NUOVI CRITERI DIAGNOSTICI E PROGNOSTICI NEL MIELOMA … · Bone Marrow Plasma Cells (%)...
51
Percorsi diagnostico-terapeutici nel Mieloma Multiplo nella regione Liguria Genova 28 Novembre 2018 2018 NUOVI CRITERI DIAGNOSTICI E PROGNOSTICI NEL MIELOMA MULTIPLO Elena Zamagni “ Seràgnoli ” Institute of Hematology Bologna University School of Medicine
Transcript of NUOVI CRITERI DIAGNOSTICI E PROGNOSTICI NEL MIELOMA … · Bone Marrow Plasma Cells (%)...

Percorsi diagnostico-terapeutici nel
Mieloma Multiplo
nella regione Liguria
Genova
28 Novembre
20182018
NUOVI CRITERI DIAGNOSTICI E
PROGNOSTICI NEL MIELOMA MULTIPLO
Elena Zamagni
“Seràgnoli” Institute of Hematology
Bologna University School of Medicine

DRUGS DEVELOPMENT IN MULTIPLE MYELOMA

< 3 g/dL serum
AND
MonoclonalGammopathy of
uncertain significance(MGUS)
Present(serum/urine)
AND
SymptomaticMultipleMyeloma
≥ 3 g/dL serum
AND/OR
Smoldering Multiple
Myeloma (SMM)
Monoclonal component
Classification of monoclonal gammopathies
AND
< 10%
AND
Absent
> 10%b
AND
Present
10-60%
AND
Absent
Bone MarrowPlasma Cells (%)
Mieloma-defining event (CRAB)
Concomitant diseases that can mimic MM:-Increase of serum Cr due to diabetes or hypertension-Anemia due to idon-vitamin deficiency, chronic disease,..
-Diffuse osteoporosis-Hyperparatiroidism-Single asymptomatic bone lesion
Kyle RA, IMWG, BJH 2003
Absent

REVISED IMWG DIAGNOSTIC CRITERIA
Rajkumar V et al, Lancet Oncol 2014

Wester R and Sonneveld P Haematologica 2016;101(5):518-20.

IMWG MRD criteria
Response SubCategory Response Criteria
Sustained MRD-negative MRD negativity in the marrow (NGF or NGS, or both) and by imaging as
defined below, confirmed minimum of 1 year apart. Subsequent evaluations
can be used to further specify the duration of negativity (eg, MRD-negative
at 5 years)†
Flow MRD-negative Absence of phenotypically aberrant clonal plasma cells by NGF‡ on bone
marrow aspirates using the EuroFlow standard operation procedure for MRD
IMWG MRD negativity criteria
(requires a complete response)
marrow aspirates using the EuroFlow standard operation procedure for MRD
detection in multiple myeloma (or validated equivalent method) with a
minimum sensitivity of 1 in 10⁵ nucleated cells or higher
Sequencing
MRD-negative
Absence of clonal plasma cells by NGS on bone marrow aspirate in which
presence of a clone is defined as less than two identical sequencing reads
obtained after DNA sequencing of bone marrow aspirates using the
LymphoSIGHT platform (or validated equivalent method) with a minimum
sensitivity of 1 in 10⁵ nucleated cells§ or higher
Imaging positive
MRD-negative
MRD negativity as defined by NGF or NGS plus disappearance of every area
of increased tracer uptake found at baseline or a preceding PET/CT or
decrease to less mediastinal blood pool SUV or decrease to less than that of
surrounding normal tissue
Kumar SK, et al. Lancet Oncology 2016;17(8):e328-e346

Transition from MGUS/SMM to MM
Genetic events: genetic instability, accumulation of abnormalities
Epigenetic events
Clonal selection: expansion of altered clones already present in MGUS
Permissive microenvironment
Ghobrial I et al, Blood 2014
Ahn IE et al, JCO 2015
Bianchi G et al, Blood 2015
Permissive microenvironment
Reduction of immune surveillance

MGUS: Evolution in whom and at what rate?
However, majority doesnot develop MM
MGUS 1%/year
Kyle RA et al. NEJM 2007Proposed risk factors:
-Monoclonal-(M)-spike 1.5 g/dl or higher
-Skewed FLC-ratio (ref 0.26-1.65)
-Immunoparesis
-Non-IgG M-spikeLandgren O et al. Clin Cancer Res 2011
Kyle RA et al, NEJM 2018
MGUS 1%/year


SMM: Heterogeneus disease
3%/year from 5-10 years1%/year thereafter
Perez-Persona E, et al. Blood. 2007;110:2586-92.
10%/year

PROGNOSTIC FACTORS OF PROGRESSION IN SMM
• MC concentration (cut-off 3 g/dL)
• Changes in MC over time (“evolving pattern”): progressive increase of atleast 10% in the first 6 months if initial MC > 3g/dL or progressive annualincrease within 3 years if MC < 3 g/dL
• FLC ratio alteration
• BM plasma cells
• MRI FLs• MRI FLs
• Immunoparesis
• Presence of Proteinuria, in particular if > 500 mg/24h (NO PROGNOSTICVALUE OF BJ POSITIVITY!)
• Aberrant BM PCs phenotype
• Cytogenetic abnormalities
Rajkumar V et al, Blood 2005
Gonzalez de la Calle et al, Leukemia 2016
Rosinol L et al, Mayo Clinic Proc 2007
Dhodapkar MV et al, Blood 2014
Kyle R et al, NEJM 2007
Vd Donk et al. Haematologica 2014;99:984-996
Fernández Larrea C et al. ASH 2014

Ultra-high risk SMM
Use the higher value if discrepancy between
BM aspiration and biopsy
Median TTP: 55 m
Median TTP: 15 m
Median TTP: 7 m
1. Rajkumar SV et al. N Engl J Med 2011; 365:474-475
2. Kastritis E, et al. Leukemia. 2013 Apr;27(4):947-53
3. Waxman AJ, et al. J Clin Oncol 32:5s, 2014 (suppl; abstr 8607)
4. Larsen JT at al, Leukemia 2013
5. Hillengass J, et al. J Clin Oncol 2010;28:1606-1610
6. Kastritis E, et al. Leukemia. 2013 Apr;27(4):947-53
Median TTP: 13 m
Median TTP: NR
Pro
gres
sion
-fre
e su
rviv
al
Time since MRI Treatment (months)
1.0
60 1812 3024 4236 5448 60
0.8
0.6
0.4
0.2
0
> 1
Log-rank p < 0.001
Whole MRI: FLs

PROGNOSTIC VALUE OF WBMRI: IMPORTANCE OF FOLLOW-UP
Critical evaluation of doubt lesions!

REVISED IMWG DIAGNOSTIC CRITERIA: BIOMARKERS OF MALIGNANCY
Rajkumar , Lancet Oncol 2014

Definition of high risk SMM
RajKumar V S et al, Blood 2015

Smoldering Multiple Myeloma: prognostic factors
Evolution pattern of the M-spike: evolving vs non evolving (n:206)
• Evolving SMM (25%): at least 10% increase in the M-protein size within the first 12months from diagnosis when baseline M- protein was ≥ 30 g/L or progressive increasein MP in each of the annual consecutive measurements during a period of 3 years inpatients with an initial MP < 30 g/L
• Non-evolving (75%): Stable serum M-protein until progression occurs
Evolving SMM
• Risk progression at
Pro
babi
lity
of p
rogr
essi
on
• Risk progression at 2 years: 45%
• Risk progression at 5 years: 78%
• IgA isotype: 38% vs.
24%; p=0.061
Fernández Larrea C et al. Leukemia. 2018
Pro
babi
lity
of p
rogr
essi
on
Evolving SMM
Non-evolving SMM

Smoldering Multiple Myeloma: prognostic factors
Bence Jones proteinuria in SMM as a predictor marker of progression to symptomatic MM
González- Calle V et al. Leukemia 2016

• del(17p13), t(4;14), +1q21 showed significant impact on TTP
TTP P
All pts 4.9 years
+1q21 versus no gain of 1q21 3.7 years 5.3 years 0.013
del(17p13) versus no del(17p13) 2.7 versus 4.9 years 0.019
Del(17p), t(4;14), and +1q21 predict progression from smoldering to symptomatic MM (n=248)
Smoldering Multiple Myeloma: prognostic factors
• Multivariate analysis: t(4;14), +1q21, HD, reduction of uninvolved immunoglobulins and risk score defined by Kyle et al. as independent factors for adverse outcome
• Conclusion: specific chromosomal aberrations drive transition from asymptomatic to symptomatic disease
t(4;14) versus no t(4;14) 2.9 versus 5.2 years 0.021
HD versus NHD 3.9 versus 5.7 years 0.036
Neben et al. JCO 2013

� No uniform accepted definition of high-risk or intermediate-risk SMM1
% Progressing to Symptomatic MM
Mayo Clinic2
3 Criteria:1/3 Criteria(Low risk)
2/3 Criteria(Intermediate
risk)
3/3 Criteria(High risk)
1. M-protein ≥3 g/dL2. ≥10% clonal bone
marrow plasma cells 25% 51% 76%
Risk models for the stratification of SMMSmoldering Multiple Myeloma: prognostic factors
marrow plasma cells3. Free light-chain
<0.125 or >8
25% 51% 76%
PETHEMA3
2 Criteria:0/2 Criteria(Low risk)
1/2 Criteria(Intermediate
risk)
2/2 Criteria(High risk)
1. ≥95% abnormal plasma cells
2. Low uninvolved serum immunoglobulins
4% 46% 72%
1. Rajkumar SV, et al. Blood. 2015;125(20):3069-3075;2. Dispenzieri A, et al. Blood. 2008;111(2):785-789; 3. Pérez-Persona E, et al. Blood. 2007;110(7):2586-2592.
TTP 1,9 yTTP: 5 yTTP 10 y

IMF Smoldering Multiple Myeloma (SMM) retrospective chart review

New Paradigm for SMM: risk-adapted approach
Low Risk
Smoldering Myeloma (14%)*
Stratification according to risk of progression
Intermediate Risk High Risk
Ultra-high risk (5-10%) =
MM
Kristinsson S Y et al NEJM 2013Ghobrial I et al, Blood 2014 Rajkumar V et al, Blood 2015 *Using the Swedish Myeloma registry, 2494 pts from 2008 to 2011
Low Risk(40%)
• TTP 25% at 5 yrs• Follow up as
MGUS (6-12 mos)
Intermediate Risk(30%)
High Risk(30%)
• TTP 50% at 5 yrs• Close follow up
every 3-6 months
• TTP 70% at 5 yrs• Candidates for clinical
trials (early treatment)

High-risk SMM seems to benefit from therapy. However, there are still fundamental questions for which wedo not yet have clear answers:
• What is the most appropriate treatment?
Shall we treat smoldering multiple myeloma in the near future?Ola Landgren
2017
Clinical trials and long term follow-up are needed to address these important questions
• What is the most appropriate treatment? • Instead of using powerful 3-drugs therapy, is it enough to use more gentle therapy (eg, a 2-drug combination)?• What is the optimal duration?• In case of a recurrence, can therapy be resumed with the same efficacy?
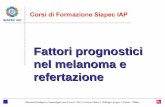
SMM: future directionsCurrent paradigm Proposed future directions
High-risk SMM MM (early detection)
Intermediate-risk SMM Indolent MM
Low-risk SMM Monoclonal gammopathy
Landgren O, ASH 2017
Dispenzieri A, Blood 2014

IMWG: M-protein, bone marrow plasma cells, and
organ impairment define plasma cell disorder
• < 10% BMPC AND
• < 3 g/dL M protein AND
• No MDE
• ≥ 10% to 60% BMPC OR
• ≥ 3 g/dL serum M protein OR
• ≥ 500 mg/24 hr urine M protein AND
• No MDE
• PCPD, AND
• 1 or more MDE
o CRAB
o ≥ 60% BMPC
o ≥ 100 FLC ratio
MGUS SMM MM
Rajkumar SV, et al. Lancet Oncol. 2014;15:e538-e548.
o ≥ 100 FLC ratio
o > 1 MRI focal lesion
MDE, myeloma-defining events
No MDE MDE

REVISED IMWG DIAGNOSTIC CRITERIA: from CRAB to slim- CRAB to MDE
MDE
Rajkumar , Lancet Oncol 2014
CRAB

• Definition of myeloma bone disease (CRAB):clear evidence of one or more sites of osteolytic bone destruction (at least 5 mm or more in size) seen on CT, WBLDCT, PET/CT, regardless of weather they can be visualized on skeletal radiography or not
REVISED IMWG DIAGNOSTIC CRITERIA: new definition of MDE
Bone disease
Rajkumar V. et al., Lancet Oncology 2014
• If doubt lesions on CT or PET/CT: close follow-up every 3-6 months and/or biopsy of the lesion
• Oseoporosis per se not attributable to myeloma is not sufficient for CRAB

SYSTEMATIC REVIEWNEW IMAGING TECHNIQUES HAD A HIGHER DETECTION
RATE AS COMPARED TO WBXR*
* Except for ribs and skull
Regelink JC et al. BJH 2013;162:50-61.

PET/CT neg (97 pts): 30% at 2 yrs
TTP TTP
PET/CT pos (74 pts): 75% at 2 yrs
P= 0.0008 P= 0.004
PET/CT neg: median 60 mos
PET/CT pos with osteolyses (16 pts): median 21 mos (87% at 2 yrs)
Siontis B. et al, Blood Cancer J 2015

Hillengas J et al. BCJ 2017
• Retrospective analysis of 212 pts with suspected SMM studied by WBXR and WBCT within 30 days• 25% higher sensitivity of WBCT (WBXR false negative)

WHAT IMAGING TO USE FOR STAGING?

WHAT IMAGING TO USE FOR STAGING?
WBLDCT PET/CT MRI
• Widely available
• Patient-friendly (fast scanningtime, < 15 min)
• Relatively low radiation dose (3-4mSv)
• Can contemporary depict lytic lesions and disease metabolism
• Prognostic significance of FLs and SUV
• Highest sensitivity for early bone damage
• No radiation exposure
• Prognostic significance of FLs and diffuse pattern
Choice usually made according to local clinical practice, resources, expertise and national guidelines
• Relatively cheap
• No need for iv contrastadministration
• Gold standard for CT-guided biopsy,surgery, RT planning, evaluation ofstability of fractures
• Comparison with post-treatment evaluation
• Gold standard to assess EMD
• Gold standard for detection of diffuse BM involvement, differential diagnosis between osteoporotic and pathological fractures, cord compression

•Definition of renal failure:
•measured or estimated glomerular filtration rates less than 40 mL/min (which
corresponds to about a 40% decrease from the lower limit of the normal glomerular
filtration rates) be used instead of a fixed serum creatinine concentration to fulfil the
CRAB criteria
REVISED IMWG DIAGNOSTIC CRITERIA: new definition of MDE
Laboratory
•the criteria have also been updated to clarify that only renal failure caused by light-
chain cast nephropathy (based on typical histological changes or presumptive
diagnosis based on the presence of high involved FLC levels, typically >1500 mg/L) is
regarded as a myeloma-defining events.
Rajkumar SV, et al. Lancet Oncol. 2014;15:e538-e548.

Selective vs non selective
proteinuria
Dimopoulos MA et al (IMWG Consensus), J Clin Oncol 2016; 34:1544-1557MIDD, monoclonal Ig deposition disease.

DIAGNOSTIC EVALUATION

Myeloma Is Not One Disease
~ 25% pts dead in 3 yrs
Kumar SK, et al. Leukemia. 2014;28:1122-1128
> 50% ptsalive at 5 yrs

Prognostic factors in MM
Patient-related
• Age
• Performance status, comorbidities
Disease-related
• High β2 microglobulin
• Low albumin
• Renal impairment
ISSDisease burden
• Renal impairment
• LDH above the upper limit
• Cytogenetic abnormalities
• Gene expression profile
• Circulating plasma cells
• Extramedullary disease
• High proliferation rate
Therapy-related
• Quality of response
• Early relapse
Disease biology
Dynamic Model
At diagnosis

Why Risk Stratify?
• Two important goals
– Counsel: Need to provide pt with realistic expectations
based on the currently available treatments
– Therapy: Decide if particular therapies can be chosen
based on their differential effects on the high-risk and
standard-risk disease
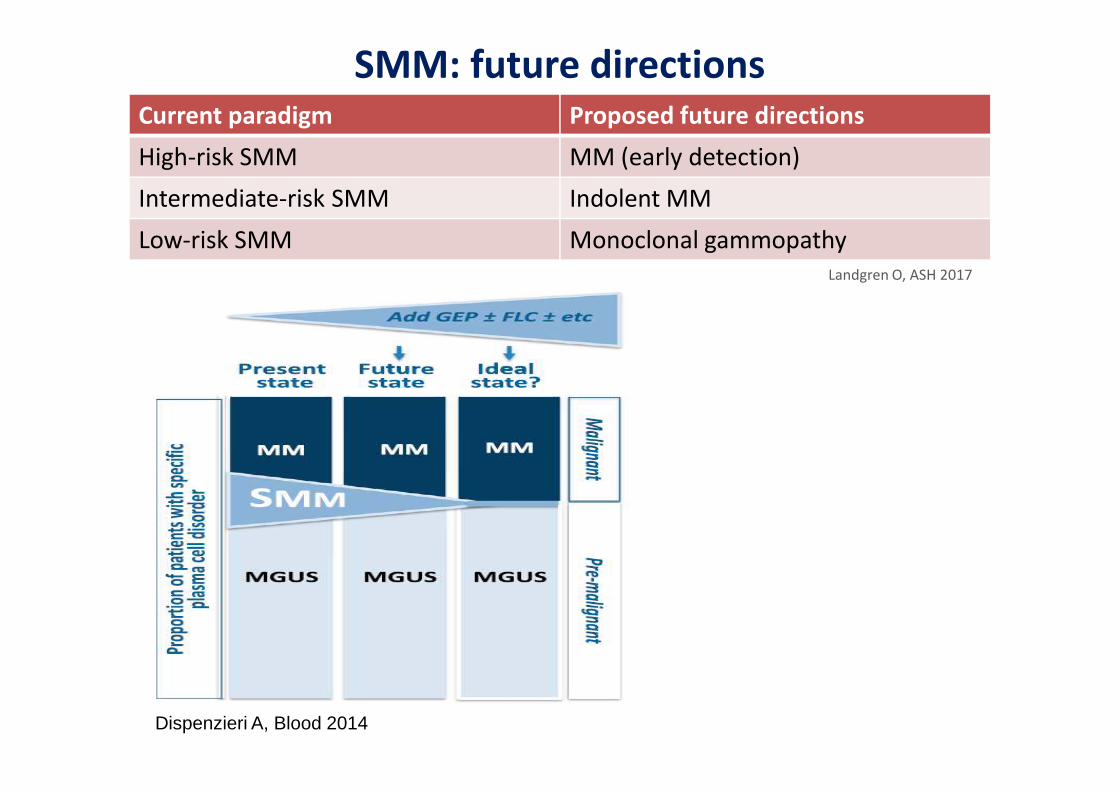
Consensus statement
•Translocations t(4;14), t(14;16), t(14;20), and del(17/17p) and any nonhyperdiploid
karyotype are HR cytogenetics in NDMM regardless of treatment.
•Gain(1q) is associated with del(1p) carrying poor risk.
•Increased risk with increased number of lesions (DOUBLE HIT MM)
•Combinations of ≥3CA confer ultra-HR with <2 years survival.•Combinations of ≥3CA confer ultra-HR with <2 years survival.
•Routine testing should include t(4;14) and del(17p).
•Clinical classifications may combine these lesions with ISS, serum LDH, or HR gene
expression signatures.
Sonneveld P, et al.. Blood 2016; 127:2955-2962
High-risk Standard-risk
Cytogenetic
abnormality
FISH: t(4;14), t(14;16), t(14;20),
del(17/17p), gain(1q)
Nonhyperdiploid Karyotipe
Karyotype del(13)
GEP: high-risk signature
All others including: FISH: t(11;14), t(6;14)

Gene Expression–Based Classifications
Signatures
• GEP70• GEP17• HOVON• HOVON• IFM
Shaughnessy JD Jr, et al. Blood. 2007;109:2276-2284.

The International Staging System (ISS)Prognostic model based on β2-microglobulin and albumin
Patients < 65 y
Stage Criteria
Iβ2m < 3.5 mg/L
& albumin ≥ 3.5 g/dL
Patients > 65 y
II Not stage I or III
III β2m ≥ 5.5 mg/L
Greipp et al. J Clin Oncol 2005;23:3412-20

Prognostic factor Criteria
ISS stage
I Serum β2-microglobulin < 3.5 mg/L; serum albumin ≥ 3.5 g/dL
II Not ISS stage I or III
III Serum β2-microglobulin > 5.5 mg/L
High riskPresence of del(17p) and/or translocation t(4;14) and/or
Standard risk factors for myeloma and the R-ISS
A total of 3,060 pts with NDMM enrolled onto 11 international, multicenter clinical trials
All patients received new drugs (IMIDs or PIs)
CA, chromosomal abnormalities; iFISH, interphase fluorescent in situ hybridisation;
ISS, International Staging System; R-ISS, Revised International Staging System.
CA by iFISHHigh risk
Presence of del(17p) and/or translocation t(4;14) and/or
translocation t(14;16)
Standard risk No high-risk CA
LDHNormal Serum LDH < upper limit of normal
High Serum LDH > upper limit of normal
A new model for risk stratification for MM
R-ISS stage
I ISS stage I, standard-risk CA by iFISH and normal LDH
II Not R-ISS stage I or III
III ISS stage III and either high-risk CA by iFISH or high LDH
Palumbo A, et al. J Clin Oncol 2015;33:2863–9.

Revised ISS staging system
28%
62%
10%
Palumbo A, et al. J Clin Oncol 2015;33:2863–9.
OS @ 5yrs
82%
62%
40%
PFS @ 5yrs
55%
36%
24%

• High-risk can refer to many different characteristics and the magnitude of risk
can be influenced by different treatmens
• There is a lack of prospective randomized trials which might strongly support
choices of therapy in this settingchoices of therapy in this setting
• Management of high-risk MM includes a complicated set of steps requiring
an aggressive treatment approach
• The short-term goal of therapy is to achieve a rapid and complete response
and then to use different treatment strategies to further deepen the level of
response and maintain it below the detection level
Sonneveld P, et al.. Blood 2016; 127:2955-2962

Depth of response correlate with survivalMRD is the best biomarker to predict outcome
Lahuerta JJ, et al. JCO 2017;35(25):2900-2910 GEM2000 - GEM2005MENOS65 - GEM2010MAS65
Meta-analysis of MRD studies (CR patients) Munshi NC, et al. JAMA Oncol 2017;3(1):28-35

PFS
MRD negativity is a prognostic marker for PFS and OS
across the spectrum of patients with MM
OS
Lahuerta JJ, et al. JCO 2017;35(25):2900-2910

MRD SHOULD BE EVALUATED INSIDE AND OUTSIDE
THE BONE MARROW IN MULTIPLE MYELOMA
4
6
Rasche L et at, Nature Comm 2017 Growing heterogeneity with growing size of the lesions

FDG PET/CT FOR EVALUATION OF METABOLIC RESPONSE TO THERAPY AND MRD
both negative (47% pts)
either positive
COMPLEMENTARITY BETWEEN PET/CT AND BM FLOW CYTOMETRY*
Newly diagnosed transplant-eligible patients evaluated
4
7
Moreau P. et al, JCO 2017
patients evaluated pre-maintenance
*Sensitivity 10-4

• Who are the patients at risk of persistence of disease metabolism in FLs(imaging MRD positivity)?
• Those with EMD at diagnosis
• Those with para-skeletal disease
Patient 359 454 502 635 751 767
Diagnosis
ISS III III I III I I
1q+(50%) 1q+(85%) &
4
8
Relapse
M-protein - - + - - +
MRD (NGF, 10-
6)neg neg neg neg neg neg
Bone-relatedplasmacytomas
+ + + + NE +
FISH 1q+(59%) del17p(22%)1q+(50%)
& 1p-(61%)1q+(85%) &
1p-(89%)NE -
Bone-related plasmacytomas
+ + + + NE +
Paiva B et al, presented at ASH 2017

WHAT IMAGING TO USE AFTER TREATMENT?
PET/CT FUNCTIONAL MRI
• Results reproduced in large
prospective independent studies
• Higher reliability for diffuse BM
infiltration
• Early changes during treatment
4
9
• Prognostic significance in CR
patients (MRD monitoring) and
complementarity with bone
marrow techniques
• Small studies in heterogeneous
patient populations to date
PET/CT has the strongest recommendation to date

Table 6: Recommendations for use of 18F-FDG PET/CT in MM
Recommendation Grade
Active MM:
18F-FDG PET/CT can be considered as part of the initial workup in patients with newly diagnosed MM since itprovides information useful for prognostication and allows to more carefully assess the bulk of the disease,particularly in patients with extramedullary sites of the disease. This latter indication for use of 18F-FDG PET/CTapplies also to patients with relapsed/refractory MM
B
In newly diagnosed MM, EMD and >3 FLs on 18F-FDG PET/CT identify subgroups of patients with unfavorableoutcomes, particularly those who are candidates to receive upfront ASCT. Controversies exist about theprognostic role of SUVmax
B
18F-FDG PET/CT is by now the preferred technique for evaluating and monitoring response to therapy. Metabolicchanges assessed by 18F-FDG PET/CT provide an earlier evaluation of response compared to MRI
A
18F-FDG PET/CT should be coupled with sensitive bone marrow-based assays as part of MRD detection insideand outside the bone marrow
B
Cavo M. et al, Lancet Oncology 2017

Actions to achieve, maintain MRD negativity and
improve the prognosis• Integrate all active treatment tools up-front through:
• Sequential blocks of therapy
• Combination regimens
• Inclusion of new novel-agents:
• Second generation PI
• Monoclonal Ab
• Most effective treatments at relapse
• To treat the disease early on:
• In most malignancies early detection and intervention is a pre-requisite for
cure
• Design of more individualized approach :
• Risk-adapted treatment strategies
• MRD-adapted treatment strategies