha SF, et al. Gastroenterol Hepatol, 2009.
www.downstatesurgery.org
Presenter
Presentation Notes
BAE=balloon-assisted enteroscopy CTE=CT enteroscopy Here is a simplified algorithm for evaluating OGIB after initial endoscopy prove negative. The first, or rather the third step of choice, is capsule endoscopy after a negative small bowel follow through or conventional enteroclysis. If CE is contraindicated secondary to suspected obstruction or neoplasm, CTE may also be performed instead followed by balloon-assissted enteroscopy. If enteroscopy is negative another enteroscopy attempt should be made as lesions may be missed the first time. If CE is safe to perform the results are either positive or negative with high index of clinical suspicion, we proceed with balloon-assisted enteroscopy. BAE is also the next step if CT enterography is negative or equivocal.

Pasha SF, et al. Gastroenterol Hepatol, 2009. Garca BM, et al. Radiographics, 2010.
CT Angiography www.downstatesurgery.org
Presenter
Presentation Notes
Other modalities include RBC bleeding scan and/or angiography for evaluating severe GI bleeding. RBC nuclear scan can detect GI bleeding at a rate of 0.1-0.4 ml/min and has higher sensitivity than angiography, but permits limited localization. CT angiography may also be employed for both localization and directing treatment. However, the site and location of bleeding may still remain elusive. If bleeding is brisk, proceeding with mesenteric angiography may detect source of GI bleeding and is likely if bleeding rate is 0.5 ml/min or higher< The bleeding may be stopped with therapeutic embolization with gelfoam or coils. Localization is successful 50-75% of the time. While these new diagnostic and therapeutic modalities have signficantly reduced surgical intervention. Refractory bleeding may still require surgical intervention via intraoperative enteroscopy In younger patients, OGIB workup should include a Technetium-99 pertechnate Meckel scan.

Failed Medical Management
Then Operative Intervention !
www.downstatesurgery.org
Presenter
Presentation Notes
While we surgeons are no superheroes, consultations are requested from us after all else fails to manage and prevent recurrent anemia and GI bleeding # PRBCNeed for Sx%Mortality% 044 1-3614 4-51728 >55743

Surgical Goal
Stop persistent bleeding
Restore GI continuity
Prevent malnutrition
Increase caloric intake
Improve satiety Fein M., et al. Ann Surg, 2008.
www.downstatesurgery.org
Presenter
Presentation Notes
So that we may surgically stop persistent hemorrhage. If the source is not localized after radiographic and endoscopic evaluation, surgeons may opt to perform a laparotomy with intraoperative enteroscopy, whose diagnostic yield is 58-88%. However, rebleeding may recur in up to 60%, not to mention possible complications associated with laparotomy. The indications for surgical therapy in patients with OGIB are: Patients who require blood transfusions despite optimal iron replacement therapy Patients with associated symptoms (wt loss, abd pain) History of tumors that could metastasize to SB Because chronic GI bleeding and anemia may be debilitating, our other surgical goals included preventing further malnutrition, increasing caloric intake and improving satiety

Gertler R., et al. Am J Gastroenterol, 2009.
www.downstatesurgery.org
Presenter
Presentation Notes
If the patient has very localized area of bleeding, then a wedge resection is indicated. If the bleeding is a result of watermelon stomach which is localized to the antrum, then an antrectomy is performed with either Billroth I or Billroth reconstruction. Should the lesion be a result of diffuse angiodysplasia as found in our patient, then a total gastrectomy is warranted with reconstruction without or with a pouch.

Complications
Weight loss
Esophageal reflux
Dumping syndrome
Post – gastrectomy syndromes
Poor nutritional status
Fein M, et al. Ann Surg, 2008.
www.downstatesurgery.org
Presenter
Presentation Notes
Some of the complications following gastrectomy include weight loss, reflux, dump syndrome, other post-gastrectomy syndromes and poor nutritional status owing to lack of hunger and early satiety to name a few. These complications cause significant increase post-operative morbidity and reduce perceived quality of life.

To Pouch or Not ….
No increased morbidity or mortality
Less dumping & heartburn
Better food intake
Less weight loss
Improved quality of life Fein M, et al. Ann Surg, 2008.
www.downstatesurgery.org
Presenter
Presentation Notes
What can we do as surgeons to change life without a stomach? In a meta-analysis study of 9 RCTs comparing pouch vs no pouch following total gastrectomy, pouch procedures demonstrated no significant increase in morbidity or mortality; pts had less dumping and heart burn; and improved quality of life as measure by the Gastrointestinal Quality of Life Index (GQLI), a multi-dimensional questionnaire assessing physical, emotional and social function.

Fein M., et al. Ann Surg, 2008.
www.downstatesurgery.org
Presenter
Presentation Notes
While reconstruction with a pouch decreases morbidity and improves nutritional status, quality of life as measured by GQLI is significantly improved as well albeit 2 years after surgery.

Remember This . . .
Early endoscopy improves diagnosis
Capsule endoscopy
Surgical intervention is last resort
Happy hunting
www.downstatesurgery.org


















