nyeri dada
20
INTEGRATIVE LECTURE INTEGRATIVE LECTURE Topic: Topic: Chest Pain Chest Pain Div. Cardiology Div. Cardiology Div. Endocrinology Div. Endocrinology Div. Gastro-enterology Div. Gastro-enterology Div. Pulmonology Div. Pulmonology
-
Upload
aji-setia-utama -
Category
Documents
-
view
154 -
download
2
Transcript of nyeri dada

INTEGRATIVE LECTUREINTEGRATIVE LECTURE
Topic:Topic:
Chest PainChest Pain
Div. CardiologyDiv. CardiologyDiv. EndocrinologyDiv. Endocrinology
Div. Gastro-enterologyDiv. Gastro-enterologyDiv. PulmonologyDiv. Pulmonology

CLINICAL SCENARIOCLINICAL SCENARIO
CASE:CASE:
A 45 years-old man came to your clinic, because of A 45 years-old man came to your clinic, because of chest discomfort.chest discomfort. He’s been having this symptom He’s been having this symptom since 3 hours prior to admission. He felt burning since 3 hours prior to admission. He felt burning pain and heaviness substernally and radiated to pain and heaviness substernally and radiated to epigastrium. He is heavy smoker and history of epigastrium. He is heavy smoker and history of high blood sugar was noted since 5 years ago. high blood sugar was noted since 5 years ago. The blood sugar was not well controlled. The blood sugar was not well controlled.

CLINICAL SCENARIOCLINICAL SCENARIO
PHYSICAL EXAMINATION:PHYSICAL EXAMINATION:
BP = 175/100 mmHg; pulse = 98 bpm; BP = 175/100 mmHg; pulse = 98 bpm; respiration = 18/minrespiration = 18/min
SS1 1 and Sand S2 2 were single, apical impulse was not were single, apical impulse was not
displaceddisplaced
Neither murmur nor rales notedNeither murmur nor rales noted
1.1. What is the differential diagnosis of this gentleman? What is the differential diagnosis of this gentleman? 2.2. What do you want to do first?What do you want to do first?

Differential Diagnosis of Px Admitted to Hospitals with Acute Chest Pain Differential Diagnosis of Px Admitted to Hospitals with Acute Chest Pain Ruled Not Myocardial Infarction (dd/ nyeridada akut selain infark miokard)Ruled Not Myocardial Infarction (dd/ nyeridada akut selain infark miokard)
DIAGNOSIS PERCENT
1. Gastro-esophageal disease 42
a. Gastro-esophageal reflux (30)
b. Esophageal motility disorders (13)
c. Peptic ulcer (10)
d. Gall-stones (5)
2. Coronary Artery Disease 31
3. Chest wall syndromes 28
Harrison’s Principle of Internal Medicine, 15th edition

Differential Diagnosis of Px Admitted to Hospitals Differential Diagnosis of Px Admitted to Hospitals with Acute Chest Pain with Acute Chest Pain
Ruled Not Myocardial InfarctionRuled Not Myocardial Infarction
DIAGNOSIS PERCENT
5. Pericarditis 4
6. Pleuritis/pneumonia 2
7. Pulmonary embolism 2
8. Lung cancer 1.5
9. Aortic aneurysm 1
10. Aortic stenosis 1
11.Herpes zoster 1
Harrison’s Principle of Internal Medicine, 15th edition

Typical Clinical Features of Major Causes of Typical Clinical Features of Major Causes of Acute Chest DiscomfortAcute Chest Discomfort
Condition Duration Quality Location
UAP 10-20 min pressure retro-sternal
tightness (ksesakan),
heaviness
AMI > 30 min more severe retro-sternal
Esophageal reflux 10-60 min burning sub-sternal
epigastric
Esophageal spasm2-30 min burning retro-sternal
pressure
Musculo-skeletal synd variable aching (sakit) variableHarrison’s Principle of Internal Medicine, 15th edition

Typical Clinical Features of Major Causes of Typical Clinical Features of Major Causes of Acute Chest DiscomfortAcute Chest Discomfort
Condition Duration Quality Location
Pleuritis/pneumonia variable pleuritic unilateral/
localized
Pulmonary embolism abrupt onset pleuritic lateral
minutes – hours side of embolism
Emotional/psychiatric
conditions variable, may be variable variable
fleeting retrosternal
Harrison’s Principle of Internal Medicine, 15th edition

What procedures do you want to do first?

DIAGNOSTIC PROCESS IN ACUTE DIAGNOSTIC PROCESS IN ACUTE CORONARY SYNDROMESCORONARY SYNDROMES
CHEST DISCOMFORTCHEST DISCOMFORT
HISTORY & PE & ECG & ENZYMESHISTORY & PE & ECG & ENZYMES
ST ELEVATIONST ELEVATION NON-ST ELEVATIONNON-ST ELEVATION
PRESUMED AMIPRESUMED AMI= STEMI= STEMI
SAMPLE ENZYMESSAMPLE ENZYMES
POSitive-ENZYMESPOSitive-ENZYMES NEGative-ENZYMESNEGative-ENZYMES
UAPUAPGa adaGa ada
NONNONCARDIAC-PAINCARDIAC-PAIN
NSTEMI NSTEMI (ada peningkatan enzim2 hati)(ada peningkatan enzim2 hati)

Eelectrocardiogram

CHEST X-RAY : frontal viewCHEST X-RAY : frontal view

CLINICAL SCENARIOCLINICAL SCENARIO
LABORATORY:LABORATORY: Hb = 15.5 gr%; WBC = 9800; ESR = 30 mm/hHb = 15.5 gr%; WBC = 9800; ESR = 30 mm/h Urinalysis: Urinalysis: glucosuria (++) glucosuria (++) Random Blood Sugar = Random Blood Sugar = 350 mg/dL350 mg/dL; ; Ureum/creatinin = normalUreum/creatinin = normal CK (creatinin kinase) – MB = 15 IU (< 25 IU)CK (creatinin kinase) – MB = 15 IU (< 25 IU) LDH = 125 IU (120 – 240 IU)LDH = 125 IU (120 – 240 IU) Na = 128 meq/L ; K+ = 4.2 meq/L Na = 128 meq/L ; K+ = 4.2 meq/L
What is the most likely diagnosis?What is the most likely diagnosis?

NOMENCLATURE OF ACS

DIAGNOSIS :1. Unstable Angina Pectoris2. Hypertension stage 23. Diabetes Mellitus
TREATMENT ???

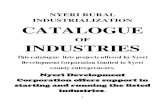
-35%
-30%
-25%
-20%
-15%
-10%
-5%
0%
any
dia
bet
es
end
po
ints
MI
mic
ro
vasc
ula
rs
Ret
inal
lase
r
cata
ract
Mic
roal
bu
min
uri
a
12%
16%
25%
29%
24%
33%
UKPDS:UKPDS:Glucose Control Study SummaryGlucose Control Study Summary
P=0.029
P=0.052
P=0.0099
P=0.0031
P=0.046
P<0.001

Joint National Committee VII (JNC-VII)U . S . D E PARTME NT OF H EALTH AND HUMAN S E RV I C E S; National Institutes of HealthNational Heart, Lung, and Blood Institute

TREATMENT OF UAP in ICU:TREATMENT OF UAP in ICU:
1. OXYGEN 2 – 4 L/m via O2 masker1. OXYGEN 2 – 4 L/m via O2 masker2. ASPIRIN 100 – 160 mg/d or other anti platelet2. ASPIRIN 100 – 160 mg/d or other anti platelet3. ISOSORBID DINITRATE via syringe pump3. ISOSORBID DINITRATE via syringe pump
2 – 4 mg/h2 – 4 mg/h4. BETA BLOCKERS: 4. BETA BLOCKERS:
Atenolol 50 – 100 mg OD Atenolol 50 – 100 mg OD Metoprolol 50 – 100 mg ODMetoprolol 50 – 100 mg ODBisoprolol 5 – 10 mg ODBisoprolol 5 – 10 mg OD
5. HEPARIN or LWM-HEPARIN5. HEPARIN or LWM-HEPARINEnoxaparin 1 mg/kg BW/12 hourslyEnoxaparin 1 mg/kg BW/12 hoursly
6.CALCIUM BLOCKERS 6.CALCIUM BLOCKERS if pain persist if pain persistDiltiazem 30 – 90 mg TIDDiltiazem 30 – 90 mg TIDAmlodipine 5 – 10 mg ODAmlodipine 5 – 10 mg ODVerapamil 80 mg TID Verapamil 80 mg TID

TREATMENT OF DIABETES MELLITUS IN Acute Coronary Syndromes

CLINICAL SCENARIOCLINICAL SCENARIO
During hospitalization During hospitalization at 5 at 5thth hospitalisation day: hospitalisation day: He suffered from nausea, epigastrial pain and He suffered from nausea, epigastrial pain and bloody vomiting bloody vomiting Vital signs were still normalVital signs were still normal
What is the most likely diagnosis?What is the most likely diagnosis?
What is the initial treatment?What is the initial treatment?
What procedure do you want to suggest?What procedure do you want to suggest?

Sources of Bleeding in Sources of Bleeding in Acute Upper Gastrointestinal BleedingAcute Upper Gastrointestinal Bleeding
Sources of Bleeding Proportion of Px (%)
Ulcers 36 – 62
Varices 4 - 31
Mallory – Weiss tears 4 - 13
Gastro-duodenal erosions 3 - 11
Erosive esophagitis 2 - 8
Malignancy 1 - 4
No source identified 7 - 25
Harrison’s Principle of Internal Medicine, 15th edition